
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr. , 18 March 2022
Sec. Pediatric Surgery
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.849992
This article is part of the Research Topic Pediatric Thoracic Surgery View all 12 articles
 Martin Riis Ladefoged1,2*
Martin Riis Ladefoged1,2* Steven Kwasi Korang1,3
Steven Kwasi Korang1,3 Simone Engmann Hildorf4Jacob Oehlenschlæger4
Simone Engmann Hildorf4Jacob Oehlenschlæger4 Susanne Poulsen5
Susanne Poulsen5 Magdalena Fossum2,4,6
Magdalena Fossum2,4,6 Ulrik Lausten-Thomsen5
Ulrik Lausten-Thomsen5Background: Esophageal atresia is corrected surgically by anastomosing and recreating esophageal continuity. To allow the removal of excess fluid and air from the anastomosis, a prophylactic and temporary intraoperative chest tube (IOCT) has traditionally been placed in this area during surgery. However, whether the potential benefits of this prophylactic IOCT overweigh the potential harms is unclear.
Objective: To assess the benefits and harms of using a prophylactic IOCT during primary surgical repair of esophageal atresia.
Data Sources: We conducted a systematic review with a meta-analysis. We searched Cochrane Central Register of Controlled Trials (2021, Issue 12), MEDLINE Ovid, Embase Ovid, CINAHL, and Science Citation Index Expanded and Conference Proceedings Citation Index—(Web of Science). Search was performed from inception until December 3rd, 2021.
Study Selection: Randomized clinical trials (RCT) assessing the effect of a prophylactic IOCT during primary surgical repair of esophageal atresia and observational studies identified during our searches for RCT.
Data Extraction and Synthesis: Two independent reviewers screened studies and performed data extraction. The certainty of the evidence was assessed by GRADE and ROBINS-I.
PROSPERO Registration: A protocol for this review has been registered on PROSPERO (CRD42021257834).
Results: We included three RCTs randomizing 162 neonates, all at overall “some risk of bias.” The studies compared the placement of an IOCT vs. none. The meta-analysis did not identify any significant effect of profylacitic IOCT, as confidence intervals were compatible with no effect, but the analyses suggests that the placement of an IOCT might lead to an increase in all-cause mortality (RR 1.66, 95% CI 0.76–3.65; three trials), serious adverse events (RR 1.08, 95% CI 0.58–2.00; three trials), intervention-requiring pneumothorax (RR 1.65, 95% CI 0.28–9.50; two trials), and anastomosis leakage (RR 1.66, 95% CI 0.63–4.40). None of our included studies assessed esophageal stricture or pain. Certainty of evidence was very low for all outcomes.
Conclusions: Evidence from RCTs does not support the routine use of a prophylactic IOCT during primary surgical repair of esophageal atresia.
Esophageal atresia refers to a group of congenital anomalies in which the continuity of the esophagus is interrupted (1). Tracheoesophageal anomalies are divided into subtypes depending on anatomy and the most prominent (85%) subtype has a tracheoesophageal fistula to the distal esophageal segment (1). The prevalence of esophageal atresia varies according to country and time period (2–8). Observational studies from 1981 to 2018 have estimated the prevalence to span from 0.88 to 4.55 per 10,000 births in China and in Germany, respectively. Recent European studies suggest that the prevalence is relatively stable over time (9–11) and that males are most affected with a male:female ratio of 1:0.74 (9).
At birth, the neonate presents with typical drooling of saliva, inability to swallow, choking, coughing, cyanotic attacks, and distended abdomen if the subtype involves a fistula to the trachea (11). The diagnosis is confirmed by the inability to pass a feeding tube into the stomach (11, 12) and a plain X-ray showing the non-progression of the feeding tube located in a blind-ending pouch (11, 12). Prenatal diagnostics having improved from 26 to 36% during the last 30 years (9). Postnatal diagnosis occurs on the first day after birth in 83% of cases, the remaining 15% of cases within the first week, and only in 1.2% after the first week (9).
Most cases seem to occur sporadically, therefore the etiology is likely to be multifactorial involving multiple genes and complex gene-environment interactions (13, 14). Despite observational studies suggesting various maternal risk factors (10, 13, 15), the exact etiology is still unclear (13, 14). Since esophageal atresia is an early organogenesis defect, associated anomalies are frequency found (9, 16–19). Isolated esophageal atresia occurs in ~45–53% of the cases, whereas 32–47% have multiple anomalies, and 24–25% have an association or a syndrome, the most common being VACTERL association occurring in ~10% (9, 16–21). Among the most common associated anomalies are congenital heart defects (23–29% of cases), other gastrointestinal anomalies (16–21%), urinary tract anomalies (15–16%), and limb anomalies (13–14%) (9, 16–19).
Left untreated, the condition is fatal due to starvation, infection, and respiratory complications and survival therefore relies on early surgical correction (1, 11). The surgery aims to reconstruct the continuity of the esophagus and eliminate any possible fistulae (11, 14), which can be done either as a transpleural thorascopical procedure, or as open surgery, most commonly extrapleural (11, 22).
The mortality rate in isolated esophageal atresia range from 4.3 to 8.1% (7, 8, 17, 23–25), but varies with the type of atresia (with higher mortality and morbidity in the long gap esophageal atresia presentation), and mortality increases furthermore in case of prematurity and/or low birth weight, and with the presence of associated abnormalities, notably major cardiac and chromosomal anomalies (2, 6, 9, 26, 27). Even after hospital discharge, the children have increased mortality with post-discharge mortality is primarily due to respiratory compromise, including sudden infant death, aspiration, tracheomalacia, and reactive airway disease (23, 28, 29).
The most common postoperative complications are anastomosis leakage, fistula recurrence, anastomotic strictures, respiratory complications, and infections (25, 30–40). Anastomotic leakage is one of the most common serious complications occurring in about 5–17% of cases (25, 34, 35). Leakage into the mediastinum result mainly from anastomotic tension (particularly in cases with increased gap length) leading to ischemia of the esophageal ends, particularly in the small, friable lower segment and sub-optimal surgical technique; sepsis and even use of prosthetic materials can contribute (36–38). Major leaks are uncommon and tend to present with acute deterioration associated with pneumothorax and sepsis, and may require emergency decompression with placement of a postoperative chest tube (35, 39, 40). Most leaks heal spontaneously given proper drainage and antibiotics and only few require surgical intervention (35, 39, 40).
Long-term complications include strictures of the anastomotic region [incidence 25–75% (25, 34, 41, 42)], gastroesophageal reflux [incidence 22–63% (43)], esophagitis, tracheomalacia, feeding difficulties [incidence up to 80% (30, 44)], pulmonary symptoms, and developmental challenges (30–33, 45). These long-term complications have an impact on quality of life (28) in both patients and parents, especially in the case of tracheal and esophageal complications (6, 31, 46–50).
During the esophageal repair a prophylactic intraoperative chest tube (IOCT) has traditionally been placed close to the anastomosis to drain access fluid and air through a one-way system (51, 52). The routine use of prophylactic IOCTs is now debated (11, 39, 40, 52) and at the European Reference Network for rare Inherited and Congenital Anomalies (ERNICA) consensus conference, no consensus was found with only 21.4% of the members voting for the use of IOCTs (22). However, IOCTs are still used and reported as common as in 54% of the cases in the UK (53), 57% in Belgium (54), and 69% in an international survey, respectively (55).
IOCTs are not without drawback as they can cause insertion site infection (56) and when improperly placed, the tube can cause disruption of the site of anastomosis or penetration of proximal myotomy (57). IOCTs may also cause considerable postoperative pain, which would decrease inspiratory effort tand need for administration of more opoids, both leading to secondary effects such as atelectasis and pneumonia (58). Importantly, in some cases, IOCTs are insufficient to drain major leaks, necessitating the placement of a new chest tube (39, 40).
Whether the potential benefits of the prophylactic IOCT overweigh the potential harms is therefore unclear (22). Accordingly, the objective of this study was to examine the benefits and harms of prophylactic IOCT during primary surgical repair of esophageal atresia.
We conducted a systematic review of the existing literature according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines (PRISMA) and the Cochrane Handbook for Systematic Reviews of Intervention (59, 60). The predefined methodology, and method for this review in general, is described in our protocol, registered in June 2021 (61).
We searched for RCTs assessing the effect of a prophylactic IOCT during primary surgical repair of esophageal atresia and related observational studies identified during our searches for RCTs.
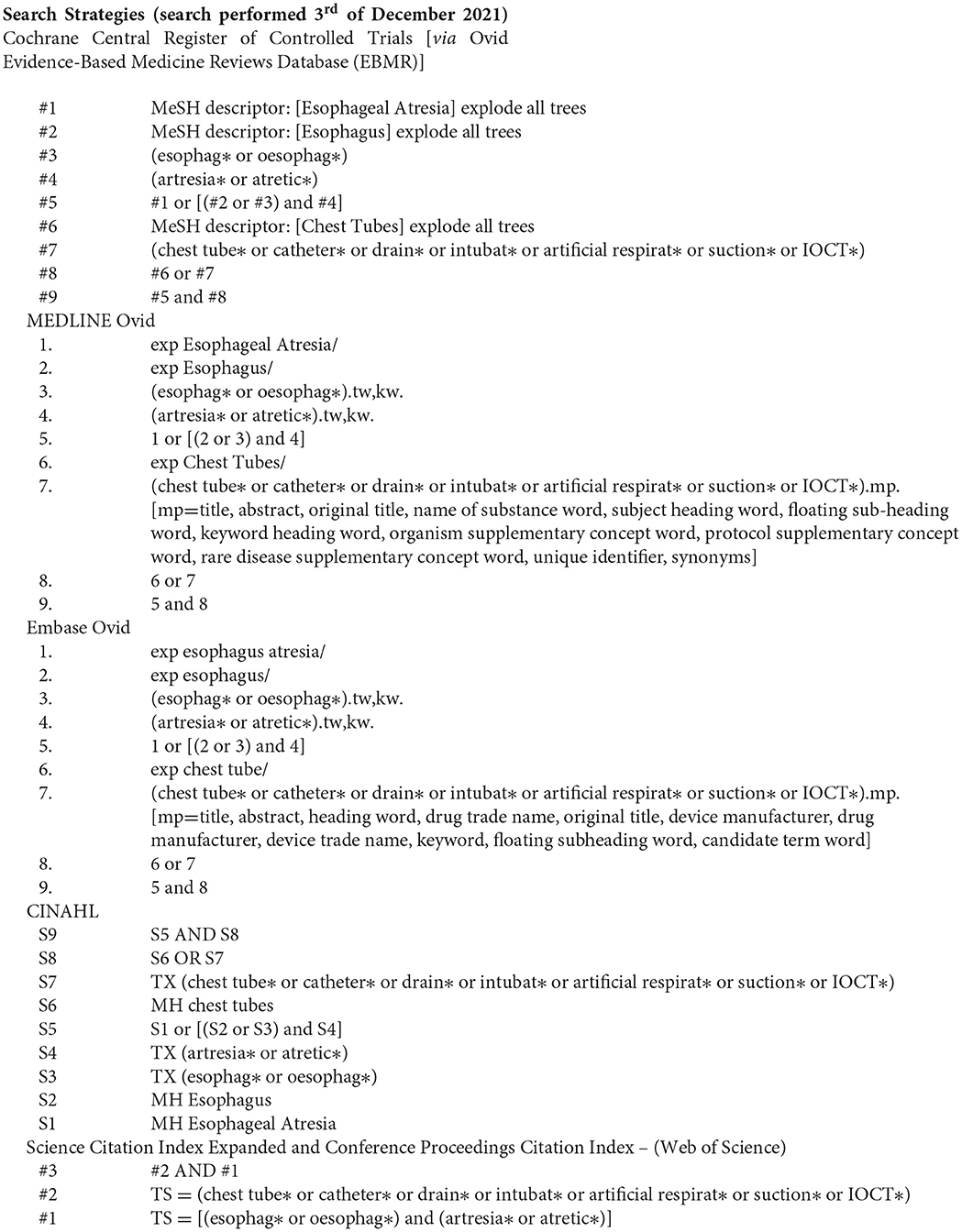
We searched the Cochrane Central Register of Controlled Trials, MEDLINE Ovid, Embase Ovid, CINAHL, and Science Citation Index Expanded and Conference Proceedings Citation Index—(Web of Science). The search strategy was developed by an information specialist from the Cochrane Hepato-Biliary Group. The search strategy can be found in Appendix 1.
Studies were included irrespectively of publication type, publications status, and language. Two independent reviewers (MRL and SKK) screened and found relevant studies, performed data-extraction using an EXCEL data extraction sheet, and systematically checked risks of bias. We planned to contact trial authors if relevant data were unclear or missing. A description of the data collection process can be found in our protocol.
We followed the Cochrane Handbook for Systematic Reviews of Interventions to examine the risk of bias (62), including the ROBIN-I tool for non-randomized studies (63). Two authors, MRL and SKK, independently assessed the risk of bias in the included trials. In case of disagreements, a third author (ULT) would arbitrate.
The primary outcomes were: (1) all-cause mortality, (2) serious adverse events, and (3) pneumothorax - requiring intervention. Secondary outcomes were: (1) sepsis or mediastinitis, (2) anastomosis leakage, (3) esophageal stricture, and (4) pain (measured by any valid score). For every relevant outcome, the risk ratios (RRs) were calculated with a 95% confidence interval (CI).
We pooled the data from relevant studies that were estimated to be clinically homogeneous using the Review Manager 5.4.1 software. If more than one study provides usable data in any single comparison, we performed a meta-analysis. We used RR for dichotomous outcomes, and by utilizing the fixed-effect (Mantel-Haenszel model).
A systematic search done December 3rd, 2021, identified a total of 953 records from databases and registers. A total of 894 were excluded based on the title and abstract. We assessed 19 full-text original articles, of which following studies were included: three RCTs (64–66) and two case-control studies (51, 52) for narrative description in the discussion. See Figure 1: PRISMA flowchart and Table 1: Table of excluded studies regarding details on inclusion and exclusion of the studies.
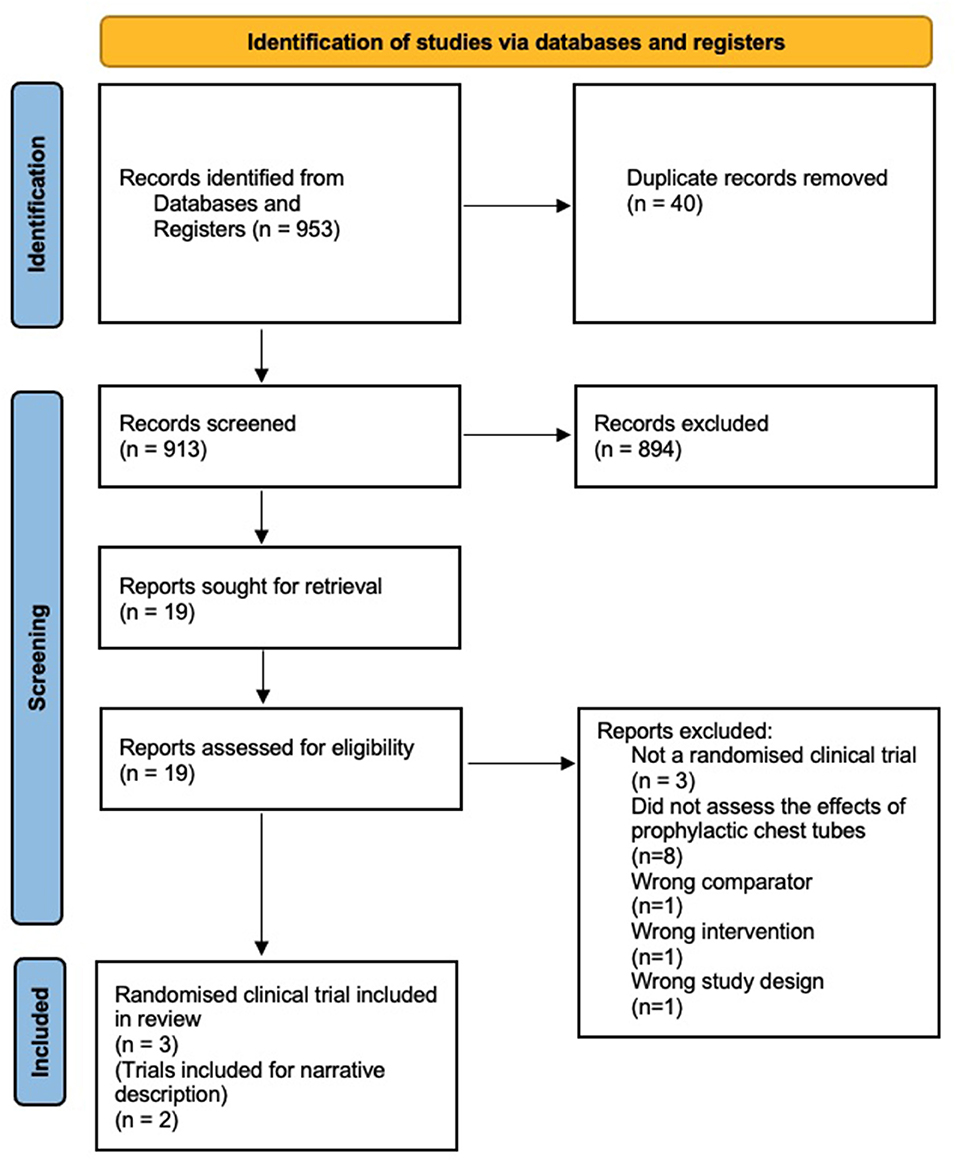
Figure 1. PRISMA flowchart.
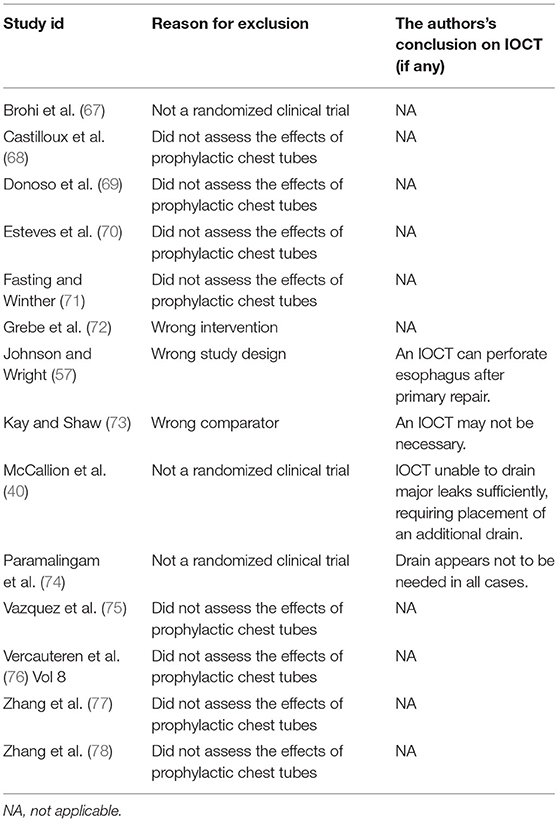
Table 1. Table of excluded studies.
We identified and included three RCTs randomizing a total of 162 neonates with esophageal atresia and distal tracheoesophageal fistula into intervention and control group. The trials compared mortality, serious adverse events, intervention-requiring pneumothorax, and anastomosis leakage (see Table 2: summary of findings). The risk of bias assessment is shown in Figure 2. All trials were assessed to be at overall “some concerns” for risk of bias. None of the trials adequately describe the randomization process or referred to a publish protocol.
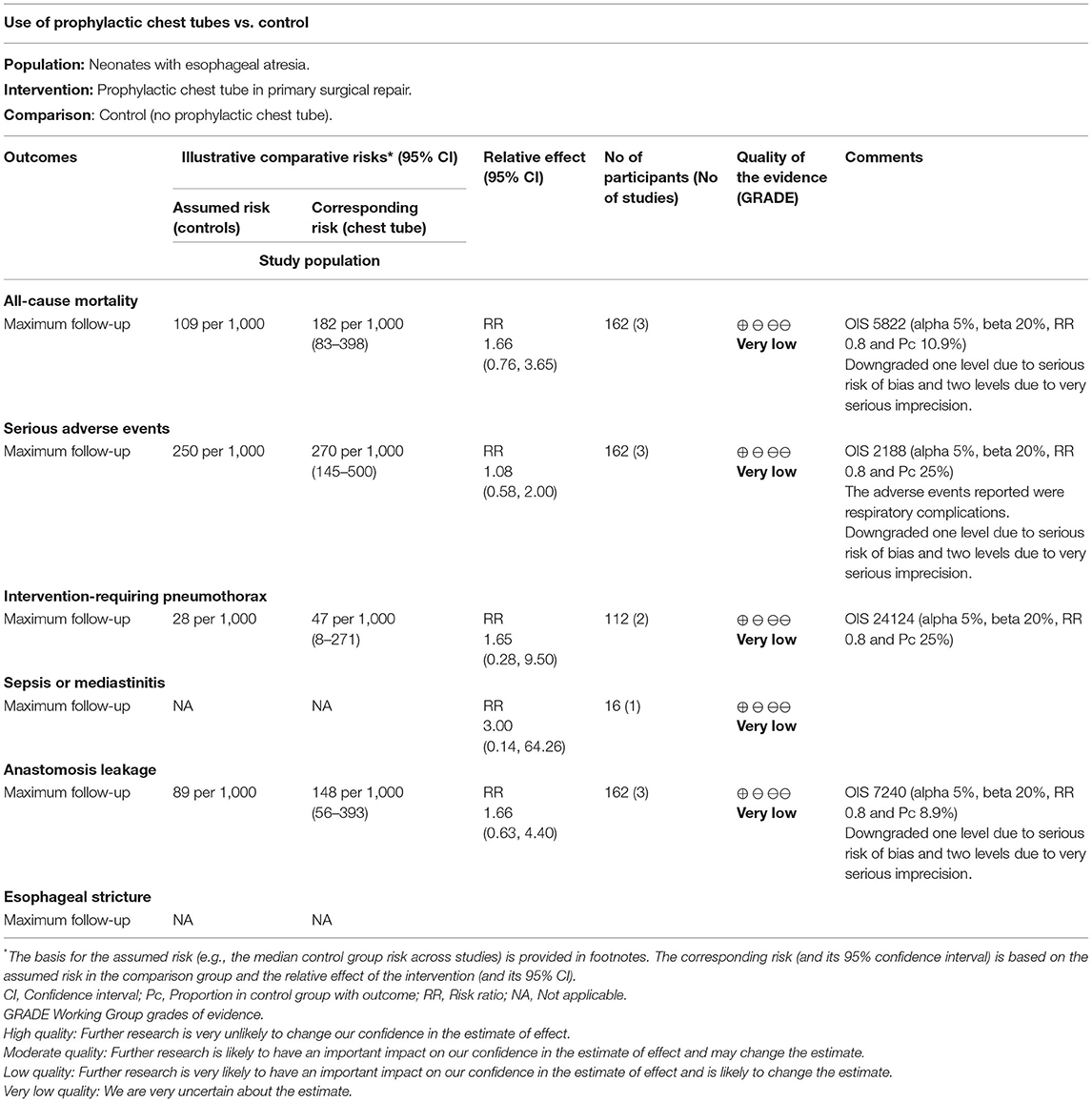
Table 2. Summary of findings, randomized clinical trials.
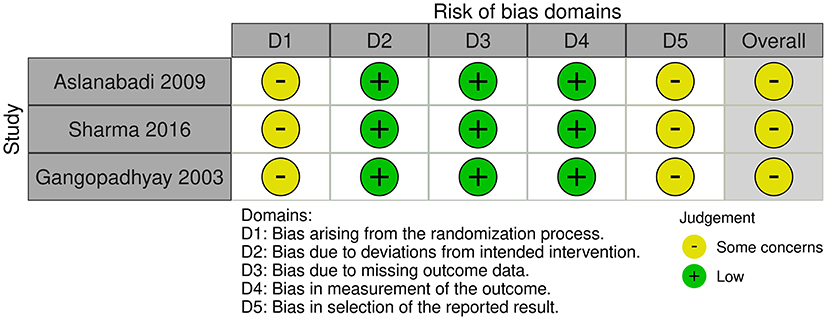
Figure 2. Risk of bias assessment.
A meta-analysis of three trials, randomizing 162 participants, showed that an IOCT might result in an increased risk of mortality compared to neonates undergoing surgery without an IOCT, but the confidence interval was compatible with no effect [RR 1.66, 95% CI 0.76–3.65; P = 0.21; 2.8% of optimal information size (OIS); very low certainty of evidence; Figure 3].
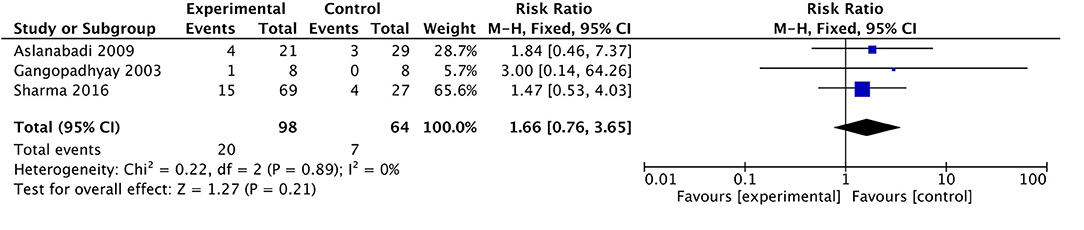
Figure 3. Forest plot for all-cause mortality.
A meta-analysis of three trials, randomizing 162 participants, showed that an IOCT might result in an increased risk of having a serious adverse event compared with neonates with esophageal atresia undergoing surgery without an IOCT, but the confidence interval was compatible with no effect (RR 1.08, 95% CI 0.58–2.00; P = 0.81; 7.4% of OIS; very low certainty of evidence; Figure 4).

Figure 4. Forest plot for serious adverse events.
The serious adverse effects assessed in the trials were respiratory complications including respiratory distress, pneumonia, pneumothorax, lung collapse, and apnea as well as mortality.
A meta-analysis of the two trials, randomizing 112 participants, showed that an IOCT might result in an increased risk of having an intervention-requiring pneumothorax compared with neonates with esophageal atresia undergoing surgery without an IOCT, but the confidence interval was compatible with no effect (RR 1.65, 95% CI 0.28–9.50; P = 0.58; 0.46% of OIS; very low certainty of evidence; Figure 5).

Figure 5. Forest plot for intervention-requiring pneumothorax.
One included trial (65), reporting sepsis, showed that an IOCT might result in an increased risk of having sepsis compared with neonates with esophageal atresia undergoing surgery without an IOCT, but the confidence interval was compatible with no effect (RR 3.00, 95% CI 0.14–64.26).
Three trials, randomizing 162 participants, showed that an IOCT might result in an increased risk of anastomosis leakages compared with neonates with esophageal atresia undergoing surgery without an IOCT, but the confidence interval was compatible with no effect (RR 1.66, 95% CI 0.63–4.40; P = 0.30; 2.24 % of OIS; very low certainty of evidence; Figure 6).

Figure 6. Forest plot for anastomosis leakage.
None of the included trials reported on esophageal stricture.
None of the included studies did a measurement of pain.
We identified and included three RCTs randomizing a total of 162 neonates with esophageal atresia and distal tracheoesophageal fistula into intervention and control group. The trials compared mortality, serious adverse events, intervention-requiring pneumothorax, and anastomosis leakage.
We found no evidence of a beneficial effect of placing a prophylactic IOCT during primary surgical repair from neither of the included studies. The evidence from RCTs shows potential harm when assessing all-cause mortality and serious adverse events, but the results were very uncertain. All studies were assessed to be at overall “some concerns” for risk of bias. The risk of bias assessment is shown in Figure 2. The statistical heterogeneity was low for all our meta-analyses. It was not possible to assess the preplanned subgroups regarding esophageal stricture and pain due to the lack of relevant data.
Two observational studies (51, 52) seem to support the overall results from the three RCTs in terms of mortality, serious adverse events, and anastomosis leakage that found no beneficial effect of placing a prophylactic IOCT. Furthermore, observational data from Nquyen et al. (51) suggest that the placement of a prophylactic IOCT may increase the risk of various complications such as an increase in the risk of developing esophageal stricture. These observational studies were assessed by ROBINS-I to be at overall serious (51) and critical risk of bias (52) and should therefore be interpreted with caution. Finally, we identified but excluded for various reasons (see Table 1) an additional 4 studies, no of which were in favor of routine ICOT (see Table 1).
This review draws strengths from the strict methodology, including following a protocol registered before the literature search began, systemically assessing for risk of bias, and adhering to all recommendations from the Cochrane Collaboration, including the use of ROBINS-I. The search strategy was developed by an information specialist from the Cochrane Hepato-Biliary Group. Our study also differs from a recent review by Anand et al. (79) on the topic by adding GRADE assessment of the included studies and abstaining from mixing RCTs with observational studies in the meta-analyses. In Anand et al., the meta-analysis included a mix of extrapleural and transpleural repair (51, 52) and an observation study, where some of the participants received IOCTs by a non-prophylactic indication (74). Although the overall conclusions in the present study are fairly similar to the study by Anand et al., inclusion of non-randomized studies with their inherently different study designs in a meta-analysis may severely compromise the validity of their results, as their lack of randomization makes them highly at risk for confounding bias resulting in an imbalance in prognostic factors associated with the outcome (80).
We only identified three RCTs, systematically comparing the intervention with an IOCT to no IOCT in 162 neonates undergoing primary repair for esophageal atresia. None of our meta-analyses reached the optimal information size. In addition to evaluate overall improvement in treatment techniques and clinical outcomes, future trials should also assess pain and esophageal stricture as this would be an important outcome for the children and parents. Importantly, the associated malformations and genetic aberrations often found in esophageal atresia and the difference in exact anatomical presentation [with or without fistula(e)] make this a relatively heterogeneous pathology. The patients included in these RCTs all presented with distal tracheoesophageal fistula, but with various details on pre-surgical gap length and on associated malformations; further complicating the comparison between studies and the transferability of the conclusion to other patient subgroups.
Esophageal atresia is a relatively rare condition; particularly considering the numerous subtypes with various possible anatomical presentations and associated malformation. Rare diseases pose challenges to methodology when designing RCTs that are adequately powered to draw definitive conclusions, as small patient sample sizes are statistically vulnerable to small deviations in the observed number of outcomes (81). Innovative clinical trial methods minimizing sample size requirements (82) and optimal research infrastructure (83), possibly through international collaborations, may improve future productivity of robust research in esophageal atresia.
We did not identify any studies advocating for the use of prophylactic IOCTs. Based on the limited amount of research on this topic and results from the included studies, we did not find sufficient evidence to support or discontinue the routine use of prophylactic IOCTs for neonates undergoing surgical repair of esophageal atresia, as all confidence intervals were compatible with no effect. Further trials, ideally multicentric, are warranted to explore the effects of the prophylactic IOCT for neonates undergoing surgical repair of esophageal atresia. Importantly, future trials should adhere to SPIRIT guidelines (84).
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
ML drafted the protocol and review, extracted data, co-ordinated the review, analyzed the data, and revised the review. SK drafted and revised the protocol, extracted data, analyzed the data, interpreted the data, commented on, revised the review, interpreted the data, provided supervision, and provided a methodological and statistical expertise. SH revised and commented on the protocol and review and provided supervision. JO and MF revised and commented on the protocol and review and provided clinical expertise. SP revised and commented on the review. UL-T drafted the protocol, conceived and designed the review, revised the protocol, commented on, revised the review, provided supervision, and clinical expertise. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The review author team would like to acknowledge the information specialist Sarah Klingenberg from the Cochrane Hepato-Biliary Group for the development of our search strategy.
2. Zhou Y, Mao X, Zhou H, Qin Z, Wang L, Cai Z, et al. Epidemiology of birth defects based on a birth defect surveillance system in Southern Jiangsu, China, 2014–2018. J Matern Fetal Neonatal Med. (2020) 35:1–7. doi: 10.3389/fpubh.2020.00378
3. Sfeir R, Michaud L, Sharma D, Richard F, Gottrand F. National esophageal atresia register. Eur J Pediatr Surg. (2015) 25:497–9. doi: 10.1055/s-0035-1569466
4. Demikova NS, Vydrych YV, Podolnaya MA, Lapina AS, Asanov AY. Prevalence and descriptive epidemiology of esophageal atresia in the Russian Federation. Birth Defects Res A Clin Mol Teratol. (2016) 106:854–9. doi: 10.1002/bdra.23553
5. Lupo PJ, Isenburg JL, Salemi JL, Mai CT, Liberman RF, Canfield MA, et al. Population-based birth defects data in the United States, 2010-2014: a focus on gastrointestinal defects. Birth Defects Res. (2017) 109:1504–14. doi: 10.1002/bdr2.1145
6. Wittekindt B, Schloesser R, Doberschuetz N, Salzmann-Manrique E, Grossmann J, Misselwitz B, et al. Epidemiology and outcome of major congenital malformations in a large German county. Eur J Pediatr Surg. (2019) 29:282–9. doi: 10.1055/s-0038-1642630
7. Cassina M, Ruol M, Pertile R, Midrio P, Piffer S, Vicenzi V, et al. Prevalence, characteristics, and survival of children with esophageal atresia: a 32-year population-based study including 1,417,724 consecutive newborns. Birth Defects Res A Clin Mol Teratol. (2016) 106:542–8. doi: 10.1002/bdra.23493
8. Schmedding A, Wittekindt B, Schloesser R, Hutter M, Rolle U. Outcome of esophageal atresia in Germany. Dis Esophagus. (2020) 34:doaa093. doi: 10.1093/dote/doaa093
9. Pedersen RN, Calzolari E, Husby S, Garne E, EUROCAT working group. Oesophageal atresia: prevalence, prenatal diagnosis and associated anomalies in 23 European regions. Arch Dis Child. (2012) 97:227–32. doi: 10.1136/archdischild-2011-300597
10. Oddsberg J, Lu Y, Lagergren J. Maternal diabetes and risk of esophageal atresia. J Pediatr Surg. (2010) 45:2004–8. doi: 10.1016/j.jpedsurg.2010.06.008
11. Höllwarth ME, Till H. Chapter 44. Esophageal atresi. In: Puri P, editor. Pediatric Surgery: General Principles and Newborn Surgery. Berlin; Heidelberg: Springer (2020). p. 661–80.
12. Morini F, Conforti A, Zani A, Sindjic-Antunovic S, Koivusalo A, Friedmacher F, et al. Diagnostic workup of neonates with esophageal atresia: results from the EUPSA esophageal atresia registry. Front Pediatr. (2020) 8:489. doi: 10.3389/fped.2020.00489
13. Felix JF, de Jong EM, Torfs CP, de Klein A, Rottier RJ, Tibboel D. Genetic and environmental factors in the etiology of esophageal atresia and/or tracheoesophageal fistula: an overview of the current concepts. Birth Defects Res A Clin Mol Teratol. (2009) 85:747–54. doi: 10.1002/bdra.20592
14. Harmon CM, Coran AG. Chapter 69. Congenital anomalies of the esophagus In: Coran AG, editor. Pediatric Surgery. 7th ed. Philadelphia, PA: Mosby (2012). p. 893–918. doi: 10.1016/B978-0-323-07255-7.00069-6
15. Källén B, Finnström O, Lindam A, Nilsson E, Nygren K-G, Otterblad PO. Congenital malformations in infants born after in vitro fertilization in Sweden. Birth Defects Res A Clin Mol Teratol. (2010) 88:137–43. doi: 10.1002/bdra.20645
16. Oddsberg J, Lu Y, Lagergren J. Aspects of esophageal atresia in a population-based setting: incidence, mortality, and cancer risk. Pediatr Surg Int. (2012) 28:249–57. doi: 10.1007/s00383-011-3014-1
17. Sfeir R, Michaud L, Salleron J, Gottrand F. Epidemiology of esophageal atresia. Dis Esophagus. (2013) 26:354–5. doi: 10.1111/dote.12051
18. Stoll C, Alembik Y, Dott B, Roth M-P. Associated malformations in patients with esophageal atresia. Eur J Med Genet. (2009) 52:287–90. doi: 10.1016/j.ejmg.2009.04.004
19. van Heurn LWE, Cheng W, de Vries B, Saing H, Jansen NJG, Kootstra G, et al. Anomalies associated with oesophageal atresia in Asians and Europeans. Pediatr Surg Int. (2002) 18:241–3. doi: 10.1007/s003830100692
20. Stoll C, Alembik Y, Dott B, Roth M-P. Associated anomalies in cases with esophageal atresia. Am J Med Genet A. (2017) 173:2139–57. doi: 10.1002/ajmg.a.38303
21. Brosens E, Ploeg M, van Bever Y, Koopmans AE, IJsselstijn H, Rottier RJ, et al. Clinical and etiological heterogeneity in patients with tracheo-esophageal malformations and associated anomalies. Eur J Med Genet. (2014) 57:440–52. doi: 10.1016/j.ejmg.2014.05.009
22. Dingemann C, Eaton S, Aksnes G, Bagolan P, Cross KM, De Coppi P, et al. ERNICA consensus conference on the management of patients with esophageal atresia and tracheoesophageal fistula: diagnostics, preoperative, operative, and postoperative management. Eur J Pediatr Surg. (2020) 30:326–36. doi: 10.1055/s-0039-1693116
23. Choudhury SR, Ashcraft KW, Sharp RJ, Murphy JP, Snyder CL, Sigalet DL. Survival of patients with esophageal atresia: influence of birth weight, cardiac anomaly, and late respiratory complications. J Pediatr Surg. (1999) 34:70–3. doi: 10.1016/S0022-3468(99)90231-2
24. Lilja HE, Wester T. Outcome in neonates with esophageal atresia treated over the last 20 years. Pediatr Surg Int. (2008) 24:531–6. doi: 10.1007/s00383-008-2122-z
25. Zimmer J, Eaton S, Murchison LE, De Coppi P, Ure BM, Dingemann C. State of play: eight decades of surgery for esophageal atresia. Eur J Pediatr Surg. (2019) 29:39–48. doi: 10.1055/s-0038-1668150
26. Sfeir R, Rousseau V, Bonnard A, Gelas T, Aumar M, Panait N, et al. Risk factors of early mortality and morbidity in esophageal atresia with distal tracheoesophageal fistula: a population-based cohort study. J Pediatr. (2021) 234:99–105.e1. doi: 10.1016/j.jpeds.2021.02.064
27. Bairdain S, Zurakowski D, Vargas SO, Stenquist N, McDonald M, Towne MC, et al. Long-gap esophageal atresia is a unique entity within the esophageal atresia defect spectrum. Neonatology. (2017) 111:140–4. doi: 10.1159/000449241
28. Tan Tanny SP, Comella A, Hutson JM, Omari TI, Teague WJ, King SK. Quality of life assessment in esophageal atresia patients: a systematic review focusing on long-gap esophageal atresia. J Pediatr Surg. (2019) 54:2473–8. doi: 10.1016/j.jpedsurg.2019.08.040
29. Tan Tanny SP, Fearon E, Hawley A, Brooks J-A, Comella A, Hutson JM, et al. Predictors of mortality after primary discharge from hospital in patients with esophageal atresia. J Pediatr. (2020) 219:70–5. doi: 10.1016/j.jpeds.2019.12.031
30. Acher CW, Ostlie DJ, Leys CM, Struckmeyer S, Parker M, Nichol PF. Long-term outcomes of patients with tracheoesophageal fistula/esophageal atresia: survey results from tracheoesophageal fistula/esophageal atresia online communities. Eur J Pediatr Surg. (2016) 26:476–80. doi: 10.1055/s-0035-1570103
31. Harmsen WJ, Aarsen FJ., van der Cammen-van Zijp MHM, van Rosmalen JM, Wijnen RMH, Tibboel D, et al. Developmental problems in patients with oesophageal atresia: a longitudinal follow-up study. Arch Dis Child Fetal Neonatal Ed. (2017) 102:F214–9. doi: 10.1136/archdischild-2015-309976
32. Nurminen P, Koivusalo A, Hukkinen M, Pakarinen M. Pneumonia after repair of esophageal atresia-incidence and main risk factors. Eur J Pediatr Surg. (2019) 29:504–9. doi: 10.1055/s-0038-1675775
33. Rayyan M, Allegaert K, Omari T, Rommel N. Dysphagia in children with esophageal atresia: current diagnostic options. Eur J Pediatr Surg. (2015) 25:326–32. doi: 10.1055/s-0035-1559818
34. Allin B, Knight M, Johnson P, Burge D, BAPS-CASS. Outcomes at one-year post anastomosis from a national cohort of infants with oesophageal atresia. PLoS ONE. (2014) 9:e106149. doi: 10.1371/journal.pone.0106149
35. Chittmittrapap S, Spitz L, Kiely EM, Brereton RJ. Anastomotic leakage following surgery for esophageal atresia. J Pediatr Surg. (1992) 27:29–32. doi: 10.1016/0022-3468(92)90098-R
36. Lal DR, Gadepalli SK, Downard CD, Ostlie DJ, Minneci PC, Swedler RM, et al. Challenging surgical dogma in the management of proximal esophageal atresia with distal tracheoesophageal fistula: outcomes from the Midwest Pediatric Surgery Consortium. J Pediatr Surg. (2018) 53:1267–72. doi: 10.1016/j.jpedsurg.2017.05.024
37. Upadhyaya VD, Gangopadhyaya AN, Gopal SC, Upadhyaya A, Sharma SP, Gupta DK, et al. Is ligation of azygos vein necessary in primary repair of tracheoesophageal fistula with esophageal atresia? Eur J Pediatr Surg. (2007) 17:236–40. doi: 10.1055/s-2007-965693
38. Teague WJ, Karpelowsky J. Surgical management of oesophageal atresia. Paediatr Respir Rev. (2016) 19:10–5. doi: 10.1016/j.prrv.2016.04.003
39. Spitz L. Esophageal atresia. Lessons I have learned in a 40-year experience. J Pediatr Surg. (2006) 41:1635–40. doi: 10.1016/j.jpedsurg.2006.07.004
40. McCallion WA, Hannon RJ, Boston VE. Prophylactic extrapleural chest drainage following repair of esophageal atresia: is it necessary? J Pediatr Surg. (1992) 27:561. doi: 10.1016/0022-3468(92)90446-E
41. Friedmacher F, Kroneis B, Huber-Zeyringer A, Schober P, Till H, Sauer H, et al. Postoperative complications and functional outcome after esophageal atresia repair: results from longitudinal single-center follow-up. J Gastrointest Surg. (2017) 21:927–35. doi: 10.1007/s11605-017-3423-0
42. Koivusalo AI, Pakarinen MP, Rintala RJ. Modern outcomes of oesophageal atresia: single centre experience over the last twenty years. J Pediatr Surg. (2013) 48:297–303. doi: 10.1016/j.jpedsurg.2012.11.007
43. Krishnan U, Mousa H., Dall'Oglio L, Homaira N, Rosen R, Faure C, et al. ESPGHAN-NASPGHAN guidelines for the evaluation and treatment of gastrointestinal and nutritional complications in children with esophageal atresia-tracheoesophageal fistula. J Pediatr Gastroenterol Nutr. (2016) 63:550–70. doi: 10.1097/MPG.0000000000001401
44. Gibreel W, Zendejas B, Antiel RM, Fasen G, Moir CR, Zarroug AE. Swallowing dysfunction and quality of life in adults with surgically corrected esophageal atresia/tracheoesophageal fistula as infants: forty years of follow-up. Ann Surg. (2017) 266:305–10. doi: 10.1097/SLA.0000000000001978
45. Morini F, Conforti A, Bagolan P. Perioperative complications of esophageal atresia. Eur J Pediatr Surg. (2018) 28:133–40. doi: 10.1055/s-0038-1636941
46. Legrand C, Michaud L, Salleron J, Neut D, Sfeir R, Thumerelle C, et al. Long-term outcome of children with oesophageal atresia type III. Arch Dis Child. (2012) 97:808–11. doi: 10.1136/archdischild-2012-301730
47. Rozensztrauch A, Smigiel R, Patkowski D. Congenital esophageal atresia-surgical treatment results in the context of quality of life. Eur J Pediatr Surg. (2019) 29:266–70. doi: 10.1055/s-0038-1641597
48. Sistonen SJ, Pakarinen MP, Rintala RJ. Long-term results of esophageal atresia: Helsinki experience and review of literature. Pediatr Surg Int. (2011) 27:1141–9. doi: 10.1007/s00383-011-2980-7
49. Witt S, Dellenmark-Blom M, Dingemann J, Dingemann C, Ure BM, Gomez B, et al. Quality of life in parents of children born with esophageal atresia. Eur J Pediatr Surg. (2019) 29:371–7. doi: 10.1055/s-0038-1660867
50. Witt S, Dellenmark-Blom M, Flieder S, Dingemann J, Abrahamsson K, Jönsson L et al. Health-related quality of life experiences in children and adolescents born with esophageal atresia: a Swedish-German focus group study. Child Care Health Dev. (2019) 45:79–88. doi: 10.1111/cch.12619
51. Nguyen MVL, Delaplain PT, Lim JC, Golden JM, Gayer CP. The value of prophylactic chest tubes in tracheoesophageal fistula repair. Pediatr Surg Int. (2020) 36:687–96. doi: 10.1007/s00383-020-04664-6
52. Gawad N, Wayne C, Bass J, Nasr A. A chest tube may not be needed after surgical repair of esophageal atresia and tracheoesophageal fistula. Pediatr Surg Int. (2018) 34:967–70. doi: 10.1007/s00383-018-4307-4
53. Burge DM, Shah K, Spark P, Shenker N, Pierce M, Kurinczuk JJ, et al. Contemporary management and outcomes for infants born with oesophageal atresia. Br J Surg. (2013) 100:515–21. doi: 10.1002/bjs.9019
54. Reusens H, Matthyssens L, Vercauteren C, van Renterghem K Belgian Belgian Association of Paediatric Surgery (BELAPS). Multicentre survey on the current surgical management of oesophageal atresia in Belgium and Luxembourg. J Pediatr Surg. (2017) 52:239–46. doi: 10.1016/j.jpedsurg.2016.11.010
55. Zani A, Eaton S, Hoellwarth ME, Puri P, Tovar J, Fasching G, et al. International survey on the management of esophageal atresia. Eur J Pediatr Surg. (2014) 24:3–8. doi: 10.1055/s-0033-1350058
56. Kwiatt M, Tarbox A, Seamon MJ, Swaroop M, Cipolla J, Allen C, et al. Thoracostomy tubes: A comprehensive review of complications and related topics. Int J Crit Illn Inj Sci. (2014) 4:143–55. doi: 10.4103/2229-5151.134182
57. Johnson JF, Wright DR. Chest tube perforation of esophagus following repair of esophageal atresia. J Pediatr Surg. (1990) 25:1227–30. doi: 10.1016/0022-3468(90)90511-7
58. Ponsky TA, Rothenberg SS, Tsao K, Ostlie DJ, St Peter SD, Holcomb GW. Thoracoscopy in children: is a chest tube necessary? J Laparoendosc Adv Surg Tech A. (2009) 19(Suppl 1):S23–25. doi: 10.1089/lap.2008.0090.supp
59. Lefebvre C, Glanville J, Briscoe S, Littlewood A, Marshall C, Metzendorf M-I, et al. Chapter 4 - Searching for and selecting studies. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane (2021). Available online at: www.training.cochrane.org/handbook (accessed January 10, 2022).
60. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
61. Link to protocol registred on PROSPERO. Available online at: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=257834 (accessed June 28, 2021).
62. Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Chapter 8 - Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.2. Cochrane (2021). Available online at: www.training.cochrane.org/handbook (accessed January 10, 2022).
63. Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. (2016) 355:i4919. doi: 10.1136/bmj.i4919
64. Aslanabadi S, Jamshidi M, Tubbs RS, Shoja MM. The role of prophylactic chest drainage in the operative management of esophageal atresia with tracheoesophageal fistula. Pediatr Surg Int. (2009) 25:365–8. doi: 10.1007/s00383-009-2345-7
65. Gangopadhyaya A. Is retropleural drainage necessary after definitive repair of esophageal atresia and tracheoesophageal fistula? J Indian Assoc Pediatr Surg. (2003) 8:86–90.
66. Sharma S, Pathak S, Husain A, Pandey DC, Kunwer R, Chaturvedi J. Retropleural drainage: yes or no in primary repair of esophageal atresia with tracheoesophageal fistula. Int J Contemp Med Res. (2016) 3:3.
67. Brohi AR, Syal AA, Mengal N. Oesophageal atresia - Experience of 7 years with data evaluation. Med Forum Monthly. (2011) 22:3–7.
68. Castilloux J, Noble AJ, Faure C. Risk factors for short- and long-term morbidity in children with esophageal atresia. J Pediatr. (2010) 156:755–60. doi: 10.1016/j.jpeds.2009.11.038
69. Donoso F, Kassa A-M, Gustafson E, Meurling S, Lilja HE. Outcome and management in infants with esophageal atresia - a single centre observational study. J Pediatr Surg. (2016) 51:1421–5. doi: 10.1016/j.jpedsurg.2016.03.010
70. Esteves E, Pessoa C, Paguada-Ruiz LK, Castro KC. Thoracoscopic management of esophageal atresia and its related complications: lessons after the first 106 cases. In: Proceedings of the 28th Annual Congress for Endosurgery in Children. Santiago (2019). doi: 10.1089/lap.2019.29028.abstracts
71. Fasting H, Winther LK. Oesophageal atresia and tracheo-oesophageal fistula. Early and late results in 86 patients. Scand J Thorac Cardiovasc Surg. (1978) 12:147–51. doi: 10.3109/14017437809100366
72. Grebe S, Schnapka J, Menardi G. Esophageal atresia - analysis of the postoperative morbidity in 61 cases. Zentralbl Chir. (1999) 8:144–6.
73. Kay S, Shaw K. Revisiting the role of routine retropleural drainage after repair of esophageal atresia with distal tracheoesophageal fistula. J Pediatr Surg. (1999) 34:1082–5. doi: 10.1016/S0022-3468(99)90571-7
74. Paramalingam S, Burge DM, Stanton MP. Operative intercostal chest drain is not required following extrapleural or transpleural esophageal atresia repair. Eur J Pediatr Surg. (2013) 23:273–5. doi: 10.1055/s-0032-1330845
75. Vazquez AG, Novillo IC, Diaz ML, Sanchez RT, Carretero SF, Zegarra CM, et al. Technical modifications in thoracoscopic repair of esophageal atresia. Our experience. J Laparoendosc Adv Surg Tech. (2011) 21:A76. doi: 10.1089/lap.2011.9999
76. Vercauteren C, Reusens H, De Backer A, Tambucci R, Van Cauwenberge S, Leyman P, et al. Oesophageal atresia: a multicenter retrospective study on surgical treatment and 1-year follow-up. ISDE. (2019) 32(Supplement 1):30. doi: 10.1093/dote/doz047.92
77. Zhang J, Wu Q, Chen L, Wang Y, Cui X, Huang W, et al. Clinical analysis of surgery for type III esophageal atresia via thoracoscopy: a study of a Chinese single-center experience. J Cardiothorac Surg. (2020) 15:55. doi: 10.1186/s13019-020-01097-z
78. Zhang M, Lin Y, Xie W, Yu J, Huang Q, Li J, et al. The multidisciplinary management of recurrent tracheoesophageal fistula after esophageal atresia: Experience with 135 cases from a tertiary center. J Pediatr Surg. (2021) 56:1918–25. doi: 10.1016/j.jpedsurg.2020.12.019
79. Anand S, Singh A, Krishnan N, Yadav DK. Whether prophylactic intraoperative chest drain insertion in esophageal atresia-tracheoesophageal fistula is an evidence-based practice or just a prejudice: a systematic review and meta-analysis. J Pediatr Surg. (2021). doi: 10.1016/j.jpedsurg.2021.06.015. [Epub ahead of print].
80. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.2. Cochrane (2021). Available online at: www.training.cochrane.org/handbook (accessed January 10, 2022).
81. Mitani AA, Haneuse S. Small data challenges of studying rare diseases. JAMA Netw Open. (2020) 3:e201965. doi: 10.1001/jamanetworkopen.2020.1965
82. Gagne JJ, Thompson L, O'Keefe K, Kesselheim AS. Innovative research methods for studying treatments for rare diseases: methodological review. BMJ. (2014) 349:g6802. doi: 10.1136/bmj.g6802
83. Whicher D, Philbin S, Aronson N. An overview of the impact of rare disease characteristics on research methodology. Orphanet J Rare Dis. (2018) 13:14. doi: 10.1186/s13023-017-0755-5
84. Chan A-W, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, Krleža-Jerić K et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. (2013) 158:200–7. doi: 10.7326/0003-4819-158-3-201302050-00583
Keywords: chest tube, neonates, tracheoesophageal fistula, esophageal atresia, pediatric surgery
Citation: Ladefoged MR, Korang SK, Hildorf SE, Oehlenschlæger J, Poulsen S, Fossum M and Lausten-Thomsen U (2022) Necessity of Prophylactic Extrapleural Chest Tube During Primary Surgical Repair of Esophageal Atresia: A Systematic Review and Meta-Analysis. Front. Pediatr. 10:849992. doi: 10.3389/fped.2022.849992
Received: 06 January 2022; Accepted: 21 February 2022;
Published: 18 March 2022.
Edited by:
Mario Lima, University of Bologna, ItalyReviewed by:
Enrico Ciardini, Pediatric Surgery Unit S. Chiara Hospital, ItalyCopyright © 2022 Ladefoged, Korang, Hildorf, Oehlenschlæger, Poulsen, Fossum and Lausten-Thomsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin Riis Ladefoged, bWFydGluLXJpaXNAaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.