 Catherine Billard1*
Catherine Billard1* Camille Jung2
Camille Jung2 Arnold Munnich3
Arnold Munnich3 Sahawanatou Gassama1,4
Sahawanatou Gassama1,4 Monique Touzin1,4
Monique Touzin1,4 Anne Mirassou1
Anne Mirassou1 Thiébaut-Noël Willig5,6
Thiébaut-Noël Willig5,6- 1Association pour la Recherche sur les Troubles des Apprentissages, Paris, France
- 2Clinical Research Center, Centre Hospitalier Intercommunal de Créteil, Créteil, France
- 3Université de Paris and Imagine Institute (INSERM UMR1163), Paris, France
- 4Centre Ressource sur les Troubles des Apprentissages, Paris Santé Réussite, Paris, France
- 5ELSAN & EvEnTAil Assessment Center, Toulouse, France
- 6Association Française de Pédiatrie Ambulatoire, Orléans, France
Background: Learning disabilities (LDs) are a major public health issue, affecting cognitive functions and academic performance for 8% of children. If LDs are not detected early and addressed through appropriate interventions, they have a heavy impact on these children in the social, educational, and professional spheres, at great cost to society. The BMT-i (Batterie Modulable de Tests informatisée, or “computerized Adaptable Test Battery”) enables fast, easy, reliable assessments for each cognitive domain. It has previously been validated in children ages 4–13 who had no prior complaints. The present study demonstrates the sensitivity of the BMT-i, relative to reference test batteries, for 191 children with cognitive difficulties.
Materials and Methods: These 191 subjects were included in the study by the 14 pediatricians treating them for complaints in five cognitive domains: written language [60 (cases)]; mathematical cognition (40); oral language (60); handwriting, drawing, and visuospatial construction (45); and attention and executive functioning (45). In accordance with a predefined protocol, the children were administered BMT-i tests first, by their pediatricians, and reference tests later, by specialists to whom the BMT-i test results were not disclosed. Comparison of BMT-i and reference test results made it possible to evaluate sensitivity and agreement between tests.
Results: For each of the five domains, the BMT-i was very sensitive (0.91–1), and normal BMT-i results were highly predictive of normal results for specialized reference tests [negative likelihood ratio (LR–): 0–0.16]. There was close agreement between BMT-i and reference tests in all domains except attention and executive functioning, for which only moderate agreement was observed.
Conclusion: The BMT-i offers rapid, reliable, simple computerized assessments whose sensitivity and agreement with reference test batteries make it a suitable first-line instrument for LD screening in children 4–13 years old.
Introduction
The high prevalence of learning disabilities (LDs)—estimated at 8% among children ages 3–17 (1)—makes them a public health priority worldwide. LDs are neurodevelopmental disorders that impact one or more cognitive functions in affected children, who may struggle with the development of academic skills (written language and mathematical cognition), early language and fine motor skill acquisition, or maintaining attention (DSM-5) (2). Current models attempt to integrate (i) neuropsychological knowledge about learning, (ii) underlying cognitive abilities, and (iii) neurobiological aspects, including potential inheritance and environmental factors (3). Researchers are overwhelmingly in favor of early LD detection because the efficacy of rapid treatment has been demonstrated (4–8). The diversity of the domains affected, alone or in combination, requires thorough evaluation of the nature, severity, and development of deficits (2, 9, 10). The consequences of LDs on the personal, academic, and later, professional lives of children depend on how early they are treated (8). Recommendations made by the French National Authority for Health (HAS) define treatment paths for children with LDs in France according to the severity of the disorders and how quickly they progress (11). These HAS recommendations indicate the role of physicians in screening, referral to specialists, and coordination with teachers. Though countries differ in how they manage LD treatment (12), evaluation of affected cognitive domains and the progression of deficits requires carefully validated instruments in the language of the children assessed (13).
The computerized Adaptable Test Battery (BMT-i) is a set of tests for the first-line assessment of children's academic skills and cognitive functions, from kindergarten (age 4) to seventh grade (age 13). It permits broad exploration of written language abilities (reading fluency, reading comprehension, and spelling), mathematical cognition (numbers, arithmetic, and problem-solving), and three further cognitive domains (verbal, non-verbal, and attention and executive functioning). BMT-i tests are meant to be simple to administer, short (10–30 min per domain, depending on age), and easy to score, and they can be taken at school or during an appointment with a health professional. Their purpose is rapid identification of children who require specialized assessments for precise LD diagnosis (14, 15).
We recently reported the validation of the BMT-i for a sample of 1,074 French children with no prior complaints (15). Here we present its validation for a group of children with cognitive difficulties suggesting possible LDs. We demonstrate that the sensitivity of the BMT-i and its agreement with reference test batteries make it a robust tool for initial detection of LDs in children.
Materials and Methods
Participants
The study population consisted of children suspected of having LDs due to complaints concerning one or more of the following cognitive domains: written language (WL); mathematical cognition (MC); oral language (OL); handwriting, drawing, and visuospatial construction (HV); and attention and executive functioning (AE). Child patients were recruited by 14 pediatricians at their offices or in hospitals (Figure 1). These practitioners had expertise in LDs including the use of the BMT-i for their professional screening practice. All pediatricians collaborating to the study received a 2-days specific training on the use of the BMT-i as part of the protocol. In addition, a member of the research team (who had no access to the specialized evaluations) was available to address questions.
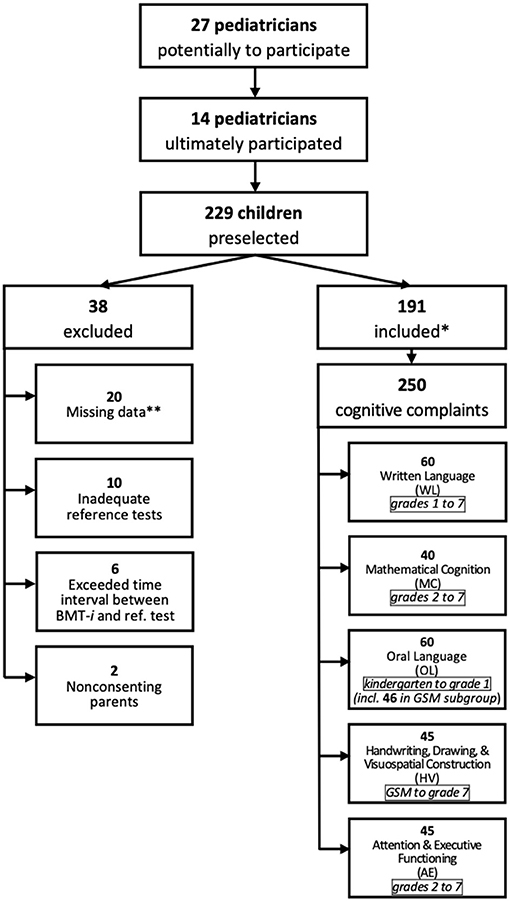
Figure 1. Study recruitment. *With complaints in one or more cognitive domains. **Excluded because >1 datum missing. GSM, final year of French kindergarten (grande section de maternelle).
The number of subjects included (>184 children) was calculated from the desired accuracy of 5% with a 95% confidence interval, for an expected sensitivity of 0.85 and a disease prevalence of 75% in this population with complaint. Nearly two hundred children were included, about a quarter of whom had cognitive complaints in multiple domains. Few children were lost to follow-up.
To be eligible for inclusion, children had to be (i) at least 4 years old and no more than 13 years and 11 months old, (ii) registered with the French social security system, (iii) seeing their pediatrician for a complaint, defined by symptoms their parents described, that called for a specialized evaluation within 4 months. Children known to have an intellectual disability or autism spectrum disorder, or whose both parents were not speaking French, or who had been in the French school system for <2 years, were not eligible. Pediatricians approached the legal representatives of eligible children, offering to include them in the study.
Written informed consent was first obtained from the legal representatives of children who were to be included. The study protocol was approved by an ethics committee (CPP 2018-A-O1870-55).
Test Administration
Once consent was obtained, the children had appointments with their pediatricians, who administered the BMT-i tests assessing the particular cognitive domains corresponding to their complaints. Then, within 4 months, these children were reassessed by specialists uninformed of the BMT-i results, using reference test batteries. Study coordinators verified inclusions and protocol observance, and independently collected the BMT-i and reference test battery data. Table 1 presents BMT-i and corresponding reference battery tests, according to age and cognitive domain.
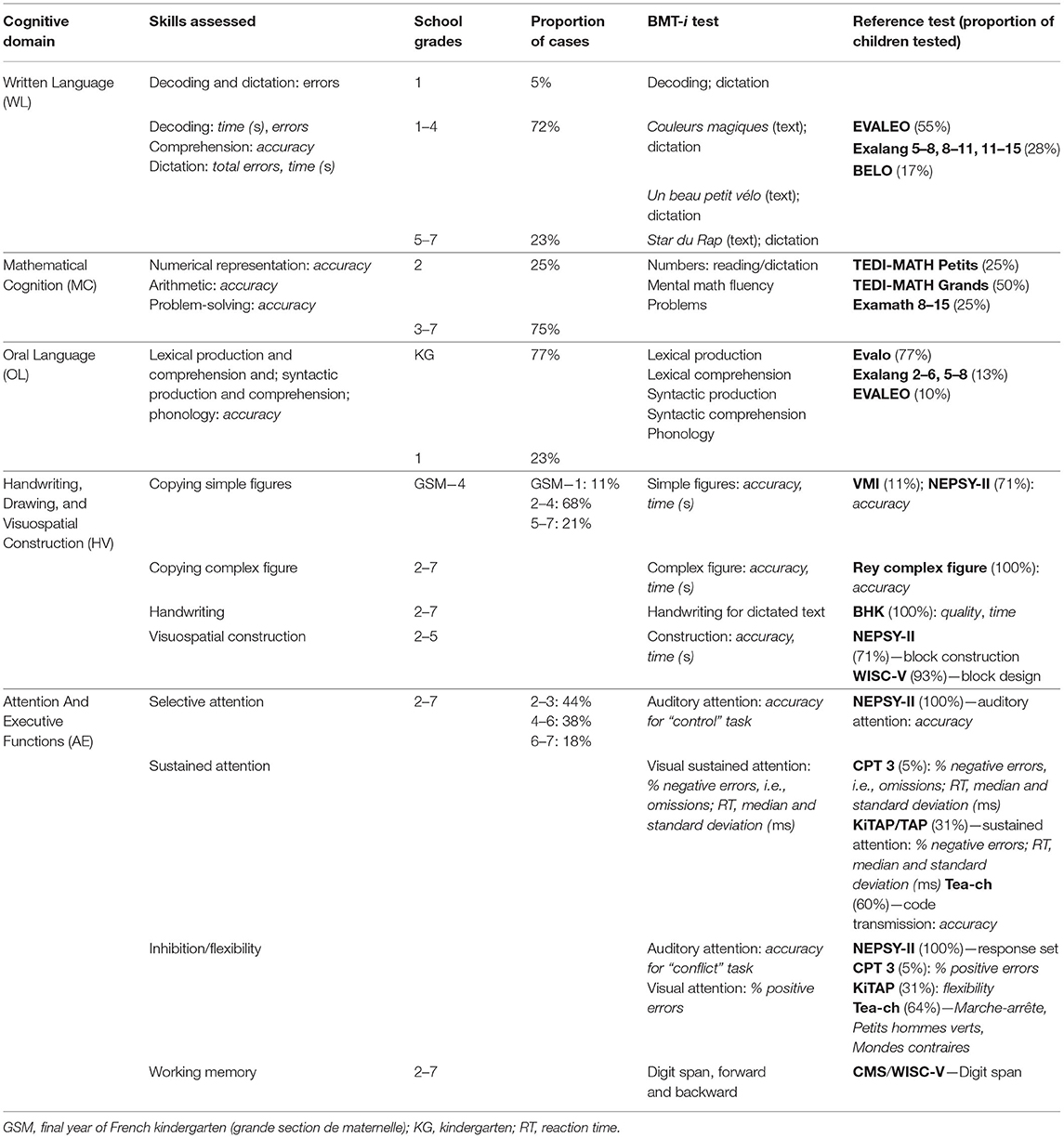
Table 1. Breakdown of BMT-i and reference tests used, by cognitive domain and school grade.
Administration of BMT-i Tests by Pediatricians
For each participant, pediatricians recorded medical history, including perinatal data and information on prior treatment for the complaint; noted if one of the parents spoke a language other than French; and identified any financial hardship entitling the patient to free care. Parents were provided with a questionnaire they passed on to their child's teacher on which the latter rated their student's difficulties (none, moderate, or major) in each cognitive domain. During individual appointments under normal conditions and lasting 30–40 min, pediatricians administered the BMT-i tests corresponding to their patient's complaint and school grade (Table 1) (14, 15).
Reading (speed, accuracy, and comprehension) and spelling tests assessed WL complaints. For complaints concerning MC, number reading and dictation, mental math, and problem-solving tests were used. In the case of OL complaints, tests evaluating phonology, lexical production and comprehension, and syntactic production and comprehension were administered. For HV-related complaints, children were asked to copy simple and complex figures, where speed and quality reflected drawing abilities, and perform 15 cube construction tasks, where the same variables measured visuospatial construction skills. A handwriting score was assigned for dictations. In addition, motor skills were assessed using the European-French Developmental Coordination Disorder Questionnaire (DCDQ-FE), which detects motor skill deficits (16). When children's complaints concerned attention and executive functioning, the sustained visual attention and controlled auditory attention tests assessed their ability to maintain attention, selective attention, inhibition, and flexibility (15, 17), while forward and backward digit span tests evaluated working memory. Functional difficulty in everyday settings was measured according to DSM-5 criteria (2).
Test results for each child were anonymized, assigned codes, and sent to the research team through a secure online platform to be checked and recorded. The pediatricians referred their child patients to professionals specialized in the cognitive domains concerned, informing these specialists of the study protocol but not disclosing BMT-i results.
Administration of Reference Tests
The specialists performed their evaluations under the usual conditions of their work. Pediatricians gave the specialists a letter from the research team that specified the tests to be administered for each cognitive domain, chosen from among the commonly used, carefully validated test batteries indicated by the researchers. Recommended minimal WL skills (18, 19)—reading speed, accuracy, and comprehension, as well as spelling—were measured with the EVALEO (20), Exalang (21, 22), or BELO (23) speech-language batteries (Table 1). For MC, skills in numeric representation, mental math, and problem-solving were assessed with tests from three batteries adapted to children's school grades and, like the BMT-i, designed according to current neuropsychological models (24–26): TEDI-MATH (27), TEDI-MATH Grands (28), and Examath 8–15 (29). Recommended OL skills (30, 31) were assessed by speech-language pathologists using five standard language production and comprehension tests from the Evalo (32), Exalang (33), and EVALEO (20) batteries. Psychomotor or occupational therapists assessed HV abilities—handwriting, drawing, and visuospatial construction (34–36)—by having children (i) copy figures from the VMI (36) or NEPSY-II (37) test batteries; (ii) copy the Rey complex figure (38); (iii) write, measuring speed and quality with the BHK scale (39); and (iv) complete NEPSY-II (37) or WISC-V (40) cube construction tasks. To measure attention (17) and executive functioning (41) (AE), a neuropsychologist administered an IQ test (WISC-V) and the NEPSY-II Auditory Attention & Response Set subtest (37), along with others from the Conners Continuous Performance Test (CPT 3) (42), TAP/KiTAP (43), and Tea-ch (44) batteries that assess sustained attention and inhibition/flexibility. Working memory was gauged with the WISC-V Digit Span (40) or CMS Numbers (45) subtest. Functional impairment in daily life was evaluated with the Behavior Rating Inventory of Executive Function (BRIEF) (46).
Analysis of Data
Data were analyzed for each of the five cognitive domains in question. For OL in particular, which concerned 60 children, the researchers also compared results from a short version of the BMT-i (an evaluation of lexical comprehension, syntactic production, and phonological quality, lasting about 10 min) with those for the five-skill speech-language assessment. In addition, they analyzed data for a homogeneous subgroup (46 out of the 60 children) whose members were all in the last year of French kindergarten (grande section de maternelle, or GSM) and had been evaluated using the same speech-language battery (Evalo).
Differences in school grades and reference test battery norms necessitated harmonization of scores before they could be compared. Thus, scores were converted to a three-point scale −0, or normal, if the cumulative percentage was >20%; 1, or low, if it was between 7 and 20%; and 2, or very low, if it was ≤7%—while preserving the correspondence between cumulative percentages, standard scores, and z-scores, in accordance with the American Academy of Clinical Neuropsychology consensus statement (47).
Score conversions were performed independently by pediatricians, for the BMT-i, and specialists, for reference batteries, in accordance with the study protocol. Each skill was rated on the basis of these BMT-i scores: a level of 2 was assigned when one of the scores was very low; 1 if multiple scores were low, and 0 in all other cases, including when only one score was low. Pediatricians then made one of three recommendations: specialized testing needed, if at least one of the skills had a very low rating (level 2); the need for specialized testing to be discussed, if multiple skills had low ratings (level 1); or no need for specialized testing, in any other case (level 0). Similarly, specialists categorized children as having a disorder (=2), moderately impaired (=1), or normal (=0).
For each cognitive domain, an independent expert (neuropsychologist or speech therapist) otherwise unassociated with the study performed a blind analysis of the pediatricians' and specialists' findings. The independent expert also rescored BMT-i and Rey complex figure copying tests. When the original score did not match the later one, a definitive score was assigned after discussion with the research team. For the assessment of attention in particular, explicit qualitative aspects observed in 4 of the children—e.g., transient fatigability, fluctuation, or slowness—influenced the interpretation of scores in the professional's conclusion, which was retained. For the purpose of calculating BMT-i sensitivity and specificity, scores indicating disorders (=2) or moderate deficits (=1) were grouped together, to distinguish both from normal (=0) scores.
Statistical Analysis
Sensitivity, specificity, and both positive (LR+) and negative (LR–) likelihood ratios were calculated from the findings of the pediatricians (BMT-i) and specialists (reference test batteries). The desired sensitivity was >85%. The LR+ estimates the probability of correctly diagnosing a disorder when test results are positive. The supplemental diagnostic value of the test is low if the LR+ is between 1 and 2, intermediate if between 2 and 5, and high if >5. In contrast, the LR– estimates the probability of correctly rejecting diagnosis of a disorder when test results are negative. The supplemental diagnostic value of the test is low if the LR– is between 0.5 and 1, intermediate if between 0.2 and 0.5, considerable if between 0.1 and 0.2, and high if <0.1. The correlation between converted BMT-i and reference battery test scores was evaluated using the Matthews correlation coefficient (MCC), a derivative of the Pearson correlation coefficient for unbalanced populations (48). Agreement between the findings of pediatricians and specialists was measured with Cohen's kappa (κ), where values in the range of 0.21–0.40 indicate fair agreement; 0.41–0.60, moderate; 0.61–0.80, substantial; and 0.81–1.00, almost perfect agreement (49). Raw OL test scores for the GSM subgroup were compared using the Pearson correlation coefficient (r). The Pearson correlation coefficient was also calculated for comparison of raw scores from the BMT-i controlled auditory attention test and the NEPSY test.
Results
Characteristics of Study Population
Figure 1 illustrates the study inclusion process and provides a breakdown of the 250 complaints by cognitive domain. Only 14 of the 27 pediatricians initially identified were able to take part in the study. Spread across France −12 in cities and 2 in suburban areas −9 of them had private practices, while the remaining 5 worked in hospitals.
Of the 229 children preselected, 191 were included between March 31, 2019, and September 1, 2020, 28% of them presenting with complaints that concerned 2 or 3 cognitive domains. Due to parental refusal of consent or failure to follow the study protocol, 38 of the 229 children were excluded. For the 191 children included, 250 assessments for one of the five cognitive domains were conducted: 60 for WL; 40 for MC; 60 for OL, including the GSM subgroup of 46 children; 45 for HV; and 45 for AE. All children had a normal evaluation of their vision and hearing, and were searched for emotional disorders. Moreover, children included for a complaint affecting attention/executive functions did not receive any treatment during and between the two evaluations (BMT-i and specialized assessments). Teacher questionnaires were missing in 9% of the cases. Of the 250 assessments, 3% were missing a single skill score; 9%, DCDQ-FE (HV) data; and 15%, DSM-5 evaluations (AE). Table 2 summarizes population characteristics for each cognitive complaint. Children from bilingual (defined as one parent speaking a language other than French) and underprivileged families made up half (50%) of those in the OL category. Boys predominated in the MC (67%), HV (75%), and AE (73%) categories. Over half of the children included were undergoing reeducation, but the percentage varied by cognitive domain, ranging from 28% for OL to 72% for WL.
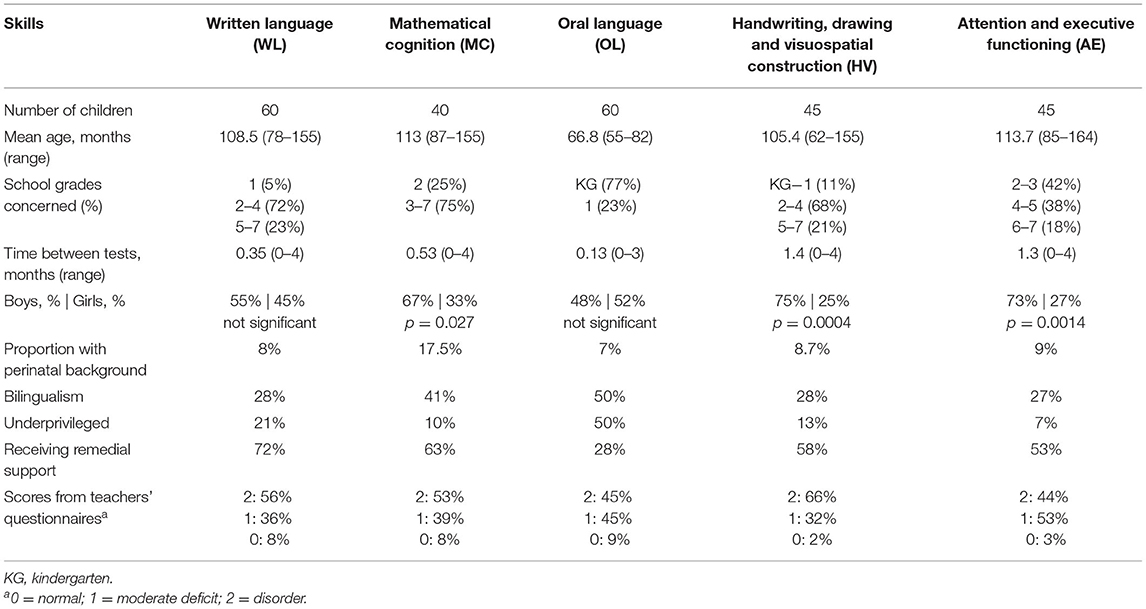
Table 2. Characteristics of study population.
Agreement Between Scores Assigned by Pediatricians and Specialists
For each of the five cognitive domains considered, Figure 2 gives an overview of assessments made by specialists, pediatricians, and teachers, and Tables 3–7 provide statistics measuring the correspondence between the findings of pediatricians and specialists.

Figure 2. Agreement of BMT-i and teachers' questionnaires with specialized assessments. a GSM subgroup assessed by Evalo (n = 46); GSM, final year of French kindergarten (grande section de maternelle); κ, Cohen's kappa; KG, kindergarten; Q Teacher, teachers' questionnaire; Spe, specialized. Possible scores were 0 (normal), 1 (moderate deficit), 2 (disorder).
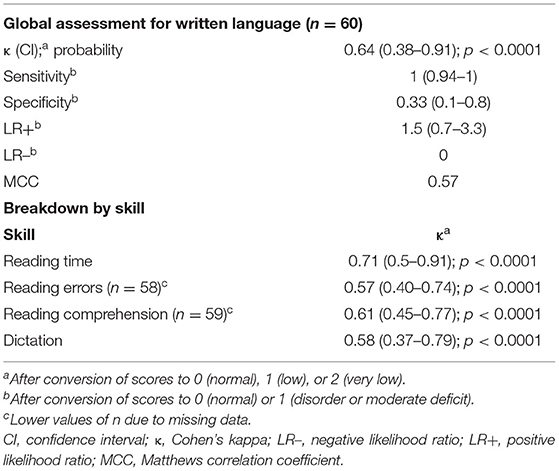
Table 3. Written language: BMT-i sensitivity and agreement with specialized assessments.
For WL (Table 3), analysis revealed substantial agreement between pediatricians' and specialists' scores (κ = 0.64), maximum sensitivity for the BMT-i (1), low specificity (0.33), and an intermediate MCC value (0.57). Values of κ were also satisfactory for each skill considered. They were higher for reading speed (0.71) and comprehension (0.61) than for accuracy (0.57) and spelling (0.58).
The speech-language pathologists diagnosed disorders for 91% of the participants, and pediatricians esteemed specialized testing was required for 88% of them (Figure 2). In 92% of the cases, teachers' questionnaires described complaints of major (49%) or moderate (43%) severity, in disagreement with the conclusions of the speech-language pathologist (kappa = 0.14). Speech-language assessments revealed very low reading speed (for 82% of children) and spelling (for 83%) levels, while the level of reading comprehension was low for only half of the children. A quarter of the children assessed as having disorders were not undergoing reeducation at the time of the study.
For MC (Table 4), analysis likewise showed considerable agreement between pediatricians' and specialists' scores (κ = 0.76), maximum sensitivity (1), high specificity (0.71), and a high MCC (0.82). Values of κ were moderate for conversion of numeric representations (0.49) and mental math (0.47). There was moderate to no agreement for problem-solving assessments, depending on the reference test battery used. It was low with TEDI-MATH Petits, moderate with Examath, and nil with TEDI-MATH Grands.
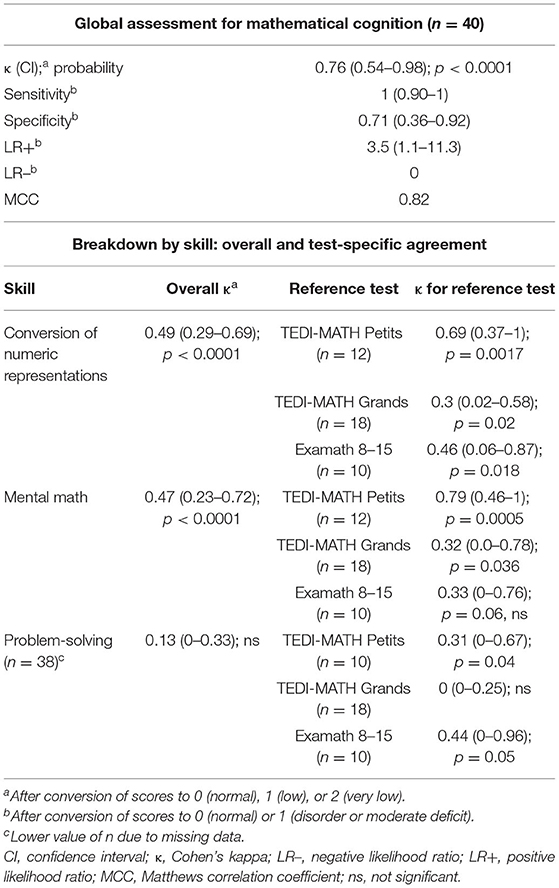
Table 4. Mathematical cognition: BMT-i sensitivity and agreement with specialized assessments.
Most children with MC complaints were diagnosed with disorders: 82% according to pediatricians using the BMT-i, and 80% according to specialists. In 92% of the cases, teachers' questionnaires described complaints of major (53%) or moderate (39%) severity (Figure 2); however, agreement with the conclusions of the speech-language pathologist was low (κ = 0.27).
The profile of deficits detected by the speech-language pathologist was mixed: mental math was severely affected for 65% of the cases; conversion of numeric representations, for 45%; and problem-solving, for 36%. At the time of the study, two-thirds of the children were undergoing speech-language reeducation for written language or mathematics.
Table 5 gives comparative statistics for OL assessments (n = 60). They indicate moderate agreement between the pediatrician's and specialist's global assessments for all five skills tested (κ = 0.58), high sensitivity (0.98), moderate specificity (0.60), and a moderate MCC value (0.66). Results are similar when we compare the short version of the BMT-i to the full speech-language assessment. However, for the GSM subgroup (n = 46), there was substantial agreement (κ = 0.68), and the sensitivity (0.98), specificity (0.75), and MCC value (0.73) were all satisfactory. For these 46 children, similar values were obtained when comparing results for the short BMT-i to those for the full speech-language assessment (sensitivity = 0.95; specificity = 1; MCC = 0.80).
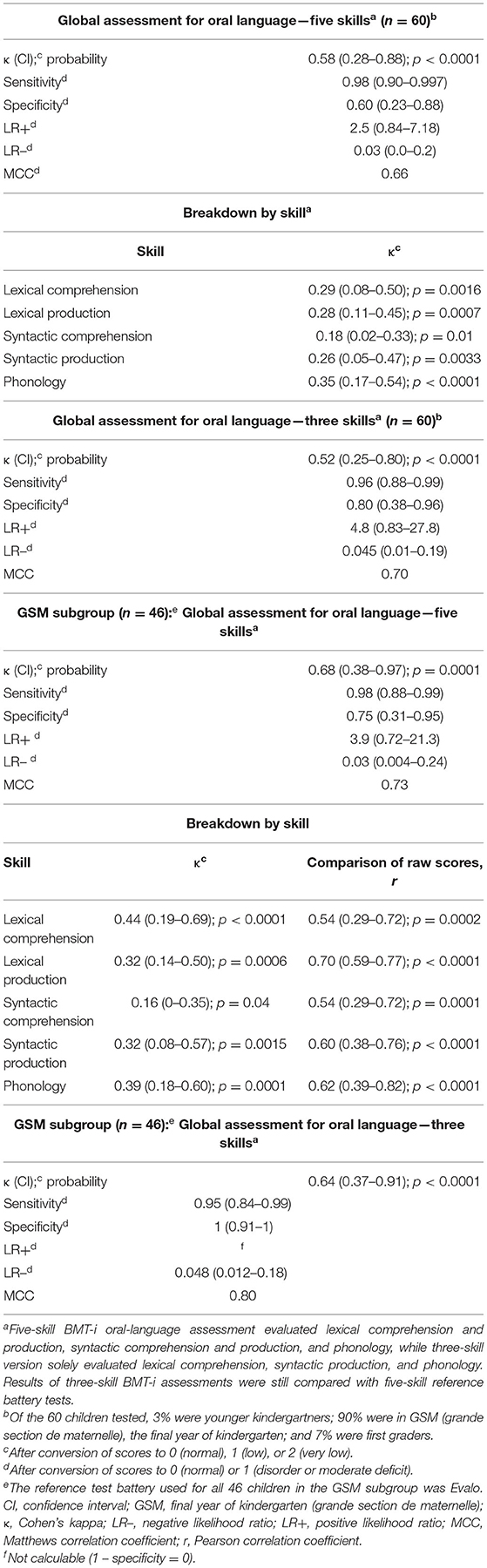
Table 5. Oral language: BMT-i sensitivity and agreement with specialized assessments.
If we consider the study population as a whole, κ values for each skill were low. Yet, in the GSM subgroup, BMT-i and reference test scores were strongly correlated for each of the five skills assessed (r: 0.54–0.70; p: < 0.0001–0.0002).
The majority of both the study population and the GSM subgroup were assessed as having OL disorders by the pediatrician (88%) and the specialist (85%) alike, though only 28% were following a course of speech-language reeducation at the time of the study. In 89% of the cases, the teachers' questionnaires described complaints of major (45%) or moderate (42%) severity, and they were not sufficiently in agreement with the speech-language pathologist's assessment (κ = 0.17) (Figure 2). The latter revealed a mixed profile of lexical or syntactic deficits for 75% of the cases and phonological deficits for 40%.
Table 6 presents data for the HV domain. Here there was an outstanding level of agreement between the pediatrician's and specialist's assessments (κ = 0.88). The BMT-i sensitivity, specificity, and MCC statistics all had maximum values (=1). Levels of agreement nonetheless differed by skill: they were high for handwriting, moderate for the Rey complex figure, and low for the visuospatial construction tests. There was no agreement for copying of simple figures.
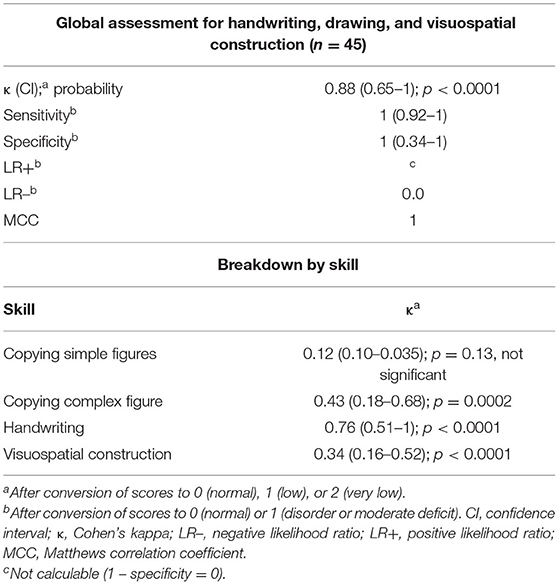
Table 6. Handwriting, drawing, and visuospatial construction: BMT-i sensitivity and agreement with specialized assessments.
Most pediatrician's (91%) and specialist's (89%) assessments diagnosed disorders. For 98% of all cases, teachers' questionnaires indicated complaints of major (62%) or moderate (36%) severity and were in disagreement with the specialist's assessment (κ = 0.05) (Figure 2). DCDQ-FE responses showed that developmental coordination disorder was suspected for 63% of the children, but there was a lack of agreement with the assessments of the pediatrician (κ = 0.01; not significant) and the specialist (κ = 0.02; not significant). Children's HV profiles varied, but handwriting deficits were detected in 80% of the initial assessments and 83% of the specialized assessments. One out of two children had difficulties with the complex figure copying task.
The systematic psychometric evaluation in AE domain confirmed the absence of mental disability: the average values of the Verbal Comprehension Index (VCI), Fluid Reasoning Index (FRI) and Visual Spatial Index (VSI) were 105, 104, and 100, respectively. None of the children had any of those indexes below 81. AE disorders were reported for 67% of the BMT-i and of the specialized test (Figure 2). The global AE assessments of the pediatrician and the neuropsychologist (Table 7) were fair in agreement (κ = 0.38), sensitivity high (0.91), and specificity (0.56) and MCC value (0.49) both modest. On the other hand, normal BMT-i results suggested that a normal neuropsychological assessment was fairly likely (LR– = 0.16). There was a low but acceptable level of agreement for the sustained attention and flexibility/inhibition tests. For the selective attention and digit span tests, the level of agreement was insufficient.
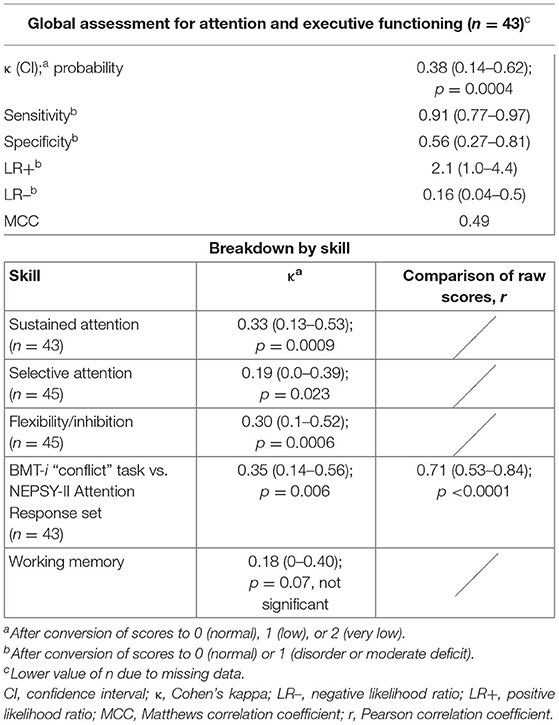
Table 7. Attention and executive functioning: BMT-i sensitivity and agreement with specialized assessments.
In 97% of the cases, teachers' questionnaires revealed attentional complaints of major (44%) or moderate (53%) severity, though there was no agreement with the specialist's assessment (κ = 0.08) (Figure 2). DSM-5 criteria were met (≥6 symptoms) in 82% of all cases for inattention and in 47% of the cases for hyperactivity/impulsivity, but there was no agreement with the overall neuropsychological assessment (κ: 0.01 and 0.01, respectively; not significant). In five children (10%), neither of the two DSM-5 scales confirmed the diagnostic criteria for ADHD but four of the five had abnormal results with both the BMT-i and the specialized evaluations. For the BRIEF assessments, the mean Global Executive Composite was at the disorder threshold (T-score: 70) and the mean Metacognition Index was close to it (T-score: 69). These values did not vary with the findings of the neuropsychological assessments.
Children's attentional profiles were very diverse. Disorders of selective attention were identified for 38% of the cases; of sustained attention, for 35%; and of flexibility/inhibition, for 49% of the specialized assessments. The correlation between NEPSY raw scores (Response set) and BMT-i auditory attention results (“conflict” task) was highly significant [r = 0.71 (0.53–0.84); p < 0.0001].
Discussion
For our cohort of children with cognitive complaints, we have reported the sensitivity of the BMT-i in the domains concerned (2, 9–11) and its agreement with the reference test batteries used by specialists. This study was only possible due to the earlier validation of the BMT-i with a vast cross-sectional sample of French school children with no complaints (15). The large proportion of children receiving no remedial support despite difficulties detected during the initial examination underscores the value of screening with the BMT-i. The fact that 28% of children were struggling in more than one cognitive domain also argues for a single, comprehensive battery to screen for difficulties in multiple skill areas (15).
Our findings confirm the high sensitivity (0.91–1) of overall BMT-i assessments compared with specialized batteries, for each of the domains considered. Furthermore, the likelihood of normal BMT-i results accurately predicting normal results for a specialized assessment was considerable. Specificity varied across domains (0.33–1): high for MC and HV; moderate for OL and AE; and low for WL. The likelihood that BMT-i results indicating a deficit would accurately predict the identification of a disorder through a specialized assessment was fair for MC, HV, and OL; moderate for AE; and low for WL. The level of agreement between global BMT-i assessments and specialists' assessments was excellent for MC and HV; substantial for WL, as well as for OL in the GSM subgroup; but lower for AE. Thus, the BMT-i offers a level of performance expected of first-line screening instruments whose aim is to identify the majority of children in need of referral to a specialist.
The extent to which BMT-i and specialized assessments agreed on a test-by-test basis varies between cognitive domains. Agreement was lowest for arithmetic problems (MC), syntactic comprehension (OL), copying of simple figures (HV), and selective attention (AE).
A consensus exists on the need for validated tools suitable for each cognitive domain—not only to identify students who are struggling, but also to determine the profile and magnitude of their cognitive strengths and weaknesses, and to monitor progress made (3–5, 50). The BMT-i also provides such information for the particular skills affected. For example, by profiling and gauging the severity of deficits in individual WL skills, the BMT-i can help choose the appropriate next step (18), be it an urgent referral for a specialized assessment in the event of a severe deficit or one affecting reading comprehension (19), or an educational intervention in the event of a deficit in reading speed alone (51). For MC, from kindergarten to middle school, the BMT-i, in accordance with current neuropsychological models (24–26, 52), offers a first-line assessment of numeric representation and arithmetic skills, which are weaker among French students (53). With regards to OL, use of the shorter three-test BMT-i allows for efficient and reliable detection of language deficits among older kindergartners (GSM). Interviews alone are not as effective in identifying such deficits (54), especially in underprivileged settings (30, 31). HV test results complement the information provided by the DCDQ-FE, which is limited to motor deficits (16), permitting detection of handwriting, drawing, and visuospatial impairments seen in children with developmental coordination disorder (55) or as isolated conditions (56). The BMT-i affords a comprehensive vision of the various components of writing (speed, handwriting, and spelling), to help define a remedial program when dysgraphia is present (57). In the case of AE difficulties, a preliminary formal computerized assessment of cognitive functions using the BMT-i supplements' data from questionnaires, evaluates the severity of any associated academic deficits (58), and can affirm the need for a neuropsychological assessment, which is recommended in the presence of AE complaints (17, 41, 58).
International recommendations propose supplementing the standard psychometric evaluations—e.g., Wechsler (40), NEPSY (37), and KABC II (59) scales—with test batteries measuring academic skills. There are numerous English-language test batteries of this sort, including the Wechsler Individual Achievement Test–Second Edition (WIAT-II) (60), Wide Range Achievement Test−5th Edition (WRAT5) (61), Woodcock-Johnson IV Tests of Early Cognitive and Academic Development (ECAD) (62), and the Kaufman Test of Educational Achievement–Second Edition (KTEA-II) (63), taken to be the standard instruments. With the exception of the WIAT-II, normed with a limited sample of francophone Canadians, none has been calibrated for a French-speaking population (64). Furthermore, as these batteries are used in combination with a psychometric evaluation, they are better described as integral components of long and costly specialized assessments than as screening tools. While the EPOCY (65), based on the KTEA-II, is a French-language battery, it only evaluates academic skill levels. None of these instruments is computerized, nor do they allow for simultaneous evaluation of skills and underlying cognitive functions. Conversely, the BMT-i is the only general standardized modular instrument for first-line assessment of the strengths and weaknesses of children's academic skills and cognitive functioning.
There are, however, several limitations of our study. Firstly, our sample solely consisted of children with cognitive complaints. A study simultaneously considering cohorts of children with and without complaints would undoubtedly have been more balanced, but obtaining reliable normative data for a representative population without prior complaints was a crucial prerequisite for a study of children with complaints (48). Hence, this external validation cannot be regarded as a cohort study with systematic evaluation of all possibly affected domains in LDs nor as a conclusive diagnostic study. Indeed, the population studied included both children seen for the first time and children already taken into care but needing further specialized evaluation. Secondly, we observed a high frequency of parental bilingualism and of OL difficulties—though this is consistent with data from the literature (30, 31)—as well as a disproportionately large number of boys with attentional and HV disorders (2, 66). Thirdly, in contrast with the United States, there is a lack of consensus in France regarding which specialized test batteries are to be preferred. This drove us to use multiple reference tests for each cognitive domain, selecting them on the basis of the quality of their validation (67). The specialized assessments included, in addition to the basic skills that were compared to those of the BMT-i, many other tests assessing more precisely the different cognitive functions in order to build a therapeutic project adapted to the child. A final limitation of the study concerns the low level of agreement between certain skills in the domains of CM (problem-solving), LO (syntactic comprehension), GR (copying simple figures), and AE (selective attention and working memory). Several factors might explain this, such as the diversity of reference tests; differences between tasks, as was the case for syntactic comprehension and problem-solving; or different test-taking modes, i.e., computer vs. pencil and paper (for attention tests).
In conclusion, the BMT-i is a test battery for first-line screening of LDs in children. To our knowledge, no other tool for initial assessment of all cognitive domains concerned is available (15, 47). The various situations in which children are affected by Learning Disorders open many other fields of future studies and possible applications using the battery. The BMT-i could be used for initial assessment when educational intervention methods fail to improve the child's learning difficulties (5, 11). It could also be used to detect sequelae of acquired cerebral or perinatal lesions or as a first cognitive assessment in others groups of neurodevelopmental disorders, such as intellectual disabilities or autism spectrum disorders. The BMT-i is quickly administered, sensitive, easy to interpret, and affordable for all. It is an easy, low-cost means of identifying children requiring referral to specialists for more precise diagnoses and appropriate remediation (3–5, 8, 11, 13).
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by CPP 2018-A-O1870-55 Comité de protection des personnes Sud MEDITERRANEE CHU de Cimiez, CS 91179-06003 NICE CEDEX1. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
CB, CJ, and T-NW designed the study. MT, SG, and AMi selected the reference tests. CB, SG, and MT led the study and collected data. CB and CJ performed analyses. AMi and MT discussed the results. CB wrote the manuscript. CJ, AMu, and T-NW revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The conception and initiation of the project was supported through grants from ARS: Agence Régionale de Santé (Regional Health Agency) from the following regions: Auvergne-Rhône-Alpes (2018-DA-126), Bourgogne-Franche Comté (ARSBFC/2018//841), Bretagne (2019/DIS/01A), Centre Loire, Occitanie (1.2.22/C258), Provence-Alpes Côte d'Azur. An additional grant was provided by the Fondation d'entreprise Hermès, through the involvement of the local network Recital 63 devoted to NDD in Puy-de-Dôme, France.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor declared a shared affiliation with one of the authors AMu.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The study would not have been possible without the availability and the accuracy of the professionals of the BMT-i teams: i.e., the pediatricians who participated in the inclusions: Frédérique Barbe, Valérie Bernard, Anne Chevé, Dora CoIto, Patricia Dworzak-Ropert, Anne Honegger, Fabienne Kochert, Séverine Le Ménestrel, Fany Lemouel, Anne Piollet, Florence Pupier, Mario Spéranza, Andréas Werner, and Thiébaut-Noël Willig; all the numerous specialized professionals who performed the reference assessments, speech therapists, neuropsychologists, psychomotricians, occupational therapists. The project was elaborated and the results were analyzed thanks to a collaboration of the authors of the article with Jean-Christophe Thalabard for methodological advice, and Mario Speranza, Frédérique Barbe, Patricia Dworzak-Ropert and their team, with Doriane Renault, Stéphanie Iannuzzi, Cecilia Galbiati, Frédérique Edmond. Special thanks to Karen Decque and Joëlle Gardette for their participation in the Oral Language domain, to Zoé Depoid, Mélanie Guettier, Sabrina Ahade, Caroline Delloye, Solenne Ilhe, and Alexandre Deloge for their participation in the Graphism, handwriting and visuoconstruction domain, to Maxime Brussieux for his support. We gratefully acknowledge the involvement of the Association Française de Pédiatrie Ambulatoire (AFPA): Dr. S. Hubinois, Dr. F. Kochert for the implementation of the research and the following supports: Dr. M. Navel (AFPA) for the financial follow up of the project, Mrs. E. Grassin (AFPA) for technical assistance on the project.
Abbreviations
AE, attention and executive functioning; BMT-i, Batterie Modulable de Tests informatisée (computerized Adaptable Test Battery); DCDQ-FE, European-French Developmental Coordination Disorder Questionnaire; HV, handwriting, drawing, and visuospatial construction; κ, Cohen's kappa; LD, learning disability; LR, likelihood ratio; MC, mathematical cognition; MCC, Matthews correlation coefficient; OL, oral language; WL, written language.
References
1. Cortiella C, Horowitz SH. The State of Learning Disabilities: Facts, Trends, and Emerging Issues. 3rd ed. New York, NY: National Center for Learning Disabilities (2014). 48 p. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK332880/ (accessed May 30, 2021).
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. (DSM-5) Arlington, VA: American Psychiatric Publishing (2013). 183 p.
3. Grigorenko EL, Compton DL, Fuchs LS, Wagner RK, Willcutt EG, Fletcher JM. Understanding, educating, and supporting children with specific learning disabilities: 50 years of science and practice. Am Psychol. (2020) 75:37–51. doi: 10.1037/amp0000452
4. Fletcher JM, Grigorenko EL. Neuropsychology of learning disabilities: the past and the future. J Int Neuropsychol Soc. (2017) 23:930–40. doi: 10.1017/S1355617717001084
5. Hale JB, Alfonso V, Berninger V, Bracken B, Christo C, Clark E, et al. Critical issues in response-to-intervention, comprehensive evaluation, and specific learning disabilities identification and intervention: an expert white paper consensus. Learning Disability Q. (2010) 33:223–36. doi: 10.1177/073194871003300310
6. Torgesen JK. The prevention of reading difficulties. J School Psychol. (2002) 40:7–26. doi: 10.1016/S0022-4405(01)00092-9
7. Fuchs LS, Vaughn S. Responsiveness-to-intervention: a decade later. J Learn Disabil. (2012) 45:195–203. doi: 10.1177/0022219412442150
8. Reynolds AJ, Sou-Ruu Ou, Temple JA. A multicomponent, preschoool to third grade preventing intervention and educational attainment at 35 years of age. JAMA Pediatrics. (2018) 172:246–56. doi: 10.1001/jamapediatrics.2017.4673
9. Learning Disabilities Association of America. Types of learning Disabilities. (2017). Available online at: https://ldaamerica.org/types-of-learning-disabilities/ (accessed May 30, 2021).
10. World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: WHO (1992). 248 p. Available online at: https://apps.who.int/iris/handle/10665/37958 (accessed May 30, 2021).
11. Haute Autorité de Santé (HAS). Comment Améliorer le Parcours de Santé d'un Enfant Avec Troubles Spécifiques du Langage et des Apprentissages? Guide Parcours de soins. (2018). 60 p. Saint Denis, France. Available online at: https://www.has-sante.fr/upload/docs/application/pdf/2018-01/synthese_troubles_dys_v4.pdf (accessed May 30, 2021).
12. Grünke M, Cavendish WM. Learning disabilities around the globe: making sense of the heterogeneity of the different viewpoints. Learn Disabil Contemp J. (2016) 14:1–8.
13. Hayes AM, Dombrowski E, Shefcyk A, Bulat J. Learning Disabilities Screening and Evaluation Guide for Low- and Middle-Income Countries. Research Triangle Park. RTI Press Publication (2018).
14. Billard C, Mirassou A, Touzin M. La Batterie Modulable de Tests informatisée (BMT-i). Isbergues: OrthoÉdition (2019).
15. Billard C, Thiebaut E, Gassama S, Thalabard JC, Touzin M, Mirassou A, et al. The computerized adaptable test battery (BMT-i) for rapid assessment of children's academic skills and cognitive functions: a validation study. Front Pediatr. (2021) 9:656180. doi: 10.3389/fped.2021.656180
16. Ray-Kaeser S, Thommen EI, Martini R, Jover M, Gurtner B, Bertrand AM. Psychometric assessment of the French European Developmental Coordination Disorder Questionnaire (DCDQ-FE). PLoS ONE. (2019) 14:e0217280. doi: 10.1371/journal.pone.0217280
17. Hall CL, Valentine AZ, Groom MJ, Walker GM, Sayal K, Daley D et Hollis CP. The clinical utility of the continuous performance test and objective measures of activity for diagnosing and monitoring ADHD in children: a systematic review. Eur Child Adolesc Psychiatry. (2016) 25:677–99. doi: 10.1007/s00787-015-0798-x
18. Snowling MJ, Hulme C, Nation K. Defining and understanding dyslexia: past, present and future. Oxford Rev Educ. (2020) 46:501–13. doi: 10.1080/03054985.2020.1765756
19. Nippold MA. Reading comprehension deficits in adolescents: addressing underlying language abilities. Lang Speech Hearing Serv Schools. (2017) 48:125–31. doi: 10.1044/2016_LSHSS-16-0048
20. Launay L, Maeder C, Roustit J, Touzin M. Évaluation du Langage écrit et du Langage Oral 6 - 15 ans (EVALEO 6-15). Isbergues: OrthoÉdition (2018).
23. Pech-George C, George F. Batterie d'Évaluation de Lecture et d'Orthographe (BELO). Paris: De Boeck Supérieur (2012).
24. Dehaene S., Cohen L. Towards an anatomical and functional model of number processing. Math Cogn. (1995) 1:83–120.
25. Brendefur JL, Johnson ES, Keith WT, Strother S, Severson HH. Developing a multi-dimensional early elementary mathematics screener and diagnostic tool: the primary mathematics assessment. Early Childhood Educ J. (2018) 46:153–7. doi: 10.1007/s10643-017-0854-x
26. Karagiannakis G, Noël MP. Mathematical profile test: a preliminary evaluation of an online assessment for mathematics skills of children in grades 1–6. Behav Sci. (2020) 10:126. doi: 10.3390/bs10080126
27. Nieuwenhoven C, Grégoire J, Noël MP. Tedi-Math. Test diagnostique des compétences de base en mathématiques. Montreuil: ECPA par Pearson (2001).
30. Reilly S, Cook F, Edith L, Bavin EI, Bretherton L, Cahir P, et al. Cohort profile: the early language in victoria study (ELVS). Int J Epidemiol. (2018) 47:11–20. doi: 10.1093/ije/dyx079
31. Bishop DVM, Snowling MJ, Thompson PA, Greenhalg T. Identifying language impairments in children. PLoS ONE. (2016) 11:158753. doi: 10.1371/journal.pone.0158753
34. Del Giudice E, Grossi D, Crisanti AF, Latte F, Fragassi NA, Trojano L. Spatial cognition in children. I. Development of drawing-related (visuospatial and constructional) abilities in preschool and early school years. Brain Dev. (2000) 22:362–7. doi: 10.1016/S0387-7604(00)00158-3
35. Trojano L, Conson M. Visuospatial and visuoconstructive deficits. In: Goldenberg G, Miller B, editors. Handbook of Clinical Neurology. Amsterdam: Elsevier Press (2008). p. 373–91.
36. Beery KE, Buktenica NA, Beery NA. Visual-Motor Integration (VMI). Parsipannany: Modern Curriculum Press (2010).
37. Korkman M, Kirk U, Kemp S. NEPSY II. Bilan neuropsychologique de l'enfant. Montreuil: ECPA par Pearson (2012).
39. Charles M, Soppelsa R, Albaret JM. Échelle d'évaluation rapide de l'écriture chez l'enfant (BHK). Montreuil: ECPA par Pearson (2004).
40. Wechsler D. WISC V. Échelle d'intelligence de Wechsler pour enfants et adolescents. Montreuil: ECPA par Pearson (2016).
41. Diamond A., Ling DS. Executive functions. Ann Rev Psychol. (2013) 64:135–68. doi: 10.1146/annurev-psych-113011-143750
43. Zimmermann P, Fimm B, Leclercq M. Test d'Évaluation de l'Attention TAP/KITAP. Herzogenrath, Allemagne: Psytest (2010).
44. Manly T, Robertson IH, Anderson V, Mimmo-Smith I. Test d'Évaluation de l'Attention chez l'enfant (Tea-ch). Montreuil: ECPA par Pearson (2006).
46. Gioia GA, Isquith PK, Guy SC, Kenworthy L, Roy A, Fournet N, et al. Adaptation et validation en français de l'Inventaire d'Évaluation Comportementale des Fonctions Exécutives (BRIEF: Behavior Rating Inventory of Executive Function). Paris: Hogrefe (2013).
47. Guilmette TJ, Sweet JJ, Hebben N, Koltai D, Mark Mahone E, Spiegler BJ, et al. American Academy of Clinical Neuropsychology consensus conference statement on uniform labeling of performance test scores. Clin Neuropsychol. (2020) 34:437–53. doi: 10.1080/13854046.2020.1722244
48. Jurman G, Riccadonna S, Furlanello C. A comparison of MCC and CEN error measures in multi-class prediction. PLoS ONE. (2012) 7:e41882. doi: 10.1371/journal.pone.0041882
49. Landis JR, Koch GG. An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics. (1977) 33:363–74. doi: 10.2307/2529786
50. Core Principles: Best Practices in the Use of Cognitive Assessment in Learning Disability Identification. 21/01/2020 LDA Learning Disability Association of America. Available online at: https://ldaamerica.org/info/best-practices-cognitive-assessment-ld/ (accessed May 30, 2021).
51. Hudson A, Wee Koh P, Moore KA, Binks-Cantrell E. Fluency interventions for elementary students with reading difficulties: a synthesis of research from 2000–2019. Educ Sci. (2020) 10:52. doi: 10.3390/educsci10030052
52. Geary DC, vanMarle K, Chu FW, Rouder J, Hoard MK, Nugent L. Early conceptual understanding of cardinality predicts superior school-entry number-system knowledge. Psychol Sci. (2018) 29:191–205. doi: 10.1177/0956797617729817
53. Fishbein B, Foy P, Yin L. TIMMS 2019 User Guide for the International Database. International Results in Mathematics and Science Study. International Association for the Evaluation of Educational Achievement (IEA). Trends in Trends in Mathematics and Science Study. Available online at: https://www.iea.nl/sites/default/files/2021-01/TIMSS-2019-User-Guide-for-the-International-Database.pdf" (accessed May 30, 2021).
54. Hendricks AE, Adlof SM, Alonzo CN, Fox AB, Hogan TP. Identifying children at risk for developmental language disorder using a brief, whole-classroom screen. J Speech Lang Hear Res. (2019) 62:896–908. doi: 10.1044/2018_JSLHR-L-18-0093
55. Vaivre-Douret L, Lalanne C Golse B. Developmental coordination disorder, an umbrella term for motor impairments in children: nature and co-morbid disorders. Front Psychol. (2016) 7:502. doi: 10.3389/fpsyg.2016.00502
56. Margolis AE, Broitman J, Davis JM, Alexander L, Hamilton A, Liao Z, et al. Estimated prevalence of nonverbal learning disability among north american children and adolescents. JAMA Network Open. (2020) 3:e202551. doi: 10.1001/jamanetworkopen.2020.2551
57. Glosse C, Van Reybroeck M. Do children with dyslexia present a handwriting deficit? Impact of word orthographic and graphic complexity on handwriting and spelling performance. Res Dev Disabil. (2020) 97:103553. doi: 10.1016/j.ridd.2019.103553
58. Pritchard AE, Nigro CA, Jacobson LA, Mark Mahone E. The role of neuropsychological assessment in the functional outcomes of children with ADHD. Neuropsychol Rev. (2012) 22:54–68. doi: 10.1007/s11065-011-9185-7
59. Kaufman AS, N.L Kaufman NL. KABC-II - Batterie pour l'examen psychologique de l'enfant. 2n ed. Montreuil: ECPA par Pearson (2008).
60. Wechsler D. Test de rendement individuel de Wechsler - deuxième édition - version pour francophones WIAT II CDN-F. Toronto: Pearson Canada Assessment (2008).
61. Wilkinson GS, Robertson GJ. Wide Range Achievement Test. 5th ed. (WRAT5). Melbourne: Pearson (2017).
62. Villarreal V. Test review. Woodcock- Johnson IV Tests of Achievement (WJ IV) Mather N et Woodcock RW; Early Cognitive Academic Development (ECAD) Schrank F, Mather N, McGrew K. Rolling Meadow, IL: Riverside. J Psychoed Assess. (2015) 33:391–8. doi: 10.1177/0734282915569447
63. Frame LB, Vidrine SM, Hinojosa R. Test Review: Kaufman AS, & Kaufman NL. Kaufman Test of Educational Achievement, Third Edition (KTEA-3) et Kaufman AS, N.L Kaufman NL Kaufman Test of Educational Achievement, 3rd ed. Pearson, 2014. J Psychoed Assess. (2016) 34:811–8. doi: 10.1177/0734282916632392
64. Lafay A, Cattini J. Analyse psychométrique des outils d'évaluation mathématique utilisés auprès des enfants francophones. Can J Speech Lang Pathol Audiol. (2018) 42:127–44.
65. Zanga A. EPOCY 2-3 - Épreuve de positionnement en cycles 2 et 3. Évaluation qualitative et quantitative des compétences en mathématiques, en orthographe et en lecture. Montreuil: ECPA par Pearson (2011).
66. Blank R, Barnett A, Cairney J, Green D, Kirby A, Polatajko H, et al. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev Med Child Neurol. (2019) 61:242–85. doi: 10.1111/dmcn.14132
Keywords: BMT-i, test battery, screening, learning disabilities, academic skills, cognitive functions, validity, child
Citation: Billard C, Jung C, Munnich A, Gassama S, Touzin M, Mirassou A and Willig T-N (2021) External Validation of BMT-i Computerized Test Battery for Diagnosis of Learning Disabilities. Front. Pediatr. 9:733713. doi: 10.3389/fped.2021.733713
Received: 30 June 2021; Accepted: 31 August 2021;
Published: 01 October 2021.
Edited by:
Sabine Plancoulaine, INSERM U1153 Centre de Recherche Épidémiologie et Statistique, FranceReviewed by:
Sunil Karande, King Edward Memorial Hospital and Seth Gordhandas Sunderdas Medical College, IndiaMarie-Odile Livet, Centre Hospitalier du Pays d'Aix, France
Copyright © 2021 Billard, Jung, Munnich, Gassama, Touzin, Mirassou and Willig. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catherine Billard, Y2F0aGVyaW5lLmJpbGxhcmQzQGdtYWlsLmNvbQ==