 Corina Nailescu
Corina Nailescu Marcia L. Shew
Marcia L. Shew
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pediatr. , 30 November 2022
Sec. Pediatric Nephrology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.1057454
This article is part of the Research Topic Infections and Post-Transplant Lymphoproliferative Disease after Pediatric Kidney Transplantation View all 8 articles
Malignancies are found between the first three reasons of mortality in pediatric and adult kidney transplant recipients, who overall have disproportionately higher rates of cancer compared to the general population, including human papillomavirus (HPV)-related genital, anal and oropharynx region cancers. Therefore, preventing HPV in this patient population is extremely important. HPV-vaccine was demonstrated to prevent HPV infection in individuals with intact immune systems. In addition, recent data reported less precancerous HPV lesions and cervical cancers with use of HPV vaccine. Since HPV is a sexually transmitted virus that is typically acquired shortly after the onset of sexual activity, it is best to administer the HPV vaccine immunization prior to the onset of sexual activity. This article reviews the epidemiology and pathophysiology of the HPV infection, as well as its role in the development of HPV-related pre-cancerous lesions and cancers in both general population and kidney transplant recipients. The focus is on the most effective primary prophylactic strategy, which is the HPV vaccination. The particularities of HPV vaccination strategies in kidney transplant recipients are compared to the general population. In addition, the article analyzes the various causes of suboptimal HPV immunization rates in kidney transplant candidates and recipients and discusses vaccination optimization strategies that can be applied during childhood and adolescence to reduce the burden of HPV-related disease states and cancer among adult kidney transplant recipients.
Cancers in general are between the first three reasons of death in adult solid organ transplant (SOT) recipients, including kidney transplant (KT) recipients (1). It is disturbing to know that by 30 years following transplantation, 26%–41% of SOT recipients who had received their transplants as children, would have developed some form of malignancy (2). Overall, the cancer rate in adults who received a KT as children was six times higher compared to general population (3). As an example, female KT recipients have a 14-fold increased risk of cervical cancer and a 50-fold increased risk of vulvar cancer, male KT recipients have an increased risk for penile cancers and both female and male KT recipients have a 100-fold increased risk for anal cancers (4–7). The common denominator for all these cancer types is the infection with different types of human papillomavirus (HPV) (8).
Understanding that adult KT patients carry a high-risk for cancers, including HPV-related ones, and that the treatment for these diseases can negatively impact the graft viability and life expectancy, medical professionals need to get an early start with the most efficacious preventive strategies during childhood and adolescence (4). This article will delineate the most efficient primary prevention strategy, the HPV vaccination, which applied by pediatric professionals during childhood and adolescence has been proven to reduce the risk for HPV-associated malignancies for KT recipients during their adult life (9, 10).
HPV is known as the most prevalent sexually transmitted infection (11). Worldwide, the estimated lifetime probability of being infected is greater than 80% for women and 90% for men (12). Certain types, including HPV 16, −18, −31, −33, −35, −39, −45, −51, −52, −56, −58 and −59, are responsible for greater than 95% of HPV-related cancers (4, 13). HPV has been identified as a cause for cervical, vaginal, vulvar, penile, anal, and oropharyngeal cancers in >91%, 75%, 69%, 63%, 91% and 70%, respectively (4, 14). Of all the HPV-related malignancies, cervical carcinoma, which is linked to HPV in over 90% of the cases, deserves a special consideration, as it is the second most common cancer and cause of cancer death in women at international level (4, 14). HPV 16 carries the highest risk for development of invasive cervical cancer (15). Specifically in adult women KT recipients, cervical cytology was diagnosed as atypical in 25.8% of cases, while the cervical presence of HPV was detected in 22.5% of the patients (16). HPV 16, and to a smaller degree HPV 18, are also the root cause for most oropharyngeal and anal cancers (17, 18). Specifically, adult KT recipients had almost three-fold higher adjusted odds of having anal high-risk HPV lesions compared to healthy controls (19). Of note, certain non-oncogenic HPV types such as 6 and 11 are associated with genital warts and respiratory papillomatosis (20). Specifically, adult KT recipients had a higher hazard of genital warts compared to the general population (HR = 3.3; 95% confidence interval, 2.76–3.93) (21). While non-oncogenic, these HPV types can nevertheless lead to serious and difficult to treat disease in the face of immunosuppression (22, 23).
The natural history of HPV infection is better understood in the cervix, as it is thought that women in general encounter one or multiple types of HPV infections within the first two years after their sexual debut (24, 25). Luckily, many of these early HPV cervical infections become non-detectable within two years (24). Whether this non-detection represents total clearance of the virus or suppression in a latent stage is generally unknown (26). If high-risk HPV infections are persistent, they can progress to precancerous lesions known as cervical intraepithelial neoplasia (CIN) (graded as 1, 2 and 3) (27). Such pre-cancerous lesions can over time can progress to invasive malignant lesions (27). Risk factors associated with acquiring new HPV infections and progressing to CIN or even cancer include young age sexual debut, tobacco use, and higher number of sex partners, as well as immunocompromised state (28). Indeed, immunosuppression has been associated with poor cell mediated viral clearance leading to increased infection rates, persistent infections, accelerated reactivation from the latent phase and accelerated progression of precancerous disease to cancer (29–33).
By contrast, the natural history of HPV infection in the anal and oropharyngeal regions is less clear. However, similar to cervical dysplasia, anal cancer has its cytologic precursors that may be treated early to prevent progression (34). Both anal and oral cancers carry similar risk factors for acquisition of the virus (34). In studies specific to KT, individual findings have shown an increased presence of HPV (compared to non-immunosuppressed populations) in the oral cavity (35), higher prevalence of genital warts (21) and increased risk of HPV infections and cancer in the anal region (36, 37).
Prevention strategies have been developed to protect the general population from the HPV-related cancers. As primary prevention, the development and clinical use of the HPV vaccine has allowed a very effective intervention against HPV- related cancers in the general population (38). Secondary prevention, involving the detection of early cancer mostly using cervical cytology (Pap smear methodology), as well as HPV testing, has also been successfully used in the general population (39). Unfortunately, applying such primary and secondary HPV prevention strategies to immunosuppressed patients, including KT recipients, has been less than optimal. This article should help KT professionals understand the HPV vaccination particularities in the patient population they are carrying for, in comparison to the general population, thus hopefully resulting in improved immunization rates.
Three types of HPV vaccines are available. The quadrivalent HPV vaccine is effective against types 6, 11, 16 and 18 and it was approved in 2006 for female patients age 9–26 and in 2009 for males age 9–26, as well. The bivalent vaccine, effective against HPV types 16 & 18 was approved only for female patients age 10–25 in 2009. The 9-valent vaccine, which is effective against HPV types 6, 11, 16, 18, 31, 33, 45, 52 and 58 was licensed for both female and male patients age 9–26 in 2014 (40). In the United States only the 9-valent vaccine is currently available.
HPV vaccines are extremely efficacious in preventing persistent HPV infections with oncogenic types, as well as the development of premalignant and malignant HPV-related pathology (41). Multiple studies have shown a reduction in abnormal cervical precancerous lesions, cervical cancers and anal cancers secondary to the use of HPV vaccine (38, 42, 43). For example, after the introduction of the HPV vaccine in 2006, during 2008–2015, the rates of CIN2+ in the state of Connecticut declined by 30%–74% among women aged 21–26 years, with greater declines observed in the younger women (42). In regards to anal intraepithelial neoplasia, the efficacy of the quadrivalent HPV vaccine in preventing it was estimated to be 50.3% (95% confidence interval 25.7–67.2) in the intention-to-treat population and 77.5% (95% confidence interval 39.6–93.3) in the per-protocol efficacy polupation (43). In addition, there is also emerging evidence of possible oropharyngeal cancer prevention with the use of HPV vaccine (44). It should be noted that the vaccine is approved to prevent HPV-related cervical and anal precancer and cancer, but it is not approved to prevent HPV-related oral cancer (45).
When the vaccine series is initiated before age 15, the regimen consists of two doses. The second dose should be administered six to twelve months after the initial one. For patients who accidentally receive the two vaccine doses less than five months apart, a third dose of the HPV vaccine is recommended (46).
When the vaccine series is initiated between age 15 and 26, the regimen consists of three doses. The recommended schedule for this three-dose regimen is to be administered at time zero, at one to two months and at six months after the initial one. The vaccine is not routinely offered after age 26 (40) (Table 1).
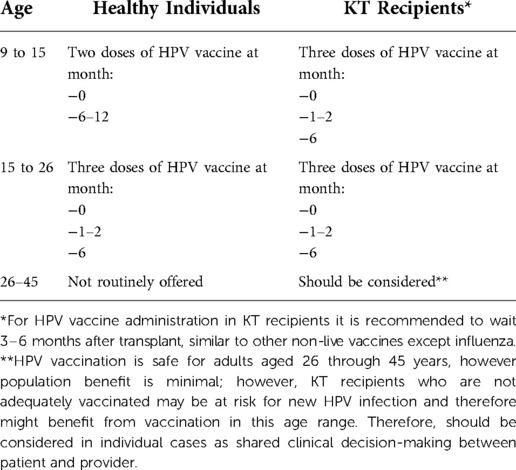
Table 1. Dosing and timing recommendations for HPV vaccine administration.
The HPV vaccine is effective in preventing infection, but not in clearing previously acquired infections (46, 47). Since HPV is a sexually transmitted infection typically acquired shortly after the sexual debut (48), HPV vaccination is optimal when administered before the onset of sexual activity (4). In the United States, 5% to 25% of males residing in metropolitan areas reported having sexual intercourse before age 13 (49). The data on such sexual experiences of adolescents, as well as the known robust immune responses that adolescents have compared to older individuals, formed the basis for the recommendation of administering the HPV vaccine at 11 to 12 years of age (4, 46). However, the HPV vaccine can be given as early as nine years of age (46) with catch-up vaccination through age 26.
In healthy populations, the seroconversion rates are 95%–100% after vaccination (50, 51). This vaccination-induced immune response is clearly much more robust compared to the natural infection, as in one study only 54%–69% of women with incident HPV 16 or 18 infections had antibodies (52).
Data from a ten-year post-bivalent HPV vaccination follow-up European study performed in immunocompetent individuals found that seropositivity rates remained relatively high: 100% for HPV-16 and 99.2% for HPV-18; using mathematical models, immunity was predicted to remain above natural infection levels for at least 30 years (53). In addition, sustainability of neutralizing antibodies induced by HPV vaccines in a combined follow-up analysis of data from two randomized, double-blinded, multicenter, phase 3 trials showed that HPV vaccine-induced seroprotection can be maintained up to 12 years (54).
The studies evaluating the vaccine in reducing HPV disease endpoints in immunosuppressed individuals, including human immunodeficiency virus (HIV) patients and SOT recipients, continue to be limited, but emerging. For example, the quadrivalent HPV vaccine has been recently shown to reduce HPV infections and genital warts in HIV women (55, 56). There is also recent data demonstrating that in immunosuppressed individuals (HIV-infected, with a SOT history, including KT, or being on medications that suppress the immune system), HPV vaccination was associated with the development of less CIN2 + precancerous lesions (9, 10). In addition, there are several case reports describing the resolution of genital and non-genital difficult-to-treat recalcitrant warts after HPV vaccine administration (57, 58).
The dosing for KT recipients, which actually applies to all SOT recipients, is slightly different than for the general population. In essence, while healthy individuals less than 15 need only two doses of the vaccine, KT recipients should always receive three doses, regardless of their age (59). Furthermore, while in healthy individuals the vaccine is not routinely offered after age 26, in KT recipients it can be taken into consideration (4) (24), (Table 1).
Timing of the HPV vaccine for KT recipients should be as recommended for the general population. It is optimal to vaccinate whenever possible prior to transplantation, during the last stages of chronic kidney disease (CKD) or while on dialysis, as it has been shown that after transplantation the vaccine responses are reduced (4, 60).
The HPV vaccines are efficacious in SOT recipients, including KT, but nevertheless the immune response appears to be reduced compared to the general population (4). The very first study of the HPV vaccine in SOT recipients that was done in 47 adults, both females and males, showed lower seroconversion rates: 63.2%, 68.4%, 63.2% and 52.6% for HPV 6, 11, 16 and 18, respectively, compared to historical healthy controls (61). More recently, a Belgian study assessed the 9-valent HPV vaccine response in adults with kidney, lung and heart transplants and found lower seroconversion rates, ranging from 46% for HPV45 to 72% for HPV58 (62). The very first pediatric study included 57 age 9–21 subjects with KT and showed that seropositivity was significantly lower (62.5%, 50.0%, 75.0% and 50.0% for HPV 6, 11, 16 and 18, respectively), compared to patients with advanced CKD (63). Our multicenter study included 72 patients, females and males age 10–16 with KT and reported that the KT recipients were significantly lower in terms of seroconverting (72.4%, 69.0%, 89.7% and 62.1%, for HPV 6, 11, 16 and 18, respectively), compared to patients with CKD (100%, 100%, 100% and 94.4%) (60). The evidence points out that it is optimal to vaccinate whenever possible before transplantation, during the last stages of CKD or on dialysis (4). If HPV vaccine was not administered before transplant, it is still recommended after, at least three to six months post-transplantation for the best optimal immune response given the circumstances (64).
Five years post-HPV vaccination in SOT recipients, seropositivity rates dropped from 100% immediately post-vaccination to 94.6% for HPV-16 and from 91.2% to 78.4% for HPV-18 in a recent Australian study (65). This study raised the question of the utility of revaccinating SOT recipients after a number of years. It has been shown that in immunocompetent individuals, revaccination with the HPV vaccine resulted in an increase in antibody titers and anamnestic responses from B cell memory (66). To this date, re-vaccination with HPV vaccine has not been studied in immunosuppressed individuals and in addition, the exact neutralizing antibody titer needed to prevent infection is unknown, therefore the need for revaccination in SOT recipients has not been so far demonstrated (4).
In a study of pediatric KT recipients from University of Minnesota followed long-term it was noted that at 20 years post-KT, 13% of the patients were suffering from a form of malignancy, while by 30 years post-KT, 26% (3). Despite the fact that KT recipients are known to have a high risk for malignancies, including HPV-associated malignancies, unfortunately they do not appear to be ideally protected by primary prevention: they end up either not immunized, or immunized beyond the recommended time (67). It is known that the HPV vaccine acceptance by either patients or caregivers has always been a problem even in healthy populations (68, 69). When it comes to KT patients, HPV vaccination status is even less optimal, likely because data on safety and efficacy has been scant until recently (67). However, recent studies provided more evidence that patients who are likely to need a KT in the future respond best to the HPV vaccine before transplant, while with CKD or on dialysis (60, 63). Since the leading causes of end-stage renal disease in children are congenital anomalies of the kidneys and the urinary tracts in which the kidney function diminishes slowly, pediatric nephrologists should be able to better plan a KT compared to their colleagues who care for adults when it comes to vaccinations (67). Therefore, the results of the recent studies brought forward new information to help pediatric medical professionals in their work to complete the HPV vaccine administration ideally prior to transplantation if possible (4). It is also to emphasize that pediatric nephrologists have dialysis as a temporary treatment option for their patients with end-stage renal disease, which allows them to best prepare their patients for a transplant, including establishing a complete vaccination status (4). In the case of SOT other than the KT, it is not always possible to plan so much in advance, therefore it is equally important for general pediatricians to make sure HPV vaccination happens promptly at the minimum vaccination age.
KT recipients appear to be vaccinated later than the recommended time (60). This is likely because these patients are chronically ill with CKD while awaiting transplantation and therefore there is less concern about sexual activity, as demonstrated in patients with other types of chronic diseases (60, 70). Surprisingly, a recent study of children with CKD showed that growth and sexual maturation are only slightly delayed compared to healthy subjects, which is contrary to what it was previously thought (4, 71), therefore it is important that they are administered the HPV vaccine without delays (60). In general, routine pediatric immunizations in KT candidates and recipients are more likely to be administered by their primary care providers, while vaccines that differ from the routine schedules, including the HPV, are more likely to be administered by transplant professionals, who are likely to be more familiar with dosing them appropriately (4, 67). Thus, it is important for both general pediatricians and pediatric transplant nephrologists to be aware of the immunization guidelines for KT candidates and recipients and stay in close communication, to ensure an ongoing fully immunized status for their patients (4).
In addition, vaccine hesitancy has been an even greater issue in successfully vaccinating children and adolescents, therefore general pediatricians and pediatric transplant nephrologists can help to overcome reluctance by educating their patients regarding to the safety profile and the benefits of the HPV vaccine (72). In order to improve HPV immunization in the general population, different interventions have been shown to be somewhat effective, including provider education, collaboration between physicians and pharmacists and systems changes (73, 74). In a recent study, such interventions modestly increased HPV vaccination rates from 60% preintervention to 69% postintervention (75). Another intervention showed more promising results, as parents who watched an educational video had 3-times greater odds of accepting that their children receive the HPV vaccine (76).
In conclusion, in order to optimally protect KT patients from acquiring HPV-associated cancers, pediatric transplant professionals should advocate that their patients get the HPV vaccine before transplantation, provided that they have reached age nine. If the KT occurs during the series, vaccination should be completed afterwards, resuming the series at least 3–6 months after transplant. If still unvaccinated post-transplant, medical professionals should recommend the HPV vaccine even after age 26. Further research will be needed to assess the effectiveness of the HPV vaccine when given before transplantation in preventing actual HPV-related pathology. Consideration is being given to administering the vaccine at an earlier than currently recommended age. If proven effective enough and safe, this could change the life of many patients, who otherwise would become transplanted without the HPV vaccine and therefore would miss the opportunity to mount a strong serologic response pre-transplant.
CN was responsible for the literature review and manuscript writing. MLS was responsible for the article's concept, structure and for corrections. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
SOT, solid organ transplant; KT, kidney transplant; HPV, human papilloma virus; CIN, cervical intraepithelial neoplasia; HIV, human immunodeficiency virus; CKD, chronic kidney disease.
1. Chua A, Cramer C, Moudgil A, Martz K, Smith J, Blydt-Hansen T, et al. Kidney transplant practice patterns and outcome benchmarks over 30 years: the 2018 report of the NAPRTCS. Pediatr Transplant. (2019) 23(8):e13597. doi: 10.1111/petr.13597
2. Robinson C, Chanchlani R, Kitchlu A. Malignancies after pediatric solid organ transplantation. Pediatric Nephrol (Berlin, Germany). (2021) 36(8):2279–91. doi: 10.1007/s00467-020-04790-2
3. Serrano OK, Bangdiwala AS, Vock DM, Chinnakotla S, Dunn TB, Finger EB, et al. Post-Transplant malignancy after pediatric kidney transplantation: retrospective analysis of incidence and risk factors in 884 patients receiving transplants between 1963 and 2015 at the university of Minnesota. J Am Coll Surg. (2017) 225(2):181–93. doi: 10.1016/j.jamcollsurg.2017.04.012
4. Nailescu C, Ermel AC, Shew ML. Human papillomavirus-related cancer risk for solid organ transplant recipients during adult life and early prevention strategies during childhood and adolescence. Pediatr Transplant. (2022) 26(7):e14341. doi: 10.1111/petr.14341
5. Hinten F, Meeuwis KA, van Rossum MM, de Hullu JA. HPV-related (pre)malignancies of the female anogenital tract in renal transplant recipients. Crit Rev Oncol Hematol. (2012) 84(2):161–80. doi: 10.1016/j.critrevonc.2012.02.008
6. Liao JB, Fisher CE, Madeleine MM. Gynecologic cancers and solid organ transplantation. Am J Transplant. (2019) 19(5):1266–77. doi: 10.1111/ajt.15292
7. Jiang S, Regmi S, Jackson S, Calvert C, Jarosek S, Pruett T, et al. Risk of genitourinary malignancy in the renal transplant patient. Urology. (2020) 145:152–8. doi: 10.1016/j.urology.2020.06.077
8. Smith JS, Lindsay L, Hoots B, Keys J, Franceschi S, Winer R, et al. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: a meta-analysis update. Int J Cancer. (2007) 121(3):621–32. doi: 10.1002/ijc.22527
9. Silverberg MJ, Leyden WA, Lam JO, Chao CR, Gregorich SE, Huchko MJ, et al. Effectiveness of “catch-up” human papillomavirus vaccination to prevent cervical neoplasia in immunosuppressed and non-immunosuppressed women. Vaccine. (2020) 38(29):4520–3. doi: 10.1016/j.vaccine.2020.05.004
10. Nichols A, Nahm W, Rabinovitz H, Ioannides T. Keratinocyte carcinomas in immunocompromised patients are reduced after administration of the nonavalent human papillomavirus vaccine. J Drugs in Dermatol: JDD. (2022) 21(5):526–8. doi: 10.36849/JDD.6536
11. Dunne EF, Park IU. HPV And HPV-associated diseases. Infect Dis Clin North Am. (2013) 27(4):765–78. doi: 10.1016/j.idc.2013.09.001
12. Chesson HW, Dunne EF, Hariri S, Markowitz LE. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex Transm Dis. (2014) 41(11):660–4. doi: 10.1097/OLQ.0000000000000193
13. Serrano B, Brotons M, Bosch FX, Bruni L. Epidemiology and burden of HPV-related disease. Best Pract & Res Clin Obstet & Gynaecol. (2018) 47:14–26. doi: 10.1016/j.bpobgyn.2017.08.006
14. Szymonowicz KA, Chen J. Biological and clinical aspects of HPV-related cancers. Cancer Biol Med. (2020) 17(4):864–78. doi: 10.20892/j.issn.2095-3941.2020.0370
15. Satterwhite CL, Torrone E, Meites E, Dunne EF, Mahajan R, Ocfemia MC, et al. Sexually transmitted infections among US women and men: prevalence and incidence estimates, 2008. Sex Transm Dis. (2013) 40(3):187–93. doi: 10.1097/OLQ.0b013e318286bb53
16. Eleutério J Jr, Cavalcante LR, Gonçalves AKS, Eleutério RMN, Giraldo PC. Prevalence of high-risk HPV and atypia in liquid-based cytology of cervical and intra-anal specimens from kidney-transplanted women. Diagn Cytopathol. (2019) 47(8):783–7. doi: 10.1002/dc.24180
17. Antonsson A, Neale RE, Boros S, Lampe G, Coman WB, Pryor DI, et al. Human papillomavirus status and p16(INK4A) expression in patients with mucosal squamous cell carcinoma of the head and neck in Queensland, Australia. Cancer Epidemiol. (2015) 39(2):174–81. doi: 10.1016/j.canep.2015.01.010
18. Alemany L, Saunier M, Alvarado-Cabrero I, Quirós B, Salmeron J, Shin HR, et al. Human papillomavirus DNA prevalence and type distribution in anal carcinomas worldwide. Int J Cancer. (2015) 136(1):98–107. doi: 10.1002/ijc.28963
19. Larsen HK, Kjaer SK, Haedersdal M, Kjaer AK, Bonde JH, Sørensen SS, et al. Anal human papillomavirus infection in kidney transplant recipients compared with immunocompetent controls. Clin Infect Dis. (2022) :ciac285. doi: 10.1093/cid/ciac285. [Epub ahead of print].35438132
20. Giuliano AR, Anic G, Nyitray AG. Epidemiology and pathology of HPV disease in males. Gynecol Oncol. (2010) 117(2 Suppl):S15–9. doi: 10.1016/j.ygyno.2010.01.026
21. Larsen HK, Thomsen LT, Haedersdal M, Dehlendorff C, Schwartz Sorensen S, Kjaer SK. Risk of genital warts in renal transplant recipients-A registry-based, prospective cohort study. Am J Transplant. (2019) 19(1):156–65. doi: 10.1111/ajt.15056
22. Komlos KF, Kocjan BJ, Kosorok P, Luzar B, Meglic L, Potocnik M, et al. Tumor-specific and gender-specific pre-vaccination distribution of human papillomavirus types 6 and 11 in anogenital warts and laryngeal papillomas: a study on 574 tissue specimens. J Med Virol. (2012) 84(8):1233–41. doi: 10.1002/jmv.23318
23. García-Romero CS, Akaki-Caballero M, Saavedra-Mendoza AG, Guzmán-Romero AK, Canto P, Coral-Vázquez RM. Molecular subtypification of human papillomavirus in Male adult individuals with recurrent respiratory papillomatosis. Auris Nasus Larynx. (2015) 42(5):385–9. doi: 10.1016/j.anl.2015.03.006
24. Imburgia TM, Shew ML, Gravitt PE, Katzenellenbogen RA. Considerations for child cancer survivors and immunocompromised children to prevent secondary HPV-associated cancers. Transplantation. (2021) 105(4):736–42. doi: 10.1097/TP.0000000000003444
25. Ferris DG, Brown DR, Giuliano AR, Myers E, Joura EA, Garland SM, et al. Prevalence, incidence, and natural history of HPV infection in adult women ages 24 to 45 participating in a vaccine trial. Papillomavirus Res (Amsterdam, Netherlands). (2020) 10:100202. doi: 10.1016/j.pvr.2020.100202
26. Gravitt PE, Winer RL. Natural history of HPV infection across the lifespan: role of viral latency. Viruses. (2017) 9(10):267. doi: 10.3390/v9100267
27. El-Zein M, Ramanakumar AV, Naud P, Roteli-Martins CM, de Carvalho NS, Colares de Borba P, et al. Determinants of acquisition and clearance of human papillomavirus infection in previously unexposed young women. Sex Transm Dis. (2019) 46(10):663–9. doi: 10.1097/OLQ.0000000000001053
28. Matsumoto K, Yoshikawa H. Human papillomavirus infection and the risk of cervical cancer in Japan. J Obstet Gynaecol Res. (2013) 39(1):7–17. doi: 10.1111/j.1447-0756.2012.01977.x
29. Orlando G, Bianchi S, Fasolo MM, Mazza F, Frati ER, Rizzardini G, et al. Cervical human papillomavirus genotypes in HIV-infected women: a cross-sectional analysis of the VALHIDATE study. J Prev Med Hyg. (2017) 58(4):E259–e65. doi: 10.15167/2421-4248/jpmh2017.58.4.804
30. Long ME, Chantigian PDM, Weaver AL. Cervical cytology and histology after solid organ transplant: a longitudinal cohort study. J Low Genit Tract Dis. (2018) 22(4):362–6. doi: 10.1097/LGT.0000000000000414
31. Veroux M, Corona D, Scalia G, Garozzo V, Gagliano M, Giuffrida G, et al. Surveillance of human papilloma virus infection and cervical cancer in kidney transplant recipients: preliminary data. Transplant Proc. (2009) 41(4):1191–4. doi: 10.1016/j.transproceed.2009.03.015
32. Berkhout RJ. Bouwes bavinck JN, ter schegget J. Persistence of human papillomavirus DNA in benign and (pre)malignant skin lesions from renal transplant recipients. J Clin Microbiol. (2000) 38(6):2087–96. doi: 10.1128/JCM.38.6.2087-2096.2000
33. Pietrzak B, Mazanowska N, Ekiel AM, Durlik M, Martirosian G, Wielgos M, et al. Prevalence of high-risk human papillomavirus cervical infection in female kidney graft recipients: an observational study. Virol J. (2012) 9:117. doi: 10.1186/1743-422X-9-117
34. Jongen VW, Richel O, Marra E, Siegenbeek van Heukelom ML, van Eeden A, de Vries HJC, et al. Anal squamous intraepithelial lesions (SILs) in human immunodeficiency virus-positive men who have sex with men: incidence and risk factors of SIL and of progression and clearance of low-grade SILs. J Infect Dis. (2020) 222(1):62–73. doi: 10.1093/infdis/jiz614
35. Rose B, Wilkins D, Li W, Tran N, Thompson C, Cossart Y, et al. Human papillomavirus in the oral cavity of patients with and without renal transplantation. Transplantation. (2006) 82(4):570–3. doi: 10.1097/01.tp.0000231706.79165.e5
36. Grąt K, Grąt M, Wronka KM, Pietrzak B, Suchońska B, Walter de Walthoffen S, et al. Cervical human papillomavirus infection in the early postoperative period after liver transplantation: prevalence, risk factors, and concordance with anal infections. Clin Transplant. (2017) 31(3):e12894. doi: 10.1111/ctr.12894
37. Miyaji KT, Infante V, Picone CM, Levi JE, Oliveira ACS, Lara AN, et al. Human papillomavirus (HPV) seroprevalence, cervical HPV prevalence, genotype distribution and cytological lesions in solid organ transplant recipients and immunocompetent women in sao paulo, Brazil. PloS one. (2022) 17(1):e0262724. doi: 10.1371/journal.pone.0262724
38. Arbyn M, Xu L. Efficacy and safety of prophylactic HPV vaccines. A cochrane review of randomized trials. Expert Rev Vaccines. (2018) 17(12):1085–91. doi: 10.1080/14760584.2018.1548282
39. Ogilvie GS, van Niekerk D, Krajden M, Smith LW, Cook D, Gondara L, et al. Effect of screening with primary cervical HPV testing vs cytology testing on high-grade cervical intraepithelial neoplasia at 48 months: the HPV FOCAL randomized clinical trial. Jama. (2018) 320(1):43–52. doi: 10.1001/jama.2018.7464
40. Human papillomavirus vaccines: wHO position paper, may 2017-recommendations. Vaccine. (2017) 35(43):5753–5. doi: 10.1016/j.vaccine.2017.05.069
41. Brown DR, Garland SM, Ferris DG, Joura E, Steben M, James M, et al. The humoral response to gardasil over four years as defined by total IgG and competitive luminex immunoassay. Hum Vaccin. (2011) 7(2):230–8. doi: 10.4161/hv.7.2.13948
42. Niccolai LM, Meek JI, Brackney M, Hadler JL, Sosa LE, Weinberger DM. Declines in human papillomavirus (HPV)-associated high-grade cervical lesions after Introduction of HPV vaccines in Connecticut, United States, 2008-2015. Clin Infect Dis. (2017) 65(6):884–9. doi: 10.1093/cid/cix455
43. Palefsky JM, Giuliano AR, Goldstone S, Moreira ED Jr., Aranda C, Jessen H, et al. HPV Vaccine against anal HPV infection and anal intraepithelial neoplasia. N Engl J Med. (2011) 365(17):1576–85. doi: 10.1056/NEJMoa1010971
44. Diana G, Corica C. Human papilloma virus vaccine and prevention of head and neck cancer, what is the current evidence? Oral Oncol. (2021) 115:105168. doi: 10.1016/j.oraloncology.2020.105168
45. Daley EM, Thompson EL, Beckstead J, Driscoll A, Vamos C, Piepenbrink RP, et al. Discussing HPV and oropharyngeal cancer in dental settings: gender and provider-type matter. Hum Vaccin Immunother. (2021) 17(12):5454–9. doi: 10.1080/21645515.2021.1996809
46. Recommendations on the use of quadrivalent human papillomavirus vaccine in males–advisory committee on immunization practices (ACIP), 2011. MMWR Morbidity and Mortality Weekly Report. (2011) 60(50):1705–8.22189893
47. Guerra FM, Rosella LC, Dunn S, Wilson SE, Chen C, Deeks SL. Early impact of Ontario's Human papillomavirus (HPV) vaccination program on anogenital warts (AGWs): a population-based assessment. Vaccine. (2016) 34(39):4678–83. doi: 10.1016/j.vaccine.2016.08.020
48. Collins S, Mazloomzadeh S, Winter H, Blomfield P, Bailey A, Young LS, et al. High incidence of cervical human papillomavirus infection in women during their first sexual relationship. BJOG: an Int J Obstet and Gynaecol. (2002) 109(1):96–8. doi: 10.1111/j.1471-0528.2002.01053.x
49. Lindberg LD, Maddow-Zimet I, Marcell AV. Prevalence of sexual initiation before age 13 years among Male adolescents and young adults in the United States. JAMA Pediatr. (2019) 173(6):553–60. doi: 10.1001/jamapediatrics.2019.0458
50. Steben M, Tan Thompson M, Rodier C, Mallette N, Racovitan V, DeAngelis F, et al. A review of the impact and effectiveness of the quadrivalent human papillomavirus vaccine: 10 years of clinical experience in Canada. J Obstet and Gynaecol Can: JOGC. (2018) 40(12):1635–45. doi: 10.1016/j.jogc.2018.05.024
51. Garland SM, Kjaer SK, Muñoz N, Block SL, Brown DR, DiNubile MJ, et al. Impact and effectiveness of the quadrivalent human papillomavirus vaccine: a systematic review of 10 years of real-world experience. Clin Infect Dis. (2016) 63(4):519–27. doi: 10.1093/cid/ciw354
52. Carter JJ, Koutsky LA, Hughes JP, Lee SK, Kuypers J, Kiviat N, et al. Comparison of human papillomavirus types 16, 18, and 6 capsid antibody responses following incident infection. J Infect Dis. (2000) 181(6):1911–9. doi: 10.1086/315498
53. Schwarz TF, Galaj A, Spaczynski M, Wysocki J, Kaufmann AM, Poncelet S, et al. Ten-year immune persistence and safety of the HPV-16/18 AS04-adjuvanted vaccine in females vaccinated at 15-55 years of age. Cancer Med. (2017) 6(11):2723–31. doi: 10.1002/cam4.1155
54. Mariz FC, Gray P, Bender N, Eriksson T, Kann H, Apter D, et al. Sustainability of neutralising antibodies induced by bivalent or quadrivalent HPV vaccines and correlation with efficacy: a combined follow-up analysis of data from two randomised, double-blind, multicentre, phase 3 trials. The Lancet Infect Dis. (2021) 21(10):1458–68. doi: 10.1016/S1473-3099(20)30873-2
55. McClymont E, Ogilvie G, Albert A, Johnston A, Raboud J, Walmsley S, et al. Impact of quadrivalent HPV vaccine dose spacing on immunologic response in women living with HIV. Vaccine. (2020) 38(15):3073–8. doi: 10.1016/j.vaccine.2020.02.075
56. McClymont E, Lee M, Raboud J, Coutlée F, Walmsley S, Lipsky N, et al. The efficacy of the quadrivalent human papillomavirus vaccine in girls and women living with human immunodeficiency virus. Clin Infect Dis. (2019) 68(5):788–94. doi: 10.1093/cid/ciy575
57. Wyant WA, Burke GW, Ioannides T, Nichols AJ. Systemic 9-valent human papillomavirus vaccine for recalcitrant common cutaneous warts in preparation for renal transplant. JAAD Case Rep. (2022) 22:62–3. doi: 10.1016/j.jdcr.2022.02.004
58. Maor D, Brennand S, Goh MS, Fahey V, Tabrizi SN, Chong AH. A case of acquired epidermodysplasia verruciformis in a renal transplant recipient clearing with multimodal treatment including HPV (gardasil) vaccination. Australas J Dermatol. (2018) 59(2):147–8. doi: 10.1111/ajd.12684
59. Garland SM, Brotherton JML, Moscicki AB, Kaufmann AM, Stanley M, Bhatla N, et al. HPV Vaccination of immunocompromised hosts. Papillomavirus Res (Amsterdam, Netherlands). (2017) 4:35–8. doi: 10.1016/j.pvr.2017.06.002
60. Nailescu C, Nelson RD, Verghese PS, Twombley KE, Chishti AS, Mills M, et al. Human papillomavirus vaccination in Male and female adolescents before and after kidney transplantation: a pediatric nephrology research consortium study. Front Pediatr. (2020) 8:46. doi: 10.3389/fped.2020.00046
61. Kumar D, Unger ER, Panicker G, Medvedev P, Wilson L, Humar A. Immunogenicity of quadrivalent human papillomavirus vaccine in organ transplant recipients. Am J Transplant. (2013) 13(9):2411–7. doi: 10.1111/ajt.12329
62. Boey L, Curinckx A, Roelants M, Derdelinckx I, Van Wijngaerden E, De Munter P, et al. Immunogenicity and safety of the 9-valent human papillomavirus vaccine in solid organ transplant recipients and adults infected with human immunodeficiency virus (HIV). Clin Infect Dis. (2021) 73(3):e661–e71. doi: 10.1093/cid/ciaa1897
63. Nelson DR, Neu AM, Abraham A, Amaral S, Batisky D, Fadrowski JJ. Immunogenicity of human papillomavirus recombinant vaccine in children with CKD. Clin J Am Soc Nephrol: CJASN. (2016) 11(5):776–84. doi: 10.2215/CJN.09690915
64. Chin-Hong PV, Reid GE. Human papillomavirus infection in solid organ transplant recipients: guidelines from the American society of transplantation infectious diseases community of practice. Clin Transplant. (2019) 33(9):e13590 doi: 10.1111/ctr.13590
65. MacIntyre CR, Shaw PJ, Mackie FE, Boros C, Marshall H, Seale H, et al. Long term follow up of persistence of immunity following quadrivalent human papillomavirus (HPV) vaccine in immunocompromised children. Vaccine. (2019) 37(37):5630–6. doi: 10.1016/j.vaccine.2019.07.072
66. Olsson SE, Villa LL, Costa RL, Petta CA, Andrade RP, Malm C, et al. Induction of immune memory following administration of a prophylactic quadrivalent human papillomavirus (HPV) types 6/11/16/18 L1 virus-like particle (VLP) vaccine. Vaccine. (2007) 25(26):4931–9. doi: 10.1016/j.vaccine.2007.03.049
67. Fox TG, Nailescu C. Vaccinations in pediatric kidney transplant recipients. Pediatric Nephrol (Berlin, Germany). (2019) 34(4):579–91. doi: 10.1007/s00467-018-3953-z
68. Dempsey AF, Patel DA. HPV Vaccine acceptance, utilization and expected impacts in the U.S.: where are we now? Hum Vaccin. (2010) 6(9):715–20. doi: 10.4161/hv.6.9.12730
69. Donahue KL, Stupiansky NW, Alexander AB, Zimet GD. Acceptability of the human papillomavirus vaccine and reasons for non-vaccination among parents of adolescent sons. Vaccine. (2014) 32(31):3883–5. doi: 10.1016/j.vaccine.2014.05.035
70. Castellino SM, Allen KE, Pleasant K, Keyes G, Poehling KA, Tooze JA. Suboptimal uptake of human papillomavirus (HPV) vaccine in survivors of childhood and adolescent and young adult (AYA) cancer. J Cancer Surviv: Res and Practice. (2019) 13(5):730–8. doi: 10.1007/s11764-019-00791-9
71. Franke D, Winkel S, Gellermann J, Querfeld U, Pape L, Ehrich JH, et al. Growth and maturation improvement in children on renal replacement therapy over the past 20 years. Pediatric Nephrol (Berlin, Germany). (2013) 28(10):2043–51. doi: 10.1007/s00467-013-2502-z
72. Szilagyi PG, Albertin CS, Gurfinkel D, Saville AW, Vangala S, Rice JD, et al. Prevalence and characteristics of HPV vaccine hesitancy among parents of adolescents across the US. Vaccine. (2020) 38(38):6027–37. doi: 10.1016/j.vaccine.2020.06.074
73. Teeter BS, Jensen CR, Thomas JL, Martin BC, McElfish PA, Mosley CL, et al. Perceptions of HPV vaccination and pharmacist-physician collaboration models to improve HPV vaccination rates. Exploratory Research in Clinical and Social Pharmacy. (2021) 2:100014. doi: 10.1016/j.rcsop.2021
74. Kessler R, Auwaerter P. Strategies to improve human papillomavirus (HPV) vaccination rates among college students. J Am College Health: J of ACH. (2021) :1–8. doi: 10.1080/07448481.2021.1965146. [Epub ahead of print].
75. Perkins RB, Legler A, Jansen E, Bernstein J, Pierre-Joseph N, Eun TJ, et al. Improving HPV vaccination rates: a stepped-wedge randomized trial. Pediatr. (2020) 146(1):e20192737. doi: 10.1542/peds.2019-2737
Keywords: human pappillomavirus, vaccination, kidney transplantation, malignancy, adolescence
Citation: Nailescu C and Shew ML (2022) Human papillomavirus infection-related cancer risk for kidney transplant recipients during adult life can be reduced by vaccination during childhood and adolescence. Front. Pediatr. 10:1057454. doi: 10.3389/fped.2022.1057454
Received: 29 September 2022; Accepted: 15 November 2022;
Published: 30 November 2022.
Edited by:
Blanche Chavers, University of Minnesota Twin Cities, United StatesReviewed by:
Timo Jahnukainen, Helsinki University Hospital, Finland© 2022 Nailescu and Shew. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Corina Nailescu Y25haWxlc2NAaXUuZWR1
Specialty Section: This article was submitted to Pediatric Nephrology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.