 Amy K. Connery1*
Amy K. Connery1* Radhika S. Raghunathan2
Radhika S. Raghunathan2 Alison M. Colbert1Laszlo Erdodi3Seth Warschausky4Alissa Huth-Bocks5H. Gerry Taylor6
Alison M. Colbert1Laszlo Erdodi3Seth Warschausky4Alissa Huth-Bocks5H. Gerry Taylor6 Trivellore Raghunathan7Patricia Berglund7
Trivellore Raghunathan7Patricia Berglund7 Angela D. Staples8Angela Lukomski9Jazmine Kirkland5Jennifer Cano8Renee Lajiness-O’Neill4,8the PediaTrac Project Consortium**
Angela D. Staples8Angela Lukomski9Jazmine Kirkland5Jennifer Cano8Renee Lajiness-O’Neill4,8the PediaTrac Project Consortium**
- 1Children’s Hospital Colorado, Department of Physical Medicine and Rehabilitation, University of Colorado School of Medicine, Aurora, CO, United States
- 2Department of Mental Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States
- 3Psychology, University of Windsor, Ontario, ON, Canada
- 4Physical Medicine and Rehabilitation, Michigan Medicine, Ann Arbor, MI, United States
- 5Pediatrics, Case Western Reserve University, University Hospitals, Cleveland, OH, United States
- 6Abigail Wexner Research Institute at Nationwide Children’s Hospital, and Pediatrics, The Ohio State University, Columbus, OH, United States
- 7Institute of Social Research, University of Michigan, Ann Arbor, MI, United States
- 8Psychology, Eastern Michigan University, Ypsilanti, MI, United States
- 9Nursing, Eastern Michigan University, Ypsilanti, MI, United States
Caregiver report is the most feasible way to assess early childhood development but is susceptible to the influences of response style and sociodemographic factors. In a sample of 571 caregiver-infant dyads (47.8% female; 48% White), we compared caregiver reports on the Ages and Stages Questionnaire-Third Edition (ASQ-3) with reports on a novel, web-based assessment, PediaTrac™. Ratings on PediaTrac correlated with ratings on the ASQ-3 at all time points (2, 4, 6, and 9 months). Caregiver age, response style, and sociodemographic factors accounted for significant variance on both measures. Developmental reporting of early childhood skills is influenced by caregiver response style and sociodemographic factors. These influences must be considered in order to ensure the accurate identification of infant developmental status.
1. Introduction
While there is widespread consensus that the identification of and early intervention for childhood developmental delays can improve outcomes and prevent long-term problems (1, 2), there are limited reliable and valid methods available for detecting these delays within the first two years of life (3). Reliable methods of assessing children during infancy and early toddlerhood are needed to improve developmental surveillance and better target interventions (4, 5).
Tests of early developmental skills with strong psychometric properties do exist (6, 7). While these performance-based tests are often considered to be the “gold standard,” they are costly, time and resource-intensive and require specialized personnel for administration and interpretation (8). Typically, these tests are not feasible in the context of well child medical visits, routine developmental monitoring programs, and large-scale research projects. Moreover, they are often only available to children already identified as “at risk” and to children living in more urban, or highly resourced areas.
A more feasible method of developmental monitoring and assessment is caregiver (e.g., parent) report. Caregiver report is commonly used in pediatric well child visits and developmental outcome research (4, 5). Research outcomes and conclusions, as well as decisions by primary care providers to refer children for further assessment or interventions, are frequently based on caregiver reports and governmental and educational institutions utilize these types of metrics for financial and programming decisions (9). However, these tools are not without limitations, and these shortcomings are frequently underestimated, underappreciated or not considered in clinical and policy decision making and research, leading to increased measurement error at the individual level and group misassignment in research designs (8).
While caregiver reports can assess a wide spectrum of child behaviors observed in daily life by adults who spend substantial time with the child, these reports can be subject to bias. Factors contributing to bias include differing levels of caregiver knowledge about typical and atypical development (9, 10), concerns about stigmatization (11, 12) and cultural differences in what constitutes normal and abnormal development (12–14). High levels of caregiver stress can also influence reports of a child's developmental status (15, 16). Some caregiver report measures available for children over 2 years of age include embedded measures of response style (17, 18). However, these metrics are not routinely available and, to our knowledge, have not been included in any caregiver report of infant and toddler development (6, 19, 20).
In addition to response style, caregiver reports are also influenced by sociodemographic factors. While one might anticipate that children with less socioeconomic advantage [e.g., lower levels of caregiver education or other indices of socioeconomic status (SES)] would receive less favorable developmental ratings than those from more advantaged backgrounds, findings from several studies fail to confirm this expectation. Two studies found that caregivers with lower levels of education tended to rate their children higher on a developmental language inventory than those with higher levels of education (21, 22). Several other studies have also shown that caregivers with lower SES may tend to rate their child's abilities more favorably than those from higher SES backgrounds (23–27). These findings are theorized to be due to concern about the child “failing” the measure, avoidance of stigmatization, differing levels of knowledge about early development or developmental expectations, or cultural differences in interpretation of item content. Despite these findings, there is no early developmental assessment tool that is capable of systematically accounting for sociodemographic factors in score interpretation.
Some researchers have suggested that caregiver report is not sufficiently sensitive or specific to early signs of delayed development to justify its widespread use (8, 28, 29); however, a recent investigation suggests that caregivers of term and preterm infants can report newborn motor abilities with high reliability (30). Data that are inaccurate can lead to diagnostic errors, the over- or under-identification of children in need, or misleading data for financial or policy programming. However, as caregiver report is likely the most feasible, cost and time efficient way to identify children early, as well as the vital nature of early identification and intervention, further efforts are warranted to improve the accuracy of this method of early developmental assessment.
PediaTrac™, is a multi-dimensional, online survey tool constructed with contemporary item response theory (IRT) modeling methods to monitor and track infant and toddler development (30). PediaTrac queries caregivers about their child's development at multiple time points, measures caregiver response style, and gathers additional information known to influence caregiver report, including sociodemographic factors.
The current study focused on assessment of early social, communication, and cognitive skills. These domains were selected based on their greater sensitivity to caregiver characteristics and response style. Specifically, research has shown that caregiver report of language and cognitive functioning may be more subjective than more directly observable domains, such as motor skills (31–33).
In order to examine the impact of response style and sociodemographic characteristics on caregiver report, we first attempted to establish that PediaTrac, a recently developed measure, was measuring early childhood developmental constructs in the same manner as another established and widely used caregiver report measure. To establish convergent validity, we compared the PediaTrac Social/Communication/Cognition domain (SCG) to comparable scales of the Ages and Stages Questionnaire-Third Edition (ASQ-3; Personal-Social, Communication, and Problem Solving). We hypothesized that the convergent validity of the PediaTrac SCG domain would be demonstrated by its association with caregiver ratings on the three ASQ-3 scales. We then hypothesized that significant variance in caregiver report on both measures would be accounted for by sociodemographic factors (i.e., maternal age and education level) and caregiver response style.
2. Methods
2.1. Participants
This investigation is part of the larger PediaTrac study, a prospective, longitudinal investigation of a sample of 571 caregivers of infants (48% female) who were born either at term (n = 331; 49% female) or preterm (n = 240; 46% female) (30). The sample was recruited from three sites that included academic medical centers and a local community clinic: 100 from Site #1, 239 from Site #2, and 232 from Site #3. Site #1 did not have access to a preterm sample and recruited only term caregiver/infant dyads from an urban academic medical center and a socio-demographically high-risk community clinic to ensure representation of systematically excluded communities in our larger term sample. Sites #2 and #3 were large academic medical centers from which both term and preterm infants were recruited, the latter from which also a socio-demographically high-risk population was recruited. Term infants had a gestational age (GA) of ≥37 weeks at birth and a minimum birth weight of 2500 g, with no history of prenatal or intrapartum complications, neonatal abstinence syndrome, neurological injury/disease, or known genetic disorder. Preterm infants had a GA of <37 weeks. Birth weight was allowed to vary, but exclusions from the preterm group included neonatal abstinence syndrome and Down syndrome. A single infant from each multiple birth was randomly selected for enrollment. Caregivers were a minimum of 18 years old and had access to a personal device such as a smartphone, tablet, or computer. Ninety-eight percent of the respondents were biological mothers. English-language proficiency was required for participation. All American Psychological Association (APA) ethical guidelines were followed and Institutional Review Board (IRB) approval was obtained.
2.2. Study procedures
Caregivers were recruited in their last trimester of pregnancy, after their infants' birth in the hospital, or at their first newborn visit, with consent obtained after birth. Primary caregivers of term infants completed PediaTrac soon after birth, whereas caregivers of preterm infants completed it when their infants reached a postmenstrual age of 39 weeks. Sampling periods were thus based on the corrected age for preterm infants.
2.3. Study measure and variables
PediaTrac v3.0 is a web-based survey comprised of between 511 and 558 unique items covering the age range from birth to 18 months (30). Information describing the original item bank and domain development, expert panel reviews, interviews with caregivers, and the pilot validation results of PediaTrac 2.0 have been previously published (34). In PediaTrac v3.0, caregivers complete subsets of the survey ranging from ∼220–340 items, depending on the sampling period of the assessment. PediaTrac queries multiple developmental domains, including Feeding/Eating/Elimination, Sleep, Motor, Social/Communication/Cognition (SCG), Early Relational Health and Social/Sensory Information Processing, at each of 8 sampling periods [newborn (NB) and 2, 4, 6, 9, 12, 15, and 18 months].
PediaTrac has been developed using item response theory (IRT) methodology, which is a measurement framework that uses mathematical models to explain the relationship between latent traits (attributes) and their observed outcome. IRT models the likelihood of a given response to an item as a probabilistic function of the individual's score on a latent trait of interest, referred to as theta (35). IRT offers benefits over classical test theory (CTT) including sample-invariant parameter estimates (i.e., assuming no differential item functioning across populations) to metrics of reliability at both the item and test level (36–38). It is an item-oriented rather than a test-oriented test construction method. As such, it lends itself to an individualized medicine approach in assessment and subsequent care.
The focus of this investigation is on the SCG domain across 2, 4, 6, and 9 month sampling periods. IRT modeling was used to estimate theta (θ), an index of the latent trait of social/communication/cognition, for each infant at each period using the SCG domain items (35, 39). Mean theta values are on a scale similar to a z-score; a distribution centered at zero with a standard deviation metric (40). Reliability estimates ranged from .97 to .99 across all time periods and the dimensionality of the items at each sampling period has been established via exploratory factor analyses (under review).
Survey questions about sociodemographic characteristics, including maternal age and level of education, were completed during the NB period, with relevant information updated at all subsequent assessments. The degree of neighborhood deprivation was also calculated for all participants using the 2018 Area Deprivation Index (ADI), which is a validated, neighborhood-level composite of 17 education, employment, housing-quality, and poverty variables extracted from the American Community Survey and US Census Survey data (41). The ADI is represented as a state decile ranking score ranging from 1 to 10, with the least resourced neighborhoods, or census block groups, characterized by higher scores and the most resourced by lower scores.
Thirty-two validity items were specifically developed for PediaTrac to help assess response style and ensure that any variabilities in responding, if present, are accounted for in the prediction models. Validity items target three potential sources of distortion: atypical responding (ATP; previously referred to as random or RND), positive (PRS) and negative (NRS) response style. Atypical responding is operationalized as unusual endorsement of statements that have an obvious answer. The logic behind the ATP scale is that all bona fide examinees who are literate, proficient in English and attend to item content should be able to choose the one correct option. The NRS scale consists of items that provide an evaluative statement of the infant in the negative direction (i.e., indicating harsh judgment or an overly pessimistic outlook on the child's future). Conversely, the PRS scale consists of items that provide an evaluative statement of the infant in the positive direction (i.e., indicating unrealistically positive opinion or an overly optimistic outlook on the child's future). Caregivers were required to respond to a 5-point Likert scale with response anchors as follows: 1 = never; 2 = rarely; 3 = sometimes; 4 = often; 5 = always. Whether a given validity item endorsement was indicative of non-credible responding was determined based on the frequency of that response in the sample. If <10% of the individuals endorsed the item, it was considered invalid (i.e., strong evidence of non-credible responding). Items were scaled such that higher scores represented increased deviation from a more typical response pattern (42).
The Ages and Stages Questionnaire (ASQ-3) is a caregiver report for children 1–66 months of age and is one of the most widely used developmental caregiver instruments (20). The ASQ-3 is comprised of five scales (Communication, Gross Motor, Fine Motor, Problem Solving, and Personal-Social) as assessed using 21 questionnaires, one for each 2 to 3 month age interval. For the purpose of the current project, only Communication, Problem Solving, and Personal-Social scales were utilized in the analyses given that the content of these scales most logically maps to the SCG domain of PediaTrac. The ASQ-3 provides cut-off scores that designate either no concerns, the need for monitoring, or the need for further assessment. However, for the purposes of the current study, ASQ-3 scores were converted to z-scores based on means and standard deviations reported in the administration manual. For infants born preterm, caregivers completed the age-corrected ASQ-3 measure.
2.4. Statistical analyses
2.4.1. Preliminary analyses
Descriptive and exploratory analyses were conducted to examine the impact of covariates such as demographic (i.e., caregiver age at study enrollment) and sociodemographic characteristics (i.e., caregiver education, ADI), and social/communication/cognition theta values and ASQ z-scores for Communication, Problem Solving, and Personal-Social scales at the 2, 4, 6, and 9 month sampling periods.
2.4.2. Main analysis
First, to demonstrate convergent validity between the established scales of the ASQ-3 and the PediaTrac SCG domain, Pearson correlation coefficients were computed to examine the relationships between caregiver-reported social/communication/cognitive skills using the PediaTrac SCG domain thetas and z-scores for the ASQ-3 scales at each sampling period. This was a necessary first step in order to ensure that the possible effects of sociodemographic and response style could be validly interpreted as impacting related outcomes and caregiver report generally.
Second, and the primary aim of the investigation, to examine the role of sociodemographic variables and caregiver response style on SCG domain theta and ASQ-3 scales, separate cross-sectional linear regression models were conducted at each sampling period. Caregiver response styles (positive, negative or random) were the predictors in the regression models and the SCG domain thetas and z-scores for the ASQ-3 scales were the outcomes. All models were adjusted for sociodemographic characteristics (i.e., caregiver age, infant age, ADI), as well as caregiver race, which was dichotomized given that it was a categorical variable and the nature of the analyses (Black vs. non-Black and White vs. non-White). Infant age in weeks (uncorrected for premature infants) was used in analysis of age effects to obtain a more precise estimate than would be possible using sampling period as a proxy for age. Post hoc partial correlations were used to examine whether the relationship between caregiver response style and PediaTrac (SCG domain theta) outcomes were moderated by SES, for linear regression models that showed significant main effects.
3. Results
3.1. Sample characteristics
The current study sample included 571 caregivers-infant dyads. Caregivers had a mean (standard deviation) age of 30.1 (6.04) years; 53.5% were married; and 76.7% had some college or higher education. Forty-eight percent of the infants were female, 58% were born full-term, and 34% were African American/Black. See Table 1 for descriptive statistics for the full sample.
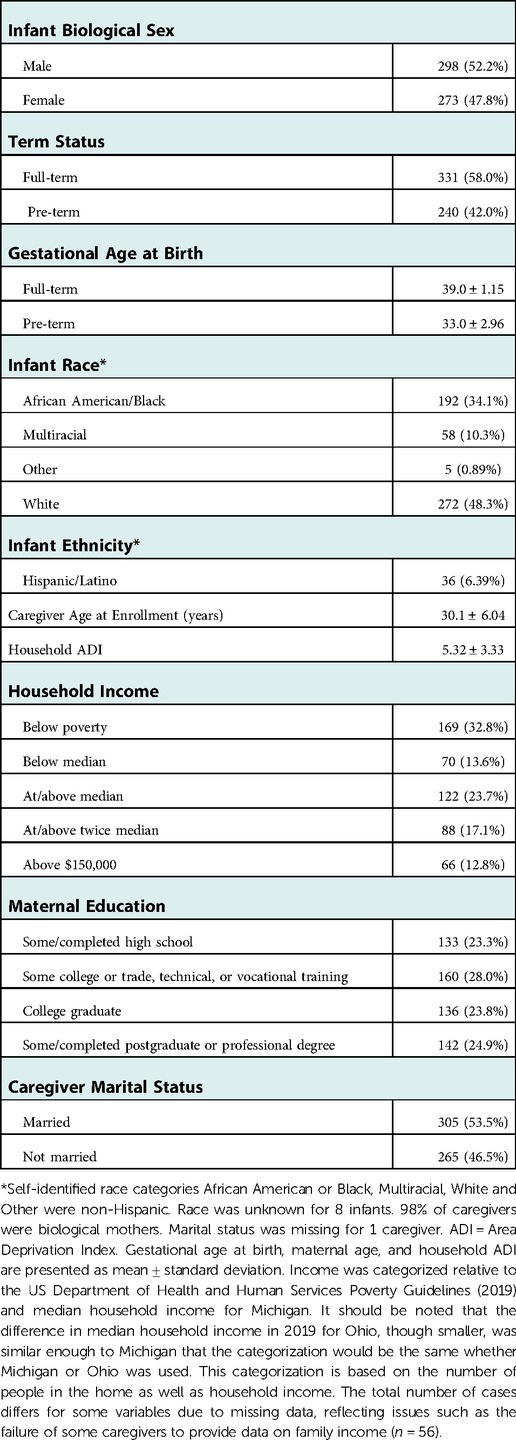
Table 1. Pooled demographics and characteristics of infants and caregivers.
Table 2 reports descriptive statistics of the SCG domain theta scores and ASQ-3 domain z-scores. Regarding interpretation of the response style scales, the cutoff associated with the top 5% of the distribution (i.e., most deviant scores) for the PRS, NRS, and ATP response styles are ≥7, 5, and 5, respectively. The base rates of “failure” (%) on the PRS, NRS, and ATP scales at these cutoffs was 9.1, 5.8, and 8.0, respectively.
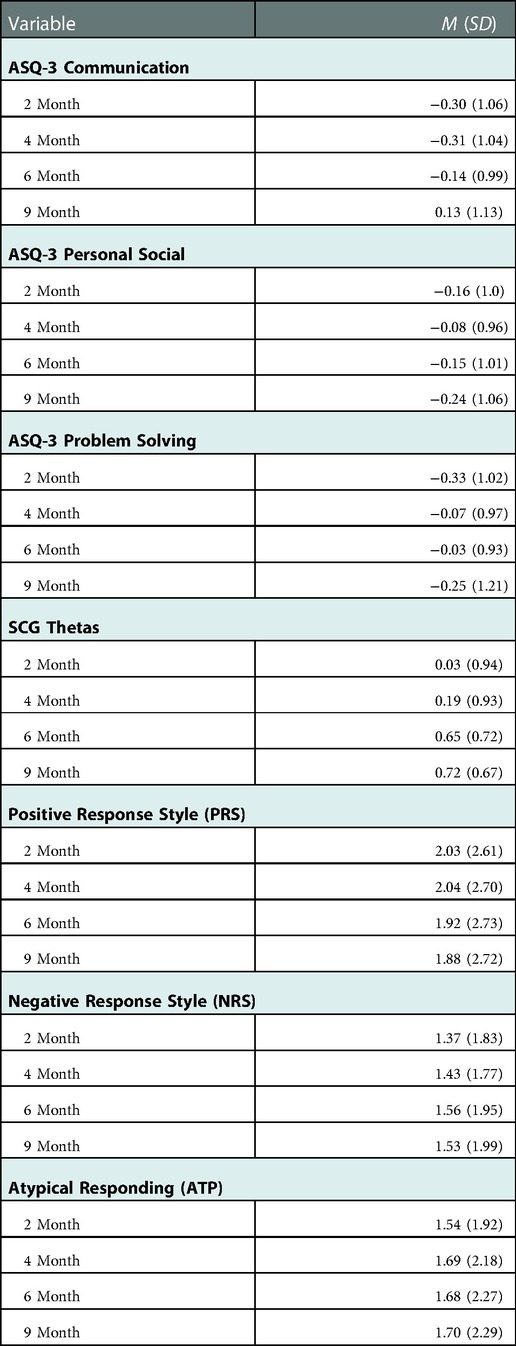
Table 2. ASQ-3, SCG theta, and caregiver response styles means and standard deviations.
3.2. Bivariate Relationship between SCG domain theta and ASQ-3 domain z-score
SCG domain theta scores were significantly positively correlated across all sampling periods with z-scores for ASQ-3 Communication (rs range .41–.53), Personal-Social (rs range .33–.44), and Problem Solving (rs range .34–.36) scales. See Table 3.
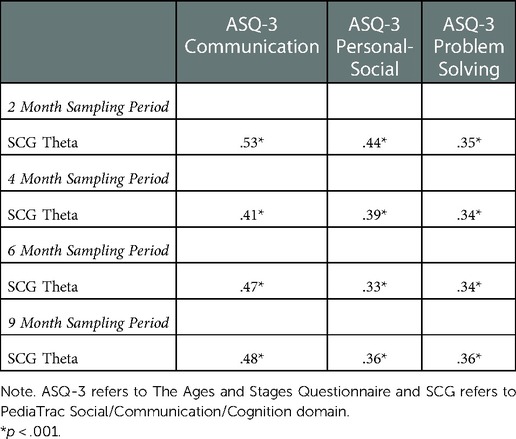
Table 3. Pearson correlation coefficients between SCG thetas and ASQ-3 domains at each sampling period .
3.3. Multivariable linear regression models
Separate multivariable linear regression models were run to examine the impact of sociodemographic variables and caregiver response style on SCG domain theta and ASQ-3 scales at each sampling period. All models included maternal education, maternal age, maternal race, infant age, and ADI state rank, in addition to the three caregiver response styles (NRS, PRS, ATP). Overall model results and significant associations are detailed below, full results are in Table 4.
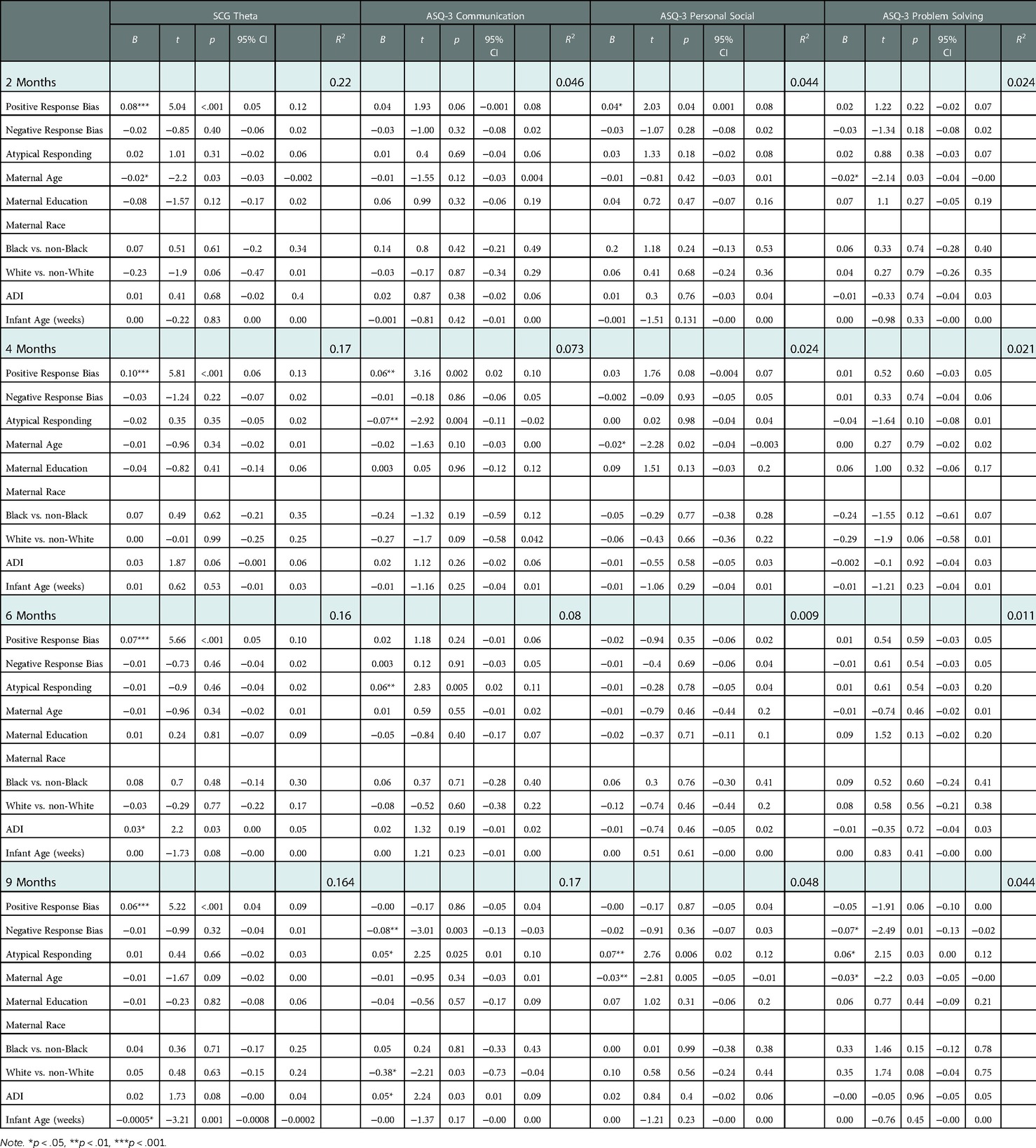
Table 4. Results of multivariate linear regression models examining caregiver response styles and sociodemographic factors on SCG and ASQ-3 domains.
3.3.1. Caregiver response styles
NRS and ATP were not significantly associated with the SCG domain thetas at any sampling period. However, at 9 months for ASQ-3 Communication and Problem Solving, overall models indicated that NRS and ATP explained a significant moderate to large proportion of variance, R2 = .17, F(9, 425) = 9.66, p < .001, and R2 = .04, F(9, 423) = 2.17, p = .02, respectively, with maternal age also explaining a significant proportion of variance in ASQ-3 Problem Solving at 9 months. NRS was significantly negatively associated with ASQ-3 Communication and Problem Solving at 9 months (b = −.08, t = −.30, p = .003 and b = −.07, t = −2.49, p = .01, respectively), indicating that higher negative perceptions of infants were associated with lower reported ASQ-3 communication and problem solving abilities.
In addition, at 9 months, the overall model for ASQ-3 Personal Social indicated that ATP and maternal age explained a moderate significant proportion of variance, R2 = .05, F(9, 424) = 2.4, p = .01. As such, at 9 months, ASQ-3 Communication, Personal Social and Problem-Solving z-scores were positively significantly associated with ATP (b = .05, t = 2.25, b = .07, t = 2.76, and b = .06, t = 2.15, respectively; all ps < .01), indicating that higher random responding was related to higher reported communication, personal-social and problem-solving skills at 9 months. See Table 4 for details.
The overall model for ASQ-3 Communication at 4 months indicated that both ATP and PRS at 4 months explained a significant moderate proportion of variance, R2 = .07, F(9, 472) = 4.11, p < .001. Here, ATP was inversely significantly associated with ASQ-3 Communication at 4 months (b = −.07, t = −2.92, p = .004), suggesting that higher random responding was related to lower reported communication at 4 months.
All SCG domain models indicated that PRS explained a significant moderate to large proportion of variance, R2 range = .16–.22, ps < .001. In addition, overall models indicated that PRS explained a small but significant proportion of variance in ASQ-3 Personal-Social model at 2 months, R2 = .04, F(9, 482) = 2.45, p = .01, and significant moderate proportion of variance in ASQ-3 communication at 4 months R2 = .07, F(9, 472) = 4.11, p < .001. In these models, PRS was significantly positively associated with SCG domain thetas at all sampling periods (bs range .06–.10, ps < .001), ASQ-3 Personal-Social at 2 months (b = .04, t = 2.03, p = .04) and ASQ-3 Communication at 4 months (b = .06, t = 3.16, p = .002), indicating that higher positive perceptions of their infants were related to higher reported PediaTrac social/communication/cognition abilities and ASQ-3 personal-social and communication skills at 2 and 4 months.
3.3.2. Sociodemographic associations
Caregiver age, along with PRS, explained a significant large proportion of variance in the SCG domain theta models at 2 months, R2 = .22, F(9, 512) = 15.9, p < .001. Caregiver age, although significantly associated with ASQ-3 Personal-Social at 4 months, did not explain a significant proportion of variance in the model, R2 = .02, F(9, 471) = 1.32, p = .22, but did account for significant moderate proportion of variance, along with ATP, at 9 months, R2 = .04, F(9, 424) = 2.40, p = .01. Caregiver age, although significantly associated with ASQ-3 Problem Solving at 2 months, did not explain a significant proportion of variance in the model, R2 = .02, F(9, 480) = 1.32, p = .23, but did account for a significant moderate proportion of variance at 9 months, R2 = .04, F(9, 423) = 2.17, p = .02.
Caregiver age was significantly inversely associated with SCG domain thetas at the 2 month sampling period, with younger caregivers reporting higher infant social/communication/cognition skills (b = −.02, t = −2.2, p = .03). Caregiver age also significantly inversely correlated with ASQ-3 Personal-Social at 4 and 9 months, with younger caregivers reporting higher ASQ-3 Personal-Social skills (b = −.02, t = −2.28, p = .02 and b = −.03, t = −2.81, p < .001, respectively). Similarly, caregiver age was significantly inversely correlated with ASQ-3 Problem Solving scores at 2 (b = -.02, t = −2.14, p = .03) and 9 (b = -.03, t = −2.2, p = .03) months, with younger caregivers reporting higher infant problem solving abilities at 2 and 9 months of age.
With respect to other sociodemographic factors, results of adjusted multivariable regression models indicated caregiver race, along with ATP and NRS, accounted for a significant large proportion of variance in ASQ-3 Communication scores at 9 months, R2 = .17, F(9, 425) = 9.66, p < .001. Here, non-White caregivers reported higher ASQ-3 Communication scores at 9 months compared to White mothers only (b = −.38, t = −2.21, p = .03).
Further, the SCG model at 6 months indicated that ADI, along with PRS explained a significant large proportion of variance, R2 = .16, F(9, 489) = 10.70, p < .001, such that higher ADI was positively correlated with SCG domain thetas (b = .03, t = 2.2, p = .03) at 6 months. Similarly, ADI, along with NRS, ATP, and caregiver race, explained a significant and large proportion of variation in ASQ-3 Communication scores at 9 months, R2 = .17, F(9, 425) = 9.66, p < .00; with lower negative response bias, higher atypical responding, non-white race, and higher levels of education noted in infants with higher reported ASQ-3 Communication (b = .05, t = 2.24, p = .03) at 9 months.
Finally, preterm birth (i.e., as measured by weeks since date of birth), along with PRS, explained a significant large proportion of variance in SCG theta at 9 months, R2 = .16, F(9, 475) = 10.10, p < .001. Preterm birth was related to lower SCG theta values at the 9 month sampling period (b = −.0005, t = 3.21, p = .001) in the adjusted regression model. That is, the more preterm the infant was at testing, the lower their SCG abilities were rated, despite administration of the age-corrected version of the test. Preterm birth was not associated with lower ASQ-3 domains in any sampling period.
3.3.3. Post-hoc analyses
To further explore the significant relationship between SCG domain thetas, PRS and sociodemographic characteristics, post-hoc partial correlations were computed for models with significant main effects from the multivariate linear regression analyses.
At all sampling periods, a significant amount of variance (rs range = .30–.35) remained between SCG domain theta and PRS, after accounting for the effects of sociodemographic variables (i.e., caregiver education, ADI, infant age). However, the correlation between PRS and infant age (uncorrected for premature infants) at the 9 month sampling period was not significant when accounting for the main effect of SCG domain theta (partial r = −.06, p = .15); and PRS and infant age were not correlated when accounting for the relationship between PRS and SCG domain theta.
Significant main effects for caregiver response patterns and sociodemographic characteristics were found for the ASQ-3 Communication domain at 9 months. Therefore, partial correlations were computed to examine the associations of ASQ-3 Communication at 9 months with NRS and ATP, accounting for the main effects of maternal race (White vs. non-White (i.e., Black or African American, multiracial) and ADI. Caregiver race (White vs. non-White) was unrelated to ASQ-3 Communication domain after removing the effects of NRS (partial r = −.33, p = .11). Similarly, ADI was unrelated to ASQ-3 Communication at 9 months after removing the effects of NRS (partial r = .31, p = .09). Additionally, maternal race (White vs. non-White) and ADI were unrelated to ASQ-3 Communication after accounting for the effects of ATP at 9 months (partial rs = −.31 and.30, ps < .10 for maternal race and ADI, respectively). Associations of ASQ-3 Communication with NRS or ATP at 9 months remained significant even after accounting for maternal race or ADI in respective partial correlations.
4. Discussion
As expected, convergent validity was established between the Social/Communication/Cognition domain of the recently developed PediaTrac, with theta scores consistently and positively correlated with the derived z-scores of the Personal-Social, Communication, and Problem Solving scales of the more widely used and established ASQ-3 at the 4, 6, and 9 month sampling periods. Caregiver response style, maternal age, and level of neighborhood deprivation, accounted for significant variance in outcomes on both measures, demonstrating the importance of inclusion of these variables on newly developed measures, as well as for measures already in widespread use.
While the base rates of caregiver positive, negative or atypical response styles were low in the overall sample, these response tendencies accounted for significant variance in the ASQ-3 and PediaTrac caregiver ratings of infant development. PRS accounted for significant variance in caregiver ratings on the PediaTrac SCG domain at all sampling periods and on one ASQ-3 scale at a single sampling period. In contrast, although NRS and ATP were unrelated to PediaTrac caregiver-reported social/communication/cognitive development, both measures of response style were associated ASQ-3 at one or more sampling periods. Maternal age and area deprivation were also associated with PediaTrac and ASQ-3 scores, such that being a younger caregiver and living in an area with more socioeconomic deprivation were associated with caregiver ratings of better infant developmental ability. ASQ-3 Communication scores were also higher for infants of caregivers who identified as non-White compared to those identified as White but only at one sampling period.
Some studies have found that performance-based assessments yield higher rates of developmental problems than caregiver report, suggesting under-identification of these problems based on caregiver report only (43). Prior research has identified at least two factors that can compromise the validity of caregiver report including response style (44) and sociodemographic factors (10, 12, 45). However, to our knowledge no existing caregiver report of early development considers these factors in interpreting caregiver ratings. The findings of this study demonstrate the importance of considering these factors into caregiver report and accounting for them in drawing conclusions about children's actual level of developmental functioning.
Because response style and sociodemographic information are not typically incorporated into screening measures of early infant development, normative reference groups may not provide accurate estimates of an individual child's abilities. The absence of objective metrics on response style may also lead to the misidentification of children and to inaccurate estimated of the base rates of developmental problems in young children. The possibility of misidentification of developmental problems is particularly urgent in view of the fact that caregiver report is typically the only feasible method for formally assessing an infant's developmental status and milestone acquisition as part of pediatric well child visits. Integrating reporter response style and sociodemographic characteristics into the most commonly used assessments is thus well justified as a means for improving the accuracy of these reports. Inclusion of measures of response bias is also consistent with the need for accurate and systematic early childhood developmental surveillance systems (4, 5).
The present study has several noteworthy limitations. First, although caregiver reports were collected longitudinally through 24 months of age, the current investigation focused on cross-sectional findings during early infancy, limiting our ability to examine potential differences in the nature and implications of response styles and sociodemographic factors across a wide span of early childhood development (46). Additionally, the study design of PediaTrac excluded caregivers under 18 years of age, which may have limited our ability to capture the full range of influence of younger caregiver age on caregiver report. Lastly, restriction of the study sample to caregivers with English language proficiency and functional literacy skills may also have restricted our ability to identify the full range of sociodemographic influences on caregiver reporting.
5. Future directions
The present study demonstrates the need to take caregiver response styles and sociodemographic factors into account in interpreting caregiver ratings of infant development. Although additional investigation of the effects of these factors on caregiver ratings is planned as part of the larger PediaTrac study, further research is needed to better understand the factors that contribute to variations in response style. A deeper understanding of the reasons for the different ways in which caregivers approach child developmental reporting and an understanding of how persons from various backgrounds approach caregiver questionnaires would allow for more inclusive screening of infants and improve the accuracy of these data.
The development of PediaTrac continues as an ongoing longitudinal, multi-site investigation. To reduce burden and enhance utilization and clinical acceptance, we anticipate designing an adaptive [i.e., computer adaptive test (CAT)] version of PediaTrac that caregivers can complete on an iPad or other digital source that can be integrated into the electronic medical record (EMR) system, and for which trajectories of development can be visualized in real-time. The investigators are currently using a host of data analytic methods to develop complex algorithms for which socio-demographic and response style sources of variation can be corrected or systemically accounted for at the time of assessment so that more precise and individualized estimates of infant or toddler developmental status (e.g., motor, social/communication cognition, sleep, etc.) can be obtained.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Multi-site reliant IRB at the University of Michigan. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
On Behalf Of
**PediaTrac Project Consortium
Casey Swick1, Samantha Goldstein1, Michelle Lobermeier1, Amanda Hicks1, Natasha Lang1, Gabrielle LeDoux1, Shannon Franz2, Najae Dixon2, Kirsten Oard2, Katherine Rosenblum3, John Barks4, Lesa Dieter5, Jazmine Kirkland5, Yanisa Robbins5 and Emily Gorjanc5
1Psychology, Eastern Michigan University, MI, United States
2Physical Medicine and Rehabilitation, University of Michigan, MI, United States
3Department of Psychiatry, University of Michigan, MI, United States
4Department of Pediatrics, University of Michigan, MI, United States
5Pediatrics, Rainbow Babies & Children's Hospital, Case Western Reserve University, OH, United States
Author contributions
AKC, RSR, AMC, RL-O: conceptualization, data curation, analysis, writing. RL-O, LE, SW, AH-B, HGT, AL: funding acquisition, project administration, review and editing. TR: funding acquisition, data curation, formal analysis. AS, JC, PB, JK: data curation and analysis. PediaTrac Project Consortium: validation, data curation. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number (R01HD095957). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. SW effort also was supported in part by the Mildred E. Swanson Foundation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that couldbe construed as a potential conflict of interest.
The reviewer AR declared a shared parent affiliation with the authors SW, TR, PB to the handling editor at the time of review.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Doyle O, Harmon CP, Heckman JJ, Tremblay RE. Investing in early human development: timing and economic efficiency. Econ Hum Biol. (2009) 7(1):1–6. doi: 10.1016/j.ehb.2009.01.002
2. Almas AN, Degnan KA, Nelson CA, Zeanah CH, Fox NA. IQ At age 12 following a history of institutional care: findings from the Bucharest early intervention project. Dev Psychol. (2016) 52(11):1858–66. doi: 10.1037/dev0000167
3. Siu AL. Screening for speech and language delay and disorders in children aged 5 years or younger: us preventive services task force recommendation statement. Pediatrics. (2015) 136(2):e474–e81. doi: 10.1542/peds.2015-1711
4. Zubler JM, Wiggins LD, Macias MM, Whitaker TM, Shaw JS, Squires JK, et al. Evidence-Informed milestones for developmental surveillance tools. Pediatrics. (2022) 149(3). doi: 10.1542/peds.2021-052138
5. Lipkin PH, Macias MM, Hyman SL, Levy SE, Spooner SA, Rodgers B, et al. Promoting optimal development: identifying infants and young children with developmental disorders through developmental surveillance and screening. Pediatrics. (2020) 145(1):1103–23. doi: 10.1542/peds.2019-3449
6. Bayley N, Aylward GP. Bayley scales of infant and toddler development. 4th ed. San antonio, TX: Pearson (2019).
8. Villagomez AN, Muñoz FM, Peterson RL, Colbert AM, Gladstone M, MacDonald B, et al. Neurodevelopmental delay: case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. (2019) 37:7623–41. doi: 10.1016/j.vaccine.2019.05.027
9. Simpson GA, Colpe L, Greenspan S. Measuring functional developmental delay in infants and young children: prevalence rates from the NHIS-D. Paediatr Perinat Epidemiol. (2003) 17(1):68–80. doi: 10.1046/j.1365-3016.2003.00459.x
10. McCune YD, Richardson MM, Powell JA. Psychosocial health issues in pediatric practices: parents’ knowledge and concerns. Pediatrics. (1984) 74(2):183–90. doi: 10.1542/peds.74.2.183
11. Geere JL, Gona J, Omondi FO, Kifalu MK, Newton CR, Hartley S. Caring for children with physical disability in Kenya: potential links between caregiving and carers’ physical health. Child Care Health Dev. (2013) 39(3):381–92. doi: 10.1111/j.1365-2214.2012.01398.x
12. Ertem IO, Atay G, Dogan DG, Bayhan A, Bingoler BE, Gok CG, et al. Mothers’ knowledge of young child development in a developing country. Child Care Health Dev. (2007) 33(6):728–37. doi: 10.1111/j.1365-2214.2007.00751.x
13. Daley TC. From symptom recognition to diagnosis: children with autism in urban India. Soc Sci Med. (2004) 58(7):1323–35. doi: 10.1016/S0277-9536(03)00330-7
14. Li Y, Liu J, Liu F, Guo G, Anme T, Ushijima H. Maternal child-rearing behaviors and correlates in rural minority areas of yunnan, China. J Dev Behav Pediatr. (2000) 21(2):114–22. doi: 10.1097/00004703-200004000-00005
15. Pollari J. When children move: some stresses and coping strategies. Early Child Dev Care. (1988) 41(1):113–21. doi: 10.1080/0300443880410110
16. Veldhuizen S, Bedard C, Rodriguez C, Cairney J. Psychological distress and parent reporting on child health: the case of developmental delay. Res Dev Disabil. (2017) 63:11–7. doi: 10.1016/j.ridd.2017.02.006
17. Reynolds C, Kamphaus R. Behavior assessment for children: Third edition. (BASC-3). Bloomington, MN: Pearson (2015).
18. Gioia GA, Isquith PK, Guy SC, Kenworthy L. Behavior rating inventory of executive function®, second edition (BRIEF®2). Child Neuropsychol (Neuropsychol Dev Cogn Sect C). (2000) 6(3):235–8. doi: 10.1076/chin.6.3.235.3152
19. Achenbach TM, Rescorla LA. Manual for the ASEBA Preschool Forms & Profiles Child Behaviour Checklist (CBCL) Ages 1 1/2 - 5. Manual for the ASEBA Preschool Forms and Profiles. (2000).
20. Squires J, Bricker D. Ages & stages questionnaires, third edition (ASQ-3): a parent-completed childn monitoring system. 3rd ed. Baltimore: Paul H. Brookes Publishiing Co., Inc. (2009).
21. Feldman HM, Dollaghan CA, Campbell TF, Kurs-Lasky M, Janosky JE, Paradise JL. Measurement properties of the MacArthur communicative development inventories at ages one and two years. Child Dev. (2000) 71(2):310–22. doi: 10.1111/1467-8624.00146
22. Fenson L. Macarthur communicative development inventories: user’s guide and technical manual. Cengage Learning. (1993) 1993.
23. Pomés M, Squires J, Yovanoff P. Psychometric examination of a spanish translation of a developmental screening instrument. J Early Child Res. (2016) 14(2):132–45. doi: 10.1177/1476718X14529279
24. Armijo I, Schonhaut L, Cordero M. Validation of the Chilean version of the ages and stages questionnaire (ASQ-CL) in community health settings. Early Hum Dev. (2015) 91(12):671–6. doi: 10.1016/j.earlhumdev.2015.10.001
25. Kendall S, Nash A, Braun A, Bastug G, Rougeaux E, Bedford H. Acceptability and understanding of the ages & stages questionnaires®, third edition, as part of the healthy child programme 2-year health and development review in England: parent and professional perspectives. Child Care Health Dev. (2019) 45(2):251–6. doi: 10.1111/cch.12639
26. Yue A, Jiang Q, Wang B, Abbey C, Medina A, Shi Y, et al. Concurrent validity of the ages and stages questionnaire and the bayley scales of infant development III in China. PLoS One. (2019) 14(9):e0221675. doi: 10.1371/journal.pone.0221675
27. van Heerden A, Hsiao C, Matafwali B, Louw J, Richter L. Support for the feasibility of the ages and stages questionnaire as a developmental screening tool: a cross-sectional study of South African and Zambian children aged 2-60 months. BMC Pediatr. (2017) 17(1):55. doi: 10.1186/s12887-017-0802-3
28. Colbert AM, Connery AK, Lamb MM, Bauer D, Olson D, Paniagua-Avila A, et al. Caregiver rating of early childhood development: reliability and validity of the ASQ-3 in rural Guatemala. Early Hum Dev. (2021) 161:105453. doi: 10.1016/j.earlhumdev.2021.105453
29. Connery A, Berrios-Siervo G, Arroyave P, Bauer D, Hernandez S, Paniagua A, et al. Responding to the Zika epidemic: preparation of a neurodevelopmental testing protocol to evaluate young children in rural Guatemala. Am J Trop Med Hyg. (2018) 100:tpmd180713. doi: 10.4269/ajtmh.18-0713
30. Lajiness-O’Neill R, Warschausky S, Huth-Bocks A, Taylor HG, Brooks J, Lukomski A, et al. Pediatrac V.3.0 protocol: a prospective, longitudinal study of the development and validation of a web-based tool to measure and track infant and toddler development from birth through 18 months. BMJ Open. (2021) 11(12):e050488. doi: 10.1136/bmjopen-2021-050488
31. Hsiao C, Richter L, Makusha T, Matafwali B, van Heerden A, Mabaso M. Use of the ages and stages questionnaire adapted for South Africa and Zambia. Child Care Health Dev. (2017) 43(1):59–66. doi: 10.1111/cch.12413
32. Olvera Astivia OL, Forer B, Dueker GL, Cowling C, Guhn M. The ages and stages questionnaire: latent factor structure and growth of latent mean scores over time. Early Hum Dev. (2017) 115:99–109. doi: 10.1016/j.earlhumdev.2017.10.002
33. Juneja M, Mohanty M, Jain R, Ramji S. Ages and stages questionnaire as a screening tool for developmental delay in Indian children. Indian Pediatr. (2012) 49(6):457–61. doi: 10.1007/s13312-012-0074-9
34. Lajiness-O’Neill R, Brooks J, Lukomski A, Schilling S, Huth-Bocks A, Warschausky S, et al. Development and validation of PediaTracTM: a web-based tool to track developing infants. Infant Behav Dev. (2018) 50:224–37. doi: 10.1016/j.infbeh.2018.01.008
35. Embretson SE, Reise SP. Item response theory for psychologists. Item Response Theory Psychol. (2013). doi: 10.4324/9781410605269
36. Kamata A, Bauer DJ. A note on the relation between factor analytic and item response theory models. Struct Equ Model. (2008) 15(1):136–53. doi: 10.1080/10705510701758406
37. Stenbeck M, Hambleton RK, Swaminathan H, Rogers HJ. Fundamentals of item response theory. Contemp Sociol. (1992) 21(2):289. doi: 10.2307/2075521
38. Hambleton RK, Swaminathan H. Item response theory. Principles and applications. New York: Springer Dordrecht (1987). 332 S.
39. der Linden WV, Hambleton RK. Handbook of modern item response theory. J Am Stat Assoc. (1997) 92(439):1227. doi: 10.2307/2965612
40. Depaoli S, Tiemensma J, Felt JM. Assessment of health surveys: fitting a multidimensional graded response model. Psychol Heal Med. (2018) 23:13–31. doi: 10.1080/13548506.2018.1447136
41. Singh GK. Area deprivation and widening inequalities in US mortality, 1969-1998. Am J Public Health. (2003) 93(7):1137–43. doi: 10.2105/AJPH.93.7.1137
42. Erdodi LA. Aggregating validity indicators: the salience of domain specificity and the indeterminate range in multivariate models of performance validity assessment. Appl Neuropsychol. (2019) 26(2):155–72. doi: 10.1080/23279095.2017.1384925
43. Rosenberg SA, Zhang D, Robinson CC. Prevalence of developmental delays and participation in early intervention services for young children. Pediatrics. (2008) 121(6):e1503–e9. doi: 10.1542/peds.2007-1680
44. Giromini L, Young G, Sellbom M. Assessing negative response bias using self-report measures: new articles, new issues. Psychol Inj Law. (2022) 15:1–21. doi: 10.1007/s12207-022-09444-2
45. Simpson S, D’Aprano A, Tayler C, Toon Khoo S, Highfold R. Validation of a culturally adapted developmental screening tool for Australian aboriginal children: early findings and next steps. Early Hum Dev. (2016) 103:91–5. doi: 10.1016/j.earlhumdev.2016.08.005
Keywords: caregiver report, infant development, early childhood development, response style, sociodemographic factors
Citation: Connery AK, Raghunathan RS, Colbert AM, Erdodi L, Warschausky S, Huth-Bocks A, Gerry Taylor H, Raghunathan T, Berglund P, Staples AD, Lukomski A, Kirkland J, Cano J and Lajiness-O’Neill R (2023) The influence of sociodemographic factors and response style on caregiver report of infant developmental status. Front. Pediatr. 10:1080163. doi: 10.3389/fped.2022.1080163
Received: 25 October 2022; Accepted: 12 December 2022;
Published: 11 January 2023.
Edited by:
Edson Zangiacomi Martinez, University of São Paulo, BrazilReviewed by:
Renato Arruda, University of São Paulo, BrazilAnnette Richard, University of Michigan, United States
© 2023 Connery, Raghunathan, Colbert, Erdodi, Warschausky, Huth Bocks, Taylor, Raghunathan, Berglund, Staples, Lukomski, Kirkland, Cano and Lajiness-O'Neill. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amy K. Connery YW15LmNvbm5lcnlAY2hpbGRyZW5zY29sb3JhZG8ub3Jn
Specialty Section: This article was submitted to Children and Health, a section of the journal Frontiers in Pediatrics