 Xavier Carbonell-Estrany1*Eric A. F Simões2,3
Xavier Carbonell-Estrany1*Eric A. F Simões2,3 Louis J Bont4
Louis J Bont4 Angela Gentile5,6
Angela Gentile5,6 Nusrat Homaira7,8Marcelo Comerlato Scotta9,10
Nusrat Homaira7,8Marcelo Comerlato Scotta9,10 Renato T Stein9
Renato T Stein9 Juan P Torres11
Juan P Torres11 Jarju Sheikh12
Jarju Sheikh12 Shobha Broor13Najwa Khuri-Bulos14D James Nokes15,16Patrick K Munywoki15
Shobha Broor13Najwa Khuri-Bulos14D James Nokes15,16Patrick K Munywoki15 Quique Bassat17,18,19,20,21
Quique Bassat17,18,19,20,21 Arun K Sharma22Sudha Basnet22,23
Arun K Sharma22Sudha Basnet22,23 Maria Garba24Joanne De Jesus-Cornejo25Socorro P Lupisan26Marta C Nunes27,28Maduja Divarathna29John R Fullarton30
Maria Garba24Joanne De Jesus-Cornejo25Socorro P Lupisan26Marta C Nunes27,28Maduja Divarathna29John R Fullarton30 Barry S Rodgers-Gray30Ian Keary30Mark Donald C Reñosa31
Barry S Rodgers-Gray30Ian Keary30Mark Donald C Reñosa31 Charl Verwey32David P Moore32Faseeha Noordeen29
Charl Verwey32David P Moore32Faseeha Noordeen29 Sushil Kabra13Marynéa Silva do Vale33
Sushil Kabra13Marynéa Silva do Vale33 Rolando Paternina-De La Ossa34,35
Rolando Paternina-De La Ossa34,35 Cristina Mariño36Josep Figueras-Aloy37Leonard Krilov38
Cristina Mariño36Josep Figueras-Aloy37Leonard Krilov38 Eitan Berezin39
Eitan Berezin39 Heather J Zar40Krishna Paudel41
Heather J Zar40Krishna Paudel41 Marco Aurelio Palazzi Safadi39
Marco Aurelio Palazzi Safadi39 Ghassan Dbaibo42
Ghassan Dbaibo42 Imane Jroundi43Runa Jha44
Imane Jroundi43Runa Jha44 Rukshan A. M Rafeek29Rossiclei de Souza Pinheiro45Marianne Bracht46Rohitha Muthugala47
Rukshan A. M Rafeek29Rossiclei de Souza Pinheiro45Marianne Bracht46Rohitha Muthugala47 Marcello Lanari48
Marcello Lanari48 Federico Martinón-Torres49
Federico Martinón-Torres49 Ian Mitchell50Grace Irimu51Apsara Pandey52,53
Ian Mitchell50Grace Irimu51Apsara Pandey52,53 Anand Krishnan13
Anand Krishnan13 Asuncion Mejias54,55Marcela Santos Corrêa da Costa56
Asuncion Mejias54,55Marcela Santos Corrêa da Costa56 Shrijana Shrestha57
Shrijana Shrestha57 Jeffrey M Pernica58Felipe Cotrim de Carvalho59Rose E Jalango60Hafsat Ibrahim61Atana Ewa62
Jeffrey M Pernica58Felipe Cotrim de Carvalho59Rose E Jalango60Hafsat Ibrahim61Atana Ewa62 Gabriela Ensinck63
Gabriela Ensinck63 Rolando Ulloa-Gutierrez64Alexandre Lopes Miralha45Maria Florencia Lucion5,6
Rolando Ulloa-Gutierrez64Alexandre Lopes Miralha45Maria Florencia Lucion5,6 Md Zakiul Hassan65Zubair Akhtar65Mohammad Abdul Aleem65Fahmida Chowdhury65Pablo Rojo66Charles Sande15
Md Zakiul Hassan65Zubair Akhtar65Mohammad Abdul Aleem65Fahmida Chowdhury65Pablo Rojo66Charles Sande15 Abednego Musau67Khalequ Zaman65Luiza Helena68Falleiros Arlant68
Abednego Musau67Khalequ Zaman65Luiza Helena68Falleiros Arlant68 Prakash Ghimire22April Price69Kalpana Upadhyay Subedi70
Prakash Ghimire22April Price69Kalpana Upadhyay Subedi70 Helena Brenes-Chacon64Doli Rani Goswami65Mohammed Ziaur Rahman65Mohammad Enayet Hossain65Mohammod Jobayer Chisti65Nestor E Vain71
Helena Brenes-Chacon64Doli Rani Goswami65Mohammed Ziaur Rahman65Mohammad Enayet Hossain65Mohammod Jobayer Chisti65Nestor E Vain71 Audrey Lim58Aaron Chiu72Jesse Papenburg73Maria del Valle Juarez5,6
Audrey Lim58Aaron Chiu72Jesse Papenburg73Maria del Valle Juarez5,6 Thamarasi Senaratne74Shiyamalee Arunasalam29
Thamarasi Senaratne74Shiyamalee Arunasalam29 Tor A Strand23Adaeze Ayuk75Olufemi Ogunrinde24Lohanna Valeska de Sousa Tavares76Comfort Garba24Bilkisu I Garba77
Tor A Strand23Adaeze Ayuk75Olufemi Ogunrinde24Lohanna Valeska de Sousa Tavares76Comfort Garba24Bilkisu I Garba77 Jeanette Dawa78Michelle Gordon79
Jeanette Dawa78Michelle Gordon79 Eric Osoro78
Eric Osoro78 Charles N Agoti15Bryan Nyawanda80Mwanajuma Ngama15Collins Tabu60Joseph L Mathew81Andrew Cornacchia82Ganesh Kumar Rai83
Charles N Agoti15Bryan Nyawanda80Mwanajuma Ngama15Collins Tabu60Joseph L Mathew81Andrew Cornacchia82Ganesh Kumar Rai83 Amita Jain84Mateus Sfoggia Giongo9
Amita Jain84Mateus Sfoggia Giongo9 Bosco A Paes58
Bosco A Paes58
- 1Neonatology Service, Hospital Clinic, Barcelona, Spain
- 2Department of Pediatrics, School of Medicine, University of Colorado, Aurora, CO, United States
- 3Department of Epidemiology, Center for Global Health, Colorado School of Public Health, University of Colorado, Aurora, CO, United States
- 4Laboratory of Translational Immunology and Department of Paediatrics, Wilhelmina Children's Hospital, University Medical Centre Utrecht, Utrecht, Netherlands
- 5Epidemiology Department, Austral University, Buenos Aires, Argentina
- 6Ricardo Gutiérrez Children Hospital, Buenos Aires, Argentina
- 7School of Women's and Children's Health, Faculty of Medicine, University of New South Wales, Sydney, NSW, Australia
- 8Respiratory Department, Sydney Children's Hospital, Randwick, NSW, Australia
- 9Pontificia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, Brazil
- 10Hospital Moinhos de Vento, Porto Alegre, Brazil
- 11Department of Pediatrics, Division of Pediatric Infectious Diseases, Faculty of Medicine, Universidad de Chile, Santiago, Chile
- 12Medical Research Council Unit The Gambia at London School of Hygiene and Tropical Medicine, Fajara, The Gambia
- 13All India Institute of Medical Sciences, New Delhi, India
- 14University of Jordan, Amman, Jordan
- 15Centre for Geographic Medicine Research-Coast, Kenya Medical Research Institute-Wellcome Trust Research Programme, Kilifi, Kenya
- 16School of Life Sciences, University of Warwick, Coventry, United Kingdom
- 17ISGlobal, Hospital Clínic - Universitat de Barcelona, Barcelona, Spain
- 18Centro de Investigação em Saúde de Manhiça (CISM), Maputo, Mozambique
- 19Institución Catalana de Investigación y Estudios Avanzados (ICREA), Barcelona, Spain
- 20Pediatrics Department, Hospital Sant Joan de Déu, Universitat de Barcelona, Barcelona, Spain
- 21Consorcio de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP), Madrid, Spain
- 22Department of Paediatrics, Institute of Medicine, Tribhuvan University, Kathmandu, Nepal
- 23University of Bergen, Bergen, Norway
- 24Ahmadu Bello University/Teaching Hospital, Zaria, Nigeria
- 25Research Institute for Tropical Medicine, Muntinlupa, Philippines
- 26RITM-Tohoku Research Collaborating Center for Emerging Infections, Manila, Philippines
- 27South African Medical Research Council: Vaccines and Infectious Diseases Analytics Research Unit, University of the Witwatersrand, Johannesburg, South Africa
- 28Department of Science and Technology/National Research Foundation: Vaccine Preventable Diseases, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
- 29Diagnostic and Research Virology Laboratory, Department of Microbiology, Faculty of Medicine, University of Peradeniya, Peradeniya, Sri Lanka
- 30Violicom Medical Limited, Aldermaston, United Kingdom
- 31Research Institute for Tropical Medicine, Muntinlupa, Philippines
- 32Department of Paediatrics and Child Health, Chris Hani Baragwanath Academic Hospital, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
- 33Hospital Universitário da Universidade Federal do Maranhão, São Luís, Brazil
- 34Hospital Santa Casa de Ribeirão Preto, São Paulo, Brazil
- 35Centro Universitário Barão de Mauá, Ribeirão Preto, São Paulo, Brazil
- 36Hospital Militar Central, Bogotá, Colombia
- 37Neonatology Service, Hospital Clínic de Barcelona, Barcelona, Spain
- 38NYU Long Island School of Medicine, Mineola, NY, United States
- 39Hospital Santa Casa De São Paulo, São Paulo, Brazil
- 40Child Health and the SA-MRC Unit on Child and Adolescent Health, Department of Paediatrics, University of Cape Town (UCT), Cape Town, South Africa
- 41Ministry of Health and Population, Kathmandu, Nepal
- 42Center for Infectious Diseases Research, American University of Beirut, Beirut, Lebanon
- 43School of Medicine and Pharmacy, University Mohamed V, Rabat, Morocco
- 44National Public Health Laboratory, Ministry of Health & Population, Teku, Kathmandu, Nepal
- 45Universidade Federal do Amazonas, Manaus, Brazil
- 46Canadian Premature Babies Foundation, Toronto, ON, Canada
- 47National Hospital – Kandy, Kandy, Sri Lanka
- 48IRCCS-Sant'Orsola University Hospital, Bologna, Italy
- 49Hospital Clínico Universitario de Santiago, Universidade de Santiago, Santiago, Spain
- 50University of Calgary, Calgary, AB, Canada
- 51Department of Paediatrics and Child Health, University of Nairobi, Nairobi, Kenya
- 52Department of Pediatric Nursing, Maharajgunj Nursing Campus, Institute of Medicine, Tribhuwan University, Kathmandu, Nepal
- 53Pediatric Nurses Association of Nepal, Kathmandu, Nepal
- 54Nationwide Childrens Hospital, Columbus, OH, USA
- 55The Ohio State University, Columbus, OH, USA
- 56Hospital Materno-Infantil de Brasília, Brasília, Brazil
- 57Patan Academy of Health Sciences, Lalitpur, Nepal
- 58Department of Pediatrics, McMaster University, Hamilton, ON, Canada
- 59Surveillance Secretariat in Health, Ministry of Health, Brasilia, Brazil
- 60Ministry of Health Kenya, Nairobi, Kenya
- 61Bayero University/Aminu Kano Teaching Hospital, Kano, Nigeria
- 62University of Calabar/University of Calabar Teaching Hospital, Calabar, Nigeria
- 63Hospital de Niños Víctor J. Vilela de Rosario, Santa Fe, Argentina
- 64Hospital Nacional de Niños “Dr. Carlos Sáenz Herrera”, Caja Costarricense del Seguro Social (CCSS), San José, Costa Rica
- 65International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh
- 66University Hospital October 12, Madrid, Spain
- 67PSI Regional Technical Services Office, Nairobi, Kenya
- 68Metropolitan University of Santos, São Paulo, Brazil
- 69London Health Sciences Centre, London, ON, Canada
- 70Paropakar Maternity and Women's Hospital, Kathmandu, Nepal
- 71Hospital Sanatorio Trinidad, Buenos Aires, Argentina
- 72The Children's Hospital of Winnipeg, Winnipeg, MB, Canada
- 73McGill University, Montreal, QC, Canada
- 74General Sir John Kotelawala Defence University, Rathmalana, Sri Lanka
- 75University of Nigeria Teaching Hospital, Enugu, Nigeria
- 76Hospital Infantil Albert Sabin (HIAS), Fortaleza, Ceará, Brazil
- 77Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria
- 78Washington State University – Global Health Kenya, Nairobi, Kenya
- 79Orillia Soldiers’ Memorial Hospital, Orillia, Ontario, Canada
- 80Kenya Medical Research Institute- Center for Global Health Research, Centre for Geographic Medicine Research-Coast, Kilifi, Kenya
- 81Post Graduate Institute of Medical Education & Research, Chandigarh, India
- 82Ministry of Health Canada, Ottawa, ON, Canada
- 83Nepal Pediatric Society (NEPAS), Kanti Children's Hospital, Kathmandu, Nepal
- 84King George's Medical University, Uttar Pradesh, India
Introduction: The high burden of respiratory syncytial virus (RSV) infection in young children disproportionately occurs in low- and middle-income countries (LMICs). The PROUD (Preventing RespiratOry syncytial virUs in unDerdeveloped countries) Taskforce of 24 RSV worldwide experts assessed key needs for RSV prevention in LMICs, including vaccine and newer preventive measures.
Methods: A global, survey-based study was undertaken in 2021. An online questionnaire was developed following three meetings of the Taskforce panellists wherein factors related to RSV infection, its prevention and management were identified using iterative questioning. Each factor was scored, by non-panellists interested in RSV, on a scale of zero (very-low-relevance) to 100 (very-high-relevance) within two scenarios: (1) Current and (2) Future expectations for RSV management.
Results: Ninety questionnaires were completed: 70 by respondents (71.4% physicians; 27.1% researchers/scientists) from 16 LMICs and 20 from nine high-income (HI) countries (90.0% physicians; 5.0% researchers/scientists), as a reference group. Within LMICs, RSV awareness was perceived to be low, and management was not prioritised. Of the 100 factors scored, those related to improved diagnosis particularly access to affordable point-of-care diagnostics, disease burden data generation, clinical and general education, prompt access to new interventions, and engagement with policymakers/payers were identified of paramount importance. There was a strong need for clinical education and local data generation in the lowest economies, whereas upper-middle income countries were more closely aligned with HI countries in terms of current RSV service provision.
Conclusion: Seven key actions for improving RSV prevention and management in LMICs are proposed.
Introduction
Respiratory syncytial virus (RSV) lower respiratory tract infection (LRTI) causes over 3 million hospitalisations and over 100,000 deaths in children under 5 years every year (1, 2). Ninety-nine per cent of these fatalities occur in low- and middle-income countries (LMICs) where RSV has been reported to be the most frequent cause of mortality among infants beyond the neonatal period (1, 2). In light of this substantial burden, RSV LRTI prevention has been identified as a key priority by the World Health Organization (WHO) for the past 20 years (3–5). However, despite over 60 years of research, current preventive measures for RSV disease remain limited to good hygiene and the use of palivizumab, a monoclonal antibody used only for high-risk children, including premature infants (≤35 weeks' gestational age) and those with congenital heart disease and bronchopulmonary dysplasia (6). Additionally the use of palivizumab remains minimal in LMICs due to financial constraints and a lack of confidence among practitioners. This situation is expected to change in the next few years with several new preventive interventions under development, including long-acting monoclonal antibodies and maternal and infant vaccines (7).
Securing access to these interventions at a sustainable cost is often considered the prime concern relating to improving the management of RSV in LMICs (8). Indeed, WHO has stated that emerging vaccines and monoclonal antibodies should be made available to support optimal use in LMICs (9, 10). However, it should be recognised that there are other potential considerations and challenges in LMICs. These include limited access to healthcare, lack of awareness/understanding of the public health impact of RSV among healthcare professionals (HCPs) and policymakers, resource availability constraints, lack of reliable local/regional epidemiological and disease burden data to inform cost-effectiveness assessment and guide preventive efforts, and lack of access to point-of-care tests (8).
The PROUD (Preventing RespiratOry syncytial virUs in unDerdeveloped countries) Taskforce of 24 global RSV experts was established to help understand and propose solutions to these challenges. The Taskforce aims to lobby influential health providers, policymakers, public health organisations, and associations to work collaboratively to combat RSV in LMICs. As the first step to achieve this mission, the Taskforce undertook a detailed assessment of the key considerations and priorities for the prevention and management of RSV infection in LMICs with a global, online-based survey of HCPs and other key stakeholders (public health, policymakers, payers, etc) involved in RSV.
Methods
Study design
The study was conducted in 2021. The survey methodology encompassed two stages, first a qualitative stage to define the scope of the survey, followed by a quantitative stage to provide numerical data for objective analysis (11, 12).
Stage 1
The aim of stage one was to identify all the factors potentially related to the burden of RSV in LMICs, the challenges associated with this burden, and expectations for future management of RSV. This was accomplished by holding three online meetings (29th March; 1st April; 21st April 2021) with members of the PROUD Taskforce. At each meeting, five questions designed to stimulate thoughts about RSV, the burden it presents, and its current and future management in different, but complementary, situations were presented (Supplementary Material 1) and responses were gathered in sequence. Participants were given approximately 5 min to respond to each question. Individuals then took turns to read out their answers to the group to stimulate further suggestions from the other participants. The goal was to capture an exhaustive list of responses – data saturation – after going through all five questions. All responses were video recorded and documented. The responses from the meetings were compiled into a catalogue of distinct factors and used to construct a structured questionnaire (developed and approved by all Taskforce members), which constituted the second stage of the study (Supplementary Material 2).
Stage 2
The purpose of the questionnaire was to assess objectively the importance of each of the factors relative to LMICs when considering two defined scenarios: (1) The current situation regarding RSV management and, (2) Realistic future expectations for RSV management. The questionnaire was available in English on a secure online website (open from 17th August to 10th November 2021), a link to which was distributed via email by the Taskforce to HCPs, researchers, and others interested in RSV amongst their contacts in LMICs. Predicated on a previous study (11), a target of approximately 20 completed questionnaires was set for each of Least Developed/Low-Income (LD), Low-Middle-Income (LM), and Upper-Middle-Income (UM) countries, as defined by the Development Assistance Committee (DAC) List of Official Development Assistance Recipients (13). Representation from several countries withing each economic group was sought. A further approximately 20 completed questionnaires were sought from High-Income countries (HICs), to act as a reference group.
Within the questionnaire, each factor was scored on a continuous (parametric) end-anchored analogue scale from zero (very-low-relevance) to 100 (very-high-relevance) within both scenarios. The option to score any factor as “not relevant” was also provided. The order of the individual factors was randomised for scoring within each scenario to minimise unintended rationalisation of responses. Demographic details, including qualification/position, experience in RSV, and broad information on RSV testing and management in the respondent's country, were also captured on the questionnaire.
Analysis of responses to stage 2 questionnaire
Questionnaire responses were analysed to address two key, interrelated questions:
1) What are the most important overall considerations for RSV management in LMICs?
2) What are the current vs. future priorities for RSV management in LMICs?
Question 1 was addressed by principal component analysis (PCA), with the two aforementioned scenarios as the dependent variables. PCA is a well-established technique for simplifying aggregate responses such that the component factors can be ranked from highest (most important) to lowest (least important) in terms of contribution to the variance across the questionnaire responses (14). Results were analysed for all LMICs combined and then by individual economic groups (LD, LM, UM, and HIC). The top quintile of factors was reported with related factors collated into areas/themes to aid interpretation, as agreed by the Taskforce. Differences between economies were explored further by calculating the relative contribution (loading) of each area/theme to explain the variance in the PCA for the top quintile of factors for each economic group. Question 2 was addressed using linear discriminant function analysis to maximise separation of the factors into those most closely associated with the current situation vs. future expectations, using the combined results for all LMICs.
Prior to analysis, missing data were imputed using the corresponding mean for that factor within each scenario. Factors scored as “not relevant” were assigned an analytically neutral value of 50. All analyses were carried out using SPSS for Windows 15.0 (IBM Corporation, New York, USA) and Excel 365 (Microsoft Corporation, Washington, USA).
Role of the funding source
There was no funding source for this study.
Ethics approval and informed consent
Ethics approval and patient consent was not required for this study. This study was a voluntary survey of clinicians and scientists regarding RSV infection, its prevention and management. No intervention was mandated, clinical practice was not affected and clinical data were not collected.
Results
Stage 1 – online meetings
Eighteen members of the Taskforce participated in the online meetings, 16 of whom represented LMICs (AG, NH, MS, JS, ShB, NKB, JN, PM, QB, AS, SB, MG, JDJC, SL, MN, and MD) and two (XCE and BP) from HICs. A catalogue of 100 individual factors potentially relevant to the current and future management of RSV in LMICs was generated (Supplementary Material 2).
Stage 2 – questionnaire
Ninety questionnaires were completed, of which 70 were from LMICs and 20 from HICs (Table 1), after distribution to 198 people (45.5% response rate). Sixteen LMICs and nine HICs were represented in the survey (Supplementary Material 3). Overall, 34,600 numerical data points were generated for analysis, with 8% (7/90) of questionnaires returned incomplete (missing data: 1,400/36,000; 3.9%). The majority (50/70; 71%) of respondents from LMICs were medical doctors, with approximately half (37/70; 53%) having at least ten years' experience in the RSV field. Other respondents were primarily researchers and scientists, with LD and LM countries represented by a higher proportion of such professionals than UM and HICs. Knowledge/awareness of RSV within LMICs was perceived to be low by 39% (27/70) of respondents, and 23% (16/70) believed that RSV infection is afforded the necessary recognition as a priority public health issue. RSV testing for research/clinical management, was undertaken in LMICs by 43/70 (61%) of the respondents, primarily using polymerase chain reaction (PCR) tests. Palivizumab was reported to be locally available by nearly half (33/70; 47%) of respondents from LMICs, although an absence of support or public funding reduced equitable access for 48% (16/33) of these respondents. For the two lowest economic groups (LD and LM), knowledge/awareness of RSV, RSV prioritisation, RSV testing, and palivizumab publicly funded/support was notably lower than for UM countries, which were much closely aligned with HICs.
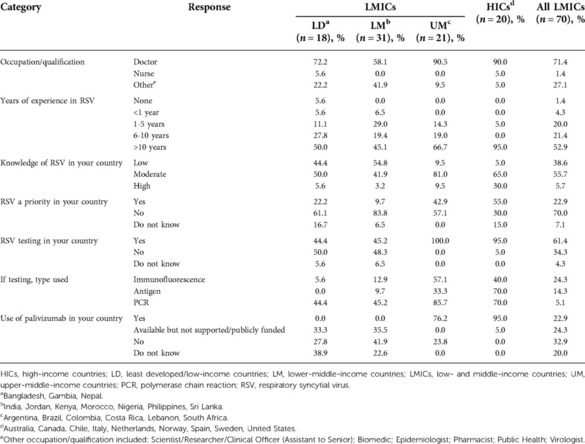
Table 1. Demographics and background information of respondents and the RSV situation in their countries.
Q1 – most important overall considerations for RSV management in LMICs
The single most important need identified for RSV management in LMICs was that for a simple, rapid, low-cost, point-of-care diagnostic test (Table 2), especially as testing access was considered limited, particularly in rural settings. The need for locally relevant data on the epidemiology and burden of RSV was also strongly represented, with two of the top five factors, and five of the top 20 factors being related to data generation on these topics, including establishing surveillance programmes, data on at-risk groups, and increasing understanding about the impact of co-infections. Affordability and access to future vaccines and prophylaxis and the need to improve service provision, including proactively establishing RSV vaccine delivery programmes and availability of oxygen and pulse oximeters, were also key themes. Other key factors identified related to clinical education, including the development of international, easy-to-follow, point-of-care guidelines, the need for a RSV vaccine, engagement with public health, policymakers and payers, and parent/public education. For the latter point, building on the lessons from coronavirus (COVID-19) to teach parents hygiene measures for avoiding RSV infection was scored highly.
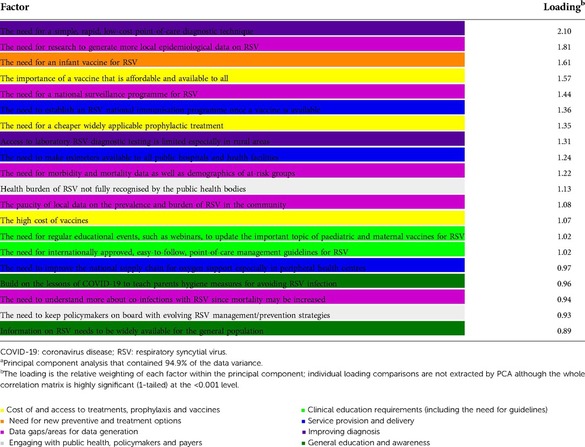
Table 2. Top quintile of most important factors (n = 20) related to both current and future management of RSV in LMICsa.
When analysed by economic status, a particular need was identified in LD and LM countries for local data generation and clinical education on RSV (Figure 1), including the need for training on RSV diagnosis and enabling distinction from bacterial infection (Supplementary Material 4). By contrast, the primary focus in UM and HICs was on the need for new preventive and treatment options for RSV, and their cost. Improving diagnosis and overall service provision was a marginally less pressing concern in UM than LD and LM countries. General education and awareness about RSV and engagement with key stakeholders appeared imperatives regardless of economic status.
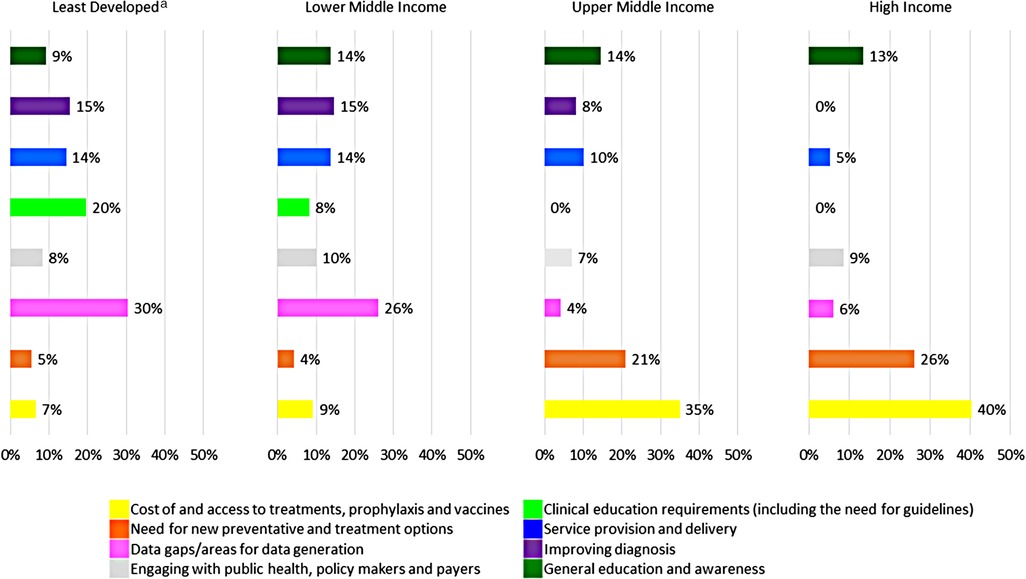
Figure 1. Most important areas related to the current and future management of respiratory syncytial virus categorised by economic groupb. bBars represent the relative contribution (loading) of each area/theme to explaining the variance in the principal component analysis for the top quintile of factors for each economic group. aIncluding low-income countries.
Q2 – current and future priorities in RSV management in LMICs
All key areas identified as important for LMICs – improved diagnosis, data generation, clinical and general education, availability and access to new interventions, and engagement with policymakers/payers etc – were strongly associated with current RSV management (Table 3). Overall, more factors aligned with current (n = 19) than future RSV management (n = 7). Factors relevant to the current situation included the possibility of leveraging the experience of managing COVID-19 with policymakers to inform strategies for RSV prevention. However, it was also recognised that vaccines for other diseases might be prioritised over RSV vaccination. Future priorities centred around on-going education (6/7; 86%).
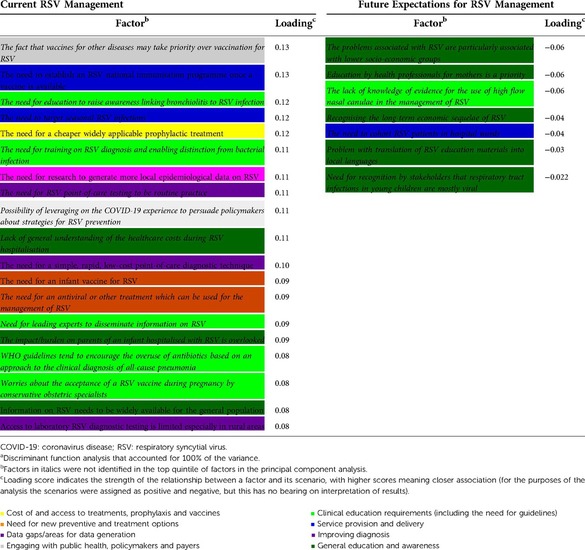
Table 3. Key factors distinguishing between current and future management of RSV in LMICsa.
Discussion
This study, led by the PROUD Taskforce, provides detailed insights into the significant considerations and priorities concerning the management and prevention of RSV in LMICs. Countries of the two lowest economic groups (LD and LM) were far more closely aligned with each other than with UM countries, which closely resembled HICs. Many of the same issues and needs were raised across all LMICs, and differences between economies predominantly related to focus or prioritisation. Predicated on the survey results, we propose seven key actions to effect change in LMICs (Table 4).
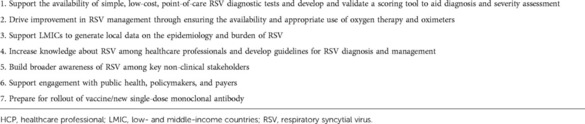
Table 4. Key actions for the prevention and management of RSV in LMICs.
First, to support the availability of a simple, low-cost, point-of-care diagnostic test, which was identified as the most important need in LMICs (Table 2). This is a particular need in LD and LM countries, where 44.4% and 45.2%, respectively, reported that RSV testing was available, and this is likely concentrated in the larger urban hospitals and universities. Confirmatory diagnosis of RSV (and other viral infections) is important to help avoid the inappropriate use of antibiotics and the spread of multi-resistant bacteria in LMICs (15). However, increased provision of such diagnostic tests is unlikely to be a viable option in many LMICs due to cost and logistical constraints (8, 16). A potential solution, particularly in lower income areas, is the validation and adoption of a scoring tool to inform clinical diagnosis and assessment of RSV disease severity (8). Such a tool could combine demographic and clinical parameters (e.g., age <6 months; infection during RSV season/during periods of increased detection; oxygen saturation <90%; tachypnoea; nasal flaring/grunting; apnoea; chest retractions; dehydration; poor feeding; cyanosis; lethargy; rales/rhonchi/wheezing) and prognostic biomarkers (17, 18). A meta-analysis or review of the currently available demographic and clinical profile data for children with RSV infection might serve as a baseline for development of a tool, and may guide local replication and data for validation. Additionally, the tool could be employed to target the use of RSV tests for confirmatory diagnosis and support local data generation.
Second, drive improvement in RSV management through availability and appropriate oxygen therapy and oximeters. LD and LM countries primarily focussed on improving the oxygen supply chain, while UM countries emphasised the need for more pulse oximeters (Supplementary Material 4). The importance of oxygen therapy and limited availability in LD countries is well-recognised and documented in a specific WHO report (19). We strongly advocate that LMICs be supported in their need for improved access to oxygen therapy, particularly considering the ongoing demands placed on respiratory support measures by COVID-19. Notably, the resolution of this issue depends on having the tools and expertise to make best use of the oxygen supply available (19, 20), and would be a core component covered in the clinical guidelines and education proposed below. Of note, oxygen administration via high-flow nasal cannulae can be very effective in severe cases and is a relatively simple technique. The emergence of COVID-19 has led to increased capacity building and logistical support, including oxygen supply for most countries, and extends an opportunity to leverage the existing enhanced infrastructure to better manage RSV.
Third, support LMICs to generate local data on the epidemiology and burden of RSV. Our findings indicate that the need for improved epidemiological and burden of illness data on RSV was driven primarily by the responses from LD and LM countries, although UM (and HICs) also expressed a desire for increased evidence (Figure 1). This aligns with a recent report indicating that only 54% (77/142) of LMICs have published data on the burden of RSV (8), and that routine surveillance for this virus may not be ongoing or sustainable. This shortfall perhaps relates to the challenges of obtaining a reliable diagnosis of RSV and capturing both hospital and community-based data, where most cases occur in the latter (2, 8, 21–23). Targeted efforts to address these data needs in LMICs are essential to support negotiations with policymakers and current and future payers (e.g., Gavi, should a vaccine become available) and inform RSV immunisation and educational programmes for HCPs and the wider population. The WHO and Bill & Melinda Gates Foundation RSV surveillance programme has been initiated in 25 countries to support the introduction of RSV immunisation (24, 25), but more investment in this initiative is necessary. Strategies to gather and publish local data should be a focus for governments, healthcare providers, and non-governmental organisations (NGOs). The Child Health and Nutrition Research Initiative (CHNRI) method (26), a widely utilised framework to maximise return on research investment, was suggested to help prioritise the data generation.
Fourth, strongly support education, teaching and training for all relevant HCPs, including the development of simple, implementable RSV management guidelines. Given the comparatively low levels of knowledge and prioritisation of RSV in LD and LM countries vs. UM and HICs (Table 1), the survey highlighted a strong need for clinical education in countries in the two lowest economic groups (Figure 1). Two key factors were highlighted: the need for simple RSV guidelines and training on distinction from bacterial infection (Supplementary Material 4). There is widespread awareness of the WHO guideline for Integrated Management of Childhood Illness (IMCI) (27) in LMICs; however, the guideline focusses on early recognition and antibiotic treatment of childhood pneumonia, and RSV is not emphasised as a principal causal agent for LRTI. We recommend, therefore, that a specific RSV management guideline be developed, recognising resource and logistical restrictions prevalent in these countries that can be easily adapted and implemented at a local level. RSV experts should undertake development in partnership with key HCPs from the target countries to ensure their perspective is accurately captured while maximising the cultural and infrastructural relevance of the guidelines (28, 29). Utilisation of a Delphi methodology or other recognised consensus building approach is recommended to maximise robustness and applicability. Essential aspects to cover are information and updates on RSV vaccines and emerging monoclonal antibodies for RSV prevention (Table 2). Ideally, the proposed guideline will provide information on RSV infection as a significant cause of viral-related LRTI and support its addition to the new IMCI with appropriate management. A multichannel educational programme, available in a range of languages, involving webinars and modular learning programmes would permit flexibility in delivery.
Fifth, build broader awareness of RSV among non-clinical stakeholders. Increasing awareness of RSV and its associated burden amongst parents, payers, and public health stakeholders was a consistent need identified across all LMICs, including HICs (Figure 1). Overall, LD and LM countries recognised the need for basic RSV education, whereas the focus in UM countries and HICs was for more specific information on risk groups, and prevention strategies (Table 3 and Supplementary Material 4). This likely reflects differences in viewed priorities, with LD countries building their response to RSV from the ground up, whilst in more developed economies, the focus was on refining existing services. Lessons learnt from COVID-19, particularly the adoption of hygiene measures, were strongly advocated to prevent RSV infection (Table 2). Education of all key stakeholders was considered fundamental to driving change, improving management, and reducing the burden of RSV in LMICs.
Sixth, support engagement with public health, policymakers, and payers across all economic groups (Table 2 and Figure 1). The health burden of RSV was perceived to be not fully recognised by public health agencies in LMICs, particularly in LD and LM countries (Supplementary File 4), which indicates that RSV is not afforded the priority it richly deserves in these nations (Table 1). The actions detailed above all support engagement and lobbying for increased recognition and funding for RSV at a local level to improve current management, and pave the way for emerging RSV preventive modalities.
Lastly, development of a safe, effective RSV vaccine and new monoclonal antibodies and preparation for rollout. Whilst there was a strong desire for these preventive interventions, concerns about cost and how this could potentially limit access were raised by all economic groups (Table 2, Figure 1, and Supplementary Material 4). Proportionally, UM and HICs placed more emphasis on cost and access than LD and LM countries, reflecting that more work is needed in the latter in terms of building RSV awareness and service provision. WHO-led negotiations with the manufacturers will be critical to ensure equitable access in LMICs. Of the potential interventions, an infant vaccine received largest support from LMICs and, perhaps surprisingly, more support than maternal vaccination offering passive protection for at-risk infants. This may reflect the cost and logistical constraints apparent with palivizumab prophylaxis and the success of other global infant vaccines (e.g., polio). Interestingly, a recently published retrospective analysis of a randomised controlled trial reported that over the first 3 months of life, maternal vaccination prevented 5.1 antimicrobial courses per 100 infants in LMICs, representing 10.9% of all antimicrobial prescribing (30). Hence, the availability of a maternal vaccine may have the potential to reduce the (over)reliance on antibiotic treatment of childhood pneumonia in these countries. The need to establish national RSV prevention programmes once a vaccine and other therapeutic interventions are available was strongly expressed; partnership with Gavi, the Vaccine Alliance, will be essential. The COVID-19 pandemic potentially offers an excellent opportunity to enhance immunisation programmes for respiratory viruses, including setting-up a similar scheme to COVAX for RSV (31).
Several limitations of the survey should be recognised. Respondents were first chosen by the Taskforce members based on known interest in RSV, and then on their willingness to complete the survey, which poses a potential selection bias. The respondents were also primarily physicians and researchers from leading national centres, reflecting the membership of the Taskforce and their contacts. These factors were not considered significant limitations, as the goal was to gain a detailed understanding of the priorities and needs within LMICs, which the respondents were certainly able to provide. The questionnaire being available only in English is another potential limitation, although a single version of the questionnaire was preferable to multiple translations. Finally, completer bias may be relevant because of the lengthy questionnaire (background information plus scoring 100 factors across two scenarios). However, missing data (3.9%) was minimal, so replacement with mean values is unlikely to have significantly influenced the results. Furthermore, the use of three meetings to generate a list of items, scoring them for relevance, and randomising the factors within the two scenarios helped mitigate any tendency to rationalise responses, which may introduce bias in surveys (32). Moreover, the methodology employed for the survey started with no predetermined questions but generated an exhaustive list of factors which is a major strength. It should also be recognised that the findings are in-line with other similar studies, supporting their veracity (8, 9, 20).
Our study has provided a novel, LMIC-led perspective on the major considerations and priorities to improve the management and reduce the substantial burden of RSV infection in LMICs, and its impact on children. Seven key actions have been proposed, all of which are eminently achievable. We call upon the support of WHO, NGOs, and other key stakeholders to make them a reality.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
XCE, BP, ES, LB, JF and BRG came up with the concept of the survey. All Taskforce members (see below) participated in the meetings and/or designed and approved the questionnaire. All other authors completed the questionnaire. XCE, BP, JF and BRG drafted the manuscript with input from ES and LB. All authors critically reviewed the manuscript and agreed upon submission for publication. All authors contributed to the article and approved the submitted version.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
PROUD taskforce
XCE, BAP, LJB, AG, NH, MS, RTS, JPTT, JS, SB, NK-B, DJN, PKM, QB, AS, SB, MG, JDJ, SPL, MCN, MD, JRF, BSR, EAFS.
Conflict of interest
The reviewer PAP declared a past co-authorship with the author(s) FMT to the handling. XCE and BP have received research funding and/or compensation as advisor/lecturer from AbbVie and AstraZeneca. JF and BRG, working for Violicom and former company, have previously received payment from AbbVie and AstraZeneca for work on various projects. MCN reports grants from the Bill & Melinda Gates Foundation, European & Developing Countries Clinical Trials Partnership, Pfizer, AstraZeneca and Sanofi-Pasteur; and personal fees from Pfizer and Sanofi-Pasteur. RTS has received fees for Advisory Board meetings and lectures for Sanofi-Pasteur, AstraZeneca, Janssen, and AbbVie. QB serves in the Independent Data Monitoring Committee (IDMC) for Respiratory Syncytial Virus (RSV) vaccine development for the protection of infants (since October 2015) (GlaxoSmithKline -GSK). JP reports grants to his institution from MedImmune, Merck, Sanofi Pasteur and AbbVie, and personal fees from AbbVie, Merck and AstraZeneca. JMP reports grants to his institution from MedImmune. HJZ has received funding for RSV-related research studies from Pfizer, AstraZeneca, Merck and the Bill & Melinda Gates Foundation. AM has received research funding from Merck and Janssen and compensation as advisor/lecturer from Sanofi-Pasteur and AstraZeneca. IM has been an investigator on studies funded by MedImmune, Regeneron, and Boehringer. MAS has received research funding from Janssen and compensation as advisor/lecturer from AbbVie, Sanofi-Pasteur and AstraZeneca. All declarations made by authors outside of the submitted work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at https://www.frontiersin.org/articles/10.3389/fped.2022.1033125/full#supplementary-material.
References
1. Shi T, McAllister DA, O'Brien KL, Simoes EAF, Madhi SA, Gessner BD, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. (2017) 390(10098):946–58. doi: 10.1016/S0140-6736(17)30938-8
2. Li Y, Wang X, Blau DM, Caballero MT, Feikin DR, Gill CJ, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. (2022) 399(10340):2047–64. doi: 10.1016/S0140-6736(22)00478-0
3. Wright PF, Cutts FT. Generic protocol to examine the incidence of lower respiratory infection due to respiratory syncytial virus in children less than five years of age: Field test version. Geneva: World Health Organization (2000). WHO document WHO/V&B/00.08.
4. Modjarrad K, Giersing B, Kaslow DC, Smith PG, Moorthy VS. WHO RSV vaccine consultation expert group. WHO consultation on respiratory syncytial virus vaccine development report from a world health organization meeting held on 23–24 march 2015. Vaccine. (2016) 34(2):190–7. doi: 10.1016/j.vaccine.2015.05.093
5. Legand A, Briand S, Shindo N, Brooks WA, de Jong MD, Farrar J, et al. Addressing the public health burden of respiratory viruses: the battle against respiratory viruses (BRaVE) initiative. Future Virol. (2013) 8(10):953–68. doi: 10.2217/fvl.13.85
6. Synagis 100 mg/ml solution for injection. November 2021. https://www.medicines.org.uk/emc/product/6963/smpc#gref, Accessed November 2021.
7. PATH. RSV vaccine and mAB snapshot, September, 2021. https://path.azureedge.net/media/documents/RSV-snapshot_28SEP2021_HighResolution.pdf, Accessed November 2021.
8. Carbonell-Estrany X, Rodgers-Gray BS, Paes B. Challenges in the prevention or treatment of RSV with emerging new agents in children from low- and middle-income countries. Expert Rev Anti Infect Ther. (2021) 19(4):419–41. doi: 10.1080/14787210.2021.1828866
9. World Health Organization. WHO preferred product characteristics for Respiratory syncytial virus (RSV) vaccines. https://apps.who.int/iris/bitstream/handle/10665/258705/WHO-IVB-17.11-eng.pdf, Accessed November 2021.
10. Sparrow E, Adetifa I, Chaiyakunapruk N, Cherian T, Fell DB, Graham BS, et al. WHO Preferred product characteristics for monoclonal antibodies for passive immunization against respiratory syncytial virus (RSV) disease in infants - key considerations for global use. Vaccine. (2022) 40(26):3506–10. doi: 10.1016/j.vaccine.2022.02.040.
11. Carbonell-Estrany X, Dall’Agnola A, Fullarton JR, Rodgers-Gray BS, Girardi E, Mussa A, et al. Interaction between healthcare professionals and parents is a key determinant of parental distress during childhood hospitalisation for respiratory syncytial virus infection [European RSV outcomes study (EROS)]. Acta Pædiatrica. (2018) 107:854–60. doi: 10.1111/apa.14224
12. Dignass AU, Paridaens K, Al Awadhi S, et al. Multinational evaluation of clinical decision-making in the treatment and management of mild-to-moderate ulcerative colitis. Scand J Gastroenterol. (2022) 57(4):424–31. doi: 10.1080/00365521.2021.2015801
13. OECD. The DAC List of ODA Recipients. https://www.oecd.org/dac/financing-sustainable-development/development-finance-standards/DAC-List-ODA-Recipients-for-reporting-2021-flows.pdf, Accessed January 2022.
14. Jolliffe IT, Cadima J. Principal component analysis: a review and recent developments. Philos Trans A Math Phys Eng Sci. (2016) 374(2065):20150202. doi: 10.1098/rsta.2015.0202
15. Pokharel S, Raut S, Adhikari B. Tackling antimicrobial resistance in low-income and middle-income countries. BMJ Glob Health. (2019) 4(6):e002104. doi: 10.1136/bmjgh-2019-002104
16. Hogan CA, Caya C, Papenburg J. Rapid and simple molecular tests for the detection of respiratory syncytial virus: a review. Expert Rev Mol Diagn. (2018) 18(7):617–29. doi: 10.1080/14737159.2018.1487293
17. Balanza N, Erice C, Ngai M, Varo R, Kain KC, Bassat Q. Host-Based prognostic biomarkers to improve risk stratification and outcome of febrile children in low- and middle-income countries. Front Pediatr. (2020) 8:552083. doi: 10.3389/fped.2020.552083
18. Caserta MT, Qiu X, Tesini B, Wang L, Murphy A, Corbett A, et al. Development of a global respiratory severity score for respiratory syncytial virus infection in infants. J Infect Dis. (2017) 215(5):750–6. doi: 10.1093/infdis/jiw624
19. World Health Organization. 2016. Oxygen therapy for children. Available at: https://www.who.int/publications/i/item/9789241549554, Accessed January 2022.
20. Duke T, English M, Carai S, Qazi S. Paediatric care in the time of COVID-19 in countries with under-resourced healthcare systems. Arch Dis Child. (2020) 105:616–7. doi: 10.1136/archdischild-2020-319333
21. Simões EAF, Dani V, Potdar V, Crow R, Satav S, Chadha MS, et al. Mortality from respiratory syncytial virus in children under 2 years of age: a prospective community cohort study in rural maharashtra, India. Clin Infect Dis. (2021) 73(Suppl_3):S193–202. doi: 10.1093/cid/ciab481
22. Murphy C, MacLeod WB, Forman LS, Mwananyanda L, Kwenda G, Pieciak RC, et al. Risk factors for respiratory syncytial virus-associated community deaths in Zambian infants. Clin Infect Dis. (2021) 73(Suppl_3):S187–92. doi: 10.1093/cid/ciab453
23. Mazur NI, Löwensteyn YN, Willemsen JE, Gill CJ, Forman L, Mwananyanda LM, et al. Global respiratory syncytial virus–related infant community deaths. Clin Infect Dis. (2021) 73(Suppl 3):S229–37. doi: 10.1093/cid/ciab528
24. World Health Organization. Global Influenza Programme: RSV data reporting and outputs. https://www.who.int/teams/global-influenza-programme/global-respiratory-syncytial-virus-surveillance/rsv-data-reporting-and-outputs, Accessed January 2022.
25. Ananworanich J, Heaton PM. Bringing preventive RSV monoclonal antibodies to infants in low- and middle-income countries: challenges and opportunities. Vaccines (Basel). (2021) 9(9):961. doi: 10.3390/vaccines9090961
26. Rudan I, Gibson JL, Ameratunga S, El Arifeen S, Bhutta ZA, Black M, et al. Setting priorities in global child health research investments: guidelines for implementation of the CHNRI method. Croat Med J. (2008) 49(6):720–33. doi: 10.3325/cmj.2008.49.720
27. World Health Organization. Integrated Management of Childhood Illness. IMCI Adaptation Guide. https://www.who.int/maternal_child_adolescent/documents/pdfs/imci_adaptation_guide_2c.pdf?ua=1, Accessed February 2022.
28. Olayemi E, Asare EV, Benneh-Akwasi Kuma AA. Guidelines in lower-middle income countries. Br J Haematol. (2017) 177:846–54. doi: 10.1111/bjh.14583
29. English M, Irimu G, Nyamai R, Were F, Garner P, Opiyo N. Developing guidelines in low-income and middle-income countries: lessons from Kenya. Arch Dis Child. (2017) 102:846–51. doi: 10.1136/archdischild-2017-312629
30. Lewnard JA, Fries LF, Cho I, Chen J, Laxminarayan R. Prevention of antimicrobial prescribing among infants following maternal vaccination against respiratory syncytial virus. Proc Natl Acad Sci USA. (2022) 119:e2112410119. doi: 10.1073/pnas.2112410119
31. World Health Organization. COVAX: Working for global equitable access to COVID-19 vaccines. https://www.who.int/initiatives/act-accelerator/covax, Accessed January 2022.
Keywords: RSV, developing countries, burden, diagnostics, management, prevention, decision research
Citation: Carbonell-Estrany X, Simões EAF, Bont LJ, Gentile A, Homaira N, Scotta MC, Stein RT, Torres JP, Sheikh J, Broor S, Khuri-Bulos N, Nokes DJ, Munywoki PK, Bassat Q, Sharma AK, Basnet S, Garba M, De Jesus-Cornejo J, Lupisan SP, Nunes MC, Divarathna M, Fullarton JR, Rodgers-Gray BS, Keary I, Reñosa MDC, Verwey C, Moore DP, Noordeen F, Kabra S, do Vale MS, Paternina-De La Ossa R, Mariño C, Figueras-Aloy J, Krilov L, Berezin E, Zar HJ, Paudel K, Safadi MAP, Dbaibo G, Jroundi I, Jha R, Rafeek RAM, Pinheiro RdS, Bracht M, Muthugala R, Lanari M, Martinón-Torres F, Mitchell I, Irimu G, Pandey A, Krishnan A, Mejias A, da Costa MCS, Shrestha S, Pernica JM, de Carvalho FC, Jalango RE, Ibrahim H, Ewa A, Ensinck G, Ulloa-Gutierrez R, Miralha AL, Lucion MF, Hassan MZ, Akhtar Z, Aleem MA, Chowdhury F, Rojo P, Sande C, Musau A, Zaman K, Helena L, Arlant F, Ghimire P, Price A, Subedi KU, Brenes-Chacon H, Goswami DR, Rahman MZ, Hossain ME, Chisti MJ, Vain Nestor E, Lim A, Chiu A, Papenburg J, Juarez MdV, Senaratne T, Arunasalam S, Strand Tor A, Ayuk A, Ogunrinde O, Tavares LVdS, Garba C, Garba BI, Dawa J, Gordon M, Osoro E, Agoti CN, Nyawanda B, Ngama M, Tabu C, Mathew JL, Cornacchia A, Rai GK, Jain A, Giongo MS and Paes BA (2022) Identifying the research, advocacy, policy and implementation needs for the prevention and management of respiratory syncytial virus lower respiratory tract infection in low- and middle-income countries. Front. Pediatr. 10:1033125. doi: 10.3389/fped.2022.1033125
Received: 31 August 2022; Accepted: 12 October 2022;
Published: 9 November 2022.
Edited by:
Josette Raymond, Hôpital de Bicêtre, FranceReviewed by:
Pedro A Piedra, Baylor College of Medicine, United StatesArturo Solis-Moya, Dr. Carlos Sáenz Herrera National Children's Hospital, Costa Rica
© 2022 Carbonell-Estrany, Simões, Bont, Gentile, Homaira, Scotta, Stein, Torres, Sheikh, Broor, Khuri-Bulos, Nokes, Munywoki, Bassat, Sharma, Basnet, Garba, De Jesus-Cornejo, Lupisan, Nunes, Divarathna, Fullarton, Rodgers-Gray, Keary, Reñosa, Verwey, Moore, Noordeen, Kabra, do Vale, Paternina-De La Ossa, Mariño, Figueras-Aloy, Krilov, Berezin, Zar, Paudel, Safadi, Dbaibo, Jroundi, Jha, Rafeek, Pinheiro, Bracht, Muthugala, Lanari, Martinón-Torres, Mitchell, Irimu, Pandey, Krishnan, Mejias, Santos Corrêa Da Costa, Shrestha, Pernica, Cotrim de Carvalho, Jalango, Ibrahim, Ewa, Ensinck, Ulloa-Gutierrez, Miralha, Lucion, Hassan, Akhtar, Aleem, Chowdhury, Rojo, Sande, Musau, Zaman, Arlant, Ghimire, Price, Subedi, Brenes-Chacon, Goswami, Rahman, Hossain, Chisti, Vain, Lim, Chiu, Papenburg, Juarez, Senaratne, Arunasalam, Strand, Ayuk, Ogunrinde, Tavares, Garba, Garba, Dawa, Gordon, Osoro, Agoti, Nyawanda, Ngama, Tabu, Mathew, Cornacchia, Rai, Jain, Giongo and Paes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xavier Carbonell-Estrany eGF2aWVyQGNhcmJvbmVsbGVzdHJhbnkubmV0
Specialty Section: This article was submitted to Pediatric Infectious Diseases, a section of the journal Frontiers in Pediatrics