
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Pediatr., 28 February 2022
Sec. Neonatology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.822551
 Zuzanna Kozłowska1*
Zuzanna Kozłowska1* Paulina Komasińska2
Paulina Komasińska2 Barbara Steinborn2Kinga Toboła-Wróbel3Marek Pietryga3Marta Szymankiewicz-Breborowicz1
Barbara Steinborn2Kinga Toboła-Wróbel3Marek Pietryga3Marta Szymankiewicz-Breborowicz1 Tomasz Szczapa4
Tomasz Szczapa4 Monika Bekiesińska-Figatowska5
Monika Bekiesińska-Figatowska5Dural venous sinus ectasia belongs to a rare group of venous sinus malformations of unknown origin and uncertain prognosis. We report the first patient with idiopathic congenital ectasia of the confluence of sinuses with thrombosis associated with bilateral polymicrogyria. It may highlight the causative relation between ischemia within the central nervous system due to torcular herophili ectasia with thrombosis in early pregnancy and the development of cortical malformations in neonates. We also highlight the role of MR neuroimaging in the diagnosis of these entities.
Dural venous sinus ectasia is a rare vascular defect representing a group of cerebral venous sinus malformations. It is mostly detected prenatally and located in the vicinity of the confluence of sinuses, an area also referred to as torcular herophili (1). The lesion results from venous sinus widening of an unknown origin. It may be associated with meningeal arteriovenous fistula, generalized ischemia, increased intracranial pressure leading to compression of the central nervous system (CNS), intracranial bleeding, consumptive coagulopathy, and circulatory failure (1). Prognosis for survival and psychomotor development is uncertain (1–3). We present the first case report of a patient with congenital ectasia of the confluence of sinuses with thrombosis diagnosed prenatally, which might have led to bilateral polymicrogyria (PMG) development.
The girl was diagnosed prenatally with a nodular, cystic-solid lesion in the posterior cranial fossa during routine ultrasound scan at the 22nd gestational week (GW) (Figures 1A,B). The mass raised suspicion of either an atypical teratoma or arachnoid cyst. On fetal magnetic resonance imaging (MRI) performed at the 23rd GW, the mass (38 × 35 × 43 mm), with features of internal bleeding (Figure 2c) and thrombosis (Figure 2f), was described as a giant dural venous sinus ectasia. The lesion pulled the cerebral hemispheres apart (Figure 2a), compressed the structures of the posterior cranial fossa (Figure 2d), and pushed the brain stem to the clivus (Figure 2g) but did not cause widening of the ventricular system (Figure 2). In the subsequent prenatal ultrasound examinations, the dimensions of the lesion gradually decreased (Figures 1C,D).
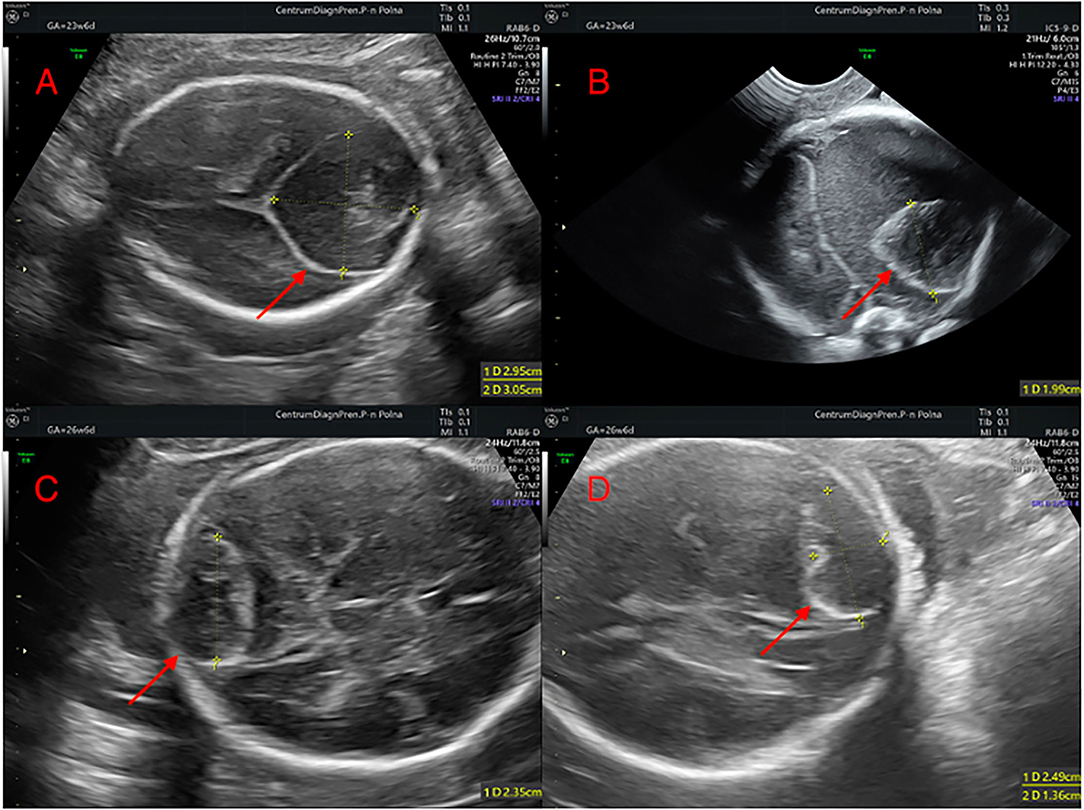
Figure 1. Prenatal ultrasound scans presenting the regression of the posterior fossa cyst: (A,B) 23 weeks of gestation; (C,D) 26 weeks of gestation.
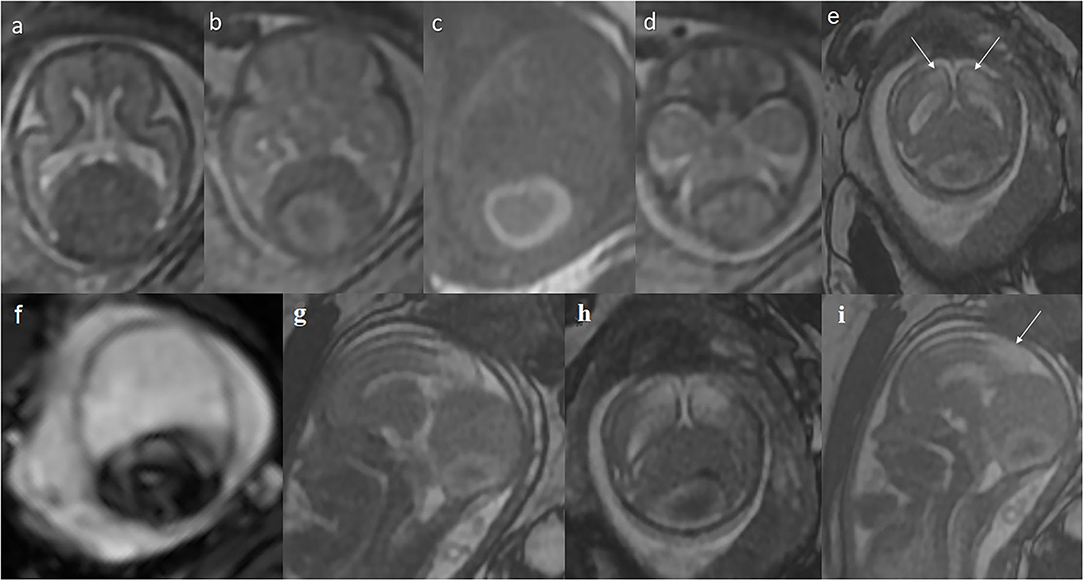
Figure 2. Prenatal MRI at the 23rd gestational week: (a–f) axial, (g,i) sagittal, and (h) coronal plane. Giant widening of the venous sinuses around the sinus confluence. The lesion lifts (h) and displaces the cerebral hemispheres apart (a,b) and compresses and displaces the posterior cranial fossa structures forward (d,g), with the brain stem pressed against the clivus (g). A thrombus (c) containing hemosiderin (g) inside. (e,i) Abnormal T2-hyperintensity of the posterior-medial parts of the cerebral hemispheres is appreciated (arrows) in FIESTA, indicating ischemia/edema caused by the huge mass of sinus ectasia.
The girl was born via C-section at 40 weeks of gestation in good condition, with Apgar score of 10 at the 1st and 5th minute of life and with a birth weight of 2,920 g. During hospitalization, in the first days of life, the physical examination and laboratory values were normal. The brain ultrasound showed neither bleeding nor other changes in the posterior cranial fossa. The brain echogenicity was normal.
In the 4th week of the girl's life, the brain MRI revealed a torcular pseudomass (20 × 8 × 12 mm) (Figures 3a,b) and deposits of hemosiderin in susceptibility-weighted imaging (SWI) sequence. The most striking finding was diffuse bilateral parasagittal occipital, parietal, and frontal polymicrogyria (Figures 3c–f). Abnormal vessels—probably venous anastomoses—were shown in the dorsal part of the midbrain (Figure 3c) and in the lower part of the left cerebellar hemisphere. On physical examination, hypertonia, tendency to scapular retraction, and epistotonus while in prone position were diagnosed. The patient was referred to the neurologic and neurosurgical outpatient clinics as well as to intensive rehabilitation.

Figure 3. First postnatal MRI scan at the age of 4 weeks. (a) Partial regression of dural ectasia (thick arrow). (b) One of the abnormal vessels (curved arrow). (c) Bilateral parasagittal polymicrogyria (thin arrows) in coronal and (d–f) axial planes.
In the 7th week of life, the girl was hospitalized due to a single episode of upper limb ejection and lower limb flexion during a gastrointestinal infection. The EEG during sleep was normal.
In the 5th month of life, a control brain MRI showed a slightly smaller mass within the torcular herophili (23 × 6 × 9 mm; Figure 4a), with smaller hemosiderin deposits in SWI sequence. The MR venography showed the flow in all dural sinuses (Figure 4b). The malformation of cortical development was prominently visualized in FLAIR sequence (Figures 4c–f).

Figure 4. MRI at the age of 5 months. (a) Further thinning of the mass. (b) Patent dural venous sinuses in MR venography. (c–f) The extent of polymicrogyria in the parasagittal parts of the occipital, parietal, and frontal lobes is even better seen now in axial FLAIR images.
The laboratory diagnostics covered genetic tests for mutations: A1298C and C677T in the MTHFR gene, G1691A in the clotting factor V gene, and G20210A in the prothrombin gene—none of which was found. Moreover, the activity of coagulation factors V, VII, VIII, protein C, and protein S was within normal limits.
At the 12th month of life, despite the malformation of cortical development, the girl's psychomotor development is harmonious, and the head circumference gains are normal.
Dural venous sinus ectasia belongs to a rare group of venous sinus malformations of unknown origin. One of the hypotheses explaining the patomechanism mentions vessel occlusion with thrombotic material causing venous hypertension and arteriovenous anastomoses formation.
Thrombus formation within the cerebral veins can occur in the prenatal and postnatal periods. Possible predisposing risk factors include an immature sinus structure with abnormal endothelium and slow blood flow, maternal coagulation disorders, prematurity, hypoxia, local and systemic inflammatory process, hematological disorders (e.g., deficiency of antithrombin III, protein C, protein S, factor V Leiden mutation, mutation of the prothrombin gene G20210 A, hyperhomocysteinemia, thrombophilia), polycythemia, and trauma (4, 5). Considering the characteristics of the MRI findings in the described case, we assume that the coagulation process occurred in utero. Despite the extensive diagnostics performed, no cause was found. Moreover, the underlying genetic etiology of PMG is heterogeneous, and mutations in more than 50 genes have been found. Genetic testing is usually performed when PMG is accompanied by other congenital malformations, dysmorphia (micro- or macrocephaly), developmental delay, or epilepsy and has the highest diagnostic yield when PMG is associated with abnormal head growth. In other cases, whole-exome or whole-genome sequencing might be performed (6). As our patient did not match any of the known phenotypes and early brain ischemia was detected, we waived the genetic testing.
Thrombus developing within the venous sinus malformation may result in brain damage in the ischemic mechanism (5, 7). A potential mechanism explaining the absence of neurological complications may be associated with the anastomoses formation that ensure proper venous blood drainage. In our patient, the abnormal vessels were found on postnatal MRI; however, early brain ischemia must have occurred. The fetal MRI at the 23rd GW shows T2-hyperintensity in the posterior parasagittal parts of both cerebral hemispheres, most likely representing ischemic insult, sufficiently distant in time not to restrict diffusion (Figures 2e,g–i). To the best of our knowledge, we present the first report of polymicrogyria co-existing with giant venous sinus ectasia with thrombus. Taking into consideration all findings in the prenatal imaging (dural abnormality and signs of brain ischemia) and the available knowledge of early ischemia as one of the possible causes of PMG (8), the case of our patient seems to prove the causative association of thrombosed giant dural sinus ectasia with PMG. Moreover, the patient presented with bilateral parasagittal parieto-occipito-frontal polymicrogyria not described before. The most resembling entity found in the literature was bilateral parasagittal parieto-occipital polymicrogyria (9).
The literature covering the topic of giant dural sinus ectasia consists mostly of case reports, in which clinical presentation and outcome differ significantly. The clinical manifestations in the neonatal period include macrocrania, hydrocephalus, seizures, consumptive coagulopathy, spontaneous thrombosis, and cardiac failure (2, 5). None of the above-mentioned manifestations was observed in our patient directly after birth. The prognosis for patients with dural sinus malformations is often poor, with mortality ranging between 38 and 67% (2). However, more recent publications report patients with no or little neurological deficits on follow-up examinations (3, 10). They suggest that, in most cases, dural venous sinus ectasia with thrombosis resolves spontaneously and is not associated with long-term disability (3). Interestingly, the outcome might not be associated with applied treatment and early postnatal symptoms. In the review of 30 cases, the difference between subgroups of neonates and older children is visible: only 26.7% of cases were diagnosed antenatally, of which 75% had a positive outcome, while a generally favorable clinical evolution involved 58.6% of patients (4). Localization of ectasia and thrombosis within the confluence of sinuses does not appear to be related with poor outcome like in the patient described in this report (3).
However, the prognosis in our patient must be considered foremostly in terms of diffuse malformation of cortical development. The wide spectrum of possible clinical manifestations of polymicrogyria ranges from normal individuals with selective impairment of cognitive functions to patients with severe encephalopathies and intractable epilepsy (10). Epilepsy develops in ~80% of patients, in majority within the first 5 years (11). Bilateral involvement, as in our patient, and involvement of more than half of a single hemisphere are poor prognostic factors (9). In the 7th week of life, the reported girl presented with limb ejections and flexions; however, we associate those symptoms with viral gastrointestinal infection at the time as the EEG was normal. The episodes have not been repeated so far, and her neurodevelopment is appropriate for her age.
An initial diagnosis of congenital dural venous sinus ectasia can be made during routine prenatal ultrasound, in which abnormalities within the posterior fossa are described. The differential diagnosis includes tumors, cysts, and Dandy–Walker syndrome (3). Surprisingly, during transfontanelle ultrasound in the first days of life, no abnormalities were found. This suggests that postnatal transfontanelle ultrasound may not always be sufficiently accurate, possibly due to lack of proper insight into the posterior fossa. Based on the available literature, we were able to identify only two cases in which brain ultrasound was mentioned as the imaging method of dural sinus ectasia in the neonatal period (1, 12). A diagnosis of polymicrogyria is possible on fetal ultrasound (13), although it is rarely reached without prenatal MRI. MRI is a method of choice both in utero and in the postnatal period for confirmation and for guiding the treatment in both entities described (14).
This report is the first to illustrate the possible causal relationship between giant dural sinus ectasia and polymicrogyria.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. Written informed consent was obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
ZK, PK, and KT-W collected, analyzed, and interpreted the patient's data and had a major contribution in writing the manuscript. BS performed and analyzed the patient's follow-up examination as well as critically revised the manuscript. MP performed, described, and interpreted the prenatal examinations. MS-B contributed to the design of the work and critically revised the manuscript. TS had a major contribution to the conception, drafting, and revising of the manuscript. MB-F retrospectively analyzed and described the patient's neuroimaging results. All authors contributed to the intellectual content of the manuscript, approved its final version, and agreed to be accountable for all aspects of the work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors wish to thank Professor A. J. Barkovich (University of California, San Francisco, CA, USA) for his valuable opinion on the causative mechanisms of polymicrogyria.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.822551/full#supplementary-material
Supplementary Figure 1. Scheme presenting the pathophysiology of polymicrogyria and torcular pseudomass development.
Supplementary Figure 2. Timeline.
1. Jenny B, Zerah M, Swift D, Le Tohic A, Merzoug V, Alvarez H, et al. Giant dural venous sinus ectasia in neonates. J Neurosurg Pediatr. (2010) 5:523–8. doi: 10.3171/2009.12.PEDS0862
2. Miller C, Guillaume D. Management of midline dural sinus malformations and review of the literature. Childs Nerv Syst. (2016) 32:1449–61. doi: 10.1007/s00381-016-3115-1
3. Fanou EM, Reeves MJ, Howe DT, Joy H, Morris S, Russell S, et al. In utero magnetic resonance imaging for diagnosis of dural venous sinus ectasia with thrombosis in the fetus. Pediatr Radiol. (2013) 43:1591–8. doi: 10.1007/s00247-013-2745-7
4. Visentin A, Falco P, Pilu G, Perolo A, Valeri B, Santini D, et al. Prenatal diagnosis of thrombosis of the dural sinuses with real-time and color Doppler ultrasound. Ultrasound Obstet Gynecol. (2001) 17:322–5. doi: 10.1046/j.1469-0705.2001.00372.x
5. Grigoriadis S, Cohen JE, Gomori JM. Prenatal thrombosis of torcular herophili with spontaneous resolution and normal outcome. J Neuroimaging. (2008) 18:177–9. doi: 10.1111/j.1552-6569.2007.00166.x
6. Stuttered CA, Brock S, Stouffs K, Fanjul-Fernandez M, Lockhart PJ, McGillivray G, et al. Genetic heterogeneity of polymicrogyria: study of 123 patients using deep sequencing. Brain Commun. (2020) 3:fcaa221. doi: 10.1093/braincomms/fcaa221
7. Sampaio L, Morana G, Severino M, Tortora D, Leao M, Rossi A. Torcular pseudomass: a potential diagnostic pitfall in infants and young children. Pediatr Radiol. (2017) 47:227–34. doi: 10.1007/s00247-016-3734-4
8. Squier W, Jansen A. Polymicrogyria: pathology, fetal origins and mechanisms. Acta Neuropathol Commun. (2014) 2:80. doi: 10.1186/s40478-014-0080-3
9. Barkovich AJ. Current concepts of polymicrogyria. Neuroradiology. (2010) 52:479–87. doi: 10.1007/s00234-009-0644-2
10. Spreafico R, Tassi L. Cortical malformations. Handb Clin Neurol. (2012) 108:535–57. doi: 10.1016/B978-0-444-52899-5.00047-2
11. Leventer RJ, Jansen A, Pilz DT, Stoodley N, Marini C, Dubeau F, et al. Clinical and imaging heterogeneity of polymicrogyria: a study of 328 patients. Brain. (2010) 133:1415–1427. doi: 10.1093/brain/awq078
12. Laurichesse Delmas H, Winer N, Gallot D, Lopes K, Perrotin F, Fluncker S, et al. Prenatal diagnosis of thrombosis of the dural sinuses: report of six cases, review of the literature and suggested management. Ultrasound Obstet Gynecol. (2008) 32:188–98. doi: 10.1002/uog.5348
13. Dhombres F, Nahama-Allouche C, Gelot A, Jouannic JM, de Villemeur TB, Saint-Frison MH, et al. Prenatal ultrasonographic diagnosis of polymicrogyria. Ultrasound Obstet Gynecol. (2008) 32:951–4. doi: 10.1002/uog.6251
Keywords: neonate, neuroimaging, cortical malformations, torcular herophili, central nervous system
Citation: Kozłowska Z, Komasińska P, Steinborn B, Toboła-Wróbel K, Pietryga M, Szymankiewicz-Breborowicz M, Szczapa T and Bekiesińska-Figatowska M (2022) Spontaneous Resolution of Congenital Dural Venous Sinus Ectasia Associated With Polymicrogyria—Case Report. Front. Pediatr. 10:822551. doi: 10.3389/fped.2022.822551
Received: 25 November 2021; Accepted: 17 January 2022;
Published: 28 February 2022.
Edited by:
Erkan Gökçe, Tokat Gaziosmanpaşa University, TurkeyReviewed by:
Flavio Giordano, University of Florence, ItalyCopyright © 2022 Kozłowska, Komasińska, Steinborn, Toboła-Wróbel, Pietryga, Szymankiewicz-Breborowicz, Szczapa and Bekiesińska-Figatowska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zuzanna Kozłowska, enV6YW5uYS5rb3psb3dza2FAeWFob28ucGw=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.