 Alicia M. Kamsheh
Alicia M. Kamsheh Matthew J. O’Connor
Matthew J. O’Connor Joseph W. Rossano
Joseph W. Rossano
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr., 08 November 2022
Sec. Pediatric Cardiology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.1020984
This article is part of the Research TopicManagement of the Hypoplastic Left Heart Syndrome: From Fetus to AdultView all 8 articles
With improvement in survival after Fontan surgery resulting in an increasing number of older survivors, there are more patients with a Fontan circulation experiencing circulatory failure each year. Fontan circulatory failure may have a number of underlying etiologies. Once Fontan failure manifests, prognosis is poor, with patient freedom from death or transplant at 10 years of only about 40%. Medical treatments used include traditional heart failure medications such as renin-angiotensin-aldosterone system blockers and beta-blockers, diuretics for symptomatic management, antiarrhythmics for rhythm control, and phosphodiesterase-5 inhibitors to decrease PVR and improve preload. These oral medical therapies are typically not very effective and have little data demonstrating benefit; if there are no surgical or catheter-based interventions to improve the Fontan circulation, patients with severe symptoms often require inotropic medications or mechanical circulatory support. Mechanical circulatory support benefits patients with ventricular dysfunction but may not be as useful in patients with other forms of Fontan failure. Transplant remains the definitive treatment for circulatory failure after Fontan, but patients with a Fontan circulation face many challenges both before and after transplant. There remains significant room and urgent need for improvement in the management and outcomes of patients with circulatory failure after Fontan surgery.
The Fontan circulation is a palliative circulation for single ventricle congenital heart disease (CHD) characterized by the lack of a subpulmonary ventricular pump with passive pulmonary blood flow driven by elevated central venous pressures. Since Francis Fontan first reported the successful treatment of two patients with tricuspid atresia in 1971, there have been multiple advances in surgical technique and postoperative management which have led to improvement in short- and long-term mortality in this patient population. Operative mortality is now close to 1% and transplant-free survival at 5 and 10 years is 95% and 90%, respectively (1–4). Today, patients have an estimated 30-year survival after Fontan of approximately 85% (1). Given the improving mortality, there is now a growing number of patients with a Fontan circulation worldwide, estimated at up to 70,000 in 2018 and expected to double over the next 20 years (1, 5). The average age of patients with a Fontan circulation is also expected to increase over the coming years, which will only add to the growing burden of morbidity among this population. These patients are at risk for the multitude of morbidities associated with this unique circulation. This review aims to describe the epidemiology and common modes of circulatory failure in patients with a Fontan circulation and examine management strategies utilized in this population.
The morbidities seen in patients with a Fontan circulation are a consequence of the baseline hemodynamic abnormalities associated the Fontan. These include elevated central venous pressure, chronically low preload to a single ventricle leading to decreased cardiac output, and impaired ability to augment cardiac output to meet metabolic demands. Some clinicians have claimed that since patients with a Fontan circulation are unable to augment their cardiac output to meet demands of exercise at low filling pressures, all patients with a Fontan have a chronic form of heart failure (1). There are a number of different definitions of heart failure in the literature, but a recent international consensus definition was proposed as the following: “a clinical syndrome with symptoms and/or signs caused by a structural and/or functional cardiac abnormality and corroborated by elevated natriuretic peptide levels and/or objective evidence of pulmonary or systemic congestion” (6–8). There is overlap between this definition and Fontan circulatory failure, for which the consensus definition is “a broad, non-specific term describing dysfunction of the Fontan circulation that affects a patient’s ability to carry out daily life activities (9).” In this review, we will include causes of heart failure under the broad array of possible underlying etiologies of Fontan circulatory failure (Table 1) (1, 9–14). There does, however, remain difficulties with interchangeability and ambiguity in use of these terms in the literature.
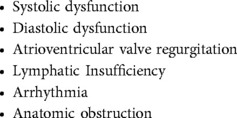
Table 1. Common etiologies of Fontan circulatory failure.
Symptomatic circulatory failure is common in patients with a Fontan. One single center cohort of patients with a Fontan circulation followed over an average of 15.7 years found that 40% exhibit clinical heart failure (10). In another cohort of adult patients with a Fontan circulation, freedom from Fontan failure was 91% at 10 years, 79% at 20 years, and 59% at 25 years after Fontan operation (15). Among all adults with CHD in the Dutch CONCOR registry, adults with single ventricle heart disease had the highest rate of admission for heart failure, with a hazard ratio of 11.4 when compared to patients with ventricular septal defect. This was more than double the hazard ratio calculated for patients with congenitally corrected transposition of the of the great arteries (16). Identified risk factors for Fontan failure include hypoplastic left heart syndrome, greater age at Fontan surgery, longer length of stay at the time of Fontan surgery, progressive systolic and diastolic ventricular dysfunction, atrioventricular valve regurgitation, sustained arrhythmia, and weight gain in adulthood (15, 17–20).
Given the high-risk of circulatory failure in this population, the American Heart Association has recommended an intensive surveillance strategy in adolescents and adults with a Fontan circulation (1). This includes obtaining an exercise stress test every 1–3 years, cardiac MRI every 2–3 years and a surveillance catheterization every 10 years. This may help to identify patients with worsening hemodynamics before they demonstrate symptoms. Once a patient with a Fontan circulation demonstrates clinical heart failure, the prognosis is quite poor (15, 16, 21–23). In a multicenter U.S. study of patients with CHD admitted for heart failure, 28% of single ventricle patients died during admission (21). Another study of patients with a Fontan found that once Fontan failure was manifest, freedom from death or transplant was 70% at 5 years and only 40% at 10 years (15). This prognosis is considerably worse than patients with a Fontan circulation without clinical symptoms, with signs and symptoms of heart failure conferring a 6.3-fold increased risk of death or transplant (22). Predictors of death or transplant that have been identified in the literature include older age, atriopulmonary or atrioventricular type Fontan, morphologic right ventricle, clinically relevant arrhythmia, low heart rate reserve, lower resting oxygen saturation, protein-losing enteropathy, elevated BNP, poorer ventricular performance, poorer functional health status, lower peak VO2, decline in percent predicted VO2 by 3 or more percentage points per year, and higher atrial pressure (2, 22–25).
Systolic ventricular function is typically normal at the time of Fontan but worsens over time (15, 23, 26). In one large cohort of Fontan patients followed for over 20 years, it was found that Fontan failure occurred at a median of 18.1 years after Fontan completion and 46% of these patients had systolic dysfunction. Fontan failure was more commonly associated with a decline in ventricular function than increasing pulmonary vascular resistance (15). About 50% of patients with a Fontan circulation that are listed for transplant have ventricular dysfunction (27–29).
The underlying cause of the decline in systolic function over time in patients with a Fontan circulation is not clear. During the earlier phases of staged palliation, the ventricle is volume loaded and exposed to chronic hypoxemia, which may predispose to dilation and later dysfunction, although studies have demonstrated that ventricular size and hypertrophy improve initially following the Fontan operation (1, 30). Hypoplastic left heart syndrome (HLHS) confers higher risk of systolic dysfunction because the right ventricular morphology is not embryologically or structurally designed to pump against systemic afterload (10, 26). Myocardial fibrosis has also been seen in this population and is associated with lower mean ejection fraction (31). Fibrosis and abnormal myofiber orientation may predispose to mechanical dyssynchrony over time, which has been demonstrated to be associated with reduced systolic function (32–34). Further, the Fontan circulation is a chronically preload deprived state, which may lead to decreased contractility due to chronic lack of fiber stretch and increased muscle stiffness (1).
Patients with a Fontan circulation are particularly affected by systolic dysfunction due to their baseline low cardiac output state. Additionally, preload is further reduced by loss of the normal suction force which occurs with descent of the atrioventricular valve towards the apex of the heart in systole. This force drives blood through the pulmonary vasculature in the normal circulation. The effect of this force becomes relatively more important in patients with a Fontan circulation who do not have a subpulmonary ventricle but is lost in patients with significant systolic dysfunction (35). There has additionally been recent interest in whether atrial function predicts exercise parameters and Fontan outcomes, although atrial function has not been comprehensively studied and the published data is mixed (36–38).
While systolic dysfunction is typically diagnosed by echocardiogram, there are challenges in using echocardiography to assess systolic function in patients with a Fontan circulation, particularly in patients with a systemic right ventricle (39, 40). There is evidence that utilization of cardiac MRI improves risk stratification in patients with a Fontan circulation and thus many centers will use a combination of echocardiography and cardiac MRI to monitor patients for systolic dysfunction over time (40). In a large study of patients with a Fontan circulation who underwent cardiac MRI, lower end-diastolic volume was the strongest predictor of transplant-free survival. For patients with ventricular dilation (end diastolic volume ≥156 ml/BSA), worse global circumferential strain was particularly predictive of death or transplant (41). On multivariable analysis, end-diastolic volume, end-systolic volume, global circumferential strain, and ventriculoarterial coupling ratio by MRI have been shown to be independently predictive of death or transplant. These measurements are thought to be more useful than ejection fraction because ejection fraction does not account for ventricular dilation. Cardiac MRI can also identify cardiac fibrosis which may contribute to dilatation and dysfunction, although additional work is needed to further elucidate the role cardiac fibrosis may have in this process (42). Further, stress MR to identify patients with decreased ability to augment their ejection fraction in response to dobutamine-stress may also help to identify patients at risk of adverse outcomes (43).
Diastolic dysfunction is increasingly being recognized in the Fontan population, affecting approximately 70% of patients, including >80% of patients with a systemic right ventricle (1, 12, 26, 34, 44–46). The single ventricle has multiple possible underlying etiologies for diastolic dysfunction, including dyssynchrony, myocardial scarring, abnormal geometry, increased wall stress, hypoxemia and history of volume loading prior to the Fontan (1, 45). There is evidence of early relaxation abnormalities leading to prolongation of isovolumetric relaxation which reduces early rapid filling and leads to abnormal wall motion and flow (34, 44). This abnormality is then later compounded by a slow reduction in ventricular compliance which also affects late diastolic filling (12, 44).
Increased filling pressures are not well tolerated by patients with a Fontan due to the requirement for passive pulmonary blood flow. Higher filling pressures lead to higher atrial pressures and a lower gradient for forward flow through the pulmonary vasculature. This leads to decreased preload and ultimately decreased stroke volume even without changes in systolic function (45).
Despite the high prevalence of diastolic dysfunction is in this population, it can be difficult to detect, particularly in early stages. Standard echocardiographic Doppler and tissue Doppler parameters are frequently abnormal but have been shown to correlate poorly with clinical outcomes and only modestly with catheterization measurements (46, 47). Cardiac catheterization is considered the standard for measurement of diastolic filling pressures but is invasive and can miss patients with early-stage diastolic dysfunction because it only measures filling pressures in the resting state (45). Speckle tracking echocardiogram has shown some promise in evaluation of diastolic function, but further work is needed to validate this method in single-ventricle patients (48).
Atrioventricular (AV) valve failure, defined as requiring valve repair or replacement or development of moderate or greater AV valve regurgitation (AVVR), is seen in approximately 7% of patients with a Fontan circulation at 5 years, 12% at 10 years and 21% at 20 years (20). AVVR in patients with a Fontan circulation may be secondary to annular dilation, leaflet dysplasia, leaflet tethering, leaflet prolapse, or abnormal subvalvar apparatus (49–51). Patients with hypoplastic left heart syndrome are at particular risk for developing AV valve failure, as systemic right ventricular morphology has been found to be an independent risk factor for AVVR (20, 26). There has also been a demonstrated association between older age at Fontan and more severe AV valve regurgitation (26).
AV valve regurgitation is poorly tolerated in this population as the regurgitation leads to an abnormal feedback loop of dysfunction, worsening dilation and worsening AVVR (50). This further decreases cardiac output and increases atrial pressure, which in turn lead to symptoms of low cardiac output or congestion. Significant AVVR also interferes with interpretation of standard indices of ventricular function, such as ejection fraction, and thus practitioners may underestimate the degree of systolic dysfunction in a single ventricle patient with AVVR (52). Furthermore, AVVR interferes with the aforementioned forward sucking force on the pulmonary venous blood during ventricular systole that becomes relatively more important in single ventricle patients (35). Given this, it is unsurprising that a patient with a Fontan circulation with AV valve failure has been found to have more than double the risk of Fontan failure (20).
Multiple imaging modalities can be utilized in the diagnosis and management of AV valve regurgitation in Fontan patients (53). Though 2D transthoracic echocardiography remains the most common imaging modality used, it is less sensitive to the diagnosis of specific etiologies such as leaflet dysplasia and structural abnormalities. The recent development of 3D echocardiography has addressed some of these limitations, by improving assessment of valve morphology, geometry and subvalvar apparatus. Cardiac MRI can evaluate flow and quantify AVVR but can be limited by artifact in patients with stents or devices. Alternatively, computed tomography can be considered in patients with metallic stents or pacemakers that do not allow for cardiac MRI.
While all patients with a Fontan circulation have lymphatic congestion secondary to the obligate increase in central venous pressure, a subset of patients will develop leakage of chyle into the bronchial, pleural, peritoneal, or intestinal cavities. This results in plastic bronchitis, chylous effusions, chylous ascities, or protein losing enteropathy (1, 14). It is estimated that protein losing enteropathy (PLE) effects between 4% and 13% of patients after Fontan (23, 54, 55). Plastic bronchitis (PB) effects comparatively fewer patients, approximately 2%–4%, although the burden of subclinical PB is likely significant (56, 57). Several factors likely contribute to which patients develop lymphatic complications and which lymphatic disease they manifest, including systemic venous pressures, anatomic Fontan obstruction, lymphatic vessel anatomic differences, prior interventions on the thoracic duct, concomitant cardiac dysfunction, increased mesenteric vascular resistance, proinflammatory state, and genetic differences (1, 58–64). A classification scheme to describe neck and thoracic lymphatics abnormalities has been developed which has been shown to be associated with adverse surgical outcomes after Fontan including mortality, duration of effusions and duration of hospital stay (62). While not a statistically significant association, possibly due to a small sample size, plastic bronchitis and need for transplant within 3 years only occurred in patients with the most severe type 4 abnormalities.
These conditions, which collectively can be referred to as lymphatic insufficiency, can lead to malnutrition, edema, immune deficiency, chronic cough, respiratory distress, hypoxemia and eventually death, although outcomes have improved in the past decade (14, 54, 65). PLE is generally diagnosed by using alpha-1 antitrypsin clearance in a 24-hour stool collection or an elevated alpha-1 antitrypsin level with serum hypoalbuminemia, symptoms of edema, and no other known cause. Imaging modalities such as lymphoscintigraphy and dynamic contrast magnetic resonance lymphangiography can also be used to support the diagnosis of PLE (64). Routine monitoring of serum albumin concentration in patients with a Fontan circulation can identify subclinical albumin loss which may indicate deteriorating hemodynamics (1). Plastic bronchitis is typically diagnosed clinically by patient expectoration of an airway cast or after bronchoscopic removal.
Arrhythmias are common in patients with a Fontan circulation. Sinus node dysfunction and supraventricular tachycardia are most common, affecting up to 60%–80% of patients with a Fontan, although exact rates vary depending on type of Fontan procedure (1). Contemporary surgical techniques such as extracardiac and lateral tunnel Fontan appear to have lower prevalence of arrhythmia as compared to the atriopulmonary type Fontan, but longer follow up is needed to evaluate these newer techniques (1, 17). Ventricular tachycardia is much less common, affecting 5%–12% of the population (66–68). It is estimated that approximately 10% of patients with a Fontan circulation will require pacemaker implantation (69).
Etiologies of arrhythmia in patients with a Fontan circulation include sinus node injury, disruption of the arterial supply of the sinus node, suture lines interfering with conduction, atrial dilation, hypertrophy leading to elevated pressures, the underlying genetic cause of the congenital heart defect causing altered tissue organization, and fibrosis secondary to injury from cyanosis or bypass resulting in altered conduction (1). Arrhythmias further worsen the limited cardiac reserve in a patient with a Fontan circulation. Patients with arrhythmia are significantly more likely to develop heart failure and in one study were found to have a 6-fold increased hazard of death or transplant (19, 22). Atrioventricular synchrony appears to be particularly important to maintain hemodynamics in patients requiring pacing after a Fontan operation (69).
Given the frequency of arrhythmia in Fontan patients, Holter monitoring is recommended every 1–2 years in adolescents and adults, and should particularly be considered in patients experiencing signs and symptoms of Fontan failure (1).
The treatment of circulatory failure in patients with a Fontan is dependent upon identification of the underlying etiology of the failure (Table 2). However, evidence-based recommendations for treatment are limited, with considerable variability among centers with respect to management (70). Surgical and catheter-based interventions, if indicated, typically have superior outcomes to medical therapy, although outcomes vary depending on intervention and indication. Oral medical therapies are typically not very effective, and if there are no surgical or catheter-based interventions to improve the circulation, patients with severe Fontan failure often require inotropic medications or mechanical circulatory support to support the circulation until transplant.
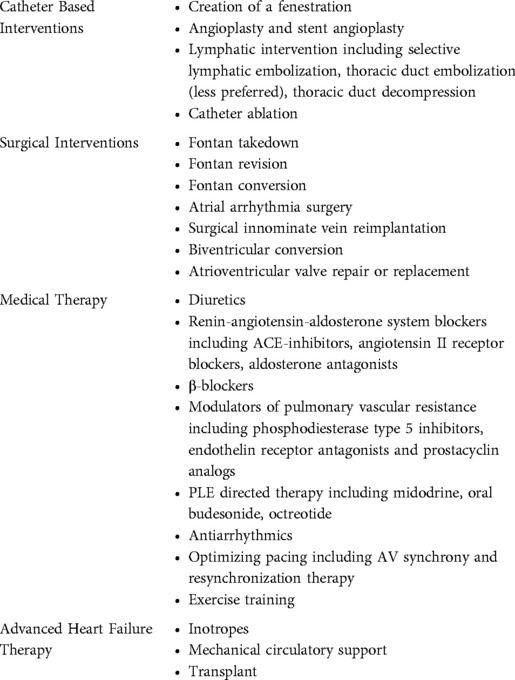
Table 2. Management strategies for Fontan circulatory failure.
Timing of referral to a heart failure specialist may also influence the outcomes of various treatment in these patients. Given concern among pediatric heart failure specialists that patients with a Fontan circulation were being referred too late, when advanced heart failure was already manifest and there was irreversible end-organ damage or clinical instability, the ACTION Network has developed a quality improvement project aimed at improving timely referral to a heart failure specialist through standardized referral guidelines. These guidelines include detailed thresholds of cardiac/systemic ventricular dysfunction, Fontan pathway dysfunction, lymphatic dysfunction, and extra-cardiac dysfunction which the ACTION group feels should prompt considered for referral to an advanced heart failure specialist (71, 72). The quality improvement metric that will be measured is proportion of Fontan patients who do not require escalation of heart failure care within 30 days of referral to the heart failure service and data collection is ongoing.
A variety of catheter-based interventions can be used to improve the Fontan circulation. In patients with obstruction within the Fontan pathway or pulmonary arteries, stent angioplasty may address obstruction and improve lymphatic failure (61, 73). Patients without a patent Fontan fenestration with PLE have been shown to benefit from creation of a fenestration, although this intervention comes at the expense of worsening hypoxemia and the risks of systemic embolization of venous thrombosis (54, 65, 74).
Lymphatic interventions for patients with lymphatic disease can also be attempted. Thoracic duct embolization and selective lymphatic embolization have been used to successfully treat patients with lymphatic insufficiency (75–77). Our institution prefers to use selective lymphatic embolization as it leaves the thoracic duct intact for other possible interventions in the future (64). Further, thoracic duct embolization can actually worsen abdominal symptoms in patients with multicompartment lymphatic disease. If selective lymphatic embolization is not successful in these patients with multicompartment involvement, there has been early promise in transcatheter thoracic duct decompression, although this procedure requires considerable technical expertise (78). Finally, in atriopulmonary Fontan patients with persistent atrial arrhythmias contributing to heart failure symptoms, catheter ablation has been demonstrated to be safe and effective at reducing arrhythmia burden, although approximately half of patients will experience a documented episode of recurrent atrial arrhythmia post procedure and close to one third will require repeat ablation (79).
Surgical interventions should also be considered in a patient experiencing Fontan circulatory failure. These include Fontan takedown, which is typically used in patients in the early postoperative period, Fontan revision, used in patients with Fontan obstruction, and Fontan conversion to a lateral tunnel or extracardiac Fontan, which is used in patients with an atriopulmonary type Fontan (80). Fontan takedown is accompanied by a very high early mortality, though it may be the only option for patients who are intolerant of Fontan physiology but may tolerate Glenn physiology until a transplant can be obtained. Fontan revision for surgical relief of Fontan obstruction can improve lymphatic dysfunction and Fontan conversion is often performed in conjunction with atrial arrhythmia surgery or pacemaker implantation to improve flow dynamics, lower incidence of arrhythmia and improve functional status (65, 81). The main drawback of surgical revision in this population is the high upfront risk. Fontan conversion has an early mortality at approximately 5%–10% with significant variability in outcomes among centers (81–83). In an analysis of the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD), Fontan revision had the highest reported mortality among all adult congenital cardiac operations (83). Risk factors for worse outcomes in patients undergoing Fontan revision include older age, presence of any STS-CHSD defined preoperative risk factor including preoperative mechanical circulatory support, diabetes, hepatic dysfunction, hypercoagulable state, renal dysfunction, complete heart block, pacemaker, implantable ICD and prior cardiothoracic operation, and concomitant pulmonary artery reconstruction (82).
Surgical innominate vein reimplantation to the lower-pressure pulmonary venous atrium (“turn down”) is another strategy that has been described in Fontan patients with lymphatic dysfunction, although it will worsen cyanosis (84, 85). Alternatively, in certain subsets of patients with a borderline second ventricle, biventricular conversion with possible recruitment of the systemic ventricle before conversion could be considered (86). Finally, in single ventricle patients with significant AV valve regurgitation, surgical intervention on the valve is an option. There is a movement in the field toward identifying the mechanism of AV valve insufficiency with earlier valve repair, perhaps prior to Fontan, and more aggressive valve replacement in specific situations (87–89). Although these procedures can be successfully performed, there remains a question of durability of repair (90).
Medical options include the use of many of the drugs used in biventricular heart failure, but with less evidence to support the practice. A recent systematic review of the evidence for medical therapy in prevention of Fontan circulatory failure identified only 9 studies which included only 267 Fontan patients total (91).
Diuretics are frequently used in systolic and diastolic dysfunction for symptomatic control. While they may reduce the filling pressure and improve symptoms of heart failure, they also decrease cardiac output and are often associated with electrolyte disarray and potential worsening of renal dysfunction (1). Reverse remodeling agents including renin-angiotensin-aldosterone system blockers and β-blockers are frequently used in clinical practice, albeit with little data to support the benefit of these drugs in single-ventricle patients with ventricular dysfunction or AV valve regurgitation (12, 45, 92–94). In one cohort study of patients after Fontan, 10 weeks of enalapril administration did not alter baseline hemodynamics, exercise capacity, or diastolic function and there was a suggestion of a worsening of short term exercise capacity (93). In another small cohort treated with ACE inhibitors for 6 months, no difference was seen in ventricular ejection fraction (94). Data demonstrating improved ventricular function, reversal in left-ventricular hypertrophy, and improved ventricular volume overload in patients with two-ventricle circulations with mitral or aortic valve regurgitation are often extrapolated to single ventricle patients, but there have been no studies specifically examining this effect in the patients with AV valve regurgitation and a Fontan (95–97). Use of beta blockers has also been examined in patients with a Fontan with heart failure, but a randomized control trial of beta blockade in children demonstrated that use of beta blockers may actually be harmful in patients with a systemic right ventricle (98). There is some evidence for a role for high dose spironolactone in failing Fontan patients specifically with PLE, although again the data remain limited to small series (65, 99, 100).
Modulators of pulmonary vascular resistance have also been used in this population, with some evidence supporting the practice. Phosphodiesterase type 5 inhibitors are of particular interest given their ability to decrease PVR, improve ventricular end-diastolic elastance, decrease arterial elastance, and increase ventricular end-systolic elastance, which in turn may improve preload and ventriculoarterial coupling (101). Small studies using sildenafil have demonstrated improved exercise capacity, improved exercise hemodynamics, and improved ventricular performance (102–106). Recent results from the larger FUEL trial demonstrated no significant change in peak oxygen consumption in patients with a Fontan circulation treated with udenafil. However, there was a statistically significant improvement in submaximal exercise measures including oxygen consumption, work rate, and ventilatory efficiency at the anaerobic threshold (107). Bosentan has also been examined in small scale trials and has shown mixed results in its effect on exercise capacity and New York Heart Association functional class (108–110). Finally, a single study of inhaled iloprost prior to exercise stress test demonstrated improved peak oxygen pulse and peak oxygen consumption and was particularly beneficial in patient with impaired exercise function at baseline (111). One subpopulation of patients with Fontan failure that may benefit from pulmonary vasodilation in particular are patients with lymphatic failure (65, 112).
If mediators of pulmonary vascular resistance are not effective, patients with protein losing enteropathy have several additional medical options which may be effective in some patients. Midodrine, an alpha-1-receptor agonist, has shown some promise, with a recent case series of four patients with refractory PLE demonstrating symptomatic improvement leading to deferral of transplant evaluation in two patients and transplant delisting in one patient (113). It is hypothesized that midodrine works by its effect on tone in the smooth muscle cells in the lymphatic vessels, though additional work is needed to confirm this hypothesis (113, 114). Additional medical treatments for patients with PLE include oral budesonide and octreotide, but use may not reduce the need for transplant over the long term (65, 115, 116).
Antiarrhythmics for control of atrial arrhythmias can improve systolic dysfunction and AV valve regurgitation. However, use of antiarrhythmic medications in patients with Fontan has been associated with a higher risk of recurrence and more adverse events compared to interventions such as catheter ablation or Fontan conversion (1, 117). In patients with a pacemaker, employing a pacing mode with atrioventricular synchrony has been demonstrated to improve Fontan hemodynamics (69). In Fontan patients with heart block or intact conduction with significant dyssynchrony, cardiac resynchronization therapy with dual-site ventricular pacing has shown mixed results though recent data has demonstrated improved indices of ventricular function that are less dependent upon ventricular anatomy and geometry. These improved indices also appear to correlate with improved New York Heart Association classification (118).
Finally, exercise training as therapy for Fontan patients should be considered, as it has been examined in a number of small studies with some demonstrating an increase in peak oxygen uptake, an increase in cardiac output, or an increase in quality of life with training (119). More study is needed to determine the optimal training type and program. However, if there is significant Fontan circulatory failure it is unlikely that exercise training alone will prevent the need for advanced heart failure therapies.
In Fontan patients with low cardiac output and compromised end-organ perfusion, intravenous inotropic support may be necessary (6). There are few data regarding the use of inotropes in patients with a Fontan circulation, and thus inotropic support in these patients is typically based on anecdotal experience and extrapolation of data from adult and pediatric patients with a biventricular circulation (120–123). Pediatric heart failure guidelines recommend milrinone or dobutamine as first line therapy with the addition of epinephrine for refractory hypotension (6). In patients with PLE, dopamine therapy can be trialed, as there is evidence it may induce remission in patients with PLE possibly through effects on lymphatic receptors (124).
Despite the lack of data, the inotropic, lusitropic, and vasodilatory properties of phosphodiesterase-3 inhibitors such as milrinone make this class of drug appealing for treatment of the failing Fontan (125, 126). Phosphodiesterase-3 inhibitors have been demonstrated to improve early postoperative hemodynamics in Fontan patients by increasing cardiac index and stroke volume index but this effect has not been specifically examined in Fontan patients remote from surgical repair (127). Interestingly, the molecular myocardial effects from milrinone appear to be unique in patients with a failing single right ventricle as compared to pediatric patients with dilated cardiomyopathy (128).
The effect of chronic inotrope use in this population remains unknown and may be harmful (129). Therefore, we recommend chronic inotrope use only in palliative circumstances or as a bridge to transplant.
Due to the increasing number of Fontan patients with circulatory failure and the long wait times for organ transplantation, the use of durable mechanical circulatory support (MCS) in this population is becoming increasingly common (130–135). Unfortunately, outcomes remain inferior when compared to patients with a biventricular circulation, though seem to be improving (130, 135–140). Encouragingly, the ACTION Network recently reported no deaths among 5 patients with a Fontan circulation supported with a Heartmate 3 device (139).
Despite improving outcomes, there remain several challenges to supporting patients with a Fontan circulation with MCS. Surgical challenges include a redo sternotomy, cumbersome mediastinal dissection and dense trabeculations within the ventricle which can require resection to avoid inflow obstruction, and challenging geometry of cannula position in single ventricle patients (134). Novel surgical approaches including atrial cannulation and excision of AV valve may be needed to place devices in smaller patients (141). Further, a ventricular assist device may not address the underlying cause of the Fontan failure. MCS is typically most beneficial in patients with ventricular dysfunction, but may not be as useful in patients with other forms of Fontan failure, where preload is limited and increasing the cardiac output can further worsen right-sided congestive symptoms (1, 134). In patients with Fontan circulatory failure without significant pump dysfunction, innovative support strategies may need to be employed. There have been single case reports of successful use of BiVAD, Syncardia Total Artificial Heart and single subpulmonary VAD in patients with Fontan circulations, but these strategies have not been widely adopted (142–144).
Additionally, temporary VAD support with Impella has been described in a limited number of pediatric and adult patients with a Fontan circulation with cardiogenic shock with encouraging results (145, 146). These devices may be used as a bridge to recovery or more durable support. Noted challenges in this population include abnormal relationships between the great arteries and abnormal orientation of the atrioventricular valves relative to the outflow tracts. Reported complications included one procedural death, increasing aortic valve insufficiency, access site thrombus, extremity ischemia, hemolysis, and renal failure.
Transplant remains the definitive treatment for circulatory failure after Fontan; however, there is significant variability in access to transplant across centers (23). A recent analysis of the STS-CHSD demonstrated an increasing number of transplants performed in patients with a Fontan over the last decade, due primarily to an increase in patients with HLHS (82). Waitlist mortality is considerable, although pediatric patients with a Fontan circulation have demonstrated similar pretransplant survival (78% at 6 months and 74% at 12 months) to other patients listed for transplant both with and without CHD (147). However, adult patients with CHD listed 1A for transplant have higher wait list mortality than non-congenital heart patients, estimated at approximately 1 in 4 (148). Risk factors for death while waiting in the pediatric population include younger age, status 1 listing, shorter interval since Fontan and ventilator support (147).
Transplantation in patients with a Fontan is high-risk, but outcomes have improved in recent decades (29, 147, 149–152). Recent approximate 1 year survival was 89%. This 1 year survival is similar to non-Fontan CHD patients, although continues to lag behind outcomes in patients without congenital heart disease (147, 151). Operative mortality and composite major morbidity and mortality remain high at 7.6% and 35%, respectively (82). Fontan patients have several baseline risk factors including multiple prior cardiac surgeries with exposure to blood products and homograft and significant aortopulmonary collateral burden. Therefore, at transplant they are at increased risk of surgical complications including complicated dissection, bleeding, and longer ischemic time, as well as longer term complications such as rejection due to presensitization (153, 154). Identified risk factors for worse outcomes include increasing age among adult patients and preserved ventricular function (28, 82). This may be because Fontan patients with preserved ventricular function are more likely to have long term malnutrition, immunosuppression, and pulmonary complications, therefore there is possible benefit to earlier referral in this population. Patients with PLE who survive transplant have been shown to have resolution of their PLE (147, 150, 155). The most common causes of death after transplant in patients with a Fontan are similar to other transplant populations and include infection, early graft failure, rejection and sudden death (147).
One area of active research in Fontan management is in multiorgan transplant. Fontan associated liver disease is common and some patients with hepatic dysfunction will undergo heart-liver transplantation. There is discrepant data regarding whether outcomes are better in Fontan patients with cirrhosis undergoing heart-liver transplant vs. heart transplant alone (156–158). It is not known which patients are likely to have reversal of hepatic dysfunction after heart transplant alone and thus universal indications for heart-liver transplant remain undefined.
Circulatory failure in patients with a Fontan circulation is becoming an increasingly common issue. Management of Fontan failure is dependent upon identification of the underlying etiology, which may include ventricular systolic and diastolic dysfunction, atrioventricular valve regurgitation, arrhythmia, and lymphatic insufficiency. Surgical and catheter-based interventions may be effective in addressing specific causes of Fontan failure but can be high risk for patients. Medical therapies are frequently tried but not very effective overall, and thus advanced heart failure therapies are often required, including inotropic infusions, ventricular assist devices, and heart transplantation. There remains considerable room for improvement in the management and outcomes of patients with circulatory failure after Fontan surgery.
All authors contributed to the design, drafting, and critically reviewing the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rychik J, Atz AM, Celermajer DS, Deal BJ, Gatzoulis MA, Gewillig MH, et al. Evaluation and management of the child and adult with Fontan circulation: a scientific statement from the American Heart Association. Circulation. (2019) 140(6):e234–84. doi: 10.1161/CIR.0000000000000696
2. Khairy P, Fernandes SM, Mayer JE Jr, Triedman JK, Walsh EP, Lock JE, et al. Long-term survival, modes of death, and predictors of mortality in patients with Fontan surgery. Circulation. (2008) 117(1):85–92. doi: 10.1161/CIRCULATIONAHA.107.738559
3. Downing TE, Allen KY, Glatz AC, Rogers LS, Ravishankar C, Rychik J, et al. Long-term survival after the Fontan operation: twenty years of experience at a single center. J Thorac Cardiovasc Surg. (2017) 154(1):243–53. e2. doi: 10.1016/j.jtcvs.2017.01.056
4. Iyengar AJ, Winlaw DS, Galati JC, Celermajer DS, Wheaton GR, Gentles TL, et al. Trends in Fontan surgery and risk factors for early adverse outcomes after Fontan surgery: the Australia and New Zealand Fontan Registry experience. J Thorac Cardiovasc Surg. (2014) 148(2):566–75. doi: 10.1016/j.jtcvs.2013.09.074
5. Schilling C, Dalziel K, Nunn R, Du Plessis K, Shi WY, Celermajer D, et al. The Fontan epidemic: population projections from the Australia and New Zealand Fontan registry. Int J Cardiol. (2016) 219:14–9. doi: 10.1016/j.ijcard.2016.05.035
6. Kirk R, Dipchand AI, Rosenthal DN, Addonizio L, Burch M, Chrisant M, et al. The international society for heart and lung transplantation guidelines for the management of pediatric heart failure: executive summary. J Heart Lung Transplant. (2014) 33(9):888–909. doi: 10.1016/j.healun.2014.06.002
7. Bozkurt B, Coats AJ, Tsutsui H, Abdelhamid M, Adamopoulos S, Albert N, et al. Universal definition and classification of heart failure: a report of the heart failure society of America, heart failure association of the European society of cardiology, Japanese heart failure society and writing committee of the universal definition of heart failure. J Card Fail. (2021) 27(4):387–413. doi: 10.1016/j.cardfail.2021.01.022
8. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2016) 37(27):2129–200. doi: 10.1093/eurheartj/ehw128
9. Alsaied T, Rathod RH, Aboulhosn JA, Budts W, Anderson JB, Baumgartner H, et al. Reaching consensus for unified medical language in Fontan care. ESC Heart Fail. (2021) 8(5):3894–905. doi: 10.1002/ehf2.13294
10. Piran S, Veldtman G, Siu S, Webb GD, Liu PP. Heart failure and ventricular dysfunction in patients with single or systemic right ventricles. Circulation. (2002) 105(10):1189–94. doi: 10.1161/hc1002.105182
11. Book WM, Gerardin J, Saraf A, Marie Valente A, Rodriguez F III. Clinical phenotypes of Fontan failure: implications for management. Congenit Heart Dis. (2016) 11(4):296–308. doi: 10.1111/chd.12368
12. Kantor PF, Redington AN. Pathophysiology and management of heart failure in repaired congenital heart disease. Heart Fail Clin. (2010) 6(4):497–506. doi: 10.1016/j.hfc.2010.06.002
13. Law YM, Ettedgui J, Beerman L, Maisel A, Tofovic S. Comparison of plasma B-type natriuretic peptide levels in single ventricle patients with systemic ventricle heart failure versus isolated cavopulmonary failure. Am J Cardiol. (2006) 98(4):520–4. doi: 10.1016/j.amjcard.2006.02.058
14. Del Castillo S, Shaddy RE, Kantor PF. Update on pediatric heart failure. Curr Opin Pediatr. (2019) 31(5):598–603. doi: 10.1097/MOP.0000000000000807
15. Sallmon H, Ovroutski S, Schleiger A, Photiadis J, Weber SC, Nordmeyer J, et al. Late Fontan failure in adult patients is predominantly associated with deteriorating ventricular function. Int J Cardiol. (2021) 344:87–94. doi: 10.1016/j.ijcard.2021.09.042
16. Zomer A, Vaartjes I, Van Der Velde E, De Jong H, Konings T, Wagenaar L, et al. Heart failure admissions in adults with congenital heart disease; risk factors and prognosis. Int J Cardiol. (2013) 168(3):2487–93. doi: 10.1016/j.ijcard.2013.03.003
17. d’Udekem Y, Iyengar AJ, Galati JC, Forsdick V, Weintraub RG, Wheaton GR, et al. Redefining expectations of long-term survival after the Fontan procedure: twenty-five years of follow-up from the entire population of Australia and New Zealand. Circulation. (2014) 130(11_suppl_1):S32–8. doi: 10.1161/CIRCULATIONAHA.113.007764
18. Byrne RD, Weingarten AJ, Clark DE, Healan SJ, Richardson TL, Huang S, et al. Sizing up Fontan failure: association with increasing weight in adulthood. Pediatr Cardiol. (2021) 42(6):1425–32. doi: 10.1007/s00246-021-02628-8
19. Ghai A, Harris L, Harrison DA, Webb GD, Siu SC. Outcomes of late atrial tachyarrhythmias in adults after the Fontan operation. J Am Coll Cardiol. (2001) 37(2):585–92. doi: 10.1016/S0735-1097(00)01141-4
20. King G, Ayer J, Celermajer D, Zentner D, Justo R, Disney P, et al. Atrioventricular valve failure in Fontan palliation. J Am Coll Cardiol. (2019) 73(7):810–22. doi: 10.1016/j.jacc.2018.12.025
21. Burstein DS, Shamszad P, Dai D, Almond CS, Price JF, Lin KY, et al. Significant mortality, morbidity and resource utilization associated with advanced heart failure in congenital heart disease in children and young adults. Am Heart J. (2019) 209:9–19. doi: 10.1016/j.ahj.2018.11.010
22. Diller G-P, Giardini A, Dimopoulos K, Gargiulo G, Müller J, Derrick G, et al. Predictors of morbidity and mortality in contemporary Fontan patients: results from a multicenter study including cardiopulmonary exercise testing in 321 patients. Eur Heart J. (2010) 31(24):3073–83. doi: 10.1093/eurheartj/ehq356
23. Atz AM, Zak V, Mahony L, Uzark K, D’agincourt N, Goldberg DJ, et al. Longitudinal outcomes of patients with single ventricle after the Fontan procedure. J Am Coll Cardiol. (2017) 69(22):2735–44. doi: 10.1016/j.jacc.2017.03.582
24. Ohuchi H, Negishi J, Noritake K, Hayama Y, Sakaguchi H, Miyazaki A, et al. Prognostic value of exercise variables in 335 patients after the Fontan operation: a 23-year single-center experience of cardiopulmonary exercise testing. Congenit Heart Dis. (2015) 10(2):105–16. doi: 10.1111/chd.12222
25. Egbe AC, Driscoll DJ, Khan AR, Said SS, Akintoye E, Berganza FM, et al. Cardiopulmonary exercise test in adults with prior Fontan operation: the prognostic value of serial testing. Int J Cardiol. (2017) 235:6–10. doi: 10.1016/j.ijcard.2017.02.140
26. Anderson PA, Sleeper LA, Mahony L, Colan SD, Atz AM, Breitbart RE, et al. Contemporary outcomes after the Fontan procedure: a Pediatric Heart Network multicenter study. J Am Coll Cardiol. (2008) 52(2):85–98. doi: 10.1016/j.jacc.2008.01.074
27. Miller JR, Simpson KE, Epstein DJ, Lancaster TS, Henn MC, Schuessler RB, et al. Improved survival after heart transplant for failed Fontan patients with preserved ventricular function. J Heart Lung Transplant. (2016) 35(7):877–83. doi: 10.1016/j.healun.2016.02.005
28. Griffiths ER, Kaza AK, von Ballmoos MCW, Loyola H, Valente AM, Blume ED, et al. Evaluating failing Fontans for heart transplantation: predictors of death. Ann Thorac Surg. (2009) 88(2):558–64. doi: 10.1016/j.athoracsur.2009.03.085
29. Jayakumar KA, Addonizio LJ, Kichuk-Chrisant MR, Galantowicz ME, Lamour JM, Quaegebeur JM, et al. Cardiac transplantation after the Fontan or Glenn procedure. J Am Coll Cardiol. (2004) 44(10):2065–72. doi: 10.1016/j.jacc.2004.08.031
30. Gewillig MH, Lundström U, Deanfield J, Bull C, Franklin R, Graham T Jr, et al. Impact of Fontan operation on left ventricular size and contractility in tricuspid atresia. Circulation. (1990) 81(1):118–27. doi: 10.1161/01.CIR.81.1.118
31. Rathod RH, Prakash A, Powell AJ, Geva T. Myocardial fibrosis identified by cardiac magnetic resonance late gadolinium enhancement is associated with adverse ventricular mechanics and ventricular tachycardia late after Fontan operation. J Am Coll Cardiol. (2010) 55(16):1721–8. doi: 10.1016/j.jacc.2009.12.036
32. Ho P-K, Lai CT, Wong SJ, Cheung Y-F. Three-dimensional mechanical dyssynchrony and myocardial deformation of the left ventricle in patients with tricuspid atresia after Fontan procedure. J Am Soc Echocardiogr. (2012) 25(4):393–400. doi: 10.1016/j.echo.2012.01.003
33. Sanchez-Quintana D, Climent V, Ho S, Anderson R. Myoarchitecture and connective tissue in hearts with tricuspid atresia. Heart. (1999) 81(2):182–91. doi: 10.1136/hrt.81.2.182
34. Rösner A, Khalapyan T, Dalen H, McElhinney DB, Friedberg MK, Lui GK. Classic-pattern dyssynchrony in adolescents and adults with a Fontan circulation. J Am Soc Echocardiogr. (2018) 31(2):211–9. doi: 10.1016/j.echo.2017.10.018
35. Rychik J, Fogel MA, Donofrio MT, Goldmuntz E, Cohen MS, Spray TL, et al. Comparison of patterns of pulmonary venous blood flow in the functional single ventricle heart after operative aortopulmonary shunt versus superior cavopulmonary shunt. Am J Cardiol. (1997) 80(7):922–6. doi: 10.1016/S0002-9149(97)00546-8
36. van der Ven JP, Alsaied T, Juggan S, Bossers SS, van den Bosch E, Kapusta L, et al. Atrial function in Fontan patients assessed by CMR: relation with exercise capacity and long-term outcomes. Int J Cardiol. (2020) 312:56–61. doi: 10.1016/j.ijcard.2020.02.060
37. Critser PJ, Truong V, Powell AW, Almeneisi H, Opotowsky AR, Ollberding NJ, et al. Cardiac magnetic resonance derived atrial function in patients with a Fontan circulation. Int J Cardiovasc Imaging. (2021) 37(1):275–84. doi: 10.1007/s10554-020-01959-6
38. van der Ven JP, Bossers SS, van den Bosch E, Dam N, Kuipers IM, van Iperen GG, et al. Dobutamine stress testing for the evaluation of atrial and diastolic ventricular function in Fontan patients. Open Heart. (2021) 8(1):e001487. doi: 10.1136/openhrt-2020-001487
39. Margossian R, Schwartz ML, Prakash A, Wruck L, Colan SD, Atz AM, et al. Comparison of echocardiographic and cardiac magnetic resonance imaging measurements of functional single ventricular volumes, mass, and ejection fraction (from the Pediatric Heart Network Fontan Cross-Sectional Study). Am J Cardiol. (2009) 104(3):419–28. doi: 10.1016/j.amjcard.2009.03.058
40. Rathod RH, Prakash A, Kim YY, Germanakis IE, Powell AJ, Gauvreau K, et al. Cardiac magnetic resonance parameters predict transplantation-free survival in patients with fontan circulation. Circ Cardiovasc Imaging. (2014) 7(3):502–9. doi: 10.1161/CIRCIMAGING.113.001473
41. Meyer SL, St. Clair N, Powell AJ, Geva T, Rathod RH. Integrated clinical and magnetic resonance imaging assessments late after Fontan operation. J Am Coll Cardiol. (2021) 77(20):2480–9. doi: 10.1016/j.jacc.2021.03.312
42. Fogel MA. The Fontan: “Straining” to understand that “the bigger they come, the harder they fall”. Washington, DC: American College of Cardiology Foundation (2021). 2490–3.
43. van den Bosch E, Bossers SS, Robbers-Visser D, Boersma E, Roos-Hesselink JW, Breur HM, et al. Ventricular response to dobutamine stress CMR is a predictor for outcome in Fontan patients. JACC Cardiovasc Imaging. (2019) 12(2):368–70. doi: 10.1016/j.jcmg.2018.07.025
44. Cheung Y, Penny D, Redington A. Serial assessment of left ventricular diastolic function after Fontan procedure. Heart. (2000) 83(4):420–4. doi: 10.1136/heart.83.4.420
45. Budts W, Ravekes WJ, Danford DA, Kutty S. Diastolic heart failure in patients with the Fontan circulation: a review. JAMA Cardiol. (2020) 5(5):590–7. doi: 10.1001/jamacardio.2019.5459
46. Margossian R, Sleeper LA, Pearson GD, Barker PC, Mertens L, Quartermain MD, et al. Assessment of diastolic function in single-ventricle patients after the Fontan procedure. J Am Soc Echocardiogr. (2016) 29(11):1066–73. doi: 10.1016/j.echo.2016.07.016
47. Menon SC, Gray R, Tani LY. Evaluation of ventricular filling pressures and ventricular function by Doppler echocardiography in patients with functional single ventricle: correlation with simultaneous cardiac catheterization. J Am Soc Echocardiogr. (2011) 24(11):1220–5. doi: 10.1016/j.echo.2011.08.011
48. Steflik D, Butts RJ, Baker GH, Bandisode V, Savage A, Atz AM, et al. A preliminary comparison of two-dimensional speckle tracking echocardiography and pressure–volume loop analysis in patients with Fontan physiology: the role of ventricular morphology. Echocardiography. (2017) 34(9):1353–9. doi: 10.1111/echo.13641
49. Takahashi K, Inage A, Rebeyka I, Ross D, Thompson R, Mackie A, et al. Real-time 3-dimensional echocardiography provides new insight into mechanisms of tricuspid valve regurgitation in patients with hypoplastic left heart syndrome. Circulation. (2009) 120(12):1091–8. doi: 10.1161/CIRCULATIONAHA.108.809566
50. Ohye RG, Gomez CA, Goldberg CS, Graves HL, Devaney EJ, Bove EL. Repair of the tricuspid valve in hypoplastic left heart syndrome. Cardiol Young. (2006) 16(S3):21–6. doi: 10.1017/S1047951106000722
51. Stamm C, Anderson RH, Ho SY. The morphologically tricuspid valve in hypoplastic left heart syndrome. Eur J Cardiothorac Surg. (1997) 12(4):587–92. doi: 10.1016/S1010-7940(97)00184-X
52. Dupuis M, Mahjoub H, Clavel MA, Côté N, Toubal O, Tastet L, et al. Forward left ventricular ejection fraction: a simple risk marker in patients with primary mitral regurgitation. J Am Heart Assoc. (2017) 6(11):e006309. doi: 10.1161/JAHA.117.006309
53. Tseng SY, Siddiqui S, Di Maria MV, Hill GD, Lubert AM, Kutty S, et al. Atrioventricular valve regurgitation in single ventricle heart disease: a common problem associated with progressive deterioration and mortality. J Am Heart Assoc. (2020) 9(11):e015737. doi: 10.1161/JAHA.119.015737
54. Mertens L, Hagler DJ, Sauer U, Somerville J, Gewillig M. Protein-losing enteropathy after the Fontan operation: an international multicenter study. J Thorac Cardiovasc Surg. (1998) 115(5):1063–73. doi: 10.1016/S0022-5223(98)70406-4
55. Feldt RH, Driscoll DJ, Offord KP, Cha RH, Perrault J, Schaff HV, et al. Protein-losing enteropathy after the Fontan operation. J Thorac Cardiovasc Surg. (1996) 112(3):672–80. doi: 10.1016/S0022-5223(96)70051-X
56. Allen KY, Downing TE, Glatz AC, Rogers LS, Ravishankar C, Rychik J, et al. Effect of Fontan-associated morbidities on survival with intact Fontan circulation. Am J Cardiol. (2017) 119(11):1866–71. doi: 10.1016/j.amjcard.2017.03.004
57. Caruthers RL, Kempa M, Loo A, Gulbransen E, Kelly E, Erickson SR, et al. Demographic characteristics and estimated prevalence of Fontan-associated plastic bronchitis. Pediatr Cardiol. (2013) 34(2):256–61. doi: 10.1007/s00246-012-0430-5
58. Rychik J, Gui-Yang S. Relation of mesenteric vascular resistance after Fontan operation and protein-losing enteropathy. Am J Cardiol. (2002) 90(6):672–4. doi: 10.1016/S0002-9149(02)02584-5
59. Ostrow AM, Freeze H, Rychik J. Protein-losing enteropathy after Fontan operation: investigations into possible pathophysiologic mechanisms. Ann Thorac Surg. (2006) 82(2):695–700. doi: 10.1016/j.athoracsur.2006.02.048
60. Bode L, Freeze HH. Applied glycoproteomics—approaches to study genetic-environmental collisions causing protein-losing enteropathy. Biochim Biophys Acta. (2006) 1760(4):547–59. doi: 10.1016/j.bbagen.2005.11.004
61. Schleiger A, Ovroutski S, Peters B, Schubert S, Photiadis J, Berger F, et al. Treatment strategies for protein-losing enteropathy in Fontan-palliated patients. Cardiol Young. (2020) 30(5):698–709. doi: 10.1017/S1047951120000864
62. Biko DM, DeWitt AG, Pinto EM, Morrison RE, Johnstone JA, Griffis H, et al. MRI Evaluation of lymphatic abnormalities in the neck and thorax after Fontan surgery: relationship with outcome. Radiology. (2019) 291(3):774. doi: 10.1148/radiol.2019180877
63. Dori Y, Keller MS, Fogel MA, Rome JJ, Whitehead KK, Harris MA, et al. MRI Of lymphatic abnormalities after functional single-ventricle palliation surgery. Am J Roentgenol. (2014) 203(2):426–31. doi: 10.2214/AJR.13.11797
64. Tomasulo CE, Chen JM, Smith CL, Maeda K, Rome JJ, Dori Y. Lymphatic disorders and management in patients with congenital heart disease. Ann Thorac Surg. (2020) 113(4):1101–11. doi: 10.1016/j.athoracsur.2020.10.058
65. John AS, Johnson JA, Khan M, Driscoll DJ, Warnes CA, Cetta F. Clinical outcomes and improved survival in patients with protein-losing enteropathy after the Fontan operation. J Am Coll Cardiol. (2014) 64(1):54–62. doi: 10.1016/j.jacc.2014.04.025
66. Pundi KN, Johnson JN, Dearani JA, Pundi KN, Li Z, Hinck CA, et al. 40-year follow-up after the Fontan operation: long-term outcomes of 1,052 patients. J Am Coll Cardiol. (2015) 66(15):1700–10. doi: 10.1016/j.jacc.2015.07.065
67. Pundi KN, Pundi KN, Johnson JN, Dearani JA, Li Z, Driscoll DJ, et al. Sudden cardiac death and late arrhythmias after the Fontan operation. Congenit Heart Dis. (2017) 12(1):17–23. doi: 10.1111/chd.12401
68. Nakamura Y, Yagihara T, Kagisaki K, Hagino I, Kobayashi J. Ventricular performance in long-term survivors after Fontan operation. Ann Thorac Surg. (2011) 91(1):172–80. doi: 10.1016/j.athoracsur.2010.07.055
69. Barber BJ, Batra AS, Burch GH, Shen I, Ungerleider RM, Brown JW, et al. Acute hemodynamic effects of pacing in patients with Fontan physiology: a prospective study. J Am Coll Cardiol. (2005) 46(10):1937–42. doi: 10.1016/j.jacc.2005.07.045
70. Anderson PA, Breitbart RE, McCrindle BW, Sleeper LA, Atz AM, Hsu DT, et al. The Fontan patient: inconsistencies in medication therapy across seven pediatric heart network centers. Pediatr Cardiol. (2010) 31(8):1219–28. doi: 10.1007/s00246-010-9807-5
71. Schumacher K, Kindel S. Considerations for advanced heart failure consultation in Fontan Patients: Guidance for primary cardiologists. Advanced Cardiac Therapies Improving Outcomes Network. Available from: http://wwwactionlearningnetworkorg (Accessed May, 2019);16.
72. Bansal N, Burstein DS, Lorts A, Smyth L, Rosenthal DN, Peng DM. Heart failure in children: priorities and approach of the ACTION collaborative. Prog Pediatr Cardiol. (2020) 59:101313. doi: 10.1016/j.ppedcard.2020.101313
73. Mets JM, Bergersen L, Mayer JE Jr, Marshall AC, McElhinney DB. Outcomes of stent implantation for obstruction of intracardiac lateral tunnel Fontan pathways. Circ: Cardiovasc Interventions. (2013) 6(1):92–100. doi: 10.1161/CIRCINTERVENTIONS.112.000099
74. Jacobs ML, Rychik J, Byrum CJ, Norwood WI Jr. Protein-losing enteropathy after Fontan operation: resolution after baffle fenestration. Ann Thorac Surg. (1996) 61(1):206–8. doi: 10.1016/0003-4975(95)00659-1
75. Kylat RI, Witte MH, Barber BJ, Dori Y, Ghishan FK. Resolution of protein-losing enteropathy after congenital heart disease repair by selective lymphatic embolization. Pediatr Gastroenterol Hepatol Nutr. (2019) 22(6):594–600. doi: 10.5223/pghn.2019.22.6.594
76. Dori Y, Keller MS, Rome JJ, Gillespie MJ, Glatz AC, Dodds K, et al. Percutaneous lymphatic embolization of abnormal pulmonary lymphatic flow as treatment of plastic bronchitis in patients with congenital heart disease. Circulation. (2016) 133(12):1160–70. doi: 10.1161/CIRCULATIONAHA.115.019710
77. DePopas EM, Veress LA, Ahmed F, Rausch CM, Annam A, Gupta R. Percutaneous thoracic duct intervention to treat plastic bronchitis related to Fontan palliation. Pediatr Pulmonol. (2017) 52(11):E97–E101. doi: 10.1002/ppul.23793
78. Smith CL, Dori Y, O’Byrne ML, Glatz AC, Gillespie MJ, Rome JJ. Transcatheter thoracic duct decompression for multicompartment lymphatic failure after Fontan palliation. Circ: Cardiovasc Interventions. (2022) 15(7):e011733. doi: 10.1161/CIRCINTERVENTIONS.121.011733
79. Moore BM, Anderson R, Nisbet AM, Kalla M, du Plessis K, d’Udekem Y, et al. Ablation of atrial arrhythmias after the atriopulmonary Fontan procedure: mechanisms of arrhythmia and outcomes. JACC Clin Electrophysiol. (2018) 4(10):1338–46. doi: 10.1016/j.jacep.2018.08.012
80. Van Melle JP, Wolff D, Hörer J, Belli E, Meyns B, Padalino M, et al. Surgical options after Fontan failure. Heart. (2016) 102(14):1127–33. doi: 10.1136/heartjnl-2015-309235
81. Brida M, Baumgartner H, Gatzoulis MA, Diller G-P. Early mortality and concomitant procedures related to Fontan conversion: quantitative analysis. Int J Cardiol. (2017) 236:132–7. doi: 10.1016/j.ijcard.2017.01.111
82. Serfas JD, Thibault D, Andersen ND, Chiswell K, Jacobs JP, Jacobs ML, et al. The evolving surgical burden of Fontan failure: an analysis of the society of thoracic surgeons congenital heart surgery database. Ann Thorac Surg. (2021) 112(1):179–87. doi: 10.1016/j.athoracsur.2020.05.174
83. Fuller SM, He X, Jacobs JP, Pasquali SK, Gaynor JW, Mascio CE, et al. Estimating mortality risk for adult congenital heart surgery: an analysis of the society of thoracic surgeons congenital heart surgery database. Ann Thorac Surg. (2015) 100(5):1728–36. doi: 10.1016/j.athoracsur.2015.07.002
84. Hraska V, Mitchell ME, Woods RK, Hoffman GM, Kindel SJ, Ginde S. editors. Innominate vein turn-down procedure for failing Fontan circulation. In: Seminars in thoracic and cardiovascular surgery: Pediatric cardiac surgery annual. (2020) Elsevier. p. 34–40
85. Hraska V, Hjortdal VE, Dori Y, Kreutzer C. Innominate vein turn-down procedure: killing two birds with one stone. JTCVS Tech. (2021) 7:253–60. doi: 10.1016/j.xjtc.2021.01.045
86. Doulamis IP, Marathe SP, Piekarski B, Beroukhim RS, Marx GR, Pedro J, et al. Biventricular conversion after Fontan completion: a preliminary experience. J Thorac Cardiovasc Surg. (2022) 163(3):1211–23. doi: 10.1016/j.jtcvs.2021.04.076
87. King G, d’Udekem Y. Commentary: moderate atrioventricular valve regurgitation may be too much to bear for a single ventricle. J Thorac Cardiovasc Surg. (2019) 158(6):1649–51. doi: 10.1016/j.jtcvs.2019.08.063
88. Stephens EH, Dearani JA. Management of the bad atrioventricular valve in Fontan… time for a change. J Thorac Cardiovasc Surg. (2019) 158(6):1643–8. doi: 10.1016/j.jtcvs.2019.08.129
89. Cetta F, Driscoll DJ. Bad atrioventricular valve, bad Fontan: stop creating bad fontans. Washington, DC: American College of Cardiology Foundation (2019).. p. 823–5.
90. Ohye RG, Gomez CA, Goldberg CS, Graves HL, Devaney EJ, Bove EL. Tricuspid valve repair in hypoplastic left heart syndrome. J Thorac Cardiovasc Surg. (2004) 127(2):465–72. doi: 10.1016/j.jtcvs.2003.07.053
91. Oldenburger NJ, Mank A, Etnel J, Takkenberg JJ, Helbing WA. Drug therapy in the prevention of failure of the Fontan circulation: a systematic review. Cardiol Young. (2016) 26(5):842–50. doi: 10.1017/S1047951115002747
92. Yim DL, Jones BO, Alexander PM, d’Udekem Y, Cheung MM. Effect of anti-heart failure therapy on diastolic function in children with single-ventricle circulations. Cardiol Young. (2015) 25(7):1293–9. doi: 10.1017/S1047951114002376
93. Kouatli AA, Garcia JA, Zellers TM, Weinstein EM, Mahony L. Enalapril does not enhance exercise capacity in patients after Fontan procedure. Circulation. (1997) 96(5):1507–12. doi: 10.1161/01.CIR.96.5.1507
94. Ohuchi H, Hasegawa S, Yasuda K, Yamada O, Ono Y, Echigo S. Severely impaired cardiac autonomic nervous activity after the Fontan operation. Circulation. (2001) 104(13):1513–8. doi: 10.1161/hc3801.096326
95. Mori Y, Nakazawa M, Tomimatsu H, Momma K. Long-term effect of angiotensin-converting enzyme inhibitor in volume overloaded heart during growth: a controlled pilot study. J Am Coll Cardiol. (2000) 36(1):270–5. doi: 10.1016/S0735-1097(00)00673-2
96. Seguchi M, Nakazawa M, Momma K. Effect of enalapril on infants and children with congestive heart failure. Cardiol Young. (1992) 2(1):14–9. doi: 10.1017/S1047951100000524
97. Leversha AM, Wilson NJ, Clarkson PM, Calder AL, Ramage MC, Neutze JM. Efficacy and dosage of enalapril in congenital and acquired heart disease. Arch Dis Child. (1994) 70(1):35–9. doi: 10.1136/adc.70.1.35
98. Shaddy RE, Boucek MM, Hsu DT, Boucek RJ, Canter CE, Mahony L, et al. Carvedilol for children and adolescents with heart failure: a randomized controlled trial. JAMA. (2007) 298(10):1171–9. doi: 10.1001/jama.298.10.1171
99. Ringel RE, Peddy SB. Effect of high-dose spironolactone on protein-losing enteropathy in patients with Fontan palliation of complex congenital heart disease. Am J Cardiol. (2003) 91(8):1031. doi: 10.1016/S0002-9149(03)00135-8
100. Okano S, Sugimoto M, Takase M, Iseki K, Kajihama A, Azuma H. Effectiveness of high-dose spironolactone therapy in a patient with recurrent protein-losing enteropathy after the Fontan procedure. Intern Med. (2016) 55(12):1611–4. doi: 10.2169/internalmedicine.55.6303
101. Shabanian R, Shahbaznejad L, Razaghian A, Kiani A, Rahimzadeh M, Seifirad S, et al. Sildenafil and ventriculo-arterial coupling in Fontan-palliated patients: a noninvasive echocardiographic assessment. Pediatr Cardiol. (2013) 34(1):129–34. doi: 10.1007/s00246-012-0400-y
102. Giardini A, Balducci A, Specchia S, Gargiulo G, Bonvicini M, Picchio FM. Effect of sildenafil on haemodynamic response to exercise and exercise capacity in Fontan patients. Eur Heart J. (2008) 29(13):1681–7. doi: 10.1093/eurheartj/ehn215
103. Van De Bruaene A, La Gerche A, Claessen G, De Meester P, Devroe S, Gillijns H, et al. Sildenafil improves exercise hemodynamics in Fontan patients. Circ Cardiovasc Imaging. (2014) 7(2):265–73. doi: 10.1161/CIRCIMAGING.113.001243
104. Hager A, Weber R, Müller J, Hess J. Predictors of sildenafil effects on exercise capacity in adolescents and adults with Fontan circulation. Clin Res Cardiol. (2014) 103(8):641–6. doi: 10.1007/s00392-014-0694-2
105. Goldberg DJ, French B, McBride MG, Marino BS, Mirarchi N, Hanna BD, et al. Impact of oral sildenafil on exercise performance in children and young adults after the Fontan operation: a randomized, double-blind, placebo-controlled, crossover trial. Circulation. (2011) 123(11):1185–93. doi: 10.1161/CIRCULATIONAHA.110.981746
106. Goldberg DJ, French B, Szwast AL, McBride MG, Marino BS, Mirarchi N, et al. Impact of sildenafil on echocardiographic indices of myocardial performance after the Fontan operation. Pediatr Cardiol. (2012) 33(5):689–96. doi: 10.1007/s00246-012-0196-9
107. Goldberg DJ, Zak V, Goldstein BH, Schumacher KR, Rhodes J, Penny DJ, et al. Results of the FUEL trial. Circulation. (2020) 141(8):641–51. doi: 10.1161/CIRCULATIONAHA.119.044352
108. Schuuring MJ, Vis JC, van Dijk AP, van Melle JP, Vliegen HW, Pieper PG, et al. Impact of bosentan on exercise capacity in adults after the Fontan procedure: a randomized controlled trial. Eur J Heart Fail. (2013) 15(6):690–8. doi: 10.1093/eurjhf/hft017
109. Hebert A, Mikkelsen UR, Thilen U, Idorn L, Jensen AS, Nagy E, et al. Bosentan improves exercise capacity in adolescents and adults after Fontan operation: the TEMPO (treatment with endothelin receptor antagonist in Fontan patients, a randomized, placebo-controlled, double-blind study measuring peak oxygen consumption) study. Circulation. (2014) 130(23):2021–30. doi: 10.1161/CIRCULATIONAHA.113.008441
110. Ovaert C, Thijs D, Dewolf D, Ottenkamp J, Dessy H, Moons P, et al. The effect of bosentan in patients with a failing Fontan circulation. Cardiol Young. (2009) 19(4):331–9. doi: 10.1017/S1047951109990023
111. Rhodes J, Ubeda-Tikkanen A, Clair M, Fernandes SM, Graham DA, Milliren CE, et al. Effect of inhaled iloprost on the exercise function of Fontan patients: a demonstration of concept. Int J Cardiol. (2013) 168(3):2435–40. doi: 10.1016/j.ijcard.2013.03.014
112. Haseyama K, Satomi G, Yasukochi S, Matsui H, Harada Y, Uchita S. Pulmonary vasodilation therapy with sildenafil citrate in a patient with plastic bronchitis after the Fontan procedure for hypoplastic left heart syndrome. J Thorac Cardiovasc Surg. (2006) 132(5):1232–3. doi: 10.1016/j.jtcvs.2006.05.067
113. Weingarten AJ, Menachem JN, Smith CA, Frischhertz BP, Book WM. Usefulness of midodrine in protein-losing enteropathy. J Heart Lung Transplant. (2019) 38(7):784–7. doi: 10.1016/j.healun.2019.04.002
114. Scallan JP, Zawieja SD, Castorena-Gonzalez JA, Davis MJ. Lymphatic pumping: mechanics, mechanisms and malfunction. J Physiol (Lond). (2016) 594(20):5749–68. doi: 10.1113/JP272088
115. Schumacher KR, Cools M, Goldstein BH, Ioffe-Dahan V, King K, Gaffney D, et al. Oral budesonide treatment for protein-losing enteropathy in Fontan-palliated patients. Pediatr Cardiol. (2011) 32(7):966–71. doi: 10.1007/s00246-011-0029-2
116. Kewcharoen J, Mekraksakit P, Limpruttidham N, Kanitsoraphan C, Charoenpoonsiri N, Poonsombudlert K, et al. Budesonide for protein losing enteropathy in patients with Fontan circulation: a systematic review and meta-analysis. World J Pediatr Congenit Heart Surg. (2020) 11(1):85–91. doi: 10.1177/2150135119872196
117. Egbe AC, Connolly HM, Khan AR, Niaz T, Said SS, Dearani JA, et al. Outcomes in adult Fontan patients with atrial tachyarrhythmias. Am Heart J. (2017) 186:12–20. doi: 10.1016/j.ahj.2016.12.015
118. Joyce J, O'Leary ET, Mah DY, Harrild DM, Rhodes J. Cardiac resynchronization therapy improves the ventricular function of patients with Fontan physiology. Am Heart J. (2020) 230:82–92. doi: 10.1016/j.ahj.2020.09.018
119. Scheffers LE, Berg L, Ismailova G, Dulfer K, Takkenberg JJ, Helbing WA. Physical exercise training in patients with a Fontan circulation: a systematic review. Eur J Prev Cardiol. (2021) 28(11):1269–78. doi: 10.1177/2047487320942869
120. Cesario D, Clark J, Maisel A. Beneficial effects of intermittent home administration of the inotrope/vasodilator milrinone in patients with end-stage congestive heart failure: a preliminary study. Am Heart J. (1998) 135(1):121–9. doi: 10.1016/S0002-8703(98)70352-7
121. Ryerson LM, Alexander PM, Butt WW, Shann FA, Penny DJ, Shekerdemian LS. Rotating inotrope therapy in a pediatric population with decompensated heart failure. Pediatr Crit Care Med. (2011) 12(1):57–60. doi: 10.1097/PCC.0b013e3181e2a437
122. Berg AM, Snell L, Mahle WT. Home inotropic therapy in children. J Heart Lung Transplant. (2007) 26(5):453–7. doi: 10.1016/j.healun.2007.02.004
123. López-Candales A, Vora T, Gibbons W, Carron C, Simmons P, Schwartz J. Symptomatic improvement in patients treated with intermittent infusion of inotropes: a double-blind placebo controled pilot study. J Med. (2002) 33(1-4):129–46. PMID: 12939113
124. Friedland-Little JM, Gajarski RJ, Schumacher KR. Dopamine as a potential rescue therapy for refractory protein-losing enteropathy in Fontan-palliated patients. Pediatr Transplant. (2017) 21(4):e12925. doi: 10.1111/petr.12925
125. Costello JM, Dunbar-Masterson C, Allan CK, Gauvreau K, Newburger JW, McGowan FX Jr, et al. Impact of empiric nesiritide or milrinone infusion on early postoperative recovery after Fontan surgery: a randomized, double-blind, placebo-controlled trial. Circ Heart Fail. (2014) 7(4):596–604. doi: 10.1161/CIRCHEARTFAILURE.113.001312
126. Ghanayem N, Berger S, Tweddell J. Medical management of the failing Fontan. Pediatr Cardiol. (2007) 28(6):465–71. doi: 10.1007/s00246-007-9007-0
127. Sorensen GK, Ramamoorthy C, Lynn AM, French J, Stevenson JG. Hemodynamic effects of amrinone in children after Fontan surgery. Anesth Analg. (1996) 82(2):241–6.8561320
128. Nakano SJ, Nelson P, Sucharov CC, Miyamoto SD. Myocardial response to milrinone in single right ventricle heart disease. J Pediatr. (2016) 174:199–203. e5. doi: 10.1016/j.jpeds.2016.04.009
129. Elkayam U, Tasissa G, Binanay C, Stevenson LW, Gheorghiade M, Warnica JW, et al. Use and impact of inotropes and vasodilator therapy in hospitalized patients with severe heart failure. Am Heart J. (2007) 153(1):98–104. doi: 10.1016/j.ahj.2006.09.005
130. Weinstein S, Bello R, Pizarro C, Fynn-Thompson F, Kirklin J, Guleserian K, et al. The use of the Berlin Heart EXCOR in patients with functional single ventricle. J Thorac Cardiovasc Surg. (2014) 147(2):697–705. doi: 10.1016/j.jtcvs.2013.10.030
131. Imielski BR, Niebler RA, Kindel SJ, Woods RK. Heartware ventricular assist device implantation in patients with Fontan physiology. Artif Organs. (2017) 41(1):40–6. doi: 10.1111/aor.12852
132. Niebler RA, Ghanayem NS, Shah TK, Bobke ADLR, Zangwill S, Brosig C, et al. Use of a HeartWare ventricular assist device in a patient with failed Fontan circulation. Ann Thorac Surg. (2014) 97(4):e115–6. doi: 10.1016/j.athoracsur.2013.11.075
133. Morales DL, Adachi I, Heinle JS, Fraser CD. A new era: use of an intracorporeal systemic ventricular assist device to support a patient with a failing Fontan circulation. J Thorac Cardiovasc Surg. (2011) 142(3):e138–40. doi: 10.1016/j.jtcvs.2011.05.018
134. Miller JR, Lancaster TS, Callahan C, Abarbanell AM, Eghtesady P. An overview of mechanical circulatory support in single-ventricle patients. Transl Pediatr. (2018) 7(2):151. doi: 10.21037/tp.2018.03.03
135. Cedars A, Kutty S, Danford D, Schumacher K, Auerbach S, Bearl D, et al. Systemic ventricular assist device support in Fontan patients: a report by ACTION. J Heart Lung Transplant. (2021) 40(5):368–76. doi: 10.1016/j.healun.2021.01.011
136. Poh CL, Chiletti R, Zannino D, Brizard C, Konstantinov IE, Horton S, et al. Ventricular assist device support in patients with single ventricles: the Melbourne experience. Interact Cardiovasc Thorac Surg. (2017) 25(2):310–6. doi: 10.1093/icvts/ivx066
137. Almond CS, Morales DL, Blackstone EH, Turrentine MW, Imamura M, Massicotte MP, et al. Berlin Heart EXCOR pediatric ventricular assist device for bridge to heart transplantation in US children. Circulation. (2013) 127(16):1702–11. doi: 10.1161/CIRCULATIONAHA.112.000685
138. Chen S, Rosenthal DN, Murray J, Dykes JC, Almond CS, Yarlagadda VV, et al. Bridge to transplant with ventricular assist device support in pediatric patients with single ventricle heart disease. ASAIO J. (2020) 66(2):205–11. doi: 10.1097/MAT.0000000000000983
139. O’Connor MJ, Lorts A, Davies RR, Fynn-Thompson F, Joong A, Maeda K, et al. Early experience with the HeartMate 3 continuous-flow ventricular assist device in pediatric patients and patients with congenital heart disease: a multicenter registry analysis. J Heart Lung Transplant. (2020) 39(6):573–9. doi: 10.1016/j.healun.2020.02.007
140. Rossano JW, VanderPluym CJ, Peng DM, Hollander SA, Maeda K, Adachi I, et al. Fifth annual pediatric interagency registry for mechanical circulatory support (Pedimacs) report. Ann Thorac Surg. (2021) 112(6):1763–74. doi: 10.1016/j.athoracsur.2021.10.001
141. Nandi D, Miller KD, Bober CM, Rosenthal TM, Montenegro LM, Rossano JW, et al. Systemic atrioventricular valve excision and ventricular assist devices in pediatric patients. Ann Thorac Surg. (2018) 105(1):170–4. doi: 10.1016/j.athoracsur.2017.05.038
142. Nathan M, Baird C, Fynn-Thompson F, Almond C, Thiagarajan R, Laussen P, et al. Successful implantation of a Berlin heart biventricular assist device in a failing single ventricle. J Thorac Cardiovasc Surg. (2006) 131(6):1407–8. doi: 10.1016/j.jtcvs.2006.02.015
143. Rossano JW, Goldberg DJ, Fuller S, Ravishankar C, Montenegro LM, Gaynor JW. Successful use of the total artificial heart in the failing Fontan circulation. Ann Thorac Surg. (2014) 97(4):1438–40. doi: 10.1016/j.athoracsur.2013.06.120
144. Prêtre R, Häussler A, Bettex D, Genoni M. Right-sided univentricular cardiac assistance in a failing Fontan circulation. Ann Thorac Surg. (2008) 86(3):1018–20. doi: 10.1016/j.athoracsur.2008.03.003
145. Coffman ZJ, Bandisode VM, Kavarana MN, Buckley JR. Utilization of an Abiomed Impella Device as a rescue therapy for acute ventricular failure in a Fontan patient. World J Pediatr Congenit Heart Surg. (2019) 10(4):518–9. doi: 10.1177/2150135119847147
146. Morray BH, Dimas VV, Lim S, Balzer DT, Parekh DR, Van Mieghem NM, et al. Circulatory support using the Impella device in Fontan patients with systemic ventricular dysfunction: a multicenter experience. Catheter Cardiovasc Interv. (2017) 90(1):118–23. doi: 10.1002/ccd.26885
147. Bernstein D, Naftel D, Chin C, Addonizio L, Gamberg P, Blume E, et al. Outcome of listing for cardiac transplantation for failed Fontan: a multi-institutional study. Circulation. (2006) 114(4):273–80. doi: 10.1161/CIRCULATIONAHA.105.548016
148. Alshawabkeh LI, Hu N, Carter KD, Opotowsky AR, Light-McGroary K, Cavanaugh JE, et al. Wait-list outcomes for adults with congenital heart disease listed for heart transplantation in the US. J Am Coll Cardiol. (2016) 68(9):908–17. doi: 10.1016/j.jacc.2016.05.082
149. Carey JA, Hamilton JL, Hilton CJ, Dark JH, Forty J, Parry G, et al. Orthotopic cardiac transplantation for the failing Fontan circulation. Eur J Cardiothorac Surg. (1998) 14(1):7–14. doi: 10.1016/S1010-7940(98)00130-4
150. Gamba A, Merlo M, Fiocchi R, Terzi A, Mammana C, Sebastiani R, et al. Heart transplantation in patients with previous Fontan operations. J Thorac Cardiovasc Surg. (2004) 127(2):555–62. doi: 10.1016/j.jtcvs.2003.08.016
151. Simpson KE, Pruitt E, Kirklin JK, Naftel DC, Singh RK, Edens RE, et al. Fontan patient survival after pediatric heart transplantation has improved in the current era. Ann Thorac Surg. (2017) 103(4):1315–20. doi: 10.1016/j.athoracsur.2016.08.110
152. Michielon G, Parisi F, Di Carlo D, Squitieri C, Carotti A, Buratta M, et al. Orthotopic heart transplantation for failing single ventricle physiology. Eur J Cardiothorac Surg. (2003) 24(4):502–10. doi: 10.1016/S1010-7940(03)00342-7
153. Lamour JM, Kanter KR, Naftel DC, Chrisant MR, Morrow WR, Clemson BS, et al. The effect of age, diagnosis, and previous surgery in children and adults undergoing heart transplantation for congenital heart disease. J Am Coll Cardiol. (2009) 54(2):160–5. doi: 10.1016/j.jacc.2009.04.020
154. Dipchand AI, Edwards LB, Kucheryavaya AY, Benden C, Dobbels F, Levvey BJ, et al. The registry of the International Society for Heart and Lung Transplantation: seventeenth official pediatric heart transplantation report—2014; focus theme: retransplantation. J Heart Lung Transplant. (2014) 33(10):985–95. doi: 10.1016/j.healun.2014.08.002
155. Schumacher KR, Yu S, Butts R, Castleberry C, Chen S, Edens E, et al. Fontan-associated protein-losing enteropathy and post–heart transplant outcomes: a multicenter study. J Heart Lung Transplant. (2019) 38(1):17–25. doi: 10.1016/j.healun.2018.09.024
156. Bryant R 3rd, Rizwan R, Zafar F, Shah SA, Chin C, Tweddell JS, et al. Contemporary outcomes of combined heart-liver transplant in patients with congenital heart disease. Transplantation. (2018) 102(2):e67–e73. doi: 10.1097/TP.0000000000001978
157. Sganga D, Hollander SA, Vaikunth S, Haeffele C, Bensen R, Navaratnam M, et al. Comparison of combined heart–liver vs heart-only transplantation in pediatric and young adult Fontan recipients. J Heart Lung Transplant. (2021) 40(4):298–306. doi: 10.1016/j.healun.2020.12.008
Keywords: Fontan, heart failure, single ventricle, medications, ventricular assist device, Fontan failure
Citation: Kamsheh AM, O’Connor MJ and Rossano JW (2022) Management of circulatory failure after Fontan surgery. Front. Pediatr. 10:1020984. doi: 10.3389/fped.2022.1020984
Received: 16 August 2022; Accepted: 18 October 2022;
Published: 8 November 2022.
Edited by:
Milan Prsa, Centre Hospitalier Universitaire Vaudois (CHUV), SwitzerlandReviewed by:
Hideo Ohuchi, National Cerebral and Cardiovascular Center, Japan© 2022 Kamsheh, O'Connor and Rossano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joseph Rossano cm9zc2Fub2pAZW1haWwuY2hvcC5lZHU=
Specialty Section: This article was submitted to Pediatric Cardiology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.