
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr. , 04 May 2022
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.799740
This article is part of the Research Topic Dental Caries and Periodontal Diseases as Non-communicable Chronic Diseases View all 4 articles
 Youzhen Zhang1,2,3,4,5Wanbing Feng1,2,3,4,5
Youzhen Zhang1,2,3,4,5Wanbing Feng1,2,3,4,5 Jingyu Li1,2,3,4,5
Jingyu Li1,2,3,4,5 Linlin Cui1,2,3,4,5*
Linlin Cui1,2,3,4,5* Zi-Jiang Chen1,2,3,4,5,6,7
Zi-Jiang Chen1,2,3,4,5,6,7Objective: The aim of this study was to evaluate the association between maternal periodontal disease (PD) and three main adverse neonatal outcomes, namely, preterm birth (PTB), low birth weight (LBW), and small for gestational age (SGA).
Methods: The Ovid Medline, Web of Science, Embase, and Cochrane Library were searched up to 6 December 2020 for relevant observational studies on an association between PD and risk of PTB, LBW, and SGA. Eligibility criteria included observational studies which compared the prevalence of PTB and/or LBW and/or SGA between PD women and periodontal health controls. The exclusion criteria included incomplete data, animal research, and mixing up various pregnancy outcomes, such as “preterm low birth weight” and languages other than Chinese and English. Data were extracted and analyzed independently by two authors. The meta-analysis was performed using Stata Statistical Software, Release 12 (StataCorp LP, College Station, TX, USA). Odds ratio (OR), confidence intervals (CIs), and heterogeneity (I2) were computed.
Results: Fourteen case-control studies and 10 prospective cohort studies, involving 15,278 participants, were identified. Based on fixed effect meta-analysis, PTB showed a significant association with PD (OR = 1.57, 95% CI: 1.39–1.77, P < 0.00001) and LBW also showed a significant association with PD (OR = 2.43, 95% CI: 1.75–3.37, P < 0.00001) in a random effect meta-analysis. However, a random effect meta-analysis showed no relationship between PD and SGA (OR = 1.62, 95% CI: 0.86–3.07, P = 0.136).
Conclusion: Our findings indicate that pregnant women with PD have a significantly higher risk of PTB and LBW. However, large prospective, blinded cohort studies with standardized diagnostic criteria of PD and adequate control of confounding factors are still required to confirm the relationship between PD and adverse neonatal outcomes.
Preterm birth (PTB), low birth weight (LBW), and small for gestational age (SGA) are the leading adverse neonatal outcomes worldwide and have significant public health implications because they are responsible for a great part of neonatal mortality and morbidity in both developed and developing countries (1–3). According to the World Health Organization (WHO), PTB is defined as a delivery that takes place before 37 weeks (<259 days) of gestation, LBW refers to birth weight of <2,500 g, and SGA refers to birth weight below the 10th percentile of birth weight for gestational age (3, 4). Convincing evidence has found the association between adverse neonatal outcomes and infections especially genitourinary infections (5, 6). However, the hypothesis that infections distant from the feto-placental unit may be associated with adverse neonatal outcomes has led to an increased awareness of the potential role of chronic bacterial infections elsewhere in the body (7).
Periodontal disease (PD) occurs in ~40% of pregnant women (8). It includes several inflammatory conditions, usually initiated by oral bacteria, starting with a reversible build-up of plaque and inflammation of gingival tissue (gingivitis), progressing to irreversible destruction of the supportive periodontal tissues of the teeth and tooth loss (periodontitis) (9). Generally, PD is clinically characterized by periodontal pocket depth (PPD), clinical attachment level (CAL), alveolar bone loss, and gingival inflammation (measured as bleeding on probing) (10). In 1996, Offenbacher et al. conducted a case-control study (11), suggesting that maternal PD could lead to a 7-fold increase in the risk of preterm LBW (PLBW). Following this groundbreaking study, numerous studies have shown an association between periodontal inflammation and adverse neonatal outcomes, including PTB, LBW, and SGA (12, 13). However, this association has not been consistent in other studies (14–17). These inconsistencies could be explained by several factors as follows: (i) lack of a unified diagnostic standard for PD (18); (ii) the variety of definitions used for adverse pregnancy outcomes (APOs), such as PLBW, preterm or LBW, and preterm and/or LBW; (iii) confounding effect of the risk factors. There have been a few systematic reviews and meta-analyses on the relationship between PD and adverse neonatal outcomes so far (19, 20). However, the heterogeneity of the previous studies still needs further exploration of confounding factors and more detailed subgroup analysis, and due to the publication of new data, it is necessary to perform a meta-analysis which can improve the evidence on the association between PD and adverse neonatal outcomes.
Given the alarming global disease burden of PD and adverse neonatal outcomes, there is an urgent need to clarify the substantial role of PD in the etiology of adverse neonatal outcomes (21), which will provide evidence for the periodontal prevention and intervention among children-bearing women, thus reducing the incidence of adverse neonatal outcomes caused by PD. Therefore, the objectives of this systematic review and meta-analysis were to evaluate the association between PD and adverse neonatal outcomes and provide suggestions for preventive medicine and public health.
This systematic review and meta-analysis were executed and reported according to the Preferred Reporting Item for Systematic Reviews and Meta-analysis statement (PRISMA) (22). An a priori protocol was written and followed. The Population/Income/Comparison/Outcome (PICO) question was set up as follows: Whether there was a higher risk of preterm birth and/or LBW and/or SGA in the population of pregnant women with periodontal disease compared with the population of periodontal health pregnant women.
The comprehensive database searches were performed by W. F. from inception to December 2020 in the following electronic sources: Ovid Medline 1946, Web of Science 1900, Embase 1947, and Cochrane Library. The following terms were used in the automatic search: “periodontal disease AND preterm delivery,” “periodontitis AND preterm delivery,” “periodontal disease AND low birth weight,” “periodontitis AND low birth weight,” “periodontal disease AND small for gestational age,” and “periodontitis AND small for gestational age.” The detailed search strategy can be found in Supplementary Table 1. A manual search of reference lists of relevant articles was also conducted. All the searched literature was exported to the reference manager software (ENDNOTE®X9, Bld 7212, Thomson Reuters), where the duplicated articles were removed. Manual checks and assessments were also performed to determine whether abstracts were unique or copies.
Two independent reviewers Y. Z. and L. C. performed the selection of articles. The first screening was carried out by reading the title and the abstract, eliminating those studies that did not meet the predetermined eligibility criteria. Subsequently, intensive reading of the full text of the remaining articles was made, finally selecting those eligible articles. Inclusion criteria were as follows: (1) observational studies, including case-control studies and prospective cohort studies; (2) compared the prevalence of PTB and/or LBW and/or SGA between PD women and periodontal health controls; (3) dichotomous data were reported or sufficient data were available to calculate the odds ratio (OR) and its 95% confidence interval (CI); and (4) when overlapped studies appeared, choose the latest and most complete one. The exclusion criteria included the following: (1) incomplete data: unclear or inappropriate definition of cases, unadjusted confounders, and unavailable data; (2) animal research; (3) PTB or LBW or SGA were not used as independent observational outcomes separately, such as PLBW, preterm or LBW, and preterm and/or LBW; and (4) languages other than Chinese and English.
The full text of eligible studies was independently reviewed by Y. Z. and L. C. Meta-analysis was performed to determine whether maternal PD had an adverse effect on PTB, LBW, and SGA separately. Data extraction was also independently performed by the two reviewers. Extracted information of all eligible studies included title, author names, year of publication, country, study design, sample size, age (average and/or range), timing of measurements, definitions of cases, primary outcomes (prevalence of PTB/LBW/SGA expressed by the number of cases, calculated OR and its 95% CI), and adjusted confounders.
The methodological quality of eligible studies was evaluated using the Newcastle–Ottawa Quality Assessment Scale (NOS) (23), a standardized tool recommended by the Cochrane Working Group to assess the risk of bias in observational studies. Criteria for qualitative assessment comprised three main items, namely, (1) selection of sample, (2) comparability, and (3) exposure. Each item had questions with options and could receive one or two points if the criterion was achieved. Studies were graded into low quality (0–6 points) and high quality (7–9 points) by two independent reviewers (Y. Z. and L. C.). The reviewers resolved discrepancies by discussion and additional comments from a non-author investigator.
All analyses were performed using Stata (version 12, StataCorp, College Station, TX), as the P-value < 0.05 was considered to be statistically significant. Q test and I2 test were used to assess the heterogeneity across studies (24). The hazard ratio was considered equivalent to OR, and to estimate pregnancy outcomes in women with PD vs. periodontal healthy controls, a fixed or random-effect model was used to calculate the pooled OR. Subgroup analysis was performed to find whether particular characteristics of studies (clinical or methodological) were associated to the value of the overall OR. Publication bias was assessed graphically and statistically via the Egger's linear regression test at P < 0.10 (25). Finally, with the metaninf algorithm in Stata, sensitivity analysis was performed by excluding one study at each turn.
Search results are presented in the flowchart (Figure 1). A total of 5,646 articles were yielded in the electronic search, and 13 articles were searched from reference lists of relevant articles, reviews, and dissertations. After title and abstract screening, 116 articles underwent full-text assessment. Subsequently, 44 studies were excluded as a result of incomplete data, 28 were excluded for mixed outcomes, 2 were excluded for animal research, 4 studies were excluded for duplicated publication, and 14 studies were excluded for other languages. Finally, 24 observational studies were included in this meta-analysis (26–49).
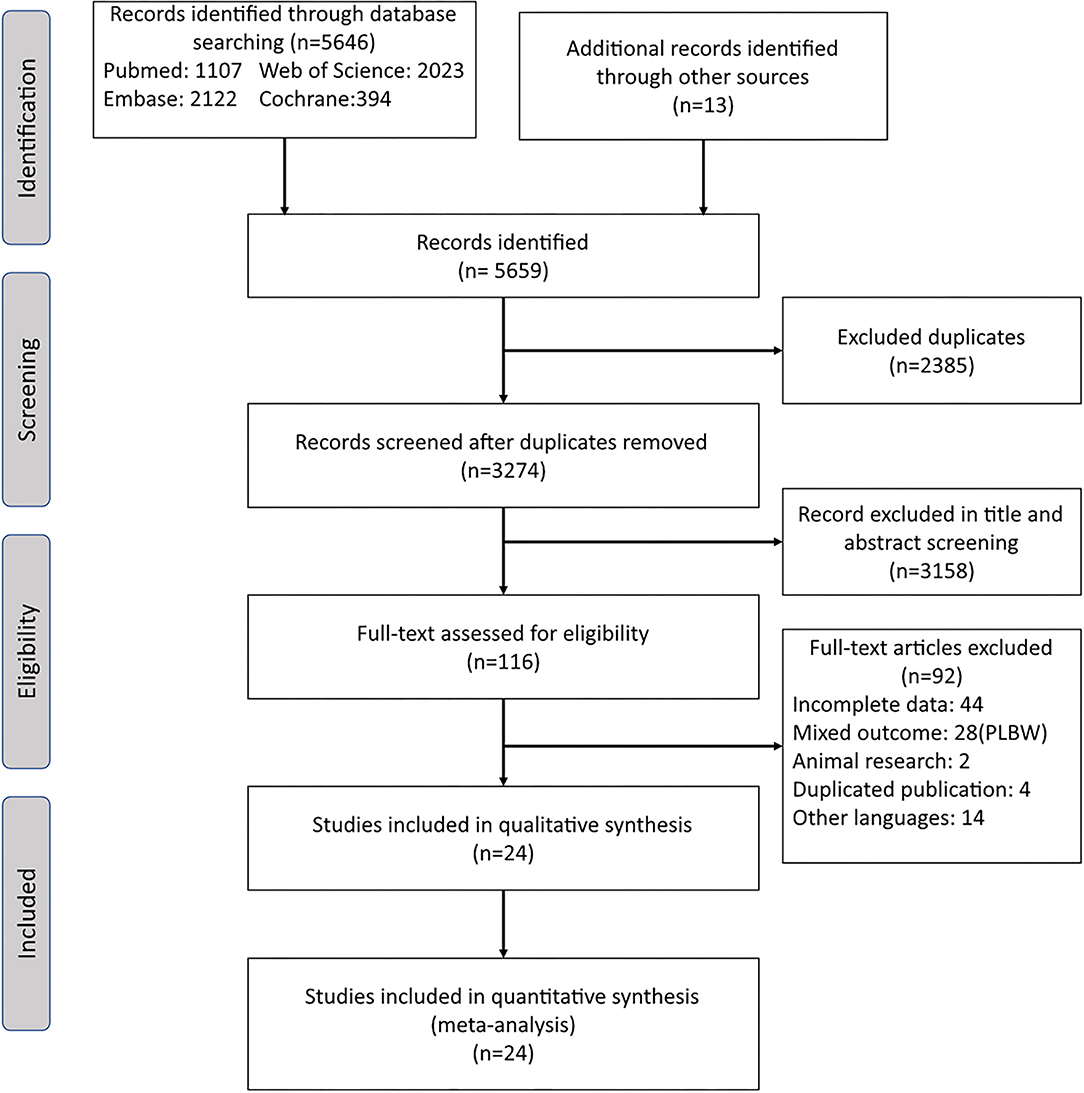
Figure 1. Flowchart of the study selection process for the present meta-analysis.
The 24 eligible studies contained 10 prospective cohort studies and 14 case-control studies, including 15,278 pregnant women. The included studies were all women of childbearing age, almost all women were older than 18. All the studies compared the prevalence of APOs between PD women and periodontally healthy controls. Among them, 15 studies investigated PTB, 14 studies investigated LBW, and 4 studies investigated SGA. Definitions of PTB, LBW, and SGA were in accordance with the WHO standard. However, definitions of PD mainly came from previous epidemiological studies and were inconsistent, including definition from Lopez et al. (≥4 teeth with ≥1 site with PPD ≥4 mm and CAL ≥3 mm at the same site), definition from Offenbacher et al. (PD ≥3 mm or CAL ≥2 mm), definition from American Centers for Disease Control and Prevention (CDC) and American Academy of Periodontology (AAP) (CDC-APP, ≥ 2 interproximal sites with CAL ≥4 mm), and other. Characteristics of all studies are displayed in Table 1.
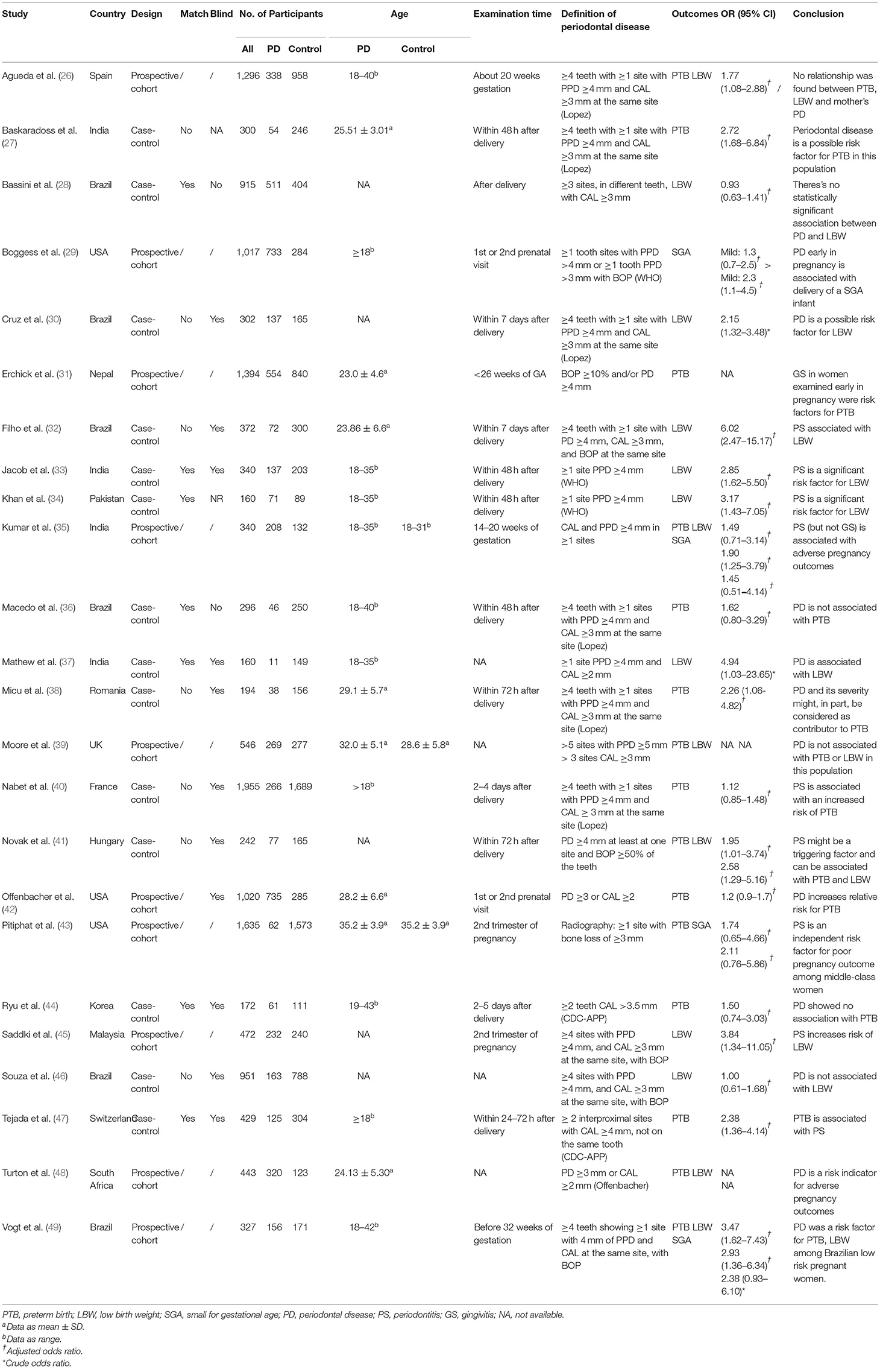
Table 1. Characters of included studies.
Results of quality assessment of the included studies using NOS for observational studies are presented in Table 2. All the included studies scored at least one star in each of the three categories: the selection and comparability of the study groups and confirmation of the outcome of interest. Overall, 10 studies were graded as high quality, and 14 studies were recognized as low quality due to an NOS score of <7. Management of possible confounders of each study is presented in Supplementary Table 2. Notably, 7 studies recruited subjects matching for confounders such as age and birth order. In 11 studies, the history of periodontal treatment was excluded before recruitment. As an important confounder of adverse neonatal outcomes, age was adjusted in 13 studies. As another important confounder, genitourinary tract infection (GTI) was adjusted in 7 studies. Management of other factors such as parity, smoking, and drug abuse in each study is recorded in Supplementary Table 2.
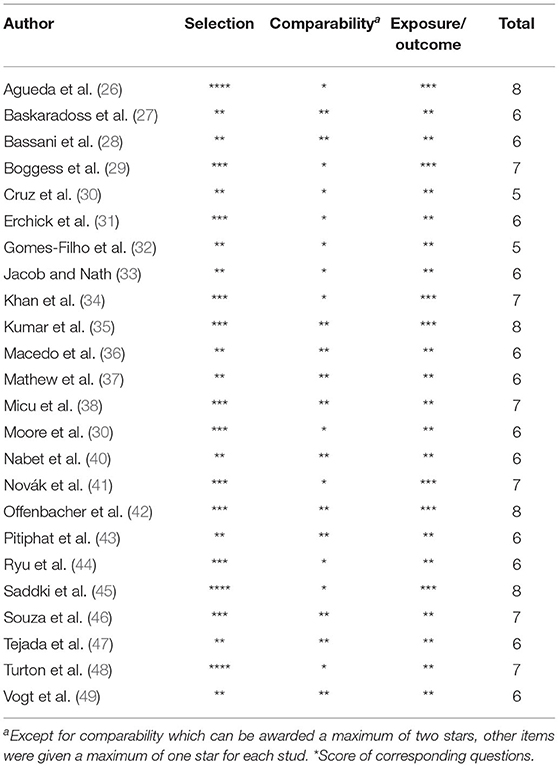
Table 2. Assessment of risk of bias based on the Newcastle–Ottawa Scale.
According to the meta-analysis presented in Figure 2, increased risk of PTB (OR: 1.57, 95% CI: 1.39–1.77, P < 0.00001, Ph = 0.364; I2 = 7.9%) was found in women with PD. Subgroups with increased risks of PTB are listed in Figure 3. In subgroup analyses by region, women with PD in Africa have a higher risk of PTB compared with other regions, and the pooled OR appears significant (OR: 2.42, 95% CI: 1.47–4.00), while Asian women with PD show a relatively lower risk (OR: 1.31, 95% CI: 1.04–1.64). Subgroup analysis showed that different criteria of PD show a significantly different risk of PTB, using criteria operated by Offenbacher, the OR of PTB increased to 2.22 (95% CI: 1.62–3.04); however, Lopez's criteria showed a relatively conservative risk (OR: 1.50, 95% CI: 1.24–1.83).
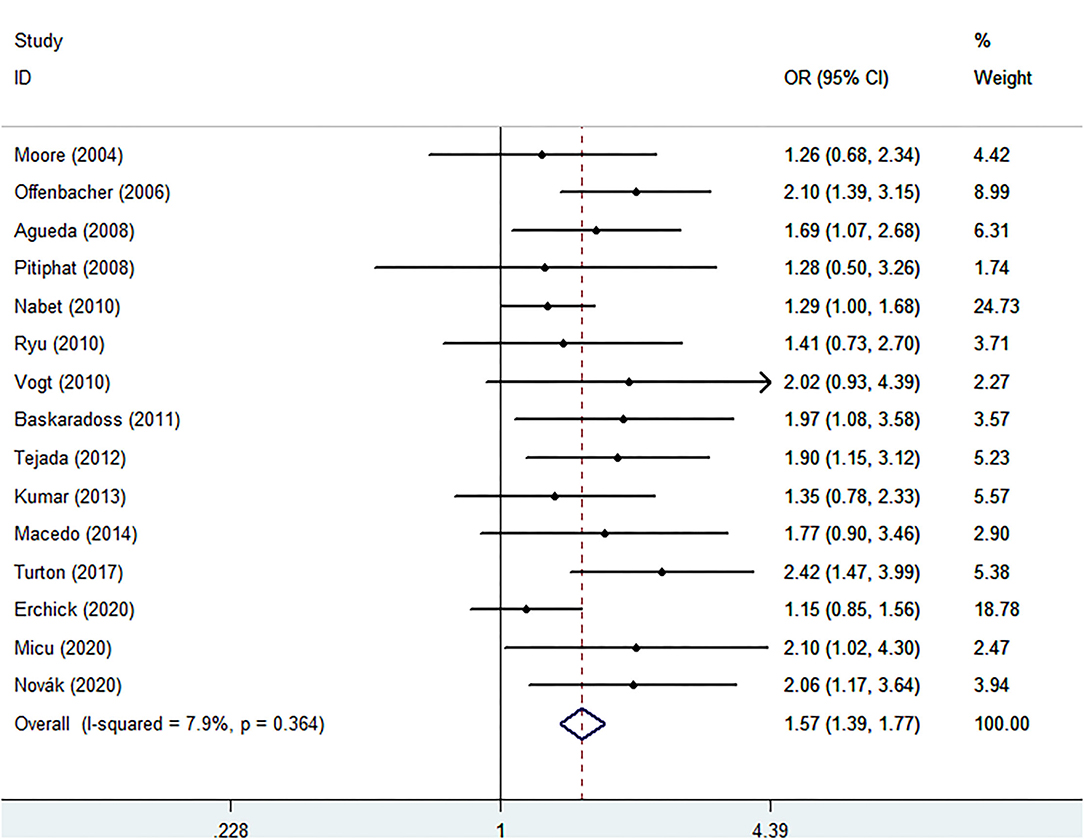
Figure 2. Forest plot of preterm birth events.
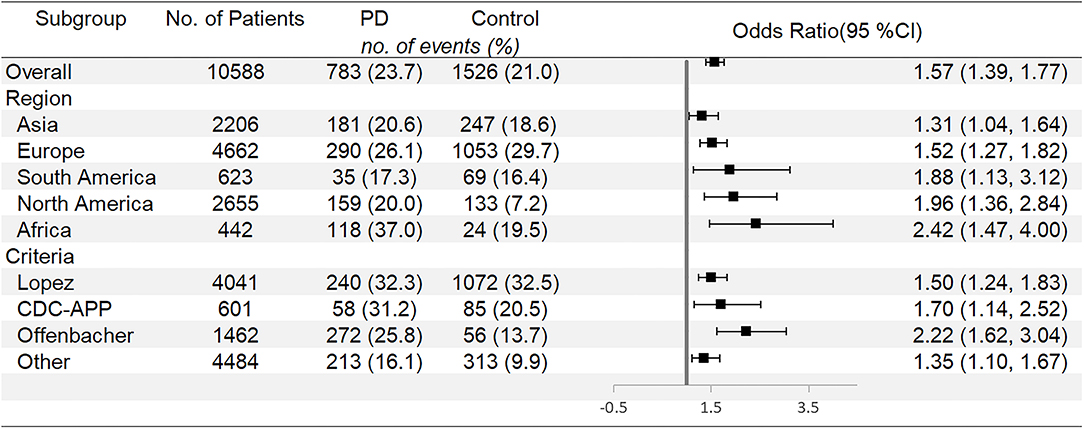
Figure 3. Subgroup analyses for preterm birth.
Meta-analysis of LBW is shown in Figure 4. Women with PD also shows increased risk of LBW compared with periodontal healthy women (OR: 2.43, 95% CI 1.75–3.37, P < 0.00001, Ph = 0.000; I2 = 82.1%). Figure 5 shows subgroup analyses for LBW. When it comes to LBW, Asia women with PD have the highest risk of LBW (OR: 3.06, 95% CI: 2.10–4.47). Different criteria of PD also show different risks of LBW. Offenbacher's criteria present the highest risk of LBW (OR: 14.74, 95% CI: 5.30–41.00). When the subgroup is divided by whether or not age is adjusted, studies with unadjusted age pooled higher OR (2.99, 95% CI: 1.80–4.95) compared with studies with adjusted age (OR: 1.92, 95% CI: 1.24–2.97). The same result is found according to GTI, with unadjusted studies pooled OR significantly higher than adjusted studies (OR: 2.87, 95% CI: 1.36–6.09 to OR: 2.14, 95% CI: 1.52–3.02).
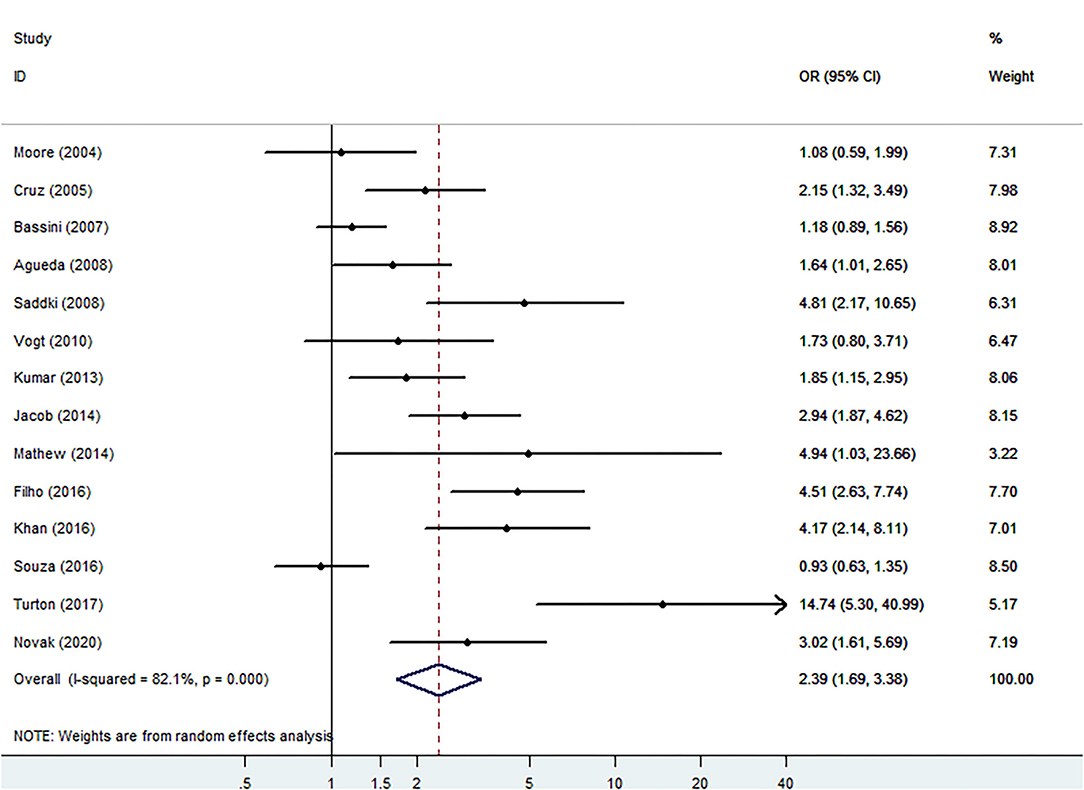
Figure 4. Forest plot of low birth weight (LBW) events.
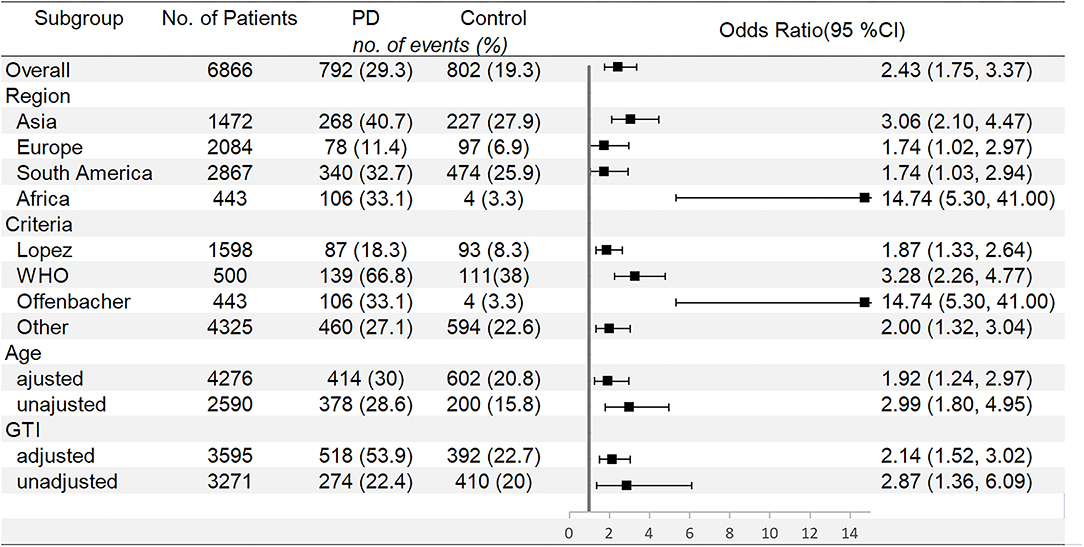
Figure 5. Subgroup analyses for LBW.
However, OR was 1.62 (95% CI: 0.86–3.07, P = 0.136, Ph = 0.07, I2 = 57.5%) for SGA presented in Figure 6 and illustrate no significant association between PD and SGA. The detailed results stratified by study characteristics are presented in Supplementary Tables 3–6.
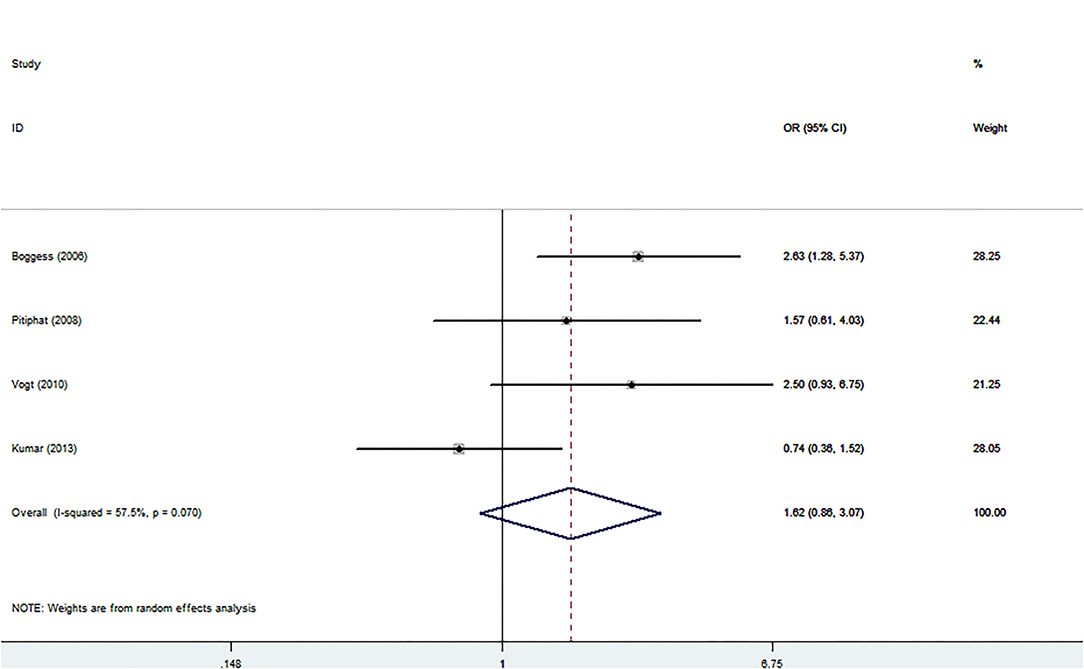
Figure 6. Forest plot of small for gestational age events.
Sensitivity analyses and publication bias of each outcome are shown in Supplementary Table 7. The sensitivity analysis reveals an influence on the pooled OR and 95% CI of SGA when Kumar's study was omitted (OR: 2.25, 95% CI: 1.37–3.69), while PTB and LBW show less influence. Publication bias was detected by Egger's linear regression test in each outcome, and only SGA shows no publication bias.
Our meta-analysis showed that pregnant women with PD had a 1.57-fold higher risk of occurring PTB and 2.43-fold higher risk of delivering LBW infants than pregnant women with a healthy periodontium. Maternal PD is an important risk factor of PTB and LBW. Moreover, women from different regions faced different risks, owing to different genetic backgrounds, dietary habits, oral hygiene habits, and preventive healthcare policies among regions. In addition, we also found that studies without adjustment of underlying confounders such as age and UTI will magnify the effect of PD on adverse neonatal outcomes.
There were numerous studies reminding vaginal infection as an important factor in adverse neonatal outcomes (50, 51). However, some studies pointed out that low-level persistent inflammation rather than infection may trigger PTB too (7, 52). Maternal PD was a chronic exposure to oral Gram-negative pathogens, which was a preventable and treatable risk factor for adverse neonatal outcomes. In women with PD, periodontal pathogens gained access to the blood circulation, and they could reside in the placenta and, worst of all, penetrate the placental barrier into the amniotic fluid and fetal circulation. Through the examination of the placental samples from women with PTB, studies had identified several microorganisms which were associated with PD, such as Aggregatibacter actinomycetemcomitans, Fusobacterium nucleatum, Porphyromonas gingivalis, and Prevotella intermedia, while these microorganisms were absent from placenta from women without periodontal infection (53, 54). The presence of these substances in the fetal-placental section could stimulate the fetal immune and inflammatory response, accompanied by the production of IgM antibodies and the increased secretion of inflammatory mediators, which in turn may cause PTB (55, 56). In this case, LBW was a result of PTB. Moreover, chronic inflammation may cause structural changes in the placenta, leading to insufficient fetal nutrient support and also resulting in LBW (57, 58).
Another explanation was that in these women, PD elevated the local and systemic level of inflammatory cytokines, promoting trophoblasts and chorioamnionic cells to secret interleukins (e.g., IL-1), prostaglandins (e.g., PGE2), tumor necrosis factor-α (TNF-α), and matrix metalloproteinases (MMPs) (59, 60). IL-1 and TNF-α acted as initial proinflammatory mediators and directly enhanced PGE2 production by inducing cyclooxygenase-2 (COX-2) expression both in the amnion and the decidua. Meanwhile, the production of MMPs in the amnion chorion, decidua, and cervix would also be enhanced, which would degrade the extracellular matrix of the fetal membranes and cervix (58, 61). The above process contributes to adverse neonatal outcomes.
This study was based on a larger and updated database, with more observed outcomes and detailed subgroup analysis compared with a previous similar study (62–64). The previous meta-analysis on PD and pregnancy outcomes showed high heterogeneity (65, 66), and the effect of various PD criteria and management of confounders may explain this high degree of heterogeneity. Our study distributes the studies into several subgroups according to different criteria, explaining the source of heterogeneity in LBW to some extent. In addition, subgroup analyses of whether adjusted GTI can eliminate the heterogeneity in SGA (Supplementary Table 7) illustrated the importance of management of confounders in future studies. The limitation should be considered when interpreting the results of this study. Egger's test revealed an apparent bias that suggested the presence of a potential publication bias, inflated estimates by a flawed methodological design in smaller studies, and/or a lack of publication of small studies with opposite results. In addition, since only PD was studied, it is unknown whether other oral diseases such as an ulcer or dental caries also had adverse effects on pregnancy outcomes. Finally, the treatment and intervention of the subjects during pregnancy had not been recorded in most literature, which makes it impossible to analyze the impact of pregnancy intervention on adverse neonatal outcomes.
Our study has potential implications for current clinical practice. Since periodontal status is a modifiable risk factor of adverse neonatal outcomes, we suggested that either obstetricians or dentists should raise their awareness of the periodontal condition in children-bearing women, and these patients should be educated to take special care of their periodontal health, provided with antenatal dental checkups and actively treated once they have signs of periodontal infection. These will reduce the incidence of adverse neonatal outcomes in pregnant women to some extent. American Academy of Periodontology (AAP) recommends bringing PD control into preconception programs and treating the disease during pregnancy, although many pregnant women are worried about the adverse effects of treatment during pregnancy, periodontal treatment is not a risk for pregnancy, and the benefits outweigh the risks of ignorance (67). Large randomized controlled trials that control the therapeutic measures need to be investigated.
In conclusion, PD was suggested as a risk factor for PTB and LBW, with a severer adverse effect in Africa and Asia separately. Therefore, improving oral health should be emphasized in children-bearing women, for the purpose of reducing the incidence of adverse neonatal outcomes. It is necessary to add oral examination into the pre-pregnancy evaluation. If PD was diagnosed, a previous treatment was suggested to avoid its adverse effect on obstetric outcomes.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
YZ performed study selection, full-text review, and drafted the manuscript. WF performed database searches. JL helped with data analyses and provided useful comments on outcome assessment. LC performed study selection, full-text review, and the revision of the manuscript. Z-JC contributed to the study concept and design. All authors contributed to this study and approved the submitted version.
This study was supported by the National Key Research and Development Program of China (2018YFC1004301), Shandong Provincial Key Research and Development Program (2018YFJH0504), Natural Science Foundation of Shandong Province of China (ZR2020MH065), and Taishan Scholars Program for Young Experts of Shandong Province, and China Health Promotion Foundation (association between ovarian response and embryo quality in women with normal ovarian reserve undergoing in vitro fertilization using a standard long protocol: a retrospective cohort study; association between the numbers of retrieved oocytes and pregnancy outcomes in women with normal ovarian reserve undergoing in vitro fertilization: a retrospective cohort study). Funders did not have any role in study design, data collection, and data analyses.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all the authors whose studies were included in this study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.799740/full#supplementary-material
PD, periodontal disease; PTB, preterm birth; LBW, low birth weight; SGA, small for gestational age; OR, odds ratio; CIs, confidence intervals; I2, heterogeneity; GTI, genitourinary tract infection; PGE2, prostaglandins; TNF-α, tumor necrosis factor-α; MMPs, matrix metalloproteinases; COX-2, cyclooxygenase-2.
1. World Health Organization. (1975). Pregnancy and Abortion in Adolescence. Report of a WHO Meeting. Geneva: World Health Organ Tech Rep Ser. p. 1–27.
2. Goldenberg RL, Rouse DJ. Prevention of premature birth. N Engl J Med. (1998) 339:313–20. doi: 10.1056/NEJM199807303390506
3. World Health O World B United Nations Population F United Nations Children's Fund. Maternal Mortality in 2005: Estimates Developed by WHO, UNICEF, UNFPA, and The World Bank (2007).
4. World Health Organization. International statistical classification of diseases and related health problems. Geneva: World Health Organization. (2015).
5. Jefferson KK. The bacterial etiology of preterm birth. Adv Appl Microbiol. (2012) 80:1–22. doi: 10.1016/b978-0-12-394381-1.00001-5
6. Mysorekar IU, Cao B. Microbiome in parturition and preterm birth. Semin Reprod Med. (2014) 32:50–5. doi: 10.1055/s-0033-1361830
7. Gibbs RS, Romero R, Hillier SL, Eschenbach DA, Sweet RL. A review of premature birth and subclinical infection. Am J Obstet Gynecol. (1992) 166:1515–28. doi: 10.1016/0002-9378(92)91628-n
8. Lieff S, Boggess KA, Murtha AP, Jared H, Madianos PN, Moss K, et al. The oral conditions and pregnancy study: periodontal status of a cohort of pregnant women. J Periodontol. (2004) 75:116–26. doi: 10.1902/jop.2004.75.1.116
9. Brown LJ Lolnditions Lolnditions and pregnancy study: periodontal status of a cohort of pregnant Periodontol 2000. (1993) 2:57–71. doi: 10.1111/j.1600-0757.1993.tb00220.x
10. Page RC, Eke PI. Case Definitions for Use in Population-Based Surveillance of Periodontitis. J Periodontol. (2007) 78(Suppl. 7S):1387–99. doi: 10.1902/jop.2007.060264
11. Offenbacher S, Katz V, Fertik G, Collins J, Boyd D, Maynor G, et al. Periodontal infection as a possible risk factor for preterm low birth weight. J Periodontol. (1996) 67(10 Suppl.):1103–13. doi: 10.1902/jop.1996.67.10s.1103
12. Guimar.dontol infection as a possible risk factor for preterm low birth weight. riodontitis. linical infection. /fped.2022.799740/full#suppleJ Clin Periodontol. (2012) 39:1024–31. doi: 10.1111/jcpe.12000
13. Reza Karimi M, Hamissi JH, Naeini SR, Karimi M. The relationship between maternal periodontal status of and preterm and low birth weight infants in Iran: a case control study. Glob J Health Sci. (2015) 8:184–8. doi: 10.5539/gjhs.v8n5p184
14. Srinivas SK, Sammel MD, Stamilio DM, Clothier B, Jeffcoat MK, Parry S, et al. Periodontal disease and adverse pregnancy outcomes: is there an association? Am J Obstet Gynecol. (2009) 200:497.e491–8. doi: 10.1016/j.ajog.2009.03.003
15. Martínez-Martínez RE, Moreno-Castillo DF, Loyola-Rodríguez JP, Sánchez-Medrano AG, Miguel-Hernández JH, Olvera-Delgado JH, et al. Association between periodontitis, periodontopathogens and preterm birth: is it real? Arch Gynecol Obstet. (2016) 294:47ecol Obsteten1007/s00404-015-3945-1
16. Fogacci MF, Cardoso EOC, Barbirato DS, de Carvalho DP, Sansone C. No association between periodontitis and preterm low birth weight: a caselementary-materiArch Gynecol Obstet. (2018) 297:71–6. doi: 10.1007/s00404-017-4556-9
17. Krüger MSDM, Casarin RP, Pinto GDS, Pappen FG, Camargo MBJ, Correa FOB, et al. Maternal periodontal disease and adverse perinatal outcomes: is there an association? A hospital-based case-control study. J Matern Fetal Neonatal Med. (2019) 32:3401–7. doi: 10.1080/14767058.2018.1464554
18. Ide M, Papapanou PN. Epidemiology of association between maternal periodontal disease and adverse pregnancy outcomes–systematic review. J Periodontol. (2013) 84(4 Suppl.):S181–94. doi: 10.1902/jop.2013.134009
19. Manrique-Corredor EJ, Orozco-Beltran D, Lopez-Pineda A, Quesada JA, Gil-Guillen VF, Carratala-Munuera C. Maternal periodontitis and preterm birth: systematic review and meta-analysis. Community Dent Oral Epidemiol. (2019) 47:243–51. doi: 10.1111/cdoe.12450
20. Savage A, Eaton KA, Moles DR, Needleman I. A systematic review of definitions of periodontitis and methods that have been used to identify this disease. J Clin Periodontol. (2009) 36:458–67. doi: 10.1111/j.1600-051X.2009.01408.x
21. Bernabe E, Marcenes W, Hernandez CR, Bailey J, Abreu LG, Alipour V, et al. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: a systematic analysis for the global burden of disease 2017 study. J Dent Res. (2020) 99:362es a doi: 10.1177/0022034520908533
22. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
23. Wells G, Shea B, O'Connell D, Peterson J, Welch V, Losos M. The Newcastle-Ottawa Scale (NOS) for assessing the quality if nonrandomized studies in meta-analyses. (2009). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed July 15, 2021).
24. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
25. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
26. Agueda A, Ramy Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. that have been used to identify this disease. J Clin Periodontol. (2008) 35:16–22. doi: 10.1111/j.1600-051X.2007.01166.x
27. Baskaradoss JK, Geevarghese A, Kutty VR. Maternal periodontal status and preterm delivery: a hospital based case-control study. J Periodontal Res. (2011) 46:542–9. doi: 10.1111/j.1600-0765.2011.01371.x
28. Bassani DG, Olinto MTA, Kreiger N. Periodontal disease and perinatal outcomes: a case-control study. J Clin Periodontol. (2007) 34:31–9. doi: 10.1111/j.1600-051X.2006.01012.x
29. Boggess KA, Beck JD, Murtha AP, Moss K, Offenbacher S. Maternal periodontal disease in early pregnancy and risk for a small-for-gestational-age infant. Am J Obstet Gynecol. (2006) 194:1316–22. doi: 10.1016/j.ajog.2005.11.059
30. Cruz SS, Costa MDN, Gomes IS, Vianna MIP, Santos CT. Maternal periodontal disease as a factor associated with low birth weight. Rev Saude Publica. (2005) 39:782–7. doi: 10.1590/s0034-89102005000500013
31. Erchick DJ, Khatry SK, Agrawal NK, Katz J, LeClerq SC, Rai B, et al. Risk of preterm birth associated with maternal gingival inflammation and oral hygiene behaviours in rural Nepal: a community-based, prospective cohort study. BMJ Open. (2020) 10:e036515. doi: 10.1136/bmjopen-2019-036515
32. Gomes-Filho IS, Pereira EC, Cruz SS, Adan LFF, Vianna MIP, Passos-Soares JS, et al. Relationship among mothers' glycemic level, periodontitis, and birth weight. J Periodontol. (2016) 87:238–47. doi: 10.1902/jop.2015.150423
33. Jacob PS, Nath S. Periodontitis among poor rural Indian mothers increases the risk of low birth weight babies: a hospital-based case control study. J Periodontal Implant Sci. (2014) 44:85–93. doi: 10.5051/jpis.2014.44.2.85
34. Khan NS, Ashraf RN, Noor S, Mahmood ur R, Mashhadi SF, Rashid Z, et al. Association of maternal periodontitis with low birth weight in newborns in a tertiary care hospital J Ayub Med Coll Abbottabad. (2016) 28:120–5.
35. Kumar A, Basra M, Begum N, Rani V, Prasad S, Lamba AK, et al. Association of maternal periodontal health with adverse pregnancy outcome. J Obstet Gynaecol Res. (2013) 39:40–5. doi: 10.1111/j.1447-0756.2012.01957.x
36. Macedo JF, Ribeiro RA, Machado FC, Assis NMSP, Alves RT, Oliveira AS, et al. Periodontal disease and oral health-related behavior as factors associated with preterm birth: a case-control study in south-eastern Brazil. J Periodontal Res. (2014) 49:458–64. doi: 10.1111/jre.12124
37. Mathew RJ, Bose A, Prasad JH, Muliyil JP, Singh D. Maternal periodontal disease as a significant risk factor for low birth weight in pregnant women attending a secondary care hospital in South India: a case-control study. Indian J Dent Res. (2014) 25:742–7. doi: 10.4103/0970-9290.152184
38. Micu IC, Roman A, Ticala F, Soanca A, Ciurea A, Objelean A, et al. Relationship between preterm birth and post-partum periodontal maternal status: a hospital-based Romanian study. Arch Gynecol Obstet. (2020) 301:1189–98. doi: 10.1007/s00404-020-05521-6
39. Moore S, Ide M, Coward PY, Randhawa M, Borkowska E, Baylis R, et al. A prospective study to investigate the relationship between periodontal disease and adverse pregnancy outcome. Br Dent J. (2004) 197:251–8. doi: 10.1038/sj.bdj.4811620
40. Nabet C, Lelong N, Colombier M-L, Sixou M, Musset A-M, Goffinet F, et al. Maternal periodontitis and the causes of preterm birth: the case-control Epipap study. J Clin Periodontol. (2010) 37:37–45. doi: 10.1111/j.1600-051X.2009.01503.x
41. Nov03090eriodontolntitis and the causes of preterm birth: the casepoor periodontal status be a warning sign for worse pregnancy outcome? Oral Health Prev Dent. (2020) 18:165–70. doi: 10.3290/j.ohpd.a43356
42. Offenbacher S, Boggess KA, Murtha AP, Jared HL, Lieff S, McKaig RG, et al. Progressive periodontal disease and risk of very preterm delivery. Obstet Gynecol. (2006) 107:29–36. doi: 10.1097/01.Aog.0000190212.87012.96
43. Pitiphat W, Joshipura KJ, Gillman MW, Williams PL, Douglass CW, Rich-Edwards JW. Maternal periodontitis and adverse pregnancy outcomes. Community Dent Oral Epidemiol. (2008) 36:3–11. doi: 10.1111/j.1600-0528.2006.00363.x
44. Ryu J-I, Oh K, Yang H, Choi B-K, Ha J-E, Jin B-H, et al. Health behaviors, periodontal conditions, and periodontal pathogens in spontaneous preterm birth: a case-control study in Korea. J Periodontol. (2010) 81:855–63. doi: 10.1902/jop.2010.090667
45. Saddki N, Bachok NA, Hussain NHN, Zainudin SLA, Sosroseno W. The association between maternal periodontitis and low birth weight infants among Malay women. Community Dentistry Oral Epidemiol. (2008) 36:296–304. doi: 10.1111/j.1600-0528.2007.00383.x
46. Souza LM, da Cruz SS, Gomes-Filho IS, Barreto ML, Passos-Soares JS, Trindade SC, et al. Effect of maternal periodontitis and low birth weight-a case control study. Acta Odontol Scand. (2016) 74:73–80. doi: 10.3109/00016357.2015.1049374
47. Tejada BM, Gayet-Ageron A, Combescure C, Irion O, Baehni P. Association between early preterm birth and periodontitis according to USA and European consensus definitions. J Maternal Fetal Neonat Med. (2012) 25:2160–66. doi: 10.3109/14767058.2012.663827
48. Turton M, Africa CWJ. Further evidence for periodontal disease as a risk indicator for adverse pregnancy outcomes. Int Dent J. (2017) 67:148–56. doi: 10.1111/idj.12274
49. Vogt M, Sallum AW, Cecatti JG, Morais SS. Periodontal disease and some adverse perinatal outcomes in a cohort of low risk pregnant women. Reprod Health. (2010) 7:29. doi: 10.1186/1742-4755-7-29
50. Chu DM, Seferovic M, Pace RM, Aagaard KM. The microbiome in preterm birth. Best Pract Res Clin Obstet Gynaecol. (2018) 52:103–13. doi: 10.1016/j.bpobgyn.2018.03.006
51. Bayar E, Bennett PR, Chan D, Sykes L, MacIntyre DA. The pregnancy microbiome and preterm birth. Semin Immunopathol. (2020) 42:487–99. doi: 10.1007/s00281-020-00817-w
52. Al Habashneh R, Khader YS, Jabali OA, Alchalabi H. Prediction of preterm and low birth weight delivery by maternal periodontal parameters: receiver operating characteristic (ROC) curve analysis. Matern Child Health J. (2013) 17:299–306. doi: 10.1007/s10995-012-0974-2
53. Offenbacher S, Jared HL, O'Reilly PG, Wells SR, Salvi GE, Lawrence HP, et al. Potential pathogenic mechanisms of periodontitis associated pregnancy complications. Ann Periodontol. (1998) 3:233–50. doi: 10.1902/annals.1998.3.1.233
54. Barak S, Oettinger-Barak O, Machtei EE, Sprecher H, Ohel G. Evidence of periopathogenic microorganisms in placentas of women with preeclampsia. J Periodontol. (2007) 78:670–6. doi: 10.1902/jop.2007.060362
55. Gomez-Lopez N, StLouis D, Lehr MA, Sanchez-Rodriguez EN, Arenas-Hernandez M. Immune cells in term and preterm labor. Cell Mol Immunol. (2014) 11:571–81. doi: 10.1038/cmi.2014.46
56. Menon R, Taylor BD. Exploring inflammatory mediators in fetal and maternal compartments during human parturition. Obstet Gynecol. (2019) 134:765–73. doi: 10.1097/aog.0000000000003470
57. Madianos PN, Bobetsis YA, Offenbacher S. Adverse pregnancy outcomes (APOs) and periodontal disease: pathogenic mechanisms. J Periodontol. (2013) 84(4 Suppl.):S170–80. doi: 10.1902/jop.2013.1340015
58. Reyes L, Phillips P, Wolfe B, Golos TG, Walkenhorst M, Progulske-Fox A, et al. Porphyromonas gingivalis and adverse pregnancy outcome. J Oral Microbiol. (2017) 9:1374153. doi: 10.1080/20002297.2017.1374153
59. Davenport ES, Williams CE, Sterne JA, Sivapathasundram V, Fearne JM, Curtis MA. The East London study of maternal chronic periodontal disease and preterm low birth weight infants: study design and prevalence data. Ann Periodontol. (1998) 3:213–21. doi: 10.1902/annals.1998.3.1.213
60. Offenbacher S. Maternal periodontal infections, prematurity, and growth restriction. Clin Obstet Gynecol. (2004) 47:808–21. doi: 10.1097/01.grf.0000141894.85221.f7
61. Kayar NA, Alptekin N, Erdal ME. Interleukin-1 receptor antagonist gene polymorphism, adverse pregnancy outcome and periodontitis in Turkish women. Arch Oral Biol. (2015) 60:1777–83. doi: 10.1016/j.archoralbio.2015.09.013
62. Khader YS, Ta'ani Q. Periodontal diseases and the risk of preterm birth and low birth weight: a meta-analysis. J Periodontol. (2005) 76:161–5. doi: 10.1902/jop.2005.76.2.161
63. Vergnes JN, Sixou M. Preterm low birth weight and maternal periodontal status: a meta-analysis. Am J Obstet Gynecol. (2007) 196:135.e131–7. doi: 10.1016/j.ajog.2006.09.028
64. Corbella S, Taschieri S, Francetti L, De Siena F, Del Fabbro M. Periodontal disease as a risk factor for adverse pregnancy outcomes: a systematic review and meta-analysis of case-control studies. Odontology. (2012) 100:232–40. doi: 10.1007/s10266-011-0036-z
65. Konopka T, Paradowska-Stolarz A. Periodontitis and risk of preterm birth and low birthweight - a meta-analysis. Ginekol Pol. (2012) 83:446–53.
66. Huang X, Wang J, Liu J, Hua L, Zhang D, Hu T, et al. Maternal periodontal disease and risk of preeclampsia: a meta-analysis. J Huazhong Univ Sci Technolog Med Sci. (2014) 34:729–35. doi: 10.1007/s11596-014-1343-8
Keywords: periodontal disease (PD), neonatal outcomes, preterm birth (PTB), low birth weight (LBW), meta-analysis
Citation: Zhang Y, Feng W, Li J, Cui L and Chen Z-J (2022) Periodontal Disease and Adverse Neonatal Outcomes: A Systematic Review and Meta-Analysis. Front. Pediatr. 10:799740. doi: 10.3389/fped.2022.799740
Received: 22 October 2021; Accepted: 31 March 2022;
Published: 04 May 2022.
Edited by:
Huawei Mao, Capital Medical University, ChinaReviewed by:
Deepti Shrivastava, Al Jouf University, Saudi ArabiaCopyright © 2022 Zhang, Feng, Li, Cui and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Linlin Cui, ZmRjbGVhcjNAMTI2LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.