 María Lasa-Lázaro1
María Lasa-Lázaro1 Esther Ramos-Boluda2Esther Mancebo1María José Castro-Panete1Rocío González-Sacristán2Javier Serradilla3,4
Esther Ramos-Boluda2Esther Mancebo1María José Castro-Panete1Rocío González-Sacristán2Javier Serradilla3,4 Ane Miren Andrés-Moreno3,4
Ane Miren Andrés-Moreno3,4 Francisco Hernández-Oliveros3,4
Francisco Hernández-Oliveros3,4 Estela Paz-Artal1,5,6
Estela Paz-Artal1,5,6 Paloma Talayero1*
Paloma Talayero1*
- 1Department of Immunology, University Hospital 12 de Octubre, Instituto de Investigación Sanitaria Hospital 12 de Octubre (imas12), Madrid, Spain
- 2Unit of Intestinal Rehabilitation and Transplant, University Hospital La Paz, Madrid, Spain
- 3Department of Pediatric Surgery, University Hospital La Paz, Madrid, Spain
- 4IdiPaz Research Institute, University Hospital La Paz, Madrid, Spain
- 5School of Medicine, Complutense University, Madrid, Spain
- 6CIBER de Enfermedades Infecciosas, ISCIII, Madrid, Spain
Background: Donor-specific anti-HLA antibodies (DSA) impact negatively on the outcome of intestinal grafts. Although the use of antibody-removal therapies (ART) is becoming more frequent in the last few years, issues regarding their timing and effectiveness remain under discussion.
Methods: In the present study, we report our experience with eight ART procedures (based on plasmapheresis, intravenous immunoglobulin, and rituximab) in eight pediatric intestinal and multivisceral transplants with de novo DSA (dnDSA).
Results: ART were performed when dnDSA appeared in two contexts: (1) concomitant with rejection (acute or chronic) or (2) without rejection or any other clinical symptom. Complete DSA removal was observed in seven out of eight patients, showing an effectiveness of 88%. In the group treated for dnDSA without clinical symptoms, the success rate was 100%, with complete DSA removal and without rejection afterward. A shorter time between DSA detection and ART performance appeared as a significant factor for the success of the therapy (p = 0.0002). DSA against HLA-A and DQ alleles were the most resistant to ART, whereas anti-DR DSA were the most sensitive. In addition, the 8-year allograft survival rate in recipients undergoing ART was similar to that in those without DSA, being significantly lower in non-treated DSA-positive recipients (p = 0.013).
Conclusion: The results confirm the effectiveness of ART in terms of DSA removal and allograft survival and encourage its early use even in the absence of clinical symptoms.
Introduction
The long-term functionality of intestinal grafts continues to pose a challenge, with the 5-year graft survival rate remaining stagnant at approximately 50% (1). While sepsis and acute cellular rejection are the leading causes of early graft loss and mortality, infections, renal failure, antibody-mediated rejection, and chronic rejection impair long-term graft and patient survival (2).
The deleterious role of anti-HLA donor-specific antibodies (DSA) in intestinal transplantation (ITx) has become more evident in recent years. The presence of de novo DSA (dnDSA) has been associated with decreased allograft survival and a higher incidence and severity of rejection (3–6). Indeed, they have been previously shown as an independent risk factor for 5-year allograft loss with a hazard ratio (HR) of 6.54 (6).
Antibody-removal therapies (ART) in solid organ transplantation include different approaches. Plasmapheresis and intravenous immunoglobulin (IVIG) are usually the first choices of treatment as they quickly remove circulating DSA. The anti-CD20 monoclonal antibody rituximab, which depletes B lymphocytes, is commonly used in combination with the two aforementioned or as second-line therapy. Other strategies for refractory cases include drugs targeting plasma cells (like proteasome inhibitors such as bortezomib and more recently anti-CD38 antibodies), complement molecules (such as the anti-C5 monoclonal antibody eculizumab), or different components of costimulatory pathways (IL6/IL6-receptor antibodies, B7-CD28 complex, etc.) (7–9).
The use of ART in ITx has extended, as evidence of the harmful effects of DSA has increased. Even though ART are used in most centers for preformed DSA (10, 11), there is still no consensus regarding DSA removal in post-transplantation. Although most centers agree on the treatment of the humoral component in the context of acute rejection (both antibody-mediated rejection alone and mixed cellular/humoral rejection), ART in the absence of clinical symptoms remain controversial. The reasons to delay treatment are several, from technical problems stemming from the need for central vein access to logistic issues such as hospitalization or the possibility of infectious complications due to B cell depletion.
In this study, we perform a retrospective analysis of the ART experience of our pediatric ITx cohort for dnDSA, with a focus on the factors that may influence the outcome, and also the effectiveness in terms of graft survival.
Materials and methods
Study cohort
The study included a cohort of 92 recipients of 118 transplants performed at the University Hospital La Paz between 1999 and 2021. This cohort was partially described previously by our group (6). Transplants without a DSA study or those in which donor HLA typing was unknown were excluded from the analysis. Transplants with preformed DSA were also excluded in order to study “pure” dnDSA recipients. Eventually, a total of 76 transplants from 67 patients were included (Figure 1A).
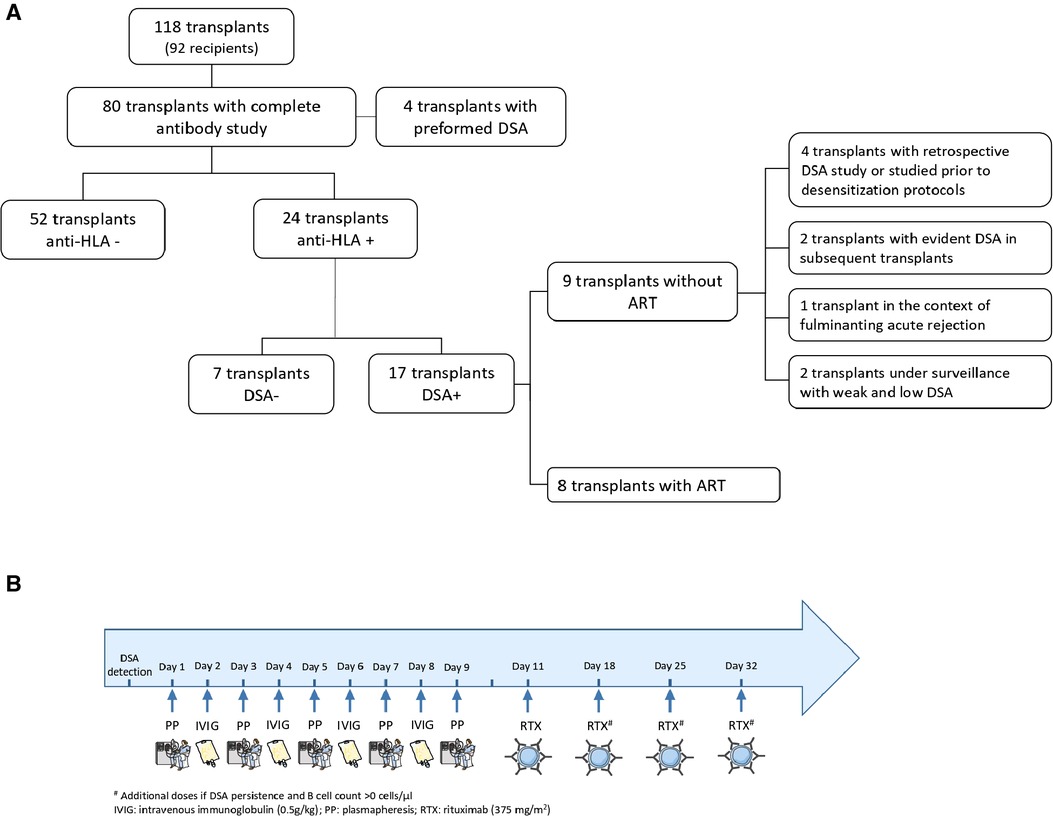
Figure 1. (A) Description of the studied cohort. (B) Antibody-removal protocol for de novo DSA.
The median age at transplant of this final cohort was 3.3 years (Table 1), with a median follow-up time of 6.9 years. The primary causes of transplantation were short bowel syndrome (48 transplants), motility disorders (13 transplants), congenital mucosal disorders (11 transplants), and others (4 transplants). A total of 59 transplants were first transplants, while 17 were retransplants. A total of 63 transplants included the liver (11 liver intestine and 52 multivisceral), whereas 13 were liver-excluded grafts (10 isolated intestinal grafts and 3 modified multivisceral).
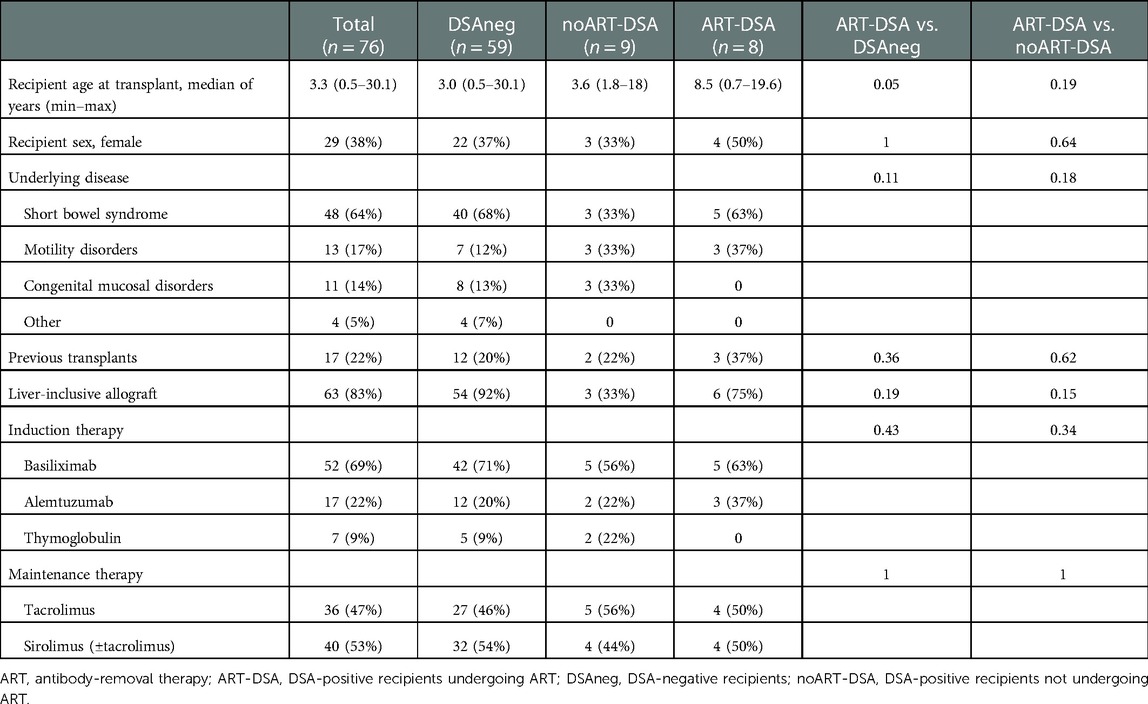
Table 1. Demographic and clinical characteristics of the final studied cohort.
Immunosuppression and ART protocol
Different induction protocols were used as previously reported (12) (Table 1). Maintenance immunosuppression was based on tacrolimus (blood levels of 10–15 ng/ml until the 3rd month and 5–10 ng/ml from the 3rd month onward). When induction was made with basiliximab, corticosteroids were also required as part of maintenance therapy. Sirolimus (2 mg/m2 daily with blood levels in the 5–10 ng/ml range) was used according to what was previously reported by our group (12) in 40 transplants (8 combined with tacrolimus and 32 in monotherapy).
The standard post-transplant ART protocol consisted of five plasmapheresis sessions together with four doses of 0.5 g/kg IVIG (a total of 2 g/kg) on alternate days. Rituximab was administered 24–48 h later in boluses of 375 mg/m2 once a week up to a maximum of 4 weeks (Figure 1B). ART was initiated when DSA with a mean fluorescence intensity (MFI) higher than 2000 appeared.
Graft monitoring was based on symptoms, and endoscopic biopsies were performed only when rejection was clinically suspected. Rejection diagnosis was made on the basis of both clinical and histological data. Clinical symptoms were fever, nausea, vomiting, diarrhea, abdominal pain and distension, and increased stomal effluent volume. A histological diagnosis (with at least two independent pathologists) was made according to previously reported criteria (13, 14).
Anti-HLA antibody study
Sera for the period before 2010 were collected pre-transplant and studied retrospectively. From 2010 onward, they were prospectively analyzed before transplant, at 15 days post-transplant, 1 month, 3 months, 6 months, and every 6 months thereafter, and when clinical events appeared.
Anti-HLA antibodies were tested by using Luminex Technology. A LABScreen Mix (LSM) kit (One Lambda, CA, USA) was used for the initial screening. The test was considered positive when standard fluorescence intensity (SFI) was more than 15.000 for anti-HLA class I or above 20.000 for anti-HLA class II. Specificities were determined by using a LABScreen Single Antigen (LSA) kit (One Lambda, CA, USA). An MFI of over 500 was considered positive. The C1q binding assay was performed with a C1qScreen kit (One Lambda, CA, USA). The test was considered positive when the MFI was more than 500.
Statistical analysis
A statistical analysis of categorical data frequencies was carried out using Fisher's exact test or a Chi-square test. The significance of differences when comparing quantitative data was determined using the Mann–Whitney U test. For correlation analysis, Spearman's Rho was calculated. Kaplan–Meier and log-rank tests were used to perform survival analysis among groups. P-values <0.05 were considered significantly different. GraphPad Prism software (version 8.0.2) was used for the analysis.
Results
ART indications and protocols
From the final cohort of 76 transplants, dnDSA were detected in 17 patients. Of these, nine did not undergo ART (noART-DSA) because of different reasons (Figure 1A) and eight DSA-positive transplants, underwent ART (Table 2). Six recipients had multivisceral grafts and two had isolated intestinal grafts. No significant differences were observed in the recipients' clinical characteristics between this group and the DSAneg and noART-DSA groups (Table 1).
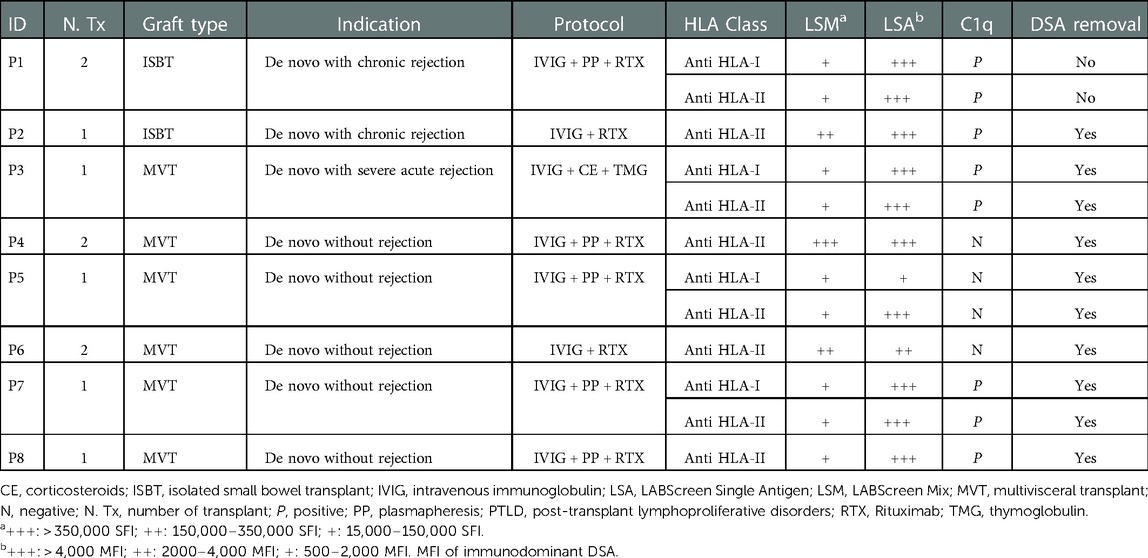
Table 2. Summary of the ART carried out.
ART was administered when dnDSA appeared in either of two scenarios: (1) acute or chronic rejection (n = 3) or (2) no rejection or any other clinical symptom (n = 5). Altogether, eight ART procedures (matching each one to one transplant from one single recipient) were performed (Table 2).
In five procedures, the standard therapy with plasmapheresis, IVIG, and rituximab (Table 2, Figure 1B) was used. In another two procedures, IVIG and rituximab were used without plasmapheresis because of the difficulty in gaining access to the central vein. Only in the recipient with dnDSA concomitant to an acute rejection episode (P3), the therapy was changed (IVIG plus thymoglobulin and corticosteroids) in order to also treat the rejection cellular component.
ART was effective in 88% of the recipients
We first defined ART effectiveness in terms of DSA removal as follows: (A) a full negativization of anti-HLA antibodies (LSM negative) or (B) no DSA detection in LSA (DSA MFI <500), maintained at least for 1 year in both cases.
In the context of dnDSA appearance concomitant with rejection, ART was administered to three recipients. In the first patient (P1), DSA monitoring started 3 years after transplantation, revealing then the existence of DSA vs. A23, A29, and DQ5 with positivity for C1q assay for A29 and DQ5 (Figure 2). However, she was not treated until chronic rejection was diagnosed 1 year later. Then, the standard therapy with plasmapheresis, IVIG, and rituximab was applied, however, with no effect, as there was no increase in antibody levels or no clinical improvement, with only subsequent graft loss.
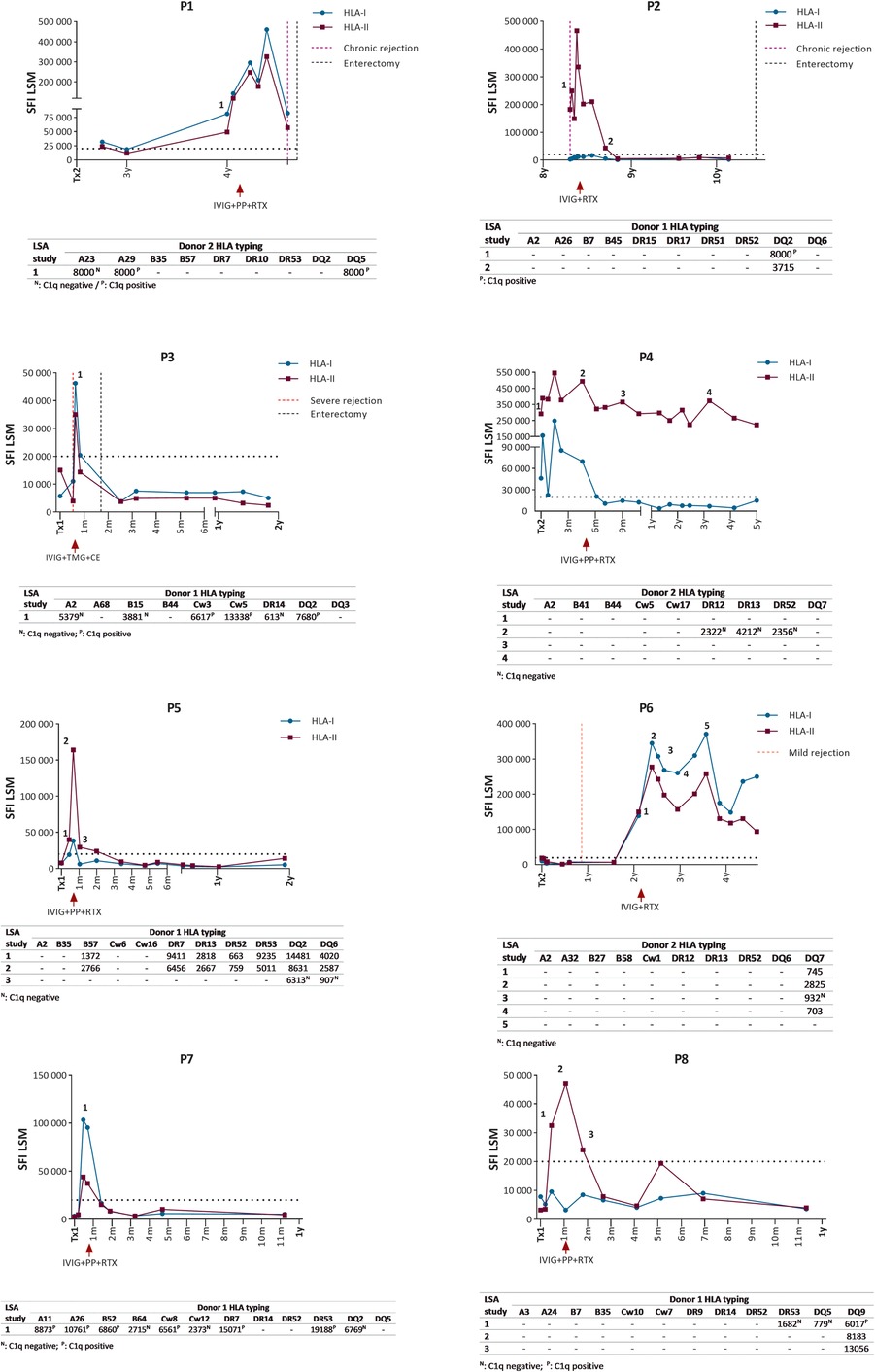
Figure 2. Evolution of anti-HLA antibodies levels (SFI) and DSA MFI in the eight treated recipients. Antibody-removal procedures and important clinical events are represented. CE, corticosteroids; HLA-I, anti-HLA class-I antibodies; HLA-II, anti-HLA class-II antibodies; IVIG, intravenous immunoglobulin; LSA, LABScreen single antigen; LSM, LABScreen Mix; PP, plasmapheresis; RTX, rituximab; TMG, thymoglobulin.
Patient 2 was first monitored for DSA in the context of a chronic 8-year post-transplantation, and complement-fixing DSA vs. DQ2 was noted. For this reason, she was treated with IVIG and rituximab (no plasmapheresis was done because of a lack of vein access), and although DSA quickly disappeared, allograft loss could not be avoided.
Patient 3 suffered from a severe acute rejection in the early post-transplant period with high MFI DSA vs. multiple specificities, several of them being C1q-positive (Figure 2). He was treated with corticosteroid, thymoglobulin, and IVIG, achieving a fast DSA clearance. Nonetheless, intestinal graft loss was unavoidable, and he was enterectomized, however keeping the liver, pancreas, stomach, and duodenum grafts intact.
Therefore, although DSA removal was done in two out of the three recipients from this group (67% effectiveness), graft loss could not be avoided in any of the cases.
In five more patients (P4, P5, P6, P7, and P8), ART was administered because of dnDSA appearance in the absence of any clinical events or rejection signs. All DSA were removed in all patients (100% effectiveness) and no rejection occurred in any of the recipients after ART. No rebound was observed in any patient, and the median follow-up time was 2 years (1–6.2 years).
Therefore, considering all recipients together, ART was effective in 88% of them (7/8) (Table 2).
Time from DSA detection to ART is a significant factor for a successful outcome
An important issue under debate is the timing of ART and especially when DSA are present with good graft function. Because we observed that in patients with delayed ART, DSA were more resistant, we analyzed whether the time from DSA detection to therapy performance had any impact on the outcome. We observed that the time was significantly shorter for cleared than for persistent DSA (7 days vs. 433 days; p = 0.0002; Figure 3A), and it also significantly correlated with the time until DSA clearance (p = <0.0001; r2 = 0.86; Figure 3A).
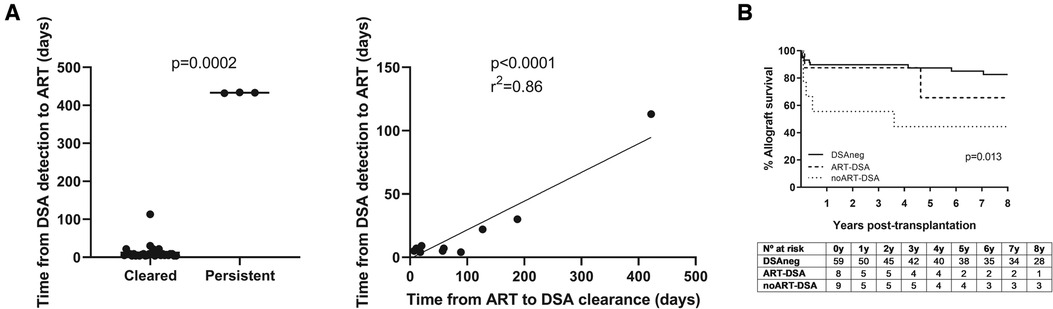
Figure 3. (A) Analysis of the elapsed time between DSA detection and antibody-removal procedure: comparison in cleared and persistent DSA and correlation with the time until DSA clearance. (B) Eight-year graft survival analysis in DSAneg, ART-DSA, and noART-DSA recipients.
Analyzing other possible factors (previously reported by others) such as HLA specificity or DSA intensity, we found that DSA against HLA-A alleles were the most resistant (60% of clearance), while DQ alleles were the ones that took the longest time to get cleared (with a 89% clearance rate and a median clearance time of 74 days). Anti-DR DSA were the most sensitive to ART (with a 100% clearance rate and a median time of 18 days) (Supplementary Table S1). As far as MFI was concerned, it was higher for persistent than for cleared DSA (median MFI: persistent = 8,354, cleared = 5,698), although this difference was not significant due to the low number of persistent DSA (p = 0.21).
Long-term allograft survival rate in treated recipients is similar to that in DSA-negative patients
After analyzing ART effectiveness in terms of DSA removal, we wanted to determine whether it had any impact on graft survival. The starkest contrast was observed at 1-year post-transplantation, with a 90% survival rate in the DSAneg and ART-DSA groups but only 50% in noART-DSA recipients (Figure 3B). Significant differences among the three groups were also maintained in the long term (p = 0.013), with 8-year allograft survival rate in DSAneg recipients being similar to that in ART-DSA patients (p = 0.37) but not to that in the noART-DSA group (p = 0.0033). Importantly, DSA characteristics were similar between the ART-DSA and the noART-DSA groups (Supplementary Table S2).
It is well known that one of the main factors affecting graft survival is rejection. In our ART-DSA group, the rejection rate before the therapy was 37.5% (Table 3), which belonged to the three transplants in which dnDSA appeared together with rejection (P1, P2, and P3). After excluding these three patients who lost their grafts and then the rejection rate after the ART could not be evaluated, no rejection episodes were observed in the remaining five cases. This rejection rate strongly differed from that observed in the noART-DSA group (p = 0.021).
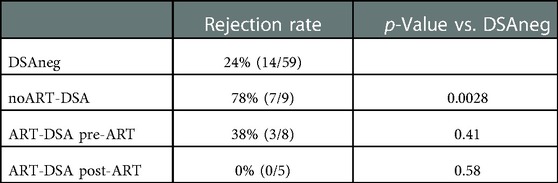
Table 3. Rejection rates in different recipient groups.
With regard to possible complications after ART, only one patient suffered from a catheter-associated bacteremia 1 month after the therapy. No further complications were observed, which underlined the safety of ART.
Discussion
The harmful effect of DSA (either preformed, de novo, or persistent) on ITx has been described in the last few years by several groups (3–5). Our previous report including 43 transplants from 36 recipients showed a deleterious impact of dnDSA on graft rejection (HR = 10.39) and survival (HR = 66.52), being an independent risk factor for 5-year allograft loss (6).
As this evidence emerged, ART was implemented. Most centers agree on the use of plasmapheresis, IVIG, and rituximab for humoral component treatment in the context of rejection (15–17). Nevertheless, ART in the absence of clinical symptoms remains controversial. While some groups support the idea of dnDSA removal soon after their appearance (15, 16) or similar treatment for strong DSA (5, 18), some centers are still reluctant to carry out such procedures without the appearance of any signs of rejection. The limited experience with the lack and disparity of information about ART indications and outcomes and technical, logistic, and clinical complications arising from the treatment are the main reasons for delaying such therapies.
In our cohort, preformed antibodies in the first transplant was mostly absent, with only 1 patient case reported from the 64 studied (data were unavailable for the remaining cases), which meant that, except in this one patient, all DSA were generated after transplantation. When we began DSA monitoring, we actually observed that DSA were mostly present in those patients with previous transplants and who had experienced severe and/or chronic rejection; however, we were not able to ascertain whether there were any causes or whether they denoted consequences. With routine DSA determination, we started to identify their correlation with chronic rejection either before their appearance (P1) or when they were already established (P2). Because these two recipients belonged to the initial period of DSA monitoring and ART, DSA were detected late (with no exact knowledge about their appearance) and chronic rejection and allograft loss could not be avoided. In another patient (P3), dnDSA appearance was observed coincident to a severe rejection episode, and this case was a clear consequence of T-cell activation. In contrast to what was reported by Gerlach (15) and Wozniak (19), who identified that dnDSA mostly appeared in the context of acute cellular rejection episodes, we observed a higher proportion of patients in whom dnDSA emerged without any clinical events, which is currently the most frequent trend in our cohort among new cases. In such patients and due to our previous experience, which related persistent DSA to chronic allograft loss, ART was performed for dnDSA with >2,000 MFI with excellent results and complete removal in 100% of patients.
In this study, we aimed to deepen our experience with ART in ITx, attempting to provide additional evidence to answer the “why, when, and how” question.
First addressing the “why”, we found two main scenarios in which ART was performed: (1) in acute rejection episodes with humoral component and (2) when dnDSA appeared without any clinical symptom. Interestingly, therapy success was closely related to indication. Thus, within the first group (dnDSA with rejection), the therapy was effective in two out of three transplants, but allograft loss could not be avoided in any patient. The best results were observed in the second group (dnDSA without rejection), in which ART was successful in all recipients with complete DSA removal, with only one procedure needed and no rejection thereafter.
This fact led us to answer the “when” question. Because we observed that in patients with delayed ART, DSA were more resistant, we analyzed whether the time from DSA detection until ART administration could have any impact on the outcome, and indeed we found a significant correlation. For example, in the patient in whom DSAs were not removed, the time from DSA to ART was the longest. This important factor, which has not been reported before, strongly makes a case for treating DSA soon after detection or as early as possible even in the absence of clinical symptoms.
With regard to the “how” question, we followed a combination based on plasmapheresis, IVIG, and rituximab. However, there is a lack of detailed information about doses in ITx, periodicity, or the drug combinations used. Also, in other solid organs, protocols differ on such matters, with a large number of administrative guidelines (20–23). Our protocol is based on the daily alternate administration of plasmapheresis and high-dose IVIG (24), which may differ from that of others, who first perform a 1-week plasmapheresis cycle, followed by IVIG administration either in low or in high doses. The timing of rituximab administration is another controversial issue, with administration ranging from 24 to 48 h (as we did) to 15 days after the end of IVIG or plasmapheresis (21, 25–27).
The final question to address is, “is it worth it?” In our experience, which showed a patient success rate of 88%, the answer is an outright yes. But, apart from the effectiveness in terms of DSA removal, another relevant finding of this work is the survival analysis showing a long-term allograft survival of ART-DSA transplants similar to those of DSAneg and higher than noART-DSA transplants. These results are in accordance with what was described by Cheng et al. (4), who reported a risk of allograft failure of 10% by 1 year and 28% by 2 years after dnDSA detection. Also, Matsumoto and Rosen-Bronson reported some preliminary data showing the same 1-year allograft survival between desensitized recipients who developed dnDSA vs. those who never developed dnDSA (16). All these facts, together with the low rate of complications observed in our cohort, encourage the use of antibody-removal protocols.
This study has some limitations that should be mentioned. The first is the reduced number of treated recipients since only 47% of DSA patients underwent ART. In light of this, a separate survival analysis according to ART indication (which would have been more accurate) could not be performed because of the small sample size. However, we used the available information as best we could, providing details of each single evolution after the therapy. Another limitation is that noART-DSA transplants mostly belong to a previous era (before ART came into vogue) and are not contemporary to ART-DSA transplants; therefore the possibility of an element of bias in the comparisons made between both groups cannot be ruled out. Finally, second-line drugs were not used because of the effectiveness of ART in our cohort. Therefore, our work does not present a full desensitization protocol that includes second- and third-line therapies.
In conclusion, the present study gathers our single-center experience with ART in pediatric ITx, showing high effectiveness in terms of DSA removal (especially for dnDSA without rejection) and an increase in allograft survival rates. The elapsed time between DSA detection and the start of treatment was a significant factor contributing to therapy success, suggesting that the early administration of ART, even in the absence of clinical symptoms, might be beneficial to patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics statement
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants’ legal guardians/next of kin was not required to participate in this study in accordance with national legislation and institutional requirements.
Author contributions
ML-L performed the acquisition, analysis, and interpretation of data and wrote the paper. EM and MJC-P contributed to the DSA studies and analysis. ER-B and RG-S were responsible for the patients’ clinical management and collection of clinical data. AMA-M, JS, and FH-O performed the transplants and contributed to the patients’ clinical follow-up. EP-A and PT designed the research, wrote the paper, and revised it critically for final approval. All authors contributed to the article and approved the submitted version.
Funding
Funding for this study was obtained from the research contract “Juan Rodés” to PT (JR19/00049), from Instituto de Salud Carlos III, Spanish Ministry of Science and Innovation and from the research grant number 20/04 from Sociedad Madrileña de Trasplantes.
Acknowledgments
We thank the technical staff of the Histocompatibility laboratory for their collaboration in the study. Thanks also to Drishyaman Kashyap for language editing services.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.1074577/full#supplementary-material.
References
1. Smith JM, Weaver T, Skeans MA, Horslen SP, Harper AM, Snyder JJ, et al. OPTN/SRTR 2016 annual data report: intestine. Am J Transplant (2018) 18(Suppl 1):254–90. doi: 10.1111/ajt.14560
2. Amin A, Farmer DG. Current outcomes after pediatric and adult intestinal transplantation. Curr Opin Organ Transplant. (2019) 24:193–8. doi: 10.1097/MOT.0000000000000608
3. Abu-Elmagd KM, Wu G, Costa G, Lunz J, Martin L, Koritsky DA, et al. Preformed and de novo donor specific antibodies in visceral transplantation: long-term outcome with special reference to the liver. Am J Transplant. (2012) 12:3047–60. doi: 10.1111/j.1600-6143.2012.04237.x
4. Cheng EY, Everly MJ, Kaneku H, Banuelos N, Wozniak LJ, Venick RS, et al. Prevalence and clinical impact of donor-specific alloantibody among intestinal transplant recipients. Transplantation. (2017) 101:873–82. doi: 10.1097/TP.0000000000001391
5. Petit LM, Rabant M, Canioni D, Suberbielle-Boissel C, Goulet O, Chardot C, et al. Impacts of donor-specific anti-HLA antibodies and antibody-mediated rejection on outcomes after intestinal transplantation in children. Pediatr Transplant. (2017) 21:e12847. doi: 10.1111/petr.12847
6. Talayero P, Ramos Boluda E, Gómez Massa E, Castro Panete MJ, Prieto Bozano G, Hernández Oliveros F, et al. Donor-specific antibodies in pediatric intestinal and multivisceral transplantation: the role of liver and human leukocyte antigen mismatching. Liver Transpl. (2018) 24:1726–35. doi: 10.1002/lt.25323
7. Loupy A, Lefaucheur C. Antibody-mediated rejection of solid-organ allografts. N Engl J Med. (2018) 379:1150–60. doi: 10.1056/nejmra1802677
8. Joher N, Matignon M, Grimbert P. HLA desensitization in solid organ transplantation: anti-CD38 to across the immunological barriers. Front Immunol. (2021) 12:688301. doi: 10.3389/fimmu.2021.688301
9. Jordan SC, Ammerman N, Choi J, Huang E, Peng A, Sethi S, et al. The role of novel therapeutic approaches for prevention of allosensitization and antibody-mediated rejection. Am J Transplant. (2020) 20:42–56. doi: 10.1111/ajt.15913
10. Gondolesi G, Blondeau B, Maurette R, Hoppenhauer L, Rodriguez-Laiz G, Schiano T, et al. Pretransplant immunomodulation of highly sensitized small bowel transplant candidates with intravenous immune globulin. Transplantation. (2006) 81:1743–6. doi: 10.1097/01.tp.0000226078.94635.76
11. Santeusanio AD, Moon J, Nair V, Iyer KR. Is there a role for desensitization in intestinal transplantation? Progress in Transplantation. (2019) 29:275–8. doi: 10.1177/1526924819855088
12. Andres AM, Talayero P, Alcolea Sanchez A, Sanchez Galan A, Serradilla Rodríguez J, Bueno Jimenez A, et al. Delayed introduction of sirolimus in paediatric intestinal transplant recipients: indications and long-term benefits. Transpl Int. (2021) 34:1895–907. doi: 10.1111/tri.13959
13. Wu T, Abu-Elmagd K, Bond G, Nalesnik MA, Randhawa P, Demetris AJ. A schema for histologic grading of small intestine allograft acute rejection. Transplantation. (2003) 75:1241–8. doi: 10.1097/01.TP.0000062840.49159.2F
14. Ruiz P, Bagni A, Brown R, Cortina G, Harpaz N, Magid MS, et al. Histological criteria for the identification of acute cellular rejection in human small bowel allografts: results of the pathology workshop at the VIII international small bowel transplant symposium. Transplant Proc. (2004) 36:335–7. doi: 10.1016/j.transproceed.2004.01.079
15. Gerlach UA, Lachmann N, Sawitzki B, Arsenic R, Neuhaus P, Schoenemann C, et al. Clinical relevance of the de novo production of anti-HLA antibodies following intestinal and multivisceral transplantation. Transpl Int. (2014) 27:280–9. doi: 10.1111/tri.12250
16. Matsumoto CS, Rosen-Bronson S. Donor-specific antibody and sensitized patients in intestinal transplantation. Curr Opin Organ Transplant. (2021) 26:245–9. doi: 10.1097/MOT.0000000000000853
17. Berger M, Zeevi A, Farmer DG, Abu-Elmagd KM. Immunologic challenges in small bowel transplantation. Am J Transplant. (2012) 12:S2–8. doi: 10.1111/j.1600-6143.2012.04332.x
18. Kubal C, Mangus R, Saxena R, Lobashevsky A, Higgins N, Fridell J, et al. Prospective monitoring of donor-specific anti-HLA antibodies after intestine/multivisceral transplantation: significance of de novo antibodies. Transplantation. (2015) 99:e49–56. doi: 10.1097/TP.0000000000000614
19. Wozniak LJ, Venick RS. Donor-specific antibodies following liver and intestinal transplantation: clinical significance, pathogenesis and recommendations. Int Rev Immunol. (2019) 38:106–17. doi: 10.1080/08830185.2019.1630404
20. Stegall MD, Gloor J, Winters JL, Moore SB, DeGoey S. A comparison of plasmapheresis versus high-dose IVIG desensitization in renal allograft recipients with high levels of donor specific alloantibody. Am J Transplant. (2006) 6:346–51. doi: 10.1111/j.1600-6143.2005.01178.x
21. Loupy A, Suberbielle-Boissel C, Zuber J, Anglicheau D, Timsit MO, Martinez F, et al. Combined posttransplant prophylactic IVIg/anti-CD 20/plasmapheresis in kidney recipients with preformed donor-specific antibodies: a pilot study. Transplantation. (2010) 89:1403–10. doi: 10.1097/TP.0b013e3181da1cc3
22. Kahwaji J, Jordan SC, Najjar R, Wongsaroj P, Choi J, Peng A, et al. Six-year outcomes in broadly HLA-sensitized living donor transplant recipients desensitized with intravenous immunoglobulin and rituximab. Transpl Int. (2016) 29:1276–85. doi: 10.1111/tri.12832
23. Moreso F, Crespo M, Ruiz JC, Torres A, Gutierrez-Dalmau A, Osuna A, et al. Treatment of chronic antibody mediated rejection with intravenous immunoglobulins and rituximab: a multicenter, prospective, randomized, double-blind clinical trial. Am J Transplant. (2018) 18:927–35. doi: 10.1111/ajt.14520
24. Takemoto SK, Zeevi A, Feng S, Colvin RB, Jordan S, Kobashigawa J, et al. National conference to assess antibody-mediated rejection in solid organ transplantation. Am J Transplant. (2004) 4:1033–41. doi: 10.1111/j.1600-6143.2004.00500.x
25. Vo AA, Lukovsky M, Toyoda M, Wang J, Reinsmoen NL, Lai CH, et al. Rituximab and intravenous immune globulin for desensitization during renal transplantation. N Engl J Med. (2008) 359:242–51. doi: 10.1097/sa.0b013e318192824f
26. Kaposztas Z, Podder H, Mauiyyedi S, Illoh O, Kerman R, Reyes M, et al. Impact of rituximab therapy for treatment of acute humoral rejection. Clin Transplant. (2009) 23:63–73. doi: 10.1111/j.1399-0012.2008.00902.x
Keywords: intestinal transplantation, multivisceral transplantation, donor-specific antibodies, antibody-removal therapies, pediatric transplantation
Citation: Lasa-Lázaro M, Ramos-Boluda E, Mancebo E, Castro-Panete MJ, González-Sacristán R, Serradilla J, Andrés-Moreno AM, Hernández-Oliveros F, Paz-Artal E and Talayero P (2023) Antibody-removal therapies for de novo DSA in pediatric intestinal recipients: Why, when, and how? A single-center experience. Front. Pediatr. 10:1074577. doi: 10.3389/fped.2022.1074577
Received: 19 October 2022; Accepted: 21 December 2022;
Published: 2 February 2023.
Edited by:
Narayan Prasad, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGI), IndiaReviewed by:
Nicole Hayde, Children's Hospital at Montefiore, United StatesDechu Puliyanda, Cedars Sinai Medical Center, United States
© 2023 Lasa-Lázaro, Ramos-Boluda, Mancebo, Castro-Panete, González-Sacristán, Serradilla, Andrés-Moreno, Hernández Oliveros, Paz-Artal and Talayero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paloma Talayero cGFsb21hLnRhbGF5ZXJvQHNhbHVkLm1hZHJpZC5vcmc=
Specialty Section: This article was submitted to Pediatric Surgery, a section of the journal Frontiers in Pediatrics