 Neamin Tesfay
Neamin Tesfay Frehiwot Legesse1
Frehiwot Legesse1 Fitsum Woldeyohannes
Fitsum Woldeyohannes
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 28 November 2022
Sec. Neonatology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.1030981
Background: The global burden of stillbirth has declined over time. However, the problem is still prominent in South Asian and Sub-Saharan African countries. Ethiopia is one of the top stillbirth-reporting countries worldwide. Despite several measures taken to reduce the burden of stillbirth; the pace of decline was not as good as the post-neonatal death. Thus, this study is aimed at identifying potential factors related to stillbirth in Ethiopia based on nationally reviewed perinatal deaths
Method: The national perinatal death surveillance data were used for this study. A total of 3,814 reviewed perinatal death were included in the study. Two model families,namely generalized estimating equation, and alternating logistic regression models from marginal model family were employed to investigate the risk factors of stillbirth. The alternating logistic regression model was selected as the best fit for the final analysis.
Result: Among reviewed perinatal deaths nearly forty percent (37.4%) were stillbirths. The findings from the multivariate analysis demonstrated that the place of birth (in transit and at home), cause of death (infection, and congenital and chromosomal abnormalities), maternal health condition (women with complications of pregnancy, placenta, and cord), delay one (delay in deciding to seek care) and delay three (delay in receiving adequate care) were associated with an increased risk of having a stillbirth. On the other hand, maternal education (women with primary and above education level) and the type of health facility (women who were treated in secondary and tertiary health care) were associated with a decreased risk of having a stillbirth.
Conclusion: The study identified that both individual (place of delivery, cause of death, maternal health condition, maternal education, and delay one) and facility level (type of health facility and delay three) factors contributed to stillbirth outcome. Therefore, policies that are aimed at encouraging institutional delivery, improving health seeking behavior, and strengthening facility-level readiness should be devised to reduce the high burden of stillbirth in Ethiopia.
Stillbirth (fetal death) is defined as the death of a fetus in the uterus before the onset of labor and during delivery (1). Stillbirth has significant national and individual implications; nationally, it is one of the important yardsticks used to assess the overall health system of a nation; and at an individual level, it can result in an unparalleled financial and psychological impact on parents (2). Globally, the rate of stillbirth has dropped from 21.4 per 1,000 live birth(LBs) in 2000, with a 2.3% annual rate of reduction(ARR), to 13.9 per 1,000 live birth(LBs) in 2019 (3). Despite the significant global reduction, the burden is still disproportionally high in Sub-Saharan African and South Asian countries (4).
Every Newborn Action Plan (ENAP) is one of the global initiatives designed to improve neonatal outcomes. In addition, strategies for ending preventable maternal mortality were also put in place to reduce inequality in service provision (5). To better frame those strategies, the world health organization (WHO) general assembly in 2014 adopted target of ENAP, which has a goal of reducing the stillbirth rate to only 12 deaths per 1,000 live birth by 2030 (6).
Ethiopia is one of the countries that has a very high burden of stillbirth (3). The country has reduced the rate of stillbirth from 35.8 per 1,000 LBs in 2000, with an ARR of 2.0%, to 24.6 per 1,000 LBs in 2019 (3, 7). However, compared to other health outcome indicators. the rate of reduction was rather slow and stagnant (8). The presence of noticeable regional variation is one of the reasons believed to have hampered the pace of decline at a national level (9).
One of the key strategies of ENAP is generating real-time information on every newborn death and facilitating decisions to improve the quality of service to avert similar preventable death in the future (10). To this effect, Ethiopia established the perinatal death surveillance and response system (PDSR) in 2017, which was integrated into the pre-existing maternal death surveillance and response (MDSR) system (11). Accordingly, in August 2017, the MDSR system was changed to a more comprehensive Maternal and Perinatal Death Surveillance and Response (MPDSR) system by harmonizing perinatal and maternal death surveillance systems (12).
MPDSR operates both at the community and health facility level and provides actionable data on perinatal death (mortality level, cause of death, contributing factors) in real time (13). The primary focus of PDSR system is to utilize the findings for planning appropriate and effective preventive actions; however, the system implementation has been challenged by low engagement of the community and poor utilization of the data to produce evidence-based decisions (14).
Ethiopia has adopted a multi-faceted approach to minimize the high burden of stillbirth and neonatal mortality. Beyond establishing MPDSR, some of the strategies employed include, enhancing behavioral and nutritional intervention, prevention and treatment of medical disorders, and Infection screening and monitoring during labour and delivery as well as Improving intrapartum care were the major ones (15–20). However, despite all this effort, Ethiopia is still facing a significantly high burden of stillbirth and the country has failed to achieve the national target set for 2020 (21). This is attributed to the lack of coordination, notable regional variation, and absence of a robust monitoring mechanism (22, 23).
Globally, 40% of stillbirths occur during labour, which signals the role of quality of intrapartum care in reducing the burden of stillbirth (24). In general, multiple factors could result in stillbirth, which can generally be categorized as maternal, fetal, and facility-level factors (25). Congenital malformation, infection, gestational age, sex, and birth weight are the fetal factors related to stillbirth (26–30), while maternal health conditions before and during pregnancy, maternal age, maternal parity, history of ANC visit, mode of delivery, maternal education, wealth index, birth interval, previous history of stillbirth, fetal movement monitoring are the major maternal factors (31–35). On the other hand, factors such as intrapartum monitoring, clinical management, and capacity of diagnosis are some of the facility-level predictors of stillbirth (36).
Although Ethiopia has a very high burden of stillbirth, the area has received limited attention when it comes to generating scientific evidence. Therefore, this study—among others—is aimed at identifying risk factors that are associated with stillbirth by considering both individual and facility-level factors.
Ethiopia has an estimated population of 117,876,000 in 2021, out of which 17, 216,372 are under-five children (37). Administratively, Ethiopia has nine regions and two city administrations, namely Tigray, Afar, Amhara, Oromia, Somali, Benishangul-Gumuz, Southern Nations Nationalities, and Peoples Region (SNNPR), Gambella, Harari, Addis Ababa city administration and Dire Dawa city administration (38). The country has high infant, under-five, and maternal mortality (47 per 1000LBs), (59 per 1000LBs), and (412 per 100,00 LBs), respectively (39, 40).
The study used data from Ethiopian Public Health Institutes (EPHI); perinatal death data obtained from all PDSR implementing regions for four consecutive years (2018–2021) were utilized for the study. The source population of the study are all perinates who died and were reviewed by the MPDSR committee during the study period. Accordingly, a total of 3,814 reviewed perinatal deaths were included in the study. The PDSR data was hierarchical i.e., perinates were nested in 161 reporting health facilities and 45 provinces of the country.
The dependent variable of this study is the outcome of the fetus after birth, which is classified as “Stillbirth” and “live birth”.
Both individual and facility-level variables were included as a predictor in the model. Sex, gestational age, place of birth, mode of delivery, and assigned cause of death were included as neonatal factors in the model. The medical cause of death was incorporated as individual death after the underlying cause of death was assigned using the International Classification of Diseases -Perinatal Mortality (ICD-PM) (41). On the other hand, maternal factors variables such as maternal age, maternal parity, educational status, number of antenatal care (ANC) visits, the score of delay one, and maternal health condition were included in the model. Moreover, maternal health conditions were assigned per the guidance of ICD-PM. The score of delay one, which is a delay in deciding to seek care (42), was computed using the row sum of seven variables included under this domain; namely (1) family poverty, (2) bad experience with previous health care, (3) failure to recognize the danger signs of pregnancy, (4) lack of awareness on where to seek care, (5) lack of person to take care of other children, (6) reliant on traditional practice and (7) lack of decision to go to a health facility. All of them were binary variables with “Yes” and “No” responses; and after summation of the score, to keep the normality of the data a square root transformation was carried out (43). Finally, the transformed variable was treated as continuous variables to make a parsimonious model (44).
At a facility (community) level; variables such as residence, type of region, type of health facility, a score of delay two, and a score of delay three were taken into consideration. The type of region was classified into three categories (city, agrarian, and pastoralist) based on the cultural and socio-economic backgrounds of the population (45). Furthermore, the type of facility was codified into classes (primary, secondary, and tertiary facilities) according to their manpower, medical equipment, and service provision (46). Moreover, the score of delay two(a delay to reach the facility that provides emergency obstetric care (EmONC) and delay three(a delay that occurs in receiving care after arrival at the health facility) (42), were computed similarly to the score of delay one. The score of delay two was computed using four questions: namely (1) absence of transportation, (2) expensive cost of transportation, (3) no facility within a reasonable distance and (4) poor road condition. Similarly, the score of delay three was also computed using four questions; namely, (1) long travel time from health facility to health facility (due to multiple referrals to receive optimal care), (2) long waiting time before receiving treatment, (3) mistake during an assessment, diagnosis, and treatment and (4) shortage of equipment and supplies. Both delays (two and three) were measured using binary variables and the responses were set as “Yes” and “No” options.
Death of a fetus born after 28 completed weeks of gestation or neonatal deaths through the first 28 completed days after birth (11).
Stillbirth is a fetal death (i.e., death before the complete expulsion or extraction of a product of conception from its mother) in the third trimester (≥28 completed weeks of gestation) or with birth weight ≥1,000 g or crown to heel length ≥35 cm (22).
Perinatal deaths were categorized by the time of death; antepartum, intrapartum stillbirth, unknown and neonatal. Cause of death during the antepartum and intrapartum, was taken as the cause of stillbirth in the study. Furthermore, the contributing maternal conditions were classified into five major categories per the guidance of ICD_PM_10 (Table 1) (47).
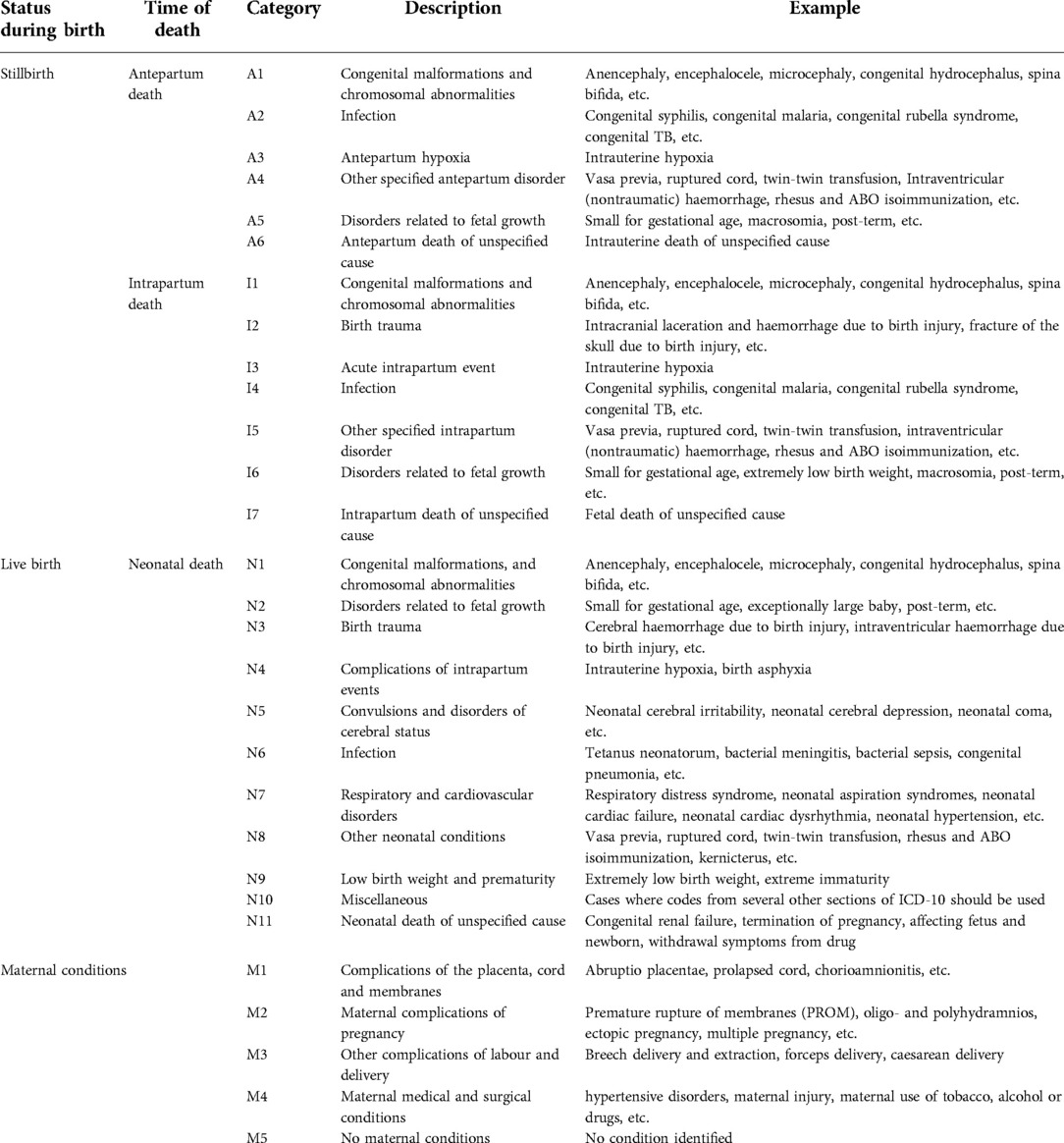
Table 1. ICD-PM categories with the specific cause of perinatal death and maternal health condition.
The data was exported from Epi -info version 7.2 to Stata version 17 for data cleaning and further analysis. Using the cleaned data descriptive [count, mean, percentage, and standard deviation(SD)] and analytical analysis (marginal model) was carried out and reported.
Both bi-variable and multivariable analyses were performed to determine the existing association with the outcome of interest. Initially, bivariate analysis was performed and variables with a p-value of 0.2 and below were retained in the model. Secondly, multicollinearity was assessed using variance inflation factor (VIF) before proceeding to multivariate analysis.
Generalized Estimating Equation (GEE) model is used to describe changes in the population while accounting for the within-cluster correlation of observations (48–50). The marginal models fitted in this study are GEE and Alternating Logistic Regression (ALR). Both marginal models were used to model the birth outcome and compare the odds of stillbirth outcome by considering the respective risk factors. Within the GEE and ALR model frameworks, health facilities were clustered, and not independent within each health facility. The response variables were the occurrence of stillbirth (Yi: binominal variable, i.e., stillbirth or live birth); and for this study, we considered that the event occurred if the perinate died before and during the onset of labour. Consequently, the response variable was coded with 1 for birth outcome with stillbirth and 0 for the alive birth outcome. The link function between the mean value and the model covariates considered for GEE, are defined by the ` working correlation structure stated below:
Where is logit link function, is -dimensional vector of known covariates, dimensional vector of unknown parameters, is the expected value of the response in the cluster i which is binomially distributed as . In addition, GEE is the non-likelihood method that captures the association within health facilities in terms of marginal correlation (50). With this GEE model, the correlation structure of the data within each health facility was assumed to be independent, unstructured, exchangeable, and first-order auto-regressive(51). Furthermore, Independence and exchangeable working assumptions can be used in virtually all applications, whether longitudinal, clustered, multivariate, or otherwise correlated. However, autoregressive AR (1) and unstructured correlation structures are less relevant for clustered data (50). In general, the parameter β is estimated by quasi-likelihood. However, when the cluster sizes become larger, the simultaneous estimation of marginal mean and dependence structure can become computationally prohibitive using GEE. As a result, alternating logistic regression measures the pairwise association of two observations in the same health facility and follows the precision estimates for the regression (β) and the association (α) parameters considered (50, 52). Furthermore, unlike GEE, no working assumptions about the thirdorder and fourth-order odds ratios are required. Alternating logistic regression measures the association using the odds ratio, which is interpretable and more applicable for binary data (50, 52). Let be the log odds ratio between outcomes and , let and , then the association of the two responses is defined as (53):
Similar to GEE, the parameter β is estimated by quasi-likelihood.
The descriptive statics (count, mean, percentage, and Standard deviation) were computed using the Stata version 17, while GEE and ALR models fit for this study were carried out with the SAS 9.4 version.
The final model was built based on the principle of generality, the goodness of fit, and parsimony. In this study, exchangeable and independence were the two working correlation assumptions of the GEE model. The best-fitted model was selected based on the minimum quasi-information criteria (QIC) and standard error, where the two criteria were used to select the working correlation structure (54). The backward selection strategy was adopted for the selection of the final variables related to stillbirth. With this method, we started a full model containing all main effects and interactions and continued the process until we get a parsimonious model. After obtaining the best-fitted model through GEE, we used the ALR model to decide the final variables fitted to the model. Furthermore, during ALR estimation, the logs odds ratio model was specified using SAS software's nesting function “NEST1”. Subsequently, we specified the function using “SUB_CLUST = Health facility” to define the subcluster(Health facilities) within the cluster(Provinces) (55). Lastly, the odds ratio of the final model was computed using the following formula (56).
A total of 3,814 perinatal deaths were included in the study, out of which 1,417(37.2%) were stillbirths. Among reporting health facilities, nearly half (49.6%) of the reported perinatal deaths from primary level health care providers were stillbirths. Region-wise, 56.5%,47.7%, and 44.4% of the reported perinatal deaths from Oromia, Amahara, and Benshangul Gumuz were stillbirths. Furthermore, 42.5% of the reported perinatal deaths in 2020 were stillbirths (Table 2).
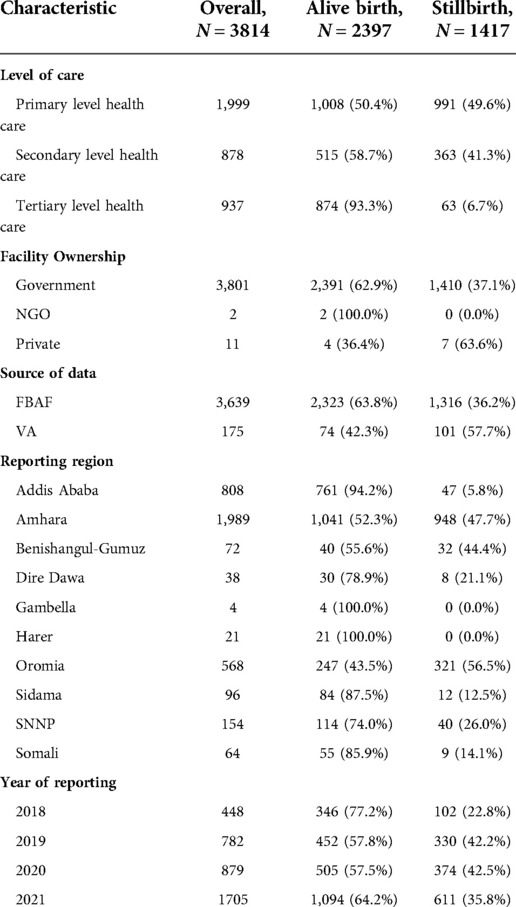
Table 2. Selected background characteristics of reporting facilities by outcome status of the perinate in Ethiopia,2021.
The average age of the mother with a stillbirth outcome was 27.4 with a standard deviation (SD) of 5.70 years. Similarly, the average maternal parity among mothers who encountered stillbirth outcomes was 2.6 with an SD of 1.88. The proportion of stillbirths was higher among women who are uneducated (46.8%) as compared to women who attended primary education (23.5%). Likewise, mothers with maternal complications of pregnancy had a higher proportion of stillbirth (66.6%) as compared to mothers who had no identified maternal complication (30.2%). Furthermore, mothers who live in rural areas had a higher proportion of stillbirths (46.7%) than mothers who lived in urban areas (25.6%) (Table 3).

Table 3. Selected background characteristics of the deceased perinate's mother by outcome status of the perinate in Ethiopia, 2021.
The average gestational week of stillbirth was 36.0 with an SD of 3.03. The proportion of stillbirth was higher among perinates who were delivered by spontaneous vaginal delivery (40.0%) as compared to perinates delivered by caesarean section (20.4%). Besides, perinates who were born in transit had a high proportion of stillbirths (71.8%) as compared to perinates who were born in a health facility (35.1%) (Table 4).
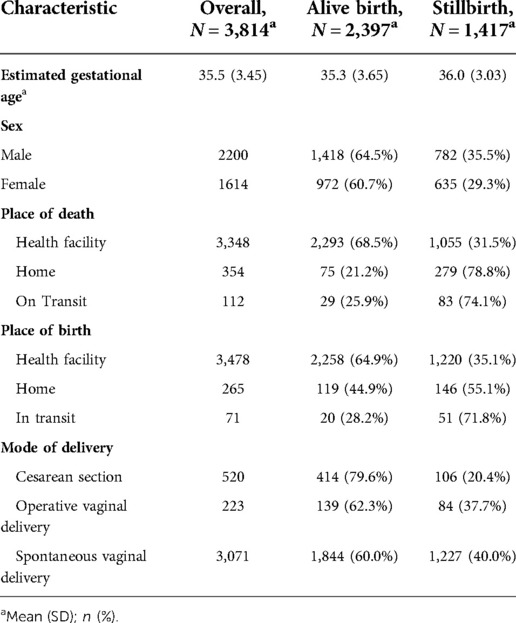
Table 4. Selected characteristics of the perinate by outcome status in Ethiopia, 2021.
The cross-cutting causes of death (birth trauma (44.4%), infection (56.3%), and congenital malformations, deformations, and chromosomal abnormalities (51.3%)) for both live and stillbirth had a relatively similar proportion of contribution to stillbirth (Table 5).
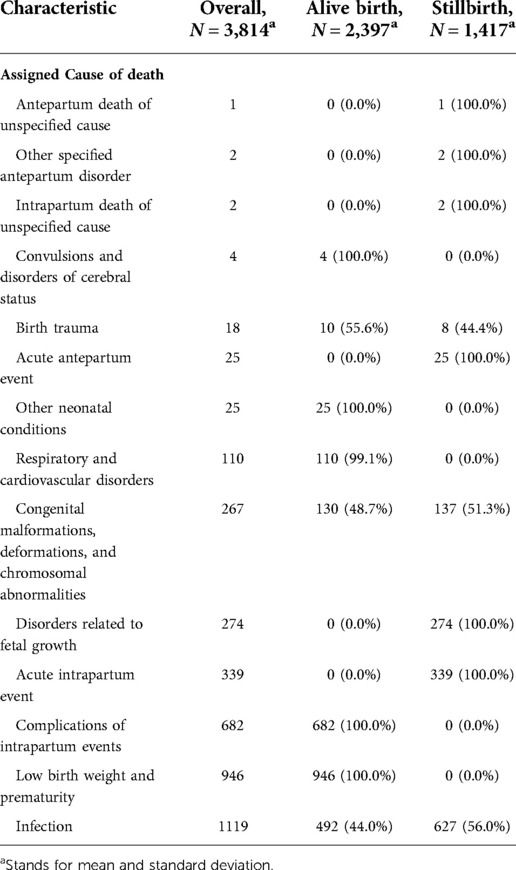
Table 5. Assigned cause of death by the outcome of the perinate in Ethiopia, 2021.
The proportion of stillbirth due to delay one was higher among perinates whose mothers were delayed in seeking care due to lack of decision to go to a health facility (54.2%) than those who were delayed in seeking care due to previous bad experiences in health facilities (18.2%). Similarly, the proportion of stillbirth because of delay two was higher among perinates whose mothers were delayed in reaching care due to expensive cost of transportation (62.3%) as compared to those who were delayed reaching care due to the absence of health facilities with reasonable distance (42.1%). Moreover, the proportion of stillbirths because of delay three was higher among perinate mothers who were not assessed and treated properly (63.9%) than those who travelled for a longer duration to get into the referred facility (33.3%) (Table 6).
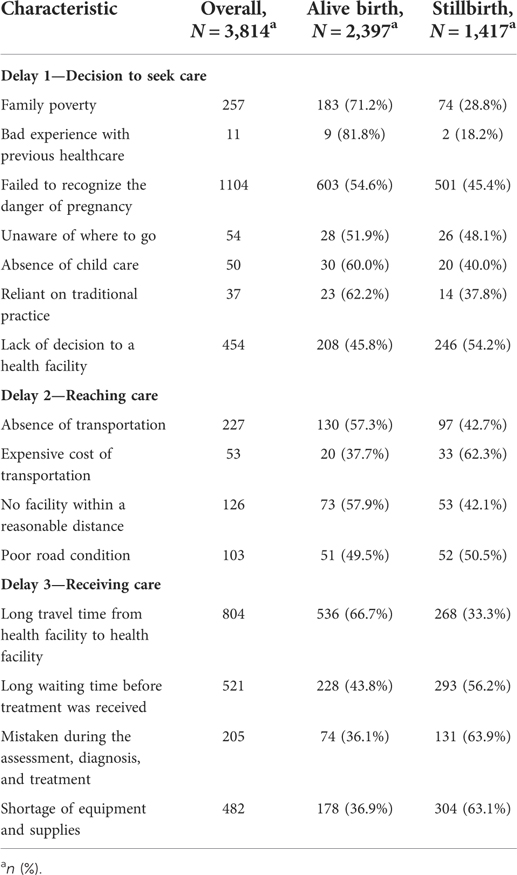
Table 6. Delay factors contribute to perinatal death by outcome status of the perinate in Ethiopia, 2021.
The marginal model was used to determine the factors that affect early neonatal death. In the analysis, both individual and facility-level factors were considered in the model.
The model with the smallest QIC and standard error was selected as the best-fitted model in the study. Accordingly, the ALR model was selected as the best-fitted model. Per the ALR model, place of birth, cause of death (infection and congenital and chromosomal abnormalities), maternal health condition, maternal education status, delay one, type of health facility, and delay three were predictors of stillbirth.
The analysis output under ALR model suggests that the place of birth had a significant association with stillbirth. It was revealed that perinate who were delivered in transit had exp(0.86) = 2.36 times higher odds of stillbirth outcome than those who were delivered at a health facility. Perinates who were delivered at home had exp(0.32) = 1.38 times higher odds of stillbirth outcome than those delivered at a health facility.
In addition, a statistically significant relationship between infection and stillbirth was demonstrated. The odds of giving a stillbirth were much higher among perinates with infection [exp(0.77) = 2.16] than perinates without infection. Similarly, perinates with congenital malformations, deformations, and chromosomal abnormalities had a higher risk of stillbirth [exp(1.07) = 2.92] as compared to perinate without congenital and chromosomal abnormalities.
With respect to the maternal health condition, it was indicated that a mother with placenta, cord, and membranes complications, and a mother with maternal complications of pregnancy, were significantly related to stillbirth. This indicates that the estimated odds of having a stillbirth in women who had placenta, cord, and membranes complications were exp.(0.26) = 1.30 times higher than a woman without any of those maternal complications. Similarly, the odds of having a stillbirth in women who had complications of pregnancy was exp.(0.78) = 2.18 times higher compared to women without any maternal complications.
Maternal education also has a role in the stillbirth outcome, as indicated in Table 2, women with a secondary and above level of education were associated with exp(−0.25) = 0.78 times fewer odds of having stillbirth compared to women with no education. Moreover, women with primary level education had exp(−0.43) = 0.65 times less risk of having stillbirth compared to their counterparts with no education. In line with this, as the score of delay-one increases by one unit, the odds of having a stillbirth increase exp(0.37) = 1.45 times.
As depicted in Table 3, the type of healthcare provider is significantly related to stillbirth. The estimated odds of having stillbirth among women who were treated in secondary health care was exp.(−0.91) = 0.40 times lower than the estimated odds for women who were treated in primary health care. Likewise, women who were treated in tertiary health care had exp(−1.82) = 0.16 times less risk of having stillbirth compared to their counterparts treated in primary health care providers. Furthermore, as a score of delay three increases by one unit, the odds of having a stillbirth increased by exp(0.80) = 2.23 times (Table 7).
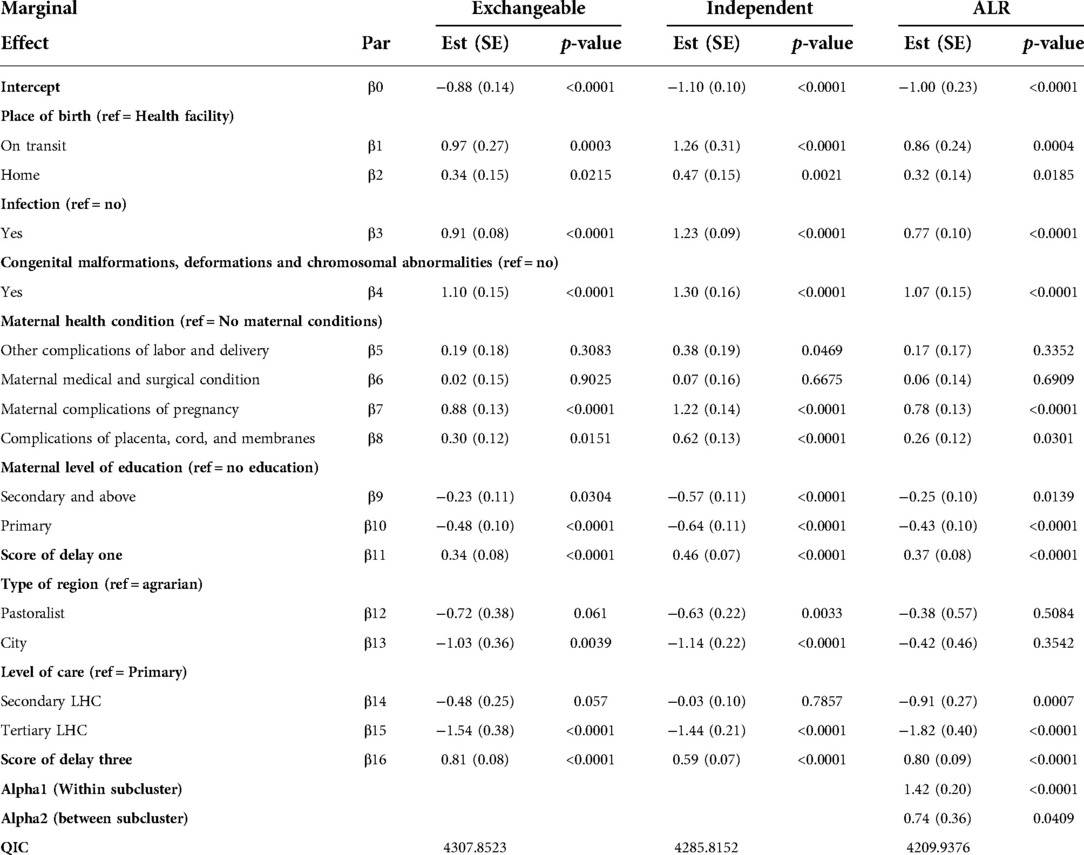
Table 7. Parameter estimates and empirical standard errors of GEE and ALR models for stillbirth.
This study utilized national PDSR data to identify the risk factors associated with stillbirth among reviewed perinatal deaths. The ALR analysis revealed that covariates like place of birth, cause of death (infection, congenital and chromosomal abnormalities), maternal health condition, maternal education status, delay one, type of health facility, and delay three were significantly associated with stillbirth.
The statistical analysis output revealed that place of birth is one of the important factors associated with stillbirth. The risk of having stillbirth was higher among perinates delivered in transit and at home as compared to those delivered at a health facility. This finding corresponds well with studies conducted in Bangladesh (57), and other five countries (India, Guatemala, Kenya, Pakistan, and Zambia) (58). This could be due to the fact that institutional delivery paves the way to early identification and management of intrapartum complications including the provision of cesarian section service, which has a significant role in the reduction of intrapartum stillbirth (59). In Ethiopia, only 48% and 43% of the women give birth at a health facility and had more than 4 ANC visits, respectively (39). However, ANC visits, levels of education, residence, and previous history of home delivery were major factors that influence institutional deliveries (60, 61). In general, the finding indicates that improving the coverage of institutional delivery is needed to reduce the high burden of stillbirth in the country.
The study also revealed that stillbirth due to infection was much higher compared to other causes. The finding was coherent with studies conducted in Ethiopia (Bahardar, Tigray, and Harir) (62–64), Afghanistan (65), Bangladesh (66), and Italy (67). The potential reasons that could explain those differences are (1) the presence of maternal infection which might lead to systemic illness in the mother, causing fetal death due to high maternal fever, respiratory distress, or other systemic reactions, without an infection being transmitted to the placenta or fetus (while the fetus is intact). (2) the second possible reason could be related to the infection of the placenta which results in reduced fetoplacental blood flow. Syphilis, malaria, and chorioamnionitis are the commonest causes of infection-related stillbirth in underdeveloped nations (68, 69). Considering this, putting in place effective measures such as improving the screening and treatment of syphilis and malaria should be coupled with interventions focused on preterm and term PROM to reduce the burden of stillbirth (70).
The study has also revealed that congenital malformations, deformations, and chromosomal abnormalities were associated with stillbirth outcomes, i.e., there is a threefold higher risk of stillbirth among perinate with congenital abnormalities than their counterparts. This finding was consistent with studies conducted in Ethiopia (71), Cameroon (28), and India (26). This could be due to a lack of maturity of the vital organs for fetal survival making the fetus prone to fatal complications and death. Neural tube defects, orofacial clefts, masculo-skeletal systemdefects, syndrome disorders, and cardiovascular system problems were prevalent congenital anomalies in Ethiopia (72).ANC visits and residence are known to have a significant role in the formation of congenital and chromosomal anomalies in Ethiopia (73). However, the lack of effective national surveillance, which can monitor and guide the prevention initiative, has untrimmed the efforts to the reduction of stillbirths due to congenital abnormalities in Ethiopia.
Women with maternal complications of pregnancy and complications of the placenta, cord, and membranes had a higher risk of having stillbirth as compared to women with no identified complication. The finding was complementary to studies conducted in Ethiopia (74), Iran (75), India (76), and Pakistan (77). This might be explained by the deteriorated maternal condition resulting in vessel compression and cessation of blood flow, as well as fetal perfusion. lastly, the combination of all these effects could lead to fetal asphyxia and death (78, 79). In line with this, history of ANC visits, urinary tract infection, being anemic, previous history of cesarean section, gestational hypertension, and diabetes were known modifiable risk factors for both maternal health conditions (i.e., Maternal complication of pregnancy and complications of the placenta, cord, and membranes) (30, 80, 81). Thus, the reduction of preventable stillbirths from the above two maternal health conditions can be achieved by controlling the predisposing factors.
Maternal education is the other variable that Is strongly associated with stillbirth outcomes. Educated women had a lower risk of having stillbirth as compared to uneducated women. In addition, the study revealed that the score of delay one had a positive dose-response relationship with stillbirth. This finding was congruent with studies conducted in Ethiopia (62), Nigeria (82), Nepal (35), Japan (83), and other six countries(Argentina, the Democratic Republic of the Congo, Guatemala, India, Pakistan, and Zambia) (84). This could be due to the assumption that educated women would have better knowledge, which enables them to make an early decision regarding their health. Considering the benefit of education, Ethiopia has launched a health extension program, which is designed to provide health education and basic health service at the community level (85). On top of this, Community Based Newborn Care (CBNC) and Integrated Community Case Management (iCCM) were included to foster the program (86). However, its implementation has been challenged due to health system (lack of regular monitoring, lack of logistics, and absence of continuous professional development activities) and community level (limited engagement of the community structure) challenges (87, 88). Overall, the finding indicated that health extension programs should be revitalized and coupled with other programs that could enhance the health-seeking behavior of women.
The type of health facility and the score of delay three were the other variables that are associated with stillbirth outcomes. Women who were treated in secondary and tertiary health care had a lower risk of having stillbirths as compared to women who were treated in primary health care. Besides, a positive dose-response relation was observed between a score of delay three and stillbirth outcomes. The finding was parallel with studies conducted in Nigeria (89), Jordan (90), Brazil (91), and Sweden (92). This might be explained by the level of health service providers' capacity of identifying and managing obstetrics emergencies. As the diagnostic capacity of the health facility increases, the risk of having an adverse outcome in fetal and maternal health will be reduced. Furthermore, the finding was concurrent with the evidence generated by the Ethiopian Service and Availability Readiness Assessment (SARA) report, where secondary and tertiary health facilities were proven to have better service availability and readiness in the provision of Emergency Newborn care (EmNeC) services (93). In addition to this, the country has invested a lot of resources in the establishment and expansion of neonatal intensive care units (NICUs) at secondary and tertiary levels of care to improve neonatal outcomes (94). Considering all this, the finding implies the presence of gaps in managing obstetrics emergencies at the lower level, in addition to poor referral linkage among health facilities.
The study has the following limitation that needs to be acknowledged. (1) All identified, confirmed, and reported perinatal death through a weekly reporting system were not reviewed and sent through the Perinatal Death Reporting Format (PDRF) to the next level, which might introduce potential bias to the study. (2) nearly all deaths were reported and reviewed from public facilities with limited involvement of private health facilities, and this could affect the representativeness of the study. (3) Lack of national guidelines and capacity for investigation of perinatal death, placental examination, genetic evaluation, and radiologic evaluation influenced the study in obtaining more in-depth data.
Almost four in ten perinatal deaths were stillbirths. Place of delivery, cause of death, maternal health condition, maternal education status, delay one, type of health care, and delay three were predictors of stillbirth. Tailored intervention should be provided to the two major causes of stillbirth (infection and congenital malformations, deformations, and chromosomal abnormalities) by improving prenatal care and ANC visit. Moreover, intervention should focus on encouraging institutional delivery by improving the health-seeking behaviour of the community. One potential solution to this could be the revitalization of the existing health extension program. Furthermore, improving the managing capacity of obstetrics emergencies at a lower level should be enhanced in terms of manpower and equipment.
The raw data supporting the conclusions of this article will be made available by the authors per the guidance of the data sharing policy of the institutes.
We used secondary data obtained from EPHI with no personal identifier information of the participants. The EPHI Review Board and Public Health Emergency Management Unit approved the research proposal with Ref. No. EPHI 6_5/437. Since the study used secondary data other ethical measures were not required.
NT planned the study, FL and MK coordinated the study, NT, MK and FW cleaned and analyze data, NT analyzed the literature, NT and FW was major contributor in writing the manuscript study. All authors contributed to the article and approved the submitted version.
The authors would like to acknowledge EPHI, particularly the Center of Public Health Emergency unit for their facilitation and support during the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization,. World health statistics 2016: Monitoring health for the SDGs sustainable development goals. Geneva (Switzerland): World Health Organization (2016). https://apps.who.int/iris/handle/10665/206498
2. Campbell HE, Kurinczuk JJ, Heazell AE, Leal J, Rivero-Arias O. Healthcare and wider societal implications of stillbirth: a population-based cost-of-illness study. BJOG. (2018) 125(2):108–17. doi: 10.1111/1471-0528.14972
4. Hug L, You D, Blencowe H, Mishra A, Wang Z, Fix MJ, et al. Global, regional, and national estimates and trends in stillbirths from 2000 to 2019: a systematic assessment. The Lancet. (2021) 398(10302):772–85. doi: 10.1016/S0140-6736(21)01112-0
5. World Health Organization. Strategies towards ending preventable maternal mortality (EPMM). Geneva (Switzerland): World Health Organization (2015).
6. World Health Organization,. Stillbirth prevention. (2022) [Cited 2022 June 1]. Available at: https://tinyurl.com/yasvan6u
7. Ethiopian Minster of health,, Reproductive Health Strategies Plan 2021–2025. (2022) [Cited 2022 June 1]. Available at: https://tinyurl.com/yrpsbmcu
8. Tesema GA, Gezie LD, Nigatu SG. Trends of stillbirth among reproductive-age women in Ethiopia based on Ethiopian demographic and health surveys: a multivariate decomposition analysis. BMC Pregnancy Childbirth. (2020) 20(1):1–1. doi: 10.1186/s12884-020-02880-5
9. Berhie KA, Gebresilassie HG. Logistic regression analysis on the determinants of stillbirth in Ethiopia. Matern Health Neonatol Perinatol. (2016) 2(1):1–0. doi: 10.1186/s40748-016-0038-5
10. World Health Organization. Making every baby count: audit and review of stillbirths and neonatal deaths. Geneva (Switzerland): World Health Organization (2016).
11. Ethiopian public health institutes,. Maternal and perinatal death surveillance and response technical guideline. Addis Ababa (Ethiopia): EPHI (2022). In [internet]. [cited 18 may 2022]. Available at: https://tinyurl.com/2p8f6rwz
12. Tesfay N, Tariku R, Zenebe A, Dejene Z, Woldeyohannes F. Cause and risk factors of early neonatal death in Ethiopia. Plos One. (2022) 17(9):e0275475. doi: 10.1371/journal.pone.0275475
13. Melberg A, Teklemariam L, Moland KM, Aasen HS, Sisay MM. Juridification of maternal deaths in Ethiopia: a study of the maternal and perinatal death surveillance and response (MPDSR) system. Health Policy Plan. (2020) 35(8):900–5. doi: 10.1093/heapol/czaa043
14. Ayele B, Gebretnsae H, Hadgu T, Negash D, G/silassie F, Alemu T, et al. Maternal and perinatal death surveillance and response in Ethiopia: achievements, challenges and prospects. PloS one. (2019) 14(10):e0223540. doi: 10.1371/journal.pone.0223540
15. Nutritional international,. Cost-effectiveness of transitioning from iron and folic acid to multiple micronutrient supplementation for pregnancy. Addis Ababa (Ethiopia) (2022). [Cited 2022 June 1]. Available at: https://tinyurl.com/v7z7j8w6
16. Kare AP, Gujo AB, Yote NY. Quality of antenatal care and associated factors among pregnant women attending government hospitals in sidama region, southern Ethiopia. SAGE Open Med. (2021) 9:20503121211058055. doi: 10.1177/20503121211058055
17. Kassie BA, Yenus H, Berhe R, Kassahun EA. Prevalence of sexually transmitted infections and associated factors among the university of gondar students, northwest Ethiopia: a cross-sectional study. Reprod Health. (2019) 16(1):1–8. doi: 10.1186/s12978-019-0815-5
18. Ajemu KF, Desta A. Level of quality of option B+ PMTCT service provision in public health facilities in mekelle zone, northern Ethiopia: cross-sectional study. BMC Health Serv Res. (2020) 20(1):1–0. doi: 10.1186/s12913-020-05429-6
19. Yitayew AE, Enyew HD, Goshu YA. Utilization and associated factors of insecticide treated bed net among pregnant women attending antenatal clinic of addis zemen hospital, north-western Ethiopia: an institutional based study. Malar Res Treat. (2018) 2018:Article ID 3647184, 9 pages. doi: 10.1155/2018/3647184
20. Bayou YT, Mashalla YJ, Thupayagale-Tshweneagae G. Patterns of caesarean-section delivery in Addis Ababa, Ethiopia. Afr J Prim Health Care Fam Med. (2016) 8(2):1–6. doi: 10.4102/phcfm.v8i2.953
21. Ethiopian Ministry of Health,. National reproductive health strategy from 2016_2020. (2022). Addis Ababa (Ethiopia): FMOH [Cited 2022 June 1]. Available at: https://tinyurl.com/mryvcs6w
22. Ethiopian ministry of health,. Health sector transformation plan II. (2022). Addis Ababa (Ethiopia): FMOH [Cited 2022 June 1]. Available at: https://tinyurl.com/y3xz25y2
23. Tesema GA, Gezie LD, Nigatu SG. Spatial distribution of stillbirth and associated factors in Ethiopia: a spatial and multilevel analysis. BMJ open. (2020) 10(10):e034562. doi: 10.1136/bmjopen-2019-034562
24. Bhutta ZA, Das JK, Bahl R, Lawn JE, Salam RA, Paul VK, et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet. (2014) 384(9940):347–70. doi: 10.1016/S0140-6736(14)60792-3
25. Bhutta ZA, Darmstadt GL, Haws RA, Yakoob MY, Lawn JE. Delivering interventions to reduce the global burden of stillbirths: improving service supply and community demand. BMC Pregnancy Childbirth. (2009) 9(1):1–37. doi: 10.1186/1471-2393-9-1
26. Mali RV, Dalal A, Khursheed R, Gan A. Association of stillbirths with maternal and fetal risk factors in a tertiary care hospital in south India. Obstet Gynecol Int. (2021) 2021:Article ID 8033248, 8 pages. doi: 10.1155/2021/8033248
27. Hirst JE, Villar J, Victora CG, Papageorghiou AT, Finkton D, Barros FC, et al. The antepartum stillbirth syndrome: risk factors and pregnancy conditions identified from the INTERGROWTH-21st project. BJOG. (2018) 125(9):1145–53. doi: 10.1111/1471-0528.14463
28. Tolefac PN, Tamambang RF, Yeika E, Mbwagbaw LT, Egbe TO. Ten years analysis of stillbirth in a tertiary hospital in sub-Sahara Africa: a case control study. BMC Res Notes. (2017) 10(1):1–6. doi: 10.1186/s13104-016-2345-3
29. Yatich NJ, Funkhouser E, Ehiri JE, Agbenyega T, Stiles JK, Rayner JC, et al. Malaria, intestinal helminths and other risk factors for stillbirth in Ghana. Infect Dis Obstet Gynecol. (2010) 2010:Article ID 350763, 7 pages. doi: 10.1155/2010/350763
30. Berhan Y. Predictors of perinatal mortality associated with placenta previa and placental abruption: an experience from a low-income country. J Pregnancy. (2014) 2014:Article ID 307043, 10 pages. doi: 10.1155/2014/307043
31. Ibrahimou B, Anozie C, de la Cruz C, Salihu H. Previous preterm birth and current maternal complications as a risk factor of subsequent stillbirth. Adv Epidemiol. (2015) 2015:Article ID 819146, 6 pages. doi: 10.1155/2015/819146
32. Sun Q, Zhang H, Zhang Y, Peng Z, Lu J, Ma X. Increased risk of stillbirth among women whose partner has Tuberculosis. BioMed Res Int. (2021) 2021:Article ID 1837881, 8 pages. doi: 10.1155/2021/1837881
33. Duan CC, Zhang XH, Li SS, Wu W, Qiu LQ, Xu J. Risk factors for stillbirth among pregnant women infected with syphilis in the zhejiang province of China, 2010–2016. Can J Infect Dis Med Microbiol. (2021) 2021:Article ID 8877962, 6 pages. doi: 10.1155/2021/8877962
34. Mulatu T, Debella A, Feto T, Dessie Y. Determinants of stillbirth among women who gave birth at hiwot fana specialized university hospital, eastern Ethiopia: a facility-based cross-sectional study. SAGE Open Med. (2022) 10:20503121221076370. doi: 10.1177/20503121221076370
35. Kc A, Nelin V, Wrammert J, Ewald U, Vitrakoti R, Baral GN, et al. Risk factors for antepartum stillbirth: a case-control study in Nepal. BMC Pregnancy Childbirth. (2015) 15(1):1–0. doi: 10.1186/s12884-015-0429-z
36. Awoleke JO, Adanikin AI. Baird-pattinson aetiological classification and phases of delay contributing to stillbirths in a Nigerian tertiary hospital. J Pregnancy. (2016) 2016:Article ID 1703809, 5 pages. doi: 10.1155/2016/1703809
37. United Nations,. World population prospect. In:[Internet]. population division; (2022) [cited 1 June 2022]. Available at: https://population.un.org/wpp/
38. Ageze L. Health facility governance in the Ethiopian health system. Bethesda Health Syst. (2012) 20:20.
39. Ethiopian Public Health Institute (EPHI) [Ethiopia] and ICF,. Ethiopia Mini demographic and health survey 2019: final report. Rockville, Maryland, USA: EPHI and ICF (2021).
40. Central Statistical Agency/CSA/Ethiopia and ICF,. Ethiopia Demographic and health survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF (2016).
41. World Health Organization. The WHO application of ICD-10 to deaths during the perinatal period: ICD-PM.
42. Tesfay N, Tariku R, Zenebe A, Mohammed F, Woldeyohannes F. Area of focus to handle delays related to maternal death in Ethiopia. PLoS One. (2022) 17(9):e0274909. doi: 10.1371/journal.pone.0274909
43. Jebena MG, Lindstrom D, Belachew T, Hadley C, Lachat C, Verstraeten R, et al. Food insecurity and common mental disorders among Ethiopian youth: structural equation modeling. PLoS One. (2016) 11(11):e0165931. doi: 10.1371/journal.pone.0165931
44. Uchechi OC. Assessing the impact of square root transformation on weibull-distributed error component of a multiplicative error model. Sci J Appl Math Stat. (2021) 9(4):94. doi: 10.11648/j.sjams.20210904.11
45. Shifti DM, Chojenta C, Holliday EG, Loxton D. Individual and community level determinants of short birth interval in Ethiopia: a multilevel analysis. PloS One. (2020) 15(1):e0227798. doi: 10.1371/journal.pone.0227798
46. Federal Ministery of Health of Ethiopia,. Health and Health Related Indicators 2016/2017. (2017) [cited 2022 Mar 1]; Available at: https://tinyurl.com/4mcu5hdb
47. Aminu M, Mathai M, van den Broek N. Application of the ICD-PM classification system to stillbirth in four sub-saharan african countries. PLoS One. (2019) 14(5):e0215864. doi: 10.1371/journal.pone.0215864
48. Hubbard AE, Ahern J, Fleischer NL, Van der Laan M, Satariano SA, Jewell N, et al. To GEE or not to GEE: comparing population average and mixed models for estimating the associations between neighborhood risk factors and health. Epidemiology. (2010) 21:467–74. doi: 10.1097/EDE.0b013e3181caeb90
49. Fitzmaurice G, Davidian M, Verbeke G, Molenberghs G, editors. Longitudinal data analysis. London (England): CRC press (2008). p. 123–40.
50. Molenberghs G, Verbeke G. Models for discrete longitudinal data. Leuven (Belgium): Library of Congress (2005).
51. Bena J, McIntyre S. Survival methods for correlated time-to-event data. MWSUG 2008 Conference (2008). p. 12–4
52. Carey V, Zeger SL, Diggle P. Modelling multivariate binary data with alternating logistic regressions. Biometrika. (1993) 80(3):517–26. doi: 10.1093/biomet/80.3.517
53. Liang KY, Zeger SL. Regression analysis for correlated data. Annu Rev Public Health. (1993) 14(1):43–68. doi: 10.1146/annurev.pu.14.050193.000355
54. Cui J. QIC Program and model selection in GEE analyses. Stata J. (2007) 7(2):209–20. doi: 10.1177/1536867X0700700205
56. Szumilas M. Explaining odds ratios. J Can Acad Child Adolesc Psychiatry. (2010) 19(3):227. PMID: 20842279
57. Khanam R, Baqui AH, Syed MI, Harrison M, Begum N, Quaiyum A, et al. Can facility delivery reduce the risk of intrapartum complications-related perinatal mortality? Findings from a cohort study. J Glob Health. (2018) 8(1):010408. doi: 10.7189/jogh.08.010408
58. Goudar SS, Goco N, Somannavar MS, Kavi A, Vernekar SS, Tshefu A, et al. Institutional deliveries and stillbirth and neonatal mortality in the global Network's maternal and newborn health registry. Reprod Health. (2020) 17(3):1–9. doi: 10.1186/s12978-020-01001-x
59. Vogel JP, Souza JP, Mori R, Morisaki N, Lumbiganon P, Laopaiboon M, et al. Maternal complications and perinatal mortality: findings of the world health organization multicountry survey on maternal and newborn health. BJOG. (2014) 121:76–88. doi: 10.1111/1471-0528.12633
60. Berelie Y, Yeshiwas D, Yismaw L, Alene M. Determinants of institutional delivery service utilization in Ethiopia: a population based cross sectional study. BMC Public Health. (2020) 20(1):1–0. doi: 10.1186/s12889-020-09125-2
61. Gebregziabher NK, Zeray AY, Abtew YT, Kinfe TD, Abrha DT. Factors determining choice of place of delivery: analytical cross-sectional study of mothers in akordet town, Eritrea. BMC Public Health. (2019) 19(1):1–1. doi: 10.1186/s12889-019-7253-8
62. Worede DT, Dagnew GW. Determinants of stillbirth in felege-hiwot comprehensive specialized referral hospital, north-west, Ethiopia, 2019. BMC Res Notes. (2019) 12(1):1–6. doi: 10.1186/s13104-019-4621-5
63. Tasew H, Zemicheal M, Teklay G, Mariye T. Risk factors of stillbirth among mothers delivered in public hospitals of central zone, tigray, Ethiopia. Afr Health Sci. (2019) 19(2):1930–7. doi: 10.4314/ahs.v19i2.16
64. Yadeta TA, Worku A, Egata G, Seyoum B, Marami D, Berhane Y. Maternal group B Streptococcus recto vaginal colonization increases the odds of stillbirth: evidence from eastern Ethiopia. BMC Pregnancy Childbirth. (2018) 18(1):1–7. doi: 10.1186/s12884-018-2044-2
65. Christou A, Dibley MJ, Rasooly MH, Mubasher A, Hofiani SM, Rashidi MK, et al.Understanding country-specific determinants of stillbirth using household surveys: the case of Afghanistan. Paediatr Perinat Epidemiol. (2019) 33(1):28–44. doi: 10.1111/ppe.12530
66. Halim A, Aminu M, Dewez JE, Biswas A, Rahman AF, van den Broek N. Stillbirth surveillance and review in rural districts in Bangladesh. BMC Pregnancy Childbirth. (2018) 18(1):1–8. doi: 10.1186/s12884-018-1866-2
67. Monari F, Zanni F, Grandi G, Lupi C, Facchinetti F. A regional audit system for stillbirth: a way to better understand the phenomenon. BMC Pregnancy Childbirth. (2019) 19(1):1–9. doi: 10.1186/s12884-018-2145-y
68. Di Mario S, Say L, Lincetto O. Risk factors for stillbirth in developing countries: a systematic review of the literature. Sex Transm Dis. (2007) 24:S11–21. doi: 10.1097/01.olq.0000258130.07476.e3
69. Aleem S, Bhutta ZA. Infection-related stillbirth: an update on current knowledge and strategies for prevention. Expert Rev Anti-Infect Ther. (2021) 19(9):1117–24. doi: 10.1080/14787210.2021.1882849
70. Shukla VV, Carlo WA. Review of the evidence for interventions to reduce perinatal mortality in low-and middle-income countries. Int J Pediatr Adolesc Med. (2020) 7(1):4–10. doi: 10.1016/j.ijpam.2020.02.004
71. Gizaw W, Feyisa M, Hailu D, Nigussie T. Determinants of stillbirth in hospitals of north shoa zone, oromia region, central Ethiopia: a case control study. Heliyon. (2021) 7(5):e07070. doi: 10.1016/j.heliyon.2021.e07070
72. Taye M, Afework M, Fantaye W, Diro E, Worku A. Congenital anomalies prevalence in Addis Ababa and the amhara region, Ethiopia: a descriptive cross-sectional study. BMC Pediatr. (2019) 19(1):1–1. doi: 10.1186/s12887-019-1596-2
73. Mekonnen D, Worku W. Congenital anomalies among newborn babies in felege-hiwot comprehensive specialized referral hospital, bahir dar, Ethiopia. Sci Rep. (2021) 11(1):1–8. doi: 10.1038/s41598-020-79139-8
74. Mengistu S, Debella A, Mulatu T, Mesfin F, Danusa KT, Dheresa M. Stillbirth and associated factors among women who gave birth at hiwot fana specialized university hospital, harar, eastern Ethiopia. Front Pediatr. (2022):10:820308. doi: 10.3389/fped.2022.82030
75. Maleki Z, Ghaem H, Seif M, Foruhari S. Incidence and maternal-fetal risk factors of stillbirth: A population-based historical cohort and a nested case-control study.
76. Altijani N, Carson C, Choudhury SS, Rani A, Sarma UC, Knight M, et al. Stillbirth among women in nine states in India: rate and risk factors in study of 886,505 women from the annual health survey. BMJ Open. (2018) 8(11):e022583. doi: 10.1136/bmjopen-2018-022583
77. Nkwabong E, Tiomela Goula G. Placenta abruption surface and perinatal outcome. J Matern Fetal Neonatal Med. (2017) 30(12):1456–9. doi: 10.1080/14767058.2016.1219988
78. Liu LC, Wang YC, Yu MH, Su HY. Major risk factors for stillbirth in different trimesters of pregnancy—a systematic review. Taiwan J Obstet Gynecol. (2014) 53(2):141–5. doi: 10.1016/j.tjog.2014.04.003
79. Wright RG, Macindoe C, Green P. Placental abnormalities associated with childbirth. Acad Forensic Pathol. (2019) 9(1–2):2–14. doi: 10.1177/1925362119851113
80. Tiruye G, Shiferaw K, Tura AK, Debella A, Musa A. Prevalence of premature rupture of membrane and its associated factors among pregnant women in Ethiopia: a systematic review and meta-analysis. SAGE Open Med. (2021) 9:20503121211053912. doi: 10.1177/20503121211053912
81. Abdel Maaboud RM, Nossair WS, Ali AE, Ibrahem SA. Incidence rate, risk factors and outcome of premature rupture of membranes (PROM) at zagazig university hospitals. Egypt J Hosp Med. (2021) 85(1):2744–50. doi: 10.21608/ejhm.2021.189845
82. Anyichie NE, Nwagu EN. Prevalence and maternal socio-demographic factors associated with stillbirth in health facilities in Anambra, south-east Nigeria. Afr Health Sci. (2019) 19(4):3055–62. doi: 10.4314/ahs.v19i4.27
83. Koshida S, Ono T, Tsuji S, Murakami T, Arima H, Takahashi K. Excessively delayed maternal reaction after their perception of decreased fetal movements in stillbirths: population-based study in Japan. Women Birth. (2017) 30(6):468–71. doi: 10.1016/j.wombi.2017.04.005
84. McClure EM, Pasha O, Goudar SS, Chomba EL, Garces AN, Tshefu AN, et al. Epidemiology of stillbirth in low-middle income countries: a global network study. Acta Obstet Gynecol Scand. (2011) 90(12):1379–85. doi: 10.1111/j.1600-0412.2011.01275.x
85. Assebe LF, Belete WN, Alemayehu S, Asfaw E, Godana KT, Alemayehu YK, et al. Economic evaluation of health extension program packages in Ethiopia. PLoS One. (2021) 16(2):e0246207. doi: 10.1371/journal.pone.0246207
86. Mengistu B, Paulos M, Agonafir N, Ameha A, Legesse H, Dankenbring E, et al. Barriers to the uptake of community-based curative child health services in Ethiopia. BMC Public Health. (2021) 21(1):1–2. doi: 10.1186/s12889-020-10013-y
87. Zebre G, Gizaw AT, Tareke KG, Lemu YK. Implementation, experience, and challenges of urban health extension program in Addis Ababa: a case study from Ethiopia. BMC Public Health. (2021) 21(1):1–2. doi: 10.1186/s12889-021-10221-0
88. Assefa Y, Gelaw YA, Hill PS, Taye BW, Van Damme W. Community health extension program of Ethiopia, 2003–2018: successes and challenges toward universal coverage for primary healthcare services. Global Health. (2019) 15(1):1–1. doi: 10.1186/s12992-019-0470-1
89. Wariri O, Onuwabuchi E, Alhassan JA, Dase E, Jalo I, Laima CH, et al. The influence of travel time to health facilities on stillbirths: a geospatial case-control analysis of facility-based data in gombe, Nigeria. Plos one. (2021) 16(1):e0245297. doi: 10.1371/journal.pone.0245297
90. Alyahya MS, Khader YS, Al-Sheyab NA, Shattnawi KK, Altal OF, Batieha A. Modifiable factors and delays associated with neonatal deaths and stillbirths in Jordan: findings from facility-based neonatal death and stillbirth audits. Am J Perinatol. (2021) 15(1):1605–718. doi: 10.1055/s-0041-1730434
91. Martins MC, Feitosa FE, Viana Júnior AB, Correia LL, Ibiapina FL, Pacagnella RD, et al. Pregnancies with an outcome of fetal death present higher risk of delays in obstetric care: a case-control study. PLoS One. (2019) 14(4):e0216037. doi: 10.1371/journal.pone.0216037
92. Sterpu I, Bolk J, Perers Öberg S, Hulthén Varli I, Wiberg Itzel E. Could a multidisciplinary regional audit identify avoidable factors and delays that contribute to stillbirths? A retrospective cohort study. BMC Pregnancy Childbirth. (2020) 20(1):1–2. doi: 10.1186/s12884-020-03402-z
93. Ethiopian Public Health Institutes,. Ethiopia Service Availability and Readiness Assessment (SARA) 2018 Final Report. (2022) [Cited 2022 June 1]. Available at: https://tinyurl.com/mujjvrvy
94. Ethiopian Ministry of Health,. Annual Performance Report 2013EFY(2020/2021). (2022) [Cited 2022 June 1]. Available at: https://tinyurl.com/28d4u55h
Keywords: stillbirth, perinatal death surveillance, delay three, congenital anomalies, Ethiopia
Citation: Tesfay N, Legesse F, Kebede M and Woldeyohannes F (2022) Determinants of stillbirth among reviewed perinatal deaths in Ethiopia. Front. Pediatr. 10:1030981. doi: 10.3389/fped.2022.1030981
Received: 29 August 2022; Accepted: 7 November 2022;
Published: 28 November 2022.
Edited by:
Nihaya A. Al-sheyab, Jordan University of Science and Technology, JordanReviewed by:
Drucilla Jane Roberts, Harvard Medical School, United States© 2022 Tesfay, Legesse, Kebede and Woldeyohannes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Neamin Tesfay bmVhbWludGVzZmF5ZTIxMjNAZ21haWwuY29t
Specialty Section: This article was submitted to Neonatology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.