
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr. , 12 January 2023
Sec. Pediatric Endocrinology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.1075738
This article is part of the Research Topic Endocrine and Cardiometabolic Alterations in Pediatric Patients with Chronic Diseases View all 7 articles
 Silvia Rodríguez-Narciso1
Silvia Rodríguez-Narciso1 Raigam Jafet Martínez-Portilla2,3
Raigam Jafet Martínez-Portilla2,3 Iris Paola Guzmán-Guzmán4Gabriela Careaga-Cárdenas5Brenda Jazmin Rubio-Navarro5Luis Fernando Barba-Gallardo5Rodolfo Delgadillo-Castañeda6
Iris Paola Guzmán-Guzmán4Gabriela Careaga-Cárdenas5Brenda Jazmin Rubio-Navarro5Luis Fernando Barba-Gallardo5Rodolfo Delgadillo-Castañeda6 José Rafael Villafan-Bernal3,7,8*
José Rafael Villafan-Bernal3,7,8*
Background: Osteocalcin plays a role in glucose metabolism in mice, but its relevance in human energetic metabolism is controversial. Its relationship with markers of energetic metabolism in the pediatric population has not been systematically addressed in infants and adolescents.
Objective: This study aims to assess the mean differences between tOC, ucOC, and cOC among healthy children and children with type 1 or type 2 diabetes (T1D or T2D) and the correlation of these bone molecules with metabolic markers.
Methods: A systematic review and metanalysis were performed following PRISMA criteria to identify relevant observational studies published in English and Spanish using PubMed, Scopus, EBSCO, and Web of Science databases. The risk of bias was assessed using New Castle–Ottawa scale. Effect size measures comprised standardized mean difference (SMD) and Pearson correlations. Heterogeneity and meta-regressions were performed.
Results: The 20 studies included were of high quality and comprised 3,000 pediatric patients who underwent tOC, cOC, or ucOC measurements. Among healthy subjects, there was a positive correlation of ucOC with WC and weight, a positive correlation of tOC with FPG, HDL-c, WC, height, and weight, and a negative correlation between tOC and HbA1c. Among diabetic subjects, a negative correlation of ucOC with HbA1c and glycemia in both T1D and T2D was found and a negative correlation between tOC and HbA1c in T1D but not in T2D. The ucOC concentrations were lower in T2D, T1D, and patients with abnormal glucose status than among controls. The serum concentrations of tOC concentrations were lower among T1D than in controls. The patient's age, altitude, and HbA1c influenced the levels of serum tOC.
Conclusion: Osteocalcin is involved in energy metabolism in pediatric subjects because it is consistently related to metabolic and anthropometric parameters.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier: CRD42019138283.
After the discovery of the effects of undercarboxylated osteocalcin (ucOC) in regulating glucose metabolism, insulin release, and insulin sensibility in mice (1), several studies in human have confirmed the relevance of this bone-derived hormone in the regulation of glucose metabolism in human adults (2–6).
In adults, previous metanalysis demonstrated significant differences in total osteocalcin (tOC) serum concentrations between type 2 diabetics (T2D) and healthy subjects (HS) (7, 8). Women with gestational diabetes exhibit significant differences in tOC serum levels compared to normal pregnant (9). However, the role of this hormone in regulating glycemia and insulin sensibility in children and adolescents has been briefly studied (10, 11), and no metanalysis formerly analyzed the role of osteocalcin in energetic metabolism nor its relationship to other metabolic parameters in this population.
During infancy and adolescence, osteocalcin serum levels are higher because of the highest osteoblast activity necessary to support bone growth and the high rate of bone remodeling (12, 13). Consequently, the osteocalcin serum levels increase to parallel the growth velocity curve (14).
Although some original studies report altered serum levels of tOC in type 1 diabetes mellitus (T1D) (15, 16), few small studies have measured ucOC and cOC (two specific types of osteocalcin) in T1D (17). Furthermore, no clarity exists on the association of ucOC with energetic metabolism markers in healthy and T2D children. Since ucOC is claimed to be the osteocalcin type with a role in the modulation of energetic metabolism (18, 19), it is necessary to clarify the role of this hormone in metabolism in human children and adolescents.
In the present study, we analyze if there are significant differences in osteocalcin serum concentrations (cOC, ucOC, and total OC) between healthy and diabetic pediatric patients. In addition, we estimated the correlation of osteocalcin with markers of energetic metabolism in pediatric subjects with normal glycemic status and with T1D or T2D.
This project was registered in the PROSPERO International prospective register of systematic reviews (registration number: CRD42019138283).
A systematic search was executed in PubMed, Scopus, Web of Science, The Cochrane Library, and PROSPERO databases to identify relevant studies published in English and Spanish restricted to human with no restriction in publication date. The query and keywords of the search are presented in Supplementary S1A. additional manual search was conducted to identify additional relevant publications. The first search was run on July 20, 2018. Afterward, the update was extended until March 20, 2022. This review was carried out adhering to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines (20), and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews and meta-analysis (21, 22). Two independent evaluators evaluated the abstracts (GCC & BJRN), blinded to authorship, authors' institutional affiliation, and study results. If the abstract fulfilled the inclusion criteria, full-text articles were then reviewed. The third and fourth investigators (JRVB & RJMP) independently resolved any disagreement between evaluators. Corresponding authors were reached by e-mail to request such data in the case of relevant studies with missing information.
We include in this systematic review and meta-analysis only observational cross-sectional studies that included pediatric patients (less than 18 years old) with T1D, T2D, or nondiabetic controls reporting mean serum levels of osteocalcin (cOC, ucOC or tOC) and/or coefficient correlations between any type of osteocalcin (cOC, ucOC or tOC) and fasting glucose, fasting insulin, HOMA-IR, HabA1c, HDL-c, LDL-c, body mass index (BMI), waist circumference (WC), height, weight, and age. We excluded studies with no information on mean levels of osteocalcin or the previously mentioned correlations. Nondiabetic controls were those groups of individuals reported as healthy by the authors of the primary studies, namely subjects without type 1, type 2 diabetes, or carbohydrate intolerance.
The following information was extracted using a datasheet based on Cochrane Consumers and Communication Review Group's data extraction template (23): author, year of publication, the country where the study was conducted, type of study, original inclusion and exclusion criteria, diabetes type, type of osteocalcin, the method for measurement of osteocalcin, intra and inter-assay coefficient of variation, the total number of patients included in the study, the total number of participants, mean BMI and age, gender, method of quantification and brand of the kit used for the measurement. Additionally, information about the mean UV index and altitude (as surrogates of sun exposure) of the city where the study was conducted was obtained from Weather Government Agencies of each Country.
Two reviewers (FEPM & RDC) independently assessed the quality of the selected studies. In case of disagreement in the evaluation, a third researcher resolved it (JRVB or RJMP). Quality assessment of observational studies was carried out using the Newcastle–Ottawa Scale for cross-sectional studies. Each study was judged on three dimensions: the study groups' selection, the groups' comparability, and the ascertainment of exposure. One star was given for each signaling question among each dimension. The total number of possible stars were nine, and studies with six or more stars were considered high-quality, while studies with less than six were considered low-quality (24).
Before analysis, all osteocalcin values were converted to the same unit of measurement. Then extracted quantitative data were pooled in the metanalysis. For data analysis, the recommendations of Cochrane Handbook were followed as described: ucOC and tOC were compared between T1D or T2D and healthy controls. The effect size was expressed as standardized mean difference (SMD) by random-effects model (REM) weighted by the inverse of the variance since all studies used randomly sampled (25). Results are presented using forest plots of SMDs and Pearson correlations for the main groups (T1D or T2D and controls). Inter-study variability was assessed using the τ2, Cochran's Q, and I2 statistics (26). The contribution of individual study heterogeneity was visually assessed by Baujat plots (25).
Additionally, the effect size was determined for correlations (Pearson or Spearman) of tOC, ucOC, or cOC with fasting glucose, fasting insulin, HOMA-IR, HabA1c, HDL-c, LDL-c, body mass index (BMI), waist circumference (WC), height, weight, and age.
Since enough information was available only for tOC, univariate and multiple meta-regressions were performed to add another approach for unexplained heterogeneity and to determine which variables influenced tOC serum levels. The following covariates individually or combined were used: patient age, altitude, UV index, HbA1c, and method for tOC quantification. I2 and R2 values were reported to present residual heterogeneity and the amount of heterogeneity explained by each variable or by the multiple meta-regression model. Residual analysis was performed to test the validity of the multiple meta-regression model.
Publication bias was visually assessed by contour-enhanced funnel plots and quantified by Egger method. Moreover, a cumulative analysis was performed and presented as a forest plot to assess an “small study effect” defined as the chance of finding a trend towards a larger effect due to the higher probability of a small study of being published when a more “significant” result is found (27, 28). Statistical analysis was conducted using R studio v1.1.463 (R Foundation for Statistical Computing) [package “meta v4.2”].
A total of 557 studies were identified by database searching, and 45 were eligible for full-text review. After review, 20 studies were retained for the systematic review and 17 for meta-analysis. Specific reasons for excluding 25 full-text studies are presented in Supplementary S1B, including no existence of a control group, the inclusion of adults and children (mixed population) in the same analysis, or with diabetic ketoacidosis. Furthermore, studies with no observational design or failure to report osteocalcin serum levels were excluded (Figure 1). Some authors were reached by email to obtain missed data about their article, but no answer was achieved. The general characteristics of the included articles are described in Table 1 (10, 11, 15–17, 29–45).
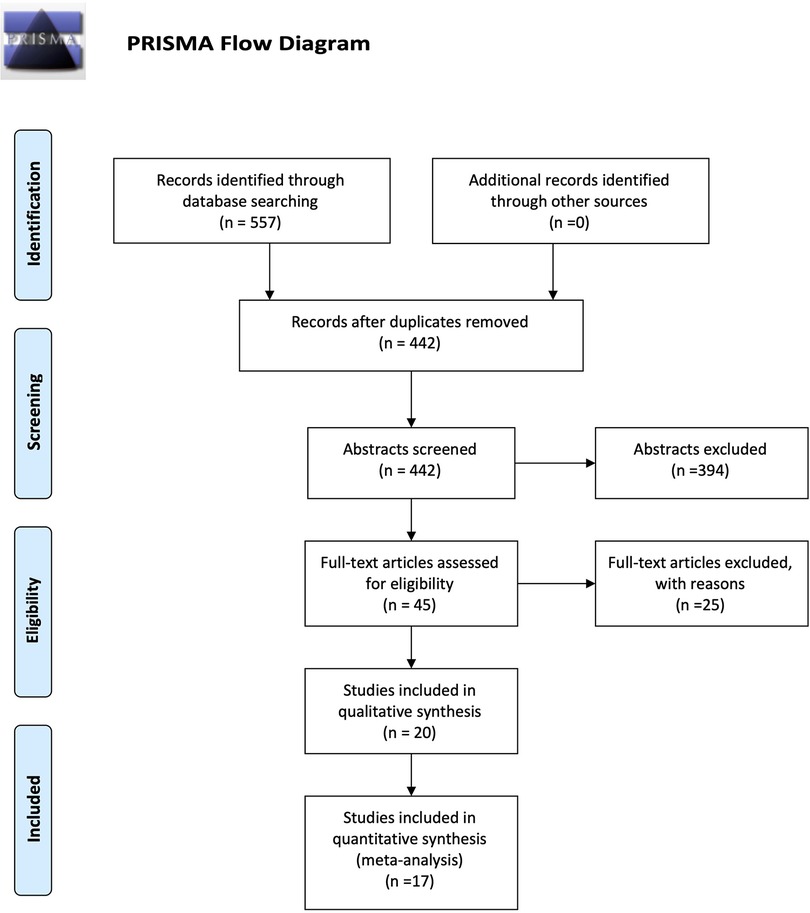
Figure 1. PRISMA flow diagram of the study.
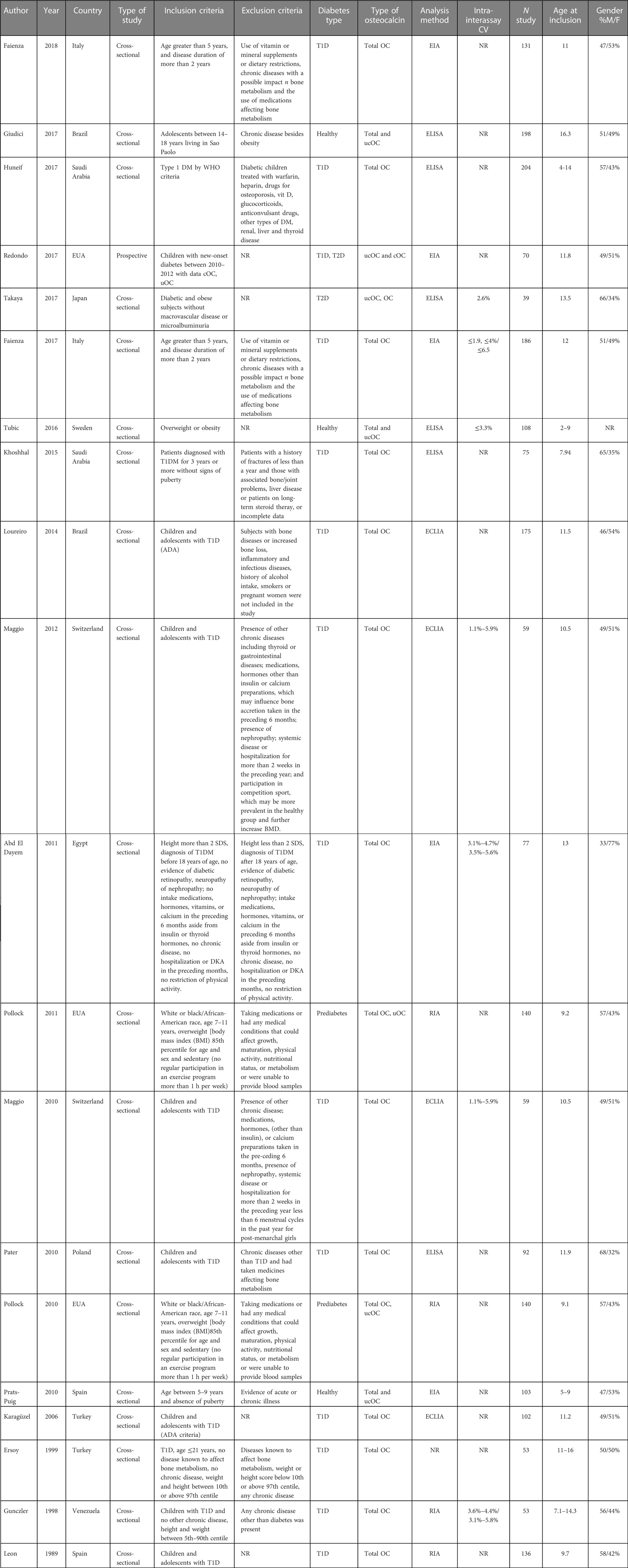
Table 1. General characteristics of the included studies.
The Newcastle–Ottawa scale was used for the quality assessment of observational studies. All studies were considered as high quality (had 6 or more points) (10, 11, 15–17, 30–35, 38, 39, 41–44) (Table 2).
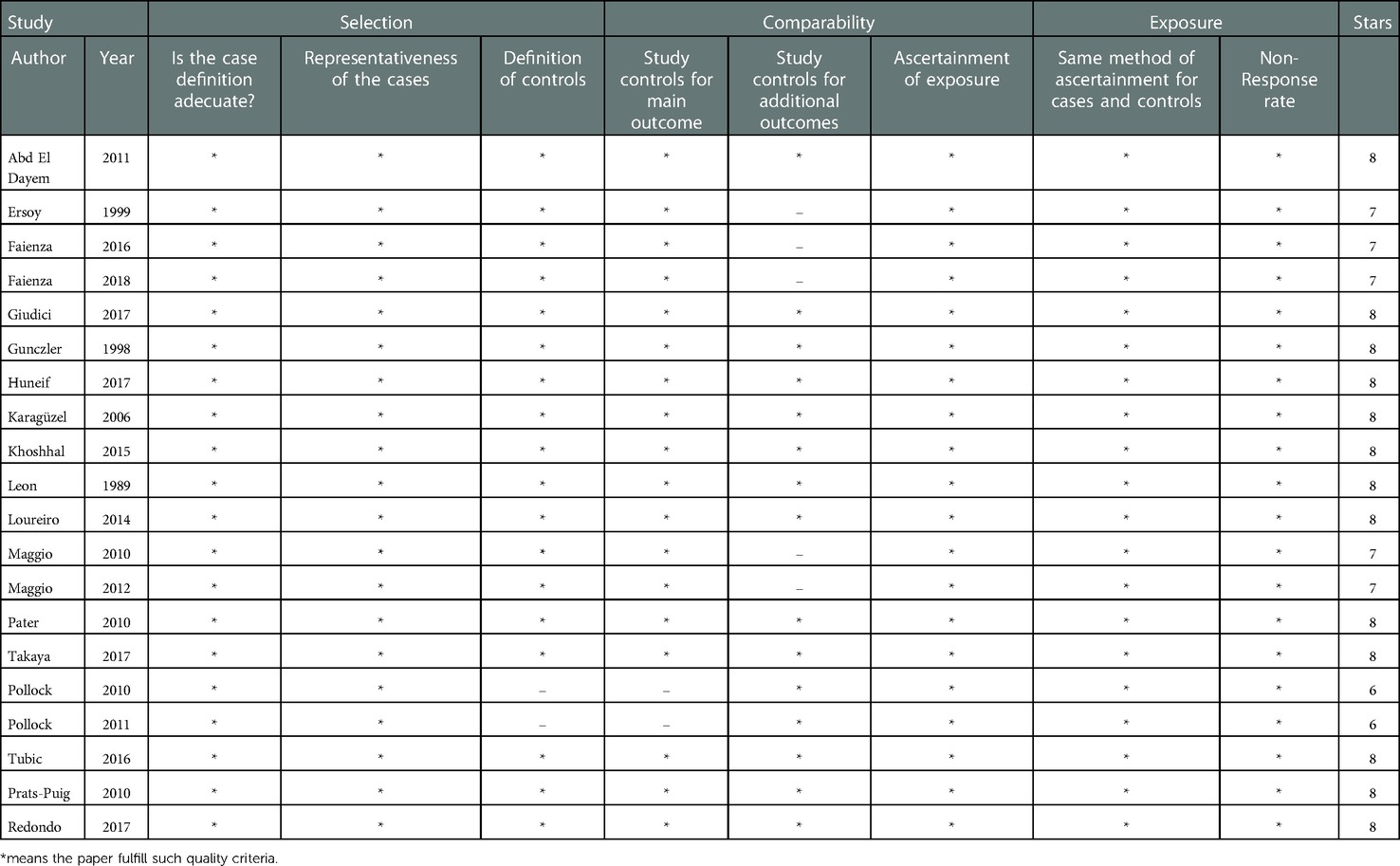
Table 2. Quality assessment of the studies included with the the Newcastle–Ottawa scale.
From the 20 included studies, a total of 3,000 pediatric patients underwent tOC, cOC, or ucOC assessment, including 983 with T1D, 30 with T2D, and 1987 healthy individuals. A total of 14 studies were performed in T1D (10, 15, 16, 30, 32, 34, 35, 39–45), two in T2D (11, 45), two in prediabetes, and three in HS. The mean patient age at inclusion was 10.6 years, and the male-to-female ratio was 1 : 0.9. The methods used for osteocalcin measurement were EIA in 5 studies (30, 35, 38, 45, 46), RIA in 4 studies (36, 37, 40, 41), ELISA in 6 studies (11, 29, 31, 43), ECLIA in 4 studies (16, 34, 42) and in one study the technique for quantification of osteocalcin was not reported. The intra-and interassay coefficients of variation were from 1.1% to 10.8%.
A total 14 studies compared the total OC serum concentrations among T1D and HS (15–17, 30, 33–35, 39–43, 47). There was lower SMD for serum levels of total OC in T1D than in HS (SMD: −2.2, CI 95%: −3.75 to −0.66). A Q value of 706.39 with 13 degrees of freedom and p < 0.001 provides evidence that the effect size varies across studies, and I2 indicates that 98.0% of the variation can be attributed to a true effect rather than a random error (Figure 2).
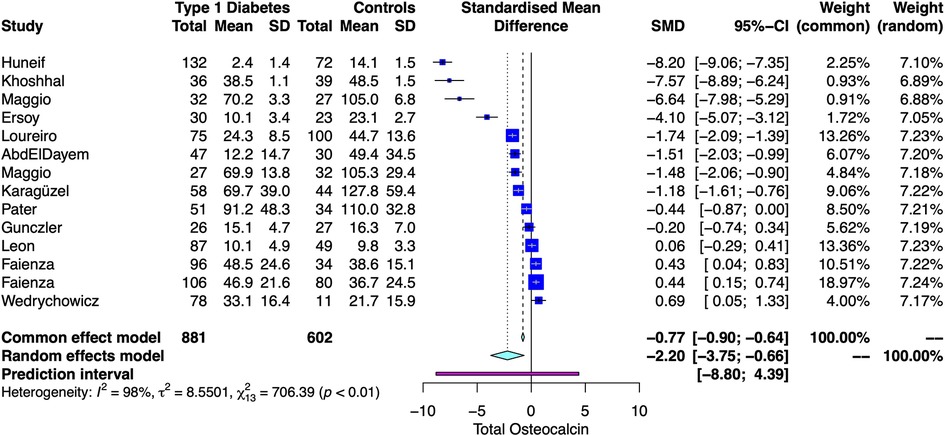
Figure 2. Forest plot with the individual results and the pooled estimates of tOC serum levels among T1D and controls.
Baujat plot showed that the studies from Faienza influenced the most to the overall results, whereas Huneif contributed the most to the overall heterogeneity (Figure 3) (15–17, 30, 35, 39, 41). The funnel plot suggested publication bias (Supplementary S2). The cumulative analysis showed no “small-study effect” on effect size (Supplementary S3).
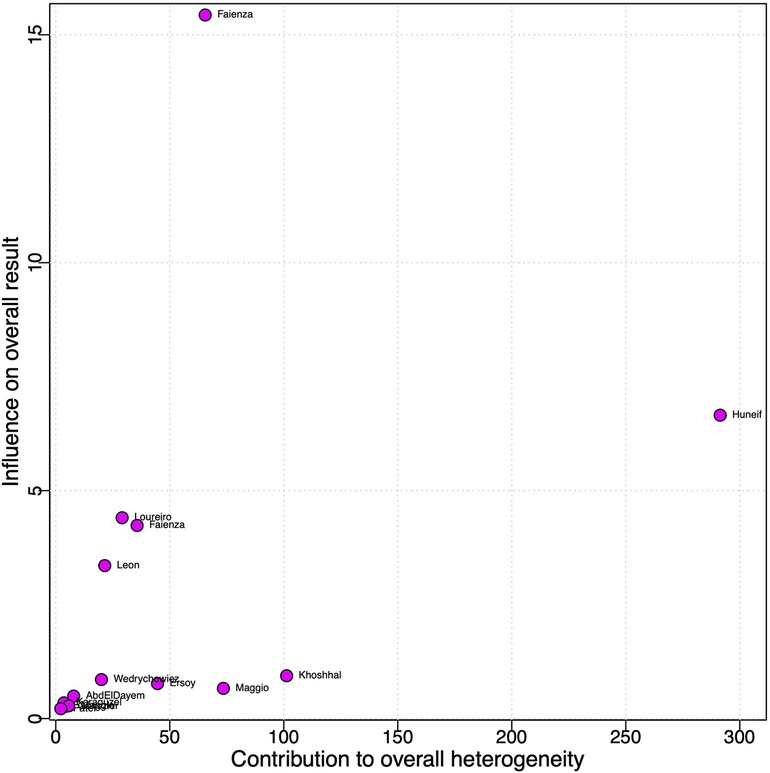
Figure 3. Baujat plot for analysis of the contribution of each study to heterogeneity in tOC serum levels.
In total, three studies compared the ucOC serum levels among individuals with abnormal glycemic status (AGS = T2D or prediabetes) and normal glycemic status. There was lower SMD for serum levels of ucOC in AGS than in HS (−1.34, CI95%: −2.42 to −0.25). A Q value of 51.95 with 2 degrees of freedom and p < 0.001 provides evidence that the effect size varies across studies, and I2 indicates that 96% of the variation can be attributed to a true effect rather than a random error (Figure 4) (11, 36, 37).
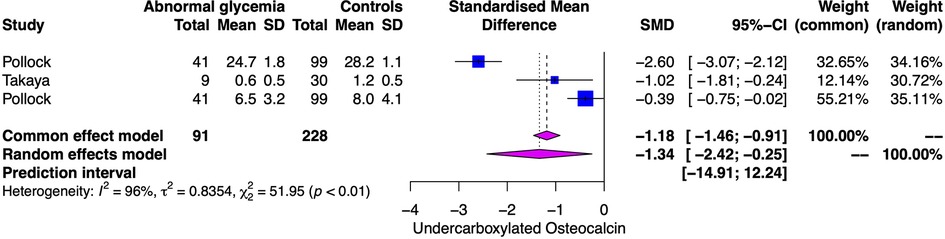
Figure 4. Forest plot with the individual results and the pooled estimates of ucOC serum levels among patients with abnormal glycemic status and controls.
Only Huneiff measured ucOC in T1D and found lower serum levels in these patients (1.08 ± 0.56 ng/ml) than in HS (2.58 ± 0.55 ng/ml) (17).
One study measured ucOC serum concentrations in pediatric patients with T2D, reporting lower ucOC serum levels among T2D (0.65 ± 0.46 ng/ml) than in controls (1.25 ± 0.49 ng/ml; p < 0.01) (11).
A total of two studies reported correlations of ucOC with metabolic and anthropometric parameters in HS (29, 31) and three in diabetic patients (11, 17, 45). In healthy subjects, significant positive correlations of ucOC with WC and weight were found but not with other parameters (Supplementary S4). In diabetic children, significant negative correlations of ucOC with HbA1c and glycemia were found in T1D and T2D (Figure 5).
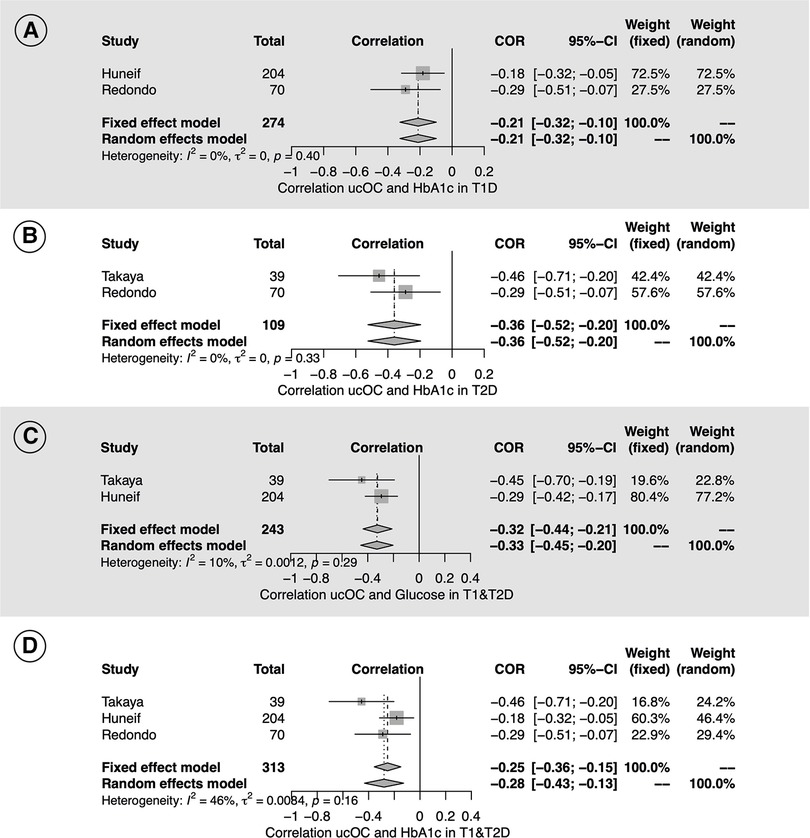
Figure 5. Forest plot with the individual results and the pooled estimates of the Pearson correlation coefficients (COR) of ucOC serum levels with HbA1c and glycemia among T1D and T2D pediatric patients.
Two studies reported correlations of tOC with metabolic and anthropometric parameters in HS (29, 31) and two in diabetic patients (30, 44). In HS, a significant positive correlation was identified for FPG, LDL-c, WC, height, and weight (Supplementary S5A–J). Among T1D children, a significant negative correlation was also found between tOC and HbA1c, but no data regarding T2D were identified in publications (Supplementary S5K).
One report compared the serum levels of cOC between HS and T2D and found no significant differences (11). No differences in T1D or T2D. Only one study performed in healthy children found that high serum levels of cOC were related to lower HMW-adiponectin in leaner children (a hormone released by osteocalcin in animals that increases insulin sensitivity). Moreover, they found that a higher ucOC-to-cOC ratio was associated with higher HOMA-β in leaner children and related with higher HMW-adiponectin in heavier children, concluding that carboxylation of osteocalcin relates to metabolic and anthropometric parameters in a weight-dependent manner (38).
Since variability was found to be high for tOC estimates, univariate and multivariate meta-regressions were performed to determine which variables influence the serum levels of tOC. In the individual meta-regressions, covariates significantly explaining the heterogeneity were patient age (R2 = 25.53%), altitude (R2 = 34.67%) and HbA1c (R2 = 26.43%) (Table 3; Figure 6).
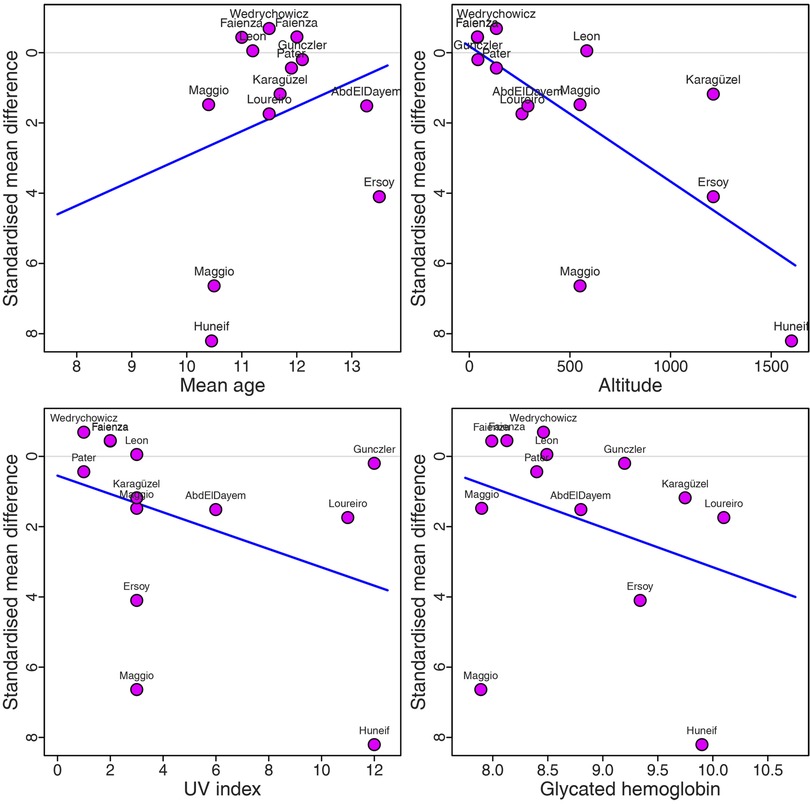
Figure 6. Meta-regressions showing variables influencing the serum levels of tOC in pediatric patients: (A) mean age. (B) Altitude. (C) UV index. (D) Glycated hemoglobin.

Table 3. Univariate meta-regression analysis of intrinsic and extrinsic determinants for tOC in T1D.
The multivariate meta-regression indicates that 62.8% of the total heterogeneity was explained by the covariate age, altitude, and HbA1c. In the moderator test, the estimated model was highly significant with QM (df = 4) = 41.21 and p < 0.0001. The patient age (p = 0.007), altitude (p = 0.008), and HbA1c (p = 0.012) have a significant influence on the levels of tOC serum, while the UV index was not significant (p = 0.64) (Table 4).
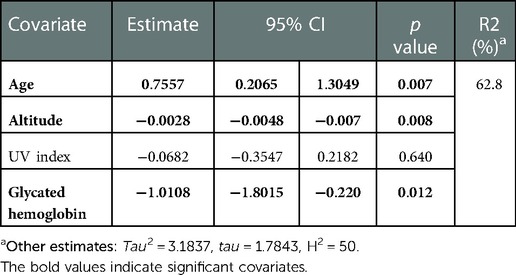
Table 4. Multivariate meta-regression analysis of intrinsic and extrinsic determinants for tOC in T1Da.
The estimated model indicates that every one-year increase in the patient's age corresponds to an increment of 0.7557 units in terms of the SMD, while keeping the other covariates constant. Similarly, for every unit of altitude increasing, the true effect size decreases at a rate of 0.0028. Finally, for every one-unit change in HbA1c, the SMD of levels of tOC serum decreases at a rate of 1.01.
Residual analysis was performed (see Supplementary S6), in which it can be noted that the assumptions of homoscedasticity, independence, and normality are satisfied—such analysis allowed the validation of the meta-regression model.
This meta-analysis revealed the following findings:
(i) Among healthy children there was a:
(a) Positive correlation of ucOC with WC and weight
(b) Positive correlation between tOC and the following parameters: FPG, LDL-c, WC, height, and weight; and a negative correlation between tOC and HbA1c.
(ii) Among diabetic children there was a:
(a) Negative correlation of ucOC with HbA1c and glycemia in both T1D and T2D.
(b) Negative correlation between tOC and HbA1c in T1D but not in T2D.
(iii) In the comparison of diabetic vs. healthy subjects:
- ucOC concentrations were lower in T2D, T1D, and patients with abnormal glucose status than among controls.
- Serum concentrations of tOC concentrations were lower in T1D than in controls.
(iv) The factors influencing serum levels of tOC were age (+), altitude (−), and glycated hemoglobin (−) explaining together 62.8% of the heterogeneity.
Since obesity, insulin resistance, glycemic, and lipid abnormalities predispose to children and adolescents to the development of chronic diseases in adulthood such as diabetes, hypertension, and cardiovascular diseases, it is quite important to identify serum markers related to abnormal metabolic phenotypes. Because osteocalcin was consistently related to FPG, HbA1c, LDL-c, WC, height, and weight in infants and adolescents, its routine clinical measurement as a marker children/adolescent metabolic status is plausible. Especially because ucOC has several metabolic effects discovered in preclinical studies, such as increased insulin synthesis, beta-cell proliferation, and insulin sensitivity throughout an action on the pancreas, adipose, and muscle tissue (48). Furthermore, a decrease in ucOC is related to fat accumulation in adipocytes and hepatocytes (49). In contrast, the administration of this hormone decreases the content of triglycerides at these cells (50), improves glucose metabolism, and prevents T2D in mice. Thus, a plausible biological explanation exists for our findings about the correlation of ucOC with glucometabolic and anthropometric parameters.
Our study has several strengths. Firstly, we conducted a rigorous systematic review by independent reviewers and a third one to evaluate and assess bias. Database searching was also done by independent investigators, all blinded to authorship and the hospital where the study was conducted, allowing us to minimize bias when selecting publications for inclusion. Secondly, the standardized mean difference was used to avoid discrepancies in unit measurements along with an exhaustive assessment of heterogeneity by 106 simulations, subgroup analysis, and meta-regression. In addition, multiple methods were used to measure bias in each group, from advanced techniques such as the Copas model to cumulative analysis, aiming to determine the trend toward higher effects in smaller studies. Finally, multiple intrinsic and extrinsic factors were analyzed by single and multivariate meta-regression to address the influence of all these factors on the variability of tOC. It allows us to understand that tOC levels were mainly influenced by age, glycemic control, and altitude but not by latitude, BMI, insulin, or other covariates. This complete analysis is a strength because it should be considered when designing clinical research involving osteocalcin or stablishing reference values. On another way, we must mention some weaknesses, including a relatively small number of studies performed in children with T2D, the use of different methods (RIA, EIA, ELISA) to measure the serum levels of osteocalcin and the non-reporting of the inter-assay coefficients of variation for all the studies. In addition, we cannot assure that the primary studies considered all factors that modify OC serum levels such as the treatment, exercise, and the season when osteocalcin was measured.
Osteocalcin is involved in energy metabolism in pediatric subjects because it is consistently related to FPG, HbA1c, LDL-c, and anthropometric parameters such as WC, height, and weight. Although serum levels of OC are highly variable among populations, such variability is explained by diverse intrinsic and extrinsic factors such as age, altitude, and glycated hemoglobin.
Moreover, its utility as a predictor of metabolic disease risk should be explored in the future, together with potential strategies to increase uCOC serum levels to improve metabolic status.
This meta-analysis provides evidence that osteocalcin is related to markers of energetic metabolism among pediatric patients with normal and abnormal glycemic status.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
SRN, RJMP and JRVB: study conception and design. GCC, BJRV, LFBG and RDC: data collection and risk of bias assessment. SRN, RJMP and JRVB: statistical analysis. SRN, RJMP, GCC and JRVB: analysis and interpretation of results. SRN, RJMP and JRVB: draft manuscript preparation. JRVB and RJMP: oversight and leadership responsibility for the research activity planning and execution. All authors contributed to the article and approved the submitted version.
We appreciate the funding of the Autonomous University of Aguascalientes during the development of this research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.1075738/full#supplementary-material.
1. Lee NK, Sowa H, Hinoi E, Ferron M, Ahn JD, Confavreux C, et al. Endocrine regulation of energy metabolism by the Skeleton. Cell. (2007) 130(3):456–69. doi: 10.1016/j.cell.2007.05.047
2. Villafän-Bernal JR, Sánchez-Enríquez S, Muñoz-Valle JF. Molecular modulation of osteocalcin and its relevance in diabetes (review). Int J Mol Med. (2011) 28(3):283–93. doi: 10.3892/ijmm.2011.706
3. Díaz-López A, Bulló M, Juanola-Falgarona M, Martínez-González MA, Estruch R, Covas MI, et al. Reduced serum concentrations of carboxylated and undercarboxylated osteocalcin are associated with risk of developing type 2 diabetes mellitus in a high cardiovascular risk population: a nested case-control study. J Clin Endocrinol Metab. (2013) 98(11):4524–31. doi: 10.1210/jc.2013-2472
4. Villafán-Bernal JR, Llamas-Covarrubias MA, Muñoz-Valle JF, Rivera-León EA, González-Hita ME, Bastidas-Ramírez BE, et al. A cut-point value of uncarboxylated to carboxylated Index is associated with glycemic Status markers in type 2 diabetes. J Invest Med. (2016) 62(1):33–6. doi: 10.2310/JIM.0000000000000015
5. Sanchez-Enriquez S, Ballesteros-Gonzalez IT, Villafán-Bernal JR, Pascoe-Gonzalez S, Rivera-Leon EA, Bastidas-Ramirez BE, et al. Serum levels of undercarboxylated osteocalcin are related to cardiovascular risk factors in patients with type 2 diabetes mellitus and healthy subjects. World J Diabetes. (2017) 8(1):11. doi: 10.4239/wjd.v8.i1.11
6. Razny U, Fedak D, Kiec-Wilk B, Goralska J, Gruca A, Zdzienicka A, et al. Carboxylated and undercarboxylated osteocalcin in metabolic complications of human obesity and prediabetes. Diabetes Metab Res Rev. (2017) 33(3):1–26. doi: 10.1002/dmrr.2862
7. Liu DM, Guo XZ, Tong HJ, Tao B, Sun LH, Zhao HY, et al. Association between osteocalcin and glucose metabolism: a meta-analysis. Osteoporos Int. (2015) 26(12):2823–33. doi: 10.1007/s00198-015-3197-8
8. Kunutsor SK, Apekey TA, Laukkanen JA. Association of serum total osteocalcin with type 2 diabetes and intermediate metabolic phenotypes: systematic review and meta-analysis of observational evidence. Eur J Epidemiol. (2015) 30(8):599–614. doi: 10.1007/s10654-015-0058-x
9. Martinez-Portilla RJ, Villafan-Bernal JR, Lip-Sosa DL, Meler E, Clotet J, Serna-Vela FJ, et al. Osteocalcin serum levels in gestational diabetes Mellitus and their intrinsic and extrinsic determinants: systematic review and meta-analysis. J Diabetes Res. (2018) 2018:4986735. doi: 10.1155/2018/4986735
10. Loureiro MB, Ururahy MAG, Freire-Neto FP, Oliveira GHM, Duarte VMG, Luchessi AD, et al. Low bone mineral density is associated to poor glycemic control and increased OPG expression in children and adolescents with type 1 diabetes. Diabetes Res Clin Pract. (2014) 103(3):452–7. doi: 10.1016/j.diabres.2013.12.018
11. Takaya J, Tanabe Y, Kuroyanagi Y, Kaneko K. Decreased undercarboxylated osteocalcin in children with type 2 diabetes mellitus. J Pediatr Endocrinol Metab. (2016) 29(8):879–84. doi: 10.1515/jpem-2015-0417
12. Wada S, Kamiya S. Bone and bone related biochemical examinations. Bone and collagen related metabolites. Osteocalcin (OC). Clin Calcium. (2006) 16(6):1017–21. PMID: 16751699.16751699
13. Tripathi T, Gupta P, Rai P, Sharma J, Gupta VK, Singh N. Osteocalcin and serum insulin-like growth factor-1 as biochemical skeletal maturity indicators. Prog Orthod. (2017) 18(1):1–8. doi: 10.1186/s40510-017-0184-y
14. Johansen JS, Giwercman A, Hartwell D, Nielsen CT, Price PA, Christiansen C, et al. Serum bone gla-protein as a marker of bone growth in children and adolescents: correlation with age, height, Serum insulin-like growth factor I, and Serum testosterone. J Clin Endocrinol Metab. (1988) 67(2):273–8. doi: 10.1210/jcem-67-2-273
15. Khoshhal KI, Sheweita SA, Al-Maghamsi MS, Habeb AM. Does type 1 diabetes mellitus affect bone quality in prepubertal children? J Taibah Univ Med Sci. (2015) 10(3):300–5. doi: 10.1016/j.jtumed.2015.03.004
16. Karagüzel G, Akcurin S, Özdem S. Bone mineral density and alterations of bone metabolism in children and adolescents with type 1 diabetes mellitus. J Pediatr Endocrinol Metab. (2006) 19(6):805–14. doi: 10.1515/JPEM.2006.19.6.805
17. Faris Shalayel MH. Type 1 diabetes mellitus (T1DM) in toddlers and schoolchildren in Najran region, Southwestern Saudi Arabia. Med J Aust. (2018) 10(12):981–8. doi: 10.21767/AMJ.2017.3184
18. Ferron M, Hinoi E, Karsenty G, Ducy P. Osteocalcin differentially regulates β cell and adipocyte gene expression and affects the development of metabolic diseases in wild-type mice. Proc Natl Acad Sci U S A. (2008) 105(13):5266–70. doi: 10.1073/pnas.0711119105
19. Ferron M, McKee MD, Levine RL, Ducy P, Karsenty G. Intermittent injections of osteocalcin improve glucose metabolism and prevent type 2 diabetes in mice. Bone. (2012) 50(2):568–75. doi: 10.1016/j.bone.2011.04.017
20. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of Observational Studies. JAMA. (2000) 283(15):2008–12. doi: 10.1001/jama.283.15.2008
21. Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D, Antes G, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement (Chinese edition). Chin J Integr Med. (2009) 7(9):889–96. doi: 10.3736/jcim20090918
22. Stovold E, Beecher D, Foxlee R, Noel-Storr A. Study flow diagrams in cochrane systematic review updates: an adapted PRISMA flow diagram. Syst Rev. (2014) 3(54):1–5. doi: 10.1186/2046-4053-3-54
23. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration (2011). Available at www.handbook.cochrane.org (updated March 2011).
24. Stang A. Critical evaluation of the Newcastle–Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25(9):603–5. doi: 10.1007/s10654-010-9491-z
25. Baujat B, Mahé C, Pignon JP, Hill C. A graphical method for exploring heterogeneity in meta-analyses: application to a meta-analysis of 65 trials. Stat Med. (2002) 21(18):2641–52. doi: 10.1002/sim.1221
26. Borenstein M, Higgins JPT, Hedges LV, Rothstein HR. Basics of meta-analysis: i2 is not an absolute measure of heterogeneity. Res Synth Methods. (2017) 8(1):5–18. doi: 10.1002/jrsm.1230
27. Lau J, Schmid CH, Chalmers TC. Cumulative meta-analysis of clinical trials builds evidence for exemplary medical care. J Clin Epidemiol. (1995) 48(1):45–57. doi: 10.1016/0895-4356(94)00106-Z
28. Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to meta-analysis part 5: complex data structures. In: Wiley Online Library, Second Edition. Introduction to meta-analysis. New York: John Wiley & Sons, Ltd (2009). p. 213–45.
29. Giudici KV, Fisberg RM, Marchioni DML, Peters BSE, Martini LA. Crosstalk between bone and fat tissue: associations between vitamin D, osteocalcin, adipokines, and markers of glucose metabolism among adolescents. J Am Coll Nutr. (2017) 36(4):273–80. doi: 10.1080/07315724.2016.1274923
30. Faienza MF, Ventura A, Delvecchio M, Fusillo A, Piacente L, Aceto G, et al. High sclerostin and dickkopf-1 (DKK-1) serum levels in children and adolescents with type 1 diabetes mellitus. J Clin Endocrinol Metab. (2017) 102(4):1174–81. doi: 10.1210/jc.2016-2371
31. Tubic B, Magnusson P, Mårild S, Leu M, Schwetz V, Sioen I, et al. Different osteocalcin forms, markers of metabolic syndrome and anthropometric measures in children within the IDEFICS cohort. Bone. (2016) 84:230–6. doi: 10.1016/j.bone.2016.01.008
32. Tsentidis C, Gourgiotis D, Kossiva L, Doulgeraki A, Marmarinos A, Galli-Tsinopoulou A, et al. Higher levels of s-RANKL and osteoprotegerin in children and adolescents with type 1 diabetes mellitus may indicate increased osteoclast signaling and predisposition to lower bone mass: a multivariate cross-sectional analysis. Osteoporos Int. (2016) 27(4):1631–43. doi: 10.1007/s00198-015-3422-5
33. Wędrychowicz A, Stec M, Sztefko K, Starzyk JB. Associations between bone, fat tissue and metabolic control in children and adolescents with type 1 diabetes mellitus. Exp Clin Endocrinol Diabetes. (2014) 122(8):491–5. doi: 10.1055/s-0034-1375666
34. Maggio ABR, Rizzoli RR, Marchand LM, Ferrari S, Beghetti M, Farpour-Lambert NJ. Physical activity increases bone mineral density in children with type 1 diabetes. Med Sci Sports Exerc. (2012) 44(7):1206–11. doi: 10.1249/MSS.0b013e3182496a25
35. Abd El Dayem SM, El-Shehaby AM, Abd El Gafar A, Fawzy A, Salama H. Bone density, body composition, and markers of bone remodeling in type 1 diabetic patients. Scand J Clin Lab Invest. (2011) 71(5):387–93. doi: 10.3109/00365513.2011.573574
36. Pollock NK, Bernard PJ, Gower BA, Gundberg CM, Wenger K, Misra S, et al. Lower uncarboxylated osteocalcin concentrations in children with prediabetes is associated with β-cell function. J Clin Endocrinol Metab. (2011) 96(7):1092–9. doi: 10.1210/jc.2010-2731
37. Pollock NK, Bernard PJ, Wenger K, Misra S, Gower BA, Allison JD, et al. Lower bone mass in prepubertal overweight children with prediabetes. J Bone Miner Res. (2010) 25(12):2484–93. doi: 10.1002/jbmr.184
38. Prats-Puig A, Mas-Parareda M, Riera-Pérez E, González-Forcadell D, Mier C, Mallol-Guisset M, et al. Carboxylation of osteocalcin affects its association with metabolic parameters in healthy children. Diabetes Care. (2010) 33(3):661–3. doi: 10.2337/dc09-1837
39. Ersoy B, Gökşen D, Darcan S, Mavi E, Öztürk C. Evaluation of bone mineral density in children with diabetes mellitus. Indian J Pediatr. (1999) 66(3):375–9. doi: 10.1007/BF02845528
40. Leon M, Larrodera L, Lledo G, Hawkins F. Study of bone loss in diabetes mellitus type 1. Diabetes Res Clin Pract. (1989) 6(3):237–42. doi: 10.1016/0168-8227(89)90035-1
41. Gunczler P, Lanes R, Paz-Martinez V, Martinis R, Esaa S, Colmenares V, et al. Decreased lumbar spine bone mass and low bone turnover in children and adolescents with insulin dependent diabetes mellitus followed longitudinally. J Pediatr Endocrinol Metab. (1998) 11(3):413–9. doi: 10.1515/JPEM.1998.11.3.413
42. Maggio ABR, Ferrari S, Kraenzlin M, Marchand LM, Schwitzgebel V, Beghetti M, et al. Decreased bone turnover in children and adolescents with well controlled type 1 diabetes. J Pediatr Endocrinol Metab. (2010) 23(7):697–707. doi: 10.1515/jpem.2010.23.7.697
43. Pater A, Sypniewska G, Pilecki O. Biochemical markers of bone cell activity in children with type 1 diabetes Mellitus. J Pediatr Endocrinol Metab. (2010) 23(1–2):81–6. doi: 10.1515/jpem.2010.23.1-2.81
44. Guarneri MP, Weber G, Gallia P, Chiumello G. Effect of insulin treatment on osteocalcin levels in diabetic children and adolescents. J Endocrinol Invest. (1993) 16(7):505–9. doi: 10.1007/BF03348892
45. Redondo MJ, Shirkey BA, Fraga DW, Gaber AO, Sabek OM. Serum undercarboxylated osteocalcin correlates with hemoglobin A1c in children with recently diagnosed pediatric diabetes. Pediatr Diabetes. (2017) 18(8):869–73. doi: 10.1111/pedi.12501
46. Faienza MF, Brunetti G, Sanesi L, Colaianni G, Celi M, Piacente L, et al. High irisin levels are associated with better glycemic control and bone health in children with type 1 diabetes. Diabetes Res Clin Pract. (2018) 141:10–7. doi: 10.1016/j.diabres.2018.03.046
47. Huneif MA, Homada EEH, Fadlelseed OE, Hamid HGM, Shalayel MHF. Type 1 diabetes mellitus (T1DM) in toddlers and schoolchildren in Najran region, Southwestern Saudi Arabia–correlation with osteocalcin and vitamin D. Med J Aust. (2017) 10(12):981–8. PMID: 21666940.
48. Mera P, Laue K, Ferron M, Confavreux C, Wei J, Galán-Díez M, et al. Osteocalcin signaling in myofibers is necessary and sufficient for optimum adaptation to exercise. Cell Metab. (2016) 23(6):1078–92. doi: 10.1016/j.cmet.2016.05.004
49. Diaz-Franco MC, Franco-Diaz de Leon R, Villafan-Bernal JR. Osteocalcin-GPRC6A: an update of its clinical and biological multi-organic interactions (review). Mol Med Rep. (2019) 19(1):15–22. doi: 10.3892/mmr.2018.9627
Keywords: osteocalcin, energetic metabolism, glucose - insulin, pediatric patient, systematic review & meta-analysis
Citation: Rodríguez-Narciso S, Martínez-Portilla RJ, Guzmán-Guzmán IP, Careaga-Cárdenas G, Rubio-Navarro BJ, Barba-Gallardo LF, Delgadillo-Castañeda R and Villafan-Bernal JR (2023) Osteocalcin serum concentrations and markers of energetic metabolism in pediatric patients. Systematic review and metanalysis. Front. Pediatr. 10:1075738. doi: 10.3389/fped.2022.1075738
Received: 20 October 2022; Accepted: 13 December 2022;
Published: 12 January 2023.
Edited by:
Jessie Zurita-Cruz, Hospital Infantil de México Federico Gómez, MexicoReviewed by:
Lourdes Barbosa, Mexican Social Security Institute (IMSS), Mexico© 2023 Villafan Bernal, Rodríguez-Narciso, Martinez-Portilla, Careaga-Cárdenas, Rubio-Navarro, Barba Gallardo and Delgadillo-Castañeda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Rafael Villafan-Bernal am9yYXZpYmVAZ21haWwuY29t
Specialty Section: This article was submitted to Pediatric Endocrinology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.