
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pediatr. , 03 January 2022
Sec. Children and Health
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.800073
This article is part of the Research Topic Exercise Challenges in Pediatric Health and Disease: The Need for Testing View all 7 articles
 Maria Vollsæter1,2*
Maria Vollsæter1,2* Trine Stensrud3†
Trine Stensrud3† Robert Maat4
Robert Maat4 Thomas Halvorsen1,2,3†
Thomas Halvorsen1,2,3† Ola Drange Røksund1,5
Ola Drange Røksund1,5 Astrid Sandnes6
Astrid Sandnes6 Hege Clemm1,2†
Hege Clemm1,2†Complaints of breathlessness during heavy exercise is common in children and adolescents, and represent expressions of a subjective feeling that may be difficult to verify and to link with specific diagnoses through objective tests. Exercise-induced asthma and exercise-induced laryngeal obstruction are two common medical causes of breathing difficulities in children and adolescents that can be challenging to distinguish between, based only on the complaints presented by patients. However, by applying a systematic clinical approach that includes rational use of tests, both conditions can usually be diagnosed reliably. In this invited mini-review, we suggest an approach we find feasible in our everyday clinical work.
Exercise related breathing complaints are common in children and adolescents, and a scenario all clinicians must be prepared to encounter. The experience of breathlessness or dyspnea during heavy exercise is a subjective feeling, and may often be difficult to verify through objective tests. Dyspnea during exercise may be caused by numerous respiratory or non-respiratory factors. This was nicely exemplified by a study by Abu Hasan et al. (1) where exercise induced breathing complaints were present in 142 included young adults, and observed in 82% during exercise testing. Importantly, normal physiological exercise limitations were demonstrated in 52%, exercise induced bronchoconstriction (EIB) in 8%, and symptoms of exercise induced laryngeal obstruction (EILO) in 9%. As most patients in fact had neither EIB nor EILO, the study supports a broader view on other causes of exercise induced breathing complaints, like dysfunctional breathing patterns (2), low aerobic capacity or other. This and other studies (3) have underlined the heterogeneous nature of exercise induced complaints, and provided support to guidelines recommending that exercise induced breathing complaints should be evaluated with objective tests (4) and that EILO might be just as frequent as EIB (5, 6).
Asthma is common in children and adolescents, and a well-established cause of EIB, with current prevalence rates 5–20% in the general population (7). Up to 90% of patients with symptomatic asthma are reported to have some degree of EIB (8). Untreated EIB may lead to exercise intolerance and reduced participation in play and sport (9). Despite guidelines prescribing objective test methods (4), studies suggest that asthma and EIB are often diagnosed simply based on wheeze as presenting symptoms, which is a highly questionable strategy (3, 10–12).
The purpose of this mini-review is to outline a practical diagnostic approach to children and adolescents presenting with exercise induced breathing complaints, focusing on separating EIB from EILO.
Exercise increases the metabolic demands of the body and leads to increased pulmonary ventilation. The increased ventilation is accomplished mainly by greater tidal volumes at low intensity exercise, while at higher intensities, the breathing frequency increases alongside a decrease of particularly the expiratory time (13, 14). The minute ventilation may rise 30 times over resting values at peak exercise (13, 15). When the minute ventilation rises during exercise, most people shift from nasal to oral breathing, to reduce airflow recistance (16). Active opening of the mouth tends to widen the laryngeal opening, allowing for higher airflow with less increase of laryngeal resistance (17).
High intensity exercise imposes stress on the respiratory system. Ideally, breathing is regulated to maximize the ability to perform. Anatomy, physiological capacities, and the state of the cardiopulmonary system are all important factors for performance. Various exercise modalities/sports may challenge ventilation, and optimal conditions for diaphragmatic and thoracic expansion depend on body posture and breathing frequency (18, 19). The larynx plays a role in some exercise modalities, where closure of the glottis facilitates elevation of thoracic and abdominal pressures (20).
Atopic asthma often starts in childhood and is characterized by allergies and bronchial mucosal eosinophilic inflammation. The patient may experience chest tightness, dyspnea, wheeze and cough during exercise, and also when exposed to allergens or airway infections (21). Asthma is a clinical diagnosis based on a combination of symptoms and objective findings. Global Initiative of Asthma (GINA) defines asthma as symptoms that vary in time and intensity, alongside variable expiratory airway obstruction (22). EIB is present in a great proportion of young people with untreated or under-treated asthma (8), but is also a feature observed in athletes with or without previous asthma (4, 23). In athletes, EIB is often a result of years of high-intensity exercise in unfavouralbe environmental conditions, such as cold air, polluted air or chlorine (24–26). EIB is suggested characterized by neutrophilic inflammation, or a combined neutrophilic and eosinophilic inflammation (27). In sports, EIB is seemingly related to prolonged mechanical, osmotic and thermic stress, with subsequent destruction of airway epithelia (28). These findings are related to the time spent exercising in harsh conditions, and also to the timing of the testing, whether this is in close relation to a period of intensive training or competition (25). Increased bronchial parasympathetic tone has been reported in skiers, suggesting that the parasympathetic nervous system is implicated in the development of EIB in athletes (29, 30).
EIB leads to respiratory symptoms during or after exercise, like chest tightness, dyspnea, cough or secretions. However, exercise related breathing complaints are poorly associated with objective findings, and tests are therefore required to diagnose both asthma and EIB (3, 31). Spirometry with reversibility measurements after inhaled beta2 agonists or ipratropium bromide is a minimum (32). Measurement of exhaled nitric oxide might reveal eosinophilic inflammation, and there are different bronchial provocation tests to diagnose bronchial hyperreactivity to direct or indirect stimuli. A direct stimulus is metacholine, a parasympatic agent acting directly on muscarine receptors on smooth mucle cells in the airway wall, leading to bronchoconstriction (33). Indirect stimuli are based on the theory that fluid and heatloss from the airways during high minute ventilation leads to bronchoconstriction (34). Exercise-tests and eucapnic voluntary hyperventilation (EVH) tests are the classical examples of such indirect stimuli, but inhaled mannitol or hypertonic saline are also based on these same principles (35). EVH is now valued as the most sensitive test available (36, 37), however EIB-test with inhaled cold or dry air, is more specific (35, 38).
EIB is a response to increased ventilation induced by high intensity exercise, with expiratory symptoms, usually peaking 3–15 mins after ending exercise (39). This response contrasts that caused by upper airway obstruction, that typically peak during exercise or just after stopping and presents on inspiration. The literature indicates that EIB is overdiagnosed in patients with EILO (40, 41).
Exercise induced laryngeal obstruction (EILO) refers to inappropriate transient adduction of the structures in the larynx during exercise and is a common cause of exercise induced respiratory symptoms. The nomenclature proposed by the joint “Task Force on Inducible Laryngeal Obstructions” (42) underlines that EILO can occur on two laryngeal levels, the supraglottic and the glottic (vocal fold) level.
EILO is a clinical diagnosis, where the exercise induced medialisation of laryngeal structures leads to inspiratory airflow obstruction during exercise, usually characterized by typical breathing complaints. The critical point of obstruction of the larynx required to produce symptoms in any given individual is difficult to assess, and probably depends on the timing of the breathing cycle, the airflow, the absolute size of the larynx or other individual differences (43). Airflow through the larynx increases with increased exercise intensity, and as increased flow through a tube inevitably sets up a negative pressure within that tube, this mechanism may be involved in the laryngeal adduction or collapse observed in EILO patients. Depending on the airflow velocity, turbulence, laryngeal architecture, and the strength of the supporting structures, the larynx of a patient with EILO will eventually yield to the negative pressure (17, 44–46). The normal or optimal relations between body size, ventilatory requirements, and the absolute size of the laryngeal aperture remain to be shown (47).
EILO is usually characterized by respiratory difficulties during inspiration, sometimes accompanied by stridor-like breath sounds. Some EILO patients develop hyperventilation or panic reactions with increasing ventilatory requirement parallel to increasing exercise intensity (43, 48). Many individuals have difficulties describing their symptoms, and inspiratory symptoms might associate to a wide spectrum of structural and functional abnormalities; therefore, testing is necessary (5, 6, 40, 49, 50). The gold standard for diagnosing EILO is the continuous laryngoscopy during exercise (CLE-test) (48). The test will reveal the level and starting point of obstruction, as well as the degree, scored by the CLE score (51), information which may guide further treatment approach (52, 53). Spirometry should be included in the diagnostic work-up in all patients with exercise related breathing complaints, however, spirometry patterns are not diagnostic for EILO, neither are bronchial hyperreactivity tests (54).
Like with EIB, environmental factors may contribute in EILO. There are reports of EILO worsening in cold and humid conditions (55, 56), as well as being more frequent among athletes participating in outdoor activities (57).
EIB and EILO both present as exercise related breathing complaints in the young. EIB is a diagnosis easily resorted to, possibly because of the high degree of awareness among physicians and patients. EILO is a less well-known diagnosis, and therefore possibly less likely to be considered. Ersson et al. found an estimated prevalence of EIB in 23% and EILO in 8% of adolescents attending first year of sports high school in Sweden, underlining the importance of EILO as differential diagnosis to EIB (58). In two other Scandinavian studies of unselected children with exercise related complaints, the EILO prevalence was 5% and 7.5% (5, 6). As for patient demographics, EILO is seemingly most common in young females (59, 60). EILO symptoms are often confused with symptoms of EIB (21, 61, 62), and retrospective reports indicate that asthma medication has often been prescribed to patients later diagnosed with EILO (63, 64). In a study of 151 EILO patients, 85% had used asthma treatments, 64% of these with no effect on exercise related symptoms (40). EIB and EILO may also coexist, leading to confusion regarding the effect of asthma treatment (6, 57, 63–66). Treating EILO as asthma might lead to overmedication, frustration, and eventually cessation of sports activities in youngsters (40).
Patients with exercise relatd breathing difficulties should be tested by means of an exercise test, and ideally with the particular type of exercise and under the particular environmental conditions that led to their symptoms (31). In routine clinical work, standardized exercise tests are usually applied, due to practical challenges setting up customized tests and contidions, and problems related to test-retest reproducibility (67, 68). Close observation and thorough reporting of symptom development during any exercise test is essential.
Most studies of both EILO and EIB include adolescents (5, 6, 69). During these years the intensity of physical exercise often increases, and they approach their ventilation limits more often than earlier. As the age-span for symptoms of both conditions is wide, it is important that we provide a test-battery suited for all ages. Both EIB and EILO can occur at a young age, well documented in EIB (70), but more scarcely in EILO (71). Alternative and appropriate means of testing should be considered in the youngest patients, as well as in patients of all ages with various impairments, as both spirometry and treadmill running or cycling might be challenging or impossible. Other forms of strenuous activity can be applied to elicit the symptoms (70, 72), an appropriate heart rate should be achieved. This may be accompanied by spirometry, or by close observation of breathing patterns during and after exercise, in order to differentiate between the two conditions EIB and EILO (Figure 1). This observation period needs to be prolonged in order to allow for EIB symptoms to arise, corresponding to the time allowed for repeated spirometries after a standard EIB test. As for EILO, there are currently no appropriate alternatives to the CLE-test.
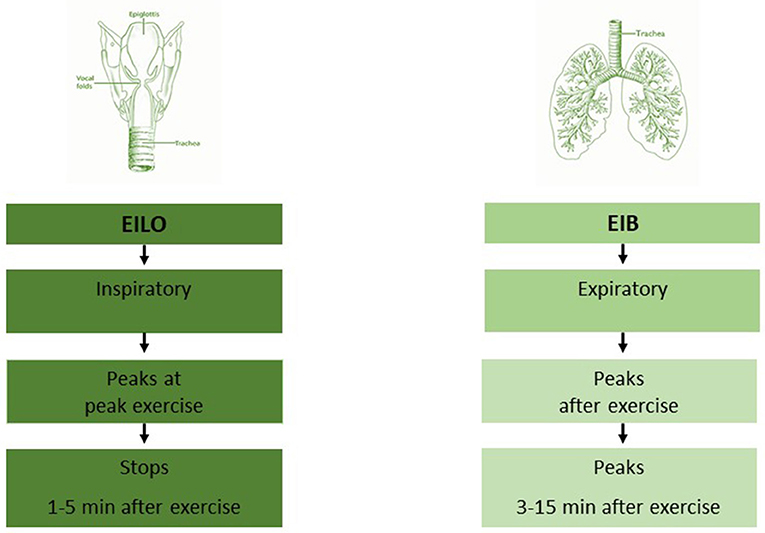
Figure 1. Work-up should be customized to the level of complaints, but always involve a thorough symptom description. Spirometry, and a standardized exercise test for *exercise induced bronchoconstriction (EIB) are logical second steps. The EIB test should always include the test-leaders thorough description of breathing patterns during and after the test, and a patient verification that the symptoms perceived during the test were similar to those that in-cited the work-up. Patients with classical symptoms of EILO observed during an exercise test may not need a CLE test, depending on the clinical situation. Persistent symptoms without findings must incite further work-up. **Diagnostic tests for BHR might include Spirometry with reversibility, PD20, EVH, Mannitol or hypertonic saline, depending on the clinical situation and department policy. EIB, exercise induced bronchoconstriction; EILO, exercise induced laryngeal obstruction; BHR, bronchial hyperresponsiveness; CLE, continuous laryngoscopy exercise test; CPET, cardiopulmonary exercise test. Modified from Paediatric Respiratory reviews (47).
We consider the standardized exercise induced bronchoconstriction (EIB) test to be the first choice and the cornerstone in the diagnostic evaluation of exercise related breathing complaints. The change after exercise in forced expiratory volume in first second (FEV1) is the main objective outcome measure of an EIB test; however, of similar importance is the patient's symptoms presentation and breathing patterns during the test. These items should be observed and thoroughly described by the test-leader, and be documented and made available for the physician interpreting the test (Figure 2). The symptoms have to be described during and after exercise, whether they are most prominent at inspiration or expiration, whether they peak at or after maximum ventilation, and the time to symptoms resolve. Also, accompanying symptoms should be described, respiratory sounds, patient reactions and breathing patterns. Video recording of the patient and the symptom presentation during the test, may be considered. The patient could even bring her/his own video of the symptoms, recorded during (or immediately after) exercise, the video should include sound. Whether the observed symptoms are representative for the breathing complaints that led to the referral for testing is of great interest. Of note, dysfunctional breathing (2) or insufficient effort is of great importance. Insufficient intensity might lead to a false negative test, as a high ventilation is required to elicit EIB. The requirement for the patient being able to reproduce symptoms during the test, is absolute for both EIB and EILO tests.
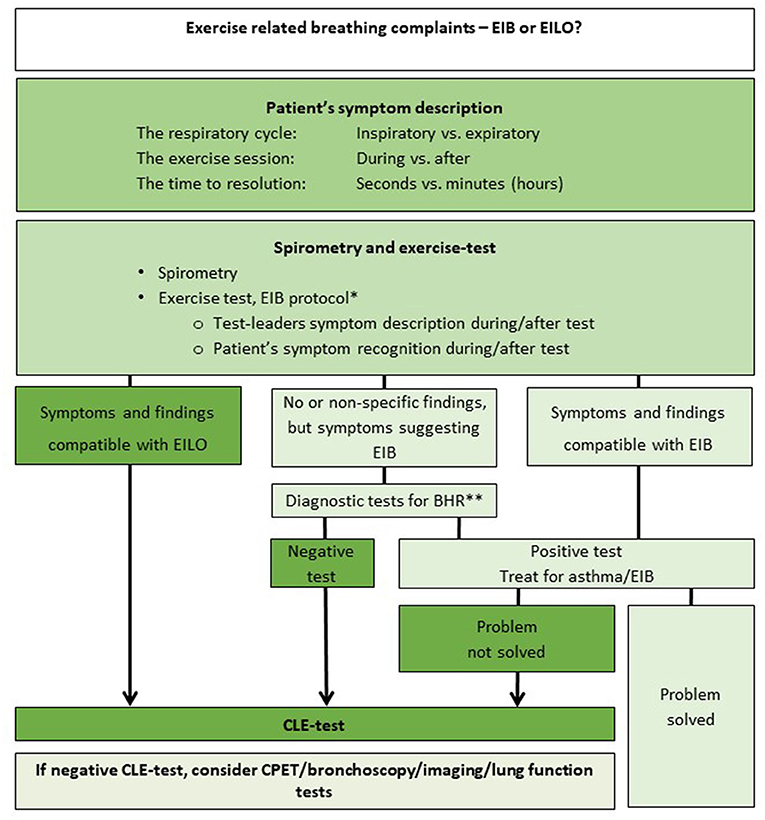
Figure 2. Symptom presentation in the patient with exercise induced breathing complaints, differences between EIB and EILO. EIB, exercise induced bronchoconstriction; EILO, exercise induced laryngeal obstruction. Modified from Paediatric Respiratory reviews (47).
A decline in FEV1 of 10% or more after exercise is considered a positive test for EIB, (73) and treatment should be initiated in accordance with recommendations (22). A negative test combined with strong clinical suspicion of EIB should incite more specific tests for bronchial hyperreactivity, a topic which is outside the scope of this article (4).
Inspiratory breathing difficulties observed during an EIB test should lead to suspicion of EILO, and a CLE-test should be considered (42). If EILO is diagnosed, breathing advice and/or other forms of treatment should follow accordingly (47, 55). There are currently no guidelines to recommend an evidence based treatment approach for EILO, and this is evidently an under-reserched area of respiratory medicine.
If the CLE test reveals normal findings and the symptoms suggest inspiratory obstruction, other diagnostic tests should be considered, guided by the nature of the presenting symptoms and their severity. A cardiopulmonary exercise test evaluates cardiopulmonary responses and limitations in relation to exercise, such as low aerobic capacity, heart disease, lung diseases with ventilatory limitations or dysfunctional breathing (2, 74), and measures breathing frequency and tidal volumes, which could be used to objectively assess breathing patterns during exercise in cases where an abnormal breathing patterns have been described.
Bronchoscopy or radiologic imaging of central airways and the thoracic cage could reveal for example tracheobronchomalacia, excessive dynamic airway collapse (75), or inborn vascular malformations that compromise central airways and thereby produce symptoms that are aggrevated by high intensity exercise. We have previously found structural abnormalities in the upper airways in ~10% of patients refered to our institution under the suspicion of EILO (76).
Exercise related breathing complaints are common in the young. The symptom presentation should be accurately described but cautiously interpreted, as widely different conditions might present with symptoms that are similarly described by patients. Important factors to consider are the timing of the breathing complaints in relation to the exercise, and if the problem is inspiratory or expiratory; i.e., inspiratory stridor or expiratory wheeze, and the time to symptom resolution after exercise. Patients with exercise related breathing difficulties should be tested by means of exercise, ideally with the type of exercise and under the environmental conditions that lead to their symptoms. Spiromtery performed before vs. after exercise and a visual representation of the larynx throughout an ongoing maximal exercise test are the two recommended means to diagnose EIB and EILO, respectively. A thorough symptoms description during the exercise tests is also important, in order to reveal (co)morbidities that may cause or blur the picture, like dysfunctional breathing.
MV, TS, RM, TH, OR, AS, and HC made a significant contribution to the conception and the design of the article and of the collection, analysis and interpretation of the data, drafting of the article, and revising it critically for content and final approval of the version to be published. All authors participate in the Upper Airway Group of Haukeland University Hospital and are collectively responsible for the final version of this paper.
Major funding institutions: Haukeland University Hospital, University of Bergen and Bergen University College.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CLE-test, continuous laryngoscopy exercise-test; CPET, cardiopulmonary exercise test; EIA, exercise induced asthma; EIB, exercise-induced bronchoconstriction; EIIS, exercise induced inspiratory symptoms; EILO, exercise induced laryngeal obstruction; FEV1, forced expiratory flow in the first second; PCA-muscle, the posterior cricoarytenoid muscle; VCD, vocal cord dysfunction.
1. Abu-Hasan M, Tannous B, Weinberger M. Exercise-induced dyspnea in children and adolescents: if not asthma then what? Ann Allergy Asthma Immunol. (2005) 94:366–71. doi: 10.1016/S1081-1206(10)60989-1
2. Boulding R, Stacey R, Niven R, Fowler SJ. Dysfunctional breathing: a review of the literature and proposal for classification. Eur Respir Rev. (2016) 25:287–94. doi: 10.1183/16000617.0088-2015
3. Henriksen AH, Tveit KH, Holmen TL, Sue-Chu M, Bjermer LA. study of the association between exercise-induced wheeze and exercise versus methacholine-induced bronchoconstriction in adolescents. Pediatr Allergy Immunol. (2002) 13:203–8. doi: 10.1034/j.1399-3038.2002.01034.x
4. Parsons JP, Hallstrand TS, Mastronarde JG, Kaminsky DA, Rundell KW, Hull JH, et al. An official American Thoracic Society clinical practice guideline: exercise-induced bronchoconstriction. Am J Respir Crit Care Med. (2013) 187:1016–27. doi: 10.1164/rccm.201303-0437ST
5. Christensen PM, Thomsen SF, Rasmussen N, Backer V. Exercise-induced laryngeal obstructions: prevalence and symptoms in the general public. Eur Arch Otorhinolaryngol. (2011). doi: 10.1007/s00405-011-1612-0
6. Johansson H, Norlander K, Berglund L, Janson C, Malinovschi A, Nordvall L, et al. Prevalence of exercise-induced bronchoconstriction and exercise-induced laryngeal obstruction in a general adolescent population. Thorax. (2015) 70:57–63. doi: 10.1136/thoraxjnl-2014-205738
7. Weiler JM, Brannan JD, Randolph CC, Hallstrand TS, Parsons J, Silvers W, et al. Exercise-induced bronchoconstriction update-2016. J Allergy Clin Immunol. (2016) 138:1292–1295.e1236. doi: 10.1016/j.jaci.2016.05.029
8. Wanrooij VH, Willeboordse M, Dompeling E, van de Kant KD. Exercise training in children with asthma: a systematic review. Br J Sports Med. (2014) 48:1024–31. doi: 10.1136/bjsports-2012-091347
9. Del Giacco SR, Firinu D, Bjermer L, Carlsen KH. Exercise and asthma: an overview. Eur Clin Resp J. (2015) 2:27984. doi: 10.3402/ecrj.v2.27984
10. Keeley DJ, Silverman M. Issues at the interface between primary and secondary care in the management of common respiratory disease2: are we too ready to diagnose asthma in children? Thorax. (1999) 54:625–8. doi: 10.1136/thx.54.7.625
11. Bush A, Fleming L. Is asthma overdiagnosed? Arch Dis Child. (2016). doi: 10.1136/archdischild-2015-309053
12. Looijmans-van den Akker I, van Luijn K, Verheij T. Overdiagnosis of asthma in children in primary care: a retrospective analysis. Br J General Pract. (2016) 66:e152–157. doi: 10.3399/bjgp16X683965
13. Hurbis CG, Schild JA. Laryngeal changes during exercise and exercise-induced asthma. Ann Otol Rhinol Laryngol. (1991) 100:34–7. doi: 10.1177/000348949110000106
14. England SJ, Bartlett D Jr. Changes in respiratory movements of the human vocal cords during hyperpnea. J Appl Physiol. (1982) 52:780–5. doi: 10.1152/jappl.1982.52.3.780
15. Carlsen KH, Anderson SD, Bjermer L, Bonini S, Brusasco V, Canonica W, et al. Exercise-induced asthma, respiratory and allergic disorders in elite athletes: epidemiology, mechanisms and diagnosis: part I of the report from the Joint Task Force of the European Respiratory Society (ERS) and the European Academy of Allergy and Clinical Immunology (EAACI) in cooperation with GA2LEN. Allergy. (2008) 63:387–403. doi: 10.1111/j.1398-9995.2008.01662.x
16. McIntosh C, Clemm HH, Sewry N, Hrubos-Strom H, Schwellnus MP. Diagnosis and management of nasal obstruction in the athlete. A narrative review by subgroup B of the IOC Consensus Group on “Acute Respiratory Illness in the Athlete”. J Sports Med Phys Fitness. (2021) 61:1144–58. doi: 10.23736/S0022-4707.21.12821-X
18. Illi SK, Held U, Frank I, Spengler CM. Effect of respiratory muscle training on exercise performance in healthy individuals: a systematic review and meta-analysis. Sports Med. (2012). 42:707–724. doi: 10.2165/11631670-000000000-00000
19. Panchasara B, Nelson C, Niven R, Ward S, Hull JH. Lesson of the month: Rowing-induced laryngeal obstruction: a novel cause of exertional dyspnoea: characterised by direct laryngoscopy. Thorax. (2015) 70:95–7. doi: 10.1136/thoraxjnl-2014-205773
20. Naito A, Niimi S. The larynx during exercise. Laryngoscope. (2000) 110:1147–50. doi: 10.1097/00005537-200007000-00015
21. de Benedictis D, Bush A. Asthma in adolescence: is there any news? Pediatr Pulmonol. (2017) 52:129–38. doi: 10.1002/ppul.23498
22. Global, Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2021. Available online at: http://www.ginasthma.org (accessed October 22, 2021).
23. Couto M, Kurowski M, Moreira A, Bullens DM, Carlsen KH, Delgado L, et al. Mechanisms of exercise-induced bronchoconstriction in athletes: current perspectives and future challenges. Allergy. (2018) 73:8–16. doi: 10.1111/all.13224
24. Levai IK, Hull JH, Loosemore M, Greenwell J, Whyte G, Dickinson JW. Environmental influence on the prevalence and pattern of airway dysfunction in elite athletes. Respirology. (2016) 21:1391–6. doi: 10.1111/resp.12859
25. Bougault V, Turmel J, St-Laurent J, Bertrand M, Boulet LP. Asthma, airway inflammation and epithelial damage in swimmers and cold-air athletes. Eur Resp J. (2009) 33:740–6. doi: 10.1183/09031936.00117708
26. Rundell KW, Smoliga JM, Bougault V. Exercise-induced bronchoconstriction and the air we breathe. Immunol Allerg Clinics. (2018) 38:183–204. doi: 10.1016/j.iac.2018.01.009
27. Hallstrand TS, Moody MW, Wurfel MM, Schwartz LB, Henderson WR Jr., Aitken ML. Inflammatory basis of exercise-induced bronchoconstriction. Am J Resp Critic Care Med.. (2005) 172:679–86. doi: 10.1164/rccm.200412-1667OC
28. Kippelen P, Anderson SD. Pathogenesis of exercise-induced bronchoconstriction. Immunol. Allergy Clin North Am. (2013) 33:299–312, vii. doi: 10.1016/j.iac.2013.02.002
29. Stang J, Stensrud T, Mowinckel P, Carlsen KH. Parasympathetic activity and bronchial hyperresponsiveness in athletes. Med Sci Sports Exerc. (2016) 48:2100–7. doi: 10.1249/MSS.0000000000001008
30. Stang J, Couto M, Carlsen KH, Stensrud T. Increased bronchial parasympathetic tone in elite cross-country and biathlon skiers: a randomised crossover study. Br J Sports Med. (2014) 49:56–61. doi: 10.1136/bjsports-2014-094053
31. Rundell KW, Im J, Mayers LB, Wilber RL, Szmedra L, Schmitz HR. Self-reported symptoms and exercise-induced asthma in the elite athlete. Med Sci Sports Exerc. (2001) 33:208–13. doi: 10.1097/00005768-200102000-00006
32. Akker IL, van der Zeijden H, Verheij TJ. Is spirometry essential in diagnosing asthma? Yes. Br J General Pract. (2016) 66:484. doi: 10.3399/bjgp16X686953
33. Cockcroft DW. Direct challenge tests: airway hyperresponsiveness in asthma: its measurement and clinical significance. Chest. (2010) 138(2 Suppl):18s–24s. doi: 10.1378/chest.10-0088
34. Daviskas E, Gonda I, Anderson SD. Local airway heat and water vapour losses. Respir Physiol. (1991) 84:115–32. doi: 10.1016/0034-5687(91)90023-C
35. Clemm HH, Engeseth M, Vollsaeter M, Kotecha S, Halvorsen T. Bronchial hyper-responsiveness after preterm birth. Paediatr Respir Rev. (2017). doi: 10.1016/j.prrv.2017.06.010
36. Anderson SD, Argyros GJ, Magnussen H, Holzer K. Provocation by eucapnic voluntary hyperpnoea to identify exercise induced bronchoconstriction. Br J Sports Med. (2001) 35:344–7. doi: 10.1136/bjsm.35.5.344
37. Hull JH, Ansley L, Price OJ, Dickinson JW, Bonini M. Eucapnic voluntary hyperpnea: gold standard for diagnosing exercise-induced bronchoconstriction in athletes? Sports Med. (2016) 46:1083–93. doi: 10.1007/s40279-016-0491-3
38. Kennedy MD, Steele AR, Parent EC, Steinback CD. Cold air exercise screening for exercise induced bronchoconstriction in cold weather athletes. Respir Physiol Neurobiol. (2019) 269:103262. doi: 10.1016/j.resp.2019.103262
39. Carlsen KH, Carlsen KC. Exercise-induced asthma. Paediatr Respir Rev. (2002) 3:154–60. doi: 10.1016/S1526-0550(02)00009-4
40. Roksund OD, Maat RC, Heimdal JH, Olofsson J, Skadberg BT, Halvorsen T. Exercise induced dyspnea in the young. Larynx as the bottleneck of the airways. Respir Med. (2009) 103:1911–8. doi: 10.1016/j.rmed.2009.05.024
41. Hull JH. Not all wheeze is asthma: time for patients to exercise their rights. Thorax. (2015) 70:7–8. doi: 10.1136/thoraxjnl-2014-206096
42. Christensen PM, Heimdal JH, Christopher KL, Bucca C, Cantarella G, Friedrich G, et al. ERS/ELS/ACCP 2013 international consensus conference nomenclature on inducible laryngeal obstructions. Eur Respir Rev. (2015) 24:445–50. doi: 10.1183/16000617.00006513
43. Christopher KL, Morris MJ. Vocal cord dysfunction, paradoxic vocal fold motion, or laryngomalacia? Our understanding requires an interdisciplinary approach. Otolaryngol Clin North Am. (2010) 43:43–66, viii. doi: 10.1016/j.otc.2009.12.002
44. Petcu LG, Sasaki CT. Laryngeal anatomy and physiology. Clin Chest Med. (1991) 12:415–23. doi: 10.1016/S0272-5231(21)00793-0
45. Fajdiga I. Snoring imaging: could Bernoulli explain it all? Chest. (2005) 128:896–901. doi: 10.1378/chest.128.2.896
46. Bent JP III, Miller DA, Kim JW, Bauman NM, Wilson JS, Smith RJ. Pediatric exercise-induced laryngomalacia. Ann Otol Rhinol Laryngol. (1996) 105:169–75. doi: 10.1177/000348949610500301
47. Roksund OD, Heimdal JH, Clemm H, Vollsaeter M, Halvorsen T. Exercise inducible laryngeal obstruction: diagnostics and management. Paediatr Respir Rev. (2017) 21:86–94. doi: 10.1016/j.prrv.2016.07.003
48. Heimdal JH, Roksund OD, Halvorsen T, Skadberg BT, Olofsson J. Continuous laryngoscopy exercise test: a method for visualizing laryngeal dysfunction during exercise. Laryngoscope. (2006) 116:52–7. doi: 10.1097/01.mlg.0000184528.16229.ba
49. Dion GR, Eller RL, Thomas RF. Diagnosing aerodynamic supraglottic collapse with rest and exercise flexible laryngoscopy. J Voice. (2012) 26:779–84. doi: 10.1016/j.jvoice.2012.01.004
50. Nielsen EW, Hull JH, Backer V. High prevalence of exercise-induced laryngeal obstruction in athletes. Med Sci Sports Exerc. (2013) 45:2030–5. doi: 10.1249/MSS.0b013e318298b19a
51. Maat RC, Røksund OD, Halvorsen T, Skadberg BT, Olofsson J, Ellingsen TA, et al. Audiovisual assessment of exercise-induced laryngeal obstruction: reliability and validity of observations. Eur Arch Otorhinolaryngol. (2009) 266:1929–36. doi: 10.1007/s00405-009-1030-8
52. Sandnes A, Andersen T, Clemm HH, Hilland M, Vollsæter M, Heimdal JH, et al. Exercise-induced laryngeal obstruction in athletes treated with inspiratory muscle training. BMJ Open Sport Exerc Med. (2019) 5:e000436. doi: 10.1136/bmjsem-2018-000436
53. Sandnes A, Hilland M, Vollsaeter M, Andersen T, Engesæter IØ, Sandvik L, et al. Severe exercise-induced laryngeal obstruction treated with supraglottoplasty. Front Surg. (2019) 6:44. doi: 10.3389/fsurg.2019.00044
54. Walsted ES, Hull JH, Sverrild A, Porsbjerg C, Backer V. Bronchial provocation testing does not detect exercise-induced laryngeal obstruction. J Asthma. (2017) 54:77–83. doi: 10.1080/02770903.2016.1195843
55. Halvorsen TWES, Bucca C, Bush A, Cantarella G, Friedrich G, Felix JF, et al. Inducible laryngeal obstruction: an official joint European Respiratory Society and European Laryngological Society statement. Eur Resp J. (2017) 50:2221. doi: 10.1183/13993003.02221-2016
56. Shembel AC, Sandage MJ, Verdolini Abbott K. Episodic laryngeal breathing disorders: literature review and proposal of preliminary theoretical framework. J Voice. (2017) 31:125.e127–e116. doi: 10.1016/j.jvoice.2015.11.027
57. Rundell KW, Spiering BA. Inspiratory stridor in elite athletes. Chest. (2003) 123:468–74. doi: 10.1378/chest.123.2.468
58. Ersson K, Mallmin E, Malinovschi A, Norlander K, Johansson H, Nordang L. Prevalence of exercise-induced bronchoconstriction and laryngeal obstruction in adolescent athletes. Pediatr Pulmonol. (2020) 55:3509–16. doi: 10.1002/ppul.25104
59. Walsted ES, Famokunwa B, Andersen L, Rubak SL, Buchvald F, Pedersen L, et al. Characteristics and impact of exercise-induced laryngeal obstruction: an international perspective. ERJ Open Res. (2021) 7:195. doi: 10.1183/23120541.00195-2021
60. Shay EO, Sayad E, Milstein CF. Exercise-induced laryngeal obstruction (EILO) in children and young adults: from referral to diagnosis. Laryngoscope. (2020) 130:E400–e406. doi: 10.1002/lary.28276
61. Lakin RC, Metzger WJ, Haughey BH. Upper airway obstruction presenting as exercise-induced asthma. Chest. (1984) 86:499–501. doi: 10.1378/chest.86.3.499
62. Rogers JH, Stell PM. Paradoxical movement of the vocal cords as a cause of stridor. J Laryngol Otol. (1978) 92:157–8. doi: 10.1017/S0022215100085169
63. Landwehr LP, Wood RP, Blager FB, Milgrom H. Vocal cord dysfunction mimicking exercise-induced bronchospasm in adolescents. Pediatrics. (1996) 98:971–4. doi: 10.1542/peds.98.5.971
64. Newman KB, Mason UG III, Schmaling KB. Clinical features of vocal cord dysfunction. Am J Respir Crit Care Med. (1995) 152:1382–6. doi: 10.1164/ajrccm.152.4.7551399
65. McFadden ER Jr., Zawadski DK. Vocal cord dysfunction masquerading as exercise-induced asthma a physiologic cause for “choking” during athletic activities. Am J Respir Crit Care Med. (1996) 153:942–7. doi: 10.1164/ajrccm.153.3.8630577
66. Wilson JJ, Wilson EM. Practical management: vocal cord dysfunction in athletes. Clin J Sport Med. (2006) 16:357–60. doi: 10.1097/00042752-200607000-00014
67. Rundell KW, Anderson SD, Spiering BA, Judelson DA. Field exercise vs laboratory eucapnic voluntary hyperventilation to identify airway hyperresponsiveness in elite cold weather athletes. Chest. (2004) 125:909–15. doi: 10.1378/chest.125.3.909
68. Stensrud T, Mykland KV, Gabrielsen K, Carlsen K-H. Bronchial hyperresponsiveness in skiers: field test versus methacholine provocation? Med Sci Sports Exerc. (2007) 39:1681–6. doi: 10.1249/mss.0b013e31813738ac
69. Haby MM, Peat JK, Mellis CM, Anderson SD, Woolcock AJ. An exercise challenge for epidemiological studies of childhood asthma: validity and repeatability. Eur Respir J. (1995) 8:729–36.
70. Vilozni D, Bentur L, Efrati O, Barak A, Szeinberg A, Shoseyov D, et al. Exercise challenge test in 3- to 6-year-old asthmatic children. Chest. (2007) 132:497–503. doi: 10.1378/chest.07-0052
71. Buchvald F, Phillipsen LD, Hjuler T, Nielsen KG. Exercise-induced inspiratory symptoms in school children. Pediatr Pulmonol. (2016) 51:1200–5. doi: 10.1002/ppul.23530
72. van Leeuwen JC, Driessen JM, de Jongh FH, Anderson SD, Thio BJ. Measuring breakthrough exercise-induced bronchoconstriction in young asthmatic children using a jumping castle. J Allergy Clin Immunol. (2013) 131:1427–1429.e1425. doi: 10.1016/j.jaci.2012.10.014
73. Anderson SD, Silverman M, Tai E, Godfrey S. Specificity of exercise in exercise-induced asthma. Br Med J. (1971) 4:814–5. doi: 10.1136/bmj.4.5790.814-c
74. Wassermann Karlmann HJ, Sue DY, Stringer WW, Sietsema KE, Sun XG, Whipp BJ. Principles of Exercise Testing and Interpretation, Fifth Edition. Wolters Kluwer: Alphen aan den Rijn (2012).
75. Weinstein DJ, Hull JE, Ritchie BL, Hayes JA, Morris MJ. Exercise-associated excessive dynamic airway collapse in military personnel. Ann Am Thorac Soc. (2016) 13:1476–82. doi: 10.1513/AnnalsATS.201512-790OC
Keywords: exercise, shortness breath, young, exercise-induced bronchoconstriction (EIB), exercise-induced laryngeal obstruction (EILO)
Citation: Vollsæter M, Stensrud T, Maat R, Halvorsen T, Røksund OD, Sandnes A and Clemm H (2022) Exercise Related Respiratory Problems in the Young—Is It Exercise-Induced Bronchoconstriction or Laryngeal Obstruction? Front. Pediatr. 9:800073. doi: 10.3389/fped.2021.800073
Received: 22 October 2021; Accepted: 09 December 2021;
Published: 03 January 2022.
Edited by:
Jean Driessen, Hanze University of Applied Sciences, NetherlandsReviewed by:
Emil Schwarz Walsted, Bispebjerg Hospital, DenmarkCopyright © 2022 Vollsæter, Stensrud, Maat, Halvorsen, Røksund, Sandnes and Clemm. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Vollsæter, bWFyaWEudm9sbHNldGVyQGhlbHNlLWJlcmdlbi5ubw==
†ORCID: Trine Stensrud orcid.org/0000-0002-5250-525X
Thomas Halvorsen orcid.org/0000-0003-1471-0225
Hege Clemm orcid.org/0000-0002-0096-4032
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.