 Birgit Böhm
Birgit Böhm Hannah Kirchhuebel
Hannah Kirchhuebel Julia Elmenhorst
Julia Elmenhorst Jan Müller
Jan Müller Renate Oberhoffer-Fritz
Renate Oberhoffer-Fritz- Department of Sport and Health Sciences, Institute of Preventive Pediatrics, Technical University Munich, Munich, Germany
Background: Endothelial function by flow-mediated dilatation assesses early markers of atherosclerotic progression. Greater amounts of physical activity and physical fitness in children are associated with cardiovascular health benefits. We aimed to explore factors, influencing endothelial function and arterial compliance in a cohort of healthy school children.
Methods: The 94 participants (41 girls, 53 boys) in the study were young, healthy children from a German school cohort. Anthropometric data, body composition and blood pressure were assessed. Blood was drawn (8 h overnight fast), assessing total cholesterol, high density lipoprotein and low density lipoprotein and triglycerides. Endothelial function was diagnosed by flow-mediated dilatation with ultrasonography (ALOKA/Hitachi, Prosound alpha 6). Tracking gates were set on the intima in B-mode. The waveform of diameter changes over the cardiac cycle was displayed in real time using the FMD-mode of the eTRACKING system. Changes in arterial diameter at baseline, ischaemia and vasodilatation were measured. A symptom limited pulmonary exercise test on a bicycle ergometer was performed to test cardiorespiratory fitness. Physical activity was assessed using GT3x accelerometers (Actigraph, USA), over 4 days (including 1 week-end day), with a minimum wear-time duration of 10 h.
Results: The median age was 12.2 years (11.8–12.8). Children were normal weight, blood lipid profiles (cholesterol, high-density lipoprotein, low-density lipoprotein, triglyceride) were in normal range. Baseline measurements during the diagnostics of endothelial function revealed higher arterial compliance of the brachial artery in boys. Boys' cardiorespiratory fitness was higher than compared to girls. Boys met the recommendations of 60 min moderate to vigorous activity, whereas girls were significantly less active and did not meet current recommendations. More time spent in sedentary activity was the main predictor for lower arterial compliance (adjusted for age and sex), accounting for 14% of the variance. No significant model revealed, analyzing the influencing factors such as anthropometric data, blood lipids, physical activity and fitness on endothelial function.
Conclusion: This is the first study on endothelial function in association to objectively measured physical activity and cardiorespiratory fitness in healthy school children in Germany. The study highlights the importance of reducing time spent being sedentary to maintain endothelial health.
Introduction
Cardiovascular (CV) dysfunction, contributing to myocardial infarction, heart failure and stroke is one of the major cause of death in today's society worldwide (1). Increased arterial compliance and impairment of arterial endothelial function play an important role in the development of atheroclerosis and are strong predictors of CV events independent of traditional risk factors in adulthood (2, 3). Several pediatric studies have already reported reduced endothelial function (FMD) in children and adolescents at risk for atherosclerotic CV disease (4, 5).
High-frequency ultrasound is considered the gold standard for assessment of endothelial function in both adults (6, 7) and children (6).
Several studies have shown a relationship between cardiorespiratory fitness (CRF) and arterial compliance (8, 9). Veijalainen et al., for example, have given evidence that limited CRF is related to lower arterial compliance and higher arterial stiffness (10) measured by pulse wave velocity between carotid and femoral arteries. Equally important, it has been proven that physical activity may have a positive effect on reducing the blood pressure and the arterial stiffness in older adults (11, 12). It reduces the risk of cardiovascular diseases and has potential benefit on improved endothelial function (9).
Also, in obese children, it has been shown that the endothelial cell function can be improved significantly through a 12-week after school activity program. The school exercise intervention program leads to an improvement of vascular repair and endothelial cell function, leading toward an improved cardiovascular health (13). Similar relationships between exercise and vascular function in overweight children and adolescents are stated in the studies of Watts et al. and Woo et al. (14, 15).
The underlying mechanisms behind arterial remodeling seem to be complex. Factors such as shear stress, inflammation, sympathetic drive and oxidative stress lead to changes in cell signaling (16, 17). Especially the increased bioavailability of nitric oxide activated by signaling pathways after physical activity plays an important role in improving arterial compliance (18). The impact of exercise may be associated with the balance between reactive oxygen species (ROS) and the antioxidant defenses which influence the availability of nitric oxide (19).
Although the relationship between physical activity and arterial stiffness is complicated, the results of the studies mentioned above have given reasonable evidence regarding the positive effects of exercise training on arterial compliance. Reasoning based on these outcomes (20), reducing the cardiovascular risk factors may also be beneficial for children and prevent them from developing atherosclerosis.
However, studies investigating the associations between physical fitness, physical activity and arterial compliance and endothelial function in healthy children are limited. Currently no data in endothelial function in a German school children cohort exist.
Moreover, little is known of the effects of time spent being sedentary on arterial compliance and endothelial function in healthy children.
Therefore, our primary objective was to explore the factors influencing endothelial function, arterial compliance in a cohort of healthy school children and to quantify associations between physical fitness, physical activity, arterial compliance and endothelial function.
Our secondary objective was to examine possible sex differences on cardiorespiratory fitness and the amount of physical activity in different intensity levels in boys and girls in Germany. Girls are known to be less physically active than boys (21, 22) and spend less time in moderate to vigorous physical activity (23). A German cohort study further described lower physical fitness of girls compared to boys (24, 25). Earlier research of our study group demonstrated sex differences on A. carotid structure in healthy children (26). Further associations between physical activity intensity levels and arterial stiffness measured by pulse wave velocity have been described (27). It is, therefore, possible that endothelial function and arterial compliance may differ by childhood sex.
Materials and Methods
Study Design and Study Population
Data collection was part of the “Get fit-stay healthy” project funded by the German Heart Foundation, a prospective study conducted in Bavaria, Germany that already started in 2013. The study focused on cardiovascular risk screening in healthy children and adolescents with the main emphasis on arterial structure and function as well as endothelial function. Ethic approval was obtained from the Ethics Committee of the Faculty of Medicine, Technical University Munich (project number: 4027/11). All data were assessed prior to the Covid-19 pandemic, with lock down restrictions in Germany from March 2020 onwards. Data analysis took part between 2017 and 2019. All pupils (n =1 54) children from sixth grade of the participating school were asked to participate in the study. N = 105 volunteered to participate in the study. Written informed consent was given by the participating children and their guardians.
Examination Process at the School
The study was performed under laboratory conditions in the medical room of the school. The room was quiet and temperature controlled. Temperature during diagnostics were 22°C (range 21–25°C, with a little ventilation if needed).
On the day of the examination the children were asked to come to school in a fasting state (8–10 h overnight fasting). The diagnostic routine started with the assessment of body composition, followed by blood collection and the diagnostic of endothelial function. The time of examination for body composition, blood collection and endothelial function was in the mornings between 7:30 and 11 am. After that the children had a light breakfast consistent of a banana and cereal, apple or orange juice and mineral water. The cardiovascular fitness test was performed later on the same day, in the same room with at least 1 h rest after breakfast. Finally, children were handed out the accelerometer which they wore for 7 days to objectively assess their physical activity.
Assessment of Body Composition and Blood Pressure
Anthropometric measurements were assessed by trained staff according to standardized guidelines (28). Portable scales and stadiometers (Seca 799, MedicallLine, Hamburg, Germany) were used for quantifying body weight to the nearest 0.1 kg (in light sports clothing) and height to the nearest 0.1 cm. A non-flexible tape (Seca 201, Hamburg, Germany) was used for the measurement of waist circumference at the middle between last rib and the anterior superior iliac spine at the midclavicular line and of hip circumference at the anterior superior iliac spine. The body mass index (BMI) was calculated as weight in kilograms divided by height in meters-squared and converted into z-scores using the reference values of a German cohort (29). According to the German Obesity Association childhood overweight was defined as a BMI between 90th and 97th percentile, obesity was defined as a BMI greater than the 97th percentile for children with the same age and sex. Underweight was defined as a BMI <10th percentile (29).
Peripheral systolic and diastolic blood pressure were measured non-invasively at rest with a Mobil-O-Graph (IEM, Healthcare, Stolberg, Germany). Blood pressure measurements were performed on the left arm with the children in supine position. In order to select the appropriate arm cuff, subjects' arm circumferences were assessed before starting the tests.
Cuffs were chosen according to the measured left upper arm circumference (five different cuff sizes were used: 14–20 cm/20–24 cm/24–32 cm/32–38 cm/38–55 cm). The Mobil-O-Graph has already been validated for measurement of peripheral blood pressure (30, 31) and 24h ABPM (ambulatory blood pressure measurement) according to the BHS and ESH criteria (32, 33). Values were classified according to German age and sex specific norm values (20, 34).
Laboratory Analysis
Blood was collected after at least an 8 h overnight fast in different tubes (Sarstedt, Nümbrecht, Germany) for preparation of serum or EDTA-plasma samples. All samples were processed within 2 h after sampling. If tests were not performed within the same day, the samples were stored frozen at −40°C. A complete blood count including reticulocytes was measured in EDTA-anticoagulated whole blood (Sysmex XE-5000). Total cholesterol, HDL-C, and triglycerides were assessed using routine methods on a Cobas Integra 800 analyzer (Roche Diagnostics, Mannheim, Germany). LDL-C was calculated according to Friedewald's formula (35).
Measurements of Endothelial Function
Before initiating the diagnostic of endothelial function by flow-mediated dilatation (FMD) the examination was explained to the children. Children laid down in a supine position and rested for at least 10 min to guarantee stable conditions during measurement. The right arm was extended and immobilized with foam supports to guarantee a comfortable position. Since the A. brachialis is located medially, the arm is slightly turned outside (supination) to allow consistent imaging of the brachial artery.
Vascular endothelial function of the right brachial artery (BA) was studied with ultrasonography (Aloka/Hitachi, Prosound alpha 6) with a high-frequency (5–13 MHz) linear-array transducer. Mean arterial pressure was determined from the Mobil-O-Graph on the contralateral arm. The transducer was placed in the distal third of the upper arm to image the brachial artery. Tracking gates were set on the intima in B-mode, the artery resulting tracking lines, indicating the tracking position, are presented on the monitor in M-mode. The waveform of diameter changes over the cardiac cycle was displayed in real time using the FMD-mode of the eTRACKING system.
Changes in arterial diameter at baseline (1 min), ischaemia (5 min) and vasodilatation (2 min) were measured. Ischemia was developed by a blood pressure cuff placed around the forearm inflated to a pressure of 220 mmHg. After 5 min the cuff was deflated, causing increased flow-mediated vasodilatation. Peak artery diameter and the time taken to reach the maximal diameter after the release of the cuff, were recorded. From these data, FMD%, an index indicating the percentage dilated at the maximum vessel diameter in peak vasodilatation after cuff deflation, relative to maximum vessel diameter at baseline, was calculated. BA distensibility was defined by arterial compliance (AC), pressure strain elastic modulus (Ep), and PWV ß according to the following formula.
AC describes the ability of an artery to change its volume due to a given change in arterial blood pressure. The compliance is calculated from the diameter of the blood vessel (D) and BP.
AC = π(Dmax2-Dmin2)/[4(BPmax-BPmin)]
Pressure strain elastic modulus (Ep) is the ratio of stress and strain on the arterial wall and measures the intrinsic stiffness (Moo). An increase in stiffness leads to a higher Ep value.
Ep=(BPmax-BPmin)/[Dmax-Dmin)/Dmin]
Beta-Index (ß) is another parameter to depict arterial stiffness. The higher the ß-Index, the lower is the arterial elasticity.
B= ln(BPmax/BPmin)/[Dmax-Dmin)/Dmin]
PWV is the velocity of the pressure wave transmitted between two portions of the arterial tree (36). PWV β is measured as the local pulse wave velocity of BA, calculated from β.
PWV β = √((β*BPmin)/(2p))
The echo-tracking system implemented in the ultrasound machine allows accurate measurements of diameter changes, based on radio frequencies (RF) signals, able to detect variations of the arterial diameters with a strictness of 0.01 mm (37).
Assessment of Cardiorespiratory Fitness
Physical fitness was tested via a symptom limited pulmonary exercise test on a bicycle ergometer (Geratherm Respiratory, Ganshorn Medical, Germany). Baseline values were established during 2 min of rest followed by 2 min of unloaded pedaling. Afterwards, an increase in load was achieved via a ramp-wise protocol of 30 watts per minute. Criteria for ending the test was the maximum exhaustion of the subject and a drop of cadence below 60/min. The test featured a breath to breath gas exchange using a metabolic chart (Vmax Encore 229, SensorMedics, Viasys Healthcare, Yorba Linda, California). All exercise tests with a respiratory exchange ratio of >1.0 were discharged because of insufficient effort. Peak oxygen uptake was defined as the highest mean uptake of any 30 s time interval during exercise. Reference values for age, body mass, body height and sex, expressed in “% predicted” were calculated as previously described (38).
Assessment of Physical Activity
Physical activity was assessed using GT3x accelerometers (Actigraph, USA), over 4 days (including 1 week-end day), with a minimum wear-time duration of 10 h. The accelerometer was positioned with an adjustable belt on the right iliac crest. Executive zeros over a period of 20 min were deleted. The time spent in inactivity as well as in light, moderate and vigorous PA was categorized using the cut-points per minutes (cpm) suggested by Evenson (39). Threshold counts < 100 cpm indicated physical inactivity, 101–2,295 cpm light PA, 2,296–4,011 cpm moderate PA and >4,012 cpm vigorous PA. Sedentary time was calculated as wear time–(time spent in light PA + moderate PA + vigorous PA) and total inactivity was defined as the sum of non-wear time and sedentary time. The time spent in different PA intensities was adapted for the number of days when the accelerometer was worn and expressed as minutes per day. All activity data measured by the ActiGraph GT3X+ was processed with the data analyzes software ActiLife, version 6.11.4 (ActiGraph, Pensacola, Florida, USA.
Data Analysis
Statistical analyses were conducted using IBM SPSS Statistics (Version 23). The study cohort was characterized by standard descriptive statistics. Data for boys and girls were compared using the Mann-Whitney test. Data distribution was initially examined for normality using the Kolmogorov-Smirnov test. Due to non-normal distributed variables descriptive statistics were presented as median and interquartile range.
Due to significant differences in cardiorespiratory fitness and physical activity levels we calculated potential relations between anthropometric data, blood lipids physical fitness and activity and endothelial function separately for boys and girls. Univariate analysis between the variables was calculated with the Spearman's correlation coefficients. We further performed linear regression analysis to determine the main predictors for endothelial function and arterial compliance. Independent variables of the vascular function, were FMD (%, in systole) and arterial compliance (AC). FMD was adjusted for baseline diameter in systole, age and sex, whereas arterial compliance was adjusted for age and sex. As dependent variables BMI z-score, Hip to waist ratio, systolic and diastolic blood pressure z-scores, cholesterol, HDL-LDL ratio, daily physical activity, time spent in sedentary, light moderate and vigorous activity levels, VO2max as well as Wattmax were integrated in the model as dependent variables. Criteria of normal distribution of the residuals were fulfilled so that logarithmic transformation was not necessary. Covariates were tested for collinearity. Correction for collinearity was not required as variance inflation factor (VIF) was <15. A value of p < 0.05 was considered to be statistically significant. Post hoc, compute achieved power was calculated; effect size d = 0.05; alpha error probability of 0.05; sample size of group 1 (n = 40) compared to sample size group 2 (n = 52). The outcome revealed the power (1-ß error prob = 0.745). Non-centrality parameter delta δ = 2.323, critical t = 1.662, Df = 85.85.
Results
Descriptive Characteristics in Boys and Girls
N = 105 participated in the study. Seven children were obese (n = 3 boys and n = 4 girls). Four boys demonstrated hypertensive blood pressure values. The data of these children were excluded from the analysis since they did not meet the criteria of being normal weight and normotensive. Overall, data of 94 healthy children (41 girls, 53 boys) were analyzed. Twelve children refused to have blood drawn. Two endothelial diagnostics had to be excluded due to artifacts during flow-mediated dilatation. All children did not take any medication, and did not suffer from known cardiovascular or metabolic disorder. The median age was 12.2 years (11.8–12.8). The characteristics of the sample population are displayed in Table 1.
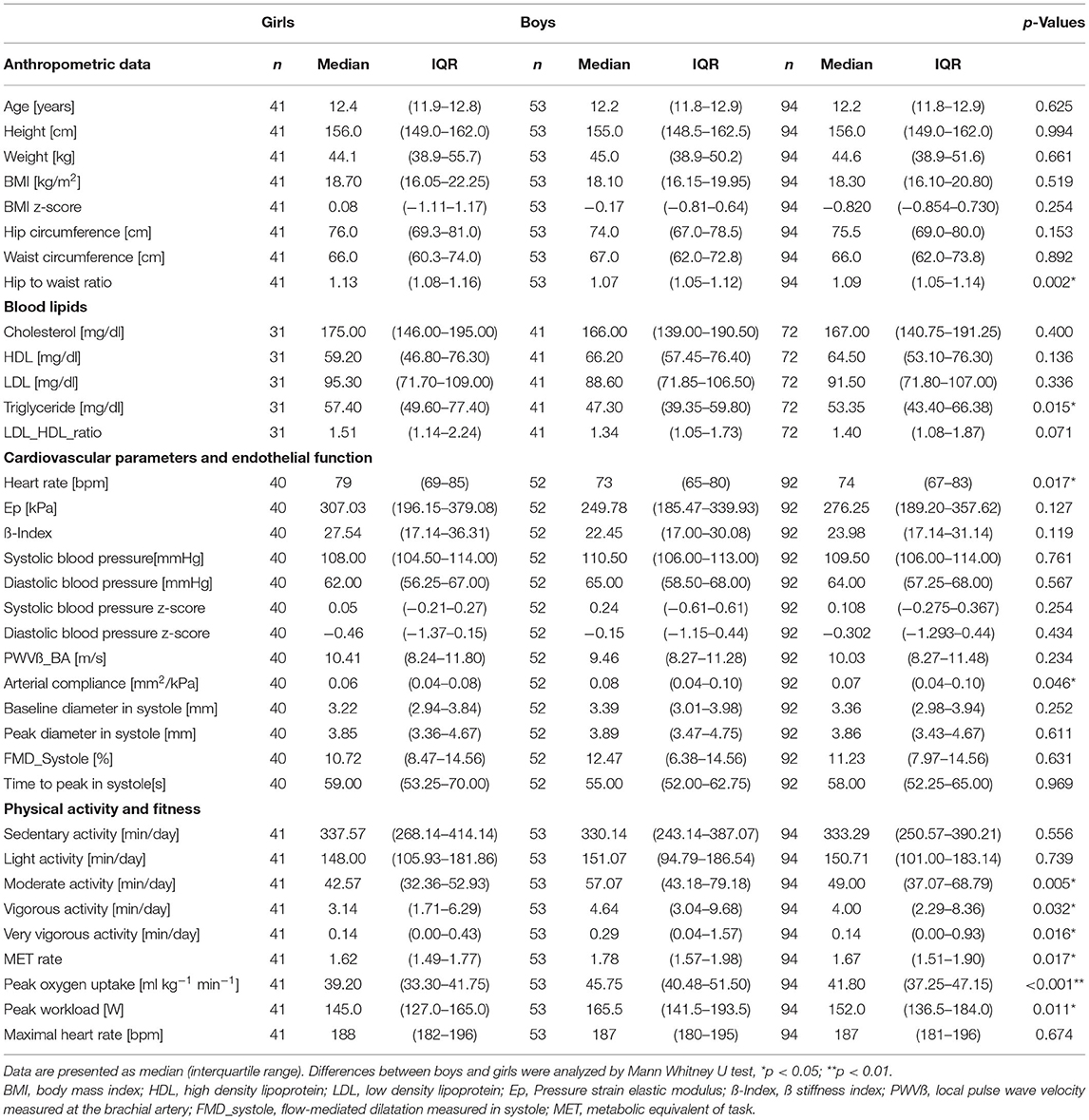
Table 1. Characteristics of the study population.
Boys and girls of the studies population did not differ in height, weight and BMI. Comparison of anthropometric differences between boys and girls only revealed a higher hip to waist ratio in girls 1.13 (1.08–1.16) compared to a 1.07 (1.05–1.17) (p = 0.002). Blood lipid profiles (cholesterol, high-density lipoprotein, low-density lipoprotein and triglyceride) were in normal range. Baseline measurements during the diagnostics of endothelial function revealed higher arterial compliance of the brachial artery in boys (p = 0.046) combined with a significantly lower heart rate at rest (p = 0.017), before cuff inflation. Boys also demonstrated higher VO2max (p < 0.001) and Wattmax values (p = 0.011) during the cardiopulmonary exercise test than girls. All children reached their age and sex-specific norm values during the symptom limited pulmonary exercise test on a bicycle ergometer (38). There was no difference between maximum heart rate in boys compared to girls.
Regarding the physical activity level of the children, boys spent significantly more time doing moderate-intensity (p = 0.005), vigorous-intensity (p = 0.032) and very vigorous-intensity physical activity (p = 0.016), respectively. The median time spent in moderate- to vigorous-intensity physical activity was 61.71 min a day (IQR, 46.21–88.86) in boys, whereas the median time spent in moderate to vigorous activity of girls was only 45.71 min a day (IQR, 34.07–59.21).
No differences between the sex sub-groups existed in time spent being sedentary and the amount of time spent in light-intensity physical activity level. Overall, boys had a higher MET rate (p = 0.017).
Relationships Between Anthropometric Data, Blood Lipids Physical Fitness, Physical Activity and Endothelial Function
Associations between anthropometric parameters, blood lipids physical fitness, physical activity, arterial compliance and endothelial function were analyzed for boys and girls as well as for the total study group. Results are displayed in Table 2.
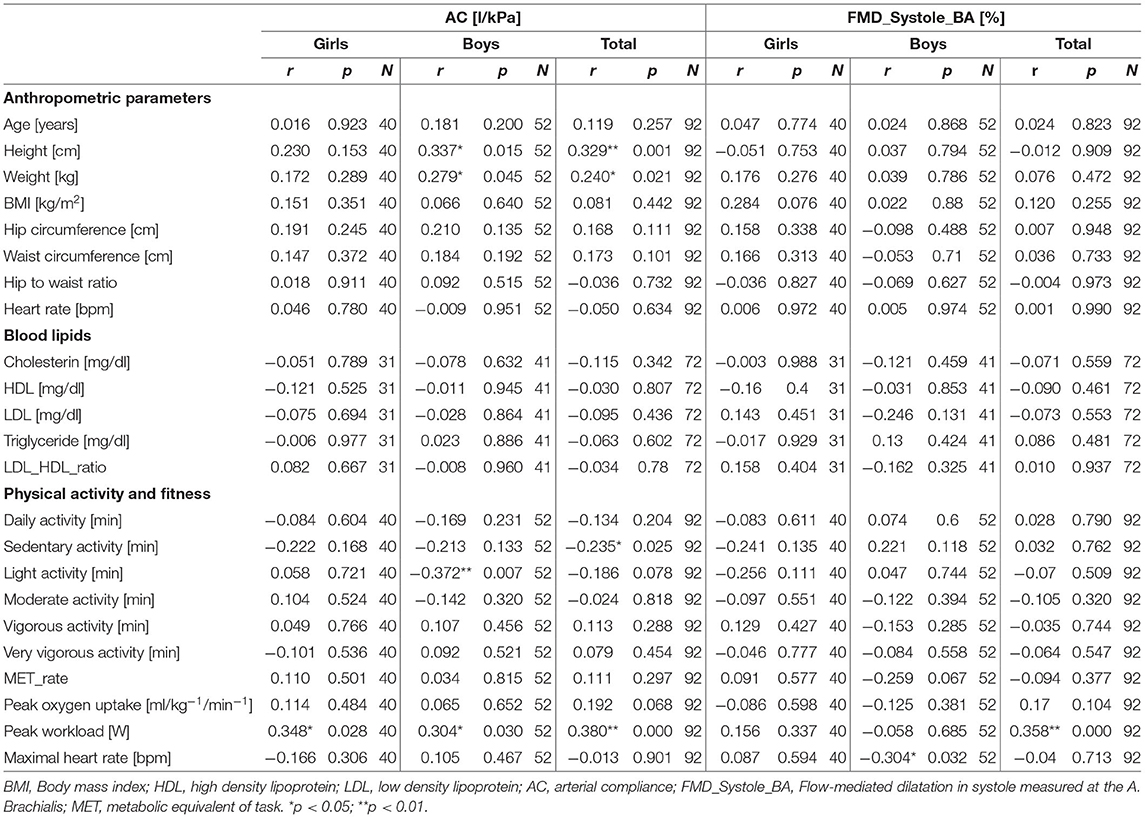
Table 2. Relationships between anthropometric parameters, blood lipids, physical activity and fitness and arterial compliance (AC) and flow-mediated dilatation at time of systole (FMD_Systole_BA).
In boys, height was positively associated to AC (r = 0.337, p = 0.015), and weight (r = 0.279, p = 0.045) demonstrated a positive relation to AC. Better physical fitness, especially the maximal workload was positively correlated to AC (r = 0.304, p = 0.030). Regarding the amount physical activity, more time spent in light activity was negatively correlated to AC (r = −0.372, p = 0.007). A negative correlation was observed between FMD% and the maximum heart rate in boys (r = −0.304, p = 0.032).
An indicator for physical strengths and fitness is the performance measured in Watt during the cardiorespiratory fitness test. In girls a positive correlation was observed between the maximum workload (Watt) and AC (r = 0.348, p = 0.028).
No associations revealed between parameters of arterial stiffness and endothelial function with the blood lipid profiles.
Predictors for Arterial Compliance and Endothelial Function
Next to the calculation of associations, we further assessed the main influencing factors for arterial compliance in children. After adjustment for age and sex (model 1), the linear regression analysis revealed that more time spent in sedentary activity (ß = −0.280, p = 0.037) was the main predictor for lower arterial compliance, accounting for 14% of the variance [R2 = 0.014, F(13,57) = 0.767]. Taking BMI and systolic blood pressure also into account the model still revealed significant (R2 = 0.0122, F(10,60) = 0.744, p = 0.027) (Table 3).
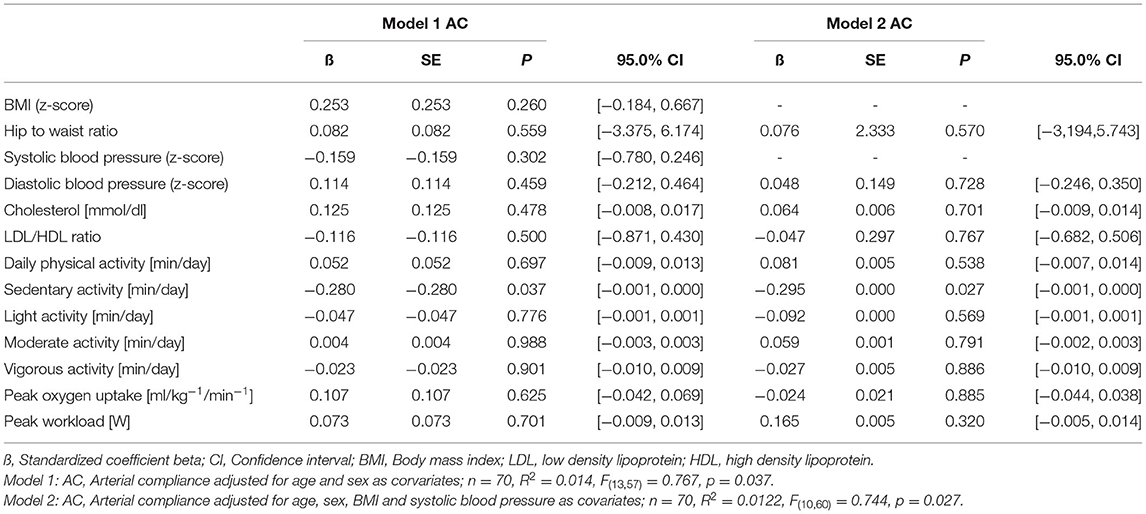
Table 3. Multivariable correlates of arterial compliance.
To determine the influencing factors for endothelial function in the total study group, FMD % in systole was adjusted for baseline diameter, age and sex (model 1) R2 = 0.098, F(13,57) = 0.479, p = 0.928 and further also adjusted for BMI and systolic blood pressure. The regression also did not analysis reveal a significant prediction model R2 = 0.077, F(11,59) = 0.449, p = 0.926 (Table 4).
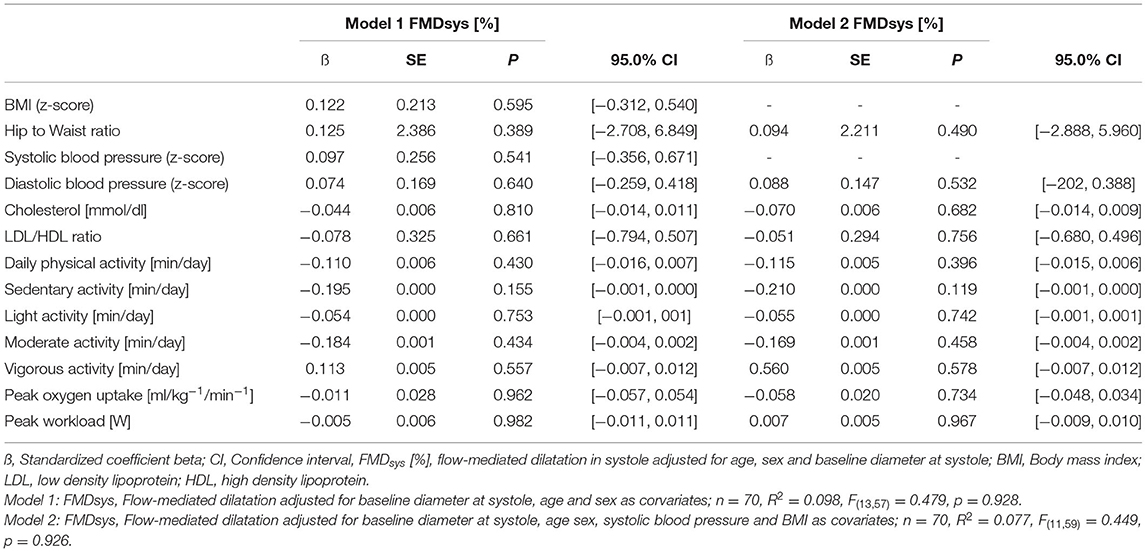
Table 4. Multivariable correlates of endothelial function measured by flow-mediated dilatation.
Discussion
The purpose of this study was to assess factors influencing the arterial compliance and endothelial function in healthy children, taking possible sex differences into account. Our data yielded two important findings:
Firstly, after adjustment for age and sex, the main predictor the amount of time spent in sedentary behavior was the main predictor for lower arterial compliance. Secondly, sex differences exist regarding physical activity levels, cardiorespiratory fitness and arterial compliance.
The Impact of Physical Activity on Arterial Compliance and Endothelial Function
Sedentary lifestyle increases the risk of prematurely developing of atherosclerosis. Regular physical activity affects endothelial function (40). The results of our study emphasize the importance of reducing and limiting the amount of time spent being sedentary, particularly the amount of recreational screen time which is recommended in the current guidelines of the World Health Organization (41). Physical activity can be described by duration of the activity and level of intensity (light, moderate, vigorous and very vigorous activity). Abbott et al. (42) described a significant relationship between physical activity and FMD%, even among a group of moderately active children. This gives credence to the importance of physical activity in early childhood. However, the underlying mechanisms behind arterial remodeling are complex. Training induces a direct impact on the vasculature (43). The pattern of blood flow and the amount of shear stress that occur during exercise may be related to the specific training characteristics, including training intensities (44). Next to moderate training intensity, high-intensity interval training is relationed to vascular function for improving the range of physiological, functional and clinical parameters, including endothelial function (45).
Children's general play and physical activity is characterized by changes in intensity levels and repeated sprint running is a natural exercise for children. A classical analysis reported that children have a preference for intermittent, explosive and intense activities of very short duration (< 15 s), which causes partly anaerobic-lactic metabolic conditions (46).
In the present study, girl's physical activity was lower than in boys. Further our data demonstrated that time spent in vigorous and very vigorous activities was significantly lower in girls than in boys. Girls only spent 45.71 min a day (IQR, 34.07–59.21) in moderate to vigorous activity and did not meet the recommendations of 60 min per day, which would confer to multiple beneficial health outcomes, such as cardiorespiratory fitness (47) cardiometabolic health (48) and cardiovascular health (49).
There is a need to reduce sedentary time and especially motivate girls to more intensive activities or to design sex-specific interventions with special attention to vigorous and very vigorous physical activity intensities in girls (e.g., ball games, robe skipping, running activities).
Favorite sports in boys (e.g., ball games and team sports such as soccer and basketball) can be defined as activities and sports with changing intensity levels similar to interval training (50).
Lower levels of physical activity have been related to stiffer arteries measured by pulse wave velocity between the femoral artery and low vascular function (51, 52).
Our findings are further in line with Veijalainen et al. (10) who observed that children with less stiff arteries have higher levels of unstructured physical activity and cardiorespiratory fitness. This was especially the case in boys whereas girls were in the opposite halve of these variables (10). However, though the authors found no associations between time spent in sedentary behavior and arterial stiffness (10), we found that time in sedentary behavior was the main predictor of lower arterial compliance, describing 14% of the evidence.
In the present study we could not demonstrate relationships between FMD and fitness after adjustment for age and sex. It has to be kept in mind that in the present population the most established risk factors for endothelial dysfunction such as smoking or hypercholesterolaemia are lacking (4). Previous studies reported data on the beneficial effect of exercise on endothelial health are most consistent in subjects with impaired endothelial function (53). One of the suggested new training types could be aerobic interval training, since data indicate that this type of training is superior in reversing endothelial dysfuction in children (54, 55).
Endothelial maximum dilatation is primarily due to endothelial cells releasing relaxing factors. To find out whether the FMD is solely dependent on the endothelium, a vasodilation through the direct action of the smooth muscles must be investigated. In adults, this is achieved by measuring vasodilation in response to glyceryl trinitrate (GTN) (42). However, it was ethically not possible to administer GTN to young healthy children in this voluntary prevention study.
In this context the time to peak is an indicator for endothelial health. Data in the present study showed that the time to peak dilation was 58 s. (sys, median) and the IQ range was 52.25–65.00 s. Our results are in line with results of Hopkins et al. who described a mean time of 60.7 (95%CI 59.0–62.5) s. to peak dilatation (56). The results are further comparable to the data of Järvisalo et al. They reported the highest mean dilation at 70.00 s. after cuff release in healthy children and adolescents (9–16 years). The majority of the subjects obtained their dilation peak diameter between 40 and 120 s, presenting a large range in response. Järvisalo et al. concluded that for true FMD peak response brachial artery diameter measurement is necessary up to 120 s. after cuff release as there is a certain variety in healthy children and adolescents (57).
Measurement of endothelial function by FMD is non-invasive, reproducible and non-painful (6), so it is particularly suitable for the investigation of young adults and children with the earliest stages of atherosclerosis, hence, providing the best opportunity for prevention (7).
Our data showed no sex differences in baseline diameter and also endothelial function, assessed by FMD was similar in both sexes. Our finding goes in line with Pahkala et al. (58). The group studied over 500 healthy boys and girls (13 years old) and reported no significant difference in endothelial function (FMD). In contrast, Hopkins et al. (56) described significant difference between boys and girls.
In this study we focused on an apparently healthy sample of school children.
Currently no reference values have been published for endothelial function assessed by FMD in children in a German cohort.
Strengths and Limitations of the Study
The major strengths of the study are that we used well established diagnostic measures for the assessment of physical examination, laboratory, ultrasound data as well as objective measurement of physical activity and cardiorespiratory fitness.
We also used established ultrasound diagnostics to assess the flow-mediated dilatation of the brachial artery as a response to a physiological stimulus (shear stress). Since we performed our diagnostics in healthy children we did not measure smooth muscle dependent vasodilatation as a response to exogenous sources of NO such as nitroglycerin due to ethical considerations. Another limitation of the study is that we did not have data on the puberty status of the children. From the possible n = 154 pupils only 68% volunteered to participate in the study. This might be due to the fact that the examinations took place in the mornings during school hours.
Conclusion
This is the first study on endothelial function in association to objectively measured physical activity and cardiorespiratory fitness in healthy school children in Germany.
Time spent in sedentary behavior was the main predictor for lower arterial compliance in healthy children. Girls were less active than boys and did not meet current WHO guidelines for moderate-intensity activity.
This highlights the importance of maintaining or making every effort to promote physical activity to an average of 60 min per day per week and to reduce time being sedentary in childhood (41). Among the lifestyle-related factors measured in the present study, time spent in sedentary behavior has a stronger effect than BMI or blood lipids or cardiovascular fitness, on lower arterial compliance in healthy children.
Future studies should consider behavior approaches to further investigate differences and preferences of physical activity in boys and girls, resulting in possible sex-specific activity interventions. Prospective studies should further deepen the knowledge of vascular adaptations with regard to different activity intensities in healthy children, resulting in a better understanding of the promotion of an active healthy lifestyle to prevent cardiovascular risk factors and endothelial dysfunction.
The promotion of an active and healthy lifestyle becomes even more important, considering the fact that the present data was collected before the corona pandemic. Due to an increased sedentary behavior and an increased lack of exercise during the pandemic, even more far-reaching effects on the health of children must be feared.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Faculty of Medicine, Technical University of Munich (project number: 4027/11). Written informed consent to participate in this study was provided by the participants' legal guardian.
Author Contributions
RO-F, BB, JE, and JM contributed to the conception and design of the study. BB was main responsible for data collection as project coordinator and drafted the manuscript. BB, JM, and JE were involved in the practical work. BB, JE, JM, and HK contributed to the statistical analysis and interpretation of the data. HK assisted drafting the manuscript and literature research. RO-F, JM, and HK critically revised the manuscript. All gave final approval and agreed to submit the work.
Funding
The study was funded by the German Heart Foundation within the project Get fit-Stay healthy–Cardiovascular risk screening in healthy German children in Bavaria. Publication of this open access article was supported by the German Research Foundation (DFG) for University libraries.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the children and their guardians for volunteer participation in the study. We further thank the participating schools for their cooperation, integrating this study within the school timetable during the mornings.
References
1. WHO. The top 10 deaths 2017. Available online at: http://www.who.int/mediacentre/factsheets/fs310/en/ (accessed May 3, 2017).
2. Ross R. The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature. (1993) 362:801–9. doi: 10.1038/362801a0
3. Han SH, Gerber TC, Suwaidi JA, Eeckhout E, Lennon R, Rubinshtein R, et al. Relationship between coronary endothelial function and coronary calcification in early atherosclerosis. Atherosclerosis. (2010) 209:197–200. doi: 10.1016/j.atherosclerosis.2009.08.027
4. Celermajer DS, Sorensen KE, Gooch VM, Spiegelhalter DJ, Miller OI, Sullivan ID, et al. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet. (1992) 340:1111–5. doi: 10.1016/0140-6736(92)93147-F
5. Urbina EM, Williams RV, Alpert BS, Collins RT, Daniels SR, Hayman L, et al. Noninvasive assessment of subclinical atherosclerosis in children and adolescents: recommendations for standard assessment for clinical research: a scientific statement from the American Heart Association. Hypertension. (2009) 54:919–50. doi: 10.1161/HYPERTENSIONAHA.109.192639
6. Slyper AH. Clinical review 168: what vascular ultrasound testing has revealed about pediatric atherogenesis, and a potential clinical role for ultrasound in pediatric risk assessment. J Clin Endocrinol Metab. (2004) 89:3089–95. doi: 10.1210/jc.2003-030644
7. Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F, Creager MA, et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. J Am Coll Cardiol. (2002) 39:257–65. doi: 10.1016/S0735-1097(01)01746-6
8. Santos-Parker JR, LaRocca TJ, Seals DR. Aerobic exercise and other healthy lifestyle factors that influence vascular aging. Adv Physiol Educ. (2014) 38:296–307. doi: 10.1152/advan.00088.2014
9. Lavie CJ, Arena R, Swift DL, Johannsen NM, Sui X, Lee DC, et al. Exercise and the cardiovascular system: clinical science and cardiovascular outcomes. Circ Res. (2015) 117:207–19. doi: 10.1161/CIRCRESAHA.117.305205
10. Veijalainen A, Tompuri T, Haapala EA, Viitasalo A, Lintu N, Vaisto J, et al. Associations of cardiorespiratory fitness, physical activity, and adiposity with arterial stiffness in children. Scand J Med Sci Sports. (2016) 26:943–50. doi: 10.1111/sms.12523
11. Vogel T, Lepretre PM, Brechat PH, Lonsdorfer-Wolf E, Kaltenbach G, Lonsdorfer J, et al. Effect of a short-term intermittent exercise-training programme on the pulse wave velocity and arterial pressure: a prospective study among 71 healthy older subjects. Int J Clin Pract. (2013) 67:420–6. doi: 10.1111/ijcp.12021
12. Yuan WX, Liu HB, Gao FS, Wang YX, Qin KR. Effects of 8-week swimming training on carotid arterial stiffness and hemodynamics in young overweight adults. Biomed Eng Online. (2016) 15:151. doi: 10.1186/s12938-016-0274-y
13. Park JH, Miyashita M, Kwon YC, Park HT, Kim EH, Park JK, et al. A 12-week after-school physical activity programme improves endothelial cell function in overweight and obese children: a randomised controlled study. BMC Pediatr. (2012) 12:111. doi: 10.1186/1471-2431-12-111
14. Woo KS, Chook P, Yu CW, Sung RY, Qiao M, Leung SS, et al. Effects of diet and exercise on obesity-related vascular dysfunction in children. Circulation. (2004) 109:1981–6. doi: 10.1161/01.CIR.0000126599.47470.BE
15. Watts K, Beye P, Siafarikas A, Davis EA, Jones TW, O'Driscoll G, et al. Exercise training normalizes vascular dysfunction and improves central adiposity in obese adolescents. J Am Coll Cardiol. (2004) 43:1823–7. doi: 10.1016/j.jacc.2004.01.032
16. Thijssen DH, Cable NT, Green DJ. Impact of exercise training on arterial wall thickness in humans. Clin Sci. (2012) 122:311–22. doi: 10.1042/CS20110469
17. Haapala EA, Vaisto J, Veijalainen A, Lintu N, Wiklund P, Westgate K, et al. Associations of objectively measured physical activity and sedentary time with arterial stiffness in pre-pubertal children. Pediatr Exerc Sci. (2017) 29:1–26. doi: 10.1123/pes.2016-0168
18. Gielen S, Schuler G, Adams V. Cardiovascular effects of exercise training: molecular mechanisms. Circulation. (2010) 122:1221–38. doi: 10.1161/CIRCULATIONAHA.110.939959
19. Green DJ, O'Driscoll G, Joyner MJ, Cable NT. Exercise and cardiovascular risk reduction: time to update the rationale for exercise? J Appl Physiol. (1985) 105:766–8. doi: 10.1152/japplphysiol.01028.2007
20. Elmenhorst J, Hulpke-Wette M, Barta C, Dalla Pozza R, Springer S, Oberhoffer R. Percentiles for central blood pressure and pulse wave velocity in children and adolescents recorded with an oscillometric device. Atherosclerosis. (2015) 238:9–16. doi: 10.1016/j.atherosclerosis.2014.11.005
21. Lampert T, Mensink GB, Romahn N, Woll A. [Physical activity among children and adolescents in Germany. Results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS)]. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz. (2007) 50:634–42. doi: 10.1007/s00103-007-0224-8
22. Schmidt SCE, Anedda B, Burchartz A, Oriwol D, Kolb S, Wasche H, et al. The physical activity of children and adolescents in Germany 2003-2017: The MoMo-study. PLoS ONE. (2020) 15:e0236117. doi: 10.1371/journal.pone.0236117
23. Kobel S, Kettner S, Lammle C, Steinacker JM. Physical activity of German children during different segments of the school day. Z Gesundh Wiss. (2017) 25:29–35. doi: 10.1007/s10389-016-0755-2
24. Woll A, Klos L, Burchartz A, Hanssen-Doose A, Niessner C, Oriwol D, et al. Cohort profile update: the motorik-modul (MoMo) longitudinal Study-physical fitness and physical activity as determinants of health development in German children and adolescents. Int J Epidemiol. (2021) 50:393–4. doi: 10.1093/ije/dyaa281
25. Woll A, Kurth BM, Opper E, Worth A, Bos K. The 'Motorik-Modul' (MoMo): physical fitness and physical activity in German children and adolescents. Eur J Pediatr. (2011) 170:1129–42. doi: 10.1007/s00431-010-1391-4
26. Bohm B, Hartmann K, Buck M, Oberhoffer R. Sex differences of carotid intima-media thickness in healthy children and adolescents. Atherosclerosis. (2009) 206:458–63. doi: 10.1016/j.atherosclerosis.2009.03.016
27. Heil L, Oberhoffer R, Bohm B. Association between physical activity intensity levels and arterial stiffness in healthy children. J Phys Act Health. (2020) 17:933–9. doi: 10.1123/jpah.2019-0594
28. WHO. Waist Circumference and Waist-hip Ratio: Report of a WHO Expert Consultation Geneva. (2008).
29. Rosario AS, Kurth BM, Stolzenberg H, Ellert U, Neuhauser H. Body mass index percentiles for children and adolescents in Germany based on a nationally representative sample (KiGGS 2003-2006). Eur J Clin Nutr. (2010) 64:341–9. doi: 10.1038/ejcn.2010.8
30. Weiss W, Gohlisch C, Harsch-Gladisch C, Tölle M, Zidek W, van der Giet M. Oscillometric estimation of central blood pressure: validation of the Mobil-O-Graph in comparison with the SphygmoCor device. Blood Press Monit. (2012) 17:128–31. doi: 10.1097/MBP.0b013e328353ff63
31. Weber T, Wassertheurer S, Rammer M, Maurer E, Hametner B, Mayer CC, et al. Validation of a brachial cuff-based method for estimating central systolic blood pressure. Hypertension. (2011) 58:825–32. doi: 10.1161/HYPERTENSIONAHA.111.176313
32. Weiss W, Tölle M, Zidek W, van der Giet M. Validation of the mobil-O-Graph: 24 h-blood pressure measurement device. Blood Press Monit. (2010) 15:225–8. doi: 10.1097/MBP.0b013e328338892f
33. Franssen PM, Imholz BP. Evaluation of the Mobil-O-Graph new generation ABPM device using the ESH criteria. Blood Press Monit. (2010) 15:229–31. doi: 10.1097/MBP.0b013e328339be38
34. Neuhauser HK, Thamm M, Ellert U, Hense HW, Rosario AS. Blood pressure percentiles by age and height from nonoverweight children and adolescents in Germany. Pediatrics. (2011) 127:e978–88. doi: 10.1542/peds.2010-1290
35. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. (1972) 18:499–502. doi: 10.1093/clinchem/18.6.499
36. Reusz GS, Cseprekal O, Temmar M, Kis E, Cherif AB, Thaleb A, et al. Reference values of pulse wave velocity in healthy children and teenagers. Hypertension. (2010) 56:217–24. doi: 10.1161/HYPERTENSIONAHA.110.152686
37. Riggio S, Mandraffino G, Sardo MA, Iudicello R, Camarda N, Imbalzano E, et al. Pulse wave velocity and augmentation index, but not intima-media thickness, are early indicators of vascular damage in hypercholesterolemic children. Eur J Clin Invest. (2010) 40:250–7. doi: 10.1111/j.1365-2362.2010.02260.x
38. Muller J, Christov F, Schreiber C, Hess J, Hager A. Exercise capacity, quality of life, and daily activity in the long-term follow-up of patients with univentricular heart and total cavopulmonary connection. Eur Heart J. (2009) 30:2915–20. doi: 10.1093/eurheartj/ehp305
39. Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sports Sci. (2008) 26:1557–65. doi: 10.1080/02640410802334196
40. Woo KS, Chook P, Yu CW, Sung RY, Qiao M, Leung SS, et al. Overweight in children is associated with arterial endothelial dysfunction and intima-media thickening. Int J Obes Relat Metab Disord. (2004) 28:852–7. doi: 10.1038/sj.ijo.0802539
41. WHO 2020 guidelines on physical activity and sedentary behaviour. Geneva: World Health Organization (2020). Available online at: https://apps.who.int/iris/bitstream/handle/10665/336656/9789240015128-eng.pdf (accessed August 18, 2021).
42. Abbott RA, Harkness MA, Davies PS. Correlation of habitual physical activity levels with flow-mediated dilation of the brachial artery in 5-10 year old children. Atherosclerosis. (2002) 160:233–9. doi: 10.1016/S0021-9150(01)00566-4
43. Green DJ. Exercise training as vascular medicine: direct impacts on the vasculature in humans. Exerc Sport Sci Rev. (2009) 37:196–202. doi: 10.1097/JES.0b013e3181b7b6e3
44. Pearson MJ, Smart NA. Aerobic training intensity for improved endothelial function in heart failure patients: a systematic review and meta-analysis. Cardiol Res Pract. (2017) 2017:2450202. doi: 10.1155/2017/2450202
45. Ramirez-Velez R, Hernandez-Quinones PA, Tordecilla-Sanders A, Alvarez C, Ramirez-Campillo R, Izquierdo M, et al. Effectiveness of HIIT compared to moderate continuous training in improving vascular parameters in inactive adults. Lipids Health Dis. (2019) 18:42. doi: 10.1186/s12944-019-0981-z
46. Ketelhut S, Kircher E, Ketelhut SR, Wehlan E, Ketelhut K. Effectiveness of multi-activity, high-intensity interval training in school-aged children. Int J Sports Med. (2020) 41:227–32. doi: 10.1055/a-1068-9331
47. Poitras VJ, Gray CE, Borghese MM, Carson V, Chaput JP, Janssen I, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. (2016) 41(6 Suppl 3):S197–239. doi: 10.1139/apnm-2015-0663
48. Janssen I, Wong SL, Colley R, Tremblay MS. The fractionalization of physical activity throughout the week is associated with the cardiometabolic health of children and youth. BMC Public Health. (2013) 13:554. doi: 10.1186/1471-2458-13-554
49. Eisenmann JC. Physical activity and cardiovascular disease risk factors in children and adolescents: an overview. Can J Cardiol. (2004) 20:295–301.
50. Eddolls WTB, McNarry MA, Stratton G, Winn CON, Mackintosh KA. High-intensity interval training interventions in children and adolescents: a systematic review. Sports medicine. (2017) 47:2363–74. doi: 10.1007/s40279-017-0753-8
51. Sakuragi S, Abhayaratna K, Gravenmaker KJ, O'Reilly C, Srikusalanukul W, Budge MM, et al. Influence of adiposity and physical activity on arterial stiffness in healthy children: the lifestyle of our kids study. Hypertension. (2009) 53:611–6. doi: 10.1161/HYPERTENSIONAHA.108.123364
52. Hopkins ND, Stratton G, Tinken TM, McWhannell N, Ridgers ND, Graves LE, et al. Relationships between measures of fitness, physical activity, body composition and vascular function in children. Atherosclerosis. (2009) 204:244–9. doi: 10.1016/j.atherosclerosis.2008.09.004
53. Green DJ, Maiorana A, O'Driscoll G, Taylor R. Effect of exercise training on endothelium-derived nitric oxide function in humans. J Physiol. (2004) 561:1–25. doi: 10.1113/jphysiol.2004.068197
54. Tjonna AE, Stolen TO, Bye A, Volden M, Slordahl SA, Odegard R, et al. Aerobic interval training reduces cardiovascular risk factors more than a multitreatment approach in overweight adolescents. Clin Sci. (2009) 116:317–26. doi: 10.1042/CS20080249
55. Bruyndonckx L, Hoymans VY, Lemmens K, Ramet J, Vrints CJ. Childhood obesity-related endothelial dysfunction: an update on pathophysiological mechanisms and diagnostic advancements. Pediatr Res. (2016) 79:831–7. doi: 10.1038/pr.2016.22
56. Hopkins ND, Dengel DR, Stratton G, Kelly AS, Steinberger J, Zavala H, et al. Age and sex relationship with flow-mediated dilation in healthy children and adolescents. J Appl Physiol (1985). 2015;119(8):926-33. doi: 10.1152/japplphysiol.01113.2014
57. Jarvisalo MJ, Ronnemaa T, Volanen I, Kaitosaari T, Kallio K, Hartiala JJ, et al. Brachial artery dilatation responses in healthy children and adolescents. Am J Physiol Heart Circ Physiol. (2002) 282:H87–92. doi: 10.1152/ajpheart.2002.282.1.H87
Keywords: endothelial (dys) function, arterial compliance, physical activity, physical fitness, children, sedentariness
Citation: Böhm B, Kirchhuebel H, Elmenhorst J, Müller J and Oberhoffer-Fritz R (2022) Sedentary Behavior in Childhood, Lower Arterial Compliance and Decreased Endothelial Function-Cross Sectional Data From a German School Cohort. Front. Pediatr. 9:787550. doi: 10.3389/fped.2021.787550
Received: 30 September 2021; Accepted: 20 December 2021;
Published: 17 February 2022.
Edited by:
Ruan Kruger, North-West University, South AfricaReviewed by:
Giulia Lona, University of Basel, SwitzerlandEmanuele Monda, University of Campania Luigi Vanvitelli, Italy
Copyright © 2022 Böhm, Kirchhuebel, Elmenhorst, Müller and Oberhoffer-Fritz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Birgit Böhm, YmlyZ2l0LmJvZWhtQHR1bS5kZQ==