
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 29 September 2022
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.1013051
This article is part of the Research Topic Behavior Change Approaches to Improve Children and Families’ Dietary Intake and 24h Movement Behaviors View all 5 articles
 Aklilu Abrham Roba1*
Aklilu Abrham Roba1* Assefa Tola1
Assefa Tola1 Desta Dugassa2
Desta Dugassa2 Maleda Tefera1
Maleda Tefera1 Tadese Gure1
Tadese Gure1 Teshager Worku1Awugchew Teshome Ayele3
Teshager Worku1Awugchew Teshome Ayele3 Tamirat Tesfaye Dasa4Hailemariam Mekonnen Workie5
Tamirat Tesfaye Dasa4Hailemariam Mekonnen Workie5 Melese Mengistu Asfaw6Abiyot Asfaw1Firehiwot Mesfin1
Melese Mengistu Asfaw6Abiyot Asfaw1Firehiwot Mesfin1 Lemma Demissie Regassa1
Lemma Demissie Regassa1 Yadeta Dessie1Fitsum Abera7
Yadeta Dessie1Fitsum Abera7 Meron Yeshitila1Meskerem Girma5Muluken Gezahagn7Feven Tezera7
Meron Yeshitila1Meskerem Girma5Muluken Gezahagn7Feven Tezera7 Nega Assefa1
Nega Assefa1 Kedir Teji Roba1
Kedir Teji Roba1There is a gap in evidence linking antenatal care (ANC) utilization, nutrition counseling, and knowledge of pregnant women about infant and young child feeding (IYCF), particularly in low-income settings. Therefore, this study aimed to identify the association between ANC follow-up and nutrition counseling with IYCF knowledge. A cross-sectional study was conducted among 390 pregnant women in the rural kebeles of the Harari region from January to June 2019. Data were collected using face-to-face interviews on tablet computers. Bivariate and multivariate logistic regression were employed. An adjusted odds ratio (with 95% CI) was used to determine the strength of association between IYCF knowledge with ANC follow-up and nutrition counseling by adjusting for educational status, occupation, gravida, and distance to the nearest health center. Overall, 54.4% [95% CI 49.2, 59.2] of currently pregnant women were knowledgeable about IYCF of which only 20% started ANC follow-up and 24.4% received nutrition counseling. Out of 288 multigravida women, only 51.4% had ANC follow-up during their last pregnancy. In the adjusted model, ANC follow-up during the current pregnancy (AOR 1.85, 95% CI 1.07–3.22), those who received nutrition counseling (AOR 1.92, 95% CI 1.09–3.38), literate in education (AOR 1.71, 95% CI 1.07–2.73), multigravida (AOR 1.96, 95% CI 1.12–3.43), and far from the nearest health center (AOR 0.95, 95% CI 0.93–0.97) were significantly associated with the mothers IYCF knowledge. Thus, health care providers should encourage mothers to attend ANC during pregnancy and provide nutrition counseling about the IYCF.
Early life nutrition, particularly during the first 1,000 days from conception to end of the 2nd year of a child, has an important influence on the growth and development of the child. This period is the “critical window”, the time in which the infant is the most vulnerable and the time when crucial brain development occurs (1). A child needs the right kind of nutrition at the right time to thrive and achieve optimal growth and development. Appropriate nutrition during this period forms an important foundation for optimal growth, health, and brain development for the future life of a child (1–4). The most appropriate feeding strategy to ensure optimal feeding for an infant and young child is the initiation of breastfeeding within 1 h of birth, keeping exclusive breastfeeding for the first 6 months, and continue breastfeeding for 2 years or beyond, along with sufficient, safe, and appropriate complementary feeding around 6 months (1, 4, 5).
Undernourished children face learning difficulties in school, earn less in later life, and face barriers to participate in their communities (4). The burden of undernutrition among under-five children remains unacceptably high throughout the world (6). Childhood undernutrition is a major public health problem in developing countries that adversely affect individuals, families, and the community at large (4). In Ethiopia, it is a deep-rooted public health problem among under-five children with stunting (37%), underweight (21%), and wasting (7%). Moreover, among these children, 12% were severely stunted, 6% were severely underweight, and 1% were severely wasted (7).
Undernutrition in children results from multiple factors (8). Maternal knowledge of recommended child feeding practices like exclusive breastfeeding for 6 months, continued breastfeeding, and timely transition to adequate complementary feeding is a key factor for optimal nutritional status, health, and growth of the children (9–13). Lack of knowledge about IYCF is the leading cause of undernutrition among infants and young children in many developing countries (14). Undernutrition is not always only the result of a lack of food but is associated with a lack of knowledge about optimal feeding practices and the provision of poor-quality food (13). The IYCF knowledge of pregnant women is crucial for promoting optimal breastfeeding practices and general child feeding practices in the first 1,000 days of life (2, 15–17).
Antenatal care (ANC] is a key strategy to improve nutrition and health knowledge and promote preventive health practices in low-resource settings (18). ANC service is an ideal entry point to provide multiple health and nutritional interventions to promote maternal and fetal wellbeing, breastfeeding behaviors, and birth preparedness. It presents a unique and lifesaving opportunity for health promotion, disease prevention, early diagnosis, and treatment of illnesses during pregnancy (19). Some studies demonstrated that ANC service utilization increases institutional delivery, utilization of postnatal care, and infant feeding behavior (20–22).
In Ethiopia, the trends of ANC utilization from a skilled provider have increased from 28% in 2005 to 74% in 2019. Also, 71% women of reproductive age received nutrition counseling during their ANC follow-up in 2019 (23). However, the effect of ANC follow-up on maternal IYCF knowledge is not yet adequately studied for evidence-based program planning and intervention in resource-limited rural settings. Thus, as part of a baseline study for a randomized controlled trial (Trial no.: PACTR201804003012418), the current study aimed to determine the association between ANC follow-up and nutrition counseling with IYCF knowledge among pregnant women in the rural areas of the Harari region, Eastern Ethiopia.
This study was carried out in rural kebeles of Harari regional state, located 525 km east of Addis Ababa, the capital of Ethiopia. The region has nine woreda administrations (six urban and three rural) with 19 urban kebele administrations and 17 rural peasant associations. The region has a total of 2,40,000 people, of which 1,23,072 were females and 53,383 are women in the reproductive age group in 2016 (24). The region has an estimated population density of 589.05 people per square kilometer with 3.9 persons per household, 3.4 and 4.6 for urban and rural households, respectively. There are six hospitals, one regional laboratory and research center, eight health centers, 32 health posts, and 40 private clinics in the region (25). The study was conducted from January to June 2019.
A community-based cross-sectional study was carried out as part of a randomized controlled trial (RCT) entitled ‘Effect of Locally Formulated Complimentary Food and Enhanced Homestead Food Production Interventions on Maternal, Infant and Young Child Nutritional Status in the First 1,000 Days in Rural Kebeles of Harari Region, Eastern Ethiopia with trial registration PACTR201804003012418'. The first 1,000 days refers to a child's life from the day he/she is conceived to he/she has completed 2 years of age (24 months) (26). All amenorrheic mothers for at least 3 months were screened for pregnancy by Human Chorionic Gonadotrophin hormone (HCG urine test) by trained data collectors with the help of health extension workers in their respective households. For HCG confirmed women, ultrasound was used to confirm the pregnancy and estimate the gestational age. The study included pregnant women residing for more than 6 months in randomly selected rural kebeles.
The sample size which was calculated for the RCT (Trial no.: PACTR201804003012418) was used for the current study with the following assumptions: 28% of Harar women meet adequate gestational weight gain (27), overall trial-wise Type I error rate of 0.05 (α p < 0.05); 80% power. By adding a 10% drop-out rate, the study recruited 100 women in each arm and obtained a total sample size of 400 pregnant women.
For the current study, a post hoc power analysis using G*Power 3.1.9.4 software was used to determine the power of the study (28). Based on the odds ratio between IYCF knowledge and ANC follow-up (1.85) and nutrition counseling (1.92), an alpha of 0.05, the sample size of 390, and a one-tailed distribution, a power of 0.99 was determined.
Pregnant women were selected using a two stages sampling procedure. First, from a total of 17 rural kebeles of the Harari region, eight were selected by simple random sampling. The randomly selected kebeles were Sukul, Hasen-Gay, Aboker Muti, Erer Ulanula, Dire Teyara, Sofi, Harewae, and Qile. Health extension workers visited every household to identify and recruit the study population in the selected kebeles. Pregnancy was asserted in three stages: mother's claim of her last menstrual period, urine test for pregnancy (HCG), and finally confirmed by ultrasound examination. The total sample size was distributed proportionally to the selected kebeles. When there was more than one pregnant woman in the household, one was selected by lottery method.
The data were collected by four trained nurses (BSc. holders) using a pretested structured questionnaire. English version of the questionnaire was adapted from the Ethiopian Demographic and Health Survey (EDHS) questionnaires which is standardized version (29, 30). It was translated to local languages (Amharic and Oromiffa) and back-translated to English by individuals with good command of both languages (English and Amharic or English and Oromiffa). A pretesting of these questionnaires was done to ensure that the wordings were appropriate to yield the required data by 20 pregnant women in the nearby kebele. Identified gaps between the English and local language versions were corrected before the actual data collection. Data was collected by tablet using ODK open-source software to reduce data entry errors. The questionnaire contained sociodemographic characteristics of the woman and her partner, current and past obstetric history, IYCF knowledge, etc. The IYCF knowledge of the woman was generated using the mean scores based on eight knowledge questions. Respondents who scored below the mean were categorized as “poor knowledge” and vice versa.
The dependent variable was IYCF knowledge while the primary explanatory variable was ANC follow-up for the current pregnancy and nutrition counseling. In addition, the study considered the following as potential confounders: educational status, occupational status, gravida, ever used modern family planning, and distance to the nearest health center.
The normality of data was determined using Shapiro-Wilk's test. Visual inspection of histograms and box plots were used to detect outliers. Percentages and mean (with standard deviation) were used to describe the findings. A binary logistic regression model was employed to identify the crude association between each variable with IYCF knowledge. All variables which had a p-value < 0.2 in the bivariate analysis were included in the multivariate binary logistic regression model. An adjusted odds ratio was used to determine the strength of the association between the dependent and independent variables. Statistical significance was determined using a p-value < 0.05. Analysis was conducted using Stata version 16.0 (31).
A total of 390 pregnant women were included in this analysis with a response rate of 97.5%. The ages range from 15 to 44 years with a mean (±SD) of 25.6 and 5.8 years. All of them were married and Muslims in their religion. Around half (49.7%) of them had never attended formal education. The majority were housewives (91.5%) and their partners were farmers (62.3%). The mean (±SD) duration to reach the nearest health post, health center, and a hospital was 19.7 (±10.5), 24.5 (±12.4), and 51.4 (±13.5) minutes, respectively. Public transport was the main means of transportation (Table 1).
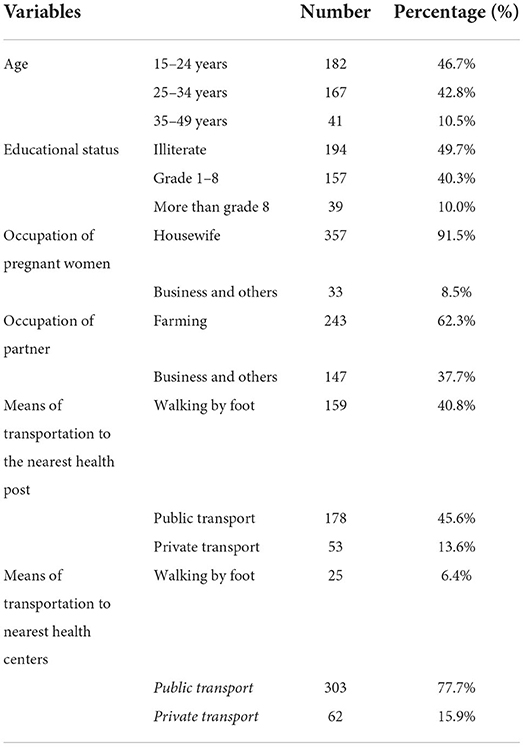
Table 1. Sociodemographic characteristics of currently pregnant women in rural areas of Harari region, eastern Ethiopia, 2019.
The majority (80%) of currently pregnant women have not started antenatal care follow-up, while only half (48.5%) of the women had a history of ANC follow-up in the previous pregnancies. Similarly, 295 (75.6%) of currently pregnant women did not receive nutrition counseling about their children during their current and previous pregnancies. Only 42 (10.8%) of currently pregnant women had a history of using modern family planning methods before this pregnancy. The number of pregnancies ranges from 1 to 11 times with the mean (±SD) of 3.36 (2.3). Similarly, the mean (±SD) of live birth was 2.32 (2.28). On the other hand, the number of currently alive children ranges from 0 to 11 with an average of 2.27 children per woman (Table 2).

Table 2. Obstetric characteristics of currently pregnant women in rural areas of Harari region, eastern Ethiopia, 2019.
Out of 288 multigravida women, 148 (51.4%) had ANC follow-up during their previous (last) pregnancy. Only 33 (22.3%) of them completed ANC follow three times and none of them attained it four times. Among the 99 women who have TT vaccination history, only 12 (12.1%) of them took it three times and the remaining took it twice (50.5%) or once (37.4%). Regarding the place of delivery of the last child, 141 (49%) mothers delivered in their own home (33.0%) or their mother's home (16%). The birth interval between the last child and the current pregnancy ranged from <1–10 years with two-thirds (63.9%) of mothers having 2–5 years intervals. The majority (82.6%) of mothers exposed their last child to sunlight. Among the index children (the last before the current one), only 58 (20.1%) and 103 (35%) took vitamin A supplements and deworming, respectively. Even if 248 (86.1%) of mothers responded as they knew the benefit of vaccination of their children, only 51 (17.7%) of children have been fully vaccinated. Furthermore, only half (49.7%) of the children had BCG scars (Table 3).
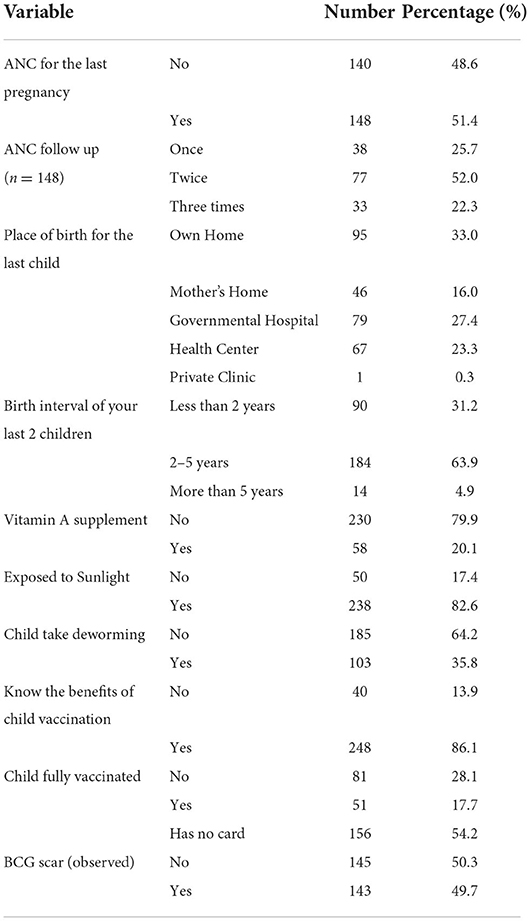
Table 3. Past obstetric history of currently pregnant women in rural areas of Harari region, eastern Ethiopia, 2019 (n = 288).
The majority (93.8%) of pregnant women heard about immediately giving breast milk to the baby after birth. The main sources of information for these women were family and friends (38.2%) and health extension workers (37.4%). Similarly, the majority (81.5%) of pregnant women knew the duration of exclusive breastfeeding. Only 60.5% of the pregnant women correctly mentioned the time to start complementary feeding. Overall, 54.4% [95% CI 49.2, 59.2] of currently pregnant women were knowledgeable about IYCF (Table 4).
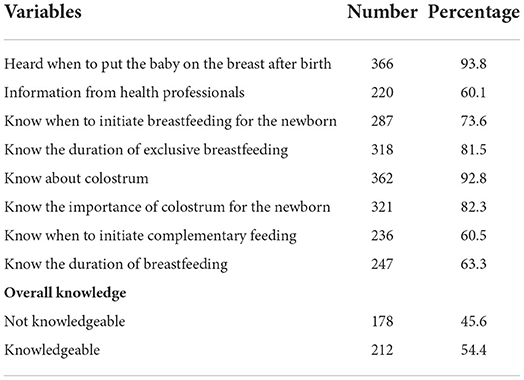
Table 4. Knowledge about infant feeding among currently pregnant women in rural areas of Harari region, eastern Ethiopia, 2019.
In the adjusted model, ANC follow-up in the current pregnancy, nutrition counseling, educational status, gravida, and distance from the nearest health center were significantly associated with the IYCF knowledge. Pregnant women who already initiated their ANC follow-up in the current pregnancy were 1.85 times (AOR = 1.85; 95% CI 1.07–3.22) more likely to have IYCF knowledge compared to those who didn't have ANC follow-up. Similarly, the odds of having IYCF knowledge among the women who received nutrition counseling were twice (AOR =1.92; 95% CI 1.09–3.38) better than their counterparts. Literate women were 1.71 times (AOR = 1.71; 95% CI 1.07–2.73) more likely to have better knowledge about IYCF than their illiterate counterparts. The probability of having IYCF knowledge among multigravida women was almost twice (AOR = 1.96; 95% CI 1.12–3.43) higher than primigravida women. Finally, when the distance from the nearest health center increased by a kilometer, there was a 5% decrease in knowledge about IYCF (AOR 0.95, 95% CI 0.93–0.97) (Table 5).
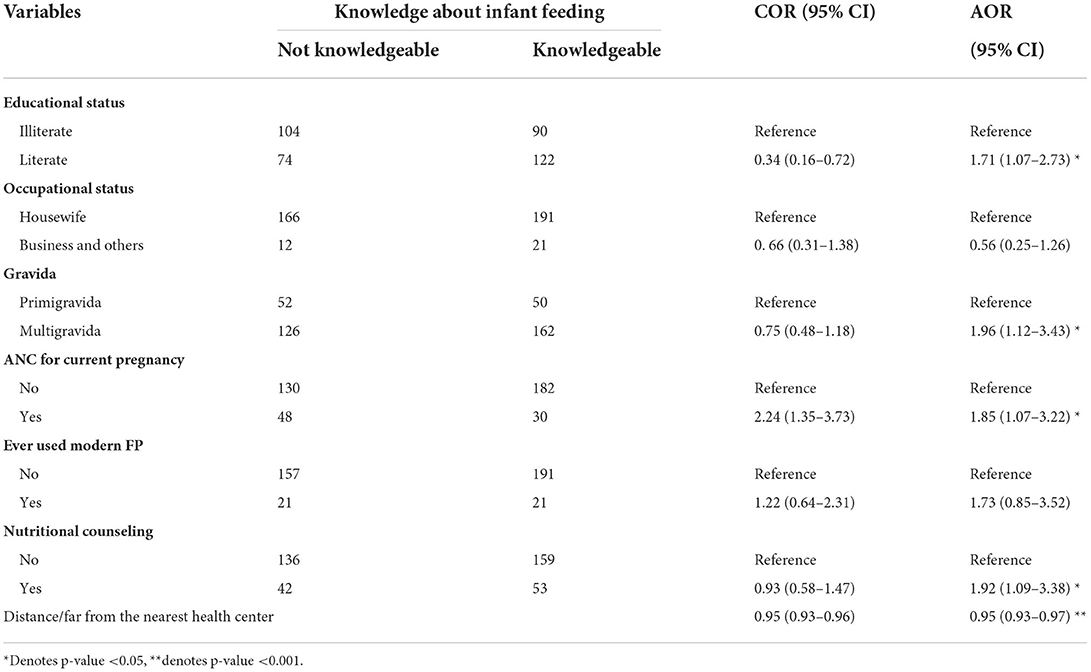
Table 5. Factors associated with Knowledge about infant feeding of currently pregnant women in rural areas of Harari region, eastern Ethiopia, 2019.
The current study identified ANC follow-up in the current pregnancy, nutrition counseling, educational status, gravida, and distance from the nearest health center as predictors of the IYCF knowledge. Also, it revealed that 54.4% of currently pregnant women were knowledgeable about IYCF. This figure was consistent with previous studies including West Gojjam Zone of Northwest Ethiopia (60%) (9), Adea Woreda of the Oromia region in Ethiopia (51%) (32), Moshi Urban of Tanzania (61.2%) (15), and Kpandai district of the Northern Region of Ghana (50%) (12). However, the IYCF knowledge in this study was higher than the findings of the Cross River State of Nigeria (20%) (13), Sagamu of southwestern Nigeria (41.4%) (33), and Kenya (46%) (18). But it was less than studies conducted in Nnewi South-East Nigeria (82.0%) (34) and the Wolaita Zone of southern Ethiopia (66.1%) (35). This variation might be due to the difference in the study population, sample size, operational definition of knowledge, and socio-economic backgrounds of the participants (13, 33–35).
Regarding the specific knowledge levels, 81.5% of mothers knew the recommended duration of exclusive breastfeeding, which was consistent with the findings done in the Shabelle Zone of the Somali Region in Eastern Ethiopia that stated 85% of the mothers knew the correct time for exclusive breastfeeding (10). In this study, 73.6% of respondents correctly mentioned immediately initiating breastfeeding after delivery. It is consistent with the study conducted in Tanzania (71%) (15) but higher than studies conducted in Shabelle Zone of Somali region (47%) (10) and in China (32.5%) (36). Furthermore, 60.5% of the mothers correctly mentioned the right time to introduce complementary feeding is at completed 6 months which was consistent with a study done in rural Hebei Province of China (63.9%) (36) but lower than the result found in Moshi Urban of Tanzania (83%) (15). Moreover, in the current study, about two–thirds (63.3%) of pregnant women correctly mentioned the duration of breastfeeding after initiating additional food. This finding was much lower than a study conducted in the Shabelle Zone of the Somali Region in Eastern Ethiopia (91%) (10). Those variations might be due to differences in the study settings and the socioeconomic status of study participants.
Maternal educational status is one of the important determinants of IYCF knowledge (37). Educated mothers can better understand the information provided by health professionals regarding IYCF than illiterate women. The positive association between maternal educational status and their IYCF knowledge was reported by previous studies (9, 17, 33, 37). However, a study in the Shabelle Zone of the Somali Region in Eastern Ethiopia presented maternal educational status did not show any significant association with the IYCF knowledge (10).
The number of lifetime pregnancies (Gravida) was also associated with the IYCF knowledge. Accordingly, those multigravida pregnant women were more knowledgeable about IYCF than primigravida. Consistent findings were reported from other similar studies as pregnant women with a higher number of children had more knowledge than those with few children (17, 35). A study in Arba Minch Zuria of southern Ethiopia showed that mothers with <3 children had less chance of being knowledgeable about optimal child feeding practices (17).
Besides improving maternal and child outcomes, attending ANC has the potential to increase maternal knowledge about dietary diversity for self and IYCF (18, 38). Our study also showed that those pregnant women who started ANC follow-up in their current pregnancy were more knowledgeable about IYCF than those who did not start ANC follow-up. It agrees with studies conducted in the Wolaita Zone of Southern Ethiopia (35), West Gojjam Zone of Northwest Ethiopia (9), Arba Minch Zuria of southern Ethiopia (17), and Western Kenya (18), and Sagamu of southwestern Nigeria (33). ANC attending is an excellent opportunity to receive health-related information. This information can improve the knowledge of attendants.
Although ANC is a good contact point to get pregnant mothers and educate them about IYCF, only few women received nutrition information (36). Our study also revealed that those pregnant women who received nutrition counseling during current and previous pregnancies had better knowledge than those who did not receive it. Similar findings were reported in previous studies (9, 15, 35). A study by Hashim et al. stated that those women who received counseling on breastfeeding during the current pregnancy had almost 4 times higher knowledge about appropriate breastfeeding knowledge (15).
Strengths of this study include pregnancy was confirmed objectively by HCG urine test and ultrasound. Also, the data was collected by tablet computers to reduce errors during data collection and entry. Furthermore, as this study is part of a randomized controlled trial, due emphasis was given to data quality from designing to the analysis stage. Though there are several strengths, it has some limitations. The study included pregnant women in rural/semi-urban areas of eastern Ethiopia. Thus, the findings may not reflect their urban counterparts. Finally, since the data was collected at a single point, a temporal relationship may not be established.
The overall IYCF knowledge of pregnant women was fair and associated with ANC follow-up, maternal education status, distance from the nearest health center, number of lifetime pregnancies (gravida), and nutrition counseling in current/previous pregnancies. Thus, improving the utilization of antenatal care and incorporating nutritional counseling is a crucial intervention to increase the IYCF knowledge, particularly in primigravida women. Local government administrators and other stakeholders should emphasize women's education, as educated women have a better consciousness of IYCF practices. The health care providers, mainly health extension workers, should encourage mothers to attend antenatal care during pregnancy and provide IYCF education.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The Ethical clearance was obtained from Haramaya University College of Health and Medical Sciences Institutional Health Research Ethics Review Committee (IHRERC/068/2018). The patients/participants provided their written informed consent to participate in this study.
AAR and all the co-authors: conceived and designed the study, acquisition of the fund and data, and critical revision of the manuscript. AAR and DD: project and resource administration. AAR, DD, MT, ATA, TTD, HW, MA, and KTR: supervision. AAR: original draft. All authors contributed to the article and approved the submitted version.
Haramaya University, Office of Research Affairs (HURG−2017-02-02-09).
We are very grateful to Haramaya University for financial and material support during the study period.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ANC, antenatal care; AOR, adjusted odds ratio; CI, confidence interval; HCG, human chorionic gonadotropin; IYCF, infant and young child feeding; ODK, open data kit; RCT, randomized controlled trial; SD, standard deviation; TT, tetanus toxoid.
1. Ruel MT. Measuring infant and young child complementary feeding practices: indicators, current practice, and research gaps. Complement Feed. (2017) 87:73–87. doi: 10.1159/000448939
2. Newby R, Brodribb W, Ware RS, Davies PS. Infant feeding knowledge, attitudes, and beliefs predict antenatal intention among first-time mothers in Queensland. Breastfeed Med. (2014) 9:266–72. doi: 10.1089/bfm.2014.0012
3. Marriott BP, White A, Hadden L, Davies JC, Wallingford JC. World Health Organization (WHO) infant and young child feeding indicators: associations with growth measures in 14 low-income countries. Matern Child Nutr. (2012) 8:354–70. doi: 10.1111/j.1740-8709.2011.00380.x
4. UNICEF WHO The The World Bank Group. UNICEF/WHO/The World Bank Group Joint Child Malnutrition Estimates: Levels and Trends in Child Malnutrition: Key Findings of the 2020 Edition (2020).
5. Tiwari S, Bharadva K, Yadav B, Malik S, Gangal P, Banapurmath C, et al. Infant and young child feeding guidelines, 2016. Indian Pediatr. (2016) 53:703–13. doi: 10.1007/s13312-016-0914-0
6. Fanzo J, Hawkes C, Udomkesmalee E, Afshin A, Allemandi L, Assery O, et al. Global Nutrition Report: Shining a Light to Spur Action on Nutrition (2018).
7. EPHI I. Ethiopia Mini Demographic And Health Survey 2019: Key Indicators. Rockville, MD: EPHI and ICF (2019).
8. Kasaye HK, Bobo FT, Yilma MT, Woldie M. Poor nutrition for under-five children from poor households in Ethiopia: Evidence from 2016 Demographic and Health Survey. PLoS ONE. (2019) 14:e0225996. doi: 10.1371/journal.pone.0225996
9. Abiyu C, Belachew T. Level and predictors of mothers' knowledge and attitude on optimal complementary feeding in West Gojjam Zone, Northwest Ethiopia. Nutr Diet Suppl. (2020) 12:113. doi: 10.2147/NDS.S257206
10. Guled RA, Mamat NM, Bakar WAMA, Assefa N, Balachew T. Knowledge, attitude and practice of mothers/caregivers on infant and young child feeding in Shabelle Zone, Somali Region, Eastern Ethiopia: a cross sectional study. Revel Sci. (2016) 6:42–54.
11. Debela BL, Demmler KM, Rischke R, Qaim M. Maternal nutrition knowledge and child nutritional outcomes in urban Kenya. Appetite. (2017) 116:518–26. doi: 10.1016/j.appet.2017.05.042
12. Bimpong KA, Cheyuo EK-E, Abdul-Mumin A, Ayanore MA, Kubuga CK, Mogre V. Mothers' knowledge and attitudes regarding child feeding recommendations, complementary feeding practices and determinants of adequate diet. BMC Nutr. (2020) 6:1–8. doi: 10.1186/s40795-020-00393-0
13. Jemide JO, Ene-Obong HN, Edet EE, Udoh EE. Association of maternal nutrition knowledge and child feeding practices with nutritional status of children in Calabar South Local Government Area, Cross River State, Nigeria. Int J Home Sci. (2016) 2:293–8.
14. Singh A, Ranjan A, Thakur A. Study of compliance and impact of infant and young child feeding counseling in Patna district, Bihar. Indian J Child Health. (2017) 4:430–4. doi: 10.32677/IJCH.2017.v04.i03.037
15. Hashim TH, Mgongo M, Katanga J, Uriyo JG, Damian DJ, Stray-Pedersen B, et al. Predictors of appropriate breastfeeding knowledge among pregnant women in Moshi Urban, Tanzania: a cross-sectional study. Int Breastfeed J. (2016) 12:1–8. doi: 10.1186/s13006-017-0102-4
16. Biks GA, Tariku A, Wassie MM, Derso T. Mother's Infant and Young Child Feeding (IYCF) knowledge improved timely initiation of complementary feeding of children aged 6–24 months in the rural population of northwest Ethiopia. BMC Res Notes. (2018) 11:1–7. doi: 10.1186/s13104-018-3703-0
17. Tamiru D, Mohammed S. Maternal knowledge of optimal breastfeeding practices and associated factors in rural communities of Arba Minch Zuria. Int J Nutr Food Sci. (2013) 2:122–9. doi: 10.11648/j.ijnfs.20130203.15
18. Perumal N, Cole DC, Ouédraogo HZ, Sindi K, Loechl C, Low J, et al. Health and nutrition knowledge, attitudes and practices of pregnant women attending and not-attending ANC clinics in Western Kenya: a cross-sectional analysis. BMC Pregnan Childb. (2013) 13:1–12. doi: 10.1186/1471-2393-13-146
19. Okedo-Alex IN, Akamike IC, Ezeanosike OB, Uneke CJ. Determinants of antenatal care utilisation in sub-Saharan Africa: a systematic review. BMJ Open. (2019) 9:e031890. doi: 10.1136/bmjopen-2019-031890
20. Berhan Y, Berhan A. Antenatal care as a means of increasing birth in the health facility and reducing maternal mortality: a systematic review. Ethiop J Health Sci. (2014) 24:93–104. doi: 10.4314/ejhs.v24i0.9S
21. Saaka M, Emmanuel K, Farruza I. Adequacy of Prenatal Care Utilization and Its Effect on Postpartum Infant Feeding Behaviors in Northern Ghana (2016).
22. Tariku A, Alemu K, Gizaw Z, Muchie KF, Derso T, Abebe SM, et al. Mothers' education and ANC visit improved exclusive breastfeeding in Dabat Health and Demographic Surveillance System Site, northwest Ethiopia. PLoS ONE. (2017) 12:e0179056. doi: 10.1371/journal.pone.0179056
23. Ethiopian Public Health Institute (EPHI) and ICF. Ethiopia Mini Demographic and Health Survey 2019: Final Report. Rockville, MD: EPHI and ICF (2021).
24. Birhanu S, Demena M, Baye Y, Desalew A, Dawud B, Egata G. Pregnant women's satisfaction with antenatal care services and its associated factors at public health facilities in the Harari region, Eastern Ethiopia. SAGE Open Med. (2020) 8:2050312120973480. doi: 10.1177/2050312120973480
25. HSDP. Health Sector Development Program IV 2010/11-2014/15. Ministry of Health Addis Ababa (2010).
26. Fox SE, Levitt P, Nelson CA, III. How the timing and quality of early experiences influence the development of brain architecture. Child Dev. (2010) 81:28–40. doi: 10.1111/j.1467-8624.2009.01380.x
27. Asefa F, Nemomsa D. Gestational weight gain and its associated factors in Harari Regional State: Institution based cross-sectional study, Eastern Ethiopia. Reprod. Health. (2016) 13:1–7. doi: 10.1186/s12978-016-0225-x
28. Razali NM, Wah YB. Power comparisons of shapiro-wilk, kolmogorov-smirnov, lilliefors and anderson-darling tests. J. Stat. Model. Anal. (2011) 2:21–33.
29. Rutstein SO, Rojas G. Guide to DHS Statistics. Demographic and Health Surveys. Maryland: ORC Macro Calverton (2006).
30. CSA-Ethiopia I. International Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Rockville: CSA and ICF (2016).
32. Agize A, Jara D, Dejenu G. Level of knowledge and practice of mothers on minimum dietary diversity practices and associated factors for 6–23-month-old children in Adea Woreda, Oromia, Ethiopia. BioMed Res Int. (2017) 2017:1–9. doi: 10.1155/2017/7204562
33. Sholeye OO, Akinpelu A, Bankole E, Diya O. Knowledge of infant feeding among mothers in sagamu, southwestern Nigeria: implications for nutrition education. Am J Food Nutr. (2016) 6:69–76. doi: 10.5251/ajfn.2016.6.3.69.76
34. Onah S, Osuorah DIC, Ebenebe J, Ezechukwu C, Ekwochi U, Ndukwu I. Infant feeding practices and maternal socio-demographic factors that influence practice of exclusive breastfeeding among mothers in Nnewi South-East Nigeria: a cross-sectional and analytical study. Int Breastfeed J. (2014) 9:1–10. doi: 10.1186/1746-4358-9-6
35. Yeshambel Wassie A, Atnafu Gebeyehu N, Abebe Gelaw K. Knowledge, attitude, and associated factors towards colostrum feeding among antenatal care attendant mothers in Gununo Health Centre, Wolaita Zone, Ethiopia 2019: Cross-Sectional Study. Int J Pediatr. (2020) 2020:1–10. doi: 10.1155/2020/3453502
36. Wu Q, Scherpbier RW, Van Velthoven MH, Chen L, Wang W, Li Y, et al. Poor infant and young child feeding practices and sources of caregivers' feeding knowledge in rural Hebei Province, China: findings from a cross-sectional survey. BMJ Open. (2014) 4:e005108. doi: 10.1136/bmjopen-2014-005108
37. Berihu A, Abera G, Berhe H, Kidanu K. Mother's knowledge on nutritional requirement of infant and young child feeding in Mekelle, Ethiopia, cross sectional study. Glob J Med Res. (2013) 13:13–24.
Keywords: infant and young child feeding, antenatal follow up, nutrition counseling, knowledge, pregnant women
Citation: Roba AA, Tola A, Dugassa D, Tefera M, Gure T, Worku T, Ayele AT, Dasa TT, Workie HM, Asfaw MM, Asfaw A, Mesfin F, Regassa LD, Dessie Y, Abera F, Yeshitila M, Girma M, Gezahagn M, Tezera F, Assefa N and Roba KT (2022) Antenatal care utilization and nutrition counseling are strongly associated with infant and young child feeding knowledge among rural/semi-urban women in Harari region, Eastern Ethiopia. Front. Pediatr. 10:1013051. doi: 10.3389/fped.2022.1013051
Received: 06 August 2022; Accepted: 12 September 2022;
Published: 29 September 2022.
Edited by:
Brittany J. Johnson, Flinders University, AustraliaCopyright © 2022 Roba, Tola, Dugassa, Tefera, Gure, Worku, Ayele, Dasa, Workie, Asfaw, Asfaw, Mesfin, Regassa, Dessie, Abera, Yeshitila, Girma, Gezahagn, Tezera, Assefa and Roba. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aklilu Abrham Roba, YWtsaWx0aW1uYXRoc2VyYWhAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.