 Valérie Klein1
Valérie Klein1 Claire Zores-Koenig2
Claire Zores-Koenig2 Laurence Dillenseger2
Laurence Dillenseger2 Claire Langlet2
Claire Langlet2 Benoît Escande2
Benoît Escande2 Dominique Astruc2
Dominique Astruc2 Isabelle Le Ray2,3
Isabelle Le Ray2,3 Pierre Kuhn2,4* and Strasbourg NIDCAP Study group2
Pierre Kuhn2,4* and Strasbourg NIDCAP Study group2- 1Service de Pédiatrie, Centre Hospitalier de Haguenau, Haguenau, France
- 2Service de Médecine et Réanimation du Nouveau-né, Centre Hospitalier Universitaire de Strasbourg, Strasbourg, France
- 3Service d'Obstétrique-Gynécologie, Centre Hospitalier Universitaire de Strasbourg, Strasbourg, France
- 4Institut de Neurosciences Cellulaires et Intégratives, CNRS, Université de Strasbourg, Strasbourg, France
Introduction: Many studies have evaluated the Neonatal Individualized Developmental Care and Assessment Program (NIDCAP), but few studies have assessed changes in infant- and family-centered developmental care (IFCDC) practices during its implementation.
Objectives: The primary objective of this single center study was to investigate the impact of the implementation of the NIDCAP program on IFCDC practices used for management of extremely preterm infants (EPIs). The secondary objective was to determine during implementation the impact of this program on the short-term medical outcomes of all EPIs hospitalized at our center.
Methods: All EPIs (<28 weeks gestational age) who were hospitalized at Strasbourg University Hospital from 2007 to 2014 were initially included. Outborn infants were excluded. The data of EPIs were compared for three time periods: 2007 to 2008 (pre-NIDCAP), 2010 to 2011, and 2013 to 2014 (during-NIDCAP implementation) using appropriate statistical tests. The clinical and caring procedures used during the first 14 days of life were analyzed, with a focus on components of individualized developmental care (NIDCAP observations), infant pain management (number of painful procedures, clinical pain assessment), skin-to-skin contact (SSC; frequency, day of initiation, and duration), and family access and involvement in the care of their children (duration of parental presence, parental participation in care). The short-term mortality and morbidity at discharge were evaluated.
Results: We examined 228 EPIs who received care during the three time periods. Over time, painful procedures decreased, but pain evaluations, parental involvement in care, individualized observations, and SSC increased (all p < 0.01). In addition, the first SSC was performed earlier (p = 0.03) and lasted longer (p < 0.01). There were no differences in mortality and morbidity, but there were reductions in the duration of mechanical ventilation (p = 0.02) and the time from birth to first extubation (p = 0.02), and an increase of weight gain at discharge (p = 0.02).
Conclusion: NIDCAP implementation was accompanied by progressive, measurable, and significant changes in IFCDC strategies. There were, concomitantly, moderate but statistically significant improvements in multiple important outcome measures of all hospitalized EPI.
Introduction
Population-based studies in Europe reported that extremely preterm infants (EPIs) remain at high risk of neonatal morbidity and neurodevelopmental sequelae despite the development of medical interventions that improved their survival during the last decade (1–3). There is also evidence that EPIs experience long-term alterations of developmental trajectories and academic outcomes (4, 5).
Besides the well-identified medical causes of these adverse outcomes, these impairments are also partly attributable to the early sensory experiences of EPIs during critical periods of brain development (6, 7). The environment of the neonatal intensive care unit (NICU) is particularly important, because it has many atypical stimuli that are not adapted to their sensory abilities and expectations. In addition, their hospitalization is often associated with an early separation from the parents, so they often lack access to biologically meaningful and developmentally supportive stimuli (6, 8–10). Caregivers have therefore developed infant- and family-centered developmental care (IFCDC) programs that address these issues. These programs aim to adapt the hospital environment and support a family-centered and individualized approach based on the evaluation of the infant's cues and family needs. Their general goal is to improve the outcomes of this highly vulnerable population of infants (11).
This holistic philosophy of care for infants incorporates theories and concepts derived from studies in neurodevelopment and neuro-behavior, parent-infant interactions and parental involvement, and breastfeeding promotion. It is based on several developmental care interventions that can be used alone, or combined into more formalized developmental care programs. The Neonatal Individualized Developmental Care and Assessment Program (NIDCAP) adjusts interventions to the needs of each child and is a highly conceptualized intervention. Previous studies confirmed the NIDCAP provided short-term benefits (12, 13). A randomized controlled trial (RCT) that examined infants with a mean gestational age (GA) of 27 weeks reported improvement in neurodevelopment at 18 months of post-menstrual age, although the long-term effects of this program are still uncertain (14–17). Moreover, it appeared that the preterm infants who benefited most from IFCDC strategies had strong involvement of parents in single family rooms, were the most immature infants with GAs <29 weeks (18).
The NIDCAP is a complex intervention that contains several interacting components. It requires important behavioral changes in the health care team and parents for support, and it affects different organizational levels within the hospital. There are numerous outcomes and they may be variable (19). Thus, a key question in evaluating the NIDCAP, as for other complex interventions, is whether it is effective in everyday practice (19, 20). Observational studies can provide additional information on the efficacy of this intervention and are complementary to RCTs in evaluating the effectiveness of this complex intervention. Observational studies are crucial because implementation of NIDCAP is a long process that is challenging for neonatal teams (21), and it requires significant involvement of the entire team and strong institutional support (14, 22). In fact, the NIDCAP requires education and training of health care professional so they can function as competent NIDCAP-certified health care professionals. There is therefore a need for more research to evaluate different methods of NIDCAP implementation (23).
A nation-wide population-based study of NICUs in France showed that family access, the involvement of parents in child care, and early initiation of skin-to-skin contact (SSC) increased between 2004 and 2011, although there were variations among centers (24). The implementation of neurodevelopmental care practices at the level of individual centers increased due to specific neurodevelopmental care training and policies that support IFCDC. In particular, there is evidence that the NIDCAP had a positive impact on early initiation of SSC and breastfeeding for very preterm infants in neonatal centers in France (24). However, this study only evaluated two core developmental care measures, and did not report data regarding parental involvement and pain management. Moreover, there are few detailed studies of the impact of the NIDCAP on IFCDC practices for EPIs at the level of individual centers during the implementation of this program.
The Department of Neonatology at Strasbourg University Hospital started to implement the NIDCAP in 2008, making this institution well-suited for a study of the efficacy of this intervention. The primary objective of this study was to evaluate the impact of the NIDCAP on IFCDC clinical practices for EPIs, with a focus on infant pain management, SSC practices, and parental presence and involvement in the care of their newborn infants. The secondary objective was to determine whether this change in practices already affected the short-term morbidity and mortality observed in the whole population of EPIs who were hospitalized at our center.
Materials and Methods
Design and Study Population
This retrospective, single-center, comparative study examined the IFCDC strategies used for EPIs in the NICU of the Strasbourg University Hospital before (2007–2008) and during (2010–2011 and 2013–2014) implementation of the NIDCAP program. All included EPIs (GA <28 weeks) were from single or multiple pregnancies, had no malformations, and were born at Strasbourg University Hospital during the indicated study periods.
Data Collection
The implementation of the NIDCAP was evaluated for EPIs who survived longer than 14 days. Three main IFCDC indicators were examined during the first 14 days of life for each EPI: (i) Exposure to the NIDCAP program (number of NIDCAP behavioral observations by NIDCAP-certified healthcare providers, and number of infants benefiting from NIDCAP interventions, based on two or more observations during the hospital stay); (ii) Pain management (number of painful procedures and number pain score evaluations); and (iii) Family-centered care practices and SSC (number of SSC, time and duration of the first SSC procedure, and number of hours parents were present and number of caring procedures in which they participated). All data were extracted from the medical records and the nursing flow surveillance sheets, where they were reported as part of standard care.
To evaluate the short-term morbidity and mortality in the study population, data were extracted from the prospective database of the neonatal care department. For all infants, survival without bronchopulmonary dysplasia, defined as no oxygen supplementation or no ventilatory support requirements at 36 weeks post-menstrual age, was determined. For EPIs who survived and completed all hospitalization at Strasbourg University Hospital, the following parameters were analyzed: duration of hospital stay, duration of mechanical ventilation, age at first extubation, duration of non-invasive ventilation, duration of oxygen supplementation, use of post-natal steroids for respiratory support, duration of parenteral nutrition, incidence of necrotizing enterocolitis, incidence of late-onset neonatal sepsis, neurosensory impairment [retinopathy of prematurity (ROP) requiring surgical treatment], intraventricular hemorrhage (IVH), periventricular leukomalacia (PVLM), and post-menstrual age and weight at discharge.
Statistical Analysis
Population Description
Quantitative data were presented as means and standard deviations or medians and ranges (as appropriate) for each study period. Differences were described using ANOVA. Qualitative data were presented as numbers and proportions, and differences were analyzed using the Chi-square test or Fisher's exact test, as appropriate.
Outcomes and NIDCAP Criteria
Population characteristics, outcomes, and NIDCAP implementation criteria were described separately for each study period. Comparisons of the first period (2007–2008) and the third period (2013–2014) were performed using linear or logistic regression, as appropriate, with adjustment for GA.
During the second and third periods, survival without broncho-pulmonary dysplasia for neonates who benefited from a NIDCAP observation or intervention and those who did not was compared using logistic regression that adjusted for GA at birth. Odds ratios and 95% confidence intervals (CIs) were presented.
Duration of mechanical ventilation, duration of hospitalization, and weight at discharge were compared using a linear model that adjusted for GA at birth. Linear regression coefficients and 95% CIs were presented.
Data management and analysis were conducted using R software version 3.6.3 (2020, 02, 29).
Ethical Considerations
This study was approved by the Ethical Committee of the Strasbourg University Medical Faculty and the Institutional Review Board. All parents provided written informed consent for their infants to participate in the prospective recording of medical data in the hospital's database of the unit which was registered at the National Commission on Informatics and Liberty (CNIL) of France.
Results
Study Population
A total of 2,530 children were admitted to the NICU of the Strasbourg University Hospital during the three study periods, and 292 of them were classified as EPIs, out of whom 242 were inborn. A total of 230 EPIs met the inclusion criteria (Figure 1). Two infants were initially excluded due to missing data. In addition, 10 infants were excluded due to congenital heart defects, 2 were excluded due to intestinal malformations, and 1 was excluded due to spinal muscular atrophy.
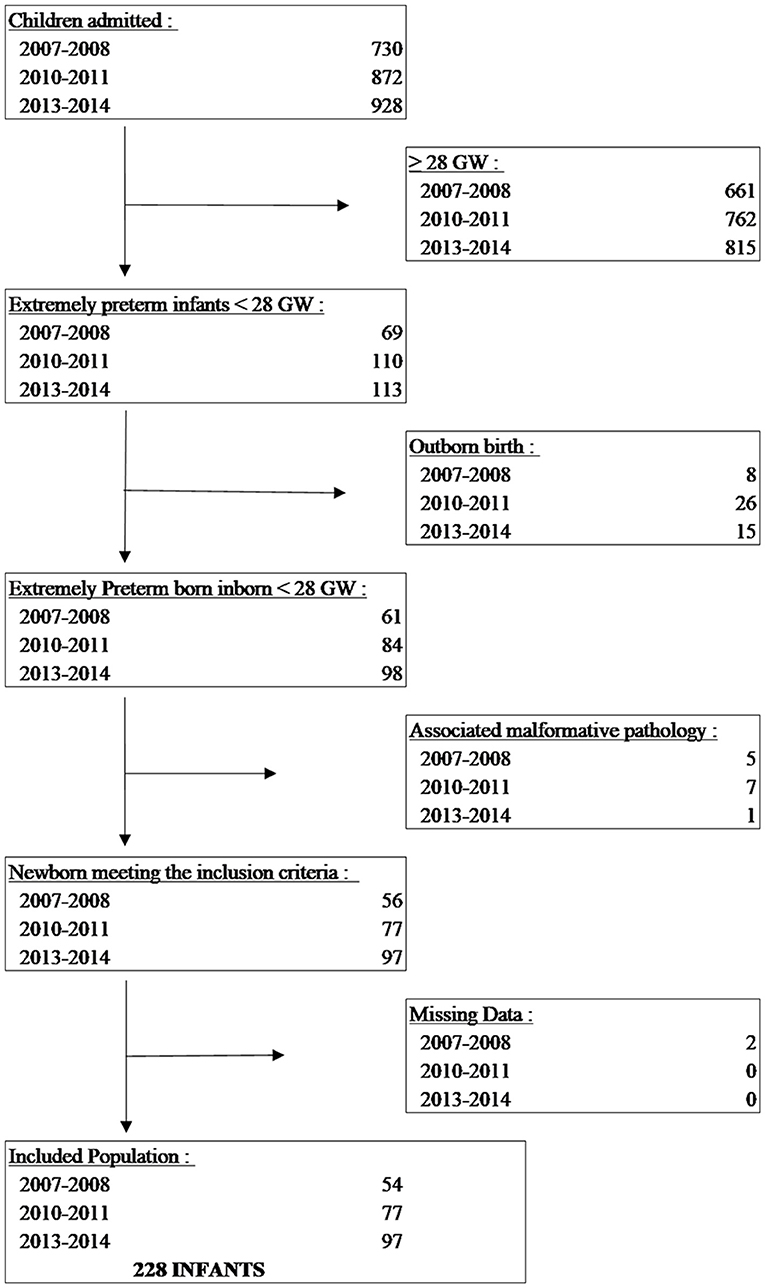
Figure 1. Identification and enrolment of extremely preterm infants.
The population was significantly more premature during the third period (2013–2014) than the first period (2007–2008), but there were no other significant differences in the three groups (Table 1). Importantly, there were no significant differences in the etiology of preterm birth.
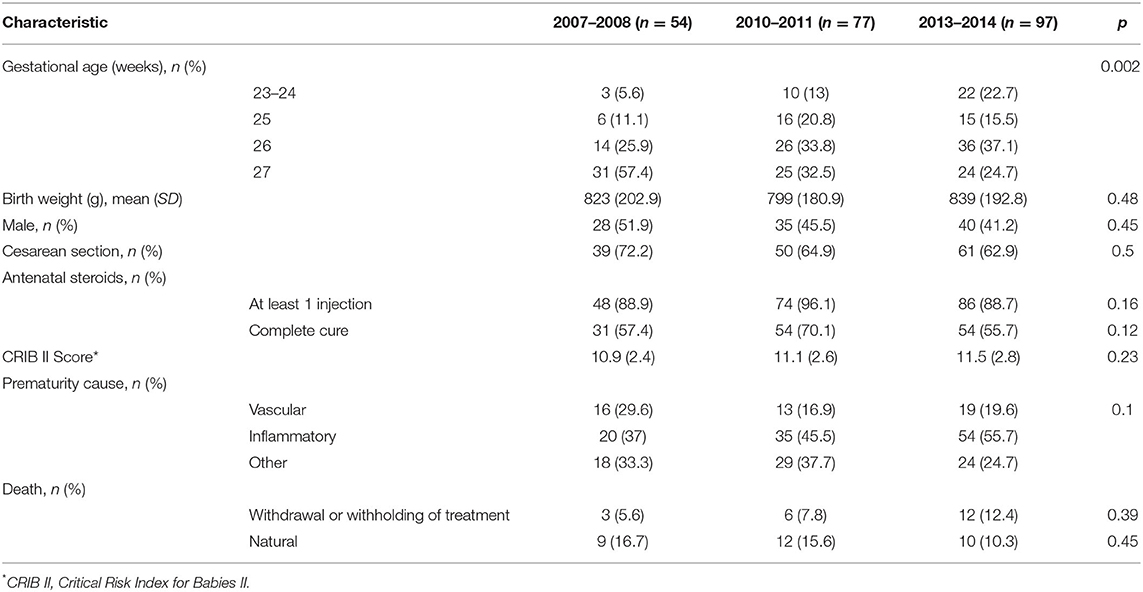
Table 1. Characteristics of extremely preterm infants during each study period.
Infant- and Family-Centered Developmental Care Strategies
We analyzed the effect of NIDCAP on the implementation of IFCDC practices by comparing the three groups (Table 2). There was a significant increase in the number of NIDCAP observations and in the number of infants who benefited from NIDCAP follow-ups (at least 2 observations). Between 2007 and 2014, there was a significant decrease in the number of painful procedures and an increase in the number of pain assessments (Figures 2, 3). Over time, the amount of SSC increased significantly (Figure 4) and the first SSC was performed significantly earlier and lasted longer. The duration of parental presence and the number of caring procedures to which the parents contributed increased significantly over time (Figure 5).
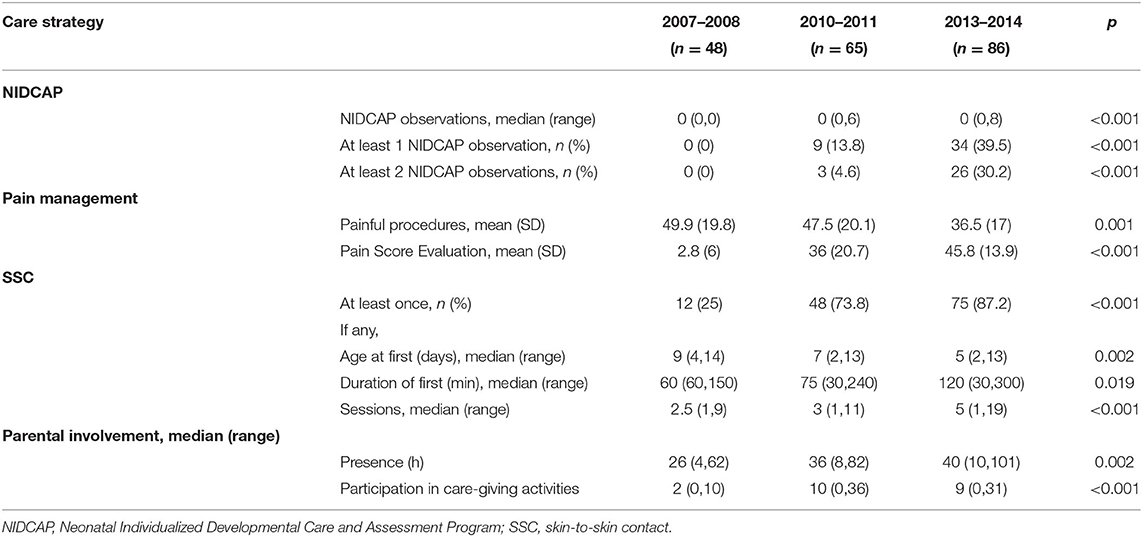
Table 2. Infant and family centered care strategies used in the two first weeks after infant birth during each study period.

Figure 2. Number of painful procedures during each study period. **p < 0.01; NS, not significant.
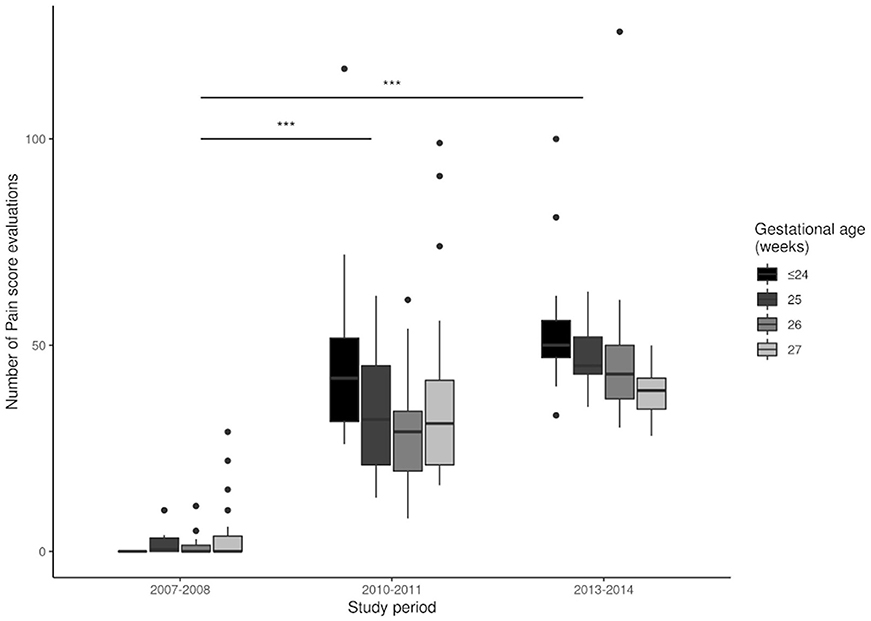
Figure 3. Number of pain score evaluations during each study period. ***p < 0.001.
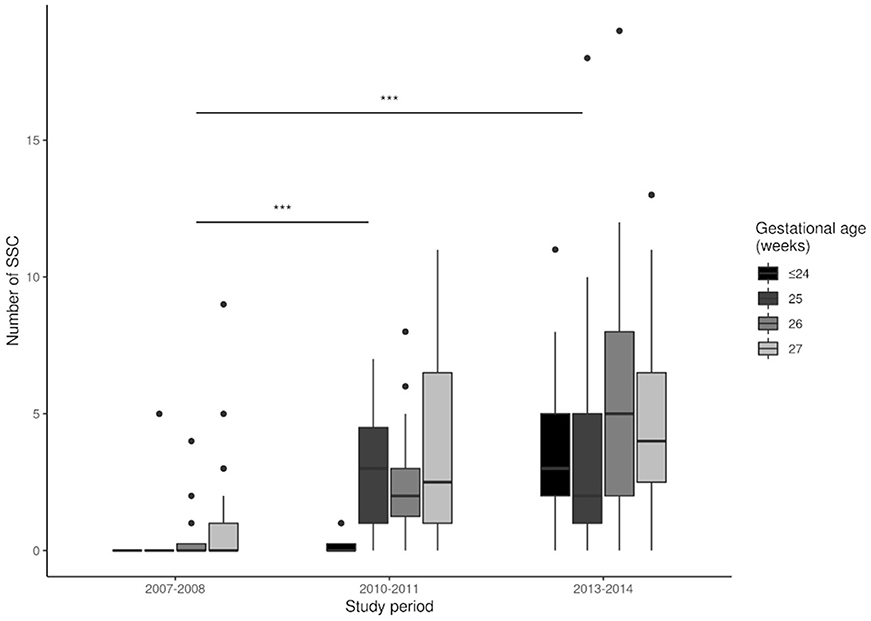
Figure 4. Number of skin-to-skin contact (SSC) events during each study period. ***p < 0.001.
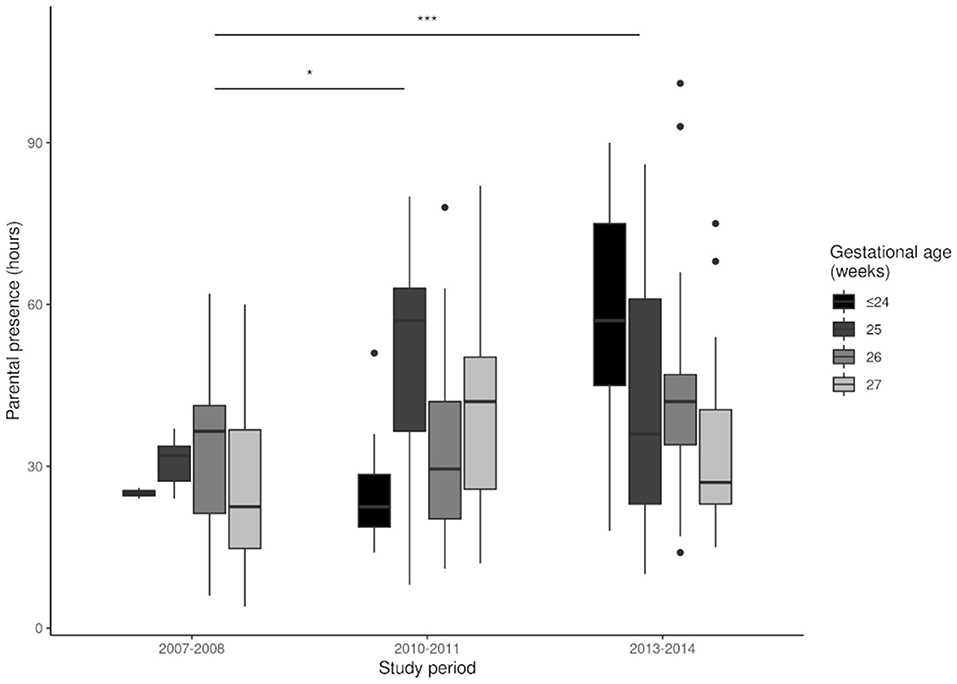
Figure 5. Parental presence during each period. *p < 0.05, ***p < 0.001.
Short-Term Medical Outcomes
There were no significant differences in survival and survival without broncho-pulmonary dysplasia during the three study periods after adjustment for GA. A comparison of the short-term outcomes of infants hospitalized until discharge home between the period 2007–2008 and the period 2013–2014 indicated there were significant reductions in the duration of mechanical ventilation (Figure 6A) and in the time from birth to first extubation (Figure 6B), and a significant increase of weight gain at discharge (Figure 7B and Table 3). There was also a significant increase in the duration of CPAP ventilation (Figure 6C). However, the three groups had no significant differences in duration of hospital stay (Figure 7A), duration of oxygen supplementation (Figure 6D), use of postnatal steroids, ROP, IVH, PVLM, late onset neonatal infection, or duration of parenteral nutrition (Table 3).
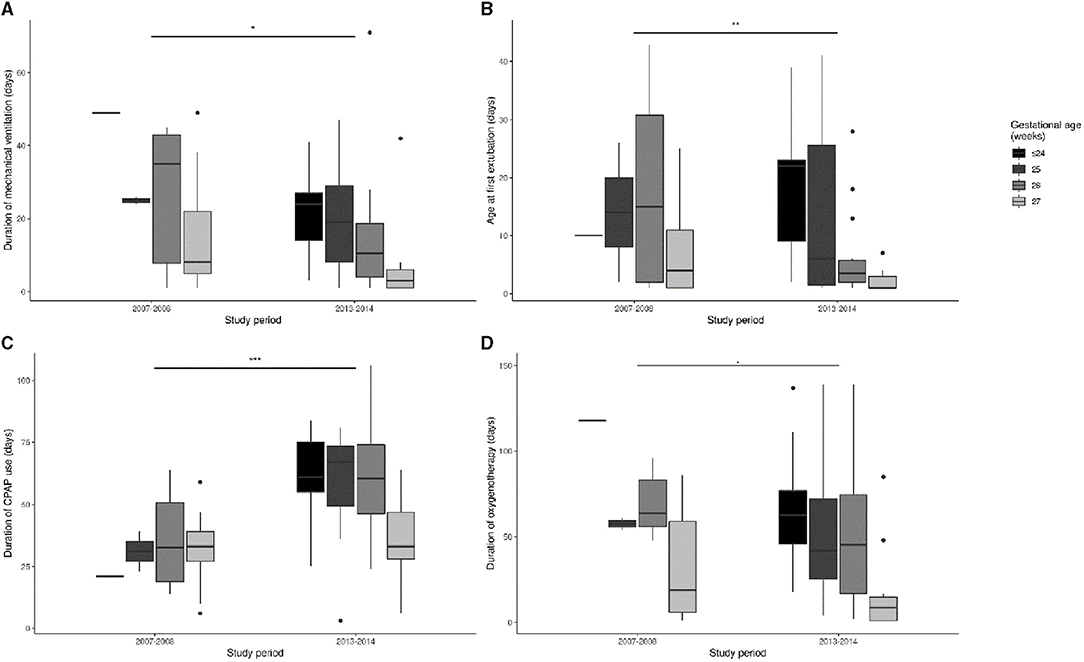
Figure 6. Time of mechanical ventilation (A), from birth to the first extubation (B), CPAP ventilation (C), and oxygen supplementation (D) during each study period. *p < 0.05, **p < 0.01, ***p < 0.001.
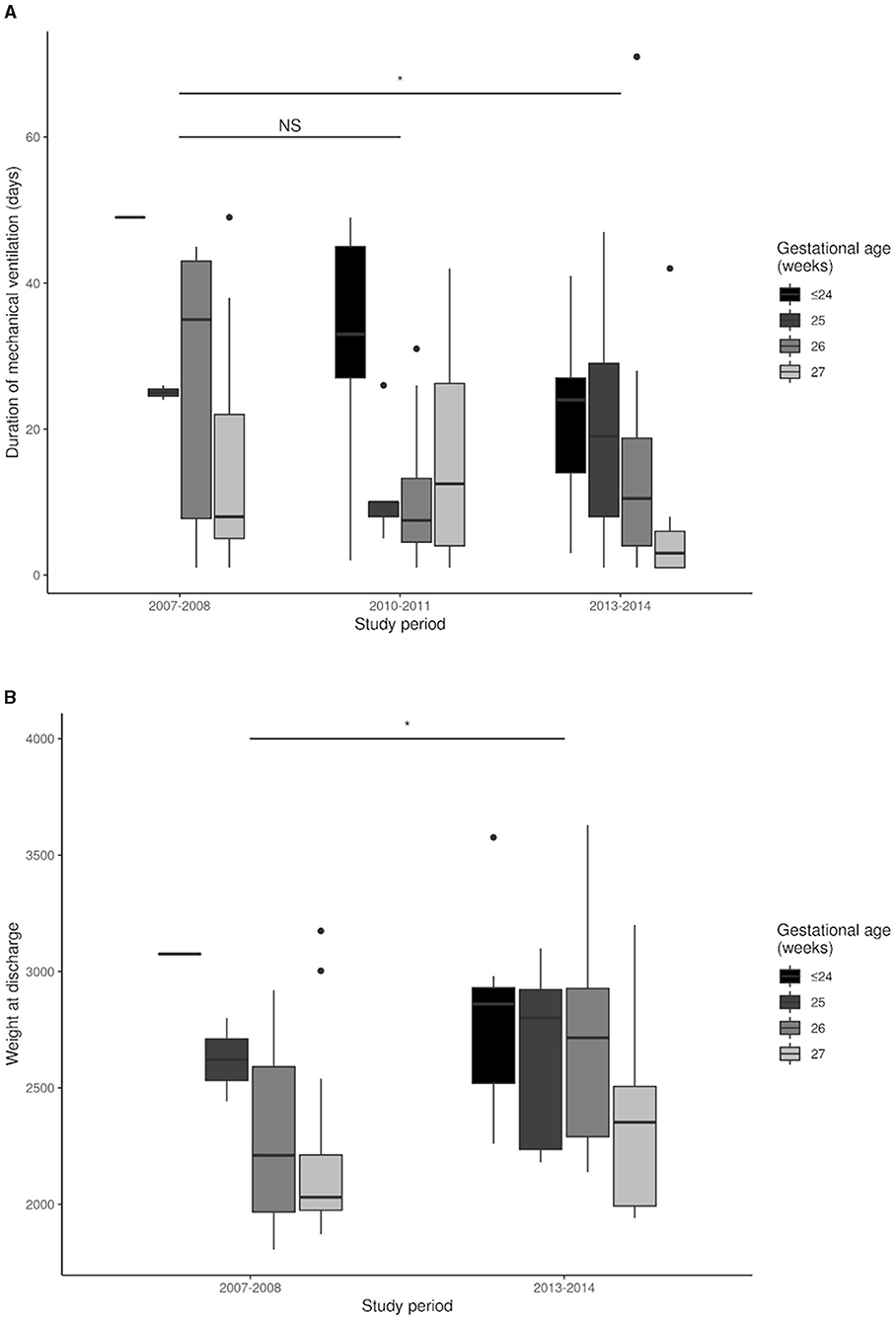
Figure 7. Duration of hospital stay (A) and weight gain at discharge (B) during each study period. *p < 0.05; NS, not significant.
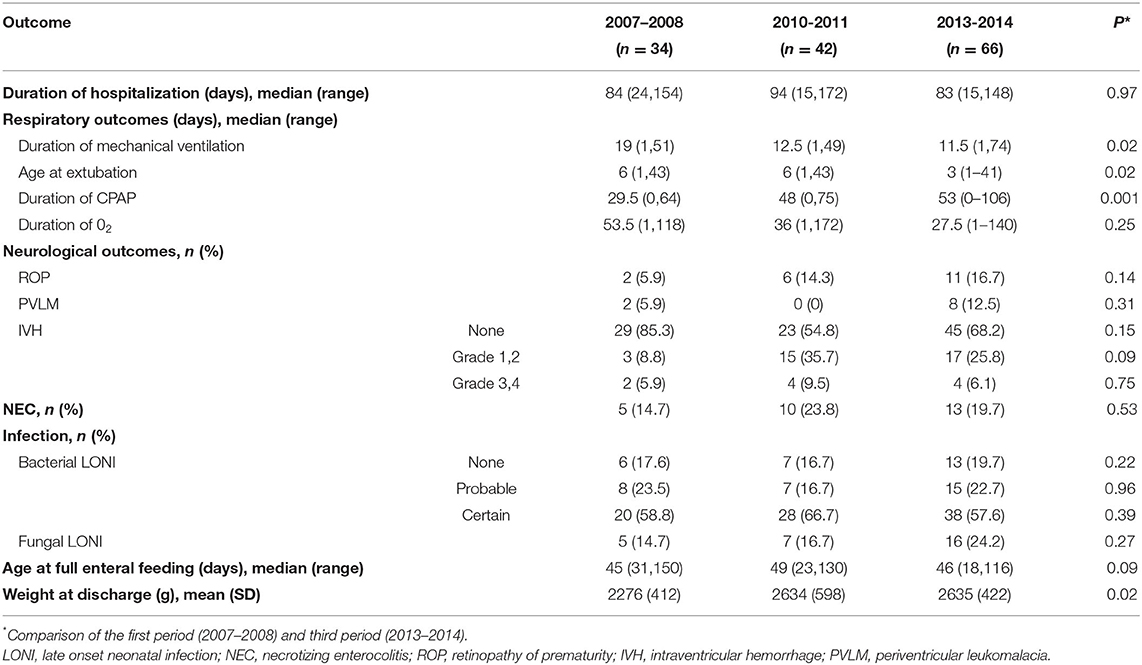
Table 3. Short-term outcomes of infants hospitalized until discharge home at the University hospital of Strasbourg, during each study period, with adjustment for gestational age.
The NIDCAP intervention (with at least 2 observations during the hospital follow-up), during the second and third periods and adjusted for GA, was not significantly associated with survival without broncho-pulmonary dysplasia, duration of mechanical ventilation, duration of hospitalization, and weight at discharge (Figures 8A–D).
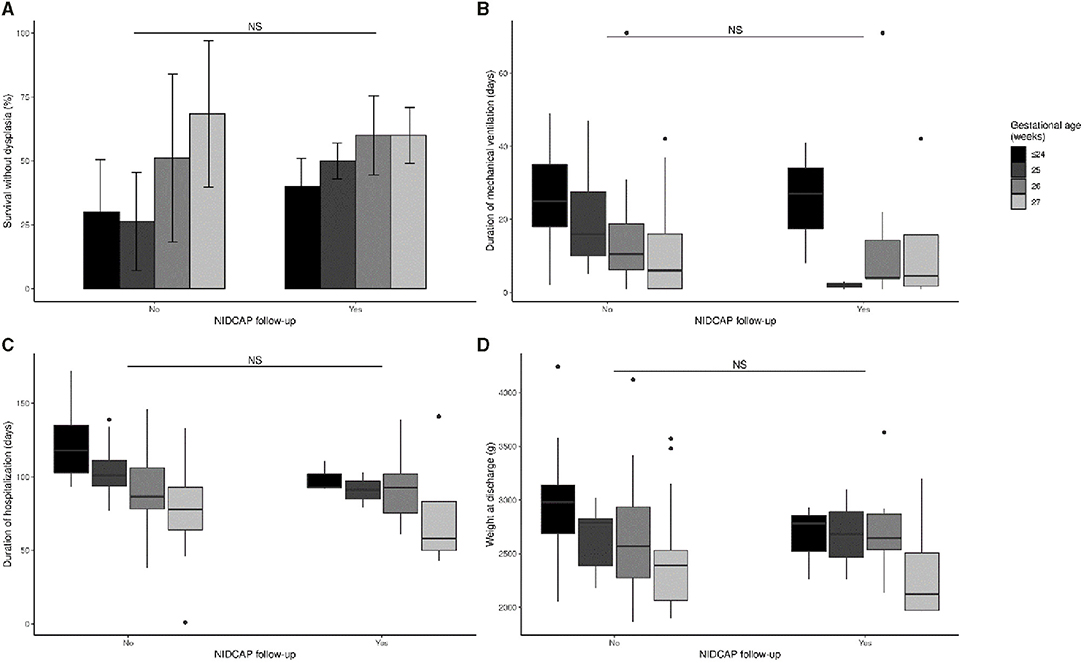
Figure 8. Impact of NIDCAP intervention on survival without dysplasia (A), duration of mechanical ventilation (B), duration of hospitalization (C), and weight gain at discharge (D). NS, not significant.
Discussion
The major result of this observational study is that the NIDCAP was effective in promoting measurable improvements in IFCDC practices at a level III regional NICU during the implementation process, in the population of EPI. This improvement in IFCDC practices was also temporally associated with moderate but measurable improvements in the short-term medical outcomes of EPIs.
This study had some limitations. It was a single center retrospective study of a relatively small number of infants. However, all the IFCDC data were fully available on the infants' charts and were reported using standard care procedures. The outcome data were also prospectively recorded for each infant supporting their validity. Previous researchers highlighted the importance of observational studies, such as the present study, for assessment of the implementation of all components of a complex intervention, because comprehensive assessments can be difficult in RCTs (19, 20). This is particularly the case for IFCDC, because there are specific barriers that preclude full evaluation (25).
NIDCAP Observations and Implementation
The implementation of the NIDCAP was associated with a significant increase in IFCDC practices. As expected, these changes were temporally associated with an increased number of NIDCAP observations, demonstrating the progressive implementation of individualized developmental care in the NICU. NIDCAP observations, which are performed by NIDCAP-certified professionals, are the cornerstone of this program (26, 27). However, we found that only a minority of EPIs benefited from NIDCAP observations, even during the third observation period.
Infant Pain Management
The NIDCAP led to a significant decrease in the number of painful procedures and an increase in the evaluation of pain scores. Due to study design, we were unable to directly evaluate pain scores in the whole study population. However, because painful procedures are the main causes of pain in the NICU (28), our data suggest there were improvements in the well-being of EPIs during the NIDCAP implementation. This is in accordance with previous reports of the beneficial impact of IFCDC on pain management. Indeed, infant pain management is an important component of IFCDC, and previous studies assessed pain to evaluate the implementation and the short- and long-term benefits of developmental care programs (29–31).
This holistic approach that uses environmental strategies based on individual evaluation of an infant's behavior and needs can reduce infant pain due to an increased number of close observations of the infant, high parental involvement as primary caregivers, and coordinated use of non-pharmacological treatments that provide pain relief. The precise and individualized evaluation of signs of withdrawal and approach of each child during NIDCAP observations may allow healthcare providers to individualize caring procedures, adjust their duration according to the tolerance of each child, and promote grasping opportunities that support autoregulation of the infant. Previous studies used NIDCAP cues to evaluate pain and integrated this into different pain scores (32–34).
Increased parental presence can improve pain management of infants, and is associated with lower pain scores. For example, the large EPIPPAIN 2 study reported that pain scores following venipuncture of newborns were lower when the parents were present (35). Other studies reported that IFCDC strategies effectively reduced pain during and after routine caring procedures (36, 37). A prospective observational study in the Netherlands reported that the implementation of NIDCAP-based stress reduction strategies which included infant pain management significantly reduced the number of painful interventions in the NICU (38). Another study reported that the NIDCAP by itself effectively decreased stress- and pain-related behaviors, physiological stress responses, and the use of sedatives and opioids in neonates (39).
Parental Presence, SSC, and Participation in Care
The NIDCAP led to significantly more presence and involvement of parents in the care of their infants, in that they had earlier, more prolonged, and an increased number of SSC procedures. Similarly, the EPIPAGE 2 study in France showed that the unit policies and the presence of a formalized developmental care program were significantly associated with an earlier initiation of SSC, which had no limitation of duration (24). Our study provided detailed data that confirmed this finding at the level of an individual center. A study in Sweden, which has active promotion of IFCDC practices, reported the average initiation of SSC for EPIs was on the sixth day of life in seven regional hospitals during 2011 (40). Longer durations of parental involvement and increased SSC were reported in countries of Northern Europe, suggesting potential progress in our unit as compared to these countries (41, 42). There is also evidence that the full integration of both parents in the care of their children in family rooms inside neonatal units, from admission until discharge, provided medical benefits to the infants, in that it significantly decreased the duration of hospital stay and the incidence of broncho-pulmonary dysplasia (18). European guidelines thus recommend provision of family rooms, including in the NICU, where the EPIs are hospitalized during their first 14 days of life (11, 43).
Short-Term Medical Outcomes
A secondary aim of this study was to determine whether implementation of the NIDCAP as an effort to increase IFCDC practices was already, despite incomplete implementation, temporally associated with benefits in the short-term medical outcomes of the children who, however, were significantly more immature overtime. Indeed, over time we observed an increased number of EPIs who were cared for in the NICU and a decrease in the gestational age of EPIs. We observed no significant changes in mortality or survival free of broncho-pulmonary dysplasia, but we found a significant decrease in the duration of mechanical ventilation, earlier first extubation, and a significant increase in body weight at discharge. We also found a significant increase in the duration of non-mechanical ventilation and a non-significant decrease in the duration of oxygen therapy. This decrease in invasive respiratory support during NIDCAP implementation is consistent with the results of a Cochrane review that evaluated developmental care (13) and of several RCTs that evaluated the NIDCAP (15, 27, 44). However, these positive results regarding respiratory support might also be due to changes in the management of respiratory distress syndrome between 2007 and 2014, as illustrated by the evolution of international recommendations (45–47). In our unit, guidelines are regularly updated to reduce the duration of mechanical ventilation, to support the increased use of non-invasive respiratory support, and to promote less-invasive surfactant administration. We also cannot totally exclude that the significant increase in body weight at discharge might be due to changes in nutritional practices, in addition to changes in IFCDC practices. However, previous research also reported that NIDCAP was associated with an increased daily weight gain (14). Moreover, increased parental involvement could also explain the increased weight gain of these infants. A Canadian multicenter, cluster randomized trial which compared standard care to Family Integrated Care (FICare; a family-centered care program with a parental involvement of at least 6 h per day) found that FICare led to a significant increase in the weight of very preterm infants at day 21. However, there were no reported benefits of FICare on infant mortality and short term morbidity (48).
Our finding that implementation of the NIDCAP did not affect the duration of hospitalization or the incidence of bronchopulmonary dysplasia was not in accordance with previous studies. In particular, these benefits were reported in a meta-analysis of well-designed and adequately powered RCTs of NIDCAP whose specific aims were to evaluate these outcomes (14). Our contrary finding may be because only about one-third of our infants benefited from at least one NIDCAP observation during the last period. Incomplete NIDCAP implementation or NIDCAP-based care that is provided by NIDCAP-educated staff members and behavioral observations that are interrupted before discharge were previously blamed for the discrepant results of two RCTs of NIDCAP (15, 16). In particular, the study by Maguire et al. showed no measurable short-term benefit from the program, but nearly 50% of children were transferred out of the NIDCAP center before hospital discharge (16). In contrast, Peters et al. identified short- and medium-term benefits for children who received the full and continuous hospital NIDCAP-based care (15, 49). In the present observational study, our comparison of periods 2 and 3 indicated no significant differences between EPIs who received NIDCAP-based care (n = 29) and whose who did not (n = 151), although there was a trend of decreased duration of mechanical ventilation and length of hospital stay in the NIDCAP group. This may be due to a lack of statistical power from our small sample size. Another possible reason for our negative findings regarding the effect of NIDCAP on the duration of hospitalization and the incidence of bronchopulmonary dysplasia may be that NIDCAP-based care requires application of the recommendations for the care of infants based on NIDCAP observations by NIDCAP-certified professionals. This implies a sufficient level of knowledge and implementation of IFCDC strategies by most caregivers who are working in the NICU.
Monitoring of IFCDC Practices and NIDCAP Implementation
The implementation of the NIDCAP takes time, as indicated by the progressive improvements in IFCDC practices observed in the present study, and it also requires changes in the hospital system. Thus, the NIDCAP is a complex intervention whose implementation may be challenging (21, 22). Monitoring of implementation of IFCDC practices, as performed in this study, is an approach that can support the efforts of caregivers. This monitoring should be continued and used as a standard for assessment of the quality of care in all neonatal units (29) because it can lead to a better neurodevelopmental outcomes of preterm infants.
At a clinical level, individualization of care should be used during the NIDCAP implementation for most infants. Training supported by the same theoretical bases at an intermediate level is available to facilitate the dissemination of NIDCAP-based care within a neonatal department and within a perinatal network where infants are transferred back from a level III referral center. Training to the Family & Infant Neuro-Development Education (FINE) (50) or the Support of Oral Feeding in Fragile Infants (SOFFI) (51) programs are more accessible for neonatal centers outside level III, and could facilitate the continuity of infant care in a perinatal network.
Although a systematic review of RCTs that examined NIDCAP found no evidence that this program improved long-term neurodevelopmental outcomes, these authors reported that NIDCAP was associated with several short-term medical benefits, including shorter hospitalization and increased Bayley Scale of Infant Development scores at 9–12 months (14). Many studies showed that improvements of infant pain management, early SSC, and parental involvement had long lasting positive effects on the neurodevelopment of preterm infants (29–31, 52–54). Because NIDCAP significantly increases the implementation of IFCDC practices, it may also provide long-term neurodevelopmental benefits, in addition to the well-documented short-term benefits.
Conclusion
Our results indicated that implementation of the NIDCAP was associated with a greater use of IFCDC practices that led to prevention of pain, increased parental involvement in the care of children, and increased SSC of parents and children. These changes occurred rapidly and were readily measurable during implementation of this program. It is essential to employ more long-term monitoring of changes in IFCDC practices to assess improvements in the quality of care delivered to these vulnerable newborn infants. Research that assesses the implementation of a complex intervention such as the NIDCAP may provide a better understanding of the efficacy of different specific practices and support their inclusion in daily practice. The effect of these changes on the developmental trajectories of EPIs needs further evaluation.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité d'Éthique de la Faculté de Medicine de Strasbourg. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Collaborative Authors
Strasbourg NIDCAP Study group: Jamal Beladdale, Caroline Briot, Céline Cayeux, Gwenaelle Fourie, Florence Gehant, Martine Hausser, Audrey Huffschmidt, Sylvie Kracher, Antoine Martenot, Jacqueline Matis, Solange Mellado, Oscar Monroy, Stéphanie Poirot, Jennifer Rondel, Christine Scheib and Isabelle Zimmer.
Author Contributions
VK participated in the design of the study, was the main contributor of data extraction and analysis, literature review, and wrote the first draft of the manuscript. CZ-K, LD, CL, BE, and DA discussed the study design, contributed to the data collection, and the writing of the manuscript. They all approved the final version of the manuscript. IL performed the statistical analysis, generated the figures, contributed to the writing of the manuscript, and reviewed the last version of the manuscript. PK was the main coordinator of the study design, data analysis, and writing of the manuscript, he thoroughly reviewed the last version of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We are very grateful to the infants and the parents who contributed to this study. We would like also to thank the whole nursing and medical teams of the department of Neonatology of the University Hospital of Strasbourg as well as Dr. Michele Billing (Director of the Quality of Care) and Mrs. Esther Wiltz (Director of the Nursing Care) for their continuous support to implement NIDCAP at our institution. Finally, we are also very indebted to Dr. Ratynski, our NIDCAP trainer, for her effective support in the implementation process and the training of health care professionals.
Abbreviations
EPI, extremely preterm infants; IFCDC, infant and family centered developmental care; NIDCAP, Neonatal Individualized Developmental Care and Assessment Program; SSC, skin-to-skin contact.
References
1. Pierrat V, Marchand-Martin L, Arnaud C, Kaminski M, Resche-Rigon M, Lebeaux C, et al. Neurodevelopmental outcome at 2 years for preterm children born at 22 to 34 weeks' gestation in France in 2011: EPIPAGE-2 cohort study. BMJ. (2017) 358:j3448. doi: 10.1136/bmj.j3448
2. Serenius F, Källén K, Blennow M, Ewald U, Fellman V, Holmström G, et al. Neurodevelopmental outcome in extremely preterm infants at 2.5 years after active perinatal care in Sweden. JAMA. (2013) 309:1810–20. doi: 10.1001/jama.2013.3786
3. Moore T, Hennessy EM, Myles J, Johnson SJ, Draper ES, Costeloe KL, et al. Neurological and developmental outcome in extremely preterm children born in England in 1995 and 2006: the EPICure studies. BMJ. (2012) 345:e7961. doi: 10.1136/bmj.e7961
4. Larroque B, Ancel P-Y, Marret S, Marchand L, André M, Arnaud C, et al. Neurodevelopmental disabilities and special care of 5-year-old children born before 33 weeks of gestation (the EPIPAGE study): a longitudinal cohort study. Lancet. (2008) 371:813–20. doi: 10.1016/S0140-6736(08)60380-3
5. Johnson S, Hennessy E, Smith R, Trikic R, Wolke D, Marlow N. Academic attainment and special educational needs in extremely preterm children at 11 years of age: the EPICure study. Arch Dis Child Fetal Neonatal Ed. (2009) 94:F283–9. doi: 10.1136/adc.2008.152793
6. Knudsen EI. Sensitive periods in the development of the brain and behavior. J Cogn Neurosci. (2004) 16:1412–25. doi: 10.1162/0898929042304796
7. Lagercrantz H, Hanson MA, Ment LR, Peebles DM editors. The Newborn Brain: Neuroscience and Clinical Applications. 2nd ed. Cambridge: Cambridge University Press (2010). doi: 10.1017/CBO9780511711848
8. Graven SN. Clinical research data illuminating the relationship between the physical environment & patient medical outcomes. J Healthc Des Proc Symp Healthc Des Symp Healthc Des. (1997) 9:15–19; discussion: 21–4.
9. Anand KJ, International Evidence-Based Group for Neonatal Pain. Consensus statement for the prevention and management of pain in the newborn. Arch Pediatr Adolesc Med. (2001) 155:173–80. doi: 10.1001/archpedi.155.2.173
10. Kuhn P, Zores C, Astruc D, Dufour A, Casper Ch. Développement sensoriel des nouveau-nés grands prématurés et environnement physique hospitalier. Arch Pédiatrie. (2011) 18(Suppl. 2):S92–102. doi: 10.1016/S0929-693X(11)71097-1
11. Overview - EFCNI. Available online at: https://newborn-health-standards.org/standards/infant-and-family-centred-care/overview/ (accessed November 30, 2020).
12. Jacobs SE, Sokol J, Ohlsson A. The newborn individualized developmental care and assessment program is not supported by meta-analyses of the data. J Pediatr. (2002) 140:699–706. doi: 10.1067/mpd.2002.123667
13. Symington A, Pinelli J. Developmental care for promoting development and preventing morbidity in preterm infants. In: The Cochrane Database of Systematic Reviews. John Wiley & Sons, Ltd. Available online at: http://onlinelibrary.wiley.com.scd-rproxy.u-strasbg.fr/doi/10.1002/14651858.CD001814/abstract (accessed September 29, 2014).
14. Ohlsson A, Jacobs SE. NIDCAP: a systematic review and meta-analyses of randomized controlled trials. Pediatrics. (2013) 131:e881–93. doi: 10.1542/peds.2012-2121
15. Peters KL, Rosychuk RJ, Hendson L, Coté JJ, McPherson C, Tyebkhan JM. Improvement of short- and long-term outcomes for very low birth weight infants: Edmonton NIDCAP trial. Pediatrics. (2009) 124:1009–20. doi: 10.1542/peds.2008-3808
16. Maguire CM, Walther FJ, Sprij AJ, Cessie SL, Wit JM, Veen S. Effects of individualized developmental care in a randomized trial of preterm infants <32 weeks. Pediatrics. (2009) 124:1021–30. doi: 10.1542/peds.2008-1881
17. Haumont D, Amiel-Tison C, Casper C, Conneman N, Ferrari F, Huppi P, et al. NIDCAP and developmental care: a European perspective. Pediatrics. (2013) 132:e551–2. doi: 10.1542/peds.2013-1447C
18. Ortenstrand A, Westrup B, Broström EB, Sarman I, Akerström S, Brune T, et al. The Stockholm Neonatal Family Centered Care study: effects on length of stay and infant morbidity. Pediatrics. (2010) 125:e278–85. doi: 10.1542/peds.2009-1511
19. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. The BMJ. (2008) 337:a1655. doi: 10.1136/bmj.a1655
20. Haynes B. Can it work? Does it work? Is it worth it? BMJ. (1999) 319:652–3. doi: 10.1136/bmj.319.7211.652
21. Mosqueda R, Castilla Y, Perapoch J, de la Cruz J, López-Maestro M, Pallás C. Staff perceptions on Newborn Individualized Developmental Care and Assessment Program (NIDCAP) during its implementation in two Spanish neonatal units. Early Hum Dev. (2013) 89:27–33. doi: 10.1016/j.earlhumdev.2012.07.013
22. Wielenga J, Smit B, Merkus M, Kok J. Individualized developmental care in a Dutch NICU: short-term clinical outcome. Acta Paediatr. (2007) 96:1409–15. doi: 10.1111/j.1651-2227.2007.00451.x
23. Sizun J, Westrup B. Early developmental care for preterm neonates: a call for more research. Arch Dis Child Fetal Neonatal Ed. (2004) 89:F384–8. doi: 10.1136/adc.2002.025114
24. Pierrat V, Coquelin A, Cuttini M, Khoshnood B, Glorieux I, Claris O, et al. Translating neurodevelopmental care policies into practice: the experience of neonatal ICUs in France—the EPIPAGE-2 Cohort study. Pediatr Crit Care Med. (2016) 17:957–67. doi: 10.1097/PCC.0000000000000914
25. Pierrat V, Goubet N, Peifer K, Sizun J. How can we evaluate developmental care practices prior to their implementation in a neonatal intensive care unit? Early Hum Dev. (2007) 83:415–8. doi: 10.1016/j.earlhumdev.2007.03.003
26. Als H. Program Guide—Newborn Individualized Developmental Care and Assessment Program (NIDCAP): An Education and Training Program for Health Care Professionals. Boston, MA: NIDCAP Federation International (1986).
27. Als H, Lawhon G, Duffy FH, McAnulty GB, Gibes-Grossman R, Blickman JG. Individualized developmental care for the very low-birth-weight preterm infant. Medical and neurofunctional effects. JAMA. (1994) 272:853–8.
28. Carbajal R, Rousset A, Danan C, Coquery S, Nolent P, Ducrocq S, et al. Epidemiology and treatment of painful procedures in neonates in intensive care units. JAMA. (2008) 300:60–70. doi: 10.1001/jama.300.1.60
29. Montirosso R, Prete AD, Bellù R, Tronick E, Borgatti R. Level of NICU quality of developmental care and neurobehavioral performance in very preterm infants. Pediatrics. (2012) 129:e1129–37. doi: 10.1542/peds.2011-0813
30. Montirosso R, Casini E, Prete AD, Zanini R, Bellù R, Borgatti R. Neonatal developmental care in infant pain management and internalizing behaviours at 18 months in prematurely born children. Eur J Pain. (2016) 20:1010–21. doi: 10.1002/ejp.826
31. Montirosso R, Giusti L, Del Prete A, Zanini R, Bellù R, Borgatti R. Does quality of developmental care in NICUs affect health-related quality of life in 5-y-old children born preterm? Pediatr Res. (2016) 80:824–8. doi: 10.1038/pr.2016.158
32. Holsti L, Grunau RE, Oberlander TF, Whitfield MF. Specific newborn individualized developmental care and assessment program movements are associated with acute pain in preterm infants in the neonatal intensive care unit. Pediatrics. (2004) 114:65–72. doi: 10.1542/peds.114.1.65
33. Holsti L, Grunau RE. Initial validation of the behavioral indicators of infant pain (BIIP). Pain. (2007) 132:264–72. doi: 10.1016/j.pain.2007.01.033
34. Lundqvist P, Kleberg A, Edberg A-K, Larsson BA, Hellström-Westas L, Norman E. Development and psychometric properties of the Swedish ALPS-Neo pain and stress assessment scale for newborn infants. Acta Paediatr. (2014) 103:833–9. doi: 10.1111/apa.12672
35. Courtois E, Cimerman P, Dubuche V, Goiset M-F, Orfèvre C, Lagarde A, et al. The burden of venipuncture pain in neonatal intensive care units: EPIPPAIN 2, a prospective observational study. Int J Nurs Stud. (2016) 57:48–59. doi: 10.1016/j.ijnurstu.2016.01.014
36. Catelin C, Tordjman S, Morin V, Oger E, Sizun J. Clinical, physiologic, and biologic impact of environmental and behavioral interventions in neonates during a routine nursing procedure. J Pain. (2005) 6:791–7. doi: 10.1016/j.jpain.2005.07.010
37. Sizun J, Ansquer H, Browne J, Tordjman S, Morin J-F. Developmental care decreases physiologic and behavioral pain expression in preterm neonates. J Pain. (2002) 3:446–50. doi: 10.1054/jpai.2002.128066
38. Roofthooft DWE, Simons SHP, Anand KJS, Tibboel D, van Dijk M. Eight years later, are we still hurting newborn infants? Neonatology. (2014) 105:218–26. doi: 10.1159/000357207
39. Westrup B, Sizun J, Lagercrantz H. Family-centered developmental supportive care: a holistic and humane approach to reduce stress and pain in neonates. J Perinatol. (2007) 27:S12–8. doi: 10.1038/sj.jp.7211724
40. Mörelius E, Angelhoff C, Eriksson J, Olhager E. Time of initiation of skin-to-skin contact in extremely preterm infants in Sweden. Acta Paediatr. (2012) 101:14–8. doi: 10.1111/j.1651-2227.2011.02398.x
41. Pallás-Alonso CR, Losacco V, Maraschini A, Greisen G, Pierrat V, Warren I, et al. Parental involvement and kangaroo care in European neonatal intensive care units: a policy survey in eight countries. Pediatr Crit Care Med J Soc Crit Care Med World Fed Pediatr Intensive Crit Care Soc. (2012) 13:568–77. doi: 10.1097/PCC.0b013e3182417959
42. Raiskila S, Axelin A, Toome L, Caballero S, Tandberg BS, Montirosso R, et al. Parents' presence and parent-infant closeness in 11 neonatal intensive care units in six European countries vary between and within the countries. Acta Paediatr. (2017) 106:878–88. doi: 10.1111/apa.13798
43. Kuhn P Sizun J Casper C GREEN study group from the French Neonatal Society. Recommendations on the environment for hospitalised newborn infants from the French neonatal society: rationale, methods and first recommendation on neonatal intensive care unit design. Acta Paediatr. (2018) 107:1860–6. doi: 10.1111/apa.14501
44. Als H, Lawhon G, Brown E, Gibes R, Duffy FH, McAnulty G, et al. Individualized behavioral and environmental care for the very low birth weight preterm infant at high risk for bronchopulmonary dysplasia: neonatal intensive care unit and developmental outcome. Pediatrics. (1986) 78:1123–32.
45. Sweet DG, Carnielli V, Greisen G, Hallman M, Ozek E, Plavka R, et al. European consensus guidelines on the management of neonatal respiratory distress syndrome in preterm infants - 2010 update. Neonatology. (2010) 97:402–17. doi: 10.1159/000297773
46. Sweet DG, Carnielli V, Greisen G, Hallman M, Ozek E, Plavka R, et al. European consensus guidelines on the management of neonatal respiratory distress syndrome in preterm infants−2013 update. Neonatology. (2013) 103:353–68. doi: 10.1159/000349928
47. Sweet DG, Carnielli V, Greisen G, Hallman M, Ozek E, Plavka R, et al. European consensus guidelines on the management of respiratory distress syndrome - 2016 update. Neonatology. (2017) 111:107–25. doi: 10.1159/000448985
48. O'Brien K, Robson K, Bracht M, Cruz M, Lui K, Alvaro R, et al. Effectiveness of Family Integrated Care in neonatal intensive care units on infant and parent outcomes: a multicentre, multinational, cluster-randomised controlled trial. Lancet Child Adolesc Health. (2018) 2:245–54. doi: 10.1016/S2352-4642(18)30039-7
49. Als H. NIDCAP: testing the effectiveness of a relationship-based comprehensive intervention. Pediatrics. (2009) 124:1208–10. doi: 10.1542/peds.2009-1646
50. Infant Journal - Family Infant Neurodevelopmental Education: An Innovative Educational Pathway for Neonatal Healthcare Professionals. Available online at: http://www.infantjournal.co.uk/journal_article.html?RecordNumber=6978 (accessed July 3, 2018).
51. Philbin MK, Ross ES. The SOFFI reference guides: text, algorithms, and appendices: a manualized method for quality bottle feedings. J Perinat Neonatal Nurs. (2011) 25:360–80. doi: 10.1097/JPN.0b013e31823529da
52. Feldman R, Eidelman AI, Sirota L, Weller A. Comparison of skin-to-skin (kangaroo) and traditional care: parenting outcomes and preterm infant development. Pediatrics. (2002) 110:16–26. doi: 10.1542/peds.110.1.16
53. Feldman R, Rosenthal Z, Eidelman AI. Maternal-preterm skin-to-skin contact enhances child physiologic organization and cognitive control across the first 10 years of life. Biol Psychiatry. (2014) 75:56–64. doi: 10.1016/j.biopsych.2013.08.012
Keywords: developmental care, extremely preterm infant, family centered care, implementation, Neonatal Individualized Developmental Care and Assessment Program, pain management, parental involvement, skin-to-skin contact
Citation: Klein V, Zores-Koenig C, Dillenseger L, Langlet C, Escande B, Astruc D, Le Ray I, Kuhn P and Strasbourg NIDCAP Study group (2021) Changes of Infant- and Family-Centered Care Practices Administered to Extremely Preterm Infants During Implementation of the NIDCAP Program. Front. Pediatr. 9:718813. doi: 10.3389/fped.2021.718813
Received: 01 June 2021; Accepted: 05 August 2021;
Published: 03 September 2021.
Edited by:
Jos M. Latour, University of Plymouth, United KingdomReviewed by:
Raghavendra N. Vanaki, HSK Hospital and Research Centre, IndiaDaniel Dirnberger, Alfred I. duPont Hospital for Children, United States
Copyright © 2021 Klein, Zores-Koenig, Dillenseger, Langlet, Escande, Astruc, Le Ray, Kuhn and Strasbourg NIDCAP Study group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pierre Kuhn, cGllcnJlLmt1aG5AY2hydS1zdHJhc2JvdXJnLmZy