 Ting Huang1
Ting Huang1 Guanggao Zhao1*Haoyuan Tan2Hua Wu3Jinmei Fu4Shunli Sun4Wendi Lv1Zihao He1Qiming Hu1
Guanggao Zhao1*Haoyuan Tan2Hua Wu3Jinmei Fu4Shunli Sun4Wendi Lv1Zihao He1Qiming Hu1 Minghui Quan5*
Minghui Quan5*- 1School of Physical Education, Nanchang University, Nanchang, China
- 2Clinical Medical College of Acupuncture Moxibusion and Rehabilitation, Guangzhou University of Chinese Medicine, Guangzhou, China
- 3Rehabilitation Medicine Center, The Second Affiliated Hospital of Jiaxing University, Jiaxing, China
- 4Jiangxi Sports Science and Medicine Center, Nanchang, China
- 5School of Kinesiology, Shanghai University of Sport, Shanghai, China
Introduction: To use a quantitative approach to examine the effects of family interventions on physical activity (PA) and sedentary behavior (SB) in children aged 2. 5–12 years.
Methods: PubMed, OVID, Web of Science, and others were searched from their inception to May 2020. Intervention studies that examined the effects of family interventions on PA among children aged 2.5–12 years were included in this meta-analysis. Lastly, subgroup analyses were conducted to examine the potential modifying effects of family intervention's characteristics and study quality.
Results: Eleven articles met the inclusion criteria for this review. Studies investigated a range of PA outcomes, including moderate-to-vigorous PA (MVPA), total PA (TPA), daily steps, and SB levels. Meta-analysis showed that family intervention had a significant effect on PA [standardized mean difference (SMD) = 0.10; 95% CI = 0.01–0.19], especially for daily steps [weight means difference (WMD) = 1,006; 95% CI = 209–1,803], but not for SB (WMD = −0.38; 95% CI = −7.21–6.46). Subgroup analyses indicated the improvements in PA occurred when children were 6–12 years old, intervention focused on PA only, intervention duration ≤ 10 weeks, and “low risk of bias” study performed.
Conclusions: Family intervention may be a promising way to promote children's PA levels, especially for daily steps.
Trial Registration: Meta-analysis protocol was registered on PROSPERO: CRD42020193667.
Introduction
Physical activity (PA) is a key factor in children's physical and mental health development (1–3), playing a crucial role in bone development (4, 5), motor ability development (6), and self-esteem cultivation (7, 8). Previous studies have shown that a low PA level and high sedentary behavior (SB) level lead to poor health (9), increase the risk of obesity (10) and coronary heart disease (11) from childhood to adolescence, and raise the risk of PA deficiency in adulthood (12, 13). However, advances in technology, automated household appliances, and convenient ways of traffic have led to a decline in PA and an increase in SB (14). Eighty percent of the world's children do not meet the PA recommendation from the World Health Organization (15). Therefore, identifying the effective ways to promote children's PA levels has great public health significance.
The family-centered intervention model is designed to interact, purposefully and systematically, with participants and their family members in family settings, to help prevent and respond to various physical and mental health problems (16). Potential mechanisms of intervention effectiveness include the construct of familial or parental social support, the theoretical and practical guidance of PA and SB to families, the technical and logistical support for parents and children activities, and the role modeling and supervision of parents. Family System Theory also believes that the PA and SB behaviors of family members influence each other (17), and parental involvement is crucial in supporting and managing children's related behaviors (PA, SB, diet, screen time, sleep) (18–22). Based on the Family System Theory, some scholars tried to apply family intervention in the field of PA promotion in children (23–25). Some studies found that family interventions can have a significant effect on increasing children's PA and decreasing SB levels (26–28), but in other studies the positive effect was not observed (29–32). Although previous qualitative reviews examined the effects of family intervention on PA and SB levels in children (22, 33), no quantitative review based on experimental studies has been conducted. Therefore, this study aims to identify the effects of family interventions on PA and SB levels in children aged 2–12 years by a using meta-analytic approach. The findings of this study will provide a reference for children's health care work.
Methods
Protocol and Registration
This research program has been registered on the PROSPERO System Evaluation Registration Platform, registration number: CRD42020193667. This study has been reported according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines (34).
Data Sources and Search Strategy
Studies were identified by structured database searching from inception until May 2020. Studies were gathered using the following databases: PubMed, OVID, Web of Science, Scopus, and China National Knowledge Internet (CNKI). The following search strings were employed:
(1) Participants: “child*,” “preschool,” “kindergar*,” “pediatric,” “young child*,” “schoolage*,” “nursery school*,” “primary school*,” “grade school*,” “elementary school,” “school*,” “elementary student*,” etc.
(2) Interventions: “intervention,” “health promotion,” “family,” “family-based,” “parent*,” “parent-based,” “home-based,” “mother*,” “father*,” “primary care giver*,” “preventi*,” “behavio*,” “behavior Change*,” “treatment,” “methods,” etc.
(3) Outcome: “physical activity,” “exercise*,” “sport*,” “healthy lifestyle*,” “activity*,” “inactivity*,” “step,” etc.
(4) Study design: search words include “random*,” “control*,” “trial,” “comparison,” “RCT (randomized controlled trials),” etc.
The exact terms were searched by “OR,” different terms were searched by “AND”. Then the references in the retrieved documents were browsed and conducted a manual retrieval, and supplemented the missing documents in the retrieval process.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Participants: children aged 2.5–12 years, basing on PubMed MeSH term definition of preschoolers (2–5 years) and children (6–12 years); (2) Interventions: family Interventions (e.g., intervene in the family, intervene with parents); (3) Outcomes: indicators include PA (including any intensities PA or steps) and SB levels; (4) Study design: randomized controlled trials (RCT) or clinical controlled trials (CCT); (5) published in peer-review journals; and (6) written in English or Chinese.
Exclusion criteria: (1) studies were review article; (2) studies were missing data of PA level as an outcome; (3) participants had physical diseases or dyskinesia; and (4) publications from the same project with a relatively small sample size.
Data Extraction and Management
Two authors (TH and ZH) and a trained research assistant separately categorized all articles and extracted data. Disagreements were resolved through discussion until there was 100% agreement. The following information was extracted: (1) studies characteristics (e.g., title, authors, publication year); (2) participant's characteristics [e.g., age, body mass index (BMI), sample size]; (3) measuring methods and outcomes; (4) types of interventions; (5) intervention focus; (6) intervention duration; and (7) the mean and standard deviation values of pre- to post-intervention differences between treatment and control groups. If there were multiple results of the same study (e.g., report both any intensities PA and steps), their data were considered as an independent study for data analysis. In the case of missing data, this information was requested from the authors a minimum of three times over four weeks.
Quality Assessment
Risk assessment was carried out using the Cochrane Risk of Bias tool (35). The evaluation included (1) Random sequence generation, (2) Allocation concealment, (3) Blinding of personnel, (4) Blinding of outcome assessment, (5) Incomplete outcome data, (6) Selective reporting, and (7) Other bias. The evaluation criteria are as follows: the “√” judgment is a low risk of bias, the “×” judgment is a high risk of bias, and the “?” judgment is an unclear risk of bias. Each study was based on an overall assessment of seven items, with a rating of high, moderate, and low risk. Two authors (TH and ZH) and a trained research assistant separately estimate and cross-audit all articles using unified standards. Disagreements were resolved through discussion until there was 100% agreement. Statistical charts of risk bias were generated by RevMan 5.3 software.
Statistical Analysis
In this review, a random-effect model was used for meta-analysis of the included studies, and STATA was used for analysis. The primary analysis processes included forest map analysis, heterogeneity test, and subgroup analysis. Statistical analysis of data from different units was performed using a 95% confidence interval (95% CI) standardized mean difference (SMD). The values of the effect size were quantified as large (≥0.8 SMD), medium (0.5 SMD– <0.8 SMD), small (0.2 SMD– <0.5 SMD), or non-significant (<0.2 SMD) (36). The weight means difference (WMD) of 95% CI was used for statistical analysis of data of the same unit. P < 0.05 was regarded as a significant difference. Depending on the characteristics of included studies, the subgroup analysis was conducted by outcomes, age, BMI, types of intervention, contents of intervention, intervention duration, measuring methods, and study quality to test whether there were differences in the effects among different subgroups.
I2 statistics were used to test the between-study heterogeneity. When I2 <25%, 25–<50%, 50– <75% and ≥75% (37), it was defined as very low, low, moderate, and high heterogeneity, respectively. The Egger's test examined publication bias. Sensitivity analysis was conducted to test the robustness of the results, by replacing the fixed-effects model with the random-effects model and removing one study at a time to test whether a single study significantly modified the pooled effect.
Results
Study Selection
A total of 1,596 articles were searched from each database, 1,585 articles were excluded according to the inclusion and exclusion criteria. Finally, 11 articles were included in this study (31, 38–47) (Figure 1).
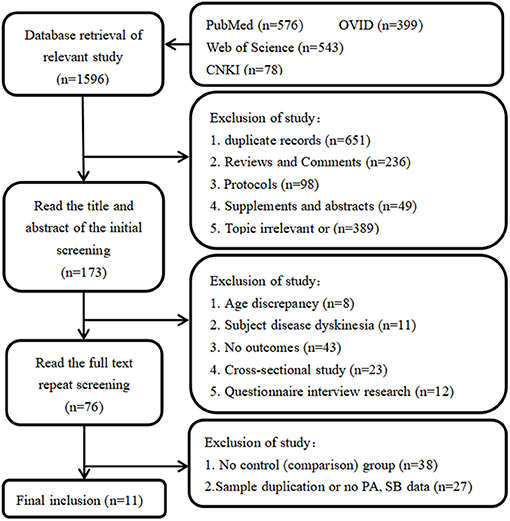
Figure 1. Article selection flow chart for the meta-analysis.
Study Characteristics
All of the included studies were published in 2012 or later, among which seven were published in 2015 or later. Of them, four studies from Australia (38, 40, 45, 46), three from the United States (31, 42, 44). The United Kingdom (47), Germany (43), Finland (41), Norway, and Sweden (39) each have one study. The included studies consisted of 10 RCTs (31, 38–41, 43–47) and 1 CCT (42), with a total of 955 participants in the treatment group and 931 participants in the control group. Five of the included studies (31, 38, 39, 42, 44) only used theory interventions, including PA knowledge education, health behavior lectures, PA counseling services, interviews, and telephone return visits. One of the included studies (41) only used behavior interventions in the specific activity tasks or activity classes that parents and children participated in together. In addition, five of the included studies (40, 43, 45–47) used both theory and behavior interventions. Most interventions included in this review targeted more than one health behavior, and intervention focus was categorized as “PA only” and “included other behavior”. Intervention focus, “PA only,” focuses only on PA improvement during the intervention, not other health behaviors. “Included other behavior” focuses not only on PA but also on improving other health behaviors (e.g., diet, sleep, screen time) (Table 1).
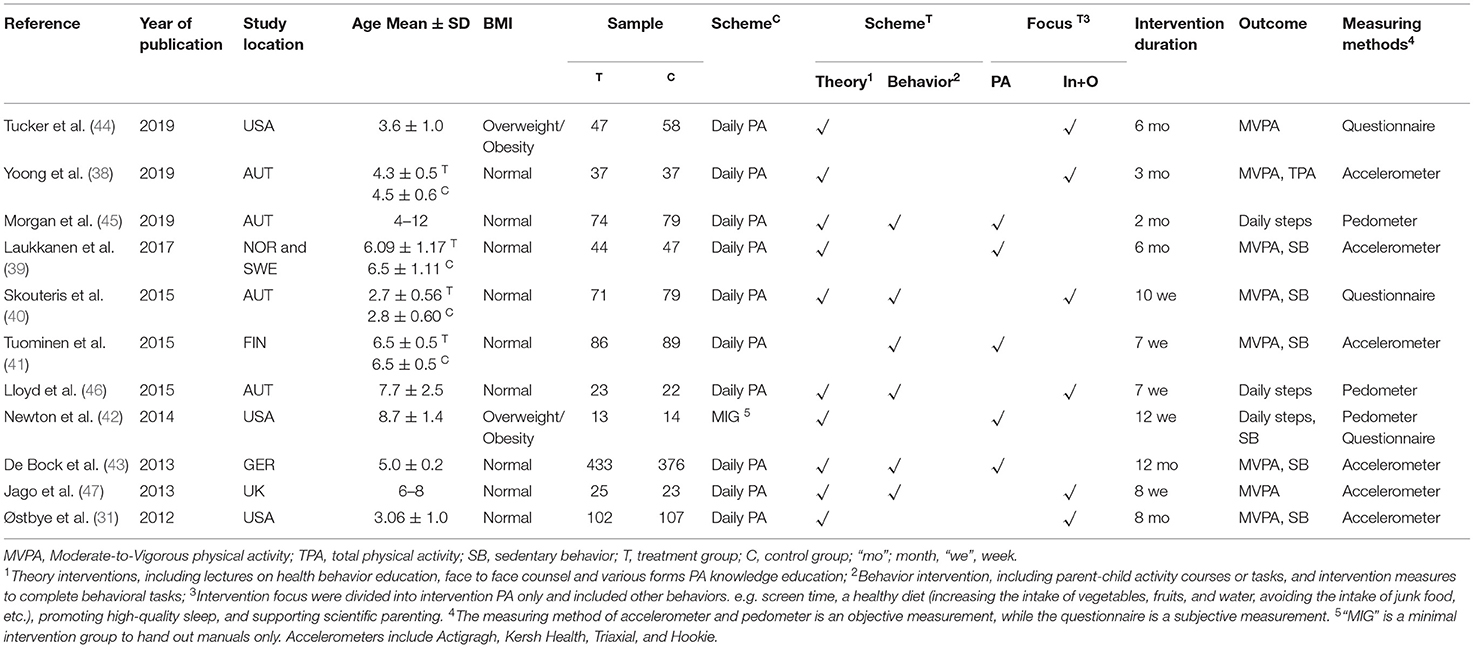
Table 1. Characteristics results of a meta-analysis on the family intervention on PA and SB in children aged 2.5–12 years.
Risk of Bias
Of the 11 articles, six articles (38, 40, 41, 43, 45, 46) were classified as low risk, two articles (31, 47) were classified as moderate risk, and three articles (39, 42, 44) were classified as high risk. All included studies were non-selective, and the integrity of the data results was described in detail. More than half of all articles described randomization, allocation concealment, and blind implementation (Figures 2, 3).
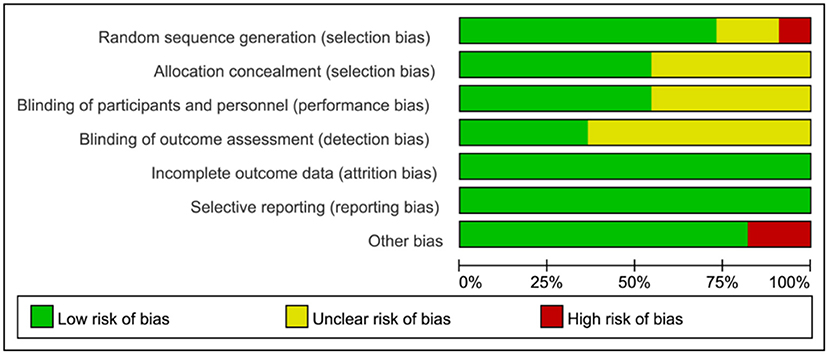
Figure 2. Risk of bias graph each risk of bias item presented as percentages.
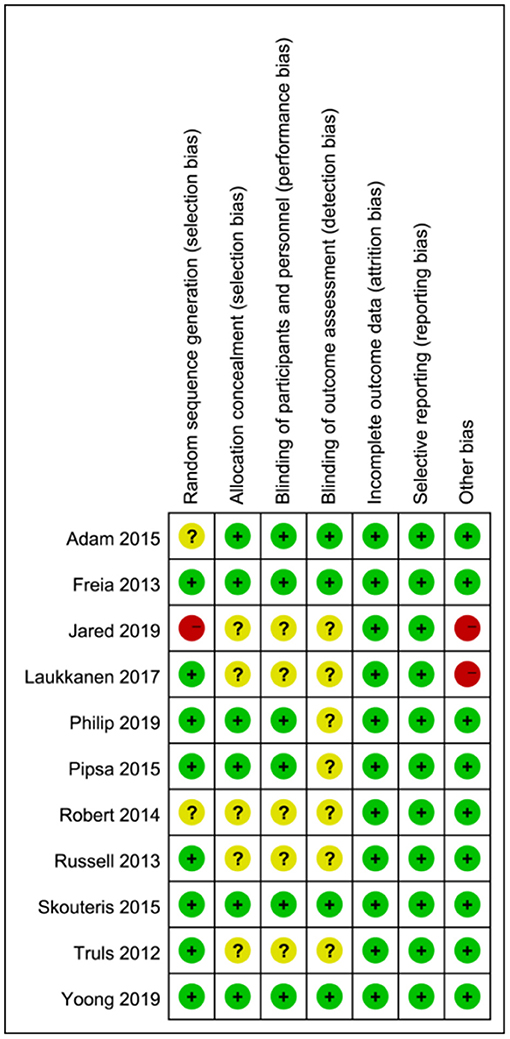
Figure 3. Risk of bias of included studies. (Green = low risk of bias; yellow = unclear risk of bias; red = high risk of bias).
Results of Meta-Analysis
The Results of PA
Meta-analysis of 11 included studies was revealed that family intervention had a significant effect on the improvement of PA in children aged 2.5–12 years (SMD = 0.10; 95% CI = 0.01–0.19). Also, no significant heterogeneity was observed across included studies (I2 = 0%, P = 0.52) (Figure 4). Publication bias was also not observed with Egger's test (P = 0.11, 95% CI = –0.24–2.08).
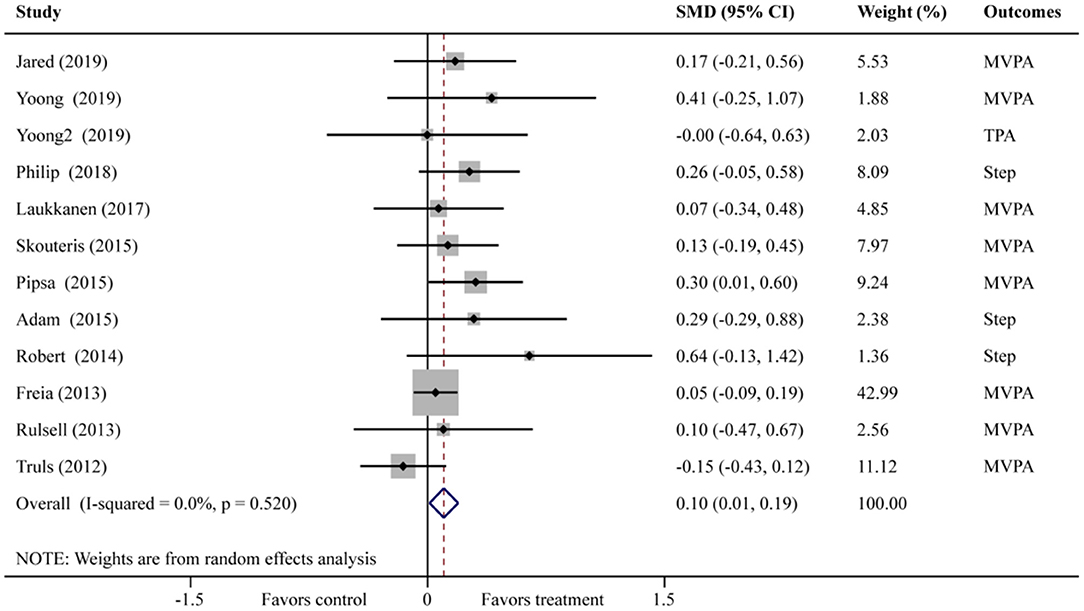
Figure 4. Forest plot of family intervention on PA in children aged 2.5–12 years. (Yoong-MVPA; Yoong2-TPA).
Subgroup analysis results showed that subgroups of “daily steps” (WMD = 1,006; 95% CI = 209–1,803), the “≥6 years” (SMD = 0.24; 95% CI = 0.04–0.45), intervention focus “PA only” (SMD = 0.16; 95% CI = 0.01–0.30), intervention duration “ ≤ 10 weeks” (SMD = 0.25; 95% CI = 0.09–0.41), and “low risk of bias” (SMD = 0.13; 95% CI = 0.02–0.23) have significant effect in PA promotion (Table 2).
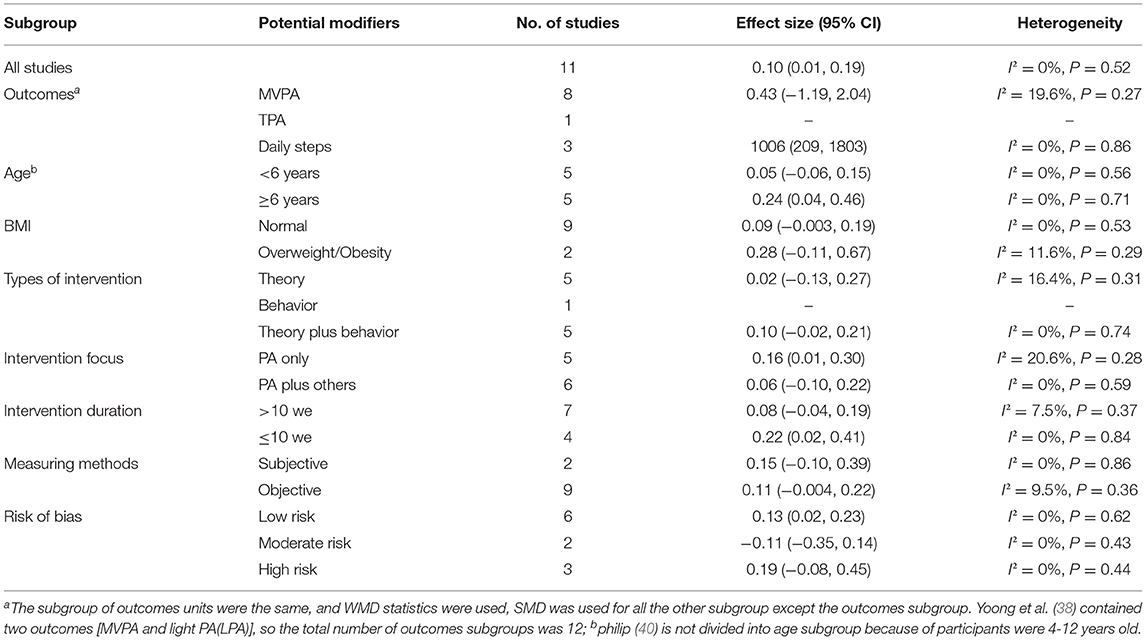
Table 2. Subgroup analysis of the effect of the family intervention on PA.
The Results of SB
Meta-analysis of 6 included studies was revealed that family intervention had no significant effect on the improvement of SB outcome in children aged 2.5–12 years (WMD =−0.38; 95% CI = −7.21–6.46) (Figure 5). There was no significant difference in all subgroups. Also noteworthy was that no significant heterogeneity was observed (I2 = 0%, P = 0.82) (Table 3). Publication bias was also not observed with Egger's test (P = 0.72, 95% CI = −1.36–1.80).
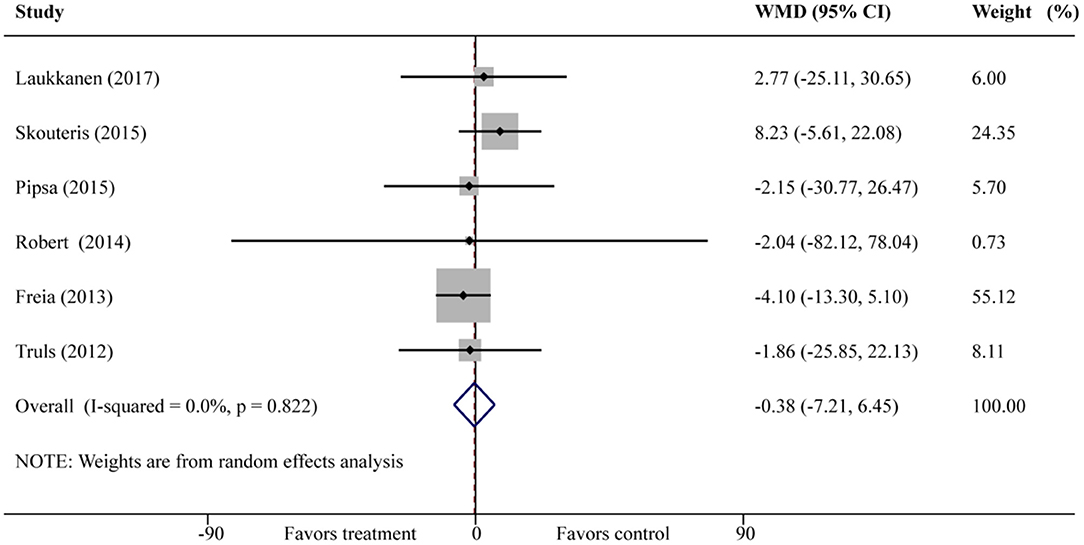
Figure 5. Forest plot of family intervention on SB in children aged 2.5–12 years.
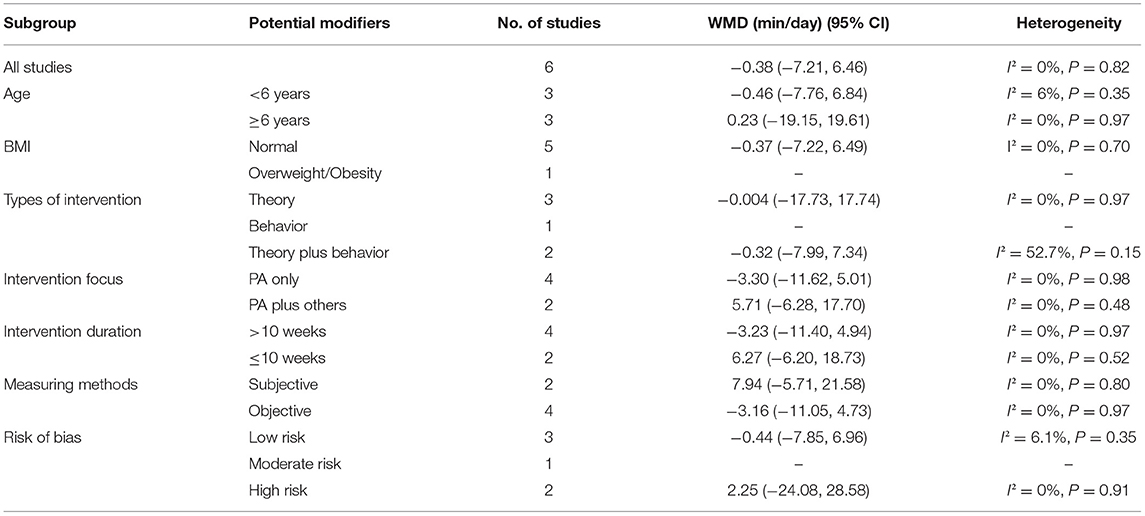
Table 3. Subgroup analysis of the effect of the family intervention on SB.
Sensitivity Analysis
Two sensitivity analyses were performed to test the robustness of our results: (1) the findings were consistent when the fixed-effects model was replaced by the random-effects model and (2) the results indicated no single study to be significantly modified by the overall trend by removing one study from the meta-analysis each time.
Discussion
Overall Effect of Family Intervention
This study aimed to quantitatively examine the effect of family interventions on the PA and SB in children aged 2.5–12 years by synthesizing the available literature in this field of inquiry. Through the combined 11 studies included, we found that family intervention could effectively improve the PA of children aged 2.5–12 years, especially for daily steps, but there was no significant effect on SB.
Comparison With Previous Findings
Findings of this study indicated that family interventions have a positive effect on PA in children aged 2.5–12 years, and this study is, therefore, a valuable extension of two published systematic reviews and meta-analysis (48, 49). A meta-analysis provides evidence that school-based interventions can be effective in increasing PA enjoyment in children (48). Jane's (49) meta-analysis, based on school and family interventions, found that family interventions (involving children and parents) had better PA improvement than school interventions (only children). On this basis, when this study concentrates on family interventions, it still found that a significant intervention effect on PA in children. This study may provide additional information and contribute to this area of inquiry from family intervention and PA.
Indeed, a growing body of evidence has shown the benefits of intervention on children's PA (47, 48), however, which index of PA is more sensitive to family intervention remains unclear. Among children, previous reviews suggested that neither active play interventions (50) nor school-based interventions (51) affect moderate-to-vigorous PA (MVPA). In accord with previous studies, findings from this study align with the earlier points indicating that family interventions have no effects on MVPA. However, family interventions significantly improved the children's daily steps by 1,006 steps per day. Among previous reviews suggested that positive relationships between daily steps and physical fitness were observed (52). Daily steps are an excellent indicator of health-related outcomes (53, 54). Some studies suggested converting MVPA to steps because daily steps were generally easier to recognize (55). Findings from this study show that have no significant improvement in MVPA but improve daily steps may be the increased activity comes from LPA, not MVPA. Although PA guideline-recommended to engage in sufficient MVPA to obtain health benefits from PA (56), previous reviews revealed that engaging in more LPA is also suitable for children's health (57, 58). Therefore, it cannot be ignored the potential health effects from family interventions to enhance LPA.
Nevertheless, the results of this review showed that family intervention had no significant effect on SB in children aged 2.5–12 years. It is a disappointing outcome for public health practitioners and researchers who consider the family a promising intervention setting (17). Previous school-based (51) or classroom-based (59) interventions have also been ineffective for SB. In general, family interventions design may focus more on PA logically not SB. Future research should consider the differences and concerns between PA and SB in study design.
Analysis of Influencing Factors
The result of subgroup analysis expressed that family interventions were more effective in increasing PA levels in certain subgroups, for example, intervention focus “PA only,” “low risk of bias”. In addition, this review showed that age might be one of the factors influencing the effectiveness of family interventions. How do these findings compare to those of other published studies? A number of studies focused on preschool children found no changes in PA and SB following PA interventions (60, 61). However, in this study, the family intervention had a significant effect on PA in children aged 6–12 years. With the growth and cognitive development, the cognitive ability of school-age children (6–12 years old) was better than preschool children (62), and they also had a better understanding of the family intervention and PA. At this time, parents could set a good example, or they live in a PA positive family, which can have a profound effect on a child's PA. Therefore, well-designed and targeted RCTs were needed for children of other ages in the future.
The study also demonstrated that intervention duration affects the effectiveness of family interventions. Intervention duration was categorized as “>10 weeks” and “ ≤ 10 weeks” based on characteristics of included studies. It was found that interventions <10 weeks may have a more significant impact on PA improvement. The short-term (≤10 weeks) intervention effects may be attributed to the curiosity of the participants in the early stages of the intervention, and they are willing to participate in the implementation. Over time, the decline in the interest and compliance of the participants led to the intervention effect not being maintained.
Strength and Limitations
This study has demonstrated several strengths. First, this is the first meta-analysis to quantitatively examine the effect of family interventions on PA in children aged 2.5–12 years, which provides additional insight in the field of family interventions and PA. Second, the meta-analysis is based on data from controlled trials studies regarded as a study design that substantially reduces selection bias and has good comparability.
There were also some limitations in this study. First, most of the included studies were distributed in developed countries, so the research results were not widely representative. However, this study has included as much as possible the latest and most comprehensive research related to this proposition. Second, the family intervention programs (focus, means, duration) varied across included studies, leading to estimation bias of the overall effect. However, sensitivity analysis showed that the reduction of any one of the included studies did not significantly affect the combined results of this study.
Conclusions
In summary, findings from this meta-analysis that family intervention can effectively improve PA of children aged 2.5–12 years, especially daily steps, but has no noticeable effect on SB. Considering that family members engage in physical activity together is safe, meaningful, and effective for not only promoting the relationship between parents and children but also the development of good habits, we should encourage family members to take up physical exercise together. Future studies should focus on considering the different characteristics of preschoolers and school-age children, exploring the optimal combination of interventions focus, means, and duration.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding authors.
Author Contributions
TH, HW, MQ, HT, and ZH designed conception and search strategy. TH, HT, MQ, and ZH designed inclusion and exclusion criteria. TH and ZH conducted the quality assessment with arbitration by TH. Summary statistics were produced by TH and data analysis was performed by MQ and TH. TH, WL, and SS wrote the first draft. All authors made substantive contributions and approved the final manuscript.
Funding
This research was funded by the National Natural Science Foundation of China, Grant Number 81703252, and supported by Shanghai Commission of Science and Technology, Grant Number 19080503000. This research was funded by the Humanities and Social Science Foundation of the Ministry of Education, Grant Number 18YJC890060. This research was funded by the Graduate Student Innovation Project of Nanchang University, Grant Number CX2019046.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2021.720830/full#supplementary-material
References
1. Lv Y, Cai L, Gui Z. Effects of physical activity and sedentary behavior on cardiometabolic risk factors and cognitive function in children: protocol for a cohort study. BMJ Open. (2019) 9:e030322. doi: 10.1136/bmjopen-2019-030322
2. Robinson LE, Stodden DF, Barnett LM. Motor competence and its effect on positive developmental trajectories of health. Sports Med. (2015) 45:1273–84. doi: 10.1007/s40279-015-0351-6
3. Zeng N, Ayyub M, Sun H. Effects of physical activity on motor skills and cognitive development in early childhood: a systematic review. Biomed Res Int. (2017) 2017:2760716. doi: 10.1155/2017/2760716
4. Nikander R, Sievänen H, Heinonen A. Targeted exercise against osteoporosis: A systematic review and meta-analysis for optimizing bone strength throughout life. BMC Med. (2010) 8:47. doi: 10.1186/1741-7015-8-47
5. Janz KF, Burns TL, Levy SM. Iowa bone development study. Tracking of activity and sedentary behaviors in childhood: the iowa bone development study. Am J Prev Med. (2005) 29:171–8. doi: 10.1016/j.amepre.2005.06.001
6. Kambas A, Michalopoulou M, Fatouros IG. The relationship between motor proficiency and pedometer-determined physical activity in young children. Pediatr Exerc Sci. (2012) 24:34–44. doi: 10.1123/pes.24.1.34
7. Duman F, Kokaçya MH, Dogru E. The role of active video-accompanied exercises in improvement of the obese state in children: a prospective study from turkey. J Clin Res Pediatr Endocrinol. (2016) 8:334–40. doi: 10.4274/jcrpe.2284
8. Reed K, Wood C, Barton J. repeated measures experiment of green exercise to improve self-esteem in UK school children. PLoS ONE. (2013) 8:e69176. doi: 10.1371/journal.pone.0069176
9. Kristensen PL, Møller NC, Korsholm L. Tracking of objectively measured physical activity from childhood to adolescence: the European youth heart study. Scand J Med Sci Sports. (2008) 18:171–8. doi: 10.1111/j.1600-0838.2006.00622.x
10. Timmons BW, Leblanc AG, Carson V. Systematic review of physical activity and health in the early years (aged 0-4 years). Appl Physiol Nutr Metab. (2012) 37:773–92. doi: 10.1139/h2012-070
11. Sääkslahti A, Numminen P, Varstala V. Physical activity as a preventive measure for coronary heart disease risk factors in early childhood. Scand J Med Sci Sports. (2004) 14:143–9. doi: 10.1111/j.1600-0838.2004.00347.x
12. Matton L, Thomis M, Wijndaele K. Tracking of physical fitness and physical activity from youth to adulthood in females. Med Sci Sports Exerc. (2006) 38:1114–20. doi: 10.1249/01.mss.0000222840.58767.40
13. Telama R, Yang X, Viikari J. Physical activity from childhood to adulthood: a 21-year tracking study. Am J Prev Med. (2005) 28:267–73. doi: 10.1016/j.amepre.2004.12.003
14. Fan X, Cao ZB. Physical activity among Chinese school-aged children: National prevalence estimates from the 2016 Physical Activity and Fitness in China-The Youth Study. J Sport Health Sci. (2017) 6:388–94. doi: 10.1016/j.jshs.2017.09.006
15. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Lancet physical activity series working group. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. (2012) 380:247–57. doi: 10.1016/S0140-6736(12)60646-1
16. Miller G. Application of theory to family-centered care: a role for social workers. Soc Work Health Care. (2012) 51:89–106. doi: 10.1080/00981389.2011.609774
17. Kitzman-Ulrich H, Wilson DK, St George SM. The integration of a family systems approach for understanding youth obesity, physical activity, and dietary programs. Clin Child Fam Psychol Rev. (2010) 13:231–53. doi: 10.1007/s10567-010-0073-0
18. Bruss MB, Morris J, Dannison L. Prevention of childhood obesity: sociocultural and familial factors. J Am Diet Assoc. (2003) 103:1042–5. doi: 10.1016/S0002-8223(03)00472-3
19. Hesketh KR, Lakshman R, van Sluijs EMF. Barriers and facilitators to young children's physical activity and sedentary behavior: a systematic review and synthesis of qualitative literature. Obes Rev. (2017) 18:987–1017. doi: 10.1111/obr.12562
20. Ek A, Sorjonen K, Eli K, Lindberg L. Associations between parental concerns about preschoolers' weight and eating and parental feeding practices: results from analyses of the child eating behavior questionnaire, the child feeding questionnaire, and the lifestyle behavior checklist. PLoS ONE. (2016) 11:e0147257. doi: 10.1371/journal.pone.0147257
21. Dong F, Howard AG, Herring AH. Parent-child associations for changes in diet, screen time, and physical activity across two decades in modernizing China: China Health and Nutrition Survey 1991-2009. Int J Behav Nutr Phys Act. (2016) 13:118. doi: 10.1186/s12966-016-0445-z
22. Vollmer RL, Mobley AR. Parenting styles, feeding styles, and their influence on child obesogenic behaviors and body weight. A review Appetite. (2013) 71:232–41. doi: 10.1016/j.appet.2013.08.015
23. Birch LL, Davison KK. Family environmental factors influencing the developing behavioral controls of food intake and childhood overweight. Pediatr Clin North Am. (2001) 48:893–907. doi: 10.1016/S0031-3955(05)70347-3
24. Jago R, Edwards MJ, Urbanski CR, Sebire SJ. General and specific approaches to media parenting: a systematic review of current measures, associations with screen-viewing, and measurement implications. Child Obes. (2013) 9:S51–72. doi: 10.1089/chi.2013.0031
25. Loprinzi PD, Trost SG. Parental influences on physical activity behavior in preschool children. Prev Med. (2010) 50:129–33. doi: 10.1016/j.ypmed.2009.11.010
26. Catenacci VA, Barrett C, Odgen L, Browning R, Schaefer CA, Hill J, et al. Changes in physical activity and sedentary behavior in a randomized trial of an internet-based versus workbook-based family intervention study. J Phys Act Health. (2014) 11:348–58. doi: 10.1123/jpah.2012-0043
27. Guagliano JM, Brown HE, Coombes E, Hughes C, Jones AP, Morton KL, et al. The development and feasibility of a randomized family-based physical activity promotion intervention: the Families Reporting Every Step to Health (FRESH) study. Pilot Feasibility Stud. (2019) 5:21. doi: 10.1186/s40814-019-0408-7
28. Ling J, Robbins LB, Wen F, Peng W. Interventions to increase physical activity in children aged 2-5 years: a systematic review. Pediatr Exerc Sci. (2015) 27:314–33. doi: 10.1123/pes.2014-0148
29. Nyberg G, Sundblom E, Norman Å, Bohman B, Hagberg J, Elinder LS. Effectiveness of a universal parental support programme to promote healthy dietary habits and physical activity and to prevent overweight and obesity in 6-year-old children: the Healthy School Start Study, a cluster-randomized controlled trial. PLoS ONE. (2015) 10:e0116876. doi: 10.1371/journal.pone.0116876
30. Peirson L, Fitzpatrick-Lewis D, Morrison K, Warren R, Usman Ali M, Raina P. Treatment of overweight and obesity in children and youth: a systematic review and meta-analysis. CMAJ Open. (2015) 3:E35–46. doi: 10.9778/cmajo.20140047
31. Østbye T, Krause KM, Stroo M, Lovelady CA, Evenson KR, Peterson BL, et al. Parent-focused change to prevent obesity in preschoolers: results from the KAN-DO study. Prev Med. (2012) 55:188–95. doi: 10.1016/j.ypmed.2012.06.005
32. Harvey-Berino J, Rourke J. Obesity prevention in preschool native-american children: a pilot study using home visiting. Obes Res. (2003) 11:606–11. doi: 10.1038/oby.2003.87
33. van Sluijs EM, Kriemler S, McMinn AM. The effect of community and family interventions on young people's physical activity levels: a review of reviews and updated systematic review. Br J Sports Med. (2011) 45:914–22. doi: 10.1136/bjsports-2011-090187
34. Moher D, Liberati A, Tetzlaff J, Altman DG. Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. (2009) 151:264–W64. doi: 10.7326/0003-4819-151-4-200908180-00135
35. Higgins JP, Altman DG, Gøtzsche PC. Cochrane Bias Methods Group; Cochrane Statistical Methods Group. The Cochrane Collaboration's tool for assessing risk of bias in randomized trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
36. Cohen J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed. Hillsdale, NJ: Lawrence Erlbaum. (1988).
37. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
38. Yoong SL, Grady A, Stacey F. A pilot randomized controlled trial examining the impact of a sleep intervention targeting home routines on young children's (3-6 years) physical activity. Pediatr Obes. (2019) 14:e12481. doi: 10.1111/ijpo.12481
39. Laukkanen A, Pesola AJ, Finni T, Sääkslahti A. Parental Support and Objectively Measured Physical Activity in Children: A Yearlong Cluster-Randomized Controlled Efficacy Trial. Res Q Exerc Sport. (2017) 88:293–306. doi: 10.1080/02701367.2017.1329924
40. Skouteris H, Hill B, McCabe M, Swinburn B, Busija L. A parent-based intervention to promote healthy eating and active behaviors in pre-school children: evaluation of the MEND 2-4 randomized controlled trial. Pediatr Obes. (2016) 11:4–10. doi: 10.1111/ijpo.12011
41. Tuominen PPA, Husu P, Raitanen J, Kujala UM, Luoto RM. The effect of a movement-to-music video program on the objectively measured sedentary time and physical activity of preschool-aged children and their mothers: A randomized controlled trial. PLoS ONE. (2017) 12:e0183317. doi: 10.1371/journal.pone.0183317
42. Newton RL Jr, Marker AM, Allen HR, Machtmes R, Han H, Johnson WD, et al. Parent-targeted mobile phone intervention to increase physical activity in sedentary children: randomized pilot trial. JMIR Mhealth Uhealth. (2014) 2:e48. doi: 10.2196/mhealth.3420
43. De Bock F, Genser B, Raat H, Fischer JE, Renz-Polster H. A participatory physical activity intervention in preschools: a cluster randomized controlled trial. Am J Prev Med. (2013) 45:64–74. doi: 10.1016/j.amepre.2013.01.032
44. Tucker JM, DeFrang R, Orth J, Wakefield S, Howard K. Evaluation of a primary care weight management program in children aged 2–5 years: changes in feeding practices, health behaviors, and body mass index. Nutrients. (2019) 11:498. doi: 10.3390/nu11030498
45. Morgan PJ, Young MD, Barnes AT, Eather N, Pollock ER, Lubans DR. Engaging fathers to increase physical activity in girls: the “dads and daughters exercising and empowered” (DADEE) randomized controlled trial. Ann Behav Med. (2019) 53:39–52. doi: 10.1093/abm/kay015
46. Lloyd AB, Lubans DR, Plotnikoff RC, Morgan PJ. Paternal lifestyle-related parenting practices mediate changes in children's dietary and physical activity behaviors: findings from the healthy dads, healthy kids community randomized controlled trial. J Phys Act Health. (2015) 12:1327–35. doi: 10.1123/jpah.2014-0367
47. Jago R, Sebire SJ, Turner KM, Bentley GF, Goodred JK, Fox KR, et al. Feasibility trial evaluation of a physical activity and screen-viewing course for parents of 6 to 8 year-old children: Teamplay. Int J Behav Nutr Phys Act. (2013) 10:31. doi: 10.1186/1479-5868-10-31
48. Burns RD, Fu Y, Podlog LW. School-based physical activity interventions and physical activity enjoyment: A meta-analysis. Prev Med. (2017) 103:84–90. doi: 10.1016/j.ypmed.2017.08.011
49. Dellert JC, Johnson P. Interventions with children and parents to improve physical activity and body mass index: a meta-analysis. Am J Health Promot. (2014) 28:259–67. doi: 10.4278/ajhp.120628-LIT-313
50. Johnstone A, Hughes AR, Martin A, Reilly JJ. Utilizing active play interventions to promote physical activity and improve fundamental movement skills in children: a systematic review and meta-analysis. BMC Public Health. (2018) 18:789. doi: 10.1186/s12889-018-5687-z
51. Jones M, Defever E, Letsinger A, Steele J, Mackintosh KA A. mixed-studies systematic review and meta-analysis of school-based interventions to promote physical activity and/or reduce sedentary time in children. J Sport Health Sci. (2020) 9:3–17. doi: 10.1016/j.jshs.2019.06.009
52. Carson V, Lee EY, Hewitt L, Jennings C, Hunter S, Kuzik N, et al. Systematic review of the relationships between physical activity and health indicators in the early years (0-4 years). BMC Public Health. (2017) 17:854. doi: 10.1186/s12889-017-4860-0
53. Poitras VJ, Gray CE, Borghese MM. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. (2016) 41:S197–239. doi: 10.1139/apnm-2015-0663
54. Fang C, Zhang J, Zhou T, Li L, Lu Y, Gao Z, et al. Associations between daily step counts and physical fitness in preschool children. J Clin Med. (2020) 9:163. doi: 10.3390/jcm9010163
55. Adams MA, Johnson WD, Tudor-Locke C. Steps/day translation of the moderate-to-vigorous physical activity guideline for children and adolescents. Int J Behav Nutr Phys Act. (2013) 10:49. doi: 10.1186/1479-5868-10-49
56. Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, et al. The Physical activity guidelines for Americans. JAMA. (2018) 320:2020–8. doi: 10.1001/jama.2018.14854
57. Dwyer T, Ponsonby AL, Ukoumunne OC. Association of change in daily step count over five years with insulin sensitivity and adiposity: population based cohort study. BMJ. (2011) 342:c7249. doi: 10.1136/bmj.c7249
58. Bassett DR Jr, Toth LP, LaMunion SR, Crouter SE. Step counting: a review of measurement considerations and health-related applications. Sports Med. (2017) 47:1303–15. doi: 10.1007/s40279-016-0663-1
59. McMichan L, Gibson AM, Rowe DA. Classroom-based physical activity and sedentary behavior interventions in adolescents: a systematic review and meta-analysis. J Phys Act Health. (2018) 15:383–393. doi: 10.1123/jpah.2017-0087
60. Larson N, Ward DS, Neelon SB, Story M. What role can child-care settings play in obesity prevention? A review of the evidence and call for research efforts. J Am Diet Assoc. (2011) 111:1343–62. doi: 10.1016/j.jada.2011.06.007
61. van Sluijs EM, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ. (2007) 335:703. doi: 10.1136/bmj.39320.843947.BE
Keywords: physical activity, family intervention, meta-analytic review, parents, children
Citation: Huang T, Zhao G, Tan H, Wu H, Fu J, Sun S, Lv W, He Z, Hu Q and Quan M (2021) Effects of Family Intervention on Physical Activity and Sedentary Behavior in Children Aged 2.5–12 Years: A Meta-Analysis. Front. Pediatr. 9:720830. doi: 10.3389/fped.2021.720830
Received: 05 June 2021; Accepted: 15 July 2021;
Published: 11 August 2021.
Edited by:
Ivana M. Milovanovic, University of Novi Sad, SerbiaReviewed by:
Ambra Gentile, University of Palermo, ItalyDamjan Jakšić, University of Novi Sad, Serbia
Copyright © 2021 Huang, Zhao, Tan, Wu, Fu, Sun, Lv, He, Hu and Quan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Minghui Quan, cXVhbm1pbmdodWlAMTYzLmNvbQ==; Guanggao Zhao, emhhb2dnMjAwMkAxNjMuY29t