
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 31 August 2021
Sec. Pediatric Gastroenterology, Hepatology and Nutrition
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.709933
This article is part of the Research Topic Nutrition During the First 1000 Days and Fetal Programming View all 10 articles
 Reyna Sámano1,2
Reyna Sámano1,2 Gabriela Chico-Barba1,3
Gabriela Chico-Barba1,3 Hugo Martínez-Rojano4,5*
Hugo Martínez-Rojano4,5* María Hernández-Trejo6
María Hernández-Trejo6 Mery Birch7Maribel López-Vázquez7Gabriela Eurídice García-López8Jesús Díaz de León7Cynthia Vanessa Mendoza-González7
Mery Birch7Maribel López-Vázquez7Gabriela Eurídice García-López8Jesús Díaz de León7Cynthia Vanessa Mendoza-González7Background: Young maternal age is associated with negative outcomes at birth and with offspring's growth. In low- and middle-income countries, adolescents' offspring growth little has been studied.
Objective: To determine the association of maternal sociodemographic characteristics with weight, length, and BMI change in adolescents' offspring in their first year of life.
Methods: This is a one-year follow-up study that included adolescent mothers and their offspring from 2010 to 2017. The infant anthropometric variables were performed at birth, 3, 6, and 12 months. Maternal health, pregnancy, and social variables were evaluated as well as birth outcomes. Crude, percentage, Z score, and percentile changes of weight, length, and BMI were evaluated from birth to 1-year-old. Statistical analyses were adjusted by maternal chronological age, socioeconomic status, breastfeeding duration, the timing of introduction of complementary feeding, among other variables.
Results: We examined 186 dyads (mother-infant). The median maternal age was 15.5 years, and the mean pre-pregnancy BMI was 20. The mean gestational age was 39.1 weeks for infants, birth weight was 3,039 g, and length at birth was 49.5-cm. Maternal chronological age, the timing of introduction of complementary feeding, socioeconomic status, and maternal occupation were associated with offspring's weight gain at 12 months. Length gain was associated with exclusive breastfeeding. Socioeconomic status and occupation were associated with offspring's BMI change. When performing adjusted multivariable analyses, weight and length at birth were associated weight and BMI at 12 months.
Conclusions: Weight at birth may negatively predict infant's weight and BMI changes at 12 months, while length at birth may positively predict the changes. Maternal chronological age, socioeconomic level, occupation, and the timing of the introduction of complementary feeding were associated with the weight change. Only exclusive breastfeeding was associated with length Z-score change in adolescents' offspring in their first 12-months of life.
Adolescent pregnancy is associated with an increased risk of eclampsia, puerperal endometritis, systemic infections, maternal mortality, and preterm delivery compared to pregnant adults (≥20 years old) (1). Most of the research related to adolescent pregnancy and their offspring outcomes comes from high-income countries (2), even though teen pregnancy has higher rates in low- and middle-income countries (3). Pregnant adolescents may be at risk of being physically immature due to delayed completion of growth, especially when they have a pre-pregnancy body mass index (BMI) of underweight (4, 5).
The reasons for the adverse maternal and neonatal outcomes in adolescents are not clear yet, but it seems that inadequate/absent prenatal care is one of the main risk factors (6). Evidence shows that adverse perinatal outcomes in adolescents can be lowered with adequate prenatal care (7). In this sense, the lack of prenatal care in adolescent mothers has been related to a high risk of low birth weight and higher risk of perinatal mortality (8). Regarding neonatal outcomes, their anthropometric measurements can be influenced by several factors, like maternal age, pre-pregnancy weight, excessive gestational weight gain, and offspring's gender and gestational age (9–11).
Social and cultural factors are also associated with perinatal outcomes in pregnant adolescents. Many pregnant adolescents drop out of school, leading to a cycle of unemployment and poverty for life. These structural challenges resonate to promote the care of adolescent mothers. For example, the adolescents who go back to school often stop breastfeeding their children, contributing to the low rates of exclusive breastfeeding (8% at 6 months) (12). Therefore, it is predicted that adolescent mothers will have more difficulties in caring for their children, such as in breastfeeding practice and vaccines for children (2).
For the adolescents' offspring, the risk of perinatal morbidity and mortality, low birth weight, small for gestational age, and severe neonatal conditions is increased (13). Also, being an adolescent mother is associated with less knowledge about parenting and infant growth; for these reasons, adolescents may become less confident in their parental abilities, as well as being immature in their behavior and expressing more problematic parenting beliefs, and therefore, less able to meet the needs of their children (14, 15). On the other hand, as adolescents are still growing, there is a nutrient competition between the mother and the fetus (16).
Currently, very few longitudinal studies have investigated the after-birth growth of adolescents' offspring. Therefore, the purpose of the study was to determine the association of maternal sociodemographic characteristics with weight, length, and BMI change in adolescents' offspring in their first year of life.
We conducted a prospective cohort study at Mexico's Instituto Nacional de Perinatología (INPer) from 2010 to 2017. INPer is a public tertiary care institution that treats high-risk pregnancies of women who do not have formal employment or health insurance. The participants were 186 dyads of pregnant adolescents and their offspring. The children were born in the toco-surgical unit of INPer, and we followed them from birth to their first year of life. Sampling was non-probabilistic, and women who met the selection criteria were included consecutively. The participants were pregnant adolescents from 10 to 19 years old, primiparous, with a singleton pregnancy, with <20 weeks of gestation, and without chronic, metabolic, or genetic diseases. All participants signed informed assent, and their respective parents or guardians signed informed consent. We eliminated the participants that had gestational diabetes or hypertensive disorders during pregnancy. Also, dyads were eliminated if the offspring had a disease that affected growth, such as hypothyroidism, diabetes, heart diseases, neoplasms, or 21-trisomy. A structured questionnaire was used to gather sociodemographic data, like age, marital status, level of education, occupation, socioeconomic level, pre-pregnancy weight, history of diseases, and smoking and alcohol drinking habits.
Trained health workers obtained the mothers' and their offspring's data using the questionnaire, clinical records, and performing interviews during the postnatal nutritional visits. We calculated the mother's chronological age at the moment of the delivery from the baseline data. We obtained the date of birth, sex, gestational age, birth weight, and length at birth directly from clinical records. We calculated gestational age at baseline evaluation or from the clinical record according to the last menstrual period. Neonatal outcomes were defined as follows: low birth weight <2,500 g, and small for gestational age as birth weight below the 10th percentile for specific gestational age and sex, according to the World Health Organization (WHO) criteria using AnthroPlus-WHO® (17).
Trained health professionals performed anthropometric measurements of the offspring at 3, 6, and 12 months. Birth weight was determined in grams on a pediatric digital scale Tanita 1583 (CMS Weighing Equipment Ltd., London, UK) with an accuracy of 0.01 kg. Length at birth was measured in centimeters with an infanto-meter Harpenden with an accuracy of 0.1 cm (CMS Weighing Equipment Ltd., London, UK). Length-for-age and weight-for-length were converted into sex-specific and gestational-age-adjusted Z-scores, respectively. Growth retardation was defined as a Z-score of length-for-age and weight-for-length and BMI below −2 SD, respectively (18).
Breastfeeding practice was prospectively assessed every 3 months during follow-up visits and was associate with growth variables: weight, length, and BMI. According to the definitions provided by the WHO (19), we evaluated any type of breastfeeding practice as the duration in months.
The socioeconomic level was considered a potential confounder; it was assessed with six dimensions of well-being within the household: Human Capital, Practical infrastructure, Connectivity and entertainment, Health infrastructure, Planning and future, and Basic infrastructure and space (20).
The Institutional Review Board and Ethics Committees from INPer approved the study with registration number 212250-49451. All data gathering was confidential. All participants received nutritional counseling to help them to improve their eating habits.
Frequencies and percentages were obtained for categorical variables. We calculated measures of central tendency and dispersion for numerical variables. We used the Kolmogorov-Smirnoff test to assess the distribution of numerical variables. Crude, percentage, Z score, and percentile changes of weight, length, and BMI were evaluated from birth to 1-year-old. Sociodemographic and clinical variables and breastfeeding duration were classified into two categories; then, weight, length, and BMI changes were compared between categories using a t-Student or a U Mann–Whitney test. Several univariate linear models were carried out to identify the variables that explained the weight, length, and BMI changes. These models were adjusted for possible confounding variables such as breastfeeding, maternal age, gestational age, educational lag, educational level, type of delivery, among others. All data were analyzed using the 21st version SPSS for Windows (IBM® Corp, Armonk, NY, USA). Statistical significance was declared at p < 0.05.
A total of 186 dyads (adolescent mothers and their children) participated in the study. All pregnancies were at term. Mean maternal age was 15.5 years and the median pre-pregnancy BMI was 20. Eighteen percent of the adolescents had a job or was a student; for educational level 27.4% had elementary school and 72.6% were at junior high, 36.6% of participants were ≤15 years, and 72.1% were from very low, low, and low-median socioeconomic levels.
The offspring' characteristics were as follows: 46% of the children were born by vaginal delivery, and 62% were female. The mean gestational age was 39.1 weeks of gestation, mean birth weight 3,039 g, and mean length at birth was 49.5 cm (Table 1).

Table 1. General characteristics of adolescent mothers and their offspring, n = 186 dyads.
Boys and girls had similar birth weights (3,019 ± 344 vs. 3,071 ± 436 g, respectively; p = 0.366). In contrast, the length was greater among the boys than the girls were (49.7 vs. 49.2 cm, respectively; p = 0.028). There were no statistical differences in birth weight between mothers ≤15 years than mothers of 16 to 19 years (3,010 ± 401 vs. 3,055 ± 371, p = 0.435); neither did the length at birth (49.4 vs. 49.5 cm, p = 0.603). Low birth weight prevalence was 6.5% (12 out of 186), the timing of the introduction of complementary feeding was ≤5 months in 125 (67.2%) infants, and only 35.5% were exclusively breastfed for at least 6 months.
After 12 months of follow-up, there was only one case of low weight for age (0.5%). In contrast, 17 children (9.1%) were already in the percentiles of overweight or obesity. The rest of the children had an appropriate weight for their age. The offspring's mean weight at 12 months was lower in mothers ≤15 years compared to ≥16 years (9,307 vs. 9,739 g, p = 0.003). Infants who initiate complementary feeding before 6 months of age weighted less at 12 months of age than infants who initiated complementary feeding after 6 months of age (9,423 vs. 9,906, p = 0.001).
Figure 1 shows length and BMI trends (percentile and Z score) from birth to 12 months old.
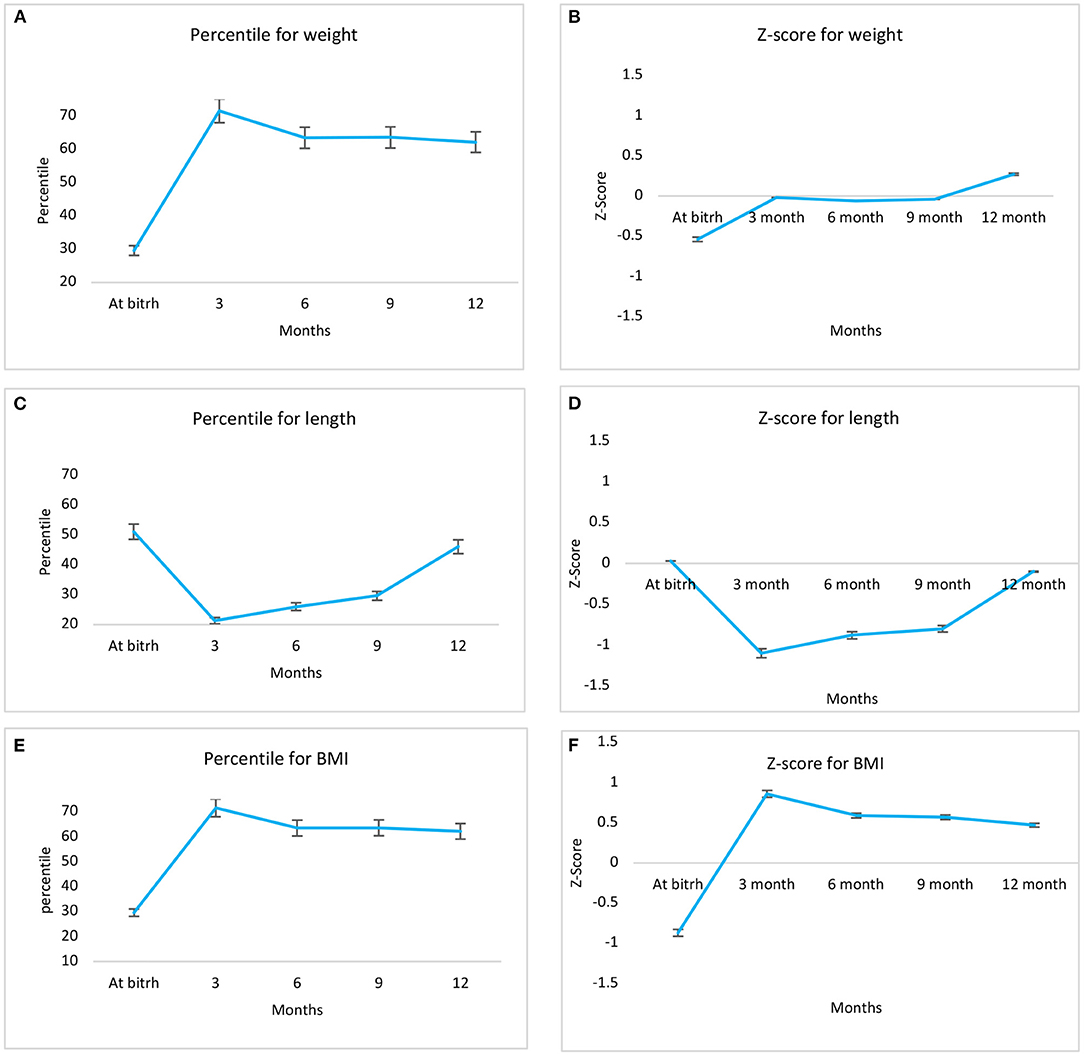
Figure 1. Trends in weight, length and BMI in percentiles (left panel A,C,E) and Z-score (right panel B,D,F), from birth to 12 months in adolescents' offspring.
Table 2 shows that adolescent's offspring from a low socioeconomic level had a mean weight change at 12 months of age lower than the children of mothers from a middle socioeconomic level. When comparing the offspring's weight at 12 months of age by mother's occupation, children from homemakers had higher weight than children of adolescent mothers who had a job or were students. Weight change during the first 12 months of life in adolescent mothers' offspring was different according to the mother's age, the timing of the introduction of complementary feeding, and the socioeconomic level.
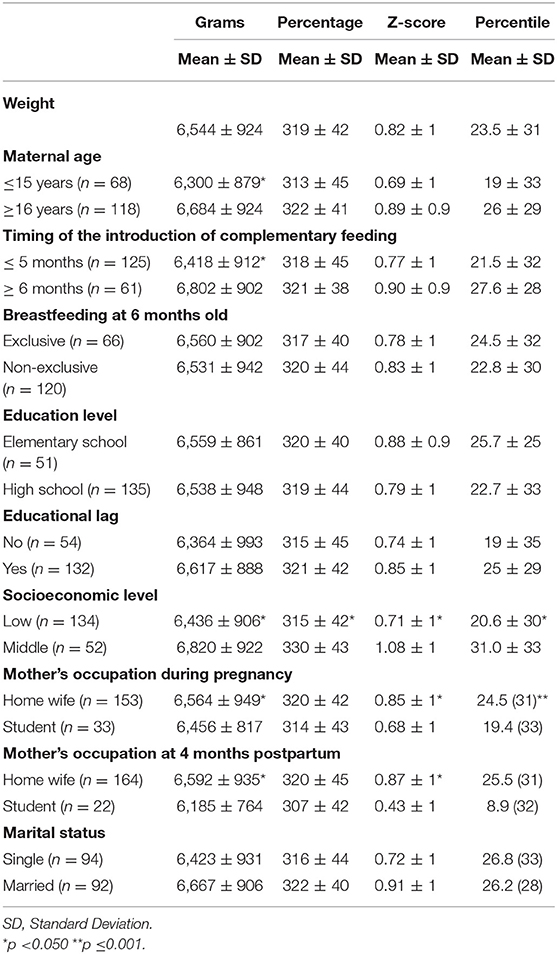
Table 2. Weight change (delta) from birth to 12-months-old, according to maternal sociodemographic characteristics.
Regarding the length measurements, the change in length Z-score during the first 12 months of life in adolescent mothers' offspring differs only by the type of breastfeeding (0.050 ± 1 vs −0.27 ± 1, p = 0.040), the rest of sociodemographic variables did not have any statistical significance (Table 3).
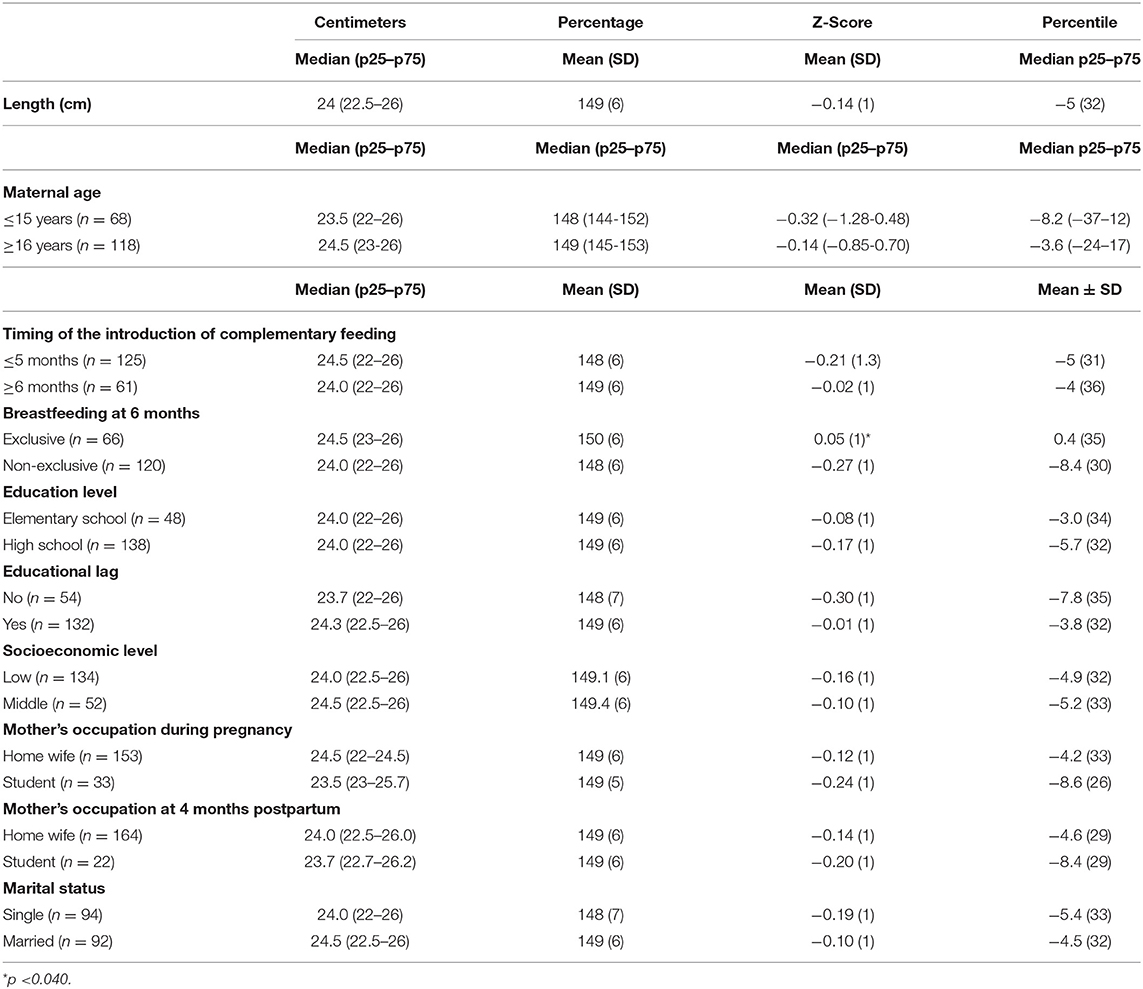
Table 3. Change of length (delta) according to sociodemographic characteristics.
Table 4 shows that the change in the BMI percentile during the first 12 months of life in adolescent mothers' offspring was statistically different by socioeconomic level and the mother's occupation during pregnancy.
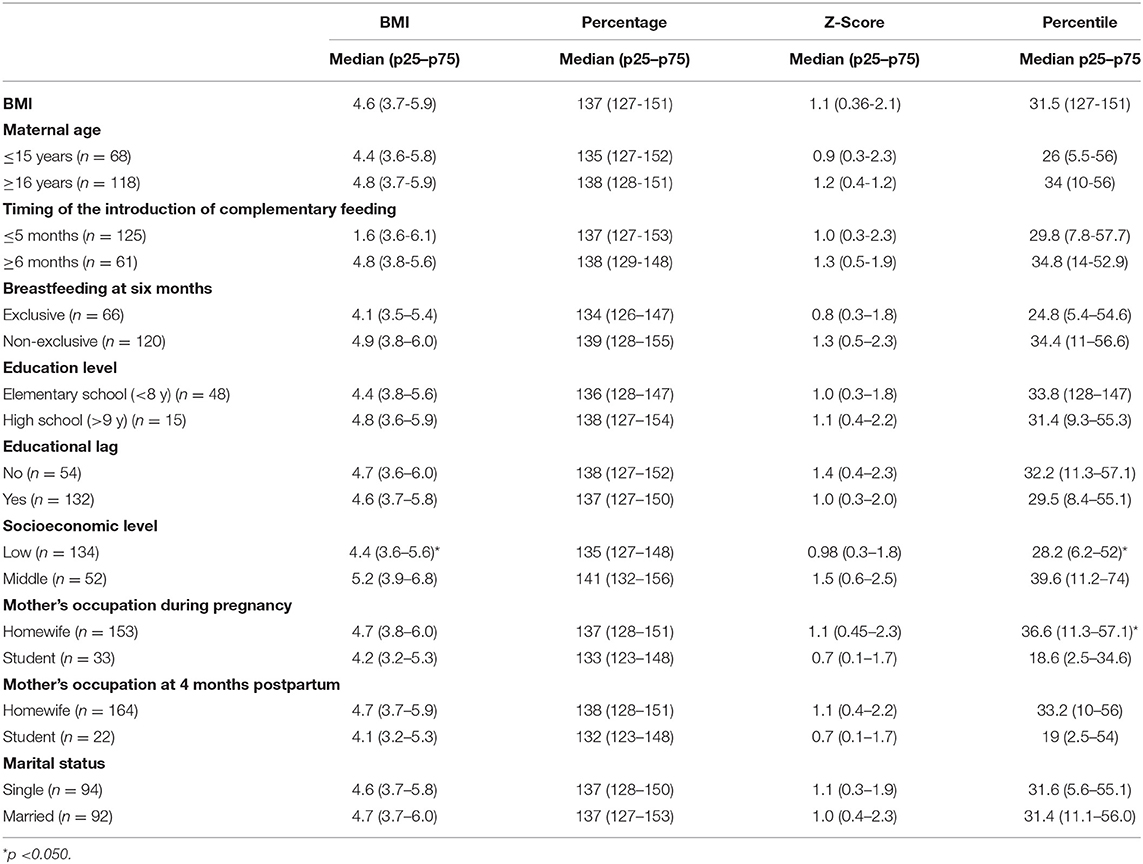
Table 4. Change of BMI (delta) according to maternal sociodemographic characteristics.
Only 35.5% of the children were exclusively breastfed for >6 months, and 67.2% began complementary feeding before 5 months of age. Weight, length, and BMI change at 12 months of the adolescent mothers' offspring were not statistically different according to the type of breastfeeding or the timing of the introduction of complementary feeding.
Tables 5, 6 show that weight and length at birth were the covariates that predicted the weight and BMI change at 12 months and maternal age, mother's occupation, and socioeconomic level, although with less power. Birth weight inversely predicted the anthropometric changes at 12 months according to all the performed models.
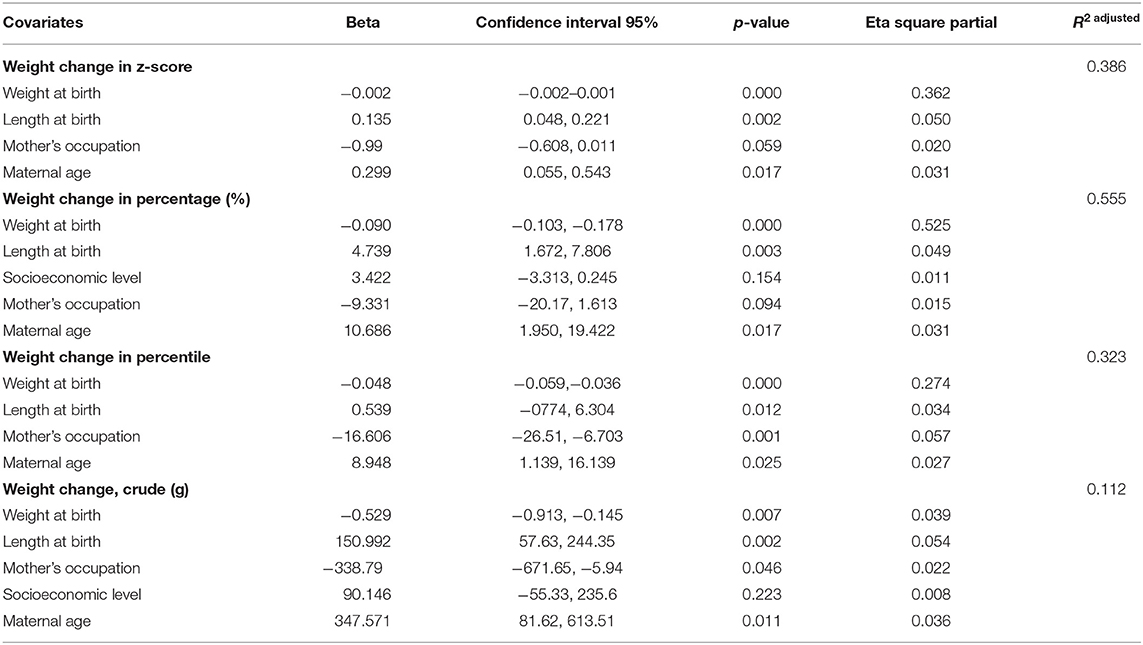
Table 5. Univariate general linear model to determine the predictor variables of weight change parameters.
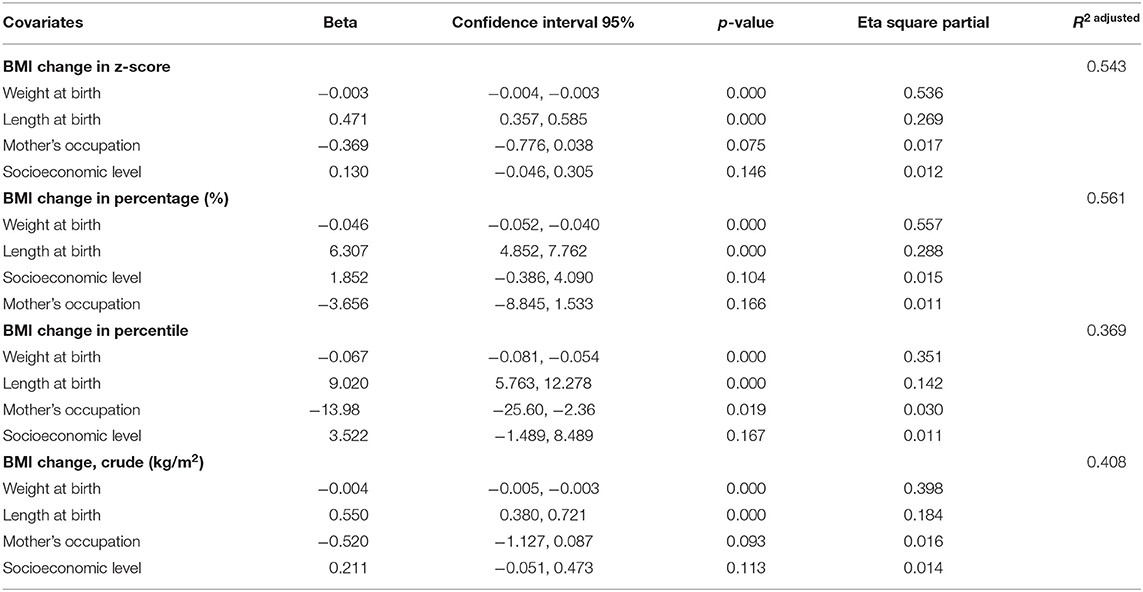
Table 6. Univariate general linear model to determine the predictor variables of BMI change parameters.
Birth weight is a health indicator of the offspring; it reflects the quality of nutrition during pregnancy, predicts immediate survival, and is essential to assess subsequent growth. In our study, the mean birth weight was 3,039 ± 382 g, which is very similar to that reported in children of adolescent mothers in Turkey, where the weight of the newborns was 2,934 g for mothers ≤15 years and 3,021 g for the children of mothers from 16 to 19 years (21). In contrast, the mean birth weight reported for Mexican children of adult mothers in Mexico City and the metropolitan area is 3,200 ± 373 g (22, 23). According to the previous data, the offspring in our study weighted 200 g less than these reports (24, 25). The offspring's anthropometric measurements can be influenced by several factors, including pre-pregnancy weight, excessive gestational weight gain, parity, gender, and gestational age (10).
Differences in pre-pregnancy body composition and gestational weight gain may have contributed to birth weight (10, 26). Studies show that adolescents tend to have low birth weight offspring, which suggests that the pregnant adolescent should receive prenatal care to look after the offspring's weight. Therefore, health care professionals should offer special attention to younger adolescents, who are the most likely to have a higher risk of adverse pregnancy outcomes. In addition, the children of adolescent mothers in developing countries are at a disadvantage at birth and during breastfeeding. In this sense, strategies should strengthen measures to prevent adolescent motherhood and to help to improve the nutrition and education of their children.
Also, offspring of mothers <15 years old have a higher risk of low birth weight. This finding is consistent with evidence showing that adolescent pregnancy is detrimental to the newborn (27–30). However, the low birth weight rate observed in our study is 6.5%, a rate that is lower than the established by the WHO (10% maximum) (31, 32). According to the WHO, in 2000, the prevalence of low birth weight in developed countries was close to 7%, while in South America, it was 9.6%. In 2015, this rate in Latin America and the Caribbean was 8.7% (33). The low rate of low birth weight that we obtained in our study could be attributed mainly to the quality and number of prenatal care visits (34, 35) received at INPer.
One of the main findings of this study was that birth weight and length at birth may predict the weight gain and BMI changes at 12 months old in the offspring of adolescent mothers. Nevertheless, in all statistical models performed, birth weight was the predictor variable on the anthropometric parameters' changes at 12 months old. Regarding the weight and length change during the first 12 months of life, both remained within the parameters of expected gain. However, the length change was slightly lower, although always within the parameters recommended by the WHO (17). Our results agree with that published by Chen et al. (36), who demonstrated that children from adolescent mothers had statistically significant lower weight (p < 0.001) and length (p < 0.001), although the speed and slope of growth were similar over time when compared with growth standards, and with data from the children of adult mothers. Wu et al. (37) also reported no significant statistical differences between children of adolescent mothers and children of adult mothers regarding children's growth and development parameters. These promising results are probably due to factors such as higher maternal education, as well as more favorable living conditions, as demonstrated by Luster et al. (38), in their study with children of teenage mothers and adult mothers from Michigan, USA.
Regarding exclusive breastfeeding, its frequency in our study group was 35.5%, which contrasts with that reported by Wambach and Cole (39), who discuss that adolescent mothers breastfeed for a shorter time than adult mothers. On the other hand, according to the National Health and Nutrition Survey 2012 (ENSANUT-2012) (40), in Mexico, the prevalence of exclusive breastfeeding in the general population was 18.5% in rural areas and 14.5% in urban areas. These figures are lower than what we observed in our study group. An explanation for these contrasting numbers is that INPer is a “child- and woman-friendly hospital,” where one of its primary purposes is to promote exclusive breastfeeding for at least 6 months.
Although the prevalence of exclusive breastfeeding was higher than that reported in urban areas of Mexico, it was not associated with weight gain in the adolescents' offspring at 12 months age, which is consistent with previous studies that show that offspring who are exclusively breastfed have a slower growth rate than that reported in infants who are fed with formula milk (41, 42).
Other research also has shown that the duration of breastfeeding is associated with slower growth during the first 12 months of the infant's life, which may contribute to the protective effects of breastfeeding against overweight and obesity at younger ages (43–46).
Our study highlighted that the timing of the introduction of complementary feeding was not associated with weight, length, and BMI changes of the children adolescent mothers at 12 months old. These findings are consistent with those reported by Dewey et al., in a systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries (47) as well as in the study by Woo et al., which included children of adolescent mothers from Mexico, the United States and China (48). In addition to the studies carried out by Briefel et al. (49), and by Chen et al. (36), in a cohort of adolescent mothers from Taiwan, in which the researchers discussed that this behavior might be due to the adverse socio-economic context in which adolescent mothers live, where the quality and quantity of food is compromised. However, one of the limitations of our study was the lack of information available on this topic. Also, the follow-up was only for 12 months to prove the impact of the timing of the introduction of complementary feeding and the practice of exclusive breastfeeding on the change in weight and length in the children of adolescent mothers.
Our finding that adolescent mothers who are engaged in household activities had offspring with a higher weight (9,648 ± 978) at 12 months old than offspring of adolescents who had a job or were students (9,648 ± 978 vs. 9,273 ± 903, respectively; p = 0.044). This finding adds up to the understanding that the care of the infant by its mother translates into better growth (36, 50). Therefore, others factors like socioeconomic level, mother's occupation, and the timing of the introduction of complementary feeding might be associated with weight, length, and BMI change in children of mothers of any age, not only in adolescents.
The strength of the study is that the potential confounders were collected prospectively. Also, the longitudinal study design permits the assessment of causal relationships.
One of the study's limitations is that we do not have data regarding diet or nutritional supplementation use during pregnancy and other aspects of the offspring's diet (in addition to breastfeeding) and paternal factors, so it is not known if we can rule out residual confounders.
Weight at birth negatively predicted offspring weight and BMI changes at 12 months, while length at birth positively predicted the changes. Only exclusive breastfeeding was associated with length Z-score change in adolescents' offspring in their first 12-months of life.
The offspring of adolescent mothers had lower weight and height, despite the fact that the speed and slope of the growth patterns were similar over time with the growth standards established by the WHO.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The Institutional Review Board and Ethics Committees from INPer approved the study with registration number 212250-49451. The participant's legal guardian/next of kin provided written informed consent to participate in this study.
RS, HM-R, and GC-B: Conceptualization. RS, HM-R, GC-B, and MH-T: Data curation and Supervision. RS, HM-R, GC-B, MH-T, MB, and ML-V: Formal analysis. RS: Funding acquisition and project administration. RS, HM-R, GC-B, MH-T, MB, ML-V, and JD: Investigation. RS, HM-R, GC-B, MH-T, MB, ML-V, GG-L, JD, and CM-G: Methodology, writing – original draft and writing – review editing. RS, HM-R, and GC-B: resources and validation. RS, HM-R, GC-B, MH-T, and ML-V: Visualization. All authors contributed to the article and approved the submitted version.
The National Institute of Perinatology (Registration Number 212250-49451) funded this research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all the participants and their children for their participation and cooperation with this study.
BMI, Body Mass Index; ENSANUT, National Health and Nutrition Survey; INPer, Instituto Nacional de Perinatología; p-BMI, Pre-pregnancy Body Mass Index; SD, Standard Deviation; WHO, World Health Organization.
1. Nove A, Matthews Z, Neal S, Camacho AV. Maternal mortality in adolescents compared with women of other ages: evidence from 144 countries. Lancet Glob Health. (2014) 2:e155–64. doi: 10.1016/S2214-109X(13)70179-7
2. Smith C, Strohschein L, Crosnoe R. Family histories and teen pregnancy in the United States and Canada. J Marriage Fam. (2018) 80:1244–58. doi: 10.1111/jomf.12512
3. Hubert C, Villalobos A, Abreu AB, Suárez-Lopez L, Castro F. Factors associated with pregnancy and motherhood among Mexican women aged 15-24. Cad Saude Publica. (2019) 35:e00142318. doi: 10.1590/0102-311x00142318
4. Neal S, Matthews Z, Frost M, Fogstad H, Camacho AV, Laski L. Childbearing in adolescents aged 12-15 years in low resource countries: a neglected issue. New estimates from demographic and household surveys in 42 countries. Acta Obstet Gynecol Scand. (2012) 91:1114–8. doi: 10.1111/j.1600-0412.2012.01467.x
5. Schaffnit SB, Urassa M, Lawson DW. “Child marriage” in context: exploring local attitudes towards early marriage in rural Tanzania. Sex Reprod Health Matters. (2019) 27:1571304. doi: 10.1080/09688080.2019.1571304
6. Ganchimeg T, Ota E, Morisaki N, Laopaiboon M, Lumbiganon P, Zhang J, et al. WHO multicountry survey on maternal newborn health research network. Pregnancy and childbirth outcomes among adolescent mothers: a World Health Organization multicountry study. BJOG. (2014) 121:40–8. doi: 10.1111/1471-0528.12630
7. Vieira CL, Coeli CM, Pinheiro RS, Brandão ER, Camargo KR Jr, Aguiar FP. Modifying effect of prenatal care on the association between young maternal age and adverse birth outcomes. J Pediatr Adolesc Gynecol. (2012) 25:185–9. doi: 10.1016/j.jpag.2011.12.070
8. Kawakita T, Wilson K, Grantz KL, Landy HJ, Huang CC, Gomez-Lobo V. Adverse maternal and neonatal outcomes in adolescent pregnancy. J Pediatr Adolesc Gynecol. (2016) 29:130–6. doi: 10.1016/j.jpag.2015.08.006
9. Thame M, Trotman H, Osmond C, Fletcher H, Antoine M. Body composition in pregnancies of adolescents and mature women and the relationship to birth anthropometry. Eur J Clin Nutr. (2007) 61:47–53. doi: 10.1038/sj.ejcn.1602484
10. Sámano R, Chico-Barba G, Martínez-Rojano H, Godinez E, Rodríguez-Ventura AL, Ávila-Koury G, et al. Pre-pregnancy body mass index classification and gestational weight gain on neonatal outcomes in adolescent mothers: A follow-up study. PLoS ONE. (2018) 13:e0200361. doi: 10.1371/journal.pone.0200361
11. Zhang W, Niu F, Ren X. Association of maternal pre-pregnancy body mass index and gestational weight gain with Chinese infant growth. J Paediatr Child Health. (2019) 55:673–9. doi: 10.1111/jpc.14274
12. Muelbert M, Giugliani ERJ. Factors associated with the maintenance of breastfeeding for 6, 12, and 24 months in adolescent mothers. BMC Public Health. (2018) 18:675. doi: 10.1186/s12889-018-5585-4
13. Soysal S, Sarioz A, Anik Ilhan G, Kocagoz A, Dizi A, Gursoy I, et al. Evaluation of late adolescent pregnancies: Is late adolescence a risk factor for preterm labor? J Matern Fetal Neonatal Med. (2019) 32:851–6. doi: 10.1080/14767058.2017.1393799
14. Sámano R, Lara-Cervantes C, Martínez-Rojano H, Chico-Barba G, Sánchez-Jiménez B, Lokier O, et al. Dietary knowledge and myths vary by age and years of schooling in pregnant mexico city residents. Nutrients. (2020) 12:362. doi: 10.3390/nu12020362
15. Pomerleau A, Scuccimarri C, Malcuit G. Mother-infant behavioral interactions in teenage and adult mothers during the first six months postpartum: Relations with infant development. Infant Ment Health J. (2003) 24:495–509. doi: 10.1002/imhj.10073
16. Scholl TO, Hediger ML, Schall JI, Khoo CS, Fischer RL. Maternal growth during pregnancy and the competition for nutrients. Am J Clin Nutr. (1994) 60:183–8. doi: 10.1093/ajcn/60.2.183
17. WHO Multicentre Growth Reference Study Group: WHO Child Growth Standards: length/height-for-age weight for-age weight-for-length weight-for height and body mass index-for-age: methods and development. Geneva: WHO. (2006). Available online at: https://www.who.int/publications/i/item/924154693X
18. de Onis M. 4. 1 The WHO Child Growth Standards. World Rev Nutr Diet. (2015) 113:278–94. doi: 10.1159/000360352
19. Guideline: protecting promoting and supporting breastfeeding in facilities providing maternity and newborn services. Geneva: World Health Organization. (2017). Available online at: https://www.who.int/nutrition/publications/guidelines/breastfeeding-facilities-maternity-newborn/en/
20. Socioeconomic Level Index of the Mexican Association of Market Research and Public Opinion Agencies (AMAI) September 2014 AMAI Regulation NSE 8 × 7. Available online at: www.amai.org/NSE/NivelSocioeconomicoAMAI.pdf (accessed January 25, 2021).
21. Karataşli V, Kanmaz AG, Inan AH, Budak A, Beyan E. Maternal and neonatal outcomes of adolescent pregnancy. J Gynecol Obstet Hum Reprod. (2019) 48:347–50. doi: 10.1016/j.jogoh.2019.02.011
22. Notzon FC, Bobadilla JL, Coria I. Birthweight distributions in Mexico City and among US Southwest Mexican Americans: the effect of altitude. Am J Public Health. (1992) 82:1014–7. doi: 10.2105/AJPH.82.7.1014
23. Flores HS. and Martínez SH. Birth weight of male and female infants born in hospitals affiliated with the Instituto Mexicano del Seguro. Social Bol Med Hosp Infant Mex. (2012) 69:30–9.
24. Abebe AM, Fitie GW, Jember DA, Reda MM, Wake GE. Teenage pregnancy and its adverse obstetric and perinatal outcomes at Lemlem Karl Hospital, Tigray, Ethiopia, 2018. Biomed Res Int. (2020) 2020:3124847. doi: 10.1155/2020/3124847
25. Kassa GM, Arowojolu AO, Odukogbe AA, Yalew AW. Adverse neonatal outcomes of adolescent pregnancy in Northwest Ethiopia. PLoS ONE. (2019) 14:e0218259. doi: 10.1371/journal.pone.0218259
26. Sámano R, Martínez-Rojano H, Chico-Barba G, Sánchez-Jiménez B, Illescas-Zarate D, Rodríguez-Ventura AL. Characteristics of the family support network of pregnant adolescents and its association with gestational weight gain and birth weight of newborns. Int J Environ Res Public Health. (2019) 16:1222. doi: 10.3390/ijerph16071222
27. Lawlor DA, Mortensen L, Andersen AM. Mechanisms underlying the associations of maternal age with adverse perinatal outcomes: a sibling study of 264 695 Danish women and their firstborn offspring. Int J Epidemiol. (2011) 40:1205–14. doi: 10.1093/ije/dyr084
28. Restrepo-Méndez MC, Barros AJ, Santos IS, Menezes AM, Matijasevich A, Barros FC. Childbearing during adolescence and offspring mortality: findings from three population-based cohorts in southern Brazil. BMC Public Health. (2011) 11:781. doi: 10.1186/1471-2458-11-781
29. Gibbs CM, Wendt A, Peters S, Hogue CJ. The impact of early age at first childbirth on maternal and infant health. Paediatr Perinat Epidemiol. (2012); 26:259–84. doi: 10.1111/j.1365-3016.2012.01290.x
30. Falster K, Hanly M, Banks E, Lynch J, Chambers G, Brownell M, et al. Maternal age and offspring developmental vulnerability at age five: A population-based cohort study of Australian children. PLoS Med. (2018) 15:e1002558. doi: 10.1371/journal.pmed.1002558
31. World Health Organization (WHO) United Nations Children's Fund (UNICEF). Low Birth weight: Country, regional and global estimates. New York: UNICEF. (2004). Available online at: https://apps.who.int/iris/handle/10665/43184
32. Belfort GP, Santos MMAS, Pessoa LDS, Dias JR, Heidelmann SP, Saunders C. Determinants of low birth weight in the children of adolescent mothers: a hierarchical analysis. Cien Saude Colet. (2018) 23:2609–20. doi: 10.1590/1413-81232018238.13972016
33. United Nations Children's Fund (UNICEF) World Health Organization (WHO). UNICEF-WHO Low birthweight estimates: Levels and trends 2000–2015. Geneva: World Health Organization; (2019). Available online at: https://www.who.int/nutrition/publications/UNICEF-WHO-lowbirthweight-estimates-2019/en/
34. Raatikainen K, Heiskanen N, Verkasalo PK, Heinonen S. Good outcome of teenage pregnancies in high-quality maternity care. Eur J Public Health. (2006) 16:157–61. doi: 10.1093/eurpub/cki158
35. Geist RR, Beyth Y, Shashar D, Beller U, Samueloff A. Perinatal outcome of teenage pregnancies in a selected group of patients. J Pediatr Adolesc Gynecol. (2006) 19:189–93. doi: 10.1016/j.jpag.2006.02.005
36. Chen YJ, Li CR, Lee SH, Hsu BQ, Wu WY, Kuo CP, Hwang SL, et al. Growth changes in infants born of adolescent mothers: Results of a national cohort study in Taiwan. Iran J Reprod Med. (2014) 12:737–46.
37. Wu WY, Li CR, Kuo CP, Chiang YC, Lee MC. The growth and development of children born to adolescent mothers in Taiwan. Ital J Pediatr. (2016) 42:80. doi: 10.1186/s13052-016-0280-5
38. Luster T, Bates L, Fitzgerald H, Vandenbelt M, Key JP. Factors related to successful outcomes among preschool children born to low-income adolescent mothers. J Marriage Fam. (2000) 62:133–46. doi: 10.1111/j.1741-3737.2000.00133.x
39. Wambach KA, Cole C. Breastfeeding and adolescents. J Obstet Gynecol Neonatal Nurs. (2000) 29:282–94. doi: 10.1111/j.1552-6909.2000.tb02050.x
40. Gonzalez de, Cosío T, Escobar-Zaragoza L, Gonzalez-Castell LD, Rivera-Dommarco JA. Infant feeding practices and deterioration of breastfeeding in Mexico. Salud Publica de Mexico. (2013) 55:170–S179.
41. Azad MB, Vehling L, Chan D, Klopp A, Nickel NC, McGavock JM, et al. CHILD study investigators. Infant Feeding and Weight Gain: Separating Breast Milk from Breastfeeding and Formula from Food. Pediatrics. (2018) 142:e20181092. doi: 10.1542/peds.2018-1092
42. Zong XN, Li H, Zhang YQ, Wu HH. Growth performance comparison of exclusively breastfed infants with partially breastfed and formula fed infants. PLoS ONE. (2020) 15:e0237067. doi: 10.1371/journal.pone.0237067
43. Nielsen GA, Thomsen BL, Michaelsen KF. Influence of breastfeeding and complementary food on growth between 5 and 10 months. Acta Paediatr. (1998) 87:911–7. doi: 10.1111/j.1651-2227.1998.tb01757.x
44. Pietrobelli A, Agosti M, MeNu Group. Nutrition in the first 1,000 Days: ten practices to minimize obesity emerging from published science. Int J Environ Res Public Health. (2017) 14:1491. doi: 10.3390/ijerph14121491
45. Lind MV, Larnkjær A, Mølgaard C, Michaelsen KF. Breastfeeding, breast milk composition, and growth outcomes. Nestle Nutr Inst Workshop Ser. (2018) 89:63–77. doi: 10.1159/000486493
46. Patro-Gołab B, Zalewski BM, Polaczek A, Szajewska H. Duration of breastfeeding and early growth: a systematic review of current evidence. Breastfeed Med. (2019) 14:218–29. doi: 10.1089/bfm.2018.0187
47. Dewey KG, Adu-Afarwuah S. Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern Child Nutr. (2008) 4:24–85. doi: 10.1111/j.1740-8709.2007.00124.x
48. Woo JG, Guerrero ML, Ruiz-Palacios GM, Peng YM, Herbers PM, Yao W, et al. Specific infant feeding practices do not consistently explain variation in anthropometry at age 1 year in urban United States, Mexico, and China cohorts. J Nutr. (2013) 143:166–74. doi: 10.3945/jn.112.163857
49. Briefel RR, Kalb LM, Condon E, Deming DM, Clusen NA, Fox MK, Harnack L, Gemmill E, Stevens M, Reidy KC. The feeding infants and toddlers study 2008: study design and methods. J Am Diet Assoc. (2010) 110:S16–26. doi: 10.1016/j.jada.2010.09.005
50. le Roux K, Christodoulou J, Stansert-Katzen L, Dippenaar E, Laurenzi C, le Roux IM, Tomlinson M, Rotheram-Borus MJ. A longitudinal cohort study of rural adolescent vs adult South African mothers and their children from birth to 24 months. BMC Pregnancy Childbirth. (2019) 19:24. doi: 10.1186/s12884-018-2164-8
Keywords: body weight, child growth, infant, pregnancy during adolescence, breastfeeding, Mexico
Citation: Sámano R, Chico-Barba G, Martínez-Rojano H, Hernández-Trejo M, Birch M, López-Vázquez M, García-López GE, Díaz de León J and Mendoza-González CV (2021) Factors Associated With Weight, Length, and BMI Change in Adolescents' Offspring in Their First Year of Life. Front. Pediatr. 9:709933. doi: 10.3389/fped.2021.709933
Received: 14 May 2021; Accepted: 29 July 2021;
Published: 31 August 2021.
Edited by:
Felipe Vadillo-Ortega, Universidad Nacional Autónoma de México, MexicoReviewed by:
Lupu Ancuta, Grigore T. Popa University of Medicine and Pharmacy, RomaniaCopyright © 2021 Sámano, Chico-Barba, Martínez-Rojano, Hernández-Trejo, Birch, López-Vázquez, García-López, Díaz de León and Mendoza-González. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hugo Martínez-Rojano, aG1hcnRpbmV6XzU5QHlhaG9vLmNvbS5teA==; aHVnby5tYXJ0aW5lenJAc2FsdWQuZ29iLm14
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.