
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Pediatr. , 02 December 2021
Sec. Neonatology
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.785524
 Juin Yee Kong1,2,3,4*†
Juin Yee Kong1,2,3,4*† Srabani Samanta Bharadwaj2,3,4,5†
Srabani Samanta Bharadwaj2,3,4,5† Amutha Chinnadurai4,6
Amutha Chinnadurai4,6 Selina Kah Ying Ho2,3,4,5
Selina Kah Ying Ho2,3,4,5Background: Rapid spread of the COVID-19 pandemic raised an urgent need for preparedness in the healthcare sector, including training of healthcare workers to cope with the burden of infected cases while ensuring proper protection of themselves. Improper infection prevention and control measures were key reasons for infection in healthcare workers during the early phase of the outbreak.
Objectives/Methods: This paper describes the combined approach of 3 restructured hospitals in Singapore in preparing and training neonatal healthcare workers' during the COVID-19 pandemic crisis, as well as lessons learnt during this process.
Results: Information sharing was conducted in the form of e-learning, emphasizing on topics like disease knowledge and infection prevention and control procedures. Skills and competency training were carried out in the form of simulation, with sessions scaled into 4 levels progressing from individual task training to larger group simulations involving multiple disciplines and departments. Challenges encountered included information fatigue by large amount of constantly changing information and multiple amendments to workflows as more information arose. Difficulties conducting training and simulation sessions included restriction of group size to mitigate infection risk amongst participants and the limited supply of personal protective equipment prioritized for direct patient care.
Conclusion: Healthcare institutions should ensure adequate dissemination of conceptual knowledge as well as skills competency training of staff in infection control measures for the protection of healthcare workers and patient safety. Ongoing training for sustainability of knowledge and skills, while adapting to the rapidly evolving situation is important in the preparation for future outbreaks.
The first case of SARS-CoV-2 infection or Coronavirus Disease 2019 (COVID-19) was detected in Singapore on 23 January 2020 (1). By 30 January 2020, the WHO declared the novel coronavirus outbreak a Public Health Emergency of International Concern (PHEIC), and subsequently a global pandemic by 11 March 2020. A WHO guidance document released stressed that “all countries should increase their level of preparedness, alert and response to identify, manage and care for new cases of COVID-19” (2). The rapid spread of SARS-CoV-2 to Singapore and the rest of the world had resulted in a scramble in healthcare workers' (HCWs) training, in order to ensure proper protection while coping with the burden of infected cases (3–6). The urgency to complete this training, coupled with initial uncertainty regarding transmission risks and viral virulence contributed to the challenges in HCWs training. Lack of knowledge in IPC and insufficient time for systematic training and practice were some of the reasons for HCWs becoming infected with COVID-19 in China (4).
In Singapore, the lessons learnt from the 2003 Severe Acute Respiratory Syndrome (SARS) outbreak resulted in the public healthcare system having a higher level of preparedness against infectious disease threats (7). Post-SARS, many of the healthcare institutions strengthened IPC measures and developed systems, processes and infrastructure to manage infectious diseases and outbreaks. A 330-bed purpose-built National Centre for Infectious Diseases (NCID) was established in 2019 to strengthen the country's capabilities in infectious disease management and prevention. However, despite the many preparations and measures taken since 2003, there was still an urgent need for training and re-training due to the uncertainties about COVID-19 and its rapid spread.
Pregnant women and infants are especially vulnerable to COVID-19, due to the higher risk of morbidities and mortality in infected mothers, in addition to the early uncertainties regarding vertical and perinatal transmissions to their newborns (8). Implementing training on management of the mother-newborn dyad affected by COVID-19 was complicated due to the varied recommendations, and the need for inter-disciplinary inter-specialty collaboration (9–14). This article describes the combined approach of 3 restructured hospitals in Singapore: (a) KK Women's and Children's Hospital, (b) National University Hospital, and (c) Singapore General Hospital; in preparing and training neonatal HCWs during the COVID-19 pandemic, as well as lessons learnt during this process. These 3 hospitals provide maternity and neonatal services to an average of 47% of Singapore's annual live birth rate of ~39,000 in the last 3 years (15). As part of the country's response to the pandemic, all suspected/confirmed COVID-19 pregnant women were transferred to one of these 3 hospitals for triage and management.
The emergence of the COVID-19 pandemic placed a huge strain on healthcare resources, and it was imperative to establish a rapid and efficient training programme. Training is more effective when HCWs understand the disease pattern, transmission risk and rationale for the recommendations. Goals should be focussed on patient care and HCW safety, ensuring that HCWs are well-prepared with adequate plans in different delivery scenarios. Training tools applied included e-learning, table-top exercises (talk-throughs), walk-throughs and real-time simulations including rapid cycle deliberate practice in-situ simulations (16). Adopting the quality improvement concept of “Going to the Gemba” approach for the walk-through was useful in observing the challenges faced at the real place [delivery room, operating theater (OT)] and has been used in pandemic preparedness (17).
Due to the need for safe distancing measures, e-learning has become an essential component of information sharing to avoid face-to-face contact. E-learning can be in the form of virtual presentations, interactive video conferencing with scenario-based discussions, or circulation of newsletters and infographics. Important topics to cover include hand hygiene technique, appropriate personal protective equipment (PPE) use (donning and doffing sequence), clinical care, and disinfection procedures. Display of posters and pictorial guides in-situ e.g., PPE guide at the entrance of patient's room can serve as reminders to HCWs. The fluid status and changing understanding of COVID-19 had resulted in frequent amendments to protocols and policies, which needed to be disseminated accurately and quickly via institutional online webpage, email and messaging groups amongst stakeholders.
Simulation has been used and proven to be effective in previous outbreaks such as the SARS, Middle East Respiratory Syndrome-Corona virus (MERS Co-V), Ebola and Influenza (H1N1) (18–20). It plays a particularly important role when developing, teaching and implementing guidelines while identifying latent threats in newly developed processes and workflows (19–21). Its strength in education lies in providing practical application of knowledge and skills, and mirroring of different real-life situations without incurring risk to patients or compromising HCW safety (22). Simulation has been widely used to aid the training of HCWs in a timely manner, during the COVID-19 pandemic (23–34).
While HCWs routinely receive training in proper PPE use, studies have shown that its use is suboptimal, accompanied with high rates of error and contamination (21, 35). The efficacy and accuracy of donning and doffing of PPE, can be further enhanced by using simulation-based training (36, 37). Experience from the SARS and Ebola outbreaks showed a decrease risk of infection when training programs and adequate PPE were available (38–41). Simulated practice also affords psychological benefits to HCWs by improving confidence and relieving emotional stress (29, 39, 41–44). This is particularly relevant as fear, anxiety, and increased stress were reported among HCWs in Singapore during the SARS outbreak (45).
In anticipation of the surge in disease volume, the plan for continuity of business in primary clinical areas and the resource allocation need to be taken into consideration when planning the simulation in each institution. The resources available in each center in terms of manpower, equipment, and patient delivery locations may require individual modification and adaptation. We propose that training is best delivered in progressive levels (Levels 1–4) directed at HCW's specific educational need with provision for adding other objectives as required within the structured framework (Figure 1). Overview of the different levels of training is summarized below:
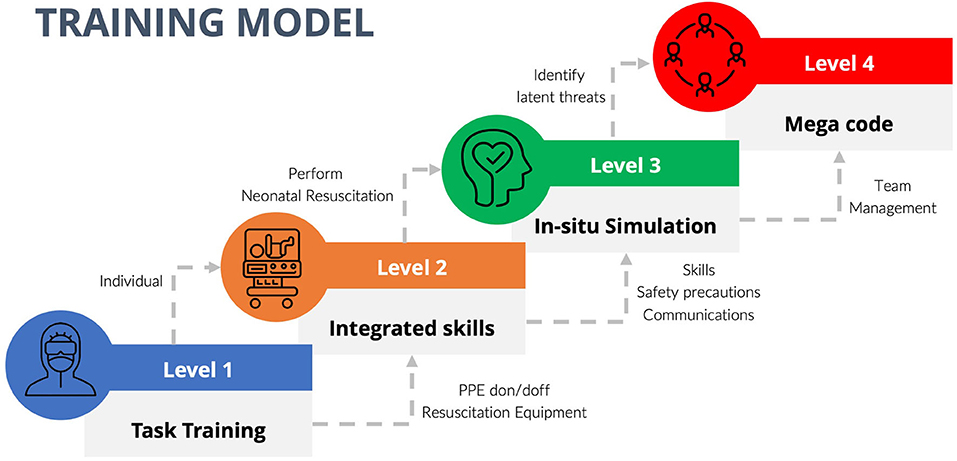
Figure 1. Structured training model with progressive levels.
This is basic level training to ensure confidence and competency in using PPE and setting up of resuscitation equipment. The target participants were HCWs involved in neonatal resuscitation including nursing, midwifery, and medical personnel. IPC principles specific to COVID-19 were explained followed by interactive discussion and actual task training.
a) Proper donning and doffing of PPE: PPE are only protective when used correctly. The task was initially demonstrated by IPC officers, with subsequent practice by participants. Doffing of PPE has been perceived to be more complicated by staff than donning and identified as an area of ongoing confusion with risk of contamination (21). Training was enhanced using deliberate practice, with expert educators present reinforcing the donning and doffing, and placing sequential visual aids at all donning and doffing areas.
b) Resuscitation equipment set-up and disconnection: Participants were made conversant with the changes in workflow and safety principles, especially with regards to positive pressure ventilation (PPV) and aerosol generating procedures (AGPs). The use of High Efficiency Particulate Air (HEPA) filter on the PPV equipment (self-inflating bag and T-piece resuscitator) was demonstrated with participants having the opportunity to practice on task trainer manikins.
Once competent with Level 1 training, participants proceeded to the next level of integrated skills training where they were required to perform the different steps of neonatal resuscitation while wearing full PPE (goggles, face shield, N95 masks or respirator, gown, gloves). Emphasis was placed not only on skills performance but also the safety precautions whilst performing AGPs, and the quality of communication between participants. This level addressed the difficulty of viewing the airway during intubation and challenges of interpersonal communication with the barrier of PPE. Target participants in the team included doctors, nurses and respiratory therapists (RTs). Examples of scenarios were (a) Performing PPV with PPE, (b) Performing intubation with/without surfactant administration with PPE, (c) communication and conveyance of information with PPE. This was conducted through low-fidelity, rapid-sequence simulation drills, using real equipment in the usual working environment (Supplementary Figure 1).
This level was aimed at familiarization of all staff involved in the admission of a newborn delivered to a suspected/confirmed COVID-19 mother and identifying any latent gaps in the existing workflow to ensure a seamless care process. The entire workflow was simulated starting from activation for delivery attendance to admission of the newborn to the Neonatal Unit. Personnel involved included doctors, nurses, RTs and admitting clerks. Some of the scenarios were (a) Term newborn with respiratory distress needing CPAP, (b) Term newborn born via meconium-stained amniotic fluid needing tracheal suctioning, (c) Extremely preterm newborn with respiratory distress syndrome, (d) Transfer of critically ill newborn to neonatal intensive care unit (Supplementary Figure 2), (e) Acute cardiorespiratory deterioration of an existing patient in the isolation unit requiring extensive resuscitation.
The facilitators encouraged participants to voice concerns and talk through problems with a view to identify latent threats and address issues (“Going to the Gemba”), and then devise solutions to overcome them (46). These were conducted at regular intervals as per duty roster and included the full team who will be involved. Many cognitive blind spots were identified at each simulation session and the workflow was amended accordingly.
This largest scale training was conducted as a multidisciplinary mega code which ran from activation and transfer of a suspected/confirmed COVID-19 mother, followed by delivery and resuscitation of the newborn, and finally the disposition of mother-newborn dyad post-delivery. The objective was to identify any gaps in communication and workflow, as well as to address technical and behavioral factors in the multidisciplinary setting. Simulation included pre-briefing, preparation of delivery area, post-delivery disposition of the mother-newborn dyad and disinfection of all involved areas (Supplementary Figure 3). Post-simulation debriefing was conducted to identify gaps in interdisciplinary communication, resource management and IPC measures. Departments involved included Neonatology, Obstetrics & Gynecology (OG), Infectious Disease, Security Services, Women's Anesthesia, Patient Transport Services, and Housekeeping Services. This type of simulation was repeated at less frequent intervals, mainly during change of staffing or if there were major changes in the workflow.
In order to ensure effective and constructive simulation, “spotters” were assigned to identify gaps and provide immediate feedback or take notes for discussion during post-simulation debriefing. Spotters were members outside of the immediate care providing team, e.g., IPC officer or patient safety lead whose focus was on the adherence of IPC measures including physical distancing while providing uncompromised patient care. When possible, they were instituted in actual case scenario as well to help remind staff with PPE donning and doffing which was identified as a challenge area.
An average of 4–6 training sessions per month (weekly level 1–2, monthly level 3–4) involving at least 50 HCWs per hospital have been conducted in the initial period from March to June 2020. Frequency of sessions varied thereafter depending on changeover of staff and patient load. E-learning and talk-throughs were conducted at least once every 3 month or when there were new orientations.
Feedback and debriefing minutes which were collected from participants after the training sessions were summarized in Table 1.
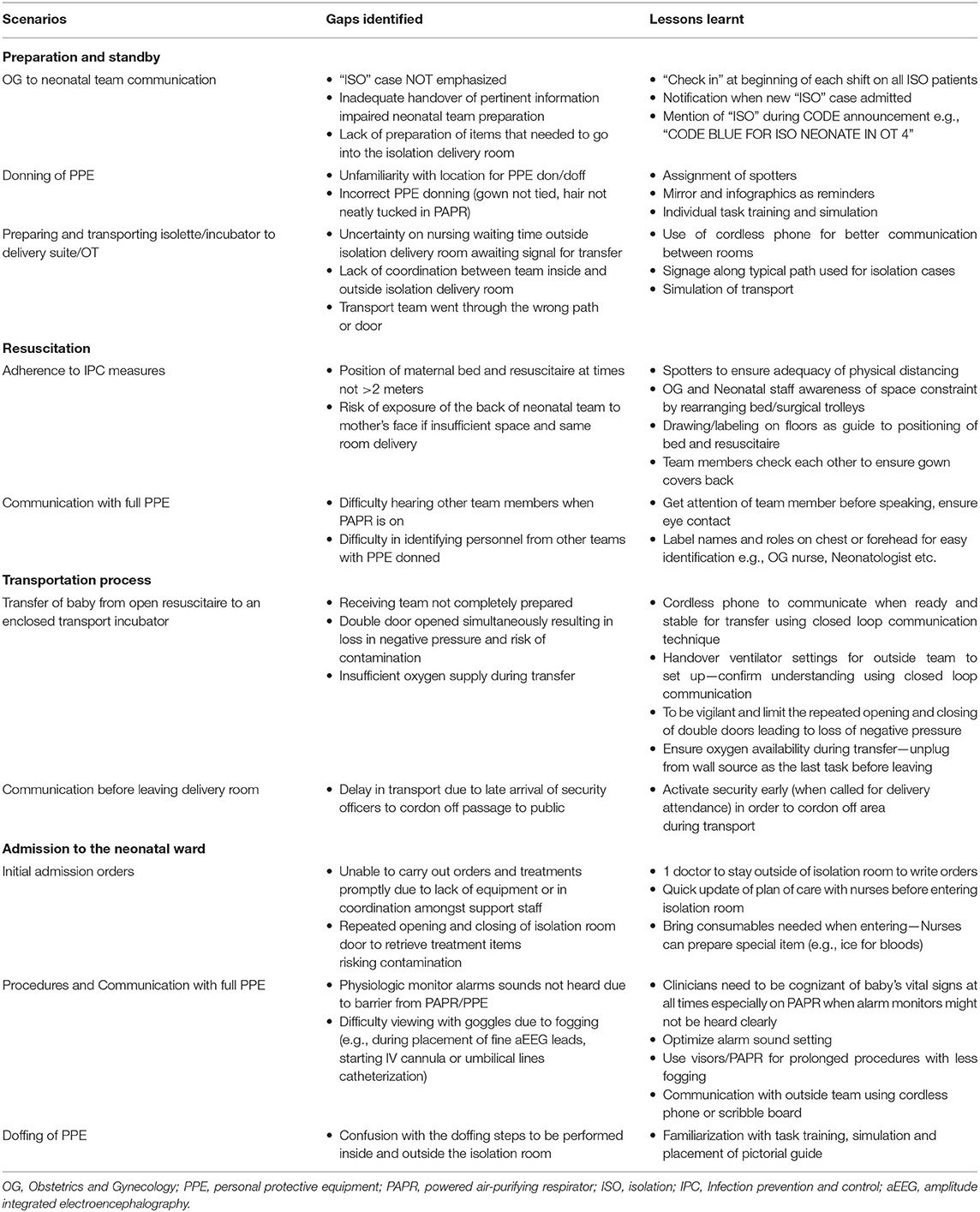
Table 1. Challenges met and lessons learnt during simulation practices.
Messaging fatigue and desensitization to information among HCWs as a result of overwhelming information load at the beginning of the outbreak, with subsequently large amount of emerging literature and updates have been described (47, 48). This could impact the ability of staff to recall the information or messages disseminated to them previously (49). Supervisors can facilitate staff learning by summarizing the large amount of data into key information in the form of infographics and posters, ensuring that training materials are clear and easily understood. Maintaining staff morale whilst instilling a sense of personal responsibility for self-learning are equally important in view of the anticipated protracted duration of the situation and the need for frequent modifications to protocols and policies.
It is important that the training session does not become a source of infection transmission. Infection risk has been reported during COVID-19 pandemic simulation exercise and it is important for educators to ensure no participants have symptoms suggestive of acute respiratory infection (50). It is proposed to conduct training in a step-wise approach, increasing the level of proficiency and involvement to ensure better transition and effective learning in trainees while minimizing need for large group gathering. There should be adequate hand hygiene stations with strict hand hygiene practiced together with enhanced disinfection of training equipment and manikins. Psychological issues like depression, anxiety, somatization symptoms, insomnia are genuine concerns faced by HCWs (51, 52). Hence, during times of increased physical workload and psychological stress, training needs to be performed with sensitivity to the HCWs emotional states.
Simulation of a newborn delivery usually involves a large multidisciplinary team comprising neonatal, obstetric, and even OT and anesthesia departments in the setting of cesarean section. It is extremely challenging to hold a realistic simulation practice session, mirroring an actual event, while adhering to capacity limits (53). Additional considerations while conducting training include registration for contact tracing, ensuring proper masking, limiting participant numbers, use of larger rooms for training and debrief to allow for distancing >2 m apart and live-video streaming to facilitate observation off-site (54). Video recording the sessions showing expert performance facilitates education to a greater audience and can be useful for future review and distribution with key debriefing points if face-to-face training is challenging. This may also aid in alleviating trainer fatigue when few educators need to conduct multiple sessions.
Realistic training and simulation mimicking real scenarios are critical for effective learning; however, this needs to be balanced with limited PPE and equipment supplies. Training amidst a worldwide shortage of PPE and equipment requires compromise and innovation. In order to conserve precious resources for direct patient care, training can include using expired or damaged equipment, utilizing visual representations and re-using or making mock PPE/equipment (29).
Meaningful scenarios have clearly defined and focussed objectives, with emphasis placed on incorporating updated knowledge and recommendations. Hence, the frequent guideline changes necessitated constant amendments to the simulation scenarios. To ensure proficiency and adaptation to new workflows, there is inevitable need for repeated simulation and retraining from time to time. Future scenarios can be based on real clinical encounters for more realistic representation of case scenarios.
Lapse of communication and identification of correct personnel was a real challenge between disciplines after donning PPE. Identifying personnel with labels e.g., “Neonatologist” and “Midwife” may help quick recognition of roles and improve communication. Having clear role allocation and rehearsing of communication techniques including non-verbal communication while maintaining closed loop communication can be useful. Clear instructions provided for access to equipment (bundling of items for ease of procedural preparation) and PPE (marking or labeling of specific areas designated for donning and doffing) can also reduce the need for repeated communication during the exercise.
In the early phases of the COVID-19 pandemic, HCWs were active in seeking training due to the evolving crises and urgency. However, sustaining clinician engagement in training has been a challenge, especially as routines resume, competing for the HCWs' time. To sustain this initial heightened desire for training and intra and interdepartmental collaboration, training champions can be identified and faculty development enhanced. Buy-in by stakeholders (clinicians, simulation, and IPC teams) with support from senior management are also necessary for sustainability.
With the protracted nature of the pandemic, ongoing training with iterative simulations are important. The long term goals should focus on skills retention and competency evaluation, which are vital to ensure quality of later performance. Ongoing training initiatives can include a combination of developing new training materials (e.g., cognitive aids, instructional videos), short follow-up training sessions, table-top exercises and simulations modified based on real case experiences and updated guidelines. Other retraining tools or methods, like mental training, using the mind as a simulator to mentally rehearse the movements of a task or operation, has been used as a supplementary tool in learning surgical skills (55, 56). Online modules should be easily accessible to staff at their convenience, to aid reinforcement of knowledge pertaining to disease updates, changes in policies, and guidelines.
Future training should progress beyond that of knowledge, skills, procedures and processes, and focus on the integration with other behavioral outcomes like teamwork, leadership and communication. Structured worksite practice involving individual task training and integrated skills training, can be peer led and performed by the on-call team members before the start of every shift. In-service simulated scenarios or tabletop exercises can be conducted less frequently (weekly to monthly) within the department to ensure smooth coordination between multidisciplinary personnel during resuscitation and transfer of patient. Grand mega codes involving interdepartmental stakeholders can take place quarterly to ensure optimal teamwork and communication between departments.
One major limitation of this current paper is the lack of prospective data collection with regards to the different domains of the training and formal assessment of clinical outcomes before and after training sessions. As the priority was to safely and effectively train and equip HCWs during the urgent phase of pandemic, proper measurement of clinical outcomes were not performed. To date, there has been no HCW transmission during training or while caring for COVID-19 positive patients.
Institutions should ensure adequate training of staff in IPC measures for specific neonatal situations. The dissemination of conceptual knowledge as well as skills competency training in anticipation and preparation for the management of a newborn with exposure to COVID-19 will ensure optimal patient care and safety for staff. Training can be performed in progressive levels from individual tasks, integrated skills, intra-departmental in-situ simulation to multidisciplinary inter-departmental Mega Code, with debriefing after to identify gaps in processes. Ongoing training for sustainability of knowledge and skills, while adapting to the rapidly evolving situation is important. It is hoped that the training lessons learnt during this pandemic will allow us to be proactive and better prepare for future pandemics and unique infectious disease threats.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
JK: conceptualization, methodology, investigations, data curation, writing-original draft, writing-review and editing, visualization, and project administration. SB: writing—original draft, investigations, data curation, writing-review and editing, and visualization. AC: writing-original draft, investigations, data curation, and writing—review and editing. SH: conceptualization, writing-original draft, writing—review and editing, project administration, and supervision. All authors agree to be accountable for the content of the work and approve of the version to be published.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to acknowledge all the stakeholders from different departments including Obstetrics and Gynaecology, Neonatology, Anaesthesiology, Operating theatres, Infection prevention and control, Housekeeping and Security at KK Women's and Children's Hospital, National University Hospital and Singapore General Hospital, for their collaboration and support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2021.785524/full#supplementary-material
Simulation Scenarios. (1) Routine care in a term well baby, (2) Advanced resuscitation in a term sick baby, (3) Stable preterm baby requiring mask CPAP, (4) Resuscitation and transfer of a sick preterm baby.
Supplementary Figure 1. Providing mask PPV to newborn delivered by emergency cesarean section to a mother with COVID-19 with PAPR on (Level 2 training).
Supplementary Figure 2. Transporting newborn infant delivered to mother with suspected COVID-19 from operating theater to isolation neonatal ICU after emergency Cesarean section (Level 3 training).
Supplementary Figure 3. Admission and stabilization of intubated infant delivered to mother with suspected COVID-19 (Level 4 training).
1. Young BE, Ong SWX, Kalimuddin S, Low JG, Tan SY, Loh J, et al. Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore. JAMA. (2020) 323:1488–94. doi: 10.1001/jama.2020.3204
2. World Health Organization (WHO) Critical Preparedness Readiness and Response Actions for COVID-19: Interim Guidance (2020).
3. The Lancet. COVID-19: protecting health-care workers. Lancet. (2020) 395:922. doi: 10.1016/S0140-6736(20)30644-9
4. Wang J, Zhou M, Liu F. Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect. (2020) 105:100–1. doi: 10.1016/j.jhin.2020.03.002
5. Zhang Z, Liu S, Xiang M, Li S, Zhao D, Huang C, et al. Protecting healthcare personnel from 2019-nCoV infection risks: lessons and suggestions. Front Med. (2020) 14:229–31. doi: 10.1007/s11684-020-0765-x
6. Tan LF. Preventing the transmission of COVID-19 amongst healthcare workers. J Hosp Infect. (2020) 105:364–5. doi: 10.1016/j.jhin.2020.04.008
8. Zamaniyan M, Ebadi A, Aghajanpoor S, Rahmani Z, Haghshenas M, Azizi S. Preterm delivery in pregnant woman with critical COVID-19 pneumonia and vertical transmission. Prenat Diagn. (2020) 40:1759–61. doi: 10.1002/pd.5713
9. Yeo KT, Biswas A, Ho SKY, Kong JY, Bharadwaj S, Chinnadurai A, et al. Guidance for the clinical management of infants born to mothers with suspected/confirmed COVID-19 in Singapore. Singapore Med J. (2021). doi: 10.11622/smedj.2021045. [Epub ahead of print].
10. Lavizzari A, Klingenberg C, Profit J, Zupancic JAF, Davis AS, Mosca F, et al. International comparison of guidelines for managing neonates at the early phase of the SARS-CoV-2 pandemic. Pediatr Res. (2020) 89:940–51. doi: 10.1038/s41390-020-0976-5
11. Chandrasekharan P, Vento M, Trevisanuto D, Partridge E, Underwood MA, Wiedeman J, et al. Neonatal resuscitation and postresuscitation care of infants born to mothers with suspected or confirmed SARS-CoV-2 infection. Am J Perinatol. (2020) 37:813–24. doi: 10.1055/s-0040-1709688
12. Devane D, Kellie F, Finucane E, Beecher C, Hanrahan V, Papageorghiou AT, et al. Review of Clinical Practice Guidelines for the Care of Pregnant Women (and Their Babies) During COVID-19 (Protocol) Cochrane Pregnancy and Childbirth COVID Group. Cochrane Pregnancy and Childbirth (2020).
13. Yeo KT, Oei JL, De Luca D, Schmölzer GM, Guaran R, Palasanthiran P, et al. Review of guidelines and recommendations from 17 countries highlights the challenges that clinicians face caring for neonates born to mothers with COVID-19. Acta Paediatr. (2020) 109:2192–207. doi: 10.1111/apa.15495
14. Mimouni F, Lakshminrusimha S, Pearlman SA, Raju T, Gallagher PG, Mendlovic J. Perinatal aspects on the covid-19 pandemic: a practical resource for perinatal-neonatal specialists. J Perinatol. (2020) 40:820–6. doi: 10.1038/s41372-020-0665-6
15. Department of Statistics Singapore Singapore (2020). Available online at: https://www.singstat.gov.sg (accessed: July 25, 2020).
16. Taras J, Everett T. Rapid cycle deliberate practice in medical education - a systematic review. Cureus. (2017) 9:e1180. doi: 10.7759/cureus.1180
17. Thull-Freedman J, Mondoux S, Stang A, Chartier LB. Going to the COVID-19 Gemba: using observation and high reliability strategies to achieve safety in a time of crisis. CJEM. (2020) 22:738–41. doi: 10.1017/cem.2020.380
18. Palamidessi Domínguez J, de la Fuente MV, Rubio Muñoz JJ, Carmona SA, Castañeda DP, Sanz NM, et al. Training on the care of patients with respiratory syndrome of middle east-coronavirus and ebola virus based on clinical simulation. Intensive Care Med Exp. (2015) 3:A732. doi: 10.1186/2197-425X-3-S1-A732
19. Abrahamson SD, Canzian S, Brunet F. Using simulation for training and to change protocol during the outbreak of severe acute respiratory syndrome. Crit Care. (2006) 10:R3. doi: 10.1186/cc3916
20. Watson CM, Duval-Arnould JM, McCrory MC, Froz S, Connors C, Perl TM, et al. Simulated pediatric resuscitation use for personal protective equipment adherence measurement and training during the 2009 influenza (H1N1) pandemic. Jt Comm J Qual Patient Saf. (2011) 37:515–23. doi: 10.1016/S1553-7250(11)37066-3
21. Phan LT, Maita D, Mortiz DC, Weber R, Fritzen-Pedicini C, Bleasdale SC, et al. Personal protective equipment doffing practices of healthcare workers. J Occup Environ Hyg. (2019) 16:575–81. doi: 10.1080/15459624.2019.1628350
22. Cheng A, Auerbach M, Hunt EA, Chang TP, Pusic M, Nadkarni V, et al. Designing and conducting simulation-based research. Pediatrics. (2014) 133:1091–101. doi: 10.1542/peds.2013-3267
23. Brydges R, Campbell DM, Beavers L, Khodadoust N, Iantomasi P, Sampson K, et al. Lessons learned in preparing for and responding to the early stages of the COVID-19 pandemic: one simulation's program experience adapting to the new normal. Adv Simul. (2020) 5:8. doi: 10.1186/s41077-020-00128-y
24. Li L, Lin M, Wang X, Bao P, Li Y. Preparing and responding to 2019 novel coronavirus with simulation and technology-enhanced learning for healthcare professionals: challenges and opportunities in China. BMJ Simul Technol Enhanc Learn. (2020) 6:196–8. doi: 10.1136/bmjstel-2020-000609
25. Choi GYS, Wan WTP, Chan AKM, Tong SK, Poon ST, Joynt GM. Preparedness for COVID-19: in situ simulation to enhance infection control systems in the intensive care unit. Br J Anaesth. (2020) 125:e236–9. doi: 10.1016/j.bja.2020.04.001
26. Shi D, Lu H, Wang H, Bao S, Qian L, Dong X, et al. A simulation training course for family medicine residents in China managing COVID-19. Aust J Gen Pract. (2020) 49:364–8. doi: 10.31128/AJGP-04-20-5337
27. Foong TW, Hui Ng ES, Wee Khoo CY, Ashokka B, Khoo D, Agrawal R. Rapid training of healthcare staff for protected cardiopulmonary resuscitation in the COVID-19 pandemic. Br J Anaesth. (2020) 125:e257–9. doi: 10.1016/j.bja.2020.04.081
28. Lim WY, Wong P, Teo LM, Ho VK. Resuscitation during the COVID-19 pandemic: lessons learnt from high-fidelity simulation. Resuscitation. (2020) 152:89–90. doi: 10.1016/j.resuscitation.2020.05.024
29. Brazil V, Lowe B, Ryan L, Bourke R, Scott C, Myers S, et al. Translational simulation for rapid transformation of health services, using the example of the COVID-19 pandemic preparation. Adv Simul. (2020) 5:9. doi: 10.1186/s41077-020-00127-z
30. Tan W, Ye Y, Yang Y, Chen Z, Yang X, Zhu C, et al. Whole-Process emergency training of personal protective equipment helps healthcare workers against COVID-19: design and effect. J Occup Environ Med. (2020) 62:420–3. doi: 10.1097/JOM.0000000000001877
31. Dieckmann P, Torgeirsen K, Qvindesland SA, Thomas L, Bushell V, Langli Ersdal H. The use of simulation to prepare and improve responses to infectious disease outbreaks like COVID-19: practical tips and resources from Norway, Denmark, and the UK. Adv Simul. (2020) 5:3. doi: 10.1186/s41077-020-00121-5
32. Muhsen WS, Marshall-Roberts R. Simulation-guided preparations for the management of suspected or confirmed COVID-19 cases in the obstetric emergency theater. J Matern Fetal Neonatal Med. (2020) 1–4. doi: 10.1080/14767058.2020.1765333
33. Kang Y, Deng L, Zhang D, Wang Y, Wang G, Mei L, et al. A practice of anesthesia scenario design for emergency cesarean section in patients with COVID-19 infection based on the role of standard patient. Biosci Trends. (2020) 14:222–6. doi: 10.5582/bst.2020.03066
34. Wong J, Goh QY, Tan Z, Lie SA, Tay YC, Ng SY, et al. Preparing for a COVID-19 pandemic: a review of operating room outbreak response measures in a large tertiary hospital in Singapore. Can J Anaesth. (2020) 67:732–45. doi: 10.1007/s12630-020-01620-9
35. Kang J, O'Donnell JM, Colaianne B, Bircher N, Ren D, Smith KJ. Use of personal protective equipment among health care personnel: results of clinical observations and simulations. Am J Infect Control. (2017) 45:17–23. doi: 10.1016/j.ajic.2016.08.011
36. Díaz-Guio DA, Ricardo-Zapata A, Ospina-Velez J, Gómez-Candamil G, Mora-Martinez S, Rodriguez-Morales AJ. Cognitive load and performance of health care professionals in donning and doffing PPE before and after a simulation-based educational intervention and its implications during the COVID-19 pandemic for biosafety. Infez Med. (2020) 28:111–7.
37. Oliveira HC, Souza LC, Leite TC, Campos JF. Personal protective equipment in the coronavirus pandemic: training with rapid cycle deliberate practice. Rev Bras Enferm. (2020) 73:e20200303. doi: 10.1590/0034-7167-2020-0303
38. Moore D, Gamage B, Bryce E, Copes R, Yassi A, Group BIRPS. Protecting health care workers from SARS and other respiratory pathogens: organizational and individual factors that affect adherence to infection control guidelines. Am J Infect Control. (2005) 33:88–96. doi: 10.1016/j.ajic.2004.11.003
39. O'Keeffe DA, Bradley D, Evans L, Bustamante N, Timmel M, Akkineni R, et al. Ebola emergency preparedness: simulation training for frontline health care professionals. MedEdPORTAL. (2016) 12:10433. doi: 10.15766/mep_2374-8265.10433
40. Abualenain JT, Al-Alawi MM. Simulation-based training in Ebola Personal Protective Equipment for healthcare workers: experience from King Abdulaziz University Hospital in Saudi Arabia. J Infect Public Health. (2018) 11:796–800. doi: 10.1016/j.jiph.2018.05.002
41. Carvalho E, Castro P, León E, Del Río A, Crespo F, Trigo L, et al. Multi-professional simulation and risk perception of health care workers caring for Ebola-infected patients. Nurs Crit Care. (2019) 24:256–62. doi: 10.1111/nicc.12396
42. LoSavio PS, Eggerstedt M, Tajudeen BA, Papagiannopoulos P, Revenaugh PC, Batra PS, et al. Rapid implementation of COVID-19 tracheostomy simulation training to increase surgeon safety and confidence. Am J Otolaryngol. (2020) 41:102574. doi: 10.1016/j.amjoto.2020.102574
43. Mark ME, LoSavio P, Husain I, Papagiannopoulos P, Batra PS, Tajudeen BA. Effect of implementing simulation education on health care worker comfort with nasopharyngeal swabbing for COVID-19. Otolaryngol Head Neck Surg. (2020) 163:271–4. doi: 10.1177/0194599820933168
44. Khan JA, Kiani MRB. Impact of multi-professional simulation-based training on perceptions of safety and preparedness among health workers caring for coronavirus disease 2019 patients in Pakistan. J Educ Eval Health Prof. (2020) 17:19. doi: 10.3352/jeehp.2020.17.19
45. Koh D, Lim MK, Chia SE, Ko SM, Qian F, Ng V, et al. Risk perception and impact of Severe Acute Respiratory Syndrome (SARS) on work and personal lives of healthcare workers in Singapore: what can we learn? Med Care. (2005) 43:676–82. doi: 10.1097/01.mlr.0000167181.36730.cc
46. Law BH, Cheung PY, Skelding S, Schmölzer GM. Table-top exercises to prepare for neonatal resuscitation in the Era of COVID-19. Resuscitation. (2020) 151:85–6. doi: 10.1016/j.resuscitation.2020.04.027
47. Kim S, So J. How message fatigue toward health messages leads to ineffective persuasive outcomes: examining the mediating roles of reactance and inattention. J Health Commun. (2018) 23:109–16. doi: 10.1080/10810730.2017.1414900
48. Koh PK, Chan LL, Tan EK. Messaging fatigue and desensitisation to information during pandemic. Arch Med Res. (2020) 51:716–7. doi: 10.1016/j.arcmed.2020.06.014
49. Baseman JG, Revere D, Painter I, Toyoji M, Thiede H, Duchin J. Public health communications and alert fatigue. BMC Health Serv Res. (2013) 13:295. doi: 10.1186/1472-6963-13-295
50. Chiu M, Crooks S, Fraser AB, Rao P, Boet S. Physical health risks during simulation-based COVID-19 pandemic readiness training. Can J Anaesth. (2020) 67:1667–9. doi: 10.1007/s12630-020-01744-y
51. Zhou Y, Wang W, Sun Y, Qian W, Liu Z, Wang R, et al. The prevalence and risk factors of psychological disturbances of frontline medical staff in china under the COVID-19 epidemic: workload should be concerned. J Affect Disord. (2020) 277:510–4. doi: 10.1016/j.jad.2020.08.059
52. Huang J, Liu F, Teng Z, Chen J, Zhao J, Wang X, et al. Care for the psychological status of frontline medical staff fighting against coronavirus disease 2019 (COVID-19). Clin Infect Dis. (2020) 71:3268–9. doi: 10.1093/cid/ciaa385
53. Pan D, Rajwani K. Implementation of simulation training during the COVID-19 pandemic: a New York Hospital Experience. Simul Healthc. (2021) 16:46–51. doi: 10.1097/SIH.0000000000000535
54. Ingrassia PL, Capogna G, Diaz-Navarro C, Szyld D, Tomola S, Leon-Castelao E. COVID-19 crisis, safe reopening of simulation centres and the new normal: food for thought. Adv Simul. (2020) 5:13. doi: 10.1186/s41077-020-00131-3
55. Rao A, Tait I, Alijani A. Systematic review and meta-analysis of the role of mental training in the acquisition of technical skills in surgery. Am J Surg. (2015) 210:545–53. doi: 10.1016/j.amjsurg.2015.01.028
Keywords: COVID-19, neonate, perinatal care, simulation, training
Citation: Kong JY, Bharadwaj SS, Chinnadurai A and Ho SKY (2021) Being Prepared During the Evolving COVID-19 Pandemic: A Neonatal Experience in Training and Simulation. Front. Pediatr. 9:785524. doi: 10.3389/fped.2021.785524
Received: 29 September 2021; Accepted: 09 November 2021;
Published: 02 December 2021.
Edited by:
Yogen Singh, Cambridge University Hospitals NHS Foundation Trust, United KingdomReviewed by:
Takanari Ikeyama, Aichi Child Health and Medical General Center, JapanCopyright © 2021 Kong, Bharadwaj, Chinnadurai and Ho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juin Yee Kong, a29uZy5qdWluLnllZUBzaW5naGVhbHRoLmNvbS5zZw==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.