 Alexandre Slowetzky Amaro1*
Alexandre Slowetzky Amaro1* Daniela Andrea Rubin2Maria Cristina Triguero Veloz Teixeira1Arcenio José Ferreira Jr.1Graciele Massoli Rodrigues3,4
Daniela Andrea Rubin2Maria Cristina Triguero Veloz Teixeira1Arcenio José Ferreira Jr.1Graciele Massoli Rodrigues3,4 Luiz Renato Rodrigues Carreiro1
Luiz Renato Rodrigues Carreiro1- 1Development Disorders Graduate Program, Center for Health and Biological Science, Universidade Presbiteriana Mackenzie, São Paulo, Brazil
- 2Department of Kinesiology, California State University, Fullerton, CA, United States
- 3Physical Education Program, Universidade São Judas Tadeu, São Paulo, Brazil
- 4Physical Education Program, Escola Superior de Educação Física de Jundiaí, Jundiaí, Brazil
Prader-Willi syndrome (PWS) is a complex genetic disorder requiring interdisciplinary team monitoring and intensive care by parents. So far there is little information on people with PWS in Brazil. Our aim was to describe health problems and treatments used by people with PWS in Brazil and their relationship to their parents' quality of life. Parents answered questionnaires about their child's medical and exercise history, behavior problems, sociodemographic characteristics, and their own quality of life. Results: The responses of the participants showed similar health problems as in other countries. Anxiety and tantrums were the behavioral problems most commonly cited by parents. Parents of people with PWS had lower scores in respect of quality of life than the Brazilian population. Behavioral problems in individuals with PWS were negatively associated with their parents' quality of life. Behavioral and medical conditions in the children were associated with reduced quality of life in the parents. We conclude that heath care should not only be directed toward those with PWS, but also their parents.
Introduction
First described by Prader, Labhart, and Willi in 1956, Prader-Willi syndrome (PWS) is the result of the absence of gene expression of the q11.2-q13 region from chromosome 15 of paternal origin. PWS affects 1:20,000 births and has a prevalence of 1:54,000 (1), and is usually caused by one of three genetic mechanisms: deletion of the paternally inherited 15q11.2-q13 region (DEL), maternal uniparental disomy (UPD), or an imprinting defect (ID) (2, 3). PWS presents a complex clinical and psychiatric phenotype with variations between its genetic subtypes that produce a range of symptoms that include severe neonatal hypotonia, growth hormone deficiency (4), poor motor skills (5), and mild to moderate cognitive deficits (6). Hyperphagia and severe obesity are the main clinical features of the syndrome (7). Hyperphagia begins at about 8 years old and reaches its apex in late adolescence and remains stable throughout life (8). Hyperphagia leads the person with PWS to seek food constantly because the individuals rarely feel full (2, 9).
The most common non-pharmacological strategies used to maintain a healthy weight in PWS include the strict control of caloric intake and the access to food, and exercise (10). However, if these strategies are implemented without adequate medical and nutritional monitoring and parental support, there can be a significant increase in maladaptive behaviors that can become a major source of family stress (11, 12). The most common of these maladaptive behaviors are food-seeking behaviors, severe emotional and behavioral outbursts, hyperphagia, tantrums, stubbornness, manipulative behavior, obsessive-compulsive behaviors, heightened anxiety, sleep disorders, self-injury behaviors, cognitive rigidity, and psychotic symptoms in adulthood (13–15).
Pharmacological treatments are commonly employed to manage the complex clinical conditions of PWS. Psychotropics are prescribed for behavior problems and neuropsychiatric disorders; laxatives for constipation problems; dermatological formulas for the treatment of the ulcerations due to constant skin picking; and antidiabetic and hypotensive drugs for the comorbidities related to obesity (16). However, for the management of hyperphagia several drugs are under study at different phases of clinical trials (10). Hormonal treatment is also extensively employed in PWS, especially growth hormone replacement therapy (GHRT) which is part of the standard of care in addition to nutrition and exercise (10). Studies have shown the benefits of GHRT in respect of psychomotor development (17), cognitive and language function (18, 19), growth in children and adolescents (20), and improved body composition (21, 22). Physical activity and exercise are highly recommended in PWS (23). Increased levels of physical activity have been associated with improved weight and body composition, muscular strength (24, 25), motor skills (25, 26), and metabolic markers related to health (26).
It is a consensus among PWS experts that early intervention and an interdisciplinary approach are the best practices to maintain the health of people with PWS (2, 27). However, the routine of visits to different specialists, drug treatments, and the management of hyperphagia and behavioral problems can overwhelm parents with a high level of physical and mental stress, leading them to a severe decline in their health and quality of life (3, 28–31).
The relationship between physical and mental health problems in children with PWS, treatments and behavior problems, and the quality of life of the parents of individuals with PWS is not well-established. A better understanding of the associations between these domains could contribute to improved intervention programs for patients with PWS and their parents. This study aimed to: (1) describe health conditions and behavioral problems in Brazilian children, adolescents and adults with PWS and (2) to examine the possible associations between health conditions and behavioral problems in individuals with PWS and their parents' quality of life.
Materials and Methods
Participants
The sample included 41 individuals (children, adolescents, and adults) aged from 1 month to 38 years with genetically confirmed PWS. The patients were recruited mainly from the database of the Graduate Program in Developmental Disorders of Mackenzie Presbyterian University, medical genetics centers of other universities, and from Brazilian PWS social networks. The primary caregiver (parent or guardian) had to be aged over 18 years and had to provide genetic diagnosis for their child or the person with PWS they cared for.
Materials and Measures
In order to collect the data of this study, we used:
Sociodemographic Questionnaire
For characterization of the sociodemographic profile of the sample comprising items that included sex, civil status, level of education, and type of health insurance.
Medical History and Exercise Questionnaire
A questionnaire was completed that included a medical and exercise history developed by Rubin et al. (32) and translated into Brazilian Portuguese and adapted for this study by the authors (unpublished data). The questionnaire comprises dichotomous questions for the presence or absence of diseases, causes of hospitalization, causes of surgeries, treatments or therapies used, types of physical activity practiced, and total weekly physical activity in number of hours/week. Parents or caregivers also reported the body mass (in kg) and height (in m) of their child measured in the last month. The reported body mass and stature were used to calculate body mass index [BMI; body mass (kg)/height squared (m2)]. BMI was then converted to BMI percentile, according to the World Health Organization guidelines (33). For those participants who were over 19 years old, the reference values for the Brazilian population were used to calculate the BMI percentile (34). All items of this questionnaire were based on parental answers.
Brief Problem Monitor for Parents (BPM-P 6/18)
This is a short version of the Child Behavior Checklist (CBCL 6/18) (35) that evaluates emotional and behavioral problems of children and adolescents between 6 and 18 years old in three scales: internalizing behavioral problems, externalizing behavioral problems, and inattention problems. Externalizing problems are behaviors such as impulsivity, nervousness, aggressiveness, impatience/restlessness, destructiveness, disobedience, teasing behavior, and fights. Internalizing problems include withdrawal, depression, anxiety, irritability, sadness, somatic complaints related to emotional functioning, shyness, excessive preoccupation, insecurity and fears (35). The BPM-P contains 19 self-reported questions scored on a 3-point Likert scale (0–2 scale), being: 0 = “Not true”; 1 = “Somewhat true” and; 2 = “Very true.” The Achenbach System of Empirically Based Assessment (ASEBA) software generates a T score for each variable, indicating the degree of deviance from normality, categorizing the participant as normal or elevated. In this study, parents of children under 6 years old and adults over 18 years old did not answer the BPM-P, since the version used only applies to 6–18 years old. This scale was used to obtain information from the perspective of the parents of the individual with PWS.
World Health Organization Quality of Life Instrument Version Brief (WHOQOL-Bref)
This is a comprehensive tool used to measure the self-perception of quality of life. The WHOQOL-bref is composed of 24 questions on a Likert scale, providing the perception of the quality of life in four domains: physical, psychological, social relations, and environment. Additionally, two questions about overall and general health are included (36). We used the Microsoft Excel worksheet developed by Pedroso (37) to calculate the output of each of the domains. This questionnaire was used to evaluate the quality of life of the parents of individuals with PWS.
Procedures
This study was first approved by the Ethics Committee of Mackenzie Presbyterian University under Code: CEP/UPM n° 784.029/08/2014 and CAEE: 34649314.2.0000.0084). The data collection occurred in three ways: (1) Parents were invited to visit the Developmental Disorders Department of Mackenzie Presbyterian University; (2) The research team visited parents in their homes; (3) The research team conducted the visit with parents remotely using telephone calls and/or video conferences. If the visit took place by phone or by video conference, the consent form was sent by e-mail and parents returned it via mail together with a copy of the genetic test confirming the diagnosis.
Statistical Analysis
This was a descriptive, exploratory, and transversal study. Data are presented as raw and percentage values. Normal distribution for continuous variables was tested using skewness and kurtosis, and comparison tests between sex and genetic subtypes were done using t-student and Mann–Whitney tests. Behavior characterization was analyzed in individuals ages 6–18 years and further evaluated with regards to the use of GHRT. We codified the classification of quality of life of parents based on Cruz et al. (38) and used the paired Student's t-test to compare the quality of life values with normal reference values according Cruz et al. (38). Spearman correlation (rs) analyses were calculated to assess the associations between the emotional and behavioral problems, age and physical and mental indicators of the individuals with PWS and the quality of life of their parents. Other associations evaluated included those between family monetary income and child's behavior and parents' quality of life. The correlation coefficient were interpreted as: 0.1–0.3, weak; 0.4–0.6, moderate; 0.7–09, strong. The significance level adopted was p ≤ 0.05. Therefore, all intervals in the present study were constructed with 95% statistical confidence. However, the p > 0.05 and p <0.1 were also analyzed because they are close to the acceptance limit (up to 5 percentage points above the alpha value adopted).
Results
Sample Description
Table 1 shows the characterization of the parents of individuals with PWS by sexes. Most parents who participated were female, married, with an average income of R$ 7.488,06 (~US$ 2,300.00) (n = 31, 25th = 2,000.00, 50th = 4,000.00, 75th = 12,000.00). The age of parents did not differ between sex [t(39) = 1.76, p = 0.87, IC (95%) = −0.92 to 13.32].
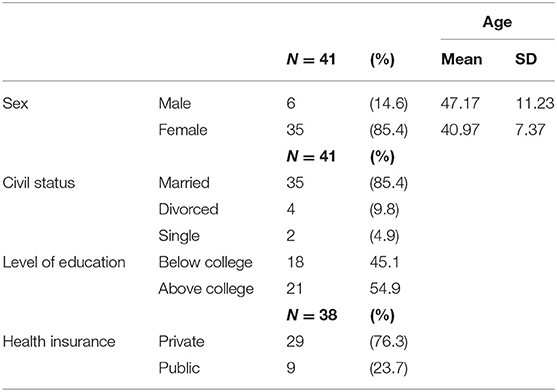
Table 1. Characterization of parents' profile.
Table 2 shows the sociodemographic and clinical characterization of the participants with PWS. There were no statistical differences between female and male participants in respect of age (U = 150.50, p = 0.157). Body mass and height were reported for 35 participants with PWS (85.37%). The analyses of the BMI percentile showed that 57.1% of participants (n = 20) were obese, 8.6% (n = 3) were overweight, 28.6% (n = 10) were of normal weight and 5.7% (n = 2) were underweight. There was no difference in the BMI percentile between participants' sex (U = 131.00, p = 0.515). Fourteen participants were presently or had been on GHRT.
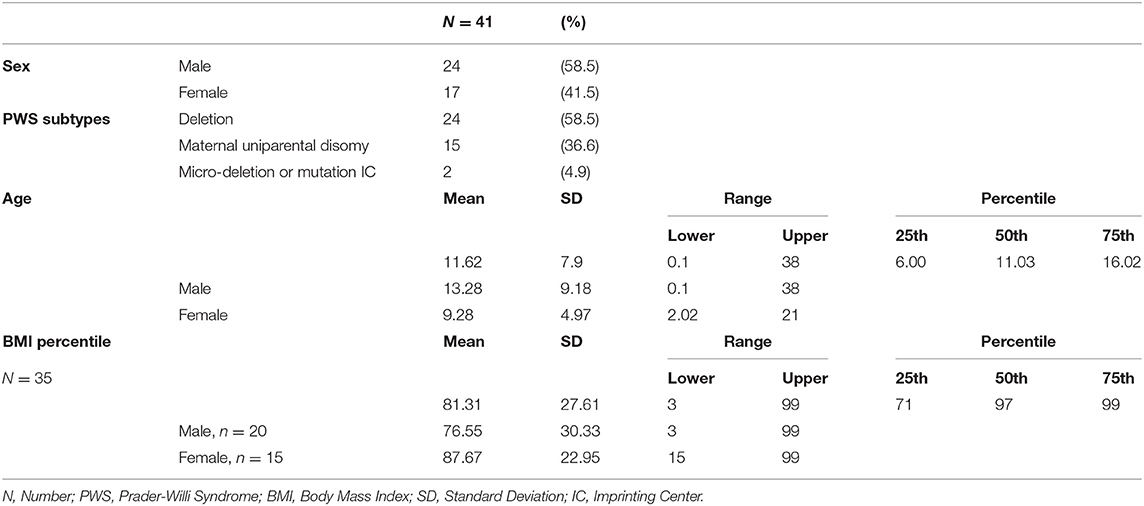
Table 2. Sociodemographic and clinic profile of PWS children, adolescents, and adults.
The number of hospitalizations did not differ as a function of PWS subtypes (DEL and UPD) (DEL M = 3.54, SD = 2.64, UPD M = 3.47, SD = 3.78, U = 0.152, and p = 0.411). The main reasons for hospitalization were cryptorchidism, adenoidectomy, tonsillectomy, and inguinal hernia. The percentage of surgery cases related to cryptorchidism and gynecoplasty was corrected by the number of participants and gender (see Table 3).
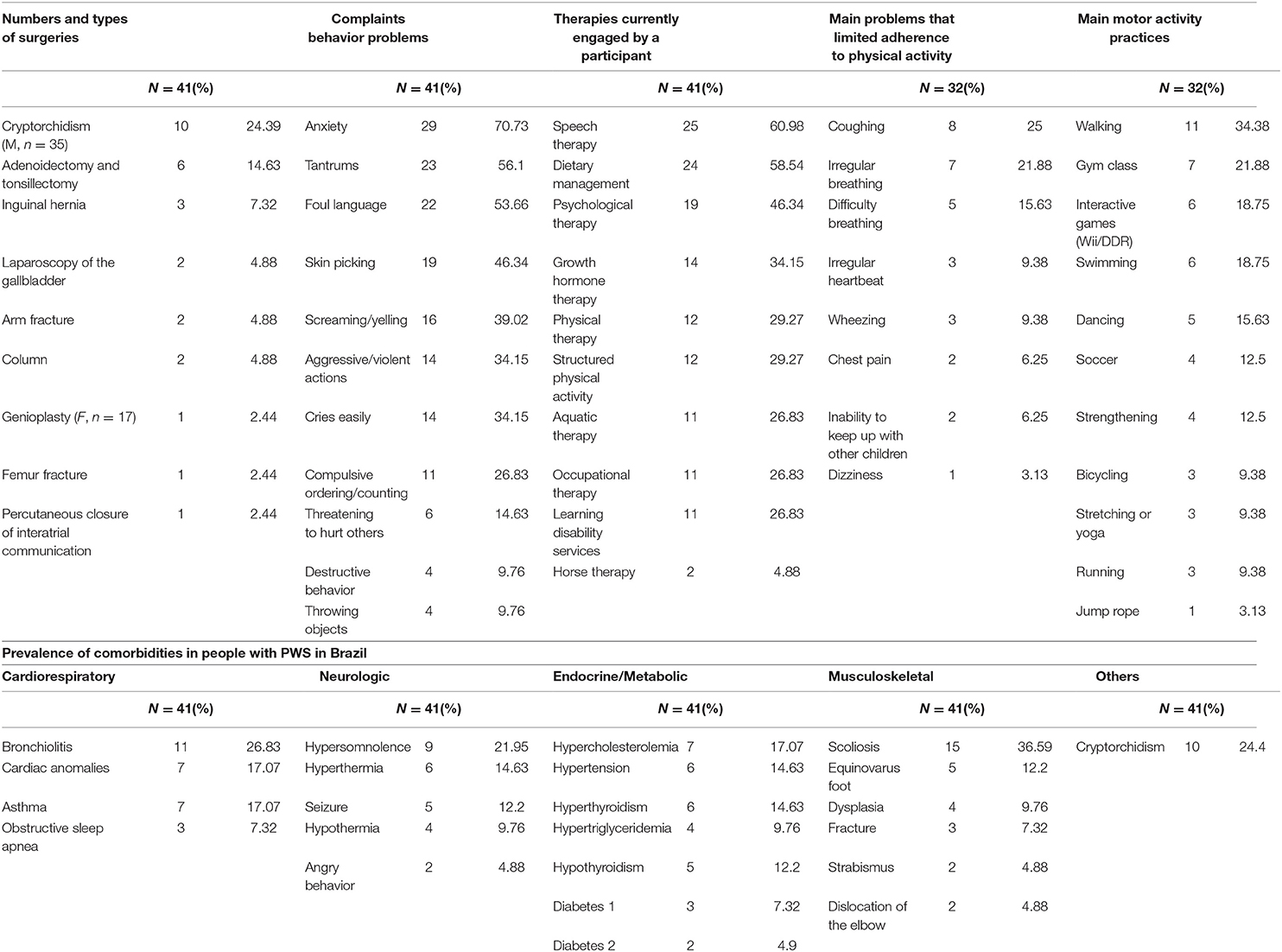
Table 3. Main surgery cases, frequency of behavioral problems, therapies used, physical activities problems, and practices.
Table 3 summarizes data related to surgeries, behavioral problems, therapies used, physical activity and comorbidities. The mean incidence of emotional and behavioral problems was 3.2 (SD = 3.2, lower = 0, upper = 11) and there were no differences among the PWS subtypes [t(37) = 0.994, p = 0.327] or sex [t(39) = −0.872, p = 0.389]. Forty-six percent of parents (46.9%, n = 15) believed that the emotional and behavioral problems of their children and adolescents could interfere in physical activity program adherence. There were no differences in the number of therapies engaged in among PWS subtypes [t(39) = −0.809, p = 0.403] or sex [t(37) = 0.495, p = 0.623]. The main barriers to physical activities reported by parents were coughing and irregular breathing. The mean number of physical activities practiced was 1.78 (SD = 1.50, lower = 0, and upper = 7) and the mean time spent in physical activity was 110.78 (SD = 121.91, lower = 0, and upper = 450) minutes per week.
We assessed the behavior problems of participants aged between 6 and 18 years old (n = 18, M = 10.38, and SD = 3.13). It was observed that 38.9% (n = 7) reached the internalizing clinical level; 66.7% (n = 12) reached the attention clinical level, and 77.8% (n = 14) reached the externalizing problems clinical level. In respect of the total score, 77.8% (n = 14) of all participants reached a clinical level. Participants who had been on GHRT in the past or were presently on GHRT presented lower externalizing scores (U = 15, p = 0.035) and a tendency to higher parental quality of life in respect of the environment domain [t(38) = 1.824, p = 0.076] in comparison to participants who had not been on GHRT.
Table 4 shows the parents' quality of life. The results revealed that parents of people with PWS present significantly lower quality of life in the psychology, social relation and environment domains compared to Brazilian reference values.

Table 4. Results of parents' quality of life (WHOQOL).
Relationships Between Characteristics in Individuals With PWS
There were significant positive and moderate correlations between the age of the person with PWS and number of hospitalizations (rs = 0.466, p = 0.002) and number of behavioral problems presented (rs = 0.399, p = 0.01). There was also a negative correlation between BMI percentile and the number of behavior problems presented by people with PWS (rs = 0.510, p = 0.002).
The age of the individuals with PWS also showed positive and moderate correlations with total number of hospitalization (rs = 0.466, p = 0.002), and total number of behavior problems (rs = 0.399, p = 0.01), externalizing problems (rs = 0.493, p = 0.038), and a marginal correlation with internalizing problems (rs = 0.467, p = 0.051). Additionally, total number of hospitalizations also showed a positive correlation with total score for behavior problems (rs = 0.479, p = 0.044), internalizing problems (rs = 0.483, p = 0.042), and marginal correlations with attention (rs = 0.418, p = 0.084) and externalizing problems (rs = 0.437, p = 0.07).
Association Between Family Income, Parent's Quality of Life, and Child Profile
There were significant moderate associations between family income and parents' quality of life social domain (rs = 0.365, p = 0.043), environment domain (rs = 0.469, p = 0.008), self-assessment domain (rs = 0.427, p = 0.017), and total (rs = 0.371, p = 0.040). The family income was also associated with the total number of therapies the person with PWS was engaged in (rs = 0.414, p = 0.021). The income also presented a marginal negative and moderate correlation with the number of behavior problems exhibited by people with PWS (rs = −0.325, p = 0.075).
Table 5 shows the associations between parents' quality of life and child demographics, medical history and behavior. The total score for quality of life of parents of persons with PWS was moderately associated with the age of the child (rs = −0.467), BMI percentile of the child (rs = −0.353, p = 0.037), and total number of hospitalization (rs = −0.483). Total quality of life was also related to the child's behaviors such as internalizing behavioral problems (rs = −0.500), externalizing behavioral problems (rs = −0.557), total behavioral problems (rs = −0.647).
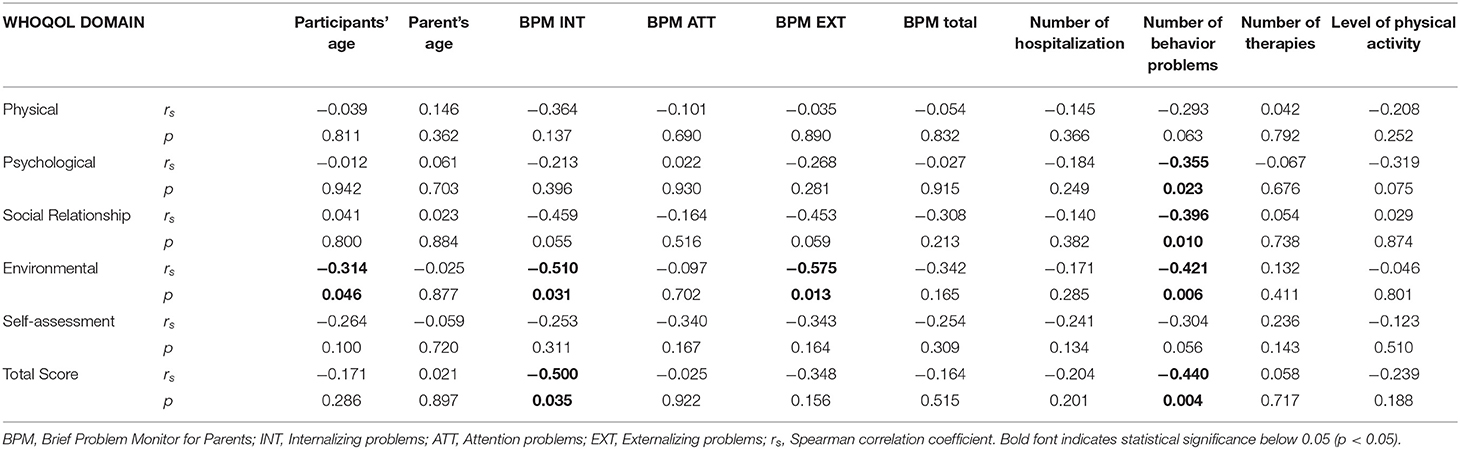
Table 5. Correlation test for parents' quality of life (WHOQOL) and BPM-P indexes and MHEQ survey.
The parents' quality of life in respect of the physical domain was moderately associated with the child's BMI (rs = −0.332, p = 0.051) and the number of the child's behavior problems (rs = −0.317). The psychological domain was associated with the child's BMI (rs = −0.377, p = 0.026), and number of behavioral problems (rs = −0.379). The social domain was associated with the child's BMI rs = −0.355, p = 0.036). The quality of life environment domain was associated with the child's age (rs = −0.402), internalizing (rs = −0.510), externalizing (rs = −0.575) problems, and total behavior problems (rs = −0.455). The self-assessment domain showed a marginal negative correlation with the age of the children (rs = −0.264) and the number of behavioral problems (rs = −0.304; Table 5).
Discussion
We report a descriptive analysis of medical, behavioral and emotional problems in Brazilian individuals with PWS and the associations with their parents' quality of life. People with PWS frequently have restricted access to health services in developing countries such as Brazil (39), often only receiving interventions for managing symptoms without a multidisciplinary approach that includes controlling food access, hormone replacement therapies, special education, and psychological interventions.
The mean BMI percentile was 81.31%, characterizing the sample as obese. This is twice as high as that in a study by Diene et al. (40) of a young French PWS sample, and very similar to results in adults reported by Grugni et al. in an Italian study (41). It is clear that the management of nutrition in people with PWS in Brazil needs to be considered very carefully. Brazilians still eat a large number of high-calorie items low on nutritional value. Additionally, a deficit in therapies and GHRT may help to explain the obesity prevalence in this study, as only 14 participants were or had been on GH. Because of the potential progression of health complications with increased obesity and age, the Brazilian population with PWS may be in a vulnerable position in respect of a premature decline in health.
The health problems reported in this study, which can lead to hospitalization, are also found in other studies of people with PWS (42). In our study, 85.4% of the group had endocrine/metabolic problems, while 68.3% had cardiorespiratory problems, and 63.5% had neurological problems. All of these conditions are a high-risk factor for death in PWS. A study conducted by Tauber et al. (43) analyzed the obituary of 64 people with PWS and found that respiratory diseases caused 61% of deaths. In adults with PWS, respiratory infections and obesity-related comorbidities that affect the cardiorespiratory system increase the mortality rate for people over 30-years of age. Among children with PWS, respiratory infections accompanied by a high fever and a lack of immunological response to medication are the major mortality risk factors (44). In our sample, cardiorespiratory symptoms such as bronchiolitis, cardiac anomalies, asthma, and obstructive sleep apnea were present in 68.3% of the sample, indicating an increased risk of death.
Neurological disorders are also a health problem requiring the attention of caregivers and professionals (Table 3). Hypothalamic dysfunction may produce an exacerbated pyrexia response in infectious conditions. However, the absence of pyrexia has been observed in severe infections. Parents, caregivers, and health professionals need to be aware of the behavioral changes and other signs that may indicate problems in people with PWS. Late diagnosis may aggravate the associated diseases and increase the risk of death (45).
The prevalence of obesity-related metabolic diseases observed in this study were consistent with those reported in other studies (46, 47). Despite the severe obesity observed in the participants of this study (71.4%; Table 2), and in many other studies (47, 48), the prevalence of metabolic diseases in PWS was low when compared to typical subjects matched by the percentage of body fat. The causes of this lower prevalence of metabolic diseases are not clear; however, care should not be neglected. In our study, 65.9% of the sample had endocrine/metabolic anomalies such as hypercholesterolemia, hyperthyroidism/hypothyroidism, hypertriglyceridemia, and diabetes 1 and 2 (Table 3). In some cases of PWS in Brazil, the controversial decision to perform bariatric surgery has been taken (49, 50). However, the long-term results may not be effective considering the psychiatric comorbidities and intellectual disability that compromise the control of eating behavior.
Deviations in the spine, equinovarus foot and dysplasia are anomalies commonly observed in PWS and, in addition to hypotonia and obesity, they contribute to a change in body center of gravity, increasing the risk of falls and fractures (Table 3) (51, 52). This study reported three cases of surgical intervention related to fall fracture and two cases of surgery due to deviations in the spine (Table 4). Maintaining high levels of daily physical activity, and actively participating in physical activity may potentially contribute to strengthening muscles and bones (26, 53–57).
Behavioral problems are a common phenotype of PWS, and, in this study, we observed that anxiety was the main disorder reported by parents. Research has consistently shown that people with PWS resulting from UPD show a higher prevalence of psychiatric disorders than those resulting from DEL (58) and that behavioral problems increase with age (15). In this study, a positive correlation was observed between the age of the children and adolescents with problems with internalizing, attention, externalizing, and overall behavior. The findings reinforce the importance of behavioral psychological therapy to guide parents on how to manage children's behavioral problems and thus improve the family and social relationship interactions of the person with PWS (59).
The most used therapy by the participants of this study was speech therapy, followed by nutritional, psychological, hormonal, physical, and others (Table 3). Speech problems due to hypotonia and adenoid hypertrophy affect a large part of the population with PWS. Speech therapy can contribute to better social interaction (60, 61). However, it is worth mentioning that nutritional treatment, currently practiced by 58% of the sample (Table 3), should be practiced by all the participants of this study due their hyperphagic behavior and obesity (12). In addition to nutrition, physical activity has the potential to contribute to the improvement of behavior and body composition problems (53, 54, 56, 57, 62).
The complaints reported during the practice of physical activity in this study (Table 3) do not seem to be related to any dysfunction that completely prevents its practice. People with PWS are mostly hypoactive. However, if properly stimulated, they can become highly motivated to practice physical activity (53, 63). In this study, the main physical activity practiced by the PWS individuals was walking. Although the benefits of walking are well-known, it is important to ensure that the walking is done in at an intensity that produces the desired adaptations (improvements in cardiorespiratory fitness, body composition and a reduction in stress level) and that more elaborate exercise routines are implemented to amplify the neuromuscular (25, 64, 65) and cognitive gains (66).
Diabetes have been reported in 25% of adults and 12% of children with PWS (40, 67). In our study sample, diabetes was reported in 12% of the participants, with 7% presenting type 1 diabetes, which is uncommon for the syndrome. As our sample comprised a broad age range (1 month to 38 years old), this could have affected the relative frequency of diabetes. The prevalence of strabismus in the PWS population has been estimated to be about 60% (16). In our study, we reported two cases with strabismus. It is likely that this result could be associated with the small sample size or parent underreporting for this item in the questionnaire.
Parents reported a lower perception of quality of life in respect of the psychological, social relations, and environmental domains than the reference values for the Brazilian population (Table 4) (38). The results of this study are consistent with previous research that shows a deterioration in the perception of quality of life among caregivers of people with PWS when compared to parents of typical children and adolescents (30).
Interestingly, it was observed in the present study that the group of participants who used GH treatment had a lower level of externalizing problems and that parents tended to have a higher perception of life quality in the environment domain. As previously demonstrated in other studies, treatment with GH stimulates cranial-brain growth, increases lean mass and activity levels among children and young adults with PWS (22, 68). It is possible to infer that the gains from GH treatment result in an overall improvement in the health status of individuals with PWS, and a consequent concomitant increase in the parents' perception of quality of life. A previous study conducted in Brazilian PWS patients also reported the benefits of GHRT (69).
In this study, there were positive associations between age, and behavioral problems and health problems leading to hospitalization in those with PWS. As expected, families with higher incomes provided the greatest number of treatments; however, the number of treatments for those with PWS was not positively related to the quality of life of the parents.
The total number of hospitalizations showed a positive correlation with behavior problems. Despite the well-described clinical phenotypes exhibited among the individuals with PWS, it is possible to see a wide range of variation within them. DNA deletion in particular has been associated with seizure frequency (70) and brain structural and neural connection abnormalities s (71, 72). It is not unreasonable to assume that different deletion sizes could lead to variations in the number and severity of the physical and psychiatric comorbidities. Amaro et al. (53) reported that physical training reduces complaints of behavioral problems by the parents of children with PWS in a case study. Thus, it is possible to that an appropriate intervention program could promote a general improvement in health that leads to a reduction in behavioral problems (73, 74). However, more studies are needed to confirm this hypothesis.
It was hypothesized in this study that a greater number of treatments and therapies attended by those with PWS would be associated with a lower quality of life in their caregivers because of the constant pressure of medical visits resulting in increased stress. However, this hypothesis was not confirmed. The data from this study suggests that behavioral problems were the main element related negatively to the quality of life of the parents, either by the total behavioral problems presented or by the magnitude of the disorders.
Previous studies have shown a negative association between quality of life in PWS caregivers related to their child's age (29, 30), genetic subtypes (30) and motor performance (75). As previously discussed, parents of children with PWS may feel overloaded because of the continuous need to pay attention to the many aspects of their child's health, from very early childhood to older ages. Furthermore, behavior problems associated with PWS can lead parents to mental and emotional exhaustion (3), which contribute significantly to reducing their quality of life. Therefore, it is necessary to pay careful attention to the parents' health during all stages of their child's life, and provide instruction on how to cope with the syndrome as well as providing physical, psychological, and social therapies.
Study Limitations
While the information presented in the study is novel as it relates to the Brazilian population, it has some limitations such as the small sample size; however, PWS is a rare disorder which makes gathering large samples difficult, and despite the small sample size, the study was able to provide a survey of the health problems in this population group and the impact of the condition on the quality of life of the parents and caregivers. In addition, data were collected through the parental report, which may lead to a potential interpretation bias. Furthermore, the participating families had a relatively high monetary income, which may not represent the overall Brazilian socio-economic reality. A final limitation is the absence of behavioral problem measures from those participants over 18 years old (19% of whole sample), because the youth version of BPM (BPM-Y) was not available in Brazil when this study was conducted.
Conclusions
This is the first Brazilian study that characterized health problems and types of interventions in a sample of children, adolescents, and adults with PWS. Furthermore, this is the first study that evaluated the association between demographics, health, and behavioral problems in people with PWS and their parents' quality of life. Additionally, this study showed that health problems of the group were similar to those shown in previous research. An increased number of therapy and treatments for those with PWS was not associated with their parents' quality of life, while behavioral problems were negatively associated with parents' quality of life. Future studies should consider to what extent access to mental health services in this population determines the effects on the quality of life and mental health of individuals with PWS and their primary caregivers. There is clear need for multidisciplinary interventions for individuals with PWS, and health teams should not only focus on monitoring their patients, but also the mental health and quality of life of caregivers and parents.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Comitê de Ética e Pesquisa Universidade Presbiteriana Mackenzie. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
AA, LC, DR, and MT designed the study, drafted and wrote the manuscript, and revised and replied to the reviewers' comments. AA and AF performed the research and acquired the data. AA, LC, GR, and DR interpreted and analyzed the data. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by the Universidade Presbiteriana Mackenzie through doctoral scholarships, the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) by supporting academic exchange through the Programa de Doutorado-sanduíche no Exterior (PDSE)—Proex number: 1133/2019.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all the amazing parents and their children for their participation in this study, their patience, affection and love.
References
1. Whittington JE, Holland AJ, Webb T, Butler J, Clarke D, Boer H. Population prevalence and estimated birth incidence and mortality rate for people with Prader-Willi syndrome in one UK health region. J Med Genet. (2001) 38:792–8. doi: 10.1136/jmg.38.11.792
2. Cassidy SB, Schwartz S, Miller JL, Driscoll DJ. Prader-Willi syndrome. Genet Med. (2012) 14:10–26. doi: 10.1038/gim.0b013e31822bead0
3. Lanfranchi S, Vianello R. Stress, locus of control, and family cohesion and adaptability in parents of children with down, williams, fragile x, and prader-willi syndromes. Am J Intellect Dev Disabil. (2012) 117:207–24. doi: 10.1352/1944-7558-117.3.207
4. Sinnema M, van Roozendaal KEP, Maaskant MA, Smeets HJM, Engelen JJM, Jonker-Houben N, et al. Different distribution of the genetic subtypes of the Prader-Willi syndrome in the elderly. Eur J Hum Genet. (2010) 18:993–8. doi: 10.1038/ejhg.2010.67
5. Lam MA, Rubin DA, Duran AT, Chavoya FA, White E, Rose DJ. A characterization of movement skills in obese children with and without Prader-Willi syndrome. Res Q Exerc Sport. (2016) 87:245–53. doi: 10.1080/02701367.2016.1182113
6. Rice L, Einfeld S. Cognitive and behavioural aspects of Prader-Willi syndrome. Curr Opin Psychiatry. (2015) 28:102–6. doi: 10.1097/YCO.0000000000000135
7. Welden JR, Zhang Z, Duncan MJ, Falaleeva M, Wells T, Stamm S. The posterior pituitary expresses the serotonin receptor 2C. Neurosci Lett. (2018) 684:132–8. doi: 10.1016/j.neulet.2018.06.051
8. Miller JL, Lynn CH, Driscoll DC, Goldstone AP, Gold A, Kimonis V, et al. Nutritional Phases in Prader - Willi Syndrome. Am J Med Genet. (2011) 155A:1040–9. doi: 10.1002/ajmg.a.33951
9. Heymsfield SB, Avena NM, Baier L, Brantley P, Bray GA, Burnett LC, et al. Hyperphagia: current concepts and future directions proceedings of the 2nd international conference on hyperphagia. Obesity. (2014) 22:1–35. doi: 10.1002/oby.20646
10. Tan Q, Orsso CE, Deehan EC, Triador L, Field CJ, Tun HM, et al. Current and emerging therapies for managing hyperphagia and obesity in Prader-Willi syndrome: a narrative review. Obes Rev. (2020) 21:e12992. doi: 10.1111/obr.12992
11. Penner V, Lima D, Ribas D, Luiza M, Mesquita G, Carolina A, et al. Eating Behaviors Nutritional intervention with hypocaloric diet for weight control in children and adolescents with Prader - Willi Syndrome. Eat Behav. (2016) 21:189–92. doi: 10.1016/j.eatbeh.2016.03.008
12. Mesquita MLG, Seraceni MFF, Carreiro LRR, Lima VP, Amaro AS, Neto JMP. Restrição alimentar e problemas de comportamento de crianças com Síndrome de Prader-Willi. Rev Bras Ter Comport e Cogn. (2014) 16:30–40. doi: 10.31505/rbtcc.v16i1.656
13. Bohonowych J, Miller J, McCandless SE, Strong T V. The global Prader - Willi syndrome registry: development, launch, and early demographics. Genes (Basel). (2019) 10:713–27. doi: 10.3390/genes10090713
14. Schwartz L, Holland A, Dykens E, Strong T, Roof E, Bohonowych J. Prader-Willi syndrome mental health research strategy workshop proceedings: the state of the science and future directions. Orphanet J Rare Dis. (2016) 11:1–7. doi: 10.1186/s13023-016-0504-1
15. Avrahamy H, Pollak Y, Shriki-Tal L, Genstil L, Hirsch HJ, Gross-Tsur V, et al. A disease specific questionnaire for assessing behavior in individuals with Prader-Willi syndrome. Compr Psychiatry. (2015) 58:189–97. doi: 10.1016/j.comppsych.2014.12.005
16. Sinnema M, Maaskant MA, van Schrojenstein Lantman-de Valk HMJ, Boer H, Curfs LMG, Schrander-Stumpel CTRM. The use of medical care and the prevalence of serious illness in an adult Prader-Willi syndrome cohort. Eur J Med Genet. (2013) 56:397–403. doi: 10.1016/j.ejmg.2013.05.011
17. Festen DAM, Wevers M, Lindgren AC, Böhm B, Otten BJ, Wit JM, et al. Mental and motor development before and during growth hormone treatment in infants and toddlers with Prader-Willi syndrome. Clin Endocrinol (Oxf). (2008) 68:919–25. doi: 10.1111/j.1365-2265.2007.03126.x
18. Dykens EM, Roof E, Hunt-hawkins H. Cognitive and adaptive advantages of growth hormone treatment in children with Prader-Willi syndrome. J Child Psychol Psychiatry. (2016) 58:1–11. doi: 10.1111/jcpp.12601
19. Myers SE, Whitman BY, Carrel AL, Moerchen V, Bekx MT, Allen DB. Two years of growth hormone therapy in young children with Prader-Willi Syndrome: physical and neurodevelopmental benefits. Am J Med Genet A. (2007) 143:443–8. doi: 10.1002/ajmg.a.31468
20. Reus L, Pillen S, Pelzer BJ, van Alfen-van der Velden JAAEM, Hokken-Koelega ACS, Zwarts M, et al. Growth hormone therapy, muscle thickness, and motor development in Prader-Willi syndrome: an RCT. Pediatrics. (2014) 134:e1619–27. doi: 10.1542/peds.2013-3607
21. Lafortuna CL, Minocci A, Capodaglio P, Gondoni LA, Sartorio A, Vismara L, et al. Skeletal muscle characteristics and motor performance after 2-year growth hormone treatment in adults with prader-willi syndrome. J Clin Endocrinol Metab. (2014) 99:1816–24. doi: 10.1210/jc.2013-3607
22. Gouveia C De, Passone B, Franco RR, Ito SS, Trindade E, Polak M, et al. Growth hormone treatment in Prader-Willi syndrome patients: systematic review and meta-analysis. BMJ Paediatr Open. (2020) 4:e000630. doi: 10.1136/bmjpo-2019-000630
23. Morales JS, Valenzuela PL, Pareja-Galeano H, Rincón-Castanedo C, Rubin DA, Lucia A. Physical exercise and Prader-Willi syndrome: a systematic review. Clin Endocrinol (Oxf). (2019) 90:649–61. doi: 10.1111/cen.13953
24. Madhav N, Oppenheim B, Gallivan M, Mulembakani P, Rubin E, Wolfe N. Disease Control Priorities, Third Edition (Volume 9): Improving Health and Reducing Poverty. The World Bank (2017).
25. Vismara L, Cimolin V, Grugni G, Galli M, Parisio C, Sibilia O, et al. Effectiveness of a 6-month home-based training program in Prader-Willi patients. Res Dev Disabil. (2010) 31:1373–9. doi: 10.1016/j.ridd.2010.07.001
26. Rubin DA, Duran AT, Haqq AM, Gertz ER, Dumont-Driscoll M. Changes in cardiometabolic markers in children with Prader-Willi syndrome and nonsyndromic obesity following participation in a home-based physical activity intervention. Pediatr Obes. (2018) 13:734–43. doi: 10.1111/ijpo.12462
27. Butler MG, Miller JL, Forster JL. Prader-Willi syndrome - clinical genetics, diagnosis and treatment approaches: an update. Curr Pediatr Rev. (2019) 15:1–37. doi: 10.2174/1573396315666190716120925
28. Passone CBG, Pasqualucci PL, Franco RR, Ito SS, Mattar LBF, Koiffmann CP, et al. Prader-Willi syndrome: what is the general pediatrician supposed to do? - A review. Rev Paul Pediatr. (2018) 36:345–52. doi: 10.1590/1984-0462/;2018;36;3;00003
29. Mao S-J, Shen J, Xu F, Zou C-C. Quality of life in caregivers of young children with Prader-Willi syndrome. World J Pediatr. (2019) 15:506–10. doi: 10.1007/s12519-019-00311-w
30. Ihara H, Ogata H, Sayama M, Kato A, Gito M, Murakami N, et al. QOL in caregivers of Japanese patients with Prader-Willi syndrome with reference to age and genotype. Am J Med Genet A. (2014) 164:2226–31. doi: 10.1002/ajmg.a.36634
31. Kayadjanian N, Schwartz L, Farrar E, Comtois KA, Strong TV. High levels of caregiver burden in Prader-Willi syndrome. PLoS One. (2018) 13:e0194655. doi: 10.1371/journal.pone.0194655
32. Rubin DA, Wilson KS, Wiersma LD, Weiss JW, Rose DJ. Rationale and design of active play @ home: a parent-led physical activity program for children with and without disability. BMC Pediatr. (2014) 14:41. doi: 10.1186/1471-2431-14-41
33. World Health Organization - WHO. Obesity. (2020). Available online at: https://www.who.int/health-topics/obesity#tab=tab_1 (accessed Dec 15, 2020).
34. Ministério da Saúde,. VIGITEL: VIGILÂNCIA DE FATORES DE RISCO E PROTEÇÃO PARA DOENÇAS CRÔNICAS POR INQUÉRITO TELEFÔNICO. Brasilia (2017). Available online at: http://www.abeso.org.br/uploads/downloads/100/5949633674659.pdf (accessed July 22, 2019).
35. Achenbach TM, McConaughy, SH, Ivanovaa, MY, Rescorla, LA,. Manual for the ASEBA Brief Problem Monitor TM for Ages 6-18 (BPM/6-18), Vol. 18 (2001). p. 13. Available online at: http://www.aseba.org/ASEBABriefProblemMonitor~Manual.pdf (accessed Feb 20, 2015).
36. Fleck MPA, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Aplicação da versão em português do instrumento de avaliação de qualidade de vida da Organização Mundial da Saúde (WHOQOL-100). Rev Saude Publica. (1999) 33:198–205. doi: 10.1590/S0034-89101999000200012
37. Pedroso B. Versão francesa da ferramenta para o cálculo dos escores e estatística descritiva do WHOQOL-bref através do Microsoft Excel. Rev Bras Qual Vida. (2014) 6:60–2. doi: 10.3895/S2175-08582014000100008
38. Cruz LN, Polanczyk CA, Camey SA, Hoffmann JF, Fleck MPA. Quality of life in Brazil: normative values for the Whoqol-bref in a southern general population sample. Qual Life Res. (2011) 20:1123–9. doi: 10.1007/s11136-011-9845-3
39. Iriart JAB, Nucci MF, Muniz TP, Viana GB, Aureliano W de A, Gibbon S. From the search for diagnosis to treatment uncertainties: challenges of care for rare genetic diseases in Brazil. Cienc Saude Coletiva. (2019) 24:3637–50. doi: 10.1590/1413-812320182410.01612019
40. Diene G, Mimoun E, Feigerlova E, Caula S, Molinas C, Grandjean H, et al. Endocrine disorder in children with Prader-Willi syndrome - data from 142 children of the French database. Horm Res Paediatr. (2010) 74:121–8. doi: 10.1159/000313377
41. Grugni G, Crinò A, Bosio L, Corrias A, Cuttini M, De Toni T, et al. The Italian national survey for Prader-Willi syndrome: an epidemiologic study. Am J Med Genet A. (2008) 146:861–72. doi: 10.1002/ajmg.a.32133
42. Sinnema M, Maaskant MA, van Schrojenstein Lantman-de Valk HMJ, Caroline van Nieuwpoort I, Drent ML, Curfs LMG, et al. Physical health problems in adults with Prader-Willi syndrome. Am J Med Genet A. (2011) 155:2112–24. doi: 10.1002/ajmg.a.34171
43. Tauber M, Diene G, Molinas C, Hébert M. Review of 64 cases of death in children with Prader-Willi syndrome (PWS). Am J Med Genet A. (2008) 146:881–7. doi: 10.1002/ajmg.a.32131
44. Vogels A, Van den Ende J, Keymolen K, Mortier G, Devriendt K, Legius E, et al. Minimum prevalence, birth incidence and cause of death for Prader-Willi syndrome in Flanders. Eur J Hum Genet. (2004) 12:238–40. doi: 10.1038/sj.ejhg.5201135
45. Driscoll DJ, Miller JL, Schwartz S, Cassidy SB. Prader-Willi Syndrome. In: GeneReviews(®). (2016). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK1330/ (cited October 18, 2016).
46. Brambilla P, Crinò A, Bedogni G, Bosio L, Cappa M, Corrias A, et al. Metabolic syndrome in children with Prader-Willi syndrome: the effect of obesity. Nutr Metab Cardiovasc Dis. (2011) 21:269–76. doi: 10.1016/j.numecd.2009.10.004
47. Grugni G, Crinò A, Bedogni G, Cappa M, Sartorio A, Corrias A, et al. Metabolic syndrome in adult patients with Prader-Willi syndrome. Nutr Metab Cardiovasc Dis. (2013) 23:1134–40. doi: 10.1016/j.numecd.2012.11.006
48. Heksch R, Kamboj M, Anglin K, Obrynba K. Review of Prader-Willi syndrome: the endocrine approach. Transl Pediatr. (2017) 6:274–85. doi: 10.21037/tp.2017.09.04
49. Cazzo E, Gestic AM, Utrini PM, Chaim DFM, Cândido EC, Jarolavsky LBS, et al. Bariatric surgery in individuals with severe cognitive impairment: report of two cases. São Paulo Med J. (2018) 136:84–8. doi: 10.1590/1516-3180.2016.0299071216
50. Franco RR, Fonoff ET, Alvarenga PG, Alho EJL, Lopes AC, Hoexter MQ, et al. Assessment of safety and outcome of lateral hypothalamic deep brain stimulation for obesity in a small series of patients with Prader-Willi syndrome. JAMA Netw Open. (2018) 1:1–9. doi: 10.1001/jamanetworkopen.2018.5275
51. Capodaglio P, Menegoni F, Vismara L, Cimolin V, Grugni G, Galli M. Characterisation of balance capacity in Prader-Willi patients. Res Dev Disabil. (2011) 32:81–6. doi: 10.1016/j.ridd.2010.09.002
52. Cimolin V, Galli M, Grugni G, Vismara L, Precilios H, Albertini G, et al. Postural strategies in Prader-Willi and Down syndrome patients. Res Dev Disabil. (2011) 32:669–73. doi: 10.1016/j.ridd.2010.11.017
53. Amaro AS, Teixeira MCVT, Mesquita MLG, Massoli GR, Rubin DA, Rodrigues LRC. Physiological adaptation after a 12-week physical activity program for patients with Prader-Willi syndrome: two case reports. J Med Case Rep. (2016) 10:1–6. doi: 10.1186/s13256-016-0966-8
54. Duran AT, Wilson KS, Castner DM, Tucker JM, Rubin DA. Association between physical activity and bone in children with Prader-Willi syndrome. J Pediatr Endocrinol Metab. (2016) 10:819–26. doi: 10.1515/jpem-2015-0233
55. Rubin DA, Wilson KS, Orsso CE, Gertz ER, Haqq AM, Castner DM, et al. A 24-week physical activity intervention increases bone mineral content without changes in bone markers in youth with PWS. Genes (Basel). (2020) 11:1–12. doi: 10.3390/genes11090984
56. Rubin DA, Wilson KS, Castner DM, Dumont-Driscoll MC. Changes in health-related outcomes in youth with obesity in response to a home-based parent-led physical activity program. J Adolesc Health. (2019) 65:323–30. doi: 10.1016/j.jadohealth.2018.11.014
57. Rubin DA, Wilson KS, Dumont-Driscoll M, Rose DJ. Effectiveness of a parent-led physical activity intervention in youth with obesity. Med Sci Sport Exerc. (2019) 51:805–13. doi: 10.1249/MSS.0000000000001835
58. Di Nuovo S, Buono S. Behavioral phenotypes of genetic syndromes with intellectual disability: comparison of adaptive profiles. Psychiatry Res. (2011) 189:440–5. doi: 10.1016/j.psychres.2011.03.015
59. Mesquita MLG de, Suriano R, Carreiro LRR, Teixeira MCTV. Treino parental para manejo comportamental de crianças com Síndrome de Prader-Willi: impacto sobre a saúde mental e práticas educativas do cuidador. Rev CEFAC. (2016) 18:1077–87. doi: 10.1590/1982-021620161850516
60. Aycan Z, Baş VN. Prader-Willi syndrome and growth hormone deficiency. J Clin Res Pediatr Endocrinol. (2014) 6:62–7. doi: 10.4274/jcrpe.1228
61. Bacheré N, Diene G, Delagnes V, Molinas C, Moulin P, Tauber M. Early diagnosis and multidisciplinary care reduce the hospitalization time and duration of tube feeding and prevent early obesity in PWS infants. Horm Res. (2008) 69:45–52. doi: 10.1159/000111795
62. Grolla E, Andrighetto G, Parmigiani P, Hladnik U, Ferrari G, Bernardelle R, et al. Specific treatment of Prader-Willi syndrome through cyclical rehabilitation programmes. Disabil Rehabil. (2011) 33:1837–47. doi: 10.3109/09638288.2010.549288
63. Nardella MT, Sulzbacher SI, Worthington-Roberts BS. Activity levels of person with Prader-Willi syndrome. Am J Ment Defic. (1983) 87:498–505.
64. Eiholzer U, Nordmann Y, L'Allemand D, Schlumpf M, Schmid S, Kromeyer-Hauschild K. Improving body composition and physical activity in Prader-Willi syndrome. J Pediatr. (2003) 142:73–8. doi: 10.1067/mpd.2003.mpd0334
65. Schlumpf M, Eiholzer U, Gygax M, Schmid S, van der Sluis I, l'Allemand D. A daily comprehensive muscle training programme increases lean mass and spontaneous activity in children with Prader-Willi syndrome after 6 months. J Pediatr Endocrinol Metab. (2006) 19:65–74. doi: 10.1515/JPEM.2006.19.1.65
66. Donnelly JE, Hillman CH, Castelli D, Etnier JL, Lee S, Tomporowski P, et al. Physical activity, fitness, cognitive function, and academic achievement in children: a systematic review. Med Sci Sports Exerc. (2016) 48:1197–222. doi: 10.1249/MSS.0000000000000901
67. Butler J V, Whittington JE, Holland AJ, Boer H, Clarke D, Webb T. Prevalence of, and risk factors for, physical ill-health in people with Prader-Willi syndrome: a population-based study. Dev Med Child Neurol. (2002) 44:248–55. doi: 10.1017/S001216220100202X
68. Butler MG, Matthews NA, Patel N, Surampalli A, Gold J, Khare M, et al. Impact of genetic subtypes of Prader-Willi syndrome with growth hormone therapy on intelligence and body mass index. Am J Med Genet A. (2019) 179:1826–35. doi: 10.1002/ajmg.a.61293
69. Quaio CRDC, Ferreira De Almeida T, Albano LMJ, Gomy I, Bertola DR, Varela MC, et al. A clinical follow-up of 35 Brazilian patients with Prader-Willi Syndrome. Clinics. (2012) 67:917–21. doi: 10.6061/clinics/2012(08)11
70. Varela MC, Kok F, Setian N, Kim CA, Koiffmann CP. Impact of molecular mechanisms, including deletion size, on Prader-Willi syndrome phenotype: Study of 75 patients. Clin Genet. (2005) 67:47–52. doi: 10.1111/j.1399-0004.2005.00377.x
71. Lukoshe A, Hokken-Koelega AC, Van Der Lugt A, White T. Reduced cortical complexity in children with prader-willi syndrome and its association with cognitive impairment and developmental delay. PLoS One. (2014) 9:e107320. doi: 10.1371/journal.pone.0107320
72. Lukoshe A, White T, Schmidt MN, van der Lugt A, Hokken-Koelega AC. Divergent structural brain abnormalities between different genetic subtypes of children with Prader-Willi syndrome. J Neurodev Disord. (2013) 5:31. doi: 10.1186/1866-1955-5-31
73. Roux-Levy PH, Bournez M, Masurel A, Jean N, Chancenotte S, Bordes M, et al. Associations between cognitive performance and the rehabilitation, medical care and social support provided to French children with Prader-Willi syndrome. Eur J Med Genet. (2020) 63:104064. doi: 10.1016/j.ejmg.2020.104064
74. Ragusa L, Crinò A, Grugni G, Reale L, Fiorencis A, Licenziati MR, et al. Caring and living with Prader-Willi syndrome in Italy: integrating children, adults and parents' experiences through a multicentre narrative medicine research. BMJ Open. (2020) 10:1–11. doi: 10.1136/bmjopen-2019-036502
Keywords: Prader-Willi syndrome, obesity, treatment, quality of life, behavior problems
Citation: Amaro AS, Rubin DA, Teixeira MCTV, Ferreira AJ Jr, Rodrigues GM and Carreiro LRR (2022) Health Problems in Individuals With PWS Are Associated With Lower Quality of Life for Their Parents: A Snapshot in the Brazilian Population. Front. Pediatr. 10:746311. doi: 10.3389/fped.2022.746311
Received: 23 July 2021; Accepted: 03 January 2022;
Published: 15 February 2022.
Edited by:
Angele Consoli, Assistance Publique Hopitaux De Paris, FranceReviewed by:
Sung Yoon Cho, Sungkyunkwan University, South KoreaTheresa V. Strong, Foundation for Prader-Willi Research, United States
Copyright © 2022 Amaro, Rubin, Teixeira, Ferreira, Rodrigues and Carreiro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandre Slowetzky Amaro, YWxlc2xvd2V0emt5QGdtYWlsLmNvbQ==