 Yong Zhou
Yong Zhou Sheng Li*
Sheng Li*- Department of Pediatrics, Yancheng Maternal and Child Health Care Hospital, Yancheng, China
We conducted the systematic review to investigate the potential relationship between the vitamin polymorphisms of D receptor (VDR) gene and childhood asthma. Relevant studies researching on VDR polymorphisms and asthma susceptibility were searched throughout Embase, PubMed, China Science and technology journal database (CQVIP), etc. till 12 April, 2021. We calculated the pooled odds ratios (OR) and its 95% confidence interval (CI) using RevMan 5.3 software and Stata 11.0. FokI (rs2228570) could significantly affect childhood asthma risk across co dominant model (Ff vs. FF: OR (95%CI) = 0.82 (0.65, 1.02), P = 0.071) and dominant model (ff+Ff vs. FF: OR (95%CI) = 0.77 (0.63, 0.95), P = 0.016), especially among Caucasians in additive model (f vs. F: OR (95%CI) = 0.63 (0.43, 0.92), P = 0.015) and dominant model (ff+Ff vs. FF: OR (95%CI) = 0.67 (0.51, 0.88), P = 0.004). TaqI (rs731236) was significantly related with childhood asthma in additive model (t vs. T: OR (95%CI) = 0.45 (0.23, 0.89), P = 0.022), co dominant model (Tt vs. TT: OR (95%CI) = 0.36 (0.17, 0.77), P = 0.009), and dominant model (tt+Tt vs. TT: OR (95%CI) = 0.36 (0.15, 0.87), P = 0.024) among Asian, as well as population-based subgroup in co dominant model (Tt vs. TT: OR (95%CI) = 0.53 (0.31, 0.94), P = 0.029). However, no evidence supported the role of ApaI (rs7975232) and BsmI (rs1544410) polymorphisms in childhood asthma. FokI and TaqI polymorphisms were found to be related with the susceptibility of childhood asthma. However, it seems that ApaI and BsmI polymorphisms are not related with childhood asthma susceptibility.
Introduction
Asthma is recognized as a chronic heterogeneous respiratory disease, which has characterized by airway inflammation and hyper-responsiveness, and the disease affects more than 300 million people worldwide, especially among children (1). The incidence, morbidity, and mortality related with asthma was influenced by several potential risk factors such as environmental factors (2), infancy microbial, biome influences, and genetic background, including vitamin D receptor (VDR) gene (3).
Vitamin D has been shown to have potent immunomodulatory properties, and Vitamin D correlated with the regulation of adaptive and innate immune function through VDR (4). Recently, increasing evidence researched on the effect of vitamin D in asthma and demonstrated that the severity of symptoms was related with vitamin D deficiency (5, 6). Among VDR polymorphisms, four SNPs, including BsmI (rs1544410), ApaI (rs7975232), FokI (rs2228570), and TaqI (rs731236) have been widely researched (7), but the relationship remains inconsistent. For example, the meta-analysis by Makoui et al. showed a statistical significant association between asthma risk and TaqI SNP (7). However, the systematically review by Zhen et al. showed no association between TaqI SNP and asthma risk (8). Additionally, thereafter, some new studies have been published (9–13).
Thus, it is necessary to update the report based on the previous results of researches to further explore the potential role of VDR genes polymorphism in childhood asthma susceptibility. Then, we designed the meta-analysis and explored this relationship in different races and source of controls. Finally, our data demonstrated that FokI and TaqI polymorphisms might be associated with childhood asthma susceptibility. However, ApaI and BsmI polymorphisms are not related with childhood asthma susceptibility.
Materials and Methods
Selection Strategy
The published studies were searched from numerous databases including Embase, PubMed, WANFANG data, China National Knowledge Infrastructure (CNKI), China Science and technology journal database (CQVIP), etc. The comprehensive systematic search process was exploited till 12 April, 2021 using the following key words: (“Vitamin D receptor” OR “VDR”) AND (“polymorphisms” OR “polymorphism” OR “variant” OR “mutant”) AND (“children” OR “child” OR “teenager” OR “pediatric”). The selection strategies in Pubmed and Embase were shown in Supplementary Tables 1, 2. Moreover, in order to enroll more researches, print-out literatures, reviews, and the references of included articles were also retrieved.
Study Selection
The following inclusion criteria were designed: (1) the study was designed as a case-control study or cohort study; (2) the subjects in the experiment group were children and/or adolescents with asthma, and subjects in the control group were healthy children and/or adolescents; (3) The study explored the association of VDR ApaI (rs7975232), TaqI (rs731236), BsmI (rs1544410), FokI (rs2228570) gene polymorphisms and asthma susceptibility; (4) genotype data were reported or could be calculated based on information provided in the study.
When the control group and the case group were family members or close family members, the study would be excluded. The non-research articles, such as reviews, comments, and conference summaries, would be excluded. When duplicated studies were found or same data were showed in more than one study, the study with the most specific information would be included in the present study, and other duplicated articles would be excluded.
Data Extraction and Quality Assessment
Based on the designed criteria, studies were screened by two investigators independently. According to the standardized form, the information including year of publication, the name of the first author, research regions, the demographic information (age, sample size, source of the control group), polymorphism detection methods, the ethnicity of the included population, and genotype data, etc.
Newcastle-Ottawa Scale (NOS) criteria was used to assess the methodological quality of included studies, and the scale was assessed according to three aspects including subjects selection, comparability, and exposure (14). The study with a score of five or more would be considered as moderate quality, and the study with a score of four or less would be considered as poor quality.
When data extraction was finished, the extraction form would be exchanged, and the disagreements were solved by discussing.
Statistic Analysis
Firstly, the Hardy-Weinberg equilibrium test (HWE) of the frequency distribution of genotypes among controls was performed. We defined the population were not in the HWE if P < 0.05. For each single nucleotide polymorphisms (SNP), we examined four models, including computational additive model [m (mutation) vs. W (Wild)], co dominant model (mm vs. WW, Wm vs. WW), dominant model (mm+ Wm vs. WW), and recessive model (mm vs. WW + Wm). The effect of VDR polymorphisms in the childhood asthma susceptibility was assessed based on the pooled odds ratio (OR) and its 95% confidence interval (95%CI). Heterogeneity among individual studies was assessed using Cochran's Q test and I2 test (15). If P < 0.05, and/or I2>50%, suggesting obvious heterogeneity between the studies, the random effects model would be selected to calculate the pooled data; If P ≥ 0.05 and/or I2 ≤ 50%, the fixed effect model would be used. RevMan 5.3 software and Stata 11.0 were enrolled to perform all statistical analyses.
Results
Studies Inclusion
The detailed information associated with search process was shown in Figure 1. In this study, a total of 197 studies were firstly searched, including 54 articles in PubMed, 104 articles in Embase, 16 articles in Wanfang data, 18 articles in CNKI, and 5 articles in CQVIP. After removing 55 duplicated documents, there were 142 articles remaining. After that, we excluded 117 articles after browsing the titles and reading the abstract. Then, total 25 articles were fully reviewed, and seven articles were excluded, including five articles with adults as study subjects and two reviews. Finally, 18 articles were included in this meta-analysis (8–13, 16–27).
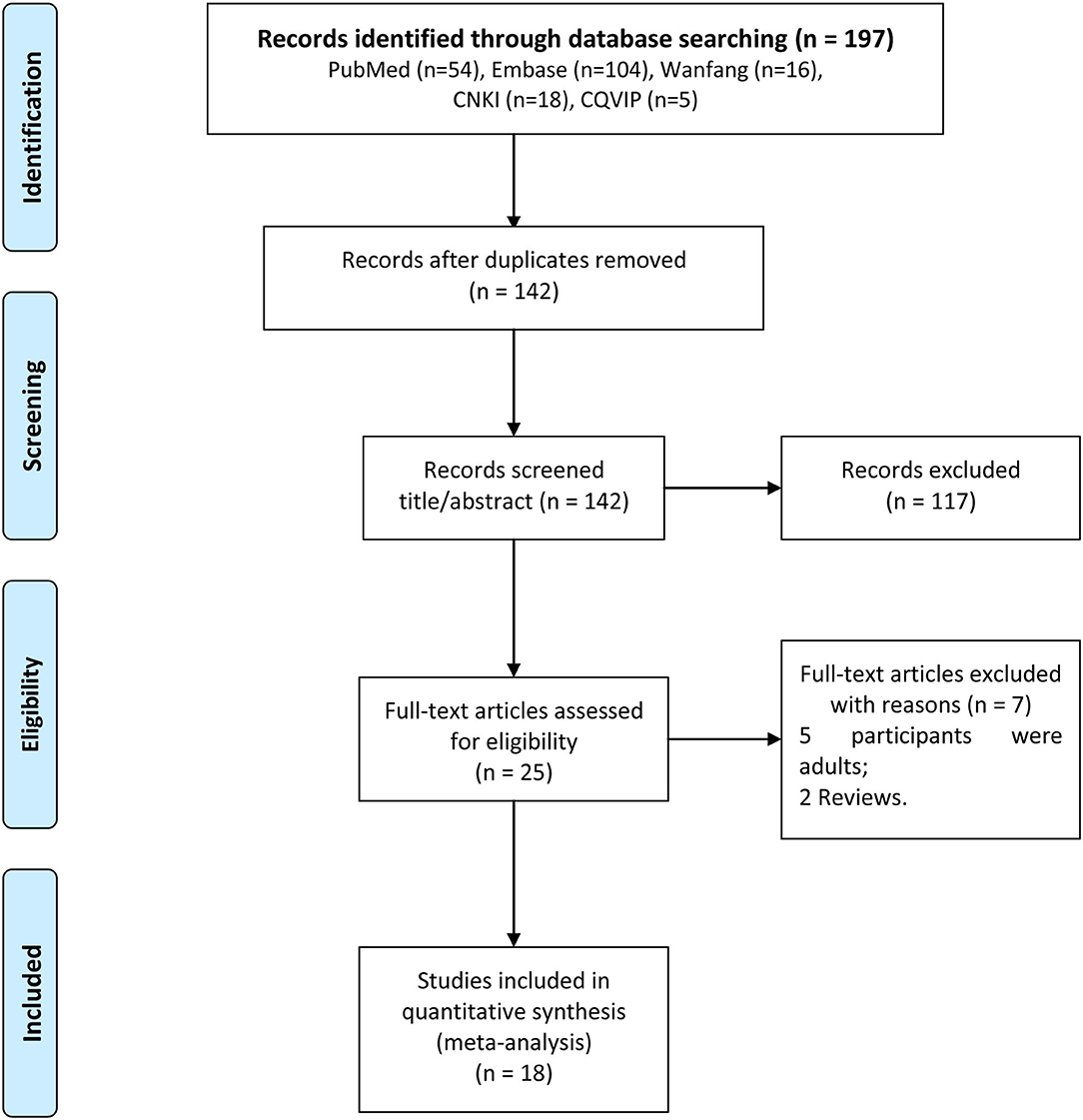
Figure 1. The detailed flow chart for study selection.
The Baseline Characteristics and Quality Assessment of Included Studies
As shown in Table 1, total 3,495 subjects including 1,392 cases in asthma group and 2,103 cases in control group were enrolled in the present study. The studies included in the meta-analysis were all published from 2010 to 2020. Among these articles, the subjects in eight studies were Asians, eight articles were Caucasians, one study were Americans, and one study were African-Americans. For subjects in the control group, there were two studies with population-based controls and 16 studies with hospital-based controls.
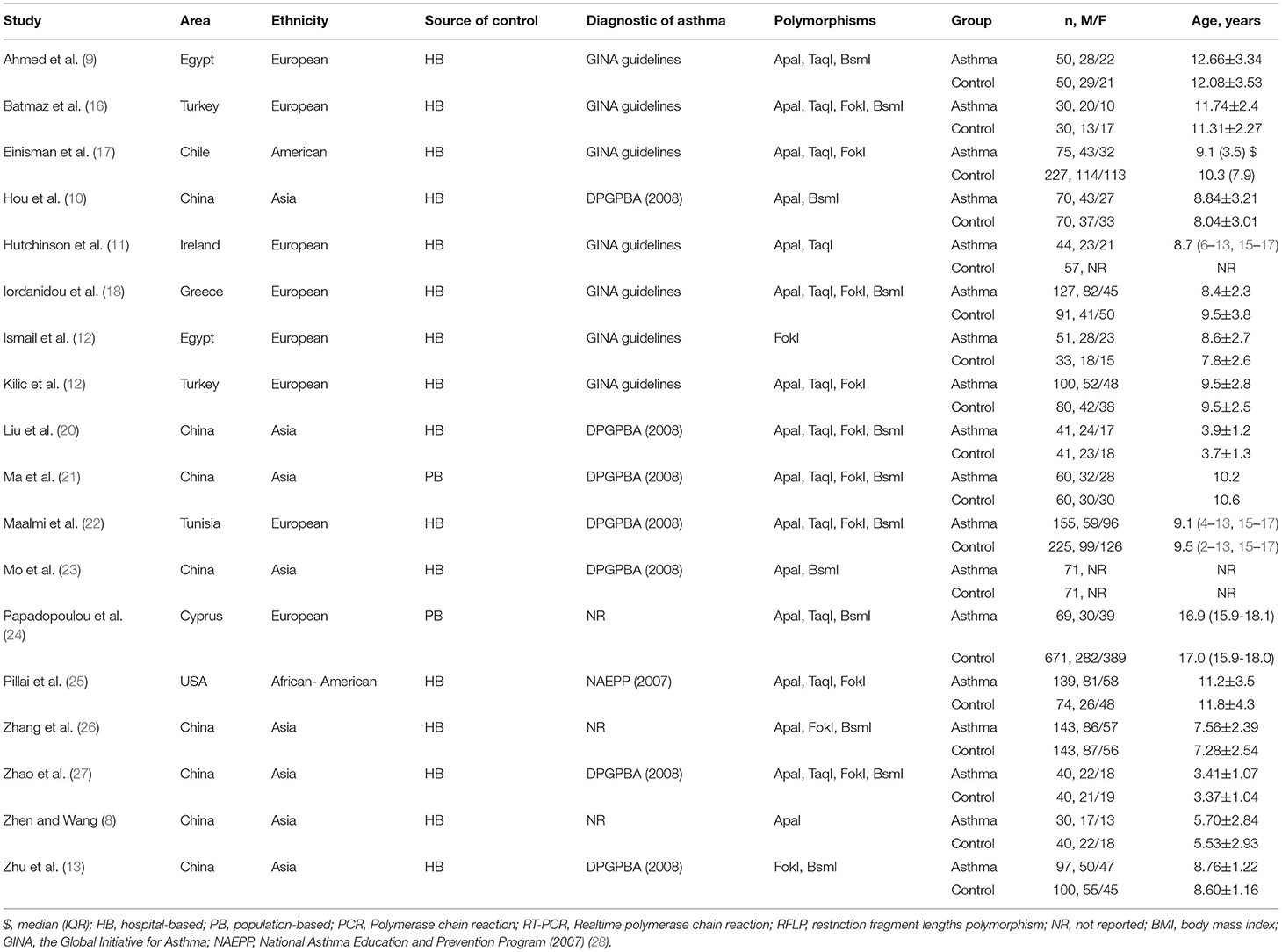
Table 1. Characteristics of the included studies.
The genotype data and HWE test results of the case group and the control group were shown in Table 2. NOS scores of all included studies ranged from 5 to 8, suggesting an overall moderate methodological quality (Table 3).

Table 2. Frequency distribution of gene polymorphisms in the experimental group and the control group.
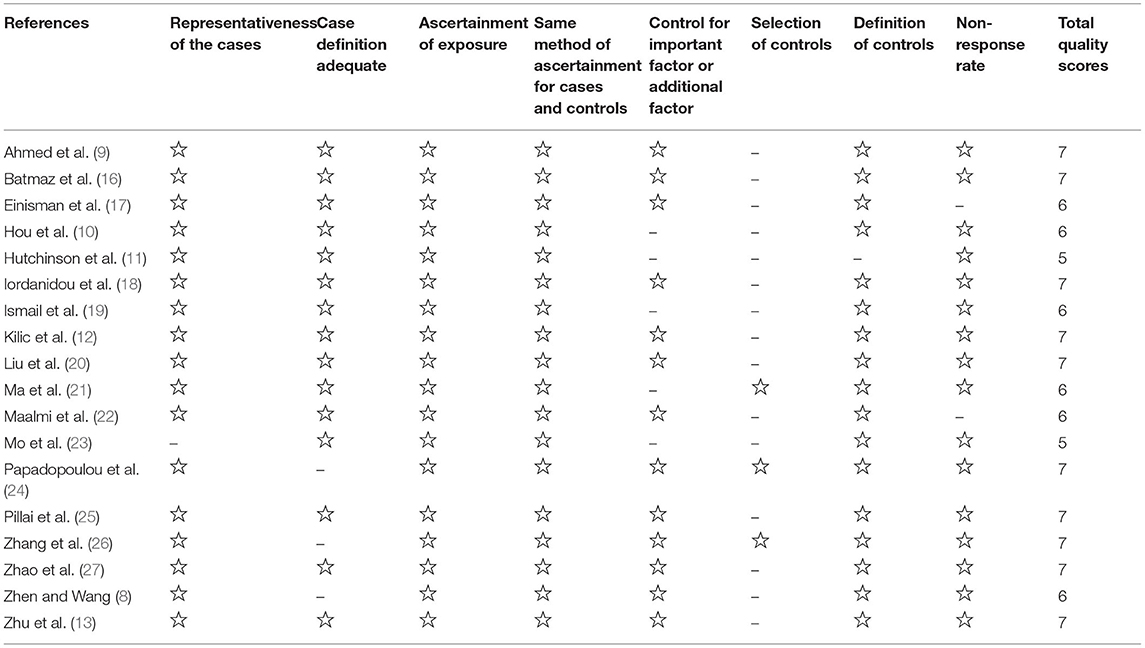
Table 3. Quality assessment of the included studies.
Meta-Analysis of VDR Polymorphism and Asthma
ApaI (rs7975232)
As shown in Figure 2, total 16 articles reported the association between ApaI (rs7975232) and asthma risk (8–12, 16–18, 20–27). Obvious heterogeneity across studies was observed in additive model (a vs. A: I2 = 89%, P < 0.00001), co dominant model (aa vs. AA: I2 = 84%, P < 0.00001; Aa vs. AA: I2 = 63%, P < 0.0006), dominant model (aa+Aa vs. AA: I2 = 77%, P < 0.00001), and recessive model (aa vs. AA+Aa: I2 = 86%, P < 0.00001). No significant association between ApaI (rs7975232) and asthma risk was calculated across additive model (a vs. A: OR (95%CI) = 0.82 (0.56, 1.21), P = 0.317), co dominant model (aa vs. AA: OR (95%CI) = 0.65 (0.31, 1.38), P = 0.263; Aa vs. AA: OR (95%CI) = 0.97 (0.66, 1.42), P = 0.866), dominant model (aa+Aa vs. AA: OR (95%CI) = 0.86 (0.55, 1.35), P = 0.520), and recessive model (aa vs. AA+Aa: OR (95%CI) = 0.73 (0.40, 1.32), P = 0.295).
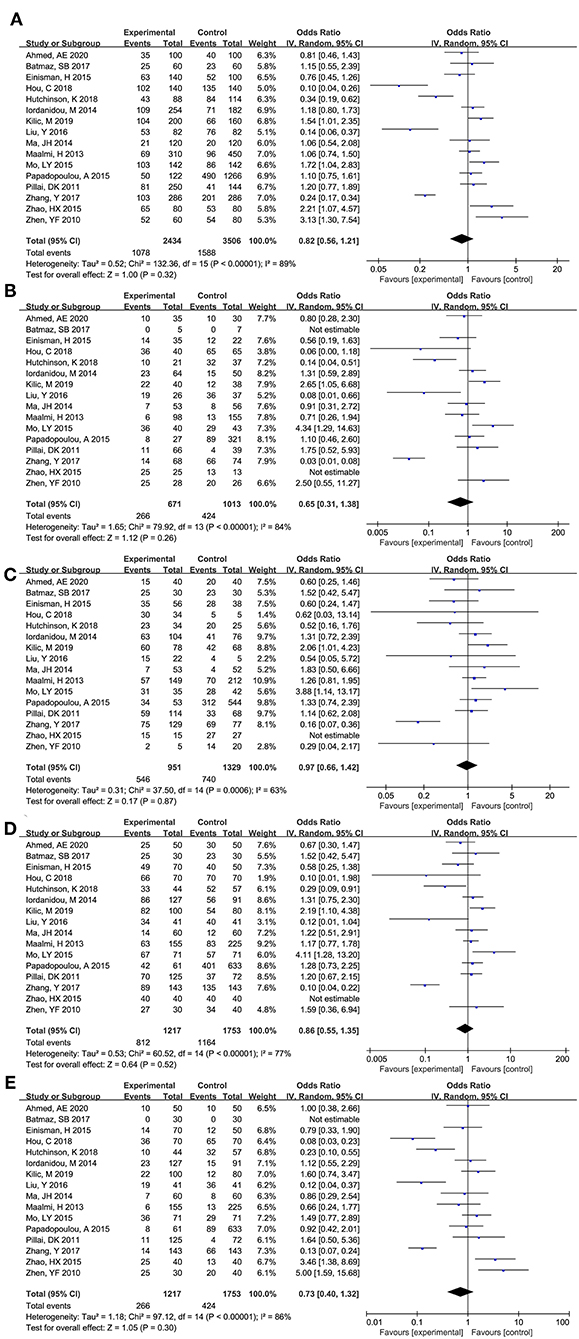
Figure 2. Forest plot for meta-analyzing the association between Vitamin D receptor ApaI (rs7975232) polymorphisms and childhood asthma. (A) additive model: a vs. A; (B) co dominant model: aa vs. AA; (C) co dominant model: Aa vs. AA; (D) dominant model: aa+Aa vs. AA; (E) recessive model: aa vs. AA+Aa.
The subgroup analysis was performed stratified by ethnicity, HWE, and source of controls (Table 4). No significant association was observed in all subgroup analysis (P>0.05). Meanwhile, the results of heterogeneity analysis showed that ethnicity, HWE, and source of subjects were not the source of heterogeneity.

Table 4. Outcomes of the subgroup analysis.
TaqI (rs731236)
As shown in Figure 3, total 12 articles researched on the role of TaqI (rs731236) in asthma risk (9, 11, 12, 16–18, 20–25, 27). Obvious heterogeneity across studies was observed in additive model (t vs. T: I2 = 71%, P < 0.0001), co dominant model (tt vs. TT: I2 = 63%, P = 0.002; Tt vs. TT: I2 = 50%, P = 0.02), dominant model (tt+Tt vs. TT: I2 = 53%, P = 0.82), and recessive model (tt vs. TT+Tt: I2 = 73%, P < 0.0001). Thus, the randomed effects model was used to calculated the pooled data, and the results showed that no significant association between TaqI (rs731236) and asthma risk was observed across additive model (t vs. T: OR (95%CI) = 0.93 (0.70, 1.23), P = 0.608), co dominant model [tt vs. TT: OR (95%CI) = 0.92 (0.49, 1.70), P = 0.783; Tt vs. TT: OR (95%CI) = 1.00 (0.72, 1.38), P = 0.996], dominant model [tt+Tt vs. TT: OR (95%CI) = 0.96 (0.70, 1.32), P = 0.817], and recessive model [tt vs. TT+Tt: OR (95%CI) = 0.87 (0.47, 1.62), P = 0.658].

Figure 3. Forest plot for meta-analyzing the association between Vitamin D receptor TaqI (rs731236) polymorphisms and childhood asthma. (A) additive model: t vs. T; (B) co dominant model: tt vs. TT; (C) co dominant model: Tt vs. TT; (D) dominant model: tt+Tt vs. TT; (E) recessive model: tt vs. TT+Tt.
Further subgroup analysis showed that HWE and source of control were two sources for the obvious heterogeneity across co dominant model (Tt vs. TT). Notably, significant association was found in additive model [t vs. T: OR (95%CI) = 0.45 (0.23, 0.89), P = 0.022], co dominant model [Tt vs. TT: OR (95%CI) = 0.36 (0.17, 0.77), P = 0.009], and dominant model [tt+Tt vs. TT: OR (95%CI) = 0.36 (0.15, 0.87), P = 0.024] among Asians. Moreover, significant association was also found in the population-based subgroup in co dominant model [Tt vs. TT: OR (95%CI) = 0.53 (0.31, 0.94), P = 0.029].
BsmI (rs1544410)
As shown in Figure 4, total 12 articles researched on the role of BsmI (rs1544410) in asthma risk (9, 10, 13, 16, 18, 20–24, 26, 27). Obvious heterogeneity across studies was observed in additive model (b vs. B: I2 = 73%, P < 0.0001), co dominant model (bb vs. BB: I2 = 68%, P = 0.003; Bb vs. BB: I2 = 56%, P = 0.03), dominant model (bb+Bb vs. BB: I2 = 68%, P = 0.002), and recessive model (bb vs. BB+Bb: I2 = 62%, P = 0.003). Thus, the randomed effects model was used to calculated the pooled data, and the results showed that no significant association between BsmI (rs1544410) and asthma risk was observed across additive model (b vs. B: OR (95%CI) = 0.87 (0.62, 1.21), P = 0.408), co dominant model (bb vs. BB: OR (95%CI) = 1.16 (0.61, 2.21), P = 0.665; Bb vs. BB: OR (95%CI) = 1.22 (0.76, 1.96), P = 0.409), dominant model (bb+Bb vs. BB: OR (95%CI) = 1.14 (0.67, 1.93), P = 0.627), and recessive model (bb vs. BB+Bb: OR (95%CI) = 0.80 (0.54, 1.20), P = 0.278).
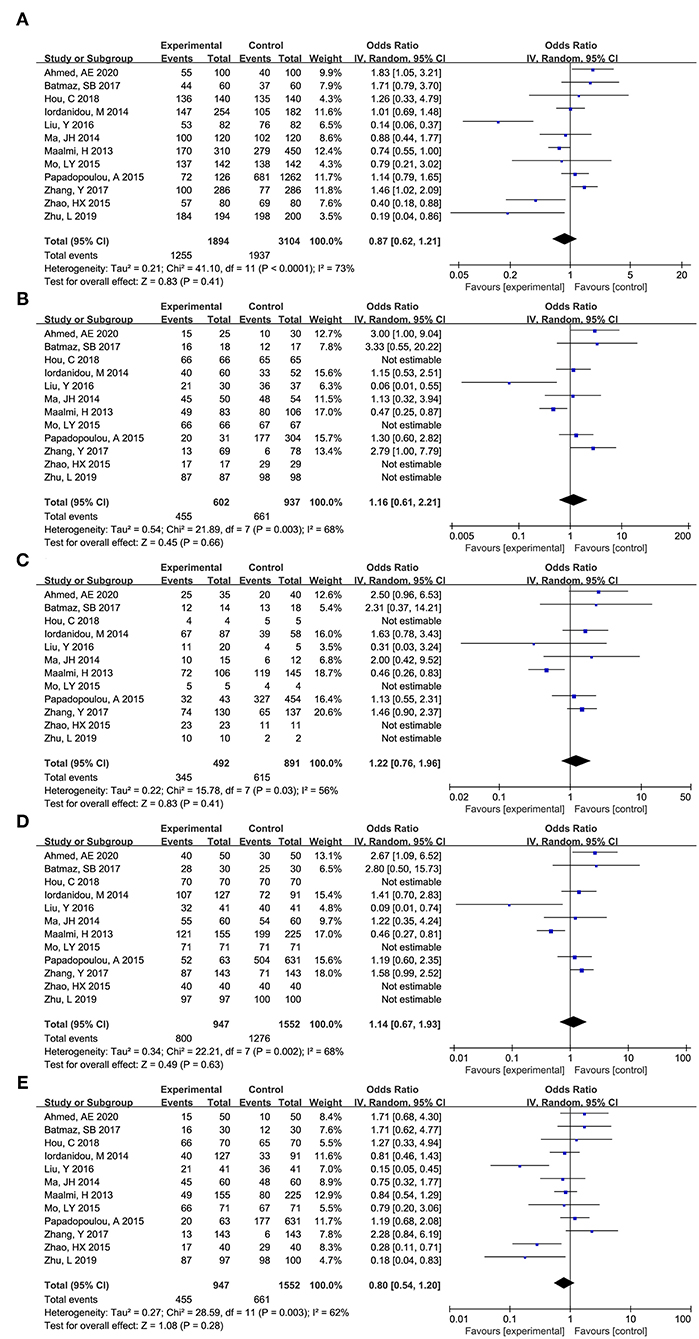
Figure 4. Forest plot for meta-analyzing the association between Vitamin D receptor BsmI (rs1544410) polymorphisms and childhood asthma. (A) additive model: b vs. B; (B) co dominant model: bb vs. BB; (C) co dominant model: Bb vs. BB; (D) dominant model: bb+Bb vs. BB; (E): recessive model: bb vs. BB+Bb.
Further subgroup analysis showed that no significant association was observed in all subgroup analysis (P > 0.05). Meanwhile, the results of heterogeneity analysis showed that ethnicity, HWE, and source of subjects were not the source of heterogeneity.
FokI (rs2228570)
As shown in Figure 5, total 12 articles researched on the role of FokI (rs2228570) in asthma risk (12, 13, 16–22, 25–27). Obvious heterogeneity across studies was observed in additive model (f vs. F: I2 = 77%, P < 0.00001), co dominant model (ff vs. FF: I2 = 68%, P = 0.0006), and recessive model (ff vs. FF+Ff: I2 = 74%, P < 0.0001). Thus, the randomed effects model was used to calculated the pooled data, and the results showed that no significant association between FokI (rs2228570) and asthma risk was observed across additive model (f vs. F: OR (95%CI) = 0.78 (0.57, 1.05), P = 0.102), co dominant model (ff vs. FF: OR (95%CI) = 0.67 (0.34, 1.34), P = 0.260), and recessive model (ff vs. FF+Ff: OR (95%CI) = 0.71 (0.39, 1.29), P = 0.266).

Figure 5. Forest plot for meta-analyzing the association between Vitamin D receptor FokI (rs2228570) polymorphisms and childhood asthma. (A) additive model: f vs. F; (B) co dominant model: ff vs. FF; (C) co dominant model: Ff vs. FF; (D) dominant model: ff+Ff vs. FF; (E): recessive model: ff vs. FF+Ff.
No significant obvious heterogeneity across studies was observed in co dominant model (Ff vs. FF: I2=0%, P = 0.89) and dominant model (ff+Ff vs. FF: I2=35%, P = 0.02), thus, the fixed effect model was used to calculate the pooled data, and the results showed that FokI (rs2228570) could significantly affect the risk of asthma across co dominant model (Ff vs. FF: OR (95%CI) = 0.82 (0.65, 1.02), P = 0.071) and dominant model (ff+Ff vs. FF: OR (95%CI) = 0.77 (0.63, 0.95), P = 0.016).
As for FokI (rs2228570), race, source of controls, HWE were not the source for the obvious heterogeneity. Subgroup analysis showed that FokI (rs2228570) SNP was significantly related with the risk of asthma in additive model (f vs. F: OR (95%CI) = 0.63 (0.43, 0.92), P = 0.015) and dominant model (ff+Ff vs. FF: OR (95%CI) = 0.67 (0.51, 0.88), P = 0.004) among Caucasians. Meanwhile, significant association was found in additive model (f vs. F: OR (95%CI) = 0.72 (0.54, 0.97), P = 0.03) and dominant model (ff+Ff vs. FF: OR (95%CI) = 0.67 (0.51, 0.88), P = 0.004) in the hospital-based subgroup. Significant association was found in additive model (f vs. F: OR (95%CI) = 1.90 (1.14, 3.17), P = 0.015), co dominant model (ff vs. FF: OR (95%CI) = 3.27 (1.18, 9.09), P = 0.023), and recessive model (ff vs. FF+Ff: OR (95%CI) = 2.97 (1.29, 6.83), P = 0.01) in population-based subgroup.
Publication Bias
No significant publication bias was observed for ApaI (rs7975232), TaqI (rs731236), BsmI (rs1544410), FokI (rs2228570) across the genotype models (P>0.05).
Discussion
Among childhood, asthma is accepted as the most common chronic disease. Recently, accumulating evidence researched the function role of VDR gene polymorphism in childhood asthma, and four SNPs, including BsmI (rs1544410), ApaI (rs7975232), FokI (rs2228570), and TaqI (rs731236), were the main gene locuses (3, 29). Based on the meta-analysis, our data showed that FokI (rs2228570) could significantly affect the risk of childhood asthma across co dominant model and dominant model, especially among Caucasians. Notably, among Asians, significant correction between TaqI (rs731236) and childhood asthma was also found in additive model (t vs. T), co dominant model (Tt vs. TT), and dominant model (tt+Tt vs. TT), as well as population-based subgroup in co dominant model (Tt vs. TT). No relationship was found between childhood asthma and the polymorphisms of ApaI (rs7975232) and BsmI (rs1544410).
Previous evidence showed that the level of Vitamin D was closely related with airway remodeling, the number of T regulatory cells, and expression level of pro-inflammatory cytokines and NF-κB (30). The connection between the deficiency of Vitamin D and poor asthma outcomes has been previously reported, such as worse symptomatology and poor lung function, and these defects could be reversed for offspring if Vitamin D was supplemented in deficient pregnant rodents (31). Zhen et al. demonstrated that, two out of four VDR polymorphisms could significantly affect the susceptibility of childhood asthma, including FokI and TaqI (8). Similarly, our study supported FokI and TaqI polymorphisms were associated with childhood asthma. Interestingly, it was different from the finding of a previous study (32), which gave support for that VDR gene ApaI (rs7975232) could contribute to asthma susceptibility.
The conflicting results might be explained by the following aspects. Firstly, it is well known that asthma is a clinical syndrome, and no gold standard test have been reported for making the diagnosis. Thus, physicians used multiple algorithms to make the final diagnosis, such as breath shortness, cough history, or wheezing history (33). Meanwhile, other baseline characteristics, such as smoking status, stress, gender, and age, were all related with the diagnosis of asthma (1). Secondly, based on genome-wide analysis studies, the researchers found that over 100 candidate genes were associated with the risk and development of asthma (34). Thirdly, the study designs and different genotyping methods might also account for the conflicting results. The obvious heterogeneity across included studies might also be attributed to these reasons.
There are some limitations should be noted. Firstly, the number of studies included in some subgroups was small, and more high-quality studies would be needed to verify the stability of the results. Secondly, since most of the included studies did not report the family history, living habits and other information of the study subjects, the quantitatively analyze based on these factors could not be performed to determine whether they affect the relationship between VDR gene polymorphisms and the childhood asthma susceptibility. Thirdly, the obvious heterogeneity across included studies could not be ignored. However, the moderate quality suggested that the analysis results had good credibility.
Conclusion
In summary, we concluded that FokI and TaqI polymorphisms were associated with childhood asthma susceptibility. However, it seems that ApaI and BsmI polymorphisms are not related with childhood asthma susceptibility. Due to these limitations, further multi-center study with high quality should be designed to verify the present conclusion.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
YZ: conception and design of the research, acquisition of data, analysis and interpretation of data, and drafting the manuscript. SL: statistical analysis and revision of manuscript for important intellectual content. All authors read and approved the final manuscript.
Funding
This study was supported by the Medical Science and Technology Development project of Yancheng (Nos. YK2019043 and YK2021051).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.843691/full#supplementary-material
References
1. Stern J, Pier J, Litonjua AA. Asthma epidemiology and risk factors. Semin Immunopathol. (2020) 42:5–15. doi: 10.1007/s00281-020-00785-1
2. Deng Q, Lu C, Norback D, Bornehag CG, Zhang Y, Liu W, et al. Early life exposure to ambient air pollution and childhood asthma in China. Environ Res. (2015) 143:83–92. doi: 10.1016/j.envres.2015.09.032
3. Makoui MH, Imani D, Motallebnezhad M, Azimi M, Razi B. Vitamin D receptor gene polymorphism and susceptibility to asthma, Meta-analysis based on 17 case-control studies. Ann Allergy Asthma Immunol. (2020) 124:57–69. doi: 10.1016/j.anai.2019.10.014
4. Wang TT, Tavera-Mendoza LE, Laperriere D, Libby E, MacLeod NB, Nagai Y, et al. Large-scale in silico and microarray-based identification of direct 1,25-dihydroxyvitamin D3 target genes. Mol. Endocrinol. (2005) 19:2685–95. doi: 10.1210/me.2005-0106
5. Amorim C, Oliveira JM, Rodrigues A, Furlanetto KC, Pitta F. Vitamin D, association with eosinophil counts and IgE levels in children with asthma. J Bras Pneumol. (2020) 47:e20200279. doi: 10.36416/1806-3756/e20200279
6. Emami Ardestani M, Movahedi A. Effect of vitamin D supplementation on improvement of symptoms in mild-to-moderate asthma patients with vitamin d insufficiency and deficiency. Tanaffos. (2020) 19:322–9.
7. Kostner K, Denzer N, Muller CS, Klein R, Tilgen W, Reichrath J. The relevance of vitamin D receptor (VDR) gene polymorphisms for cancer, a review of the literature. Anticancer Res. (2009) 29:3511–36.
8. Zhen YF, Wang L. Relationship of vitamin D receptor gene polymorphism with children asthma and wheezy bronchitis (In Chineses). Chin J Prev Vet Med. (2010) 11:1055−8.
9. Ahmed AE, Hassan MH, Toghan R, Rashwan NI. Analysis of 25-hydroxy cholecalciferol, immunoglobulin E, and vitamin D receptor single nucleotide polymorphisms (Apa1, Taq1, and Bsm1), among sample of Egyptian children with bronchial asthma, A case-control study. Ann Allergy Asthma Immunol. (2020) 55:1349–58. doi: 10.1002/ppul.24785
10. Hou C, Zhu X, Chang X. Correlation of vitamin D receptor with bronchial asthma in children. Exp Ther Med. (2018) 15:2773–6. doi: 10.3892/etm.2018.5739
11. Hutchinson K, Kerley CP, Faul J, Greally P, Coghlan D, Louw M, et al. Vitamin D receptor variants and uncontrolled asthma. J Clin Lab Anal. (2018) 50:108–16. doi: 10.23822/EurAnnACI.1764-1489.46
12. Kilic M, Ecin S, Taskin E, Sen A, Kara M. The vitamin D receptor gene polymorphisms in asthmatic children, a case-control study. Pediatr Allergy Immunol. (2019) 32:63–9. doi: 10.1089/ped.2018.0948
13. Zhu L, Li JH, Ma XB. Study on the relationship between 25-hydroxyvitamin D concentration and its receptor gene polymorphisms and childhood asthma (In Chinese). Experimental and Laboratory Medicine. (2019) 37:897–900.
14. Wells G, Shea B, O'Connell D, Peterson J, Welch V, Losos M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. (2014). Available online at: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed 20 June, 2021).
15. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
16. Batmaz SB, Arikoglu T, Uyar N, Barlas I, Kuyucu S. The effect of vitamin D pathway genes on asthma susceptibility, asthma control and vitamin D levels in Turkish Asthmatic children. Int J Hum Genet. (2017) 17:76–85. doi: 10.1080/09723757.2017.1351128
17. Einisman H, Reyes ML, Angulo J, Cerda J, López-Lastra M, Castro-Rodriguez JA. Vitamin D levels and vitamin D receptor gene polymorphisms in asthmatic children, a case-control study. Pediatr Allergy Immunol. (2015) 26:545–50. doi: 10.1111/pai.12409
18. Iordanidou M, Paraskakis E, Giannakopoulou E, Tavridou A, Gentile G, Borro M, et al. Vitamin D receptor ApaI a allele is associated with better childhood asthma control and improvement in ability for daily activities. Omics. (2014) 18:673–81. doi: 10.1089/omi.2014.0023
19. Ismail MF, Elnady HG, Fouda EM. Genetic variants in vitamin D pathway in Egyptian asthmatic children, a pilot study. Hum Immunol. (2013) 74:1659–64. doi: 10.1016/j.humimm.2013.08.284
20. Liu Y, Zhang H, Qiao Y. Relationship of vitamin D receptor gene polymorphism and children asthma and wheezy bronchitis (In Chineses). China J Modern Med. (2016) 26:36–9.
21. Ma JH, Tang CC, Zhang XH, Gao Y, Bai H. Correlation between Vitamin D receptor gene polymorphisms and asthma in Chinldren of Hui nationality in Ningxia (In Chinese). Ningxia Medical J. (2014) 36:870–3. doi: 10.13621/j.1001-5949.2014.100870
22. Maalmi H, Sassi FH, Berraies A, Ammar J, Hamzaoui K, Hamzaoui A. Association of vitamin D receptor gene polymorphisms with susceptibility to asthma in Tunisian children, a case control study. Hum Immunol. (2013) 74:234–40. doi: 10.1016/j.humimm.2012.11.005
23. Mo LY, Deng YC, Huang CZ, Liu JL. Association between polymorphism of vitamin D receptor gene and asthma in Children (In Chinese). Chin J Contemp Pediatr. (2015) 23:742–4. doi: 10.11852/zgetbjzz2015-23-07-21
24. Papadopoulou A, Kouis P, Middleton N, Kolokotroni O, Karpathios T, Nicolaidou P, et al. Association of vitamin D receptor gene polymorphisms and vitamin D levels with asthma and atopy in Cypriot adolescents, a case-control study. Multidiscip Respir Med. (2015) 10:26. doi: 10.4081/mrm.2015.304
25. Pillai DK, Iqbal SF, Benton AS, Lerner J, Wiles A, Foerster M, et al. Associations between genetic variants in vitamin D metabolism and asthma characteristics in young African Americans, a pilot study. J Investigat Med. (2011) 59:938–46. doi: 10.2310/JIM.0b013e318220df41
26. Zhang Y, Wang Z, Ma T. Associations of Genetic Polymorphisms Relevant to Metabolic Pathway of Vitamin D3 with Development and Prognosis of Childhood Bronchial Asthma. DNA Cell Biol. (2017) 36:682–92. doi: 10.1089/dna.2017.3730
27. Zhao HX, Chen XR, Wu CY, Zhuang HN. Study on the correlation of 25-(OH)-VD and Vitamin D receptor gene polymorphism of Children and asthma (In Chinese). Chin Lab Diagno. (2015). 1894–7.
28. Horner CC, Bacharier LB. Diagnosis and management of asthma in preschool and school-age children: focus on the 2007 NAEPP Guidelines. Curr Opin Pulm Med. (2009) 15:52–6. doi: 10.1097/MCP.0b013e32831da8ea
29. Ruan Z, Shi Z, Zhang G, Kou J, Ding H. Asthma susceptible genes in children, A meta-analysis. Medicine (Baltimore). (2020) 99:e23051. doi: 10.1097/MD.0000000000023051
30. Hall SC, Agrawal DK. Vitamin D and Bronchial Asthma, An Overview of Data From the Past 5 Years. Clin Ther. (2017) 39:917–29. doi: 10.1016/j.clinthera.2017.04.002
31. Yurt M, Liu J, Sakurai R, Gong M, Husain SM, Siddiqui MA, et al. Vitamin D supplementation blocks pulmonary structural and functional changes in a rat model of perinatal vitamin D deficiency. Am J Physiol Cell Physiol. (2014) 307:L859–867. doi: 10.1152/ajplung.00032.2014
32. Zhao DD, Yu DD, Ren QQ, Dong B, Zhao F, Sun YH. Association of vitamin D receptor gene polymorphisms with susceptibility to childhood asthma, A meta-analysis. Pediatr Pulmonol. (2017) 52:423–9. doi: 10.1002/ppul.23548
33. de Jong C. C. M., Pedersen E. S. L., Mozun R., Muller-Suter D., Jochmann A., Singer F., et al. (2020). Diagnosis of asthma in children, findings from the Swiss Paediatric Airway Cohort. Eur Respir J. 56 doi: 10.1183/13993003.congress-2020.4020
Keywords: vitamin D receptor, polymorphisms, childhood asthma, systematic review, susceptibility
Citation: Zhou Y and Li S (2022) Meta-Analysis of Vitamin D Receptor Gene Polymorphisms in Childhood Asthma. Front. Pediatr. 10:843691. doi: 10.3389/fped.2022.843691
Received: 26 December 2021; Accepted: 23 February 2022;
Published: 01 April 2022.
Edited by:
Viviana Moschese, University of Rome Tor Vergata, ItalyCopyright © 2022 Zhou and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheng Li, bGlzaGVuZ3ZpcDIwODRAMTYzLmNvbQ==