
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Pediatr. , 10 March 2022
Sec. Pediatric Surgery
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.836230
This article is part of the Research Topic Innovative Approaches in Pediatric Surgical Oncology View all 17 articles
 Fredrik Sundquist1
Fredrik Sundquist1 Kleopatra Georgantzi1,2
Kleopatra Georgantzi1,2 Kirsten Brunsvig Jarvis3Jesper Brok4Minna Koskenvuo5
Kirsten Brunsvig Jarvis3Jesper Brok4Minna Koskenvuo5 Jelena Rascon6
Jelena Rascon6 Max van Noesel7Per Grybäck8Joachim Nilsson8
Max van Noesel7Per Grybäck8Joachim Nilsson8 Arthur Braat9
Arthur Braat9 Mikael Sundin10Sandra Wessman11
Mikael Sundin10Sandra Wessman11 Nikolas Herold1,2Lars Hjorth12
Nikolas Herold1,2Lars Hjorth12 Per Kogner1
Per Kogner1 Dan Granberg13Mark Gaze14
Dan Granberg13Mark Gaze14 Jakob Stenman1,15*
Jakob Stenman1,15*Background: Half the children with high-risk neuroblastoma die with widespread metastases. Molecular radiotherapy is an attractive systemic treatment for this relatively radiosensitive tumor. 131I-mIBG is the most widely used form in current use, but is not universally effective. Clinical trials of 177Lutetium DOTATATE have so far had disappointing results, possibly because the administered activity was too low, and the courses were spread over too long a period of time, for a rapidly proliferating tumor. We have devised an alternative administration schedule to overcome these limitations. This involves two high-activity administrations of single agent 177Lu-DOTATATE given 2 weeks apart, prescribed as a personalized whole body radiation absorbed dose, rather than a fixed administered activity. “A phase II trial of 177Lutetium-DOTATATE in children with primary refractory or relapsed high-risk neuroblastoma - LuDO-N” (EudraCT No: 2020-004445-36, ClinicalTrials.gov Identifier: NCT04903899) evaluates this new dosing schedule.
Methods: The LuDO-N trial is a phase II, open label, multi-center, single arm, two stage design clinical trial. Children aged 18 months to 18 years are eligible. The trial is conducted by the Nordic Society for Pediatric Hematology and Oncology (NOPHO) and it has been endorsed by SIOPEN (https://www.siopen.net). The Karolinska University Hospital, is the sponsor of the LuDO-N trial, which is conducted in collaboration with Advanced Accelerator Applications, a Novartis company. All Scandinavian countries, Lithuania and the Netherlands participate in the trial and the UK has voiced an interest in joining in 2022.
Results: The pediatric use of the Investigational Medicinal Product (IMP) 177Lu-DOTATATE, as well as non-IMPs SomaKit TOC® (68Ga-DOTATOC) and LysaKare® amino acid solution for renal protection, have been approved for pediatric use, within the LuDO-N Trial by the European Medicines Agency (EMA). The trial is currently recruiting. Recruitment is estimated to be finalized within 3–5 years.
Discussion: In this paper we present the protocol of the LuDO-N Trial. The rationale and design of the trial are discussed in relation to other ongoing, or planned trials with similar objectives. Further, we discuss the rapid development of targeted radiopharmaceutical therapy and the future perspectives for developing novel therapies for high-risk neuroblastoma and other pediatric solid tumors.
Neuroblastoma (NBL) is a malignant disease that most commonly occurs in early childhood, and displays a wide heterogeneity regarding biological features, clinical presentation, morbidity, and mortality (1). It derives from neural crest cells, precursors of the sympatico-adrenergic system, manifesting in the adrenal glands and/or along the para-vertebral sympathetic ganglia (1). With an incidence of ~10 cases per million children under 15 years of age, approximately 1 in 7,000 children are affected (2). NBL is risk-stratified in terms of historical outcome in low-, intermediate- or high-risk based on age, stage, histologic classification, grade of tumor differentiation, MYCN amplification and chromosome 11q deletion status, according to The International Neuroblastoma Risk Group (INRG) Classification System (3). At least half of NBL patients are high-risk (HR). Treatment of HR-NBL generally consists of (i) an induction phase with intensive neoadjuvant chemotherapy, (ii) establishment of local control by surgery and radiotherapy, (iii) systemic remission consolidation therapy with high-dose chemotherapy and autologous stem cell reinfusion, and (iv) maintenance therapy with anti-GD2 antibodies and retinoic acid (3–5). In spite of this multimodal treatment, survival has remained at ~50% in HR-NBL. In case of a relapse, primary refractory disease or ultra-high-risk features, the outcome is dismal (1, 3, 4, 6). Historically treatment options for relapsed or refractory disease have focused on further cytotoxic chemotherapy with unsatisfying outcomes, partly due to chemo-resistance and poor bone marrow reserve after prior therapies and bone marrow disease (7). There is no consensus regarding the most effective therapy in this setting and currently two other European trials are focusing on this group of patients: The VERITAS trial comparing the combination of cytotoxic chemotherapy and intravenous targeted 131I-mIBG radiotherapy with high-dose cytotoxic chemotherapy; (VERITAS trial, Institute Gustave Roussy, Paris, France, ClinicalTrials.gov Identifier: NCT03165292) and the MINIVAN trial that compares different combinations of anti-PD1 and anti-GD2 therapy and intravenous targeted 131I-mIBG radiotherapy, (MINIVAN trial, University Hospital Southampton NHS Foundation Trust, UK, ClinicalTrials.gov Identifier: NCT02914405). In addition, the BEACON trial comparing the combination of cytotoxic chemotherapy and anti-VEGF therapy with cytotoxic chemotherapy alone; (BEACON trial, University of Birmingham, ClinicalTrials.gov Identifier: NCT02308527) was recently finalized. Also, a multinational trial evaluating the combination of Naxitamab (anti-GD2) and GM-CSF (YmAbs Therapeutics, ClinicalTrials.gov Identifier: NCT03363373) is currently recruiting in several European countries.
Neuroblastoma is known to be a radiosensitive disease, although if the disease is localized in several different sites external beam radiotherapy is not suitable. Therefore, targeted molecular radiotherapy is a more attractive treatment option in this setting, as it delivers tumor specific radiation and can target multiple sites of disease from the same administration (8–14). Studies have shown that 85–90% of neuroblastomas express the noradrenaline transporter molecule and can be targeted with the catecholamine analog, meta-iodobenzylguanidine (mIBG), labeled with 123I for imaging and with the β-emitter 131I for therapy. Molecular radiotherapy with 131I-mIBG has been used in relapsed and refractory neuroblastoma since the mid 1980's (15). Published data includes results from Phase I, Phase II trials and Pilot Studies with reported response rates ranging from 0 to 60% but there has been a wide variation in the administered radiation doses and methods of response assessment (16–20). The dose limiting toxicity for 131I-mIBG is confined to the bone marrow and attempts to increase the response rate to 131I-mIBG have included dose escalation and the use of radio-sensitizing agents, for example Topotecan. Both of these approaches require stem cell support to circumvent myelotoxicity (21, 22).
Another alternative target for molecular radiotherapy in neuroblastoma is the somatostatin receptors. Prior studies during the 1990's characterized the expression of somatostatin receptors in neuroblastoma cell lines and in vivo scintigraphic tumor imaging suggested putative therapeutic applications. Further studies confirmed that somatostatin analog therapy was effective in neuroblastoma xenografts in vivo (23–27). Recent studies based on immunohistochemistry have demonstrated expression of all known somatostatin receptors SSTR 1–5 on primary neuroblastoma (28). More specifically, SSTR 2 is expressed in the majority of neuroblastomas, even in recurrent tumors and in primary refractory disease (29). This can be utilized according to the same principle as 123I- and 131I-mIBG, by targeting SSTR with somatostatin analogs that can be labeled with 68Ga for imaging and with the β-emitter 177Lu for therapy. 177Lu-DOTATATE is composed of a somatostatin analog (TATE) and a chelator (DOTA) that binds the radio-isotope Lutetium-177. TATE binds to somatostatin receptors 1–5 (30), the binding between TATE and SSTR-2 having the highest affinity. The cytotoxic effect of Lutetium is primarily caused by emission of β-radiation. The effective range of the β-radiation is about 0.67 mm, causing a local effect on approximately 106 cells. About 10% of the radiation energy emitted is γ radiation that can be detected by SPECT imaging and utilized for dosimetry by determination of radiation dosage to the tumor target sites and to organs at risk. PET/CT, using the tracer 68Ga-DOTATATE or DOTATOC, another somatostatin analog that binds to SSTR receptors, can be used for identifying patients eligible for treatment with 177Lu-DOTATATE and this method can also be used for evaluating the response to treatment (31). 177Lu-DOTATATE therapy is thus, theoretically analogous to the well-established mIBG-therapy, but it utilizes a different targeting molecule and also a different radio-isotope for delivering beta radiation specifically to the tumor lesions.
177Lu-DOTATATE targeting the SSTRs has been shown to be effective in the treatment of neuroendocrine tumors in adults. This type of tumor-specific radiation therapy, called peptide receptor radionuclide therapy (PRRT), has recently been established as second-line treatment for grade 1 and 2 midgut neuroendocrine tumors (NET), that progress after first-line treatment with octreotide (32). 177Lu-DOTATATE has been well-tolerated in adult patients with a low incidence of hematological and renal toxicity, which are the main reported side effects. Renal irradiation is compounded by proximal tubular reabsorption of the radiolabeled somatostatin analog and co-administration of amino acid solution has been shown to reduce the risk of renal damage, as has limiting the estimated cumulative radiation dose to the kidneys to 23 Gy or less. The administration of cationic amino acids saturates the renal tubular uptake of proteins/peptides and amino acids, thereby reducing the exposure to the radionuclide (33–35). Severe delayed complications such as secondary malignancies and renal insufficiency has been reported in adult cohorts, but in general, severe side effects are rare. Brabander et al. (36) found that 1.5% of patients developed myelodysplastic syndrome and 0.7% developed acute leukemia during a median follow-up of 5 years after Lu-DOTATATE treatment in a cohort of 610 patients. No therapy-related long-term renal or hepatic failure occurred. A study by Garske-Roman et al. (37) found similar frequencies in a cohort of 200 patients and a median follow-up of 31 months. In this cohort 4% of patients developed grade 2 and 0.5% grade 4 renal toxicity (30, 36, 37). In a recent report from the NETTER-1 Trial, 2% of 111 patients developed myelodysplastic syndrome, whereas no cases of acute myeloid leukemia were reported. One patient developed diffuse large B-cell lymphoma during long-term follow-up, deemed not related to the 177Lu-DOTATATE treatment. The long-term renal function was similar in treatment and control groups, but the number of evaluable patients was small (38).
Pilot studies on pediatric patients, performed by Gains et al. at the University College London Hospitals NHS Trust, UK (UCLH) and by Kong et al. the Royal Children's Hospital, Melbourne, Australia (RCH) have shown that 68Ga-DOTATOC or DOTATATE PET/CT is a feasible method to identify patients with neuroblastoma that can benefit PRRT with 177Lu-DOTATATE. Both of these studies reported promising results from treating children with refractory or relapsed neuroblastoma with 177Lu-DOTATATE, some of which achieving remission that lasted for several years (39, 40). A phase IIa LuDO trial at UCLH, did not, however, show an objective response among 14 evaluable patients (41). In this study, dose limiting toxicity was observed only in one patient and the investigators speculate that this may have been due to concurrent use of myelosuppressive antibiotics, rather than an actual side effect of the trial treatment. The measured renal radiation dose was lower than the objective in all cases and the median value was only about 70% of the 23 Gy objective. The main reason for this was the rapid disease progression in many of the study subjects, indicating that with an intensified dosing schedule, the administered activity could have been substantially increased in most patients. Despite the negative result, the investigators conclude that 177Lu-DOTATATE may have value as a treatment for neuroblastoma and propose further clinical trials to be conducted (29). The design of the LuDO-N Trial, described in this paper, builds on the experience of the recent LuDO-Trial.
The LUDO-N Trial (EudraCT number: 2020-004445-36, ClinicalTrials.gov Identifier: NCT04903899) is a prospective, non-blinded, open-label, single arm two stage, multicenter phase II trial for pediatric patients between 18 months and 18 years old with relapsed or refractory high-risk neuroblastoma. Patients are recruited from the Nordic Society of Pediatric Hematology and Oncology (NOPHO) catchment area, including the Nordic countries and Lithuania, and from the Netherlands with a combined population of roughly 50 million. The LuDO-N Trial is sponsored by the Karolinska University Hospital (Stockholm, Sweden). Study centers have been established in each of the participating countries and the 177Lu-DOTATATE treatment will be given at the Karolinska University Hospital, Stockholm Sweden, the Princess Máxima Center, Utrecht, The Netherland and possibly at a later stage at the University College London Hospitals, London, UK. The trial aims to confirm the dose and assesses the response to 177Lu-DOTATATE (provided by Advanced Accelerator Applications, a Novartis company) as a single agent for treatment of relapsed or refractory high-risk NBL in children. The pediatric use of the Investigational Medicinal Product (IMP) 177Lu-DOTATATE, as well as non-IMPs SomaKit TOC® (68Ga-DOTATOC) and LysaKare® amino acid solution for renal protection, have been approved for the LuDO-N Trial by the European Medicines Agency (EMA). Competent authority and ethical approvals and are being applied for separately in each of the participating countries. Fourteen patients will be recruited in the first stage and provided a response, as defined by the Revised International Neuroblastoma Response Criteria (INRC) 1 month after completion of therapy, is seen in 3 or more of these patients, a further 10 will be enrolled in the second stage (42, 43). Accrual is expected to last for up to 60 months. Follow-up continues until 5 years after the last 177Lu-DOTATATE treatment or death, of all included patients, whichever occurs first. At writing, the LuDO-N Trial has opened for recruitment in Sweden and Norway and the first patient has recently received 177Lu-DOTATATE treatment within the trial.
Participants are screened and recruited by the National Principal Investigator (PI), or delegate, in each of the participating countries. It is the responsibility of the national PI to give oral and written information about the trial and to obtain written informed consent for each patient to be registered. No trial specific procedure is carried out prior to the consent form being signed by the patient and/or parents or legal guardians. All patients undergo the following assessments as part of screening. Please see Tables 1, 2.
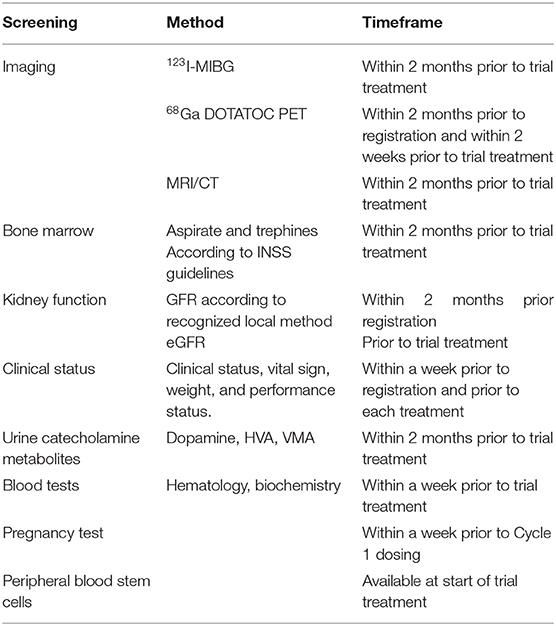
Table 1. Screening.
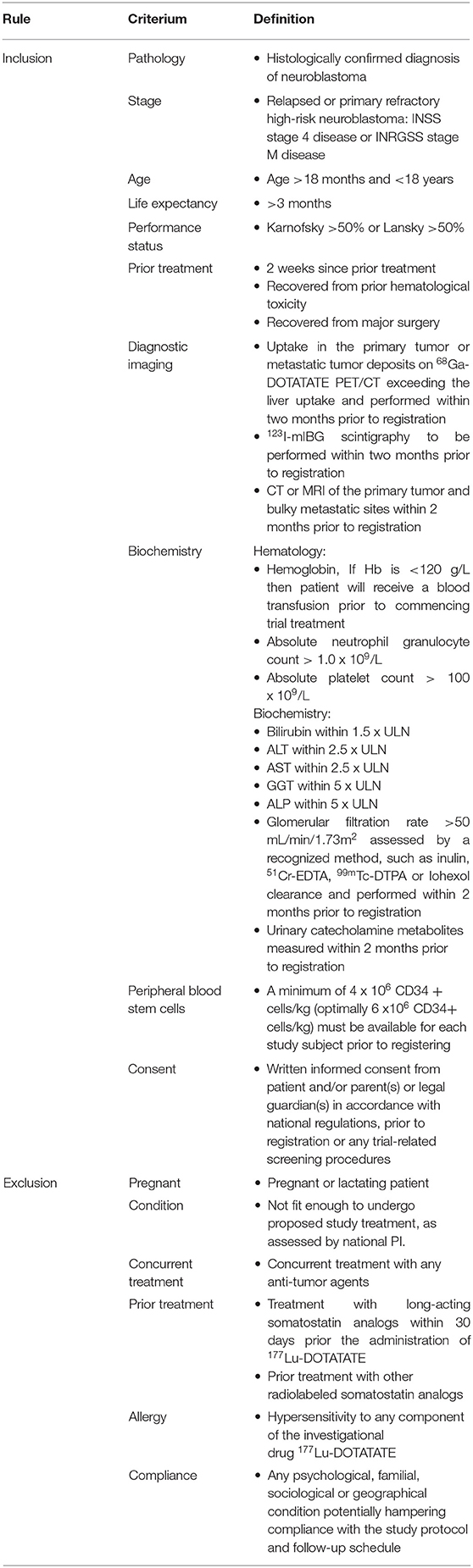
Table 2. Inclusion and Exclusion criteria.
Radiation exposure is governed by Swedish national legislation, as defined in the Swedish Radiation Safety Authority regulations SSMFS 2018:1 and 2018:5, in accordance with the European Council Directive 2013/59/EURATOM. It is recognized that children receiving molecular radiotherapy will require care and support from adults whilst receiving their treatment. Children receiving 177Lu-DOTATATE will be radioactive and will also have radioactive bodily products such as urine, saliva and vomit, all of which represent a potential radiation hazard to those adults caring for them during their treatment. Potential Supporting Persons will be informed of the risks of radiation exposure and trained in radiation hygiene and appropriate precautions to keep their personal radiation exposure as low as reasonably achievable – the ALARA principle. Patients will require specific medical interventions during their treatment from doctors, nurses and other health care professionals. These individuals will therefore receive some radiation during these tasks. Health care professionals are governed by annual radiation limits and it is essential, in keeping with the ALARA principle, that they do not receive avoidable radiation. Therefore, Supporting Persons are asked to undertake all normal child-care tasks such as washing, dressing, feeding, entertainment and support during the first 24 h after 177Lu-DOTATATE administration.
A baseline 68Ga-DOTATOC PET/CT is performed within 2 weeks, prior to 177Lu-DOTATATE treatment. A total of two doses of 177Lu-DOTATATE are administered intravenously 2–4 weeks apart. A weight-based activity of 200 MBq kg−1 is used for the first dose. The activity of the second dose is calculated based on whole body activity scans as well as SPECT CT scans to determine the absorbed kidney dose. The aim is to administer 177Lu-DOTATATE corresponding to a whole-body dose of 1,2 Gy, with a cumulative whole-body dose of about 2,4 Gy over two courses, and not exceeding a cumulative renal dose of 23 Gy, in order to avoid renal toxicity (41). Please see Table 3. LysaKare® amino acid solution for renal protection is administered as a 4-h infusion of 20 ml/kg, which corresponds to typical fluid resuscitation dose in children. This dose translates to the established adult dose of 1,000 ml in a child weighing 50 kg.
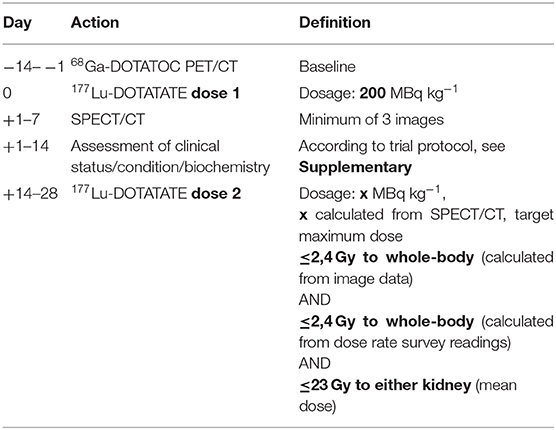
Table 3. Administration schedule.
To assess response to single agent 177Lutetium-DOTATATE treatment in patients with relapsed or refractory high-risk neuroblastoma.
• To assess long term survival and response.
• To assess treatment-related toxicity.
• To correlate tumor dosimetry with response.
• To correlate somatostatin type 2 receptor (SSTR-2) expression with 68Ga-DOTATOC PET/CT uptake.
• To correlate the uptake on 68Ga-DOTATOC PET/CT with response to 177Lu-DOTATATE therapy.
An adverse event (AE) is any untoward medical occurrence or experience in a patient administered with an investigational product and which does not necessarily have a causal relationship with the treatment. An AE can therefore be any unfavorable and unintended sign (such as a rash or an abnormal laboratory finding) symptom, or disease temporally associated with the use of the protocol treatment. Any AE occurring during the reporting period is to be reported in the eCRF. The Investigator should assess the seriousness and causality (relatedness) of all AEs experienced by the patient and document the assessments in the patient records. Each AE should be classified with the severity grade in accordance with the NCI Common Terminology Criteria for Adverse Events (CTCAE), version 5.0 (https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf). An AE not included in the CTCAE should be graded by an Investigator and recorded on the AE Form using a scale of (1) mild, (2) moderate or (3) severe. For each sign/symptom, the highest grade observed since the last visit should be recorded. Any Serious Adverse Event (SAE) occurring during the reporting period must be reported by the site investigator. Prompt initial reporting is required within 24 h after the investigator first becoming aware of the event. On becoming aware that a patient has experienced a SAE, the Investigator (or delegate) must complete, date and sign a trial specific SAE report. The report should be faxed together with a SAE fax cover sheet to Clinical Trials Office (CTO), Center for Clinical Cancer Studies (CKC), Karolinska University Hospital.
Trial data is collected and entered into the eCRF system PheedIt provided by Clinical Trials Office (CTO), Center for Clinical Cancer Studies (CKC), Karolinska University Hospital. eCRFs are required to be completed for each subject enrolled in the trial and all continuously collected data will be entered in the eCRF in a timely manner, within 1 month. All data must be entered in English. The PI is responsible for ensuring the accuracy, completeness and legibility of the data recorded in the eCRFs. Study monitors, data manager or the study statistician will review data according to the Monitoring Plan and Data Management Plan. Queries that are sent to site will require response and confirmation or correction of the data by delegated site staff. The Data Management Plan provides detailed information about data collection and data management throughout the trial.
The source documents consist of the medical records and any additional relevant documentation for trial purpose. This documentation will contain trial information such as trial number, date of informed consent, trial assignment and the name of the trial PI.
Source data for all variables will be defined in a source data log, which will be stored in the Investigator's Site File. Specific trial information such as trial title, trial number, date of informed consent, trial treatment and that the patient adheres to the inclusion and exclusion criteria should be recorded in the medical record.
Prior to site activation of each participating site must have an Investigator Site File with all essential documents in place, including authority approvals, Clinical Study Site Agreements and a signed delegations log. Key members of the site research team will be required to attend either a meeting or a teleconference covering aspects of the trial aim and design, protocol procedures, Adverse Event reporting, collection and reporting of data and record keeping.
The trial quality will be assured by trial monitoring in accordance with ICH-GCP of the trial sites in all participating countries. The monitoring will be carried out in accordance with the risk assessment and a common Monitoring Plan prepared by the monitoring unit in Sweden. At least three monitoring visits will be performed; the site initiation visit, a visit after the first included patient and a close-out visit. Additional on-site monitoring visits or more extensive source data verification may be triggered for example by poor CRF return, poor data quality, low/high SAE reporting rates, excessive number of patient withdrawals or deviations. The data recorded in the eCRFs will be controlled for consistency with the source data/hospital records during the monitoring (source data verification). Any discrepancies of data will be documented and explained in the monitoring reports.
The Investigator and site staff will permit trial-related monitoring, audits, ethical review, and regulatory inspection(s) at their site, providing direct access to source data/documents.
The sample size calculation is based on a Simon Two Stage Minimax design and the primary outcome measure of response rate assessed by the Revised International Neuroblastoma Response Criteria at 1 month after completion of therapy (42, 43). A complete response + partial response rate of 40% or more is defined as the acceptable level of response. A response of 20% or less would be considered unacceptably low. The probability of obtaining a false negative result, β (i.e., incorrectly rejecting for further study a treatment with a true response rate of ≥ 40%) is set at 20%. The probability of obtaining a false positive result, α (i.e., incorrectly accepting for further study a treatment that has a true response rate ≤ 20%) is set at 10%. Stage 1 requires 14 eligible and evaluable patients, with a minimum of 3 to be responders to proceed to stage 2. A further 10 patients will be recruited in Stage 2. A minimum of 8 responses out of 24 patients would be considered success and indicate that the treatment is active and should go onto further studies to evaluate efficacy (while taking account of toxicity). A standard Simon 2 stage has been chosen over a single stage (e.g., A'Hern) design in order to allow the trial to be stopped sooner, and to prevent unnecessary exposure of patients to radiotherapy, if insufficient responses are seen. Simon Optimal (3 responses /12 patients after first stage, 8/25 at end) and Minimax (3/14, 8/24) designs gives very similar numbers, so the decision to choose the latter is largely arbitrary (one patient fewer in total, but slightly more conservative after first stage). Sample size calculations were performed using Sample Size Tables for Clinical Trials software by Machin and Campbell. Loss to follow-up is likely to be minimal; all patients are referred from clinicians at established oncology centers with excellent close relations and regular communication or the patient's continued care is at the recruiting hospital. In addition, it is current standard practice to follow-up patients until they are 18 and then refer them to adult late effect physicians (according to long term follow-up guidelines from Children's Cancer and Leukemia Group (CCLG) and other relevant guidelines).
Response to treatment is assessed using the Revised International Neuroblastoma Response Criteria (INRC). Overall response is defined as complete response, partial response, minor response, stable disease, or progressive disease. Baseline assessment is carried out within 2 months prior to registration and an additional 68Ga-DOTATOC PET/CT is performed within 2 weeks prior to treatment. Response evaluation is performed 1 month and 4 months post treatment. Overall response integrates tumor response in the primary tumor, soft tissue and bone metastases, and bone marrow. Primary and metastatic soft tissue sites are assessed by MRI or CT, 68Ga-DOTATOC PET/CT and 123I-mIBG imaging. Target and non-target lesions are defined and scored according to the RECIST 1.1 guidelines. Assessment of bone marrow involvement is done by evaluation of bilateral aspirates and bilateral trephine biopsies from a total of four sampled sites. The analysis of the primary outcome measure is carried out on an eligible and evaluable patient basis. Patients who are registered, but for any reason did not complete treatment and/or the first response evaluation at 1 month after EOT, are deemed not evaluable, and so will be excluded from the primary analysis. Outcomes for all patients will be reported on an intention-to-treat basis. Descriptive statistics are used to summarize baseline characteristics, treatment, report harms, and response outcomes.
• Response by the Revised International Neuroblastoma Response Criteria and RECIST 1.1 guidelines at 1 month after completion of therapy (42, 43).
• Response by the Revised International Neuroblastoma Response Criteria and RECIST 1.1 guidelines at 4 months after completion of therapy.
• Progression-free Survival (PFS), defined as the time from registration until objective tumor progression or death or to date of censoring for patients who do not experience the event during trial follow-up.
• Overall Survival (OS), defined as the time from registration into the trial until date of death (death from any cause) or to date of censoring for patients who do not experience the event during trial follow-up.
• Hematological and renal toxicity according to CTCAE 5.0.
• Tumor and risk organ dosimetry (SPECT/CT), defined as the absorbed dose in Gray that the tumor sites and organs of risk receive following each administration of 177Lu-DOTATATE.
• Semi-quantitative analysis of the expression of SSTR-2 on immunohistochemistry in the primary tumor histology. The results will be correlated with tumor uptake on 68Ga-DOTATOC PET/CT.
• The uptake on 68Ga-DOTATOC PET/CT measured by SUVmax (maximum standardized uptake value). Pre-treatment SUVmax values will be correlated to the response to 177Lu-DOTATATE therapy.
The two-stage design will ensure that the study is terminated after the first stage if there is insufficient evidence of therapeutic activity. If any unexpected severe adverse events (CTC grades 3, 4) are encountered, consideration will be given to suspending the entry of new patients pending clarification of a causal relationship, and the trial may be stopped if unacceptable toxicities are observed. An interim analysis will be performed after inclusion of the first 14 patients. The main analysis of all outcome measures is planned at 6 months after completion of treatment of the last patient. In addition, subsequent analysis of all survival outcome measures will be conducted 5 years after completion of treatment of the last patient.
Active in Sweden and Norway, recruiting since May 2021.
PRRT with 177Lu-DOTATATE is an attractive new option with potentially less adverse effects and a significantly lesser exposure to radiation for persons participating in the care of the patient, as compared to 131I-mIBG -therapy (36, 37, 44). Contributing factors to these findings have not been exactly defined, but probably include a lesser extent of accumulation of 177Lu-DOTATATE in the bone marrow, as well as a shorter biological half-life and a smaller proportion of gamma-radiation emitted by 177Lu as compared to 131I. While pilot trials on 177Lu-DOTATATE at UCLH, London and RCH, Melbourne have shown promising results, the phase IIa LuDO trial recently conducted at UCLH concluded that 177Lu-DOTATATE in children was safe, but ineffective at the given dose and dosing schedule (39–41). In the LuDO trial the administration schedule was based on what was shown to be effective in an adult neuroendocrine tumor (NET) setting with a fixed administered activity every 2 months over a period of 6 months and to be within safety limits for renal and hematological toxicity. While no objective responses were seen by the standard criteria, interim assessment did show a reduction in the mIBG semiquantitative score in three patients, indicating some effect of treatment, even if it was not sustained. Compared to NET, neuroblastoma is a rapidly proliferating tumor and the intervals between administered activity may have allowed re-population that would have masked any objective responses. While the aim was to deliver a maximum kidney dose of 23 Gy to all patients, the median kidney dose actually delivered was only 16,5 Gy with this fixed activity schedule (41). The aim of the current LuDO-N trial is to establish whether 177Lu-DOTATATE can be effective as a single agent, in the treatment of relapsed or primary refractory high-risk neuroblastoma, when the dose schedule is intensified to two doses delivered 2 weeks apart and the administered activity is optimized/personalized by dosimetry. Due to an anticipated increased risk of myelotoxicity, secondary to the short recovery interval between doses, autologous hematopoietic stem cells are available as stem cell support in all patients. The intensified dosing schedule is similar to the one used successfully in previous studies on 131I-mIBG in relapsed or primary refractory high-risk neuroblastoma and it allows for an increased dose rate as compared to the LuDO trial, without increasing the cumulative radiation dose (22).
To our knowledge, there are currently two similar clinical trials on radiopharmaceutical therapy in neuroblastoma. One is under preparation: Safety Evaluation of Peptide Receptor Radionuclide Therapy (PRRT) With 177Lu-DOTA0-Tyr3-Octreotate for Refractory or Recurrent Metastatic Neuroblastoma Expressing Somatostatin Receptors (NEUROBLU 02), Institut Universitaire du Cancer Toulouse – Oncopole, Toulouse, France (ClinicalTrials.gov Identifier: NCT03966651). The NEUROBLU 02 trial uses a dose escalation design to assess the effective dose and the highest dose of 177Lu-DOTATATE, that can be given safely without the need for stem cell re-infusion. In order to make results from the NEUROBLU 2 and LuDO-N trials comparable, the dosimetry and response evaluation protocols of these two trials have been harmonized. Another similar multi-center trial in the USA, is already recruiting: 67Cu-SARTATE™ Peptide Receptor Radionuclide Therapy Administered to Pediatric Patients with High-Risk, Relapsed, Refractory Neuroblastoma (ClinicalTrials.gov Identifier: NCT04023331). The trial is sponsored by Clarity Pharmaceuticals Ltd. SARTATE, similarly to DOTATATE, binds to the SSTR-2 receptor and the cytotoxic effect of 67Cu is, also similarly to 177Lu, caused by β-radiation. Imaging and response evaluation is performed using another copper isotope 64Cu. (45, 46). In addition, 131I-mIBG has been randomized as first line treatment, in two of the treatment arms of the currently ongoing Children's Oncology Group (COG) ANBL 1531 Trial (ClinicalTrials.gov Identifier: NCT03126916), in an effort to target the metastatic disease in an early stage of the treatment. The ANBL 1531 trial uses a weight-based dosing of 131I-mIBG (47).
While the crossfire effect of β-emitters like 131I, 177Lu or 67Cu, can be beneficial for treatment of bulky disease in a refractory disease or relapse setting, there is a concern, that the radiation energy might not be sufficient to cause a cytotoxic effect in single, or small clusters of metastatic cells, containing only a limited number of target antigens (48). In this situation, most of the radiation would be dispersed to surrounding healthy tissues and subsequently, the radiation dose to the metastatic cells may be insufficient. The higher linear energy transfer (LET) and significantly shorter path length of the α-particle emission from 213Bi or 225Ac, might be preferable for effective depletion of micro-metastasis, since a lethal dose to a small number of cells, can be delivered from only 1–20 α-particle traversals of the cell nucleus (48–50). Switching from PRRT based on 131I, 177Lu or 67Cu to targeted α-particle therapy (TAT) would, however, include a loss of the cross-fire effect caused by β-emitters, due to the significantly shorter path length of the α-particles compared to β-radiation. This is highly relevant in the context of the macroscopic and microscopic tumor heterogeneity that has been described in neuroblastoma, carrying the subsequent risk that while some tumor cells would be effectively targeted and sterilized, others might escape completely unharmed (45, 46). One possibility for delivering targeted α-particle therapy to bone metastases is to utilize osteomimetic radionuclides, such as 223Ra-dichloride (Xofigo®) that incorporates into newly formed bone matrix within osteoblastic metastatic lesions (51), but this might not be a feasible approach in a growing child. Alternatively, combinations of radionuclide conjugates with different targeting molecules could be explored. While there are many targeting options for neuroblastoma, the combination of 177Lu-DOTATATE with the already established 131I-mIBG therapy, could be a viable alternative for a future follow-up trial aimed at overcoming the problem of tumor heterogeneity.
Overall survival in high-risk neuroblastoma is about 50% and long-term survival in the setting of primary refractory disease or relapse is exceedingly rare. Novel therapies, such as ALK-inhibitors can offer a possibility to reach secondary remission in a selected group of patients, but for the vast majority of cases there are currently no effective treatment options. We estimate that the potential benefits of 177Lu-DOTATATE treatment with an intensified dosing schedule, outweigh the risks in this specific group of pediatric patients with primary refractory or relapsed high-risk neuroblastoma, in whom established options for curative treatment have been exhausted. We hope that the results from the LuDO-N trial and similar trials on radiopharmaceutical therapy for high-risk neuroblastoma, will generate valuable knowledge, leading to effective therapeutic options that can significantly improve survival in the future.
The trial will be conducted according to the trial protocol, ICH-GCP, EU-directive (2001/20/EC) and applicable regulatory requirements and in accordance with the principles described in the latest version of the Declaration of Helsinki, available through the World Medical Association (WMA) website: (https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/). The patient information and informed consent-form will incorporate wording that complies with relevant data protection and privacy legislation. The protocol and patient material will be submitted to and approved by the National Ethics Committees prior to implementation. It is the responsibility of the National Coordinating Investigators to ensure that all subsequent amendments gain the necessary local approval. This does not affect the individual clinicians' responsibility to take immediate action if thought necessary to protect the health and interest of individual patients.
FS, PG, JN, MS, SW, NH, LH, PK, DG, MG, and JS conceptualized and participated in drafting the LuDO-N trial protocol. KG, KJ, JB, JR, MK, and MN contributed with valuable feedback on the trial protocol, as well as with drafting national authority applications in order to enable implementation of the trial in their respective countries. AB contributed to the dosimetry and response evaluation protocols and was responsible for setting up a system for central review of the imaging. FS, KG, MG, and JS drafted the manuscript. All authors participated in critical review of the manuscript prior to submission.
The LuDO-N trial has been supported by funding from the Swedish Cancer Society, the Swedish Childhood Cancer Fund, Region Stockholm and Applied Accelerator Applications / Novartis. In addition, all investigational and non-investigational products have been provided free of charge for the LuDO-N trial by Applied Accelerator Applications / Novartis. MG was supported by the National Institute for Health Research, University College London Hospitals, Biomedical Research Center and the Radiation Research Unit at the Cancer Research UK City of London Center Award (C7893/A28990).
This study received funding from Applied Accelerator Applications, a Novartis company. The funder had the following involvement with the study: Advice on trial design, provision of all investigational and non-investigational products, free of charge for the LuDO-N trial and review of the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We are deeply thankful to Sanna Nyström and Claudia Maes at the Center for Clinical Cancer Studies at the Karolinska University Hospital for providing expert assistance in generating the eCRF and in administrative management of the trial, as well as to Helena Aaröe, Pernilla Callerström, Rut-Inger Enryd and Sofie Garpemo at the pediatric clinical trial unit HOPE at the Karolinska University Hospital, for providing expert assistance in the setup and clinical management of the trial, and finally to Daniela Niepel at Advanced Accelerator Applications / Novartis for valuable feedback on the manuscript.
1. Matthay KK, Maris JM, Schleiermacher G, Nakagawara A, Mackall CL, Diller L, et al. Neuroblastoma. Nat Rev Dis Primers. (2016) 2:16078. doi: 10.1038/nrdp.2016.78
2. Ries LAG. Cancer Incidence and Survival Among Children and Adolescents: United States Seer Program, 1975–1995. Bethesda, MD: National Cancer Institute (1999).
3. Ladenstein R, Pötschger U, Pearson ADJ, Brock P, Luksch R, Castel V, et al. Busulfan and melphalan versus carboplatin, etoposide, and melphalan as high-dose chemotherapy for high-risk neuroblastoma (Hr-Nbl1/Siopen): an international, randomised, multi-arm, open-label, phase 3 trial. Lancet Oncol. (2017) 18:500–14. doi: 10.1016/S1470-2045(17)30070-0
4. von Allmen D, Davidoff AM, London WB, Van Ryn C, Haas-Kogan DA, Kreissman SG, et al. Impact of extent of resection on local control and survival in patients from the cog A3973 study with high-risk neuroblastoma. J Clin Oncol. (2017) 35:208–16. doi: 10.1200/JCO.2016.67.2642
5. Holmes K, Pötschger U, Pearson ADJ, Sarnacki S, Cecchetto G, Gomez-Chacon J, et al. Influence of surgical excision on the survival of patients with stage 4 high-risk neuroblastoma: a report from the Hr-Nbl1/siopen study. J Clin Oncol. (2020) 38:2902–15. doi: 10.1200/JCO.19.03117
6. Basta NO, Halliday GC, Makin G, Birch J, Feltbower R, Bown N, et al. Factors associated with recurrence and survival length following relapse in patients with neuroblastoma. Br J Cancer. (2016) 115:1048–57. doi: 10.1038/bjc.2016.302
7. Herd F, Basta NO, McNally RJQ, Tweddle DA. A systematic review of re-induction chemotherapy for children with relapsed high-risk neuroblastoma. Eur J Cancer. (2019) 111:50–8. doi: 10.1016/j.ejca.2018.12.032
8. Gatcombe HG, Marcus RB Jr, Katzenstein HM, Tighiouart M, Esiashvili N. Excellent Local Control from Radiation Therapy for High-Risk Neuroblastoma. Int J Radiat Oncol Biol Phys. (2009) 74:1549–54. doi: 10.1016/j.ijrobp.2008.10.069
9. Robbins JR, Krasin MJ, Pai Panandiker AS, Watkins A, Wu J, Santana VM, et al. Radiation therapy as part of local control of metastatic neuroblastoma: the St Jude children's research hospital experience. J Pediatr Surg. (2010) 45:678–86. doi: 10.1016/j.jpedsurg.2009.11.003
10. Casey DL, Kushner BH, Cheung NK, Modak S, LaQuaglia MP, Wolden SL. Local control with 21-Gy radiation therapy for high-risk neuroblastoma. Int J Radiat Oncol Biol Phys. (2016) 96:393–400. doi: 10.1016/j.ijrobp.2016.05.020
11. Stenman J, Herold N, Svensson PJ, Kogner P. Improved local control by extensive surgery in high-risk neuroblastoma may be dependent on adjuvant radiotherapy. J Clin Oncol. (2017) 35:1965–6. doi: 10.1200/JCO.2016.72.1175
12. Aldridge MD, Peet C, Wan S, Shankar A, Gains JE, Bomanji JB, et al. Paediatric molecular radiotherapy: challenges and opportunities. Clin Oncol. (2021) 33:80–91. doi: 10.1016/j.clon.2020.11.007
13. Arumugam S, Manning-Cork NJ, Gains JE, Boterberg T, Gaze MN. The evidence for external beam radiotherapy in high-risk neuroblastoma of childhood: a systematic review. Clin Oncol. (2019) 31:182–90. doi: 10.1016/j.clon.2018.11.031
14. Davis L, Smith AL, Aldridge MD, Foulkes J, Peet C, Wan S, et al. Personalisation of molecular radiotherapy through optimisation of theragnostics. J Pers Med. (2020) 10:174. doi: 10.3390/jpm10040174
15. Wilson JS, Gains JE, Moroz V, Wheatley K, Gaze MN. A systematic review of 131i-meta iodobenzylguanidine molecular radiotherapy for neuroblastoma. Eur J Cancer. (2014) 50:801–15. doi: 10.1016/j.ejca.2013.11.016
16. Hartmann O, Lumbroso JD, Lemerle M, Schlumberger M, Ricard M, Aubert B, et al. The therapeutic use of I-131 meta-iodobenzylguanidine (Mibg) in neuroblastoma: a phase Ii study in 12 patients. Prog Clin Biol Res. (1988) 271:655–67.
17. Lewis IJ, Lashford LS, Fielding S, Flower MA, Ackery D, Kemshead J, et al. Phase I/Ii study of 131i Mibg in chemo-resistant neuroblastoma. The United Kingdom children's cancer study group (Ukccsg). Prog Clin Biol Res. (1991) 366:463–9.
18. Lumbroso J, Hartmann O, Schlumberger M. Therapeutic use of [131i]metaiodobenzylguanidine in neuroblastoma: a phase Ii study in 26 patients. “Societe Francaise D'oncologie Pediatrique” and nuclear medicine co-investigators. J Nucl Biol Med. (1991) 35:220–3.
19. Klingebiel T, Bader P, Bares R, Beck J, Hero B, Jürgens H, et al. Treatment of neuroblastoma stage 4 with 131i-meta-iodo-benzylguanidine, high-dose chemotherapy and immunotherapy. A Pilot Study. Eur J Cancer. (1998) 34:1398–402. doi: 10.1016/S0959-8049(98)00130-0
20. Matthay KK, Yanik G, Messina J, Quach A, Huberty J, Cheng SC, et al. Phase Ii study on the effect of disease sites, age, and prior therapy on response to iodine-131-metaiodobenzylguanidine therapy in refractory neuroblastoma. J Clin Oncol. (2007) 25:1054–60. doi: 10.1200/JCO.2006.09.3484
21. Matthay KK, Quach A, Huberty J, Franc BL, Hawkins RA, Jackson H, et al. Iodine-131–metaiodobenzylguanidine double infusion with autologous stem-cell rescue for neuroblastoma: a new approaches to neuroblastoma therapy phase I study. J Clin Oncol. (2009) 27:1020–5. doi: 10.1200/JCO.2007.15.7628
22. Gaze MN, Chang Y-Ci, Flux GD, Mairs RJ, Saran FH, Meller ST. Feasibility of dosimetry-based high-dose 131i-meta-iodobenzylguanidine with topotecan as a radiosensitizer in children with metastatic neuroblastoma. Cancer Biother Radiopharm. (2005) 20:195–9. doi: 10.1089/cbr.2005.20.195
23. Maggi M, Baldi E, Finetti G, Franceschelli F, Brocchi A, Lanzillotti R, et al. Identification, characterization, and biological activity of somatostatin receptors in human neuroblastoma cell lines. Cancer Res. (1994) 54:124–33.
24. O'Dorisio M, Chen F, O'Dorisio T, Wray D, Qualman S. Characterization of somatostatin receptors on human neuroblastoma tumors. Cell Growth Differ. (1994) 5:1–8.
25. Kogner P, Borgström P, Bjellerup P, Schilling FH, Refai E, Jonsson C, et al. Somatostatin in neuroblastoma and ganglioneuroma. Eur J Cancer. (1997) 33:2084–9. doi: 10.1016/S0959-8049(97)00212-8
26. Schilling F, Bihl H, Jacobsson H, Ambros PF, Martinsson T, Borgström P, et al. Combined (111)in-pentetreotide scintigraphy and (123)I-Mibg scintigraphy in neuroblastoma provides prognostic information. Med Pediatr Oncol. (2000) 35:688–91. doi: 10.1002/1096-911x(20001201)35:6<688::aid-mpo44>3.0.co;2-7
27. Borgström P, Hassan M, Wassberg E, Refai E-, Jonsson C, Larsson SA, et al. The somatostatin analogue octreotide inhibits neuroblastoma growth in Vivo. Pediatr Res. (1997) 46:328–32. doi: 10.1203/00006450-199909000-00014
28. Georgantzi K, Tsolakis AV, Stridsberg M, Jakobson A, Christofferson R, Janson ET. Differentiated expression of somatostatin receptor subtypes in experimental models and clinical neuroblastoma. Pediatr Blood Cancer. (2011) 56:584–9. doi: 10.1002/pbc.22913
29. Alexander N, Marrano P, Thorner P, Naranjo A, Van Ryn C, Martinez D, et al. Prevalence and clinical correlations of somatostatin receptor-2 (Sstr2) expression in neuroblastoma. J Pediatr Hematol Oncol. (2019) 41:222–7. doi: 10.1097/MPH.0000000000001326
30. Reubi JC, Schär JC, Waser B, Wenger S, Heppeler A, Schmitt JS, et al. Affinity profiles for human somatostatin receptor subtypes SST1-SST5 of somatostatin radiotracers selected for scintigraphic and radiotherapeutic use. Eur J Nucl Med. (2000) 27:273–82.
31. Alexander N, Vali R, Ahmadzadehfar H, Shammas A, Baruchel S. Review: the role of radiolabeled dota-conjugated peptides for imaging and treatment of childhood neuroblastoma. Curr Radiopharm. (2018) 11:14–21. doi: 10.2174/1874471011666171215093112
32. Strosberg J, El-Haddad G, Wolin E, Hendifar A, Yao J, Chasen B, et al. Phase 3 trial of (177)lu-dotatate for midgut neuroendocrine tumors. N Engl J Med. (2017) 376:125–35. doi: 10.1056/NEJMoa1607427
33. Bernard BF, Krenning EP, Breeman WA, Rolleman EJ, Bakker WH, Visser TJ, et al. D-Lysine reduction of indium-111 octreotide and yttrium-90 octreotide renal uptake. J Nucl Med. (1997) 38:1929–33.
34. Bodei L, Cremonesi M, Zoboli S, Grana C, Bartolomei M, Rocca P, et al. Receptor-mediated radionuclide therapy with 90y-dotatoc in association with amino acid infusion: a phase I study. Eur J Nucl Med Mol Imaging. (2003) 30:207–16. doi: 10.1007/s00259-002-1023-y
35. Taylor CA, Shankar A, Gaze MN, Peet C, Gains JE, Wan S, et al. Renal protection during 177lutetium dotatate molecular radiotherapy in children: a proposal for safe amino acid infusional volume during peptide receptor radionuclide therapy. Nucl Med Commun. (2021). 43:242–6. doi: 10.1097/MNM.0000000000001497
36. Brabander T, van der Zwan WA, Teunissen JJM, Kam BLR, Feelders RA, de Herder WW, et al. Long-term efficacy, survival, and safety of [(177)Lu-Dota,Tyr]octreotate in patients with gastroenteropancreatic and bronchial neuroendocrine tumors. Clin Cancer Res. (2017) 23:4617–24. doi: 10.1158/1078-0432.CCR-16-2743
37. Garske-Roman U, Sandstrom M, Fross Baron K, Lundin L, Hellman P, Welin S, et al. Prospective observational study of (177)Lu-Dota-octreotate therapy in 200 patients with advanced metastasized neuroendocrine tumours (Nets): feasibility and impact of a dosimetry-guided study protocol on outcome and toxicity. Eur J Nucl Med Mol Imaging. (2018) 45:970–88. doi: 10.1007/s00259-018-3945-z
38. Strosberg JR, Caplin ME, Kunz PL, Ruszniewski PB, Bodei L, Hendifar A, et al. 177lu-dotatate plus long-acting octreotide versus high-dose long-acting octreotide in patients with midgut neuroendocrine tumours (Netter-1): final overall survival and long-term safety results from an open-label, randomised, controlled, phase 3 trial. Lancet Oncol. (2021) 22:1752–63. doi: 10.1016/S1470-2045(21)00572-6
39. Gains JE, Bomanji JB, Fersht NL, Sullivan T, D'Souza D, Sullivan KP, et al. 177lu-dotatate molecular radiotherapy for childhood neuroblastoma. J Nucl Med. (2011) 52:1041–7. doi: 10.2967/jnumed.110.085100
40. Kong G, Hofman MS, Murray WK, Wilson S, Wood P, Downie P, et al. Initial experience with gallium-68 dota-octreotate Pet/Ct and peptide receptor radionuclide therapy for pediatric patients with refractory metastatic neuroblastoma. J Pediatr Hematol Oncol. (2016) 38:87–96. doi: 10.1097/MPH.0000000000000411
41. Gains JE, Moroz V, Aldridge MD, Wan S, Wheatley K, Laidler J, et al. A phase Iia trial of molecular radiotherapy with 177-lutetium dotatate in children with primary refractory or relapsed high-risk neuroblastoma. Eur J Nucl Med Mol Imaging. (2020) 47:2348–57. doi: 10.1007/s00259-020-04741-x
42. Brodeur GM, Pritchard J, Berthold F, Carlsen NL, Castel V. Revisions of the international criteria for neuroblastoma diagnosis, staging and response to treatment. J Clin Oncol. (1993) 11:1466–77. doi: 10.1200/JCO.1993.11.8.1466
43. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised recist guideline (Version 1.1). Eur J Cancer. (2009) 45:228–47. doi: 10.1016/j.ejca.2008.10.026
44. Gains JE, Walker C, Sullivan TM, Waddington WA, Fersht NL, Sullivan KP, et al. Radiation exposure to comforters and carers during paediatric molecular radiotherapy. Pediatr Blood Cancer. (2015) 62:235–9. doi: 10.1002/pbc.25250
45. Gains JE, Aldridge MD, Mattoli MV, Bomanji JB, Biassoni L, Shankar A, et al. 68ga-dotatate and 123i-Mibg as imaging biomarkers of disease localisation in metastatic neuroblastoma: implications for molecular radiotherapy. Nucl Med Commun. (2020) 41:1169–77. doi: 10.1097/MNM.0000000000001265
46. Gains JE, Sebire NJ, Moroz V, Wheatley K, Gaze MN. Immunohistochemical evaluation of molecular radiotherapy target expression in neuroblastoma tissue. Eur J Nucl Med Mol Imaging. (2018) 45:402–11. doi: 10.1007/s00259-017-3856-4
47. Weiss BD, Yanik G, Naranjo A, Zhang FF, Fitzgerald W, Shulkin BL, et al. A safety and feasibility trial of 131 I-Mibg in newly diagnosed high-risk neuroblastoma: a children's oncology group study. Pediatr Blood Cancer. (2021) 68:e29117. doi: 10.1002/pbc.29117
48. Sgouros G, Bodei L, McDevitt MR, Nedrow JR. Radiopharmaceutical therapy in cancer: clinical advances and challenges. Nat Rev Drug Discov. (2020) 19:589–608. doi: 10.1038/s41573-020-0073-9
49. Nayak TK, Norenberg JP, Anderson TL, Prossnitz ER, Stabin MG, Atcher RW. Somatostatin-receptor-targeted alpha-emitting 213bi is therapeutically more effective than beta(-)-emitting 177lu in human pancreatic adenocarcinoma cells. Nucl Med Biol. (2007) 34:185–93. doi: 10.1016/j.nucmedbio.2006.11.006
50. Zhang J, Kulkarni HR, Baum RP. 225ac-dotatoc-targeted somatostatin receptor alpha-therapy in a patient with metastatic neuroendocrine tumor of the thymus, refractory to beta-radiation. Clin Nucl Med. (2021) 46:1030–1. doi: 10.1097/RLU.0000000000003792
Keywords: neuroblastoma, relapse, refractory, 177Lu-DOTATATE, PRRT, radiopharmaceutical, therapy, high-risk
Citation: Sundquist F, Georgantzi K, Jarvis KB, Brok J, Koskenvuo M, Rascon J, van Noesel M, Grybäck P, Nilsson J, Braat A, Sundin M, Wessman S, Herold N, Hjorth L, Kogner P, Granberg D, Gaze M and Stenman J (2022) A Phase II Trial of a Personalized, Dose-Intense Administration Schedule of 177Lutetium-DOTATATE in Children With Primary Refractory or Relapsed High-Risk Neuroblastoma–LuDO-N. Front. Pediatr. 10:836230. doi: 10.3389/fped.2022.836230
Received: 15 December 2021; Accepted: 31 January 2022;
Published: 10 March 2022.
Edited by:
Sabine Sarnacki, Université de Paris, FranceReviewed by:
Rodrigo L. P. Romao, Dalhousie University, CanadaCopyright © 2022 Sundquist, Georgantzi, Jarvis, Brok, Koskenvuo, Rascon, van Noesel, Grybäck, Nilsson, Braat, Sundin, Wessman, Herold, Hjorth, Kogner, Granberg, Gaze and Stenman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jakob Stenman, amFrb2Iuc3Rlbm1hbkBraS5zZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.