 Francesco La Torre1
Francesco La Torre1 Gerolmina Calabrese2Katia Signorile1Francesca Bizzoco1
Gerolmina Calabrese2Katia Signorile1Francesca Bizzoco1 Carla Mastrorilli1Antonella Strippoli1Doriana Amato1Francesco Carella1Ugo Vairo3
Carla Mastrorilli1Antonella Strippoli1Doriana Amato1Francesco Carella1Ugo Vairo3 Paola Giordano4
Paola Giordano4 Leonardo Milella2
Leonardo Milella2 Fabio Cardinale1
Fabio Cardinale1
- 1Department of Pediatrics, Giovanni XXIII Pediatric Hospital, University of Bari, Bari, Italy
- 2Pediatric Intensive Care Unit, Giovanni XXIII Pediatric Hospital, Bari, Italy
- 3Pediatric Cardiology Unit, Giovanni XXIII Pediatric Hospital, Bari, Italy
- 4Department of Interdisciplinary Medicine, Pediatric Section, University of Bari, Bari, Italy
Multisystem inflammatory syndrome in children (MIS-C) is a newly identified clinical entity still not very well known in terms of epidemiology, pathogenesis, and long-term outcome. Pulmonary involvement with acute respiratory failure is an unusual life-threatening complication of MIS-C, often a reason for admission to the pediatric intensive care unit (PICU) and the use of mechanical ventilation. We present a case of a 7-year-old male patient, previously healthy, hospitalized for MIS-C, treated with intravenous immunoglobulins (IVIG), high dose methylprednisolone, and anakinra. After 2 days of the aforementioned therapy, the patient presented with hypoxia (SatO2: 85% in ambient air room) and breathing difficulties. A chest computed tomography (CT) scan showed the presence of multiple bilateral basal parenchymal thickening and small basal pleural effusion and an arterial blood gas analysis revealed severe hypoxia (PaO2/FiO2 ratio, 170 mmHg). Because of a worsening of respiratory distress, the patient was transferred to the PICU, where invasive mechanical ventilation and a continuous infusion of anakinra (12 mg/kg/day) were started. An echocardiogram was performed, which showed an increase in pulmonary pressure (40 mmHg) with normal heart ejection fraction (55%), and the hypothesis of pulmonary vasculitis involving the pulmonary arterioles was made. Therefore, therapy with sildenafil (0.15 mg/kg/day) was promptly set up, with an immediate improvement of the clinical picture of respiratory failure, reduction of pulmonary pressure (23 mmHg), and subsequent extubation at 36 h with a regular clinical course until discharge. As far as we know, our case represents the first report of pulmonary vasculitis in an MIS-C patient. The use of sildenafil and high-dose continuous anakinra may represent a rescue therapy in cases of MIS-C with pulmonary vasculitis or with difficulty in extubation, allowing a short-term hospitalization in intensive care and improving the long-term outcome in these patients.
Introduction
Since the first phase of the COVID-19 outbreak, a new childhood multi-inflammatory syndrome temporally linked with SARS-CoV-2 infection has been reported worldwide. It has some similarities with Kawasaki disease (KD) and toxic shock syndrome (TSS) (1, 2). This condition has been named pediatric inflammatory multisystem syndrome temporally associated to SARS-CoV-2 infection (PIMS-TS) or multisystem inflammatory syndrome associated with coronavirus disease 2019 (MIS-C) (3–7). It typically displays 2–6 weeks after SARS-Cov-2 infection and has some overlapping features with KD, with a range of clinical presentations including mucocutaneous, respiratory, gastrointestinal, neurological, and cardiac symptoms. Like KD, no pathognomonic clinical findings or diagnostic tests exist. Unlike KD, however, MIS-C has been reported to predominantly affect adolescents and children aged older than 5 years and to be associated more frequently with cardiovascular (mainly myocarditis), and gastrointestinal involvement (1, 5, 6, 8, 9). The current definition of MIS-C, established by the World Health Organization in May 2020, refers to an individual aged 0–19 years, presenting with a fever for 3 days or longer, plus at least two of the following symptoms: rash; conjunctivitis; mucocutaneous inflammation; hypotension or shock; cardiac involvement; coagulopathy; and acute gastrointestinal symptoms. Laboratory evidence of increased inflammatory markers, such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), or procalcitonin plus positive evidence of recent COVID-19 infection (by oronasal swab-PCR, serology, or antigen test) or likely recent contact, are required (10). While the underlying pathophysiology of MIS-C is currently under investigation, both the innate and adaptive immune response are thought to be strongly upregulated (11–13). One of the most intriguing theories hypothesizes that the SARS-CoV-2 spike protein can act as a “superantigen,” activating both T- and B-cells, leading to the hyperinflammatory state and a subsequent cytokine storm, similar to toxic shock syndrome (TSS) induced by the staphylococcal endotoxin B (14). Furthermore, it has been observed that patients affected by MIS-C develop vasculitis with endothelial damage, as shown by high levels of MCP-1 and VEGF-A, followed by an increase in pANCA (15). Among non-specific symptoms, severe complications including cardiovascular shock and multi-organ failure appear in most severe cases of MIS-C (16–18). Vasculitis and microthrombosis, particularly at the pulmonary level, were observed by necroscopy in some patients (19), but a case report of pulmonary vasculitis has never been documented. On the other hand, MIS-C shares some clinical features with other pediatric inflammatory multisystemic syndromes, such as KD, TSS, and macrophage activation syndrome (MAS), typically associated with endothelial damage and systemic vasculitis (20–22). Current practices and published guidelines for the treatment of MIS-C support the use of intravenous immunoglobulin (IVIG) and high-dose corticosteroids as the cornerstone of therapy (3, 4, 20, 23–28), in addition to antithrombotic prophylaxis. Treatment algorithms generally recommend biologic agents as second-line medication options after initial treatment with IVIG and steroids (22, 27, 29). Anakinra is a recombinant human interleukin-1 receptor antagonist that has been previously shown to be effective with limited side effects in patients with KD (29). Many studies have shown a similar efficacy of anakinra in severe cases of MIS-C, especially in patients with a clinical course complicated by severe myocarditis, shock, and a poor response to IVIG and steroid treatment (30–33). In two large cohorts, anakinra was successfully used in 24 of 186 and 8 of 183 patients, demonstrating an overt efficacy in cases of MIS-C with severe cardiac involvement (9, 34). We present a case of MIS-C complicated by pulmonary vasculitis successfully treated with sildenafil and high doses of anakinra.
Case report
A previously healthy 7-year-old male patient was admitted to our Pediatric Department, complaining of unremitting fever above 39 °C for 5 days, fatigue, headache, and acute abdominal pain, unresponsive to non-steroidal anti-inflammatory drugs ,and antibiotic treatment with amoxicillin-clavulanate. At admission on physical examination, he presented with bilateral non-exudative conjunctivitis, skin rash on the trunk and upper limbs, and neck rigidity with some sign of meningism. He had had a pauci-symptomatic SARS-CoV-2 infection approximately 4 weeks before, characterized by 2 days of fever, asthenia, and headache. The infection had been ascertained by a positive oronasal swab for SARS-CoV-2. Laboratory findings showed marked elevation of CRP (275 mg/L) and ESR (66 mm/1th h), but also of ferritin (556 mg/L) and brain natriuretic peptide (pro-BNP; 3408 pg/ml). Marked lymphopenia (440/mmc) and hypoalbuminemia (23 g/L) were also found at admission. A molecular swab for SARS-CoV-2 was negative. The work-up excluded Epstein Barr virus, cytomegalovirus, parvovirus B19, adenovirus, and HIV infection. The echocardiography performed when he presented to the pediatric emergency unit showed signs of endocarditis (mild aortic and mitral regurgitation) with normal contractility of the myocardium and normal pulmonary pressure (26 mmHg). The abdominal ultrasound showed a thin layer of fluid among the intestinal loops and the chest x-ray showed a homogeneous parenchymal thickening in the left paracardiac basal area with small left basal pleural effusion. In view of his medical history, clinical examination, and blood and instrumental tests, a diagnosis of MIS-C related to COVID-19 infection was made. According to guidelines, IVIG at a dose of 2 g/kg associated with a high dose of metilprednisolone at a dose of 30 mg/kg were started (Table 1). Subcutaneous thromboprophylaxis with low-molecular weight heparin (LMWH) at a dose of 100 UI/kg was also initiated (Table 1). After the third bolus of high-dose corticosteroids, his fever and neurological symptoms persisted, together with a persistent elevation of CRP (135 mg/L). Therefore, intravenous anakinra (a 2 mg/kg/dose every 6 h) was started while intravenous methylprednisolone (1 mg/kg b.i.d.) was continued (Tables 1 and 2), showing a rapid response, with the disappearance of the fever and skin rash and the reduction of CRP (60 mg/L) and pro-BNP (546 pg/ml). After 2 days, he suddenly presented with progressive dyspnea, increased labored breathing, and hypoxia (SatO2: 85% in ambient air room), without any other associated symptoms. The delivery of O2 by humidified high-flow nasal cannula (HFNC) was started with a FiO2 50%. A chest CT scan was performed, showing multiple basal parenchymal thickening with small basal pleural effusion (Figure 1). An arterial blood gas analysis showed severe hypoxia (PaO2, 56 mmHg; PaO2/FiO2 ratio, 170 mmHg). The blood tests showed new slowly increasing inflammatory markers (CRP 113 mg/L, ESR 68 mm/1th h). Because of the increased work of breathing and persistent altered gas exchange, the patient was transferred to the pediatric intensive care unit (PICU), and then put on invasive mechanical ventilation. Administration of anti-IL-1 was modified and a continuous infusion of high-dose anakinra (12 mg/kg/day) was started (Tables 1 and 2). Echocardiography revealed increased pulmonary pressure (40 mmHg) with normal heart ejection fraction (55%). These results confirmed the hypothesis of ongoing pulmonary vasculitis involving pulmonary arterioles. Therefore, intravenous sildenafil at a dose of 0.15 mg/kg/day was started (35, 36) (Table 1), with a progressive reduction of pulmonary pressure (23 mmHg) and resolution of the clinical picture of respiratory failure. After 36 h from the start of the treatment, the patient’s clinical condition as well as laboratory parameters remarkably improved, and he was extubated and again transferred to our department. The treatment was well tolerated and after 3 days the CRP fell in the normal range, sildenafil was stopped, and the biologic treatment was escalated, taking off one dose of anakinra every 3 days, up to discontinuation (Table 1). At discharge, echocardiography revealed signs of previous cardiac involvement with persistent mild mitral regurgitation and total regression of aortic regurgitation, and chest x-ray showed a resolution of parenchymal thickening and pleural effusion. The treatment with LMWH was shifted to oral cardioaspirin at a dose of 5 mg/kg/day (max 100 mg/day) (Table 1). After 2 months of follow-up, the clinical examination was normal, and the blood test and cardiologic assessment with echocardiography also normalized; therefore, the cardioaspirin therapy was stopped.
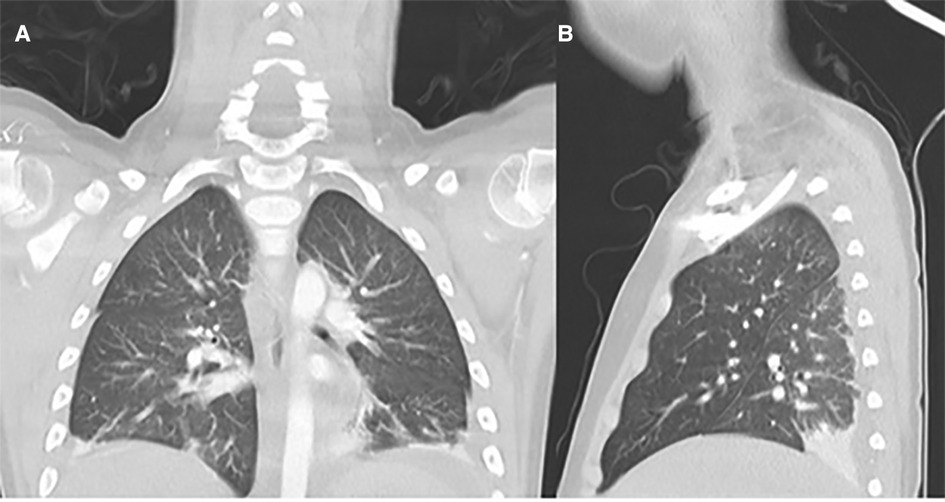
Figure 1. Chest computed tomography revealed multiple basal parenchymal thickening with small basal pleural effusion without signs of pulmonary embolism: (A) antero-posterior view; (B) latero-lateral view.
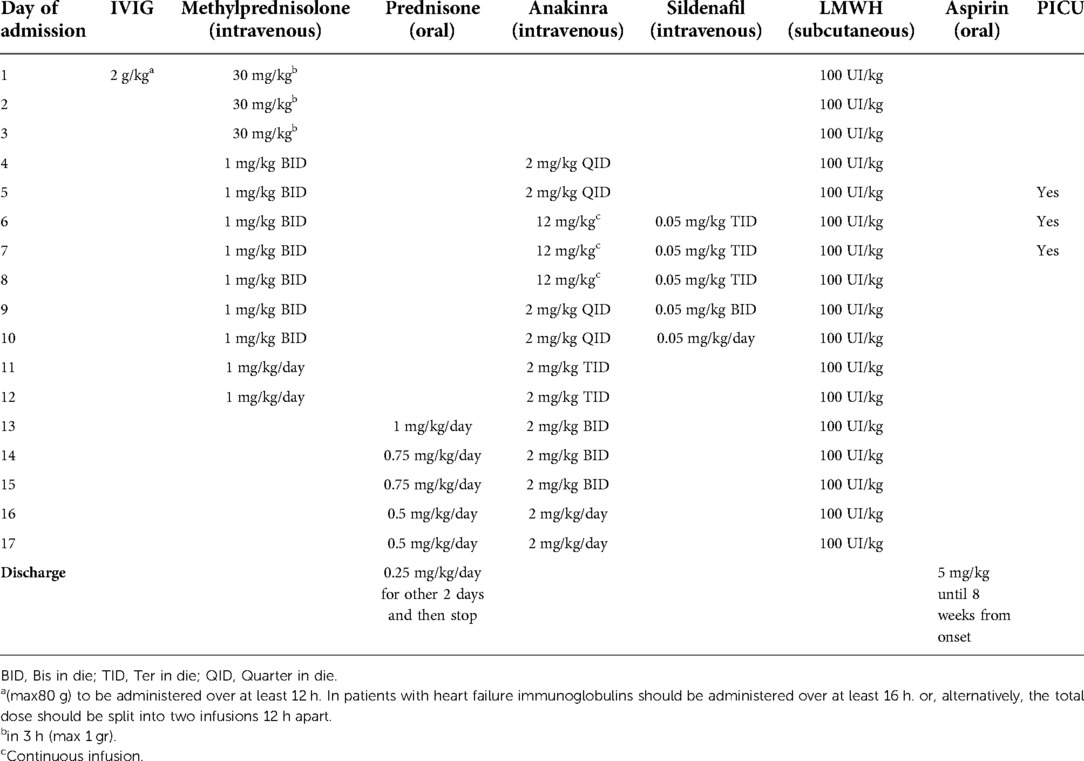
Table 1. Summary of the immunomodulatory and thromboprophylaxis therapy administered to our patient affected by MIS-C complicated with pulmonary vasculitis.
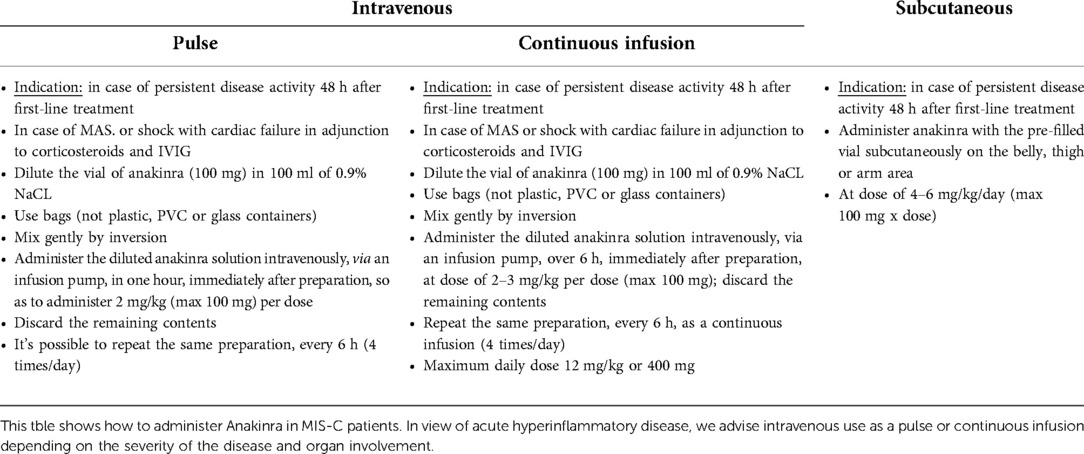
Table 2. Different modalities of Anakinra administration in MIS-C patients.
Discussion
MIS-C is a post-infectious hyperinflammatory syndrome caused by a dysregulated immune response to SARS-CoV-2 infection with severe morbidity and mortality (15, 19–22). Diffuse vascular-endothelial damage is likely to play a major role in cases with severe cardiac and neurological involvement (15, 19–22). The strong association between COVID-19 and coagulopathy suggests that multiple molecular pathways are involved and dysregulated through the disease progression, contributing to the development of thrombosis; this is true also for MIS-C (37). Endothelial dysfunction and barrier disruption lead to immune cell infiltration, and proinflammatory cytokine production, as well as thrombosis (38). MIS-C seems to have specific effects on the coagulation profile leading to hypercoagulability and a thrombogenic state; in particular, complement activation has been hypothesized as a favoring factor in thrombosis development (39). Recent studies in children have pointed to an increase in endothelial dysfunction markers in MIS-C, with a rise in soluble C5b-9 (which represents the activated product of the terminal complement cascade) and altered red blood cell morphology (39, 40). In patients with MIS-C, high levels of fibrinogen and D-dimers increase the likelihood of a thrombotic state (37). As far as we know, our case represents the first report of pulmonary arterial hypertension (PAH) likely due to pulmonary vasculitis in a pediatric patient with MIS-C. We examined several explanations for the PAH in our young patient. First, we considered a pulmonary embolism, which was ruled out by the CT scan. In addition, the echocardiographic assessment was negative for underlying heart conditions or cardiac failure. Therefore, we considered the diagnosis of pulmonary vasculitis as the only possibility of the sudden dyspnea associated with an increase of PAH after the exclusion of cardiac and other pulmonary causes, as occurring in some cases of KD with pulmonary involvement (36). Therefore, we administered sildenafil, a type 5 phosphodiesterase inhibitor, known to induce vasodilation, particularly in the pulmonary arterial district, and to inhibit endothelial proliferation. This therapy has already been shown to be effective in treating children with PAH in different conditions (35). We believe that in our case the association of sildenafil with high doses of anakinra was decisive in preventing the progression of the disease. In this regard, according to different international societies of pediatrics and rheumatology, anakinra would be considered in MIS-C patients refractory to first-line medications (IVIG and corticosteroids), or in cases complicated by MAS or shock (3, 4, 23, 27, 33). However, the effective control of the hyperinflammatory condition can depend on a window of opportunity that the step-up approach does not always allow respect. We believe that in our case, the delay of diagnosis (admission to the hospital on the 5th day of fever) along with the decision of starting the therapy with IVIG and high-dose steroids alone, without anakinra, may have played a role in the suboptimal control of symptoms, paving the way to the development of pulmonary vasculitis requiring admission to the PICU. This decision was based on recommendations from guidelines to start anakinra in MIS-C in patients without cardiac failure or MAS only in case of uncontrolled disease at 48 h after first-line treatments (3, 4, 23, 27). However, neurological involvement with meningoencephalitis and pulmonary involvement with acute respiratory failure are determining elements for admission to the PICU (8, 9, 18). In our report, the worsening of the cardio-respiratory compromise was decisive for PICU admission and prompted us to introduce a second-line treatment with high-dose intravenous anakinra and sildenafil. In our opinion, the presence of neurological involvement with overt meningism signs should be considered as criteria for starting a more aggressive treatment with anakinra, using this drug as a first-line approach. In our case, such therapy on the second day of hospitalization, after the failure of the first day of IVIG and infusion of high-dose corticosteroids, could have been started. This would have made it possible to anticipate the use of anakinra by 48 h, probably within the window of opportunity to avoid the need for intensive care and the possible complications of the hyperinflammatory picture. However, sildenafil and high doses of intravenous anakinra treatments allowed the patient to have a short-term hospitalization in the PICU and a total normalization of the neurological, cardiological, and pulmonary picture and normal long-term outcome.
Conclusion
As far as we know, our case represents the first report in pediatric literature of pulmonary vasculitis in MIS-C patients. One limitation of our report is that no pulmonary biopsy was performed to confirm our hypothesis of pulmonary vasculitis as a cause of severe respiratory distress and altered gas exchange requiring invasive mechanical ventilation. On the other hand, the rapid improvement registered in our patient with sildenafil and high doses of anakinra made the biopsy unethical to perform. We believe that the use of sildenafil and high-dose intravenous anakinra may represent an effective rescue therapy in severe cases of MIS-C with likely pulmonary vascular involvement, allowing a more rapid discharge from PICU and possibly improving the long-term outcome in these patients.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Review Board of Bari, Italy. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
FLT, PG, and FC provided the concept for the study and were major contributors to the manuscript revision. GC, AS, DA, FC, UV, and LM were involved in the patient care and collected the data regarding the patient's history and clinical course, as well as the trends in vital parameters. FLT, KS, FB, and CM collected clinical data, reviewed the literature, and drafted the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by Springer Healthcare Italia srl. for open access publication fees
Acknowledgments
The authors thank all medical and nursing staff of the Pediatric Department and of the Pediatric Intensive Care Unit of the Giovanni XXIII Pediatric Hospital of Bari for their help.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cattalini M, Della Paolera S, Zunica F, Bracaglia C, Giangreco M, Verdoni L, et al. Defining Kawasaki disease and pediatric inflammatory multisystem syndrome-temporally associated to SARS-CoV-2 infection during SARS-CoV-2 epidemic in Italy: results from a national, multicenter survey. Pediatr Rheumatol Online J. (2021) 19(1):29. doi: 10.1186/s12969-021-00511-7
2. Kıymet E, Böncüoğlu E, Şahinkaya Ş, Cem E, Çelebi MY, Düzgöl M, et al. A comparative study of children with MIS-C between admitted to the pediatric intensive care unit and pediatric ward: a one-year retrospective study. J Trop Pediatr. (2021) 67(6):fmab104. doi: 10.1093/tropej/fmab104
3. Henderson LA, Canna SW, Friedman KG, Gorelik M, Lapidus SK, Bassiri H, et al. American College of rheumatology clinical guidance for multisystem infammatory syndrome in children associated with SARS-CoV-2 and hyperinfammation in pediatric COVID-19: version 1. Arthritis Rheumatol. (2020) 72(11):1791–805. doi: 10.1002/art.41454
4. Henderson LA, Canna SW, Friedman KG, Gorelik M, Lapidus SK, Bassiri H, et al. American College of rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: version 2. Arthritis Rheumatol. (2021) 73(4):e13–29. doi: 10.1002/art.41616
5. Nakra NA, Blumberg DA, Herrera-Guerra A, Lakshminrusimha S. Multi-system inflammatory syndrome in children (MIS-C) following SARS-CoV-2 infection: review of clinical presentation, Hypothetical Pathog Proposed Management. Children (Basel). (2020) 7(7):69. doi: 10.3390/children7070069
6. Radia T, Williams N, Agrawal P, Harman K, Weale J, Cook J, et al. Multi-system inflammatory syndrome in children & adolescents (MIS-C): a systematic review of clinical features and presentation. PaediatrRespir Rev. (2020) 38:51–7. doi: 10.1016/j.prrv.2020.08.001
7. Schlapbach LJ, Andre MC, Grazioli S, Schöbi N, Ritz N, Aebi C, et al. Best practice recommendations for the diagnosis and management of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS; multisystem inflammatory syndrome in children. MIS-C) in Switzerland. Front Pediatr. (2021) 9:667507. doi: 10.3389/fped.2021.667507
8. Rafferty MS, Burrows H, Joseph JP, Leveille J, Nihtianova S, Amirian ES. Multisystem inflammatory syndrome in children (MIS-C) and the coronavirus pandemic: current knowledge and implications for public health. J Infect Public Health. (2021) 14(4):484–94. doi: 10.1016/j.jiph.2021.01.008
9. Feldstein LR, Rose EB, Horwitz SM, Collins JP, Newhams MM, Son MBF, et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N Engl J Med. (2020) 383(4):334–46. doi: 10.1056/NEJMoa2021680
10. World Health Organization. Multisystem inflammatory syndrome in children and adolescents with COVID-19. https://www.who.int/publications/i/item/multisystem-inflammatory-syndrome-in-children-and-adolescentswith-covid-19 [Accessed June 16, 2020] (2020).
11. Blatz AM, Randolph AG. Severe COVID-19 and multisystem inflammatory syndrome in children in children and adolescents. Crit Care Clin. (2022) 38(3):571–86. doi: 10.1016/j.ccc.2022.01.005
12. Vella LA, Giles JR, Baxter AE, Oldridge DA, Diorio C, Kuri-Cervantes L, et al. Deep immune profiling of MIS-C demonstrates marked but transient immune activation compared to adult and pediatric COVID-19. SciImmunol. (2021) 6(57):eabf7570. doi: 10.1126/sciimmunol.abf7570
13. McMurray JC, May JW, Cunningham MW, Jones OY. Multisystem inflammatory syndrome in children (MIS-C), a post-viral myocarditis and systemic vasculitis-A critical review of its pathogenesis and treatment. Front Pediatr. (2020) 8:626182. doi: 10.3389/fped.2020.626182
14. LaRovere KL, Riggs BJ, Poussaint TY, Young CC, Newhams MM, Maamari M, et al. Neurologic involvement in children and adolescents hospitalized in the United States for COVID-19 or multisystem inflammatory syndrome. JAMA Neurol. (2021) 78(5):536–47. doi: 10.1001/jamaneurol.2021.0504
15. Gelzo M, Giannattasio A, Maglione M, Muzzica S, D'Anna C, Scialò F, et al. Biomarkers of endothelial damage in distinct phases of multisystem inflammatory syndrome in children. Metabolites. (2022) 12(8):680. doi: 10.3390/metabo12080680
16. Levin M. Childhood multisystem inflammatory syndrome—a new challenge in the pandemic. N Engl J Med. (2020) 383(4):393–5. doi: 10.1056/NEJMe2023158
17. Belhadjer Z, Méot M, Bajolle F, Khraiche D, Legendre A, Abakka S, et al. Acute heart failure in multisystem inflammatory syndrome in children in the context of global SARS-CoV-2 pandemic. Circulation. (2020) 142(5):429–36. doi: 10.1161/CIRCULATIONAHA.120.048360
18. Feldstein LR, Tenforde MW, Friedman KG, Newhams M, Rose EB, Dapul H, et al. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA. (2021) 325(11):1074–87. doi: 10.1001/jama.2021.2091
19. Duarte-Neto AN, Caldini EG, Gomes-Gouvêa MS, Kanamura CT, de Almeida Monteiro RA, Ferranti JF, et al. An autopsy study of the spectrum of severe COVID-19 in children: from SARS to different phenotypes of MIS-C. EclinicalMedicine. (2021) 35:100850. doi: 10.1016/j.eclinm.2021.100850
20. Toubiana J, Poirault C, Corsia A, Bajolle F, Fourgeaud J, Angoulvant F, et al. Kawasaki-like multisystem inflammatory syndrome in children during the COVID-19 pandemic in Paris, France: prospective observational study. Br Med J. (2020) 369:m2094. doi: 10.1136/bmj.m2094
21. Capone CA, Subramony A, Sweberg T, Schneider J, Shah S, Rubin L, et al. Characteristics, cardiac involvement, and outcomes of multisystem inflammatory syndrome of childhood associated with severe acute respiratory syndrome coronavirus 2 infection. J Pediatr. (2020) 224:141–5. doi: 10.1016/j.jpeds.2020.06.044
22. Pouletty M, Borocco C, Ouldali N, Caseris M, Basmaci R, Lachaume N, et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): a multicentre cohort. Ann Rheum Dis. (2020) 79(8):999–1006. doi: 10.1136/annrheumdis-2020-217960
23. Mahmoud S, El-Kalliny M, Kotby A, El-Ganzoury M, Fouda E, Ibrahim H. Treatment of MIS-C in children and adolescents. CurrPediatrRep. (2022) 10(1):1–10. doi: 10.1007/s40124-021-00259-4
24. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA. (2020) 323(13):1239–42. doi: 10.1001/jama.2020.2648
25. Whittaker E, Bamford A, Kenny J, Kaforou M, Jones CE, Shah P, et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA. (2020) 324(3):259–69. doi: 10.1001/jama.2020.10369
26. Jiang L, Tang K, Levin M, Irfan O, Morris SK, Wilson K, et al. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect Dis. (2020) 20(11):e276–88. doi: 10.1016/S1473-3099(20)30651-4
27. Cattalini M, Taddio A, Bracaglia C, Cimaz R, Paolera SD, Filocamo G, et al. Rheumatology study group of the Italian society of pediatrics. Childhood multisystem inflammatory syndrome associated with COVID-19 (MIS-C): a diagnostic and treatment guidance from the rheumatology study group of the Italian society of pediatrics. Ital J Pediatr. (2021) 47(1):24. doi: 10.1186/s13052-021-00980-2
28. Felsenstein S, Willis E, Lythgoe H, McCann L, Cleary A, Mahmood K, et al. Presentation, treatment response and short-term outcomes in paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 (PIMS-TS). J Clin Med. (2020) 9(10):3293. doi: 10.3390/jcm9103293
29. Kone-Paut I, Cimaz R, Herberg J, Bates O, Carbasse A, Saulnier JP, et al. The use of interleukin 1 receptor antagonist (anakinra) in Kawasaki disease: a retrospective cases series. Autoimmun Rev. (2018) 17(8):768–74. doi: 10.1016/j.autrev.2018.01.024
30. Reiff DD, Cron RQ. Who would have predicted multisystem inflammatory syndrome in children? Curr Rheumatol Rep. (2022) 24(1):1–11. doi: 10.1007/s11926-022-01056-8
31. Mastrolia MV, Marrani E, Calabri GB, L'Erario M, Maccora I, Favilli S, et al. Fast recovery of cardiac function in PIMS-TS patients early using intravenous anti-IL-1 treatment. Crit Care. (2021) 25(1):131. doi: 10.1186/s13054-021-03548-y
32. Fouriki A, Fougère Y, De Camaret C, Blanchard Rohner G, Grazioli S, Wagner N, et al. Case report: case series of children with multisystem inflammatory syndrome following SARS-CoV-2 infection in Switzerland. Front Pediatr. (2021) 8:594127. doi: 10.3389/fped.2020.594127
33. Della Paolera S, Valencic E, Piscianz E, Moressa V, Tommasini A, Sagredini R, et al. Case report: use of anakinra in multisystem inflammatory syndrome during COVID-19 pandemic. Front Pediatr. (2021) 8:624248. doi: 10.3389/fped.2020.624248
34. Bautista-Rodriguez C, Sanchez-de-Toledo J, Clark BC, Herberg J, Bajolle F, Randanne PC, et al. Multisystem inflammatory syndrome in children: an international survey. Pediatrics. (2021) 147(2):e2020024554. doi: 10.1542/peds.2020-024554
35. Simonca L, Tulloh R. Sildenafil in infants and children. Children (Basel). (2017) 4(7):60. doi: 10.3390/children4070060
36. Nicholson GT, Samai C, Kanaan U. Pulmonary hypertension in Kawasaki disease. Pediatr Cardiol. (2013) 34(8):1966–8. doi: 10.1007/s00246-012-0510-6
37. Trapani S, Rubino C, Lasagni D, Pegoraro F, Resti M, Simonini G, et al. Thromboembolic complications in children with COVID-19 and MIS-C: a narrative review. Front Pediatr. (2022) 10:944743. doi: 10.3389/fped.2022.944743
38. Higashikuni Y, Liu W, Obana T, Sata M. Pathogenic basis of thromboinflammation and endothelial injury in COVID-19: current findings and therapeutic implications. Int J Mol Sci. (2021) 22(21):12080. doi: 10.3390/ijms222112081
39. Diorio C, McNerney KO, Lambert M, Paessler M, Anderson EM, Henrickson SE, et al. Evidence of thrombotic microangiopathy in children with SARS-CoV2 across the spectrum of clinical presentations. Blood Adv. (2020) 4:6051–63. doi: 10.1182/bloodadvances.2020003471
Keywords: anakinra, children, COVID-19, MIS-C, multisystem inflammatory syndrome in children, pulmonary hypertension, pulmonary vasculitis, sildenafil
Citation: La Torre F, Calabrese G, Signorile K, Bizzoco F, Mastrorilli C, Strippoli A, Amato D, Carella F, Vairo U, Giordano P, Milella L and Cardinale F (2023) Efficacy of sildenafil and high-dose anakinra in an MIS-C patient with pulmonary vasculitis: A case report. Front. Pediatr. 10:1015617. doi: 10.3389/fped.2022.1015617
Received: 9 August 2022; Accepted: 13 October 2022;
Published: 4 January 2023.
Edited by:
Vahid Ziaee, Tehran University of Medical Sciences, IranReviewed by:
Samar Magboul, Hamad Medical Corporation, QatarAmitabh Singh, Vardhman Mahavir Medical College and Safdarjung Hospital, India
© 2023 La Torre, Calabrese, Signorile, Bizzoco, Mastrorilli, Strippoli, Amato, Carella, Vairo, Giordano, Milella and Cardinale. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco La Torre bGF0b3JyZV9mcmFuY2VzY29AdmlyZ2lsaW8uaXQ=
Specialty Section: This article was submitted to Pediatric Rheumatology, a section of the journal Frontiers in Pediatrics