 Lorenz Sommer
Lorenz Sommer Katrin Klebermaß-Schrehof
Katrin Klebermaß-Schrehof Angelika Berger
Angelika Berger Eva Schwindt
Eva Schwindt
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 23 December 2021
Sec. Neonatology
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.771396
Objectives: To evaluate a new task-based package-organized (TPO) neonatal emergency backpack and to compare it to the classical (ABC- and material-based) backpack.
Methods: Simulation-based assessment of time to retrieve equipment for three different tasks [intraosseous access (IO), intubation and adrenaline administration] using the TPO and the classical emergency backpack was compared.
Results: Equipment retrieval times for the three tasks were assessed for 24 nurses (12 intermediate care, 12 intensive care) and were significantly faster in the TPO than in the classical backpack (IO 33 vs. 75 s, p < 0.001; intubation 53 vs. 70 s, p = 0,001; adrenaline 22 vs. 45 s, p < 0.001). The number of missing items was significantly lower using the TPO backpack for IO and adrenaline retrieval (IO 0,9 vs. 2,3 items, p < 00001, adrenaline 0.04 vs. 1, p < 0.001) but not for intubation equipment (0.9 vs. 1, not significant). The subjective rating of overall clearness was significantly higher for the TPO compared with the classical backpack (5,9 vs. 3,5, p < 0.001).
Conclusion: Task-based package organization of neonatal emergency backpacks is feasible and might be superior to ABC-/material-oriented storage.
Given that “proper preparation prevents poor performance,” a well-planned emergency kit with all potentially required material is of paramount importance in critical medical events. This is even more true for emergencies outside the “home ward” or even preclinically. Emergency kits, such as trolleys or backpacks, are used for in-hospital neonatal emergencies. However, thus far, published literature on recommendations for the content of neonatal emergency kits is scarce, and authors rarely focus on how to arrange emergency equipment (1). López-Herce Cid et al. (2) provide a list of recommended equipment in a neonatal emergency kit. Regarding “how” to store these items, they recommend “it should be organized so that equipment and medication can be found easily and intuitively.” Unfortunately, these authors do not provide any suggestions on how to do so, and to our knowledge, there is no other study concerning this topic.
Whether found on an emergency cart or trolley or in a backpack, emergency equipment is often stored according to categories of material, such as “syringes” or “tubes.” Other approaches include ABC (airway—breathing—circulation)-oriented storage, or material is stored in an escalating manner in accordance with the recent Neonatal Resuscitation Program (NRP) guidelines from the American Academy of Pediatrics (3). A common problem with all these approaches is the requirement to retrieve the complete equipment for one task from several drawers or bags because consumables, such as syringes or luer-lock caps, are often stored in other locations. This retrieval process not only wastes valuable time during an emergency event but also supposedly leads to higher stress levels in medical teams in an already very stressful situation and hence might impede resuscitation performance.
Standardized procedures and required equipment however could already be considered when designing space for equipment storage. Therefore, we developed a task-based package-oriented (TPO) emergency backpack with the goal of storing and packing together equipment for each specific task without the need to retrieve any additional material from other bags. In neonatal units, this approach is often implemented in prepacked sets for umbilical venous catheters (4).
In this study, we aimed to evaluate the hypothesis that equipment retrieval is faster and easier for medical teams with TPO emergency backpacks than for those with conventional material-oriented backpacks.
For this cross-over study bedside nursing staff from two IMCs and two ICU wards (both Children's University Hospital, Medical University Vienna) were randomly recruited. Power calculation (G*Power 3.1 for Mac, Apple Inc., USA) was based on an estimated difference of 15 s for retrieval times and revealed 24 participants. Therefore, six nurses were recruited from each ward. The nurses were asked to retrieve equipment for (1) intraosseous access (IO), (2) intubation and (3) epinephrine administration once using the classical emergency kit and once using the TPO emergency kit. The assessment began at 50% with the classical kit and at 50% with the TPO kit. The first three nurses were asked to begin with the classical kit and the last three nurses with the TPO kit—vice versa with the other IMC/ICU ward. An initial explanation was not provided for either emergency kit (classical or the new TPO kit). All assessments were performed on the ward. Primary outcome was the time required for equipment retrieval, which was measured using a standard stopwatch. Secondary outcome was the potential impact of influencing factors, which were assessed via questionnaire. This questionnaire was completed by all participants to obtain the following information:
- Previous experience in neonatal care (years)
- Working experience at the Children's University Hospital of the Medical University Vienna
- Previous experience with the classical emergency kit in real-life emergency events
- Self-evaluation of estimation of confidence in handling using the classical emergency kit (scale 1 to 6, with 1 = not very confident and 6 = very confident)
- Individual rating of overall arrangement of both emergency kits (scale 1 to 6, with 1 = very unclear and 6 = very clear arrangement)
- Assessment of frequency on how often individuals familiarize themselves with the emergency kit (weekly, monthly, 1–2 times every 6 months, 1–2 times every 12 months or never).
The classical emergency kit is an emergency backpack from X-CEN-TEK GmbH & Co KG (Wardenburg, Germany); see Figure 1; Table 1. Equipment is stored partly based on an ABC-oriented approach (i.e., “airway”), partly according to type of material (i.e., “plasts”) and partly using a task-based approach (i.e., “venous access”). Due to this mixture of packaging types, even in task-based oriented bags, the necessity to retrieve for multiple bags arises to compile all required equipment for one task. For example, the storage unit labeled “medications” contains all necessary medications, but syringes must be retrieved from a storage unit labeled “venous access.”
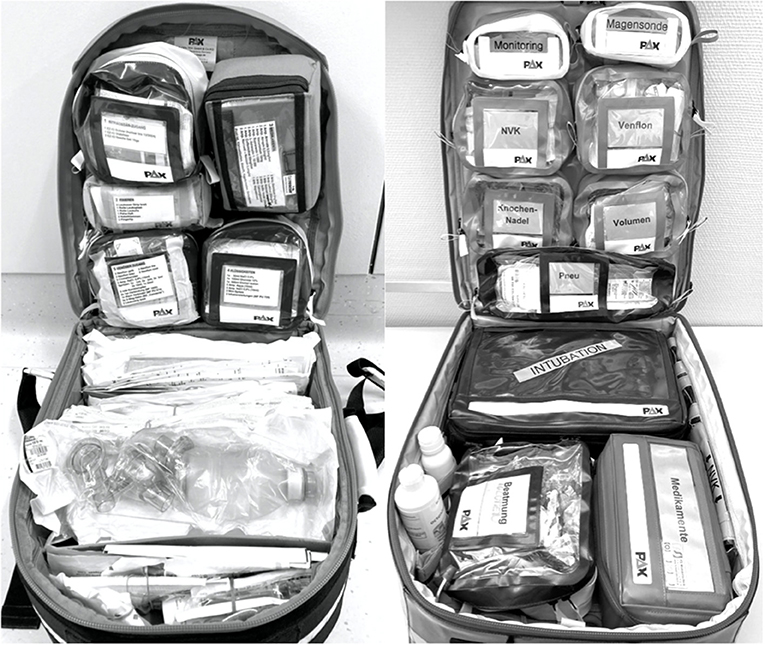
Figure 1. Classical emergency backpack (left) and task-based package-organized backpack (right): Magesonde = gastric tube, NVK = UVC (umbilical venous access), Venflon = peripheral venous access, Knochennadel = intraosseous access, Volumen = fluids, Pneu = pneumothorax, Beatmung = ventilation, Medikamente = medication.
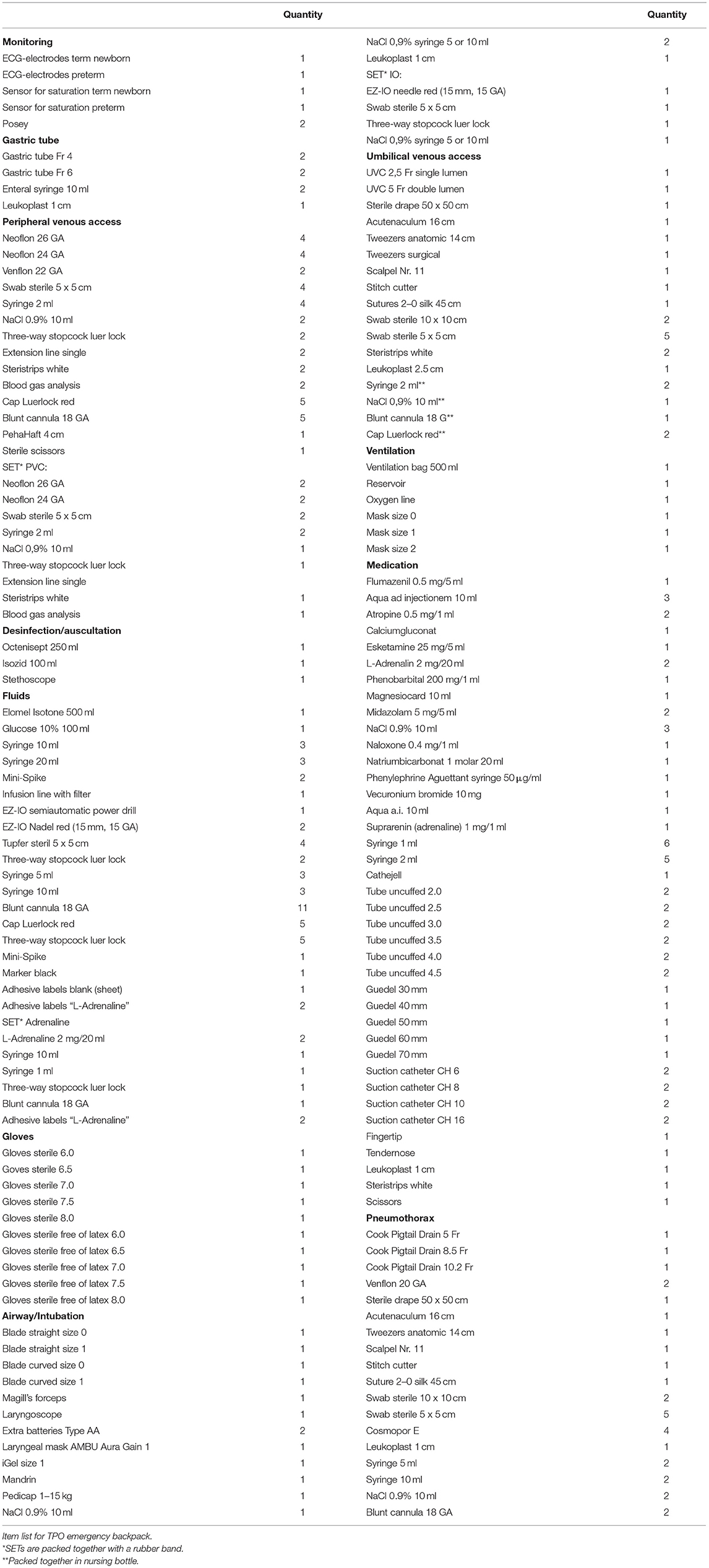
Table 1. Item list of the task-based package-organized emergency backpack.
In contrast to the classical emergency kit, the TPO backpack is thoroughly ordered according to certain tasks [monitoring, gastric tube, peripheral venous access, IO access, umbilical venous catheter, ventilation, airway/intubation, medication (including epinephrine set), pneumothorax; see Figure 1; Table 2]. There are bags for each task, each containing the complete equipment required for one certain task—and nothing else. Furthermore, some task-based oriented bag subsets are used. For example, the bag labeled “peripheral venous access” contains all requirements for venous access, including extra material and different needle sizes, and, in addition, equipment required for ONE attempt of peripheral venous access is packed together (using a rubber band) within this bag. Also, material is not stored in loose pockets to avoid a disordered arrangement.
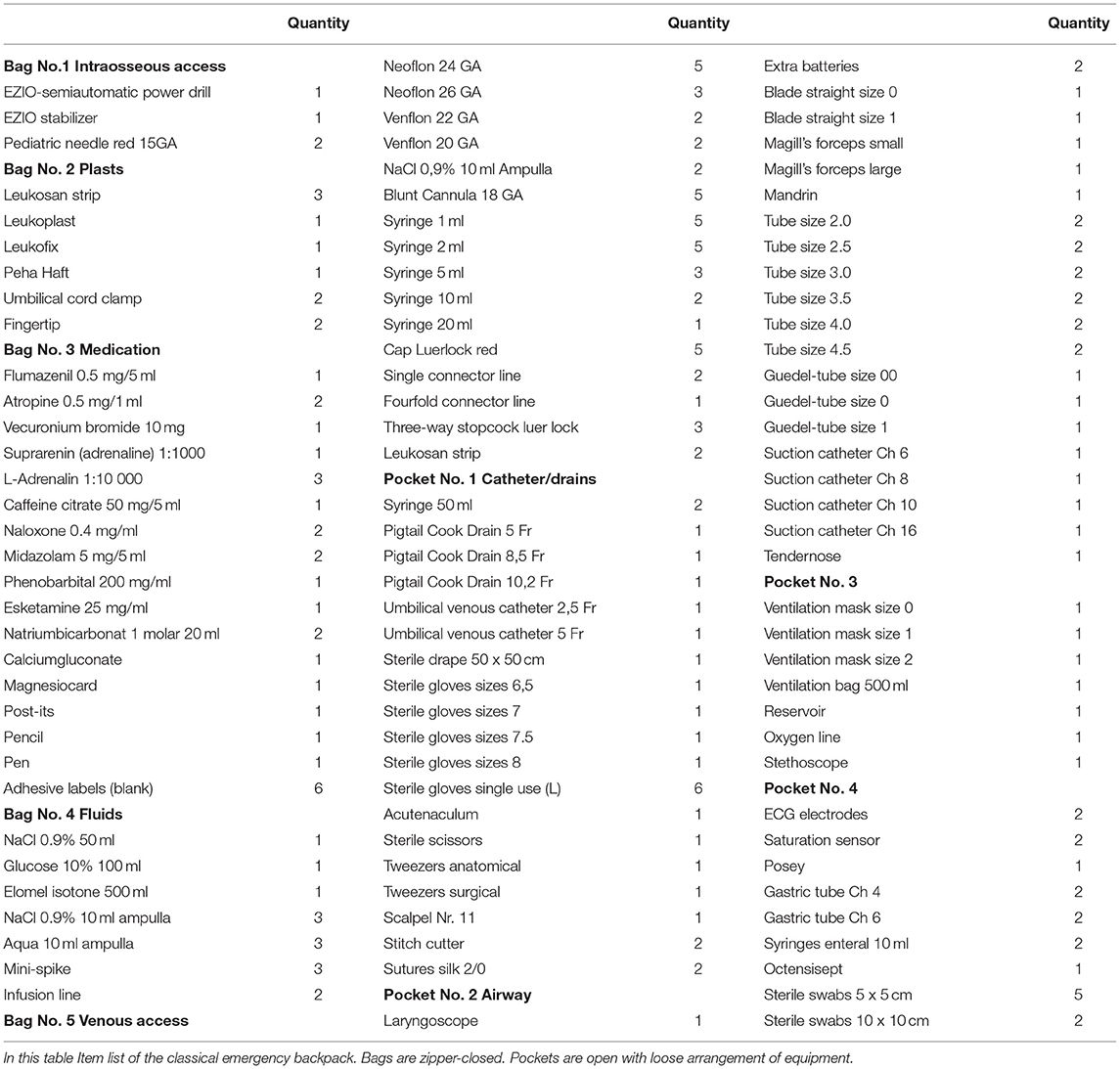
Table 2. Item list of the classical emergency backpack.
Descriptive statistics were performed using SPSS Statistics Version 23.0 (IBM). For comparison of items, such as duration or clearness of arrangement, a dependent sample t-test was used. Statistical analysis of retrieval times was performed by Kruskal-Wallis rank-sum test to correct for non-normal distribution. Correlation calculations were performed using the Pearson correlation. Level of significance was defined at p = 0.05.
This study was conducted under the approval of the ethics committee and the data protection committee of the Medical University Vienna.
Twenty-four nurses were recruited to participate in the study: 12 from intermediate care (IMC) and 12 from the intensive care unit (ICU). The ICU nurses had a mean of 13.5 (0.5-32) years of experience in neonatal medicine, and the IMC nurses had 9.5 years of experience (0.5–28; p = 0.375). The average number of years worked in our hospital was 13.5 years (range 0.5–32) for the ICU staff and 6.6 years (range 0.5–20; p = 0.08) for the IMC staff. In total, 96% of the participants were female (23/24). Seventy-five percent of both ICU (9/12) and IMC (9/12) nurses declared to have previously worked with the emergency kit in real-life emergency events.
Regarding the frequency of how often nurses familiarized themselves with the emergency kit, two nurses (8.3%) declared “never,” 13 (54.2%) “1–2 times per year,” eight (33.3%) “once a month” and zero reported “once a week.” The self-evaluation of confidence in overall handling with the classical emergency kit was 3.2 (scale from 1 to 6; 1 = not very confident and 6 = very confident). The following confidence scores for equipment retrieval were obtained: 5,3 for peripheral venous access, 3,0 for IO, 4,4 for intubation and 4,7 for epinephrine. Comparing nurses from the IMC and ICU, ICU nurses felt significantly more confident in preparing equipment for intubation (p < 0.001) and epinephrine (0.01), but this was not true for peripheral venous access, intraosseous access or overall handling with the kit.
Compared to the classical emergency kit, times required to retrieve equipment for IO access, intubation and epinephrine were significantly shorter with the TPO kit: IO 75 vs. 33 s (p < 0.001), intubation 70 vs. 53 s (p = 0.001) and epinephrine 45 vs. 22 s (p < 0.001). Details are reported in Table 3; Figure 2.
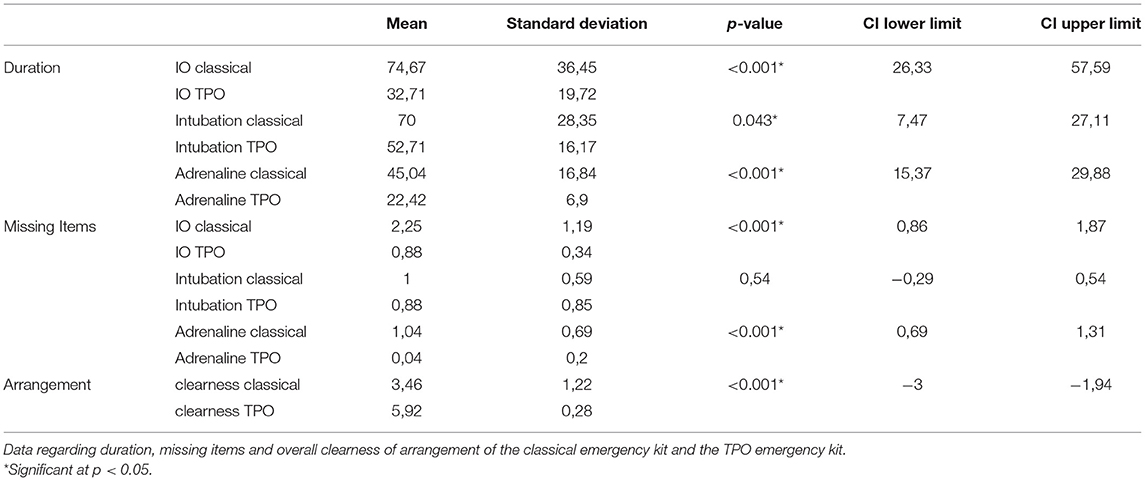
Table 3. Statistical comparison of the classical with the task-based package-organized emergency backpack.
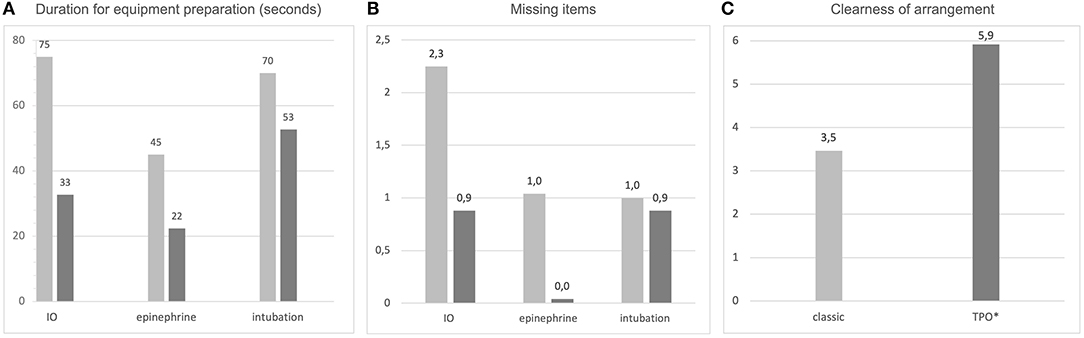
Figure 2. Comparison of the classical emergency kit with the task-based package-organized emergency kit according to (A) the time required to prepare equipment for IO access, epinephrine and intubation (numbers are given in seconds); (B) missing items in equipment preparation and (C) overall clearness of arrangement (scale from 1 to 6, with 1 = very unclear and 6 = very clear arrangement).
The number of missing items was higher using the classical kit compared to the TPO kit (Figure 2): IO 2.3 vs. 0.9 missing items (p < 0.001) and epinephrine 1 vs. 0.04 (p < 0.001). However, the difference between the number of missing items for intubation was not significant when comparing the two kits (1 vs. 0.9—not significant).
Arrangement of the emergency equipment was rated as 3,5 for the classical kit and 5,9 for the TPO kit on a scale from 1 to 6 with 1 = poorly arranged and 6 = very clearly arranged (Figure 2). This result was statistically significant (p < 0.001).
There was no correlation between the frequency of familiarization with the classical emergency kit and the duration of equipment retrieval. This was true for the use of the classical as well as for the TPO kit and for all three types of assessments (IO access, intubation and epinephrine).
Regarding the classical kit, the more years of experience in neonatal care the employees had, the faster they were in retrieval of equipment for epinephrine (p = 0.04). However, no such correlation was noted with the TPO emergency kit.
Using the TPO kit, the retrieval of intubation equipment was significantly faster in employees with more experience in neonatal care (p = 0.001). This was not true for the classical emergency kit. Details are provided in Table 4.
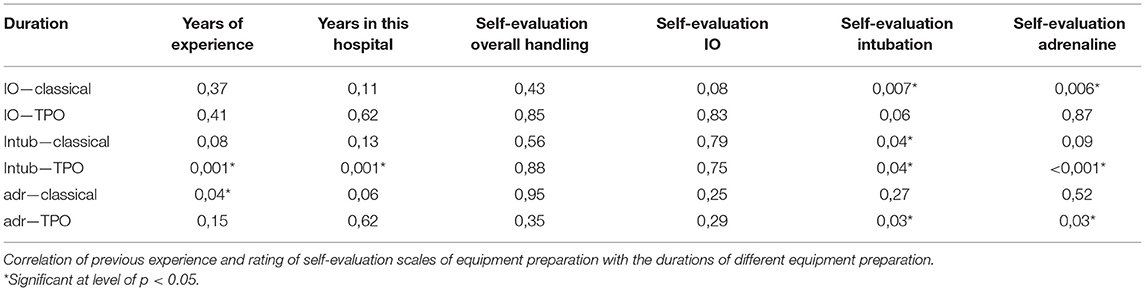
Table 4. Correlation of previous experience and self-rating with equipment retrieval times.
Personnel who rated their abilities in the overall handling of the emergency kit higher were not significantly faster in equipment retrieval (IO, intubation and epinephrine). Details on IO, intubation and epinephrine retrieval are presented in Table 4.
The time required for IO retrieval was significantly shorter among ICU personnel compared with IMC personnel (classical kit: 55 vs. 94 s, p = 0.006; TPO: 24 vs. 41 s, p = 0.04). All other parameters (time required for intubation/epinephrine retrieval or missing items) did not differ in ICU compared to IMC staff.
In stressful situations, even the simplest tasks might become extremely challenging. Therefore, in emergency events it should be made easy for medical teams to find and retrieve the required emergency equipment as fast as possible (5, 6). However, this is not only relevant for mobile emergency kits (though events outside the “home ward” are supposed to be the most stressful and challenging). This is true for all emergency carts, resuscitation rooms and, in general, all sites where critical events might occur. Furthermore, an excellent way to train and evaluate the arrangement of equipment is to simulate critical events in real-life settings (in-situ simulation training), which should be done in regular intervals to be able to dynamically adapt to changing conditions or treatment strategies.
The consideration of human factors in emergency backpacks that might impede the retrieval of material is of paramount importance (7, 8). These factors include, among others, the appropriate choice of backpack/trolley type and storage bags (size, color, type of closure systems), clear labeling of the bags and arrangement of the bags within the backpack. A successful example on how to include human factors in equipment arrangement and to evaluate the approach using in-situ simulation is provided by Lefebvre et al., describing the process of re-designing their neonatal surgical crash cart (9). To our knowledge, no study has focused on how to arrange equipment in a neonatal emergency backpack and how to consider human factors to optimize equipment preparation.
In this study we used simulation to compare the classical neonatal emergency backpack with the TPO kit and showed that equipment retrieval times for three different tasks (IO, intubation and epinephrine administration) were significantly shorter, there were fewer missing items and subjective ratings of “overall clearness” were significantly higher in the TPO kit. As a single exception, the number of missing items for intubation did not differ significantly between classical and TPO kit. This, however, was to be expected given that the “airway”-packages are very similar and, in both approaches, there is no requirement for additional equipment.
It seems obvious that the requirement of several storage bags in the classical kit that have to be identified, opened and searched for certain equipment is challenging and time-consuming. The advantage of the TPO approach clearly lies within the underlying idea that everything needed for one specific task is packed together as a set, and no additional storage bags are needed. This notion is supported even more by the use of the small subsets within the task-based bags, i.e., the equipment for one attempt of peripheral venous access is packed together separately and ready to hand.
Based on the results of this study, we conclude that neonatal emergency backpacks might preferably be arranged in a TPO-based manner rather than an ABC- or material-oriented way. As an example, we present the content and packages of our neonatal TPO emergency backpack. However, medical teams in other hospitals are asked to arrange their packages according to setting-specific requirements, treatment strategies and local customs. Further studies are required to test the TPO approach as well in carts and other emergency storage systems.
Additional factors might influence retrieval time. It is assumed that personnel are faster in equipment retrieval if they regularly familiarize themselves with the emergency backpack. Interestingly, there was no significant correlation between the frequency of self-acquaintance and the equipment retrieval time. However, this might be due to the possible answers in the questionnaire: The majority of participants chose “1–2 times every 6 months” or “1–2 times every 12 months” and the differences here might be too low to obtain significant results. To our knowledge, there is no clear data on how often personnel should familiarize themselves with emergency kits. However, in basic life support, a significant loss of effectiveness of skills, such as ventilation and chest compression, occurs as soon as four weeks after a training session (10). Hence, despite the results of this study, we still recommend regular, short-interval familiarization and training with all emergency equipment.
Within this study, when using the classical emergency backpack, personnel with more neonatal working experience showed faster retrieval times for epinephrine equipment. Interestingly, this was not the case when the TPO kit was used. One might conclude that more experience is required to reach fast retrieval times for the classical kit, and that this is not necessary for the TPO kit due to the easier storage approach. However, the opposite findings were noted for the retrieval time for intubation. Specifically, more experienced personnel retrieved equipment for intubation faster when using the TPO kit, but this finding was not significant for the classical kit. Based on the results of this study, we conclude that years of experience are not sufficient to explain the speed of equipment retrieval. One explanation might be that regular, short-interval training is more important than years of experience in the case of emergency kit handling.
The impact of the subjective self-evaluation in the handling of the emergency kit was analyzed to test the assumption that personnel with higher self-ratings might also show faster retrieval times. Surprisingly, personnel with higher ratings in the self-evaluation of “overall handling” of the emergency kit were not faster than personnel with lower ratings. This finding reflects that an individual's perception about their own preparedness for an emergency event might be incorrect. Consequently, in addition to optimizing equipment organization with TPO packages, we recommend obligatory training for the personnel regardless of self-perceptions of familiarity or experience.
In the case of an emergency event that occurs outside the NICU, standardized procedures are in order in our institution so that ICU personnel running to the site of the event also bring along the emergency backpack. Therefore, one might assume that ICU personnel would be more familiar with working with the emergency backpack and thus might show faster retrieval times. Interestingly, this was not the case in our study. When comparing ICU to IMC personnel, nearly all retrieval times as well as the number of missing items were not significantly different. One possible explanation for this finding might be that although emergency events occur more frequently in ICUs, they are still rare events. Therefore, ICU personnel might wrongly assume that they are “trained” sufficiently by real-life events. Additionally, given that ICU personnel had more years of neonatal experience, incorrect self-evaluation of preparedness for emergency events might further aggravate this issue. Consequently, we recommend that all personnel, including (or maybe especially) ICU personnel, regularly undergo training for the handling of emergency kits and equipment retrieval.
This study was conducted using in-situ simulation, but without the use of a resuscitation scenario (the participants were merely asked to retrieve the according equipment). Also, it was performed exclusively in one single institution. Further, only a subset of tasks of the TPO-bags were tested and which kit was used first was not randomized.
The results might differ in a resuscitation-based simulation scenario, a non-simulation (real life) setting or in other settings/countries.
The TPO approach in the neonatal emergency backpack seems to lead to faster retrieval times of emergency equipment, fewer missing items and clearer arrangement compared to the classical ABC or material-oriented storage approach.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Medical University Vienna, Austria. The patients/participants provided their written informed consent to participate in this study.
LS: conceptualization, methodology, investigation, formal analysis, data curation, writing—review & editing, and project administration. MH-D: conceptualization, methodology, investigation, formal analysis, and writing—review & editing. KK-S and AB: conceptualization, methodology, formal analysis, and writing—review & editing. ES: conceptualization, methodology, formal analysis, data curation, writing—original draft, visualization, and project administration. All authors contributed to the article and approved the submitted version.
ES is a neonatal consultant at the Medical University Vienna and managing partner/CEO of SIMCharacters Training GmbH (Austria), a company providing medical simulation training in German-speaking countries. However, there is no financial or other related benefit in relation to this manuscript.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rodríguez-Núñez A, López-Herce Cid J, Calvo-Macías C, Carrillo-Alvarez A. Do we need guidelines for pediatric resuscitation carts/trolleys/backpacks content and management? Resuscitation. (2017) 114:e19–20. doi: 10.1016/j.resuscitation.2017.02.027
2. López-Herce Cid J, Rodríguez Núñez A, Carrillo Álvarez Á, Zeballos Sarrato G, Martínez Fernández-Llamazares C, Calvo Macías C, et al. Materials for the paediatric resuscitation trolley or backpack: Expert recommendations. An Pediatr (Barc). (2018) 88:173.e1–7. doi: 10.1016/j.anpede.2017.05.002
3. Chan J, Chan B, Ho HL, Chan KM, Kan PG, Lam HS. The neonatal resuscitation algorithm organized cart is more efficient than the airway-breathing-circulation organized drawer: a crossover randomized control trial. Eur J Emerg Med. (2016) 23:258–62. doi: 10.1097/MEJ.0000000000000251
4. Schwindt EM, Hoffmann F, Deindl P, Waldhoer TJ, Schwindt JC. Duration to establish an emergency vascular access and how to accelerate it: a simulation-based study performed in real-life neonatal resuscitation rooms. Pediatr Crit Care Med. (2018) 19:468–76. doi: 10.1097/PCC.0000000000001508
5. Lanoix R, Golden J. The facilitated pediatric resuscitation room. J Emerg Med. (1999) 17:363–6. doi: 10.1016/S0736-4679(98)00182-6
6. Swanson C. Reorganizing a resuscitation room using six sigma (6S) principles. J Emerg Nurs. (2014) 40:371–6. doi: 10.1016/j.jen.2013.04.006
7. Haerkens MHTM, Kox M, Noe PM, Van Der Hoeven JG, Pickkers P. Crew resource management in the trauma room: a prospective 3-year cohort study. Eur J Emerg Med. (2018) 25:281–7. doi: 10.1097/MEJ.0000000000000458
8. Ricci MA, Brumsted JR. Crew resource management: using aviation techniques to improve operating room safety. Aviat Space Environ Med. (2012) 83:441–4. doi: 10.3357/ASEM.3149.2012
9. Lefebvre MS, Milloy S, Joynt C. Optimal crash cart configuration for a surgical NICU: utilizing human factors principles. Adv Neonatal Care. (2021) 21:289–396. doi: 10.1097/ANC.0000000000000814
Keywords: neonatology and pediatric intensive care, emergency equipment and supply, human factors, emergency and critical care, crew resource management (CRM)
Citation: Sommer L, Huber-Dangl M, Klebermaß-Schrehof K, Berger A and Schwindt E (2021) A Novel Approach for More Effective Emergency Equipment Storage: The Task-Based Package-Organized Neonatal Emergency Backpack. Front. Pediatr. 9:771396. doi: 10.3389/fped.2021.771396
Received: 06 September 2021; Accepted: 02 December 2021;
Published: 23 December 2021.
Edited by:
Jeroen J. van Vonderen, Leiden University Medical Center, NetherlandsCopyright © 2021 Sommer, Huber-Dangl, Klebermaß-Schrehof, Berger and Schwindt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eva Schwindt, ZXZhLnNjaHdpbmR0QG1lZHVuaXdpZW4uYWMuYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.