 Maarja Soomann1,2,3
Maarja Soomann1,2,3 Pedro D. Wendel-Garcia3,4
Pedro D. Wendel-Garcia3,4 Mark Kaufmann5
Mark Kaufmann5 Serge Grazioli6
Serge Grazioli6 Marie-Helene Perez7
Marie-Helene Perez7 Matthias P. Hilty3,4
Matthias P. Hilty3,4 Maya C. André8,9
Maya C. André8,9 Barbara Brotschi1,2,3*
Barbara Brotschi1,2,3*- 1Department of Pediatric and Neonatal Intensive Care, University Children's Hospital Zurich, Zurich, Switzerland
- 2Children's Research Center, University Children's Hospital Zurich, Zurich, Switzerland
- 3University of Zurich, Zurich, Switzerland
- 4Institute of Intensive Care Medicine, University Hospital Zurich, Zurich, Switzerland
- 5Department for Anesthesia, Surgical Intensive Care, Prehospital Emergency Medicine and Pain Therapy, University Hospital Basel, Basel, Switzerland
- 6Division of Neonatal and Pediatric Intensive Care, Department of Pediatrics, University Hospital of Geneva, Geneva, Switzerland
- 7Pediatric Intensive Care Unit, Lausanne University Hospital, Lausanne, Switzerland
- 8Division of Respiratory and Critical Care Medicine, University of Basel Children's Hospital, Basel, Switzerland
- 9Department of Pediatric Hematology and Oncology, University Children's Hospital, Eberhard Karls University, Tuebingen, Germany
The impact of the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic on pediatric intensive care units (PICUs) is difficult to quantify. We conducted an observational study in all eight Swiss PICUs between 02/24/2020 and 06/15/2020 to characterize the logistical and medical aspects of the pandemic and their impact on the management of the Swiss PICUs. The nine patients admitted to Swiss PICUs during the study period suffering from pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) and constituting 14% (9/63) of all SARS-CoV-2 positive hospitalized patients in Swiss children's hospitals caused a higher workload [total Nine Equivalents of nursing Manpower use Score (NEMS) points, p = 0.0008] and were classified to higher workload categories (p < 0.0001) than regular PICU patients (n = 4,881) admitted in 2019. The comparison of the characteristics of the eight Swiss PICUs shows that they were confronted by different organizational issues arising from temporary regulations put in place by the federal council. These general regulations had different consequences for the eight individual PICUs due to the differences between the PICUs. In addition, the temporal relationship of these different regulations influenced the available PICU resources, dependent on the characteristics of the individual PICUs. As pandemic continues, reflecting and learning from experience is essential to reduce workload, optimize bed occupancy and manage resources in each individual PICU. In a small country as Switzerland, with a relatively decentralized health care local differences between PICUs are considerable and should be taken into account when making policy decisions.
Introduction
Children have been reported to be affected by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) in 2–8% of all reported cases (1–4). In addition, they seem to experience milder disease courses, as only 0.2–2% of all affected children have been severely or critically ill (1, 4–6). In the course of the pandemic clusters of severely affected pediatric patients with symptoms similar, although distinctively different from severe Kawasaki disease were reported in Europe and North America (7–13). This new syndrome was named pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) or multisystem inflammatory syndrome in children (MIS-C) (3, 9). It's clinical and laboratory presentations have been described in depth in a series of case reports and case series by now (7–16). Most of the patients diagnosed with PIMS-TS have been treated according to protocols with corticosteroids or immunoglobulins or both, but a high need for organ supportive measures has been reported (3, 8, 17–20). In addition to having to care for patients with this new syndrome, Swiss PICUs were confronted with organizational issues arising from temporary regulations put in place by the federal council due to the pandemic.
There are eight PICUs in Switzerland, distributed all over the small country of 41,285 square kilometers with 8.6 million inhabitants (21, 22). Two PICUs are located in the French speaking part, six PICUs in the German speaking part and none in the Italian speaking part of Switzerland. The aim of our study is to describe the different logistical and medical challenges facing the Swiss PICUs during the first wave of the SARS-CoV-2 pandemic.
Materials and Methods
PICU Burden
All eight Swiss PICUs provided data on organizational characteristics and the situation in their units during the study period. These included general characteristics (total number of beds, total number of admissions, and affiliation to adult hospitals) and characteristics related to the SARS-CoV-2 pandemic (percentage of scheduled admissions, cancellation of interventions, staff recruited to adult wards, and percentage of PIMS-TS patients).
For comparing workloads the Nine Equivalents of nursing Manpower use Score (NEMS) and Riker Sedation-Agitation Scale (SAS) as well as a Swiss derivative of the two, the Swiss Society of Intensive Care Medicine (SSICM) shift categories were used (23–25). These scores are used as standard practice in all PICUs in Switzerland and filled out per patient per shift immediately after every nursing working shift. The routine length of a nursing staff shift is 9 h and planned or unplanned double shifts were not practiced. If unplanned absences occurred, units reduced their bed availability for this shift. NEMS score is well-validated and easier to use than the Therapeutic Intervention Scoring System, therefore the Swiss society of intensive care medicine has established using this scoring system nationwide (26–30). NEMS includes data on interventions as well as of therapies and reflects the workload of nurses and physicians. The score includes the following nine items: basic monitoring, intravenous medication, mechanical ventilator support, supplementary ventilator care, single vasoactive medication, multiple vasoactive medication, dialysis techniques, specific interventions in the intensive care unit (ICU), and specific interventions outside the ICU (23). The higher the NEMS Score, the more nursing manpower was needed during a certain shift or during the whole ICU stay. SAS is used to evaluate a patient's level of sedation and agitation. During each shift each patient is given a score from one to seven ranging from an unarousable patient to a dangerously agitated patient (24). SSICM shift categories integrate NEMS and SAS, category 1A of the SSICM defines the most, and category 3 the least, work-load intensive shift for ICU nurses (25). Details SSICM shift categories are shown in Table 1.
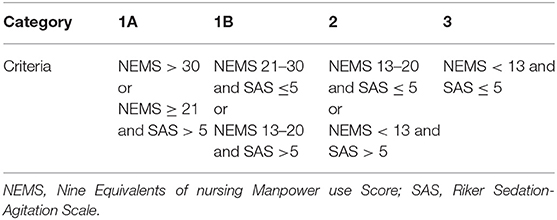
Table 1. Classification criteria for the Swiss Society of Intensive Care Medicine (SSICM) shift categories.
Patient and Population Data
In order to compare the critically ill SARS-CoV-2 pediatric patients to the regular PICU population, data on all patients hospitalized in the eight Swiss PICUs in 2019 was used. The whole year instead of the corresponding time period in 2019 was used to avoid a seasonal bias in the group representing regular PICU patients. This data was drawn from the Minimal Dataset of the Swiss Society of Intensive Care Medicine (MDSi) (31). The Pediatric Index of Mortality 2 (PIM2) was used as an indicator of predicted case severity of the patients with PIMS-TS and the general PICU population (32). Data of the patients with PIMS-TS was retrospectively gathered in all eight Swiss PICUs on patients hospitalized from February 24, 2020, the date on which the first SARS-CoV-2 PCR positive patient was reported in Switzerland, up until the June 15, 2020. Included were all patients with age below 20 years and a positive SARS-CoV-2 polymerase chain reaction (PCR) result or the diagnosis of PIMS-TS according to either the Royal College of Child Health and Pediatrics (33), the World Health Organization (34) or the Centers for Disease Control and Prevention case definitions (35), during the PICU stay. Patient data was collected from chart notes and anonymized in the respective centers with a custom made questionnaire, one center's data was obtained from the Risk Stratification in COVID-19 patients in the ICU (RISC-19-ICU) registry (36). Information was gathered also on the use of anti-inflammatory medications including corticosteroids, intravenous immunoglobulin, anakinra, and tocilizumab, which all have been licensed for use in other conditions but were used off label for PIMS-TS.
General epidemiological data on the SARS-CoV-2 pandemic in Switzerland was drawn from the official website of the Swiss Federal Office of Public Health (FOPH) (37). As no reliable serological data was available at the whole population level, the total number of SARS-CoV-2 PCR positive tests in Switzerland was used in calculations to represent number the SARS-CoV-2 cases despite our PIMS-TS group mostly being PCR negative and seropositive. Data on the demographics of Switzerland was obtained from the website of the Swiss Federal Statistical Office (21).
Definitions of Organ Dysfunction
Acute respiratory distress syndrome (ARDS) was defined according to the Pediatric Acute Lung Injury Consensus Conference definition for pediatric acute respiratory distress syndrome (38). Shock was defined as an arterial systolic blood pressure below the age adapted 5th percentile or a systolic blood pressure below two standard deviations of the age adapted mean, and/or the need for vasoactive support to maintain blood pressure in the range (39, 40). Myocardial injury was defined as ejection fraction reduced below 55% measured using the biplane Simpson method according to the current pediatric echocardiographic recommendations (41, 42). Renal dysfunction was defined according to the pRIFLE classification (43). Hepatic dysfunction was defined as the elevation of liver enzymes above the age adapted reference and elevation of prothrombin time (44). An abnormal prothrombin time or activated partial thromboplastin time (according to age adapted reference values of the local laboratories) was classified as a coagulation disorder (45).
Ethical Approval
The study proposal (KEK: 2020-00720), as well as the RISC-19-ICU (KEK: 2020-00322, ClinicalTrials.gov Identifier: NCT04357275) registry have been evaluated by the Cantonal Ethics Committee of Zurich, a member of the Swiss Association of Research Ethics Committees—Swissethics and in line with the Swiss Federal Human Research Act deemed exempt from the need for additional ethics approval. The study complies with the Declaration of Helsinki, the Guidelines on Good Clinical Practice (GCP-Directive) issued by the European Medicines Agency as well as the Swiss law and Swiss regulatory authority requirements and has been designed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies.
Statistical Analysis
Statistical analysis was conducted employing the R environment for statistical computing version 4.0.2. Comparisons of population characteristics were performed using Wilcoxon rank-sum test for continuous not normally distributed and the chi-squared test for categorical variables. Continuous not normally distributed data is presented as median with interquartile ranges (IQR) and nominal data as counts and percentages.
Results
PICU Burden
The Swiss PICUs varied in general characteristics as well as in characteristics related to the pandemic. The different medical and logistical aspects affecting the PICUs are listed in Table 2. In addition to some PICUs having to care for patients with this new syndrome, all PICUs were confronted with organizational issues arising from temporary regulations put in place by the federal council due to the pandemic. These general regulations had different consequences for the eight PICUs due to their different characteristics. As shown in Table 2, there were units (PICU 8) not affiliated to adult hospitals and without staff recruitment to adult wards, where nevertheless scheduled interventions were canceled due to regulations set by the federal council. As a consequence, this PICU was not fully occupied and had a relatively low workload. Other PICUs (PICU 5), however, were affiliated to an adult ward and staff recruitment to the adult wards was required. Therefore, cancellation of scheduled interventions was essential to have enough manpower and staff for the emergency admissions to these PICUs (PICU 5). Other PICUs (PICU 1) were also influenced by local circumstances with staff being recruited to adult wards due to staff shortage in the area despite the PICU not being affiliated with an adult hospital.
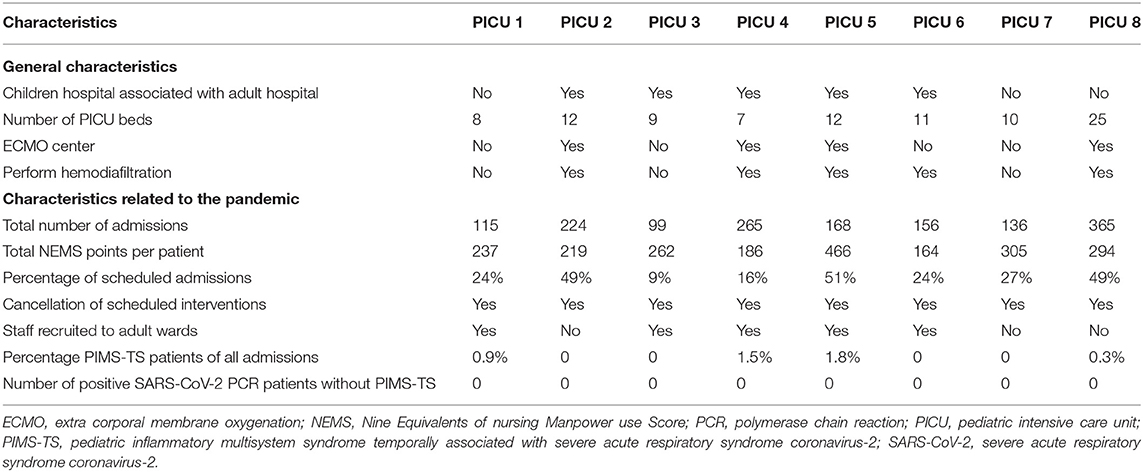
Table 2. General characteristics and characteristics related to the pandemic of the eight Swiss pediatric intensive care units between 02-24-2020 and 06-15-2020.
Four out of eight PICUs had patients admitted with PIMS-TS between February 24, 2020 and June 15, 2020. Patients with PIMS-TS constituted 0.6% of all Swiss PICU admissions (9/1,528) during this time period and 0.3–1.8% of the PICU admissions of PICUs treating patients with PIMS-TS. A comparison of patients with PIMS-TS and general pediatric intensive care unit patients hospitalized in 2019 is shown in Table 3, based on quantitative and qualitative measures of case complexity. Patients with PIMS-TS had higher total NEMS scores (p = 0.0008) and were classified to higher SSICM workload categories more frequently than general PICU patients hospitalized in 2019 (p < 0.0001).

Table 3. Comparison of PIMS-TS patients and all PICU patients hospitalized in 2019 based on quantitative and qualitative measures of case complexity.
Epidemiology of SARS CoV-2 Positive Patients
The total of 1,113 children and young adults under the age of 20 were tested positive for SARS-CoV-2 infection between February 24, 2020 and June 15, 2020 in Switzerland, of which 6% (63/1,113) had to be hospitalized [Swiss FOPH (37)]. Ten pediatric patients with a concurrent positive SARS-CoV-2 PCR result or with PIMS-TS were hospitalized in PICUs. The only patient not diagnosed with PIMS-TS was admitted to the PICU due to an acute necrotizing encephalopathy. As the role of SARS-CoV-2 in the pathogenesis and disease progression remained unclear in this case, this patient's data was excluded from the present analysis. The nine remaining patients with PIMS-TS hospitalized in Swiss PICUs constituted 14% (9/63) of all SARS-CoV-2 positive hospitalized and 1% (9/1,113) of all SARS-CoV-2 positive children and young adults under the age of 20 in Switzerland during that period [Swiss FOPH (37)]. The incidence of severe PIMS-TS requiring hospitalization at a PICU was, therefore, 0.5 per 100,000 people under the age of 20 during the study period. No information is available on seropositivity in the general population during the study period. The general characteristics of all the PIMS-TS patients, details on organ dysfunction and applied therapies are presented in Table 4.
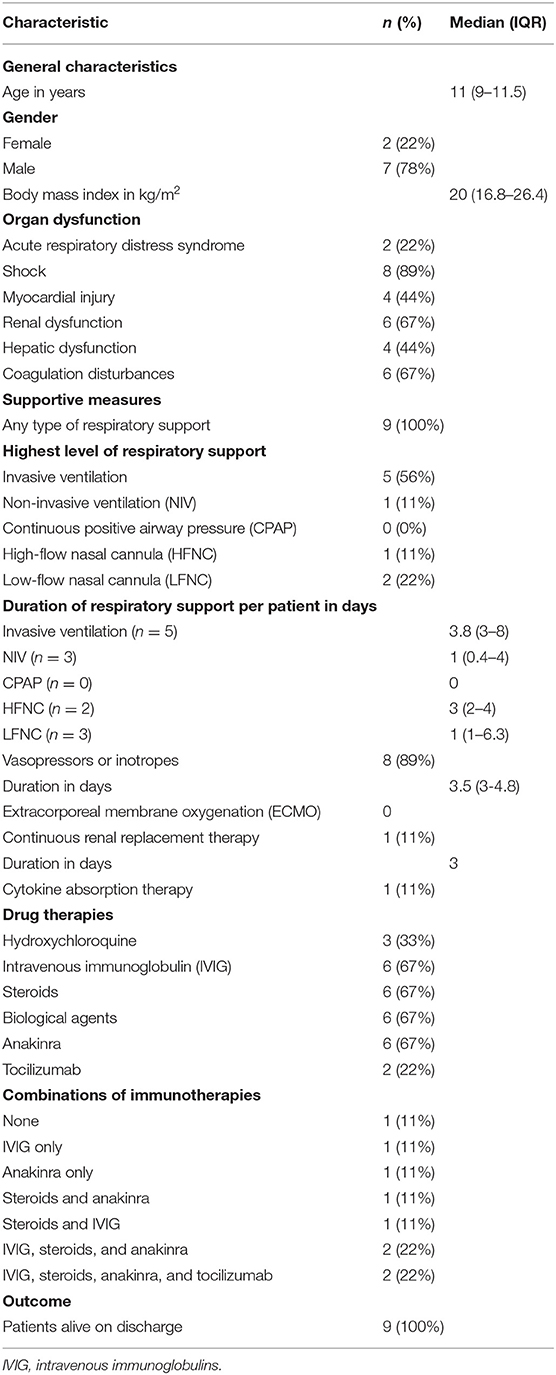
Table 4. General characteristics of patients with pediatric inflammatory multisystem syndrome temporally associated with severe acute respiratory syndrome coronavirus-2 (PIMS-TS), details on organ dysfunction and applied therapies.
Discussion
In this observational study, we describe different aspects of the first wave of the SARS-CoV-2 pandemic impacting the management of Swiss PICUs. Many of these aspects are difficult to measure and especially their temporal relationship complicates the analysis. Although, initially the disease was thought to affect predominantly adult departments, in the course of the pandemic, pediatric units and PICUs were more and more affected. Most of the staff were confronted with a pandemic, a new and unknown situation, for the first time in their life.
The absolute number of pediatric patients requiring intensive care due to severe SARS-CoV-2 and PIMS-TS during the study period was low. Similar results of hospitalized children and adolescents admitted to PICUs have been reported in other studies as well (46, 47). Although Switzerland is a small country, eight independent PICUs treat critically ill children. Each PICU is quite small, operating a relatively small number of beds. Although cooperation between the PICUs exists in several forms, every day professional exchange is not common. These circumstances explain why it took time for the PICU staff to learn about the new disease. However, in the course of the first wave of the pandemic, the PICUs recognized, that it is important to cooperate and to exchange experiences with each other to learn fast about the new disease and to improve patient outcome. As a consequence, Swiss consensus guidelines to treat pediatric patients with PIMS-TS for best practice were established by a multidisciplinary group of Swiss pediatric clinicians with expertise in intensive care, immunology, rheumatology, infectious diseases, and hematology during the second wave of the pandemic at the end of 2020 (http://transfer.imk.ch/f.php?h=3R2LIfFV&d=1).
Apart from the challenge of treating this unknown severely ill patient group, there were different logistical and organizational issues influencing the management of the PICUs. At the beginning of the pandemic a variety of measures to prepare the Swiss hospital network for the pandemic were instituted on federal level. Nationwide, scheduled interventions were canceled to reduce the need for post-interventional intensive care and to increase resources for emergency admissions. The federal government did not differentiate between adult and children's hospitals, provided services or bed occupancy of the individual PICUs. In some regions staff recruitment to the adult wards was required, a measure adopted by regional governments. Our data illustrates the effects of those measures on PICUs. For example, the comparison of PICU 5 with PICU 8 shows the different impact of the policy measures on the workload of individual PICUs. PICU 5 and 8 had almost the same, relatively high, percentage of scheduled admissions. At the same time PICU 8 was not associated to an adult hospital, lost no staff to adult wards and treated very few patients with PIMS-TS, whereas PICU 5 was associated to an adult hospital, a part of its staff was recruited to adult wards and treated significantly more children with PIMS-TS. These clearly different circumstances led to different workloads, to some extent illustrated by the difference in average total NEMS points per patient during the study period (466 vs. 294, Table 2). Although small in numbers, PIMS-TS patients admitted to PICUs were severely ill, caused a higher workload then average PICU patients (total NEMS points per patient 569 vs. per general PICU patient 92, Table 3)The total impact of these patients on total PICU workload during this period can unfortunately not be quantified based on our data.
Different measures influenced the workload and the bed occupancy of the individual PICUs differently, depending on the presence or absence of the single factors and their temporal relationships. Due to their complexity, the exact quantification and comparison of the impact of all these factors was unfortunately not possible. However, thanks to the observations and experiences of the first wave, we recognize that the individual PICUs should be organized primarily by a regional and not federal level and in accordance with but not the same to the surrounding adult hospitals. A timely analysis of the burden and duties of the individual PICU is essential to reduce the workload of the PICU and simultaneously ensure optimal bed occupancy for economic reasons. During a pandemic timely customization of measures is also essential to adapt the usual available resources to the present requirements. Although it is very important to learn of the experiences of the different countries regarding management of a PICU during a pandemic, there is not much literature. Zeng et al. give insights on the management of a PICU in the SARS-CoV-2 pandemic in southwest China. They focus on measurements ensuring the safety of both patients and medical staff (48). This paper proposes and optimizes a strategic plan for the management of SARS-CoV-2 outbreak in PICU and use risk management and process control to effectively manage the department as well as to protect both the patients and the staff (48).
Our study has some limitations. The retrospective design restricts the range of data available from the study population, this applies for both the historical comparison cohort as well as the epidemiological PIMS-TS data. The logistical aspects are difficult to measure and their temporal relationship has impact on their influence on the management of a single PICU. However, the aim of this study was to describe the different issues of the pandemic influencing the PICUs in Switzerland, a small country organized in a decentralized manner.
In conclusion, the SARS CoV-2 pandemic does not exclusively affect adult ICUs, with PICUs also having to face a variety of eventualities with a plethora of consequences. As pandemic continues, reflecting and learning from experience and cooperate with other PICUs is essential to reduce the workload, optimize the bed occupancy and dispose the resources in each individual PICU. In a small country as Switzerland, the different PICUs should be organized dependent of the local and not federal health care policy due to their different characteristics.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Cantonal Ethics Committee of Zurich, Stampfenbachstrasse 121, 8090 Zurich. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
MS and BB made the conception and the design of the study and draft the manuscript. PW-G and MK performed all statistical analyses of the study, interpreted results, and critically revised the manuscript. SG, M-HP, MH, and MA helped with acquisition of data and critical review of the manuscript. All authors have read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank the contributors of all the Swiss PICUs for their effort and help in data collecting: Tilman Humpl (University Hospital of Bern, Department of Pediatric Intensive Care), Thomas Riedel (Cantonal Hospital Graubuenden, Department of Pediatrics), Peter Rimensberger (University Hospital of Geneva, Division of Neonatology and Pediatric Intensive Care, Department of Pediatrics), Bjarte Rogdo (Children's Hospital of Eastern Switzerland, Neonatal, and Pediatric Intensive Care Unit), Martin Stocker (Children's Hospital Lucerne, Neonatal, and Pediatric Intensive Care Unit). We also thank the RISC-19-ICU collaborators represented by Thierry Fumeaux (Hospital of Nyon, Switzerland, Intensive Care Unit), Philippe Guerci (University Hospital of Nancy, France, Department of Anesthesiology and Critical care Medicine), Jonathan Montomoli (Erasmus medical Center, Rotterdam, Netherlands, Department of Intensive Care Medicine), Reto Schüpbach (University Hospital of Zurich, Zurich, Switzerland, Institute of Intensive Care Medicine).
Abbreviations
ARDS, acute respiratory distress syndrome; FOPH, Federal Office of Public Health; ICU, intensive care unit; IQR, interquartile range; MDSi, Minimal Dataset of the Swiss Society of Intensive Care Medicine; MIS-C, multisystem inflammatory syndrome in children; NEMS, Nine Equivalents of nursing Manpower use Score; PCR, polymerase chain reaction; PICU, pediatric intensive care unit; PIM2, Pediatric Index of Mortality 2; PIMS-TS, pediatric inflammatory multisystem syndrome temporally associated with severe acute respiratory syndrome coronavirus-2; pRIFLE, pediatric Risk, Injury, Failure, Loss, End Stage Renal Disease; RISC-19-ICU, Risk Stratification in COVID-19 patients in the ICU; SARS-CoV-2, severe acute respiratory syndrome coronavirus-2; SAS, Sedation-Agitation Scale; SSICM, Swiss Society of Intensive Care Medicine.
References
1. Do LAH, Anderson J, Mulholland EK, Licciardi PV. Can data from paediatric cohorts solve the COVID-19 puzzle? PLOS Pathogens. (2020) 16:e1008798. doi: 10.1371/journal.ppat.1008798
2. COVID-19 | European Centre for Disease Prevention and Control. Available online at: https://qap.ecdc.europa.eu/public/extensions/COVID-19/COVID-19.html#enhanced-surveillance-tab (accessed December 13, 2020).
3. Jiang L, Tang K, Levin M, Irfan O, Morris SK, Wilson K, et al. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect Dis. (2020) 20:e276–e88. doi: 10.1016/S1473-3099(20)30651-4
4. Wald ER, Schmit KM, Gusland DY. A pediatric infectious disease perspective on COVID-19. Clin Infect Dis. (2021) 72:1660–6. doi: 10.1093/cid/ciaa1095
5. Parri N, Lenge M, Buonsenso D. Children with COVID-19 in Pediatric Emergency Departments in Italy. N Engl J Med. (2020) 383:187–90. doi: 10.1056/NEJMc2007617
6. Liguoro I, Pilotto C, Bonanni M, Ferrari ME, Pusiol A, Nocerino A, et al. SARS-COV-2 infection in children and newborns: a systematic review. Eur J Pediatr. (2020) 1–18. doi: 10.21203/rs.3.rs-24629/v1
7. Feldstein LR, Rose EB, Horwitz SM, Collins JP, Newhams MM, Son MBF, et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N Engl J Med. (2020) 383:334–46. doi: 10.1056/NEJMoa2021680
8. Verdoni L, Mazza A, Gervasoni A, Martelli L, Ruggeri M, Ciuffreda M, et al. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. Lancet. (2020) 395:1771–8. doi: 10.1016/S0140-6736(20)31103-X
9. Viner RM, Whittaker E. Kawasaki-like disease: emerging complication during the COVID-19 pandemic. Lancet. (2020) 395:1741–3. doi: 10.1016/S0140-6736(20)31129-6
10. Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet. (2020) 395:1607–8. doi: 10.1016/S0140-6736(20)31094-1
11. Vella LA, Rowley AH. Current insights into the pathophysiology of multisystem inflammatory syndrome in children. Curr Pediatr Rep. (2021) 1–10. doi: 10.1007/s40124-021-00257-6
12. Koskela U, Helve O, Sarvikivi E, Helminen M, Nieminen T, Peltola V, et al. Multi-inflammatory syndrome and Kawasaki disease in children during the COVID-19 pandemic: a nationwide register-based study and time series analysis. Acta Paediatr. (2021) 110:3063–8. doi: 10.1111/apa.16051
13. Guimarães D, Pissarra R, Reis-Melo A, Guimarães H. Multisystem inflammatory syndrome in children (MISC): a systematic review. Int J Clin Pract. (2021) 75:e14450. doi: 10.1111/ijcp.14450
14. Whittaker E, Sinha R. COVID-19: lessons learned from a paediatric high consequence infectious diseases unit. Arch Dis Childhood. (2021). 106:e20. doi: 10.1136/archdischild-2020-319114
15. Licciardi F, Pruccoli G, Denina M, Parodi E, Taglietto M, Rosati S, et al. SARS-CoV-2-induced Kawasaki-like hyperinflammatory syndrome: a novel COVID phenotype in children. Pediatrics. (2020) 146:e20201711. doi: 10.1542/peds.2020-1711
16. DeBiasi RL, Song X, Delaney M, Bell M, Smith K, Pershad J, et al. Severe coronavirus disease-2019 in children and young adults in the Washington, DC, Metropolitan Region. J Pediatr. (2020) 223:199–203.e1. doi: 10.1016/j.jpeds.2020.05.007
17. Whittaker E, Bamford A, Kenny J, Kaforou M, Jones CE, Shah P, et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. J Am Med Assoc. (2020) 324:259–69. doi: 10.1001/jama.2020.10369
18. Wehl G, Franke J, Frühwirth M, Edlinger M, Rauchenzauner M. Successful treatment of pediatric inflammatory multisystem syndrome temporally associated with COVID-19 (PIMS-TS) with split doses of immunoglobulin G and estimation of PIMS-TS incidence in a County district in Southern Germany. Healthcare (Basel). (2021) 9:481. doi: 10.3390/healthcare9040481
19. Vukomanovic V, Krasic S, Prijic S, Ninic S, Popovic S, Petrovic G, et al. Recent experience: corticosteroids as a first-line therapy in children with multisystem inflammatory syndrome and COVID-19-related myocardial damage. Pediatr Infect Dis J. (2021) 40:e390–e4. doi: 10.1097/INF.0000000000003260
20. McArdle AJ, Vito O, Patel H, Seaby EG, Shah P, Wilson C, et al. Treatment of multisystem inflammatory syndrome in children. N Engl J Med. (2021) 385:11–22. doi: 10.1056/NEJMoa2102968
21. Office FS. Population. Available online at: https://www.bfs.admin.ch/bfs/en/home/statistiken/bevoelkerung/stand-entwicklung/bevoelkerung.html (accessed June 12, 2020).
22. Office FS. Territory and Environment. Available online at: https://www.bfs.admin.ch/bfs/en/home/statistiken/raum-umwelt.html (accessed March 20, 2021).
23. Reis Miranda D, Moreno R, Iapichino G. Nine equivalents of Nursing Manpower Use Score (NEMS). Intens Care Med. (1997) 23:760–5. doi: 10.1007/s001340050406
24. Riker RR, Picard JT, Fraser GL. Prospective evaluation of the Sedation-Agitation Scale for adult critically ill patients. Crit Care Med. (1999) 27:1325–9. doi: 10.1097/00003246-199907000-00022
25. SGI-Kat_20060309_d_2012.pdf. Available online at: https://www.sgi-ssmi.ch/files/Dateiverwaltung/de/ressorts/quali/datsa/SGI-Kat_20060309_d_2012.pdf (accessed December 13, 2020).
26. Miranda DR, Nap R, de Rijk A, Schaufeli W, Iapichino G, TISS Working Group. Therapeutic intervention scoring system. Nursing activities score. Crit Care Med. (2003) 31:374–82. doi: 10.1097/01.CCM.0000045567.78801.CC
27. Hartmann B, Junger A, Brenck F, Quinzio L, Benson M, Röhrig R, et al. Vollautomatische kalkulation des pflegeaufwandes auf einer operativen intensivstation. Intensivmedizin. (2004) 41:94–8. doi: 10.1007/s00390-004-0466-8
28. Iapichino G, Radrizzani D, Ferla L, Pezzi A, Porta F, Zanforlin G, et al. Description of trends in the course of illness of critically ill patients. Markers of intensive care organization and performance. Intens Care Med. (2002) 28:985–9. doi: 10.1007/s00134-002-1331-5
29. Frey B, Hossle JP, Seiler Sigrist M, Cannizzaro V. Measurement of resident workload in paediatric intensive care. Swiss Med Weekly. (2013) 143:w13844. doi: 10.4414/smw.2013.13844
30. Keene AR, Cullen DJ. Therapeutic Intervention Scoring System: update 1983. Crit Care Med. (1983) 11:1–3. doi: 10.1097/00003246-198301000-00001
31. MDSi-Portal. Available online at: https://www.savedata.ch/Portal/SaveData/index.php? (accessed December 15, 2020).
32. Slater A, Shann F, Pearson G, Paediatric Paediatric Index of Mortality (PIM) Study Group. PIM2: a revised version of the Paediatric Index of Mortality. Intens Care Med. (2003) 29:278–85. doi: 10.1007/s00134-002-1601-2
33. Paediatric Multisystem Inflammatory Syndrome Temporally Associated With COVID-19 (PIMS) - Guidance for Clinicians. RCPCH. Available online at: https://www.rcpch.ac.uk/resources/paediatric-multisystem-inflammatory-syndrome-temporally-associated-covid-19-pims-guidance (accessed December 31, 2020).
34. Multisystem Inflammatory Syndrome in Children and Adolescents Temporally Related to COVID-19. Available online at: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (accessed December 31, 2020).
35. HAN Archive - 00432 | Health Alert Network (HAN) (2020) Available online at: https://emergency.cdc.gov/han/2020/han00432.asp (accessed May 30, 2020).
36. Wendel Garcia PD, Fumeaux T, Guerci P, Heuberger DM, Montomoli J, Roche-Campo F, et al. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: initial report of the international RISC-19-ICU prospective observational cohort. EClinicalMedicine. (2020) 25:100449. doi: 10.1016/j.eclinm.2020.100449
37. FOPH FO of PH. Coronavirus: Situation in Switzerland. Available online at: https://www.bag.admin.ch/bag/en/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/situation-schweiz-und-international.html (accessed October 31, 2020).
38. Pediatric acute respiratory distress syndrome: consensus recommendations from the Pediatric Acute Lung Injury Consensus Conference. Pediatr Crit Care Med. (2015) 16:428–39. doi: 10.1097/PCC.0000000000000350
39. Goldstein B, Giroir B, Randolph A, Sepsis M of the ICC on P. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics*. Pediatr Crit Care Med. (2005) 6:2–8. doi: 10.1097/01.PCC.0000149131.72248.E6
40. Gebara BM. Values for systolic blood pressure. Pediatr Crit Care Med. (2005) 6:500; author reply 500–1. doi: 10.1097/01.PCC.0000167568.79952.92
41. Lopez L, Colan SD, Frommelt PC, Ensing GJ, Kendall K, Younoszai AK, et al. Recommendations for quantification methods during the performance of a pediatric echocardiogram: a report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J Am Soc Echocardiogr. (2010) 23:465–95; quiz 576–7. doi: 10.1016/j.echo.2010.03.019
42. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. (2015) 28:1–39.e14. doi: 10.1016/j.echo.2014.10.003
43. Soler YA, Nieves-Plaza M, Prieto M, García-De Jesús R, Suárez-Rivera M. pRIFLE (Pediatric Risk, Injury, Failure, Loss, End Stage Renal Disease) score identifies Acute Kidney Injury and predicts mortality in critically ill children: a prospective study. Pediatr Crit Care Med. (2013) 14:e189–e95. doi: 10.1097/PCC.0b013e3182745675
44. Squires JE, McKiernan P, Squires RH. Acute liver failure: an update. Clin Liver Dis. (2018) 22:773–805. doi: 10.1016/j.cld.2018.06.009
45. Toulon P, Berruyer M, Brionne-François M, Grand F, Lasne D, Telion C, et al. Age dependency for coagulation parameters in paediatric populations. Results of a multicentre study aimed at defining the age-specific reference ranges. Thromb Haemostasis. (2016) 116:9–16. doi: 10.1160/TH15-12-0964
46. Swann OV, Holden KA, Turtle L, Pollock L, Fairfield CJ, Drake TM, et al. Clinical characteristics of children and young people admitted to hospital with COVID-19 in United Kingdom: prospective multicentre observational cohort study. Br Med J. (2020) 370:m3249. doi: 10.1136/bmj.m3249
47. Nathan N, Prevost B, Sileo C, Richard N, Berdah L, Thouvenin G, et al. The wide spectrum of COVID-19 clinical presentation in children. J Clin Med. (2020) 9:2950. doi: 10.3390/jcm9092950
Keywords: pediatric intensive care unit, children, SARS-CoV-2 pandemic, pediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2, PIMS-TS, management
Citation: Soomann M, Wendel-Garcia PD, Kaufmann M, Grazioli S, Perez M-H, Hilty MP, André MC and Brotschi B (2022) The SARS-CoV-2 Pandemic Impacts the Management of Swiss Pediatric Intensive Care Units. Front. Pediatr. 10:761815. doi: 10.3389/fped.2022.761815
Received: 31 August 2021; Accepted: 03 January 2022;
Published: 28 January 2022.
Edited by:
Muralidharan Jayashree, Post Graduate Institute of Medical Education and Research (PGIMER), IndiaReviewed by:
Lokesh Tiwari, All India Institute of Medical Sciences (Patna), IndiaQalab Abbas, Aga Khan University, Pakistan
Copyright © 2022 Soomann, Wendel-Garcia, Kaufmann, Grazioli, Perez, Hilty, André and Brotschi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara Brotschi, QmFyYmFyYS5Ccm90c2NoaUBraXNwaS51emguY2g=