 Lechosław Paweł Chmielik1,2*
Lechosław Paweł Chmielik1,2* Anna Kasprzyk
Anna Kasprzyk
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr. , 11 January 2023
Sec. Pediatric Otolaryngology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.1077198
Background: The health—related quality of life (HRQoL) concept is nowadays increasingly and more broadly used for helping evaluate the effectiveness of medical treatment, superseding the earlier “quality of life” approach. The HRQoL concept likewise applies to otolaryngology and this narrative review study is focused on HRQoL outcomes in four key childhood otolaryngological diseases as reported in the literature.
Study aim: To retrospectively evaluate the literature on measuring HRQoL in children suffering from selected otolaryngological illnesses, during treatment.
Materials and Methods: Published studies/case reports were searched for in Medline, PubMed, Web of Science, Scopus and ORCID on the quality of life based on paediatric patient questionnaires, whether completed by subjects themselves or by their parents (by proxy). The following key words were used: health quality of life, otolaryngology/ENT, pediatrics/paediatrics. Studies before 1999 were omitted because hitherto, the “quality of life” had been imprecisely defined thus rendering any subsequent comparisions problematic.
Results: HRQoL scores and well-being were found to significantly deteriorate in child patients suffering from four important otolaryngological disorders: chronic sinusitis, nasal septum deviation, adenoid hypertrophy and hearing disease. The main problems found were infection, inflammation, disruption to family life and child-parental interaction, fitness-related issues, reduced ENT patencies and apnea.
Conclusions: The HRQoL appears to significantly deteriorate in children suffering from otolaryngological diseases. Further such studies are needed for other ENT diseases.
Numerous attempts have been made to find a uniform definition for the quality of life, but none have yet met with general acceptance (1–3). The “quality of life” issue only began being addressed in the latter half of the 20th century. Criteria used for its assessment were initially those measuring levels of social development in the USA and Western Europe. At first, only objective parameters were considered, such as material well-being and social development. Later, however, subjective and non-material parameters were added like health, freedom, and happiness, leading to the health—related quality of life (HRQoL) concept. Indeed, the latter (subjective parameters) has increasingly attracted more attention over recent times; this likewise being the case in the otolaryngology field when assessing patients' HRQoL.
Quality of life can be defined, in a simplified form, as being an area of human life that directly concerns a person, and which is important to her/him (5).
The World Health Organization (WHO) defines the “quality of life” as an individual's perception of their position in life in the context of culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. The following are included in the “quality of life” (1, 3, 6):
– Levels of freedom/independence,
– Mental health,
– Physical health,
– Social belonging,
– The environment,
– Religious beliefs, convictions, and views.
Due to the wide range of subjects covered when defining the “quality of life”, the medical field had introduced the term “health—related quality of life” (HRQoL) (1, 6).
The WHO had defined “health” in the 1940s as not only an absence of illness, but also by physical and mental well-being along with social belonging (4).
HRQoL includes those areas of life directly concerned with patient health. Other factors had not been analyzed such as freedom, income level or the quality of the natural environment (7, 8). In the 1970s, the holistic approach became embraced in medicine which generated interest in the HRQoL concept in this field. Any therapeutic process should make a patient's life active and, in as far as possible, to resemble that of a healthy person (1, 2, 6). Assessing health-related quality of life has thus also found an application in pediatric otolaryngology.
There are however specific difficulties in testing HRQoL in children and it becomes apparent to use separate questionnaires (9, 11), which are adapted to developmental changes in children. It is also necessary to account for the differences in perception of various aspects of life between children and adults. Questionnaires used in pediatrics should therefore especially assess family relations, active spending of time, self-esteem, external appearance of the child and contacts with peers (9–11). Engaging in sports and physical fitness also significantly impact the quality of life in children (11). Both parents/guardians and children can assess HRQoL, but their ratings do not always coincide. Nevertheless, both ways are important when evaluating the overall child's HRQoL (10). The reasons are that parents will inevitably have some influence on their child's diagnosis and therapy, while any physical and mental impairment in the child, or immaturity, could prevent the child (10) from completing the questionnaire on their own. Parental assessment of HRQoL that covers a long follow-up period may be more reliable because inconsistencies in children's viewpoints are removed, that have been caused by their ongoing maturation (9, 11). Greater agreement in evaluating HRQoL has been found between parents and offspring (11) when children suffer from chronic disease, as compared to healthy children and their parents (9–11).
To retrospectively evaluate measuring the health—related quality of life in children suffering from four otolaryngological illnesses when undergoing treatment by conducting a narrative review of the available literature relevant to this subject area.
Published studies on HRQoL were reviewed which focused on measuring those areas concerning the child—parent's deteriorating well-being in four otolaryngological diseases during treatment: chronic sinusitis, nasal septum deviation, adenoid hypertrophy and hearing disease. As a general point, questionnaires for measuring the HRQoL should meet certain criteria, principally (9, 10): responsiveness (the ability to detect minimal changes during testing), reliability (the ability to obtain reproducible results for consecutive measurements) and validity (the ability to measure intended parameters) (7). Questionnaires were either completed by the child subjects or, in most cases, by their parents to avoid any misunderstandings. The review consisted in searching Medline, PubMed, Web of Science and Scopus. The ORCHID digital ID search engine was also used as a safeguard to identify any possible publications of relevance that could have been missed by the other search engines. The following key words were used: health quality of life, otolaryngology/ENT, pediatrics/paediatrics, nasal septum deviation, nasal patency, chronic sinusitis, adenoid/tonsil hypertrophy, adenotonsillectomy, otitis media, hearing, and cochlear implant.
Studies prior to 2007were omitted, because the “quality of life” had up till then been imprecisely and variously defined making any direct comparisons difficult. Only HRQoL—based studies were considered in this review.
Inclusion criteria consisted of: selecting quality of life studies in pediatric otolaryngology written in English, subjects >50 and the use of validated questionnaires. Exclusion criteria were: studies written in a non-English language, ENT subjects aged >18 years, insufficient numbers of subjects, non-validated questionnaires, and any study prior to 1999 (because of the hitherto imprecise “quality of life” definition). If there were more than 10 studies found eligible per condition, then 10 were randomly selected to constitute an analyzed group. The criterion of having >50 subjects was however waived in the case of chronic sinusitis, where a n = > 20 threshold was adopted, because of the small numbers of studies meeting this original criterion. It was recognized that the Evidence Based Medicine (EBM) power of these studies may thereby be compromised.
There were 164 studies found eligible out of 12,354 studies on HRQoL in papers with tonsil hypertrophy, of which 10 were randomly entered into the study group as presented in Table 1.
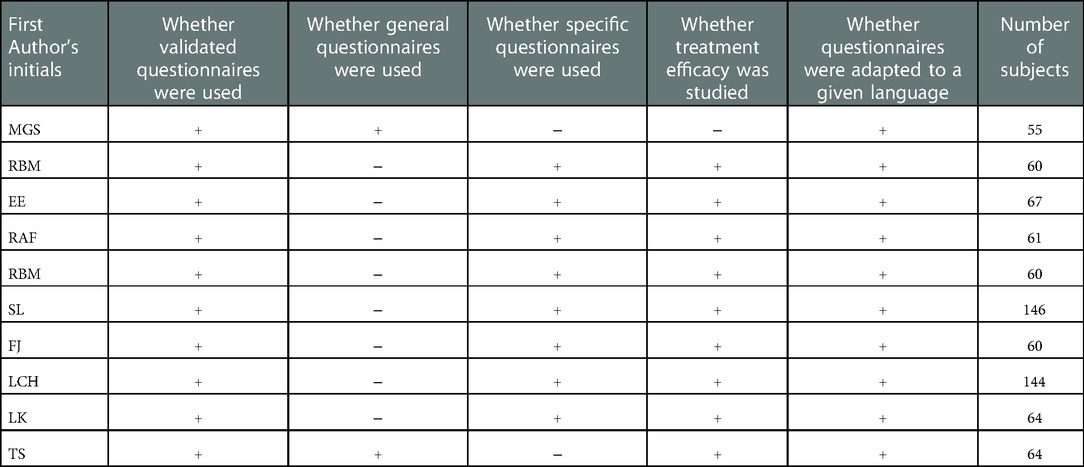
Table 1. Chosen HRQoL studies on tonsil hypertrophy.
There were 7 studies found eligible out of 2,248 studies on HRQoL in papers with chronic sinusitis that constituted the study group as presented in Table 2.

Table 2. Chosen HRQoL studies on chronic sinusitis.
There were four studies found eligible out of 10,128 studies on HRQoL in papers with nasal septum deviation that constituted the study group as presented in Table 3.
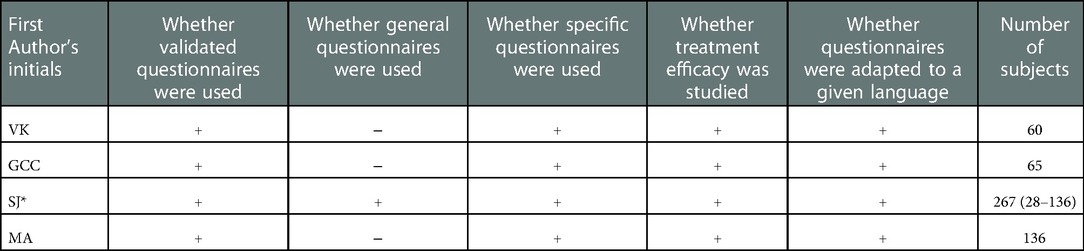
Table 3. Chosen HRQoL studies on nasal septum deviation.
There were 4 studies found eligible out of 4,355 studies on HRQoL in papers with hearing disease that constituted the study group as presented in Table 4.

Table 4. Chosen HRQoL studies on hearing disease.
Some of the reasons for rejecting studies belonging to this group were an insufficient number of subjects, (indeed, in one study, only 7 subjects were finally analyzed out of 53 patients), the use of non-randomized procedures, being published in non-English languages and studies based on adults.
Many problems and complications were found and are considered further in the next section, but mainly include: family and physical activity/function, general health, social behaviour, pain discomfort, mental and emotional health as well as impaired nasal and other ENT patencies, breathing and speech problems, apnea, disturbed sleep fatigue and dysphagia; variously appearing in either/or the short or long term.
Our review found that 23 (92%), out of the 25 studies selected for analysis, had employed specific HRQoL questionnaires, whereas general ones had been used 4 times (8%). The effect of treatment on HRQoL had also been evaluated in 23 (92%) of these studies.
Indeed, most HRQoL studies on ENT are focused on HRQoL before and after treatment using very specific tests. There are however no studies comparing the HRQoL of sick and healthy children nor ones comparing the HRQoL in children with ENT diseases with each other and with those children suffering from other diseases (12).
General purpose questionnaires from papers studies selected as eligible were: The Pediatric Quality of Life Inventory (PedsQL), Child Health Questionnaire (CHQ-PF28) and Child Health Questionnaire—Parent Form 50 (CHQ-PF50) along with the Glasgow Children's Benefit Inventory (GCBI), D15, D16, D17, SF36, Visual Analogue Score (VAS), EuroQol 5-Dimension Health Assessment (EQ5D). General quality of life was measured by the Dutch version of the Kidscreen-27 (12–17). Specific questionnaires from those ENT studies found were as follows: The Obstructive Sleep Apnea-18 (OSA-18), Obstructive Sleep Disorders-6, Pediatric Throat Disorders Outcome Test (T-14), Tonsil and the Adenoid Health Status Instrument (TAHSI), Sinus and Nasal QoL (SN-5), Nasal Obstruction Symptom Evaluation (NOSE), Otitis Media 6-item (OM-6), Speech Spatial and Qualities of Hearing Scale (SSQ), Children with Cochlear Implants: Parental Perspectives (CCIPP) (12–17).
The aim of any given study on quality of life dictates the choice of an appropriate questionnaire (13–17). General purpose ones are used for studying large populations suffering from various pathologies, which have allowed comparisons to be made between studies, notwithstanding if patients were in good health or had suffered from any illnesses, irrespective of the size of the study groups (4, 13–17). It is worth emphasizing that general purpose questionnaires are not applicable for assessing any slight changes in a single patient (11–17). Specific HRQoL research questionnaires have thus been created whenever there are specific issues to be investigated. These kinds of questionnaires are much more sensitive in detecting changes which occur over time, and they provide information about the effectiveness of treatment or the evolution of disease. Nonetheless, they are not suited for evaluating individuals with comorbidities (15–17). Assessing the quality of life is increasingly becoming more recognized as being part of a patient's clinical condition and the effectiveness of subsequent therapy, including child patients. It is therefore considered desirable to establish a baseline for quality-of-life determinants in healthy children. Studies have mainly investigated health status before and after an applied treatment by using detailed questionnaires. Recurrent tonsillitis and tonsil hypertrophy, (and its complications), are believed in many countries to reduce the quality of life in children so affected (19–29). These studies emphasize that limitations in children's health affect joint family activities, physical activity, general health, behaviour and family emotions. A very strong correlation was also found between such constraints with limitations on parents' free time. As an aside and beyond the scope of this review, it should however be noted that studies on patients suffering from sleep apnea syndrome form a quite considerably large group of articles regarding the quality of life in ENT patients (23–25).
We have also taken into account studies on HRQoL in relation to chronic sinusitis, where it has been stated that the quality of life becomes limited in areas such as general health, pain, discomfort, the influence of a child's condition/well-being on parents' emotions, physical fitness, limitations in social functioning, limitations in parents' free time and mental health. Study tools used were designed to survey longitudinal changes in the HRQoL (such as SN-15 or OSA-18) (26–29). This disease does not however reduce self-esteem nor change behaviour (26, 27).
A long-term impaired nasal patency is observed in patients with chronic rhinitis and paranasal sinusitis, where ENT examination shows discharge into the nasal cavities or at the back of the throat. Such children experience pain, a feeling of fullness in the face and having an impaired or lack of smell (30–41). Having a worse nasal patency usually leads to infection of the paranasal sinuses and ears. Parents free time may become limited, while also reducing the quality of child-parent contact due to long-term inflammatory changes and the related problems in organising how family life functions (e.g., reconciling parents' work commitments to fit in with check-up visiting dates at pediatric or ENT clinics, or in providing a sick child with care during parents' working hours).
Only single studies have compared the quality of life in healthy children to those with chronic diseases and ones investigating differences in the quality of life for particular diseases relative to each other (41, 44).
Patients with nasal septum deviation have reported chronic obstruction of the nasal cavities, thereby reducing the efficiency in how the upper respiratory tract operates (42–46). A disturbed breathing pattern in children may cause their abnormal physical and mental development. Indeed, any causes of abnormal child development may deteriorate the patient's physical fitness (being one of the determinants of peer-group position), which will also probably reduce the self-esteem of the sick child (5, 18).
A significantly deteriorating quality of life includes the following general symptoms: nervousness, fatigue, sweating, concentration disorders and excessive daytime sleepiness. Whenever obstruction to the nasal cavities occur, particularly in adenoid hypertrophy (34–36), then the local symptoms reported include changes in breathing pattern to mouth breathing (adenoid faces/long face syndrome), malocclusion, altered voice timbre, night snoring and night apnea.
Furthermore, an enlarged adenoid may impair the patency of the Eustachian tube which, inter-alia, can lead to exudative otitis media, that may lead to hearing loss (47–53). Symptoms of tonsil hypertrophy are: snoring, obstructive sleep apnea syndrome, speech disorder (slurring) and dysphagia; especially with solid foods (19–35, 49, 53).
All these ailments can be expected to directly lead to a deteriorating HRQoL, when assessed either by the patients themselves or their parents. Parental concerns may be about their child suffering from frequent upper respiratory tract infections, a decreased well-being or poorer marks at school; the latter being partly due to a more frequent absenteeism from school. The children's environment can signal changes in character as manifested by more frequent bouts of anger or conflicts with schoolmates or teachers. Such disorders may arise from ENT-related or other conditions such as hypoxia of the central nervous system, poisoning by bacterial toxins during chronic diseases of the upper respiratory tract and ears, poorer hearing caused by the Eustachian tube being blocked and chronic infections of the middle ear (49, 51).
One study showed a small deterioration in the education and social functioning aspects of HRQoL for those children suffering from a one-sided (unilateral) hearing loss/deafness (50). It also found that HRQoL was more limited in children with bilateral hearing loss than those with unilateral hearing loss. It is stressed in other studies, that children having cochlear implants were found to have similar HRQoL to healthy children (49–53). Changes in hearing threshold and tinnitus severity after stapes surgery has also been found to be important to the quality of life (54) in, however, adult patients. Nevertheless, these studies excellently highlight how HRQoL studies could be conducted in patients with ear disease.
The health-related quality of life has been found to significantly deteriorate in many areas when children are suffering from the four key otolaryngological disease reviewed. Further studies on the HRQoL thus also appear advisable on those children treated for other diseases of the ear, nose, and larynx/throat. Having standardized HRQoL questionnaires, tailored to specific issues, is important across studies. The quality of life should be an element of the patient's clinical examination.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
LPCH: conceptualization, writing (original draft preparation). GM-N: conceptualization, writing (review, supervision). AK: writing (manuscript preparation). AN: supervision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Leplège A, Hunt S. The problem of quality of life in medicine. JAMA. (1997) 278(1):47–50. doi: 10.1001/jama.1997.03550010061041
2. Ryglewicz D, Kuran W. Jakość życia i oczekiwania terapeutyczne chorych na padaczkę. Epileptologia. (2003) 11:171–8.
3. Lindert J, Sancassiani F, Massa E, Nardi AE. An overview of the international literature on health-related quality of life, mental health and psychosocial issues in people with cancer. Clin Pract Epidemiol Ment Health. (2021) 17(1):253–6. doi: 10.2174/17450179021170102534.
4. Lin XJ, Lin IM, Fan SY. Methodological issues in measuring health-related quality of life. Tzu Chi Med J. (2013) 25:8–12. doi: 10.1016/j.tcmj.2012.09.002
5. Sajid MS, Tonsi A, Baig MK. Health-related quality of life measurement. Int J Health Care Qual Assur. (2008) 21(4):365–73. doi: 10.1108/09526860810880162, Erratum in: Int J Health Care Qual Assur. 2009;22(1):76.18785462
6. Skrzypek M. O badaniach nad jakością życia i sposobach rozumienia norm. Alma Mater. (2000) 1(34):136–9.
7. Mazur J, Mierzejewska E. Health—related quality of live (HRQL) in children and adolescents—concepts study methods and lecected applications. Med Wieku Rozwoj. (2003) 7:35–48. PMID: 1470448914704489
8. Guyatt G, Fenny DH. Measuring health—related quality of life. Ann Inter Med. (1993) 118:622–9. doi: 10.7326/0003-4819-118-8-199304150-00009
9. Eiser C, Mores R. Quality of life measures in chronic diseases of childhood. Health Technol Assess. (2001) 5(4):1–57. doi: 10.3310/hta5040
10. Vitale MG, Roye D. An exploration of life outcomes measures in scoliosis and cerebral palsy. Pediatrics. (1999) 104:716.
11. Herdman M, Rajmil L, Ravens-Sieberer U, Bullinger M, Power M, Alonso J. Export consensus in the development of European heath-related quality of life measure for children and adolescents: a delihi study. Acta Paediatr. (2002) 91:1385–90. doi: 10.1111/j.1651-2227.2002.tb02838.x
12. Kao SS-T, Peters MDJ, Dharmawardana N, Stew B, Ooi EH. Scoping review of pediatric tonsillectomy quality of life assessment instruments: pediatric tonsillectomy QoL assessment tools. Laryngoscope. (2017) 127(10):2399–406. doi: 10.1002/lary.26522
13. Kosse NJ, Windisch W, Koryllos A, Lopez-Pastorini A, Piras D, Schroiff H-W, et al. Development of the diaphragmatic paralysis questionnaire: a simple tool for patient relevant outcome. Interact Cardiovasc Thorac Surg. (2021) 32(2):244–9. doi: 10.1093/icvts/ivaa258
14. Spronk I, Legemate C, Oen I, van Loey N, Polinder S, van Baar M. Health related quality of life in adults after burn injuries: a systematic review. PLoS One. (2018) 13(5):e0197507. doi: 10.1371/journal.pone.0197507
15. Balla A, Leone G, Ribichini E, Sacchi MC, Genco A, Pronio A, et al. Gastroesophageal reflux disease—health-related quality of life questionnaire: prospective development and validation in Italian: prospective development and validation in Italian. Eur J Gastroenterol Hepatol. (2021) 33(3):339–45. doi: 10.1097/MEG.0000000000001914
16. Heaney A, Stepanous J, Rouse M, McKenna SP. A review of the psychometric properties and use of the rheumatoid arthritis quality of life questionnaire (RAQoL) in clinical research. Curr Rheumatol Rev. (2017) 13(3):197–205. doi: 10.2174/1573396313666170615092324
17. Tokuno J, Chen-Yoshikawa TF, Oga T, Oto T, Okawa T, Okada Y, et al. Analysis of optimal health-related quality of life measures in patients waitlisted for lung transplantation. Can Respir J. (2020) 2020:4912920. doi: 10.1155/2020/4912920
18. Marker AM, Steele RG, Noser AE. Physical activity and health-related quality of life in children and adolescents: a systematic review and meta-analysis. Health Psychol. (2018) 37(10):893–903. doi: 10.1037/hea0000653
19. Stepan L, Huang L, Huynh J, Xie P, Woods CM, Ooi EH. Health related quality of life T-14 outcomes for pediatric bizact tonsillectomy. Medicina. (2021) 57(5):480. doi: 10.3390/medicina57050480
20. Fehrm J, Nerfeldt P, Browaldh N, Friberg D. Effectiveness of adenotonsillectomy vs watchful waiting in young children with mild to moderate obstructive sleep apnea: a randomized clinical trial: a randomized clinical trial. JAMA Otolaryngol Head Neck Surg. (2020) 146(7):647–54. doi: 10.1001/jamaoto.2020.0869
21. Lee C-H, Kang K-T, Weng W-C, Lee P-L, Hsu W-C. Quality of life after adenotonsillectomy for children with sleep-disordered breathing: a linear mixed model analysis. Int J Pediatr Otorhinolaryngol. (2014) 78(8):1374–80. doi: 10.1016/j.ijporl.2014.05.038
22. Lushington K, Kennedy D, Martin J, Kohler M. Quality-of-life but not behavior improves 48-months post-adenotonsillectomy in children with SDB. Sleep Med. (2021) 81:418–29. doi: 10.1016/j.sleep.2021.02.057
23. Türkoğlu S, Tahsin Somuk B, Sapmaz E, Bilgiç A. Effect of adenotonsillectomy on sleep problems, attention deficit hyperactivity disorder symptoms, and quality of life of children with adenotonsillar hypertrophy and sleep-disordered breathing. Int J Psychiatry Med. (2019) 54(3):231–41. doi: 10.1177/0091217419829988
24. Hassmann-Poznańska E. Komentarz do artykułu ocena skuteczności tonsillektomii lub adenotonsylektomii w leczeniu nawracających zapaleń gardła u dzieci. Medycyna Praktyczna Pediatria. (2002) 06(24):39–42.
25. Stewart MG, Friedman EM, Sulek M. Quality of life and health status in pediatric tonsil and adenoid disease. Arch Otolaryngol Head Neck Surg. (2000) 126:45–8. doi: 10.1001/archotol.126.1.45
26. Michell RB, Kelly J, Call E. Quality of life after adenotonsillectomy for obstructive sleep apnea in children. Arch Otolaryngol Head Neck Surg. (2004) 130:190–4. doi: 10.1001/archotol.130.2.190
27. Ericsson E, Lundeborg I, Hultcrantz E. Child behavior and quality of life before and after tonsillotomy versus tonsillectomy. Int J Pediatr Otorhinolaryngol. (2009) 73(9):1254–62. doi: 10.1016/j.ijporl.2009.05.015
28. Francor A, Rosenfeld RM, Rao M. Quality of life for children with obstructive sleep apnea. Otolareyngogy—Head and Neck Surgery. (2000) 123:9–16. doi: 10.1067/mhn.2000.105254
29. Przybyłowski T, Chazan R, Balcerzak J, Niemczyk K. Niezabiegowe leczenie obturacyjnego leczenia bezdechu podczas snu. Niezabiegowe Leczenie Obturacyjnego Bezdechu Podczas Snu Otolaryngologia. (2005) 4(1):11–8.
30. Ahmed S, Sami AS. Rhinosinusitis and its impact on quality of life in children. Br J Hosp Med. (2022) 83(3):1–11. doi: 10.12968/hmed.2021.0589
31. Makary CA, Tumlin P, Asad F, Wasef K, Ramadan HH. Quality of life measurement for adolescent patients with sinonasal symptoms. Laryngoscope. (2022). doi: 10.1002/lary.30232. [Epub ahead of print]
32. Lai W-Y, Kay DJ, Wei C-C, Huang F-W, Liang K-L, Yen H-R. Validation of the traditional Chinese version of the Sinus and nasal quality of life survey (SN-5) for children. Pediatr Neonatol. (2022) 63(4):410–7. doi: 10.1016/j.pedneo.2022.01.008
33. Calvo-Henriquez C, Lechien JR, Méndez-Benegassi I, Benoliel AL, Faraldo-García A, Martínez-Capoccioni G, et al. Pediatric turbinate radiofrequency ablation improves quality of life and rhinomanometric values. A prospective study. Int J Pediatr Otorhinolaryngol. (2022) 154(111050):111050. doi: 10.1016/j.ijporl.2022.111050
34. Calvo-Henríquez C, Valencia-Blanco B, Boronat-Catalá B, Maza-Solano J, Díaz-Anadón Á, Kahn S, et al. Cross-cultural adaptation of the sinus and nasal quality of life survey (SN-5) to Spanish. Int J Pediatr Otorhinolaryngol. (2020) 139(110425):110425. doi: 10.1016/j.ijporl.2020.110425
35. Sethi G, Chakravarti A. Quality of life after endoscopic sinus surgery in refractory pediatric chronic rhinosinusitis. Int J Pediatr Otorhinolaryngol. (2016) 90:160–4. doi: 10.1016/j.ijporl.2016.09.005
36. Rudnick EF, Mitchell RB. Improvements in quality of life in children after surgical therapy for sinonasal disease. Otolaryngol Head Neck Surg. (2006) 134(5):737–40. doi: 10.1016/j.otohns.2005.12.033
37. Pauli C, Fintelmann R, Klemens C. Polyposis nasi—improvement in quality of life by the influence of leukotrien receptor antagonists. Laryngorhinootologie. (2007) 4:282–6. doi: 10.1055/s-2007-966094
38. Kay DJ, Rosenfeld RM. Quality of life for children with persistent sinonasal symptoms. Otolaryngol Head Neck Surg. (2003) 128(1):17–26. doi: 10.1067/mhn.2003.41
39. Chen H, Katz PP, Shiboski S, Blanc PD. Evaluating change in health—related quality of life in adult rhinitis: responsiveness of the rhinosinusitis disability index. Health Qual Life Outcomes. (2005) 8(3):68–9. doi: 10.1186/1477-7525-3-68
40. Cunningham MJ, Chiu EJ, Landgraf JM, Gliklich RE. The health impact of chronic recurrent rhinosinusitis in children. Arch Otolaryngol Head Neck Surg. (2000) 126(11):1363–8. doi: 10.1001/archotol.126.11.1363
41. Fokens WJ, Lund VJ, Bachert C. European Position paper on rhinosinusitis and nasal polyps. Rhinology. (2020) 58(Suppl S29):1–464. doi: 10.4193/Rhin20.600
42. Valsamidis K, Titelis K, Karkos P, Markou K, Constantinidis J, Triaridis S. Predictive factors of patients’ general quality of life after nasal septoplasty. Eur Arch Otorhinolaryngol. (2019) 276(2):429–38. doi: 10.1007/s00405-018-5229-4
43. Gary CC. Pediatric nasal surgery: timing and technique. Curr Opin Otolaryngol Head Neck Surg. (2017) 25(4):286–90. doi: 10.1097/MOO.0000000000000378
44. Saniasiaya J, Abdullah B. Quality of life in children following nasal septal surgery: a review of its outcome. Pediatr Investig. (2019) 3(3):180–4. doi: 10.1002/ped4.12145
45. Manteghi A, Din H, Bundogji N, Leuin SC. Pediatric septoplasty and functional septorhinoplasty: a quality of life outcome study. Int J Pediatr Otorhinolaryngol. (2018) 111:16–20. doi: 10.1016/j.ijporl.2018.05.016
46. Chandra SR, Zemplenyi KS. Issues in pediatric craniofacial trauma. Facial Plast Surg Clin North Am. (2017) 25(4):581–91. doi: 10.1016/j.fsc.2017.06.00947.
47. Nell MJ, Grote JJ. Structural changes in the rat middle ear mucosa due to endotoxin and eustachian tube obstruction. Eur Arch Otorhinolaryngol. (1999) 256(4):167–72. doi: 10.1007/s004050050134
48. Ryding M, White P, Kalm O. Eustachian tube function and tympanic membrane findings after chronic secretory otitis media. Int J Pediatr Otorhinolaryngol. (2004) 68(2):197–204. doi: 10.1016/j.ijporl.2003.10.013
49. Lameiras AR, Silva D, Neill A, Escada P. Qualidade de vida das crianças com otite média e impacto da colocação de tubos de ventilação transtimpânicos numa população portuguesa quality of life of children with Otitis media and impact of insertion of transtympanic ventilation tubes in a Portuguese population. Acta Med Port. (2018) 31(1):30–7. doi: 10.20344/amp.9457
50. Smit AL, Burgers YRW, Swanenburg de Veye HFN, Stegeman I, Breugem CC. Hearing-related quality of life, developmental outcomes and performance in children and young adults with unilateral conductive hearing loss due to aural atresia. Int J Pediatr Otorhinolaryngol. (2021) 142(110590):110590. doi: 10.1016/j.ijporl.2020.110590
51. Chow Y, Wabnitz DAM, Ling J. Quality of life outcomes after ventilating tube insertion for otitis media in an Australian population. Int J Pediatr Otorhinolaryngol. (2007) 71(10):1543–7. doi: 10.1016/j.ijporl.2007.06.001
52. Zhumabayev R, Zhumabayeva G, Kapanova G, Tulepbekova N, Akhmetzhan A, Grjibovski A. Quality of life in children with cochlear implants in Kazakhstan. BMC Pediatr. (2022) 22(1):194. doi: 10.1186/s12887-022-03254-w
53. Skarżyński H, Piotrowska A. Screening for pre-school and school-age hearing problems: european consensus statement. Int J Pediatr Otorhinolaryngol. (2012) 76(1):120–1. doi: 10.1016/j.ijporl.2011.10.016
Keywords: health-related quality of life, pediatrics, otolaryngology, hearing loss, adenoid hypertrophy, nasal septum deviation, sinusitis
Citation: Chmielik LP, Mielnik–Niedzielska G, Kasprzyk A and Niedzielski A (2023) A review of health—related quality of life issues in children suffering from certain key otolaryngological illnesses. Front. Pediatr. 10:1077198. doi: 10.3389/fped.2022.1077198
Received: 22 October 2022; Accepted: 16 December 2022;
Published: 11 January 2023.
Edited by:
Muhammad Shahid Iqbal, Prince Sattam bin Abdulaziz University, Saudi ArabiaReviewed by:
Muhammad Zahid Iqbal, AIMST University, Malaysia© 2023 Chmielik, Mielnik–Niedzielska, Kasprzyk and Niedzielski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lechosław Paweł Chmielik bC5wLmNobWllbGlrQGNobWllbGlrLnBs
Specialty Section: This article was submitted to Pediatric Otolaryngology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.