
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 02 July 2021
Sec. Pediatric Critical Care
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.689485
This article is part of the Research Topic Critical Care of the Medically Complex Child View all 8 articles
 Julia A. Heneghan1*
Julia A. Heneghan1* Sarah A. Sobotka2
Sarah A. Sobotka2 Madhura Hallman3Neethi Pinto4
Madhura Hallman3Neethi Pinto4 Elizabeth Y. Killien5Kathryn Palumbo6
Elizabeth Y. Killien5Kathryn Palumbo6 Sinead Murphy Salem7Kilby Mann8Barbara Smith9Rebecca Steuart10Manzilat Akande11
Sinead Murphy Salem7Kilby Mann8Barbara Smith9Rebecca Steuart10Manzilat Akande11 Robert J. Graham7 for the POST-PICU Investigators of the PALISI Network and the Eunice Kennedy Shriver National Institute of Child Health Human Development Collaborative Pediatric Critical Care Research Network
Robert J. Graham7 for the POST-PICU Investigators of the PALISI Network and the Eunice Kennedy Shriver National Institute of Child Health Human Development Collaborative Pediatric Critical Care Research NetworkChildren with disabilities compose a substantial portion of admissions and bed-days in the pediatric intensive care unit (PICU) and often experience readmissions over time. Impacts of a PICU admission on post-discharge health status may be difficult to distinguish from pre-existing disability in this population. Efforts to standardize outcome measures used for children with disabilities may help identify morbidities associated with PICU hospitalizations. Although a scoping review of outcome measures to assess children after episodes of critical illness has recently been published, it is not known to what extent these measures are appropriate for use in children with disabilities. This limits our ability to effectively measure long-term outcomes following critical illness in this important patient population. Through mixed methodology of scoping review and multi-stakeholder consensus, we aimed to identify and describe instruments previously utilized for this purpose and to explore additional tools for consideration. This yielded 51 measures across a variety of domains that have been utilized in the PICU setting and may be appropriate for use in children with disabilities. We describe characteristics of these instruments, including the type of developmental domains assessed, availability of population data, validation and considerations regarding administration in children with disabilities, and ease of availability of the instrument to researchers. Additionally, we suggest needed alterations or accommodations for these instruments to augment their utility in these populations, and highlight areas for future instrument development.
Episodes of pediatric critical illness may result in mortality or morbidity across a range of domains in a child's functioning. A growing focus among practitioners of pediatric critical care is post-intensive care syndrome-pediatrics (PICS-p), which is characterized by potential changes in multiple domains of functioning in survivors of pediatric critical illness, including neurocognition, physical functioning, social functioning, and health-related quality of life (1). However, many children hospitalized with critical illness have baseline developmental delays and disabilities (2–5). These patients have been shown to be at increased risk for critical illness, as well as for death, prolonged intensive care unit length of stay, and higher medical resource utilization during episodes of critical illness (5–9). In addition, many children with complex medical conditions may be at higher risk for impaired outcomes due to their underlying diseases, susceptibility to adverse effects of therapeutic interventions, or missed educational and therapy experiences while hospitalized, making them among the most vulnerable of pediatric intensive care unit (PICU) patients.
Recent work has resulted in a scoping review as well as a core set of outcome measures used to assess children after episodes of critical illness with a focus on these PICS-p domains (10, 11). However, it is not known whether these measures are appropriate for use in children with pre-existing disabilities or complex medical needs, who make up a substantial portion of admissions to the modern PICU (5, 8, 9). Definitions and categorization of medical complexity [e.g., Children with Special Healthcare Needs (12, 13), Complex Chronic Conditions (14), Pediatric Medical Complexity Algorithm (15), Pediatric Chronic Critical Illness (16)] differ, may inconsistently overlap (17, 18), and variably incorporate assessments of functional status. Notably, not all children with medical complexity will have disabilities, and vice versa. This heterogeneity in definitions highlights the need for identifying or developing a range of instruments to capture meaningful and patient-centered outcomes, taking into consideration individual patient baselines, which may differ from population or age-based normal values. We aimed to identify and describe characteristics of instruments that may be useful to all stakeholders, including but not limited to families, intensivists, and continuity providers (e.g., medical, educational, and therapy-based professionals) in the longitudinal evaluation of children with disabilities following critical illness.
The Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) network POST-PICU Investigators and the Eunice Kennedy Shriver National Institute for Child Health and Human Development Collaborative Pediatric Critical Care Research Network (CPCCRN) conducted a scoping review of all non-mortality outcomes measured following pediatric critical illness to inform the development of a core outcome set for use in pediatric critical care outcomes research. Details of the scoping review (9) and the core outcome set (10) have been previously published. In brief, PubMed, EMBASE, PsycINFO, Cumulative Index of Nursing and Allied Health Literature, and the Cochrane Central Register of Controlled Trials Registry were queried to identify studies published between 1970 and 2017 evaluating the outcomes of survivors or families after pediatric critical illness. Studies were excluded if no post-discharge outcomes were assessed or if mortality was the only outcome examined; if the included patients were primarily adults (>18 years), preterm infants, or neonates; if the patient had not been definitively admitted to an ICU or there was no clear relationship to ICU care (e.g., only a technical procedure/condition was evaluated); if only a single subject was included; if only psychometric properties of an instrument were evaluated or reported; or if the study was not available in English. Each manuscript was dual reviewed for eligibility and each potentially eligible manuscript was subsequently dual screened for final eligibility, with discrepancies resolved by a third reviewer. Information from each manuscript, including study characteristics, was then separately extracted by two reviewers, with discrepancies resolved through consensus. This scoping review identified 366 unique instruments. Of these, 136 were selected for further review by identifying the five most commonly used instruments in each domain, as well as any instrument used in publications from 2007 to 2017.
For the purposes of this study, we included instruments from the prior review where the investigators had indicated use in children with disabilities in order to capture a population likely to overlap with the general PICU population. This yielded 49 instruments. This list was then further narrowed to include only instruments that were used more than once in the scoping review literature base. Instruments were then reviewed by content-area experts (SS, developmental and behavioral pediatrics; KM, pediatric physiatry; BS, pediatric physical therapy) and additional instruments commonly used by experts to assess diverse abilities and disabilities as well instruments which came into use following the conclusion of the scoping review were added. This resulted in a final list of 51 instruments. Additional focused data collection was undertaken to assess how the instruments were used and applied to children with disabilities and to confirm the validity of previously collected data. We abstracted data on instrument characteristics (e.g., suggested age range, reported method and duration of administration, cost, training needed for administration), available information regarding population data for children with disabilities, the types of functioning assessed, and publisher information. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) Checklist was followed (Supplementary Material).
Instruments were classified into nine categories [cognitive functioning, executive functioning, communication, physical functioning, social skills, feeding, family functioning and child quality of life, mental health (e.g., anxiety, depression, trauma), and sleep] in order to capture and delineate complex neurodevelopmental outcomes and align with typical neurodevelopmental domains. These differed from the four categories outlined in PICS-p (Physical Health, Cognitive Health, Emotional Health, and Social Health) in order to best capture the intention of the measures designed and terminology used, but physical health likely relates to our physical functioning domain, cognitive health likely includes both cognitive functioning and executive functioning, emotional health likely includes mental health, and social health likely includes family functioning and child quality of life. The additional domains (communication, social skills, feeding, and sleep) were added to build upon the existing PICS-p framework and reflect developmental domains previously tested by studies evaluating post-PICU outcomes.
Study data for both the overall scoping review and this project were collected and managed using Research Electronic Data Capture (REDCap) hosted, respectively, at the University of Utah and the University of Minnesota. Included data are presented as frequency for categorical data and median and interquartile range (IQR) for continuous data. Data analysis was performed in R (R Foundation for Statistical Computing; Vienna, Austria).
One hundred thirty-six instruments were identified as being commonly or recently used to measure post-discharge outcomes after PICU care as part of the larger scoping review (10). Of these, 49 (36.0%) instruments were identified as having been used in children with disabilities. Of the 51 instruments ultimately included in this study, 27 (52.9%) were drawn from the primary scoping review; 2 (3.9%) were initially excluded based on only a single use in the scoping review but added back based upon expert opinion. The remaining 24 (47.1%) were included based on expert opinion alone. A flow diagram of instruments is shown in Figure 1. PICS-p domains of focus did not vary significantly between those instruments identified in the scoping review and those identified by expert opinion (data not shown). A list of all included instruments divided by domain of functioning assessed, as well as selected characteristics of each instrument can be found in Tables 1–9.
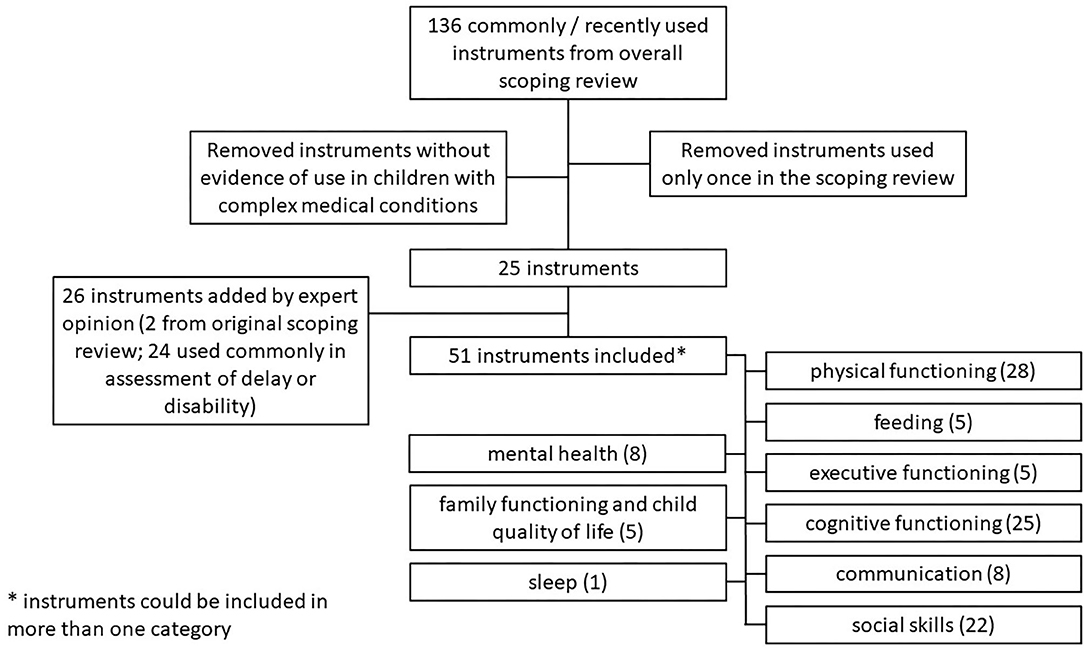
Figure 1. Flow diagram of included instruments by category.
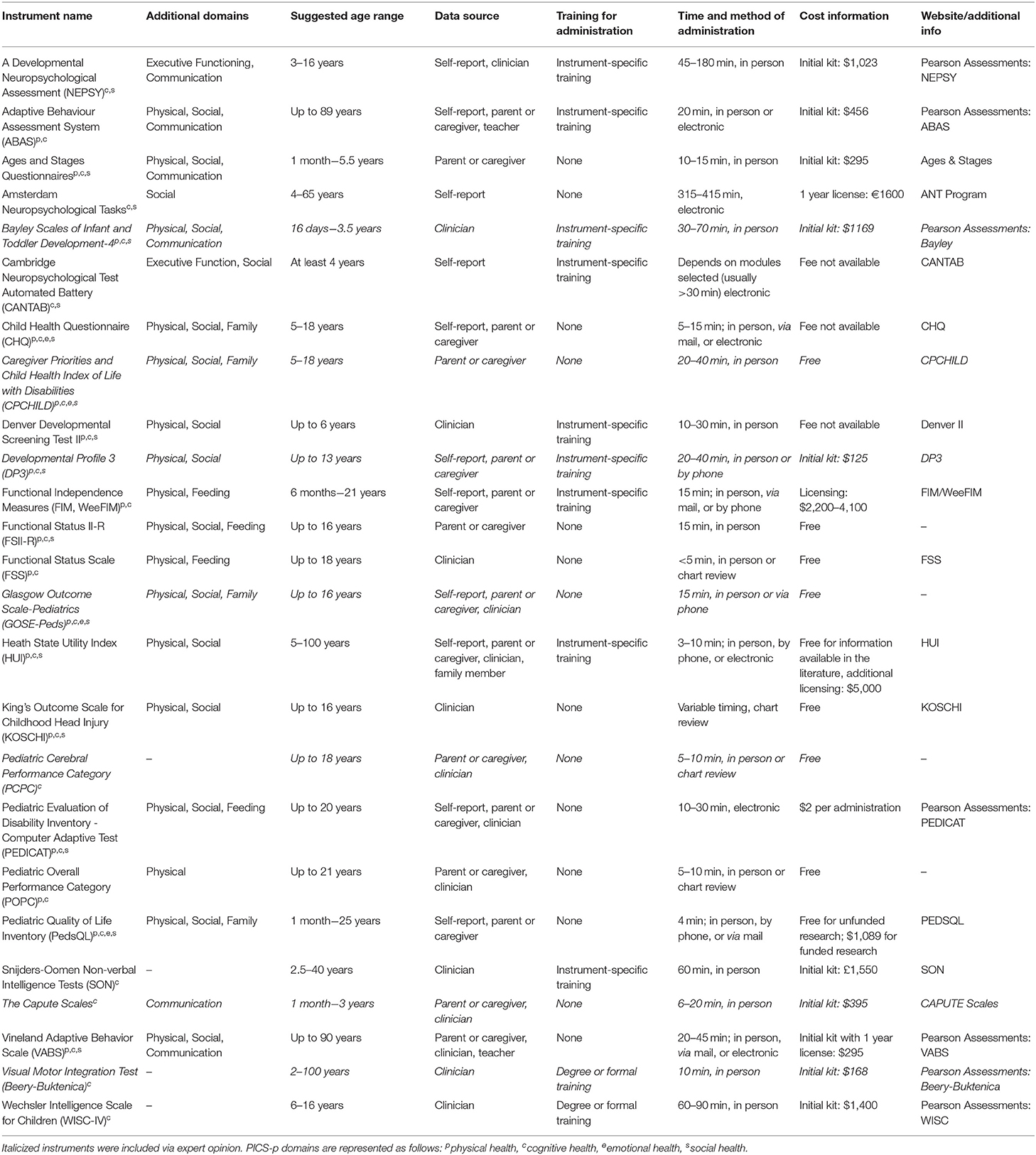
Table 1. Cognitive functioning.
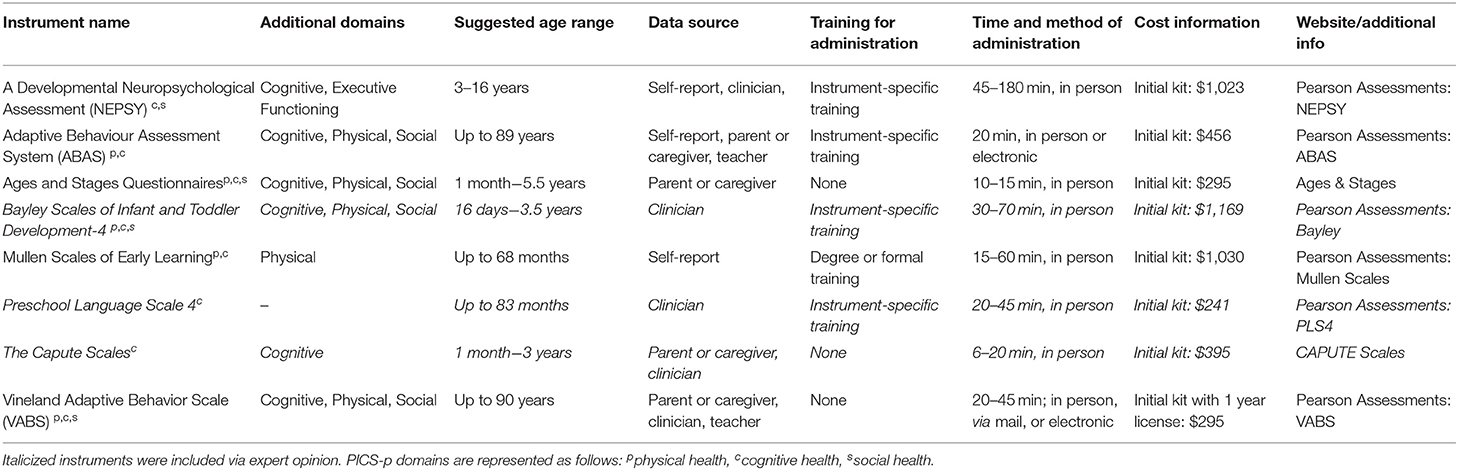
Table 2. Communication.

Table 3. Executive functioning.
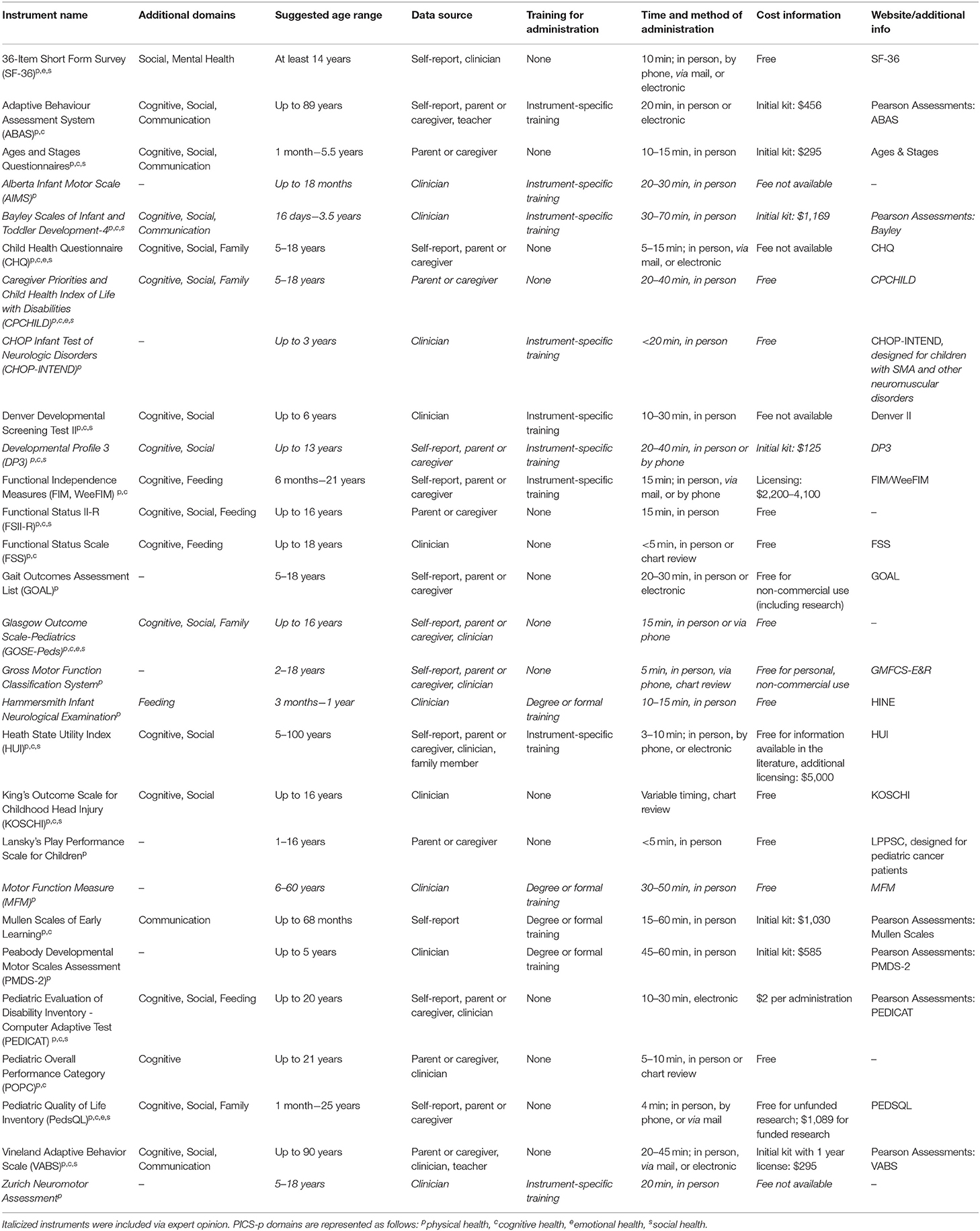
Table 4. Physical functioning.
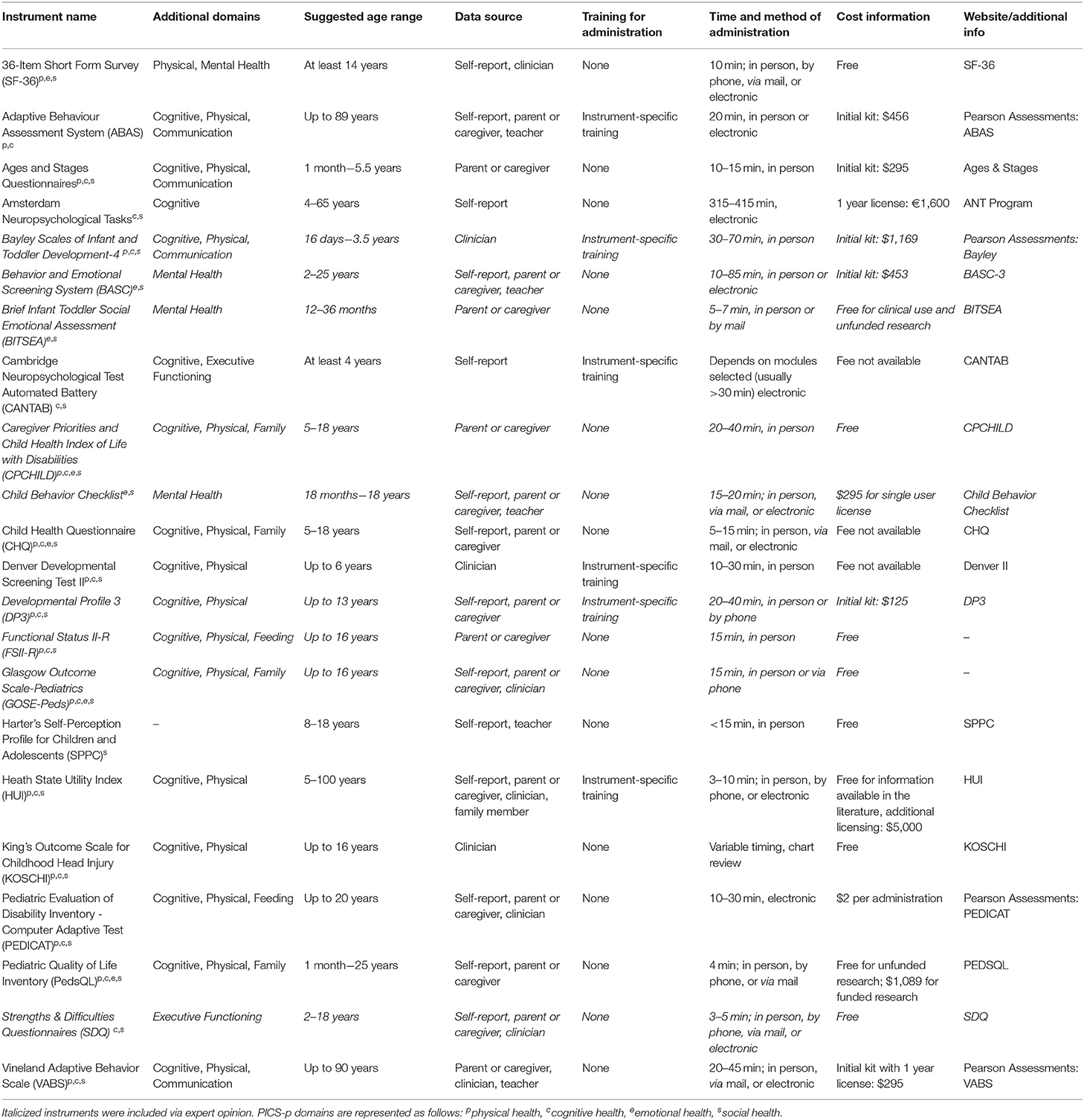
Table 5. Social skills.

Table 6. Feeding.
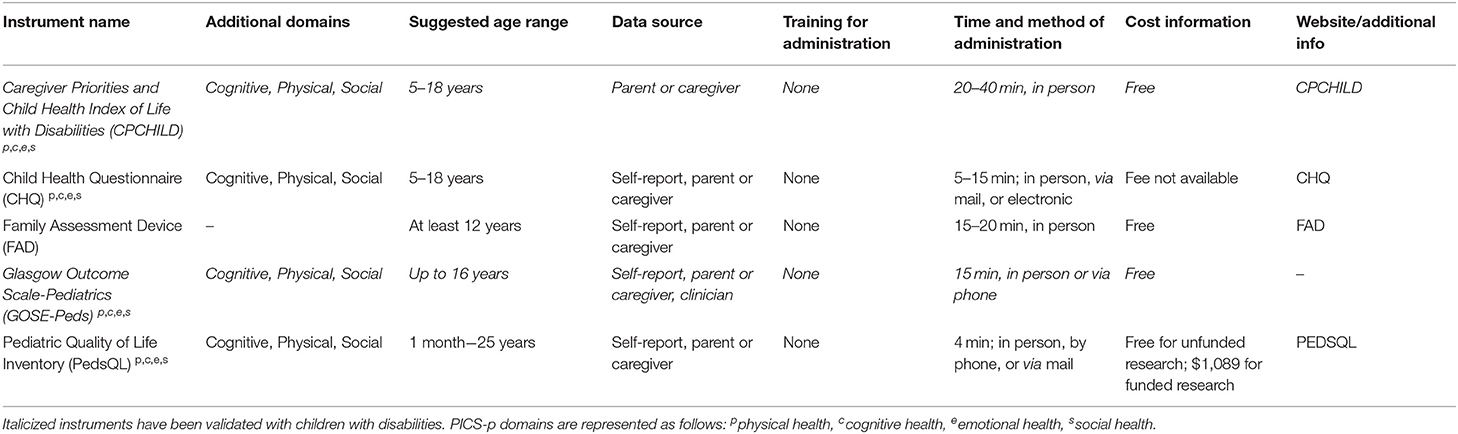
Table 7. Family functioning and child quality of life.
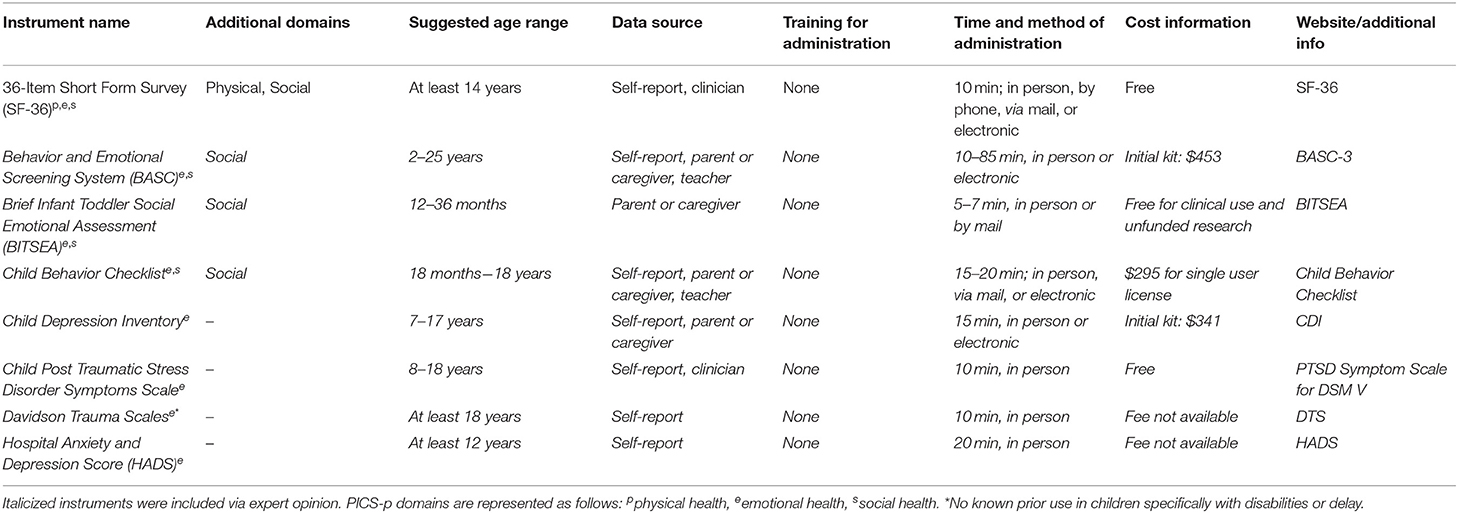
Table 8. Mental health (e.g., anxiety, depression, trauma).

Table 9. Sleep.
Despite the fact that all instruments were used in children with disabilities, only 35.3% (n = 18) had any population information available for children with specific disabilities. The instruments were most commonly used to assess children with known cognitive (n = 35, 68.6%) or physical (n = 30, 58.8%) disabilities. The domains of functioning measured by instruments included cognitive functioning (n = 25 instruments, 49.0%), executive functioning (n = 5, 9.8%), communication (n = 8, 15.7%), physical functioning (n = 28, 54.9%), social skills (n = 22, 43.1%), feeding (n = 5, 9.8%), family functioning and child quality of life (n = 5, 9.8%), mental health (including anxiety, depression, and trauma) (n = 8, 15.7%), and sleep (n = 1, 2.0%).
A minority of instruments were specifically designed for (n = 20, 39.2%) or validated in (n = 24, 47.1%) populations of children with disabilities, including cerebral palsy, intellectual disabilities, and mobility limitations. This is in contrast to the 78.4% of instruments that had normative data available for the general population. With regard to properties of administration, the targeted biological ages for each instrument were broad, often in concordance with the skills measured by each instrument, with a median minimum age of 12 months (IQR 0-60). Sixteen instruments (31.4%) started at birth, while 16 (31.4%) recommended a chronological age of at least 5 years for administration. Most instruments used in-person assessments (n = 46, 90.2%), while smaller portions used electronic (n = 14, 27.5%), mail (n = 9, 17.6%), or telephone (n = 8, 15.7%) evaluation. Parents and clinicians were the most common informants (n = 25, 49.0% of instruments each), although self-report was also common (n = 24, 47.1%). Eight instruments (15.7%) could be completed by teachers. About half of the instruments (n = 27, 52.9%) did not require special training for administration. When special training was needed for administration, it was usually instrument-specific training (n = 20, 83.3% of instruments requiring special training). Estimated time for instrument completion varied across the 45 instruments for which data were available: 10 taking <10 min, 9 taking 10–15 min, 14 taking 15–30 min, and 12 taking >30 min.
Due to the nature of their design (e.g., instruments which consist of a battery of a tests completed directly with a child rather than parent questionnaires reporting on developmental skills), it is uncommon for instruments to be able to be used retrospectively to evaluate baseline function prior to an acute illness (n = 14, 27.5%). However, most instruments can be used prospectively, either in the hospital or in an outpatient clinic setting (62.0 and 98.0%, respectively). Most of the identified instruments (n = 47, 92.2%) can be used repeatedly over time.
In terms of accessibility, almost all instruments (n = 41, 80.4%) were available in languages other than English, with 64.7% additionally available in Spanish. In addition to English, the instruments were available in a median of 4 (IQR 1-13.8) languages. Instruments were largely proprietary (n = 33, 64.7%) and required a fee for use (n = 29, 56.9%). Pricing structures varied across instruments (see Tables 1–9 for details).
Children with pre-existing disabilities represent a significant portion of admissions to the intensive care unit. Due to their neurodevelopmental vulnerabilities, they are hypothesized to be at even greater risk than typically developing children of accruing new morbidity during episodes of critical illness. Therefore, clinical providers and researchers would be remiss to not explicitly consider this patient population when evaluating outcomes following critical illness, either on an individual or population basis. This study demonstrates both the value of and the challenges inherent in applying commonly used outcome measures to populations of children with disabilities beyond those seen when assessing developmental domains more broadly. Our findings demonstrate lack of population data for children with disabilities, difficulty with validation and administration specifically related to a child's disability, and potential for instruments to suffer from scale attenuation effects, potentially hampering the research necessary to improve critical care delivery to this patient population. Ideally, instruments which are explicitly designed for children with disabilities should be prioritized for use in research when assessing this patient population, but our data suggest that such instruments are rare.
Further, our content-area experts identified a number of commonly used measures for the assessment of delay and disability which had not been identified through scoping review, likely because they have not yet (to our knowledge) been applied to the PICU survivor population. These instruments included, as examples, a number of standard assessments of emotional functioning, overall developmental assessments, specific screeners for depression and ADHD, and intellectual assessments. While some of these additions require expertise for administration, others may easily be scored and interpreted using available guides. We hope that the addition of these instruments to our review may be a resource for future researchers.
We also acknowledge and encourage the assessment of children after PICU hospitalization via interdisciplinary collaborations. Outcome measurements that coincide with outpatient needs assessment can be coupled to screen and, if indicated, direct patients to appropriate therapies and treatments. As noted below, investigators may also leverage “baseline” assessments, when batteries have been utilized for pre-PICU, school-based, or therapy evaluations. This will potentially allow investigators to determine impacts of PICU hospitalizations as well as contribute to the optimization of long-term supports.
Despite the fact that the reviewed instruments have all been used in children with disabilities, populations with heterogeneous disabilities may need nuanced accommodations, and interpretations of population means may differ substantially from normative populations. The majority of instruments (>60%) did not have population data for children with disabilities, whereas nearly 80% of the instruments had population data available for the general population. A population of children with disabilities likely will not be comparable to the general population at the time of onset of critical illness, potentially limiting our ability to effectively interpret their post-illness state. For example, children with existing severe developmental delay are known to have low health-related quality of life (HRQL) scores when examined after septic shock (19), but it is unclear if the low HRQL scores are attributable to critical illness or different norms for HRLQ in a subset of children. It is known that some populations of children with chronic medical conditions, such as cerebral palsy or chronic respiratory failure, have lower baseline HRQL scores than the general population, perhaps due to the heavy representation of physical functioning in many HRQL scores (20–22). Therefore, we would recommend that researchers consider testing that can capture pre-critical illness functioning through retrospective reporting or by aligning with outpatient providers in order to use a change from baseline as a measure of impact.
Researchers should understand that while the stated administration ages for these instruments were generally within the pediatric age range, children with disabilities may not be best assessed by an instrument designed or validated in children with typical development, particularly if participation in an instrument involves a domain of comparative weakness (e.g., verbal responses required for a child without expressive speech or the demonstration of fine motor tasks in a child with cerebral palsy). Researchers should be particularly mindful in regards to disabilities that will require accommodation across a variety of assessment tools. For example, children with sensory impairments (e.g., vision impairment or hearing impairment) that limit ability to engage with testing materials or social impairments (e.g., autism spectrum disorder) that limit ability for social response to the examiner may be inappropriately interpreted if examiners do not select or modify an instrument to account for these impairments. In the assessment of intelligence, instead of using the Wechsler Intelligence Scale for Children (WISC-IV), non-verbal children may benefit from non-verbal tests of intelligence, e.g., the Snijders-Oomen Non-verbal Intelligence Tests (23) or the Leiter Scales (24). Additionally, researchers should be mindful that the reported time for administration of these instruments may be extended in situations where children or family members need accommodations for the tool. While ease of instrument administration is an important consideration for any patient or caregiver, it is especially key for families who may already be balancing care for medically fragile children and transporting them to appointments with assistive devices. It is also possible that some measures of neurodevelopmental, psychological, or child functioning may be re-contextualized for the measurement of post-PICU impacts in children with disabilities. For example, children may display hyperactivity or inattention in response to trauma exposure, which may be measured with tools used to diagnose and follow ADHD symptoms.
The risk for scale attenuation exists when instruments designed for typically developing children are used for children with disabilities. These instruments may not be sensitive in detecting deterioration for children whose baseline scores are significantly above or below (depending on instrument scoring) population norms. Additional difficulty exists in detecting changes with instruments whose design precludes evaluating baseline function retrospectively. An example of this would be an instrument that consists of a battery of tests for the patient rather than a questionnaire that a caregiver could fill out via recall at the time of PICU admission.
Researchers should prioritize instruments that allow for longitudinal assessment with the potential for retrospective data collection and the ability to endure retest scenarios to allow for establishment of the trajectory of recovery or decline after critical illness.
Although the larger critical care community also struggles with the challenges of obtaining pre-illness and longitudinal outcomes, this may be particularly true in children with disabilities. Many children with pre-existing disabilities appear to have functional or developmental declines from their pre-illness status following critical illness, concerning for development of a “new baseline” health status. However, this may instead reflect a slower recovery trajectory and long-term monitoring may provide insight into how support services can most appropriately be structured for this population. This is particularly important in a patient population that is vulnerable to recurrent need for hospitalization and the risk of cumulative morbidities. Investigators, however, should appreciate the potential advantage of studying post-PICU outcomes in patients with disabilities. Some children will have undergone community-based neurodevelopmental testing for the provision of educational and therapy services prior to an acute illness. This potentially creates a fortuitous opportunity to compare to a “true baseline” as well as collaborate with longitudinal providers. This is particularly important as assessment during acute illness is not likely to accurately reflect a child's optimal performance, whether they have underlying disabilities or not.
This study is limited by the fact that while the inclusion strategy was broad, the initial scoping review may not have adequately queried studies specifically focusing on children with disabilities, particularly when cared for in locations other than the intensive care unit. While patients with pre-existing disabilities may need a more in-depth or individualized testing battery, the scoping review largely focused on instruments used for screening a general PICU population. Additionally, we relied on manual identification of instruments used in this patient population, which may not have been uniformly performed by those extracting data. Some instruments which may be standardly used in educational or neurodevelopmental settings to evaluate functioning in diverse pediatric cohorts may not yet have been used frequently in the PICU population. Finally, the population of children with disabilities is in and of itself heterogeneous, making generalization more challenging. However, we attempted to balance these limitations through the inclusion of specific content area experts in development and behavioral pediatrics, pediatric rehabilitation medicine, and pediatric physical therapy, in addition to inclusion of instruments at the suggestion of the remainder of the authors.
Although this work is accompanied by a parallel development of a core outcome set, which included the participation of family members in its Delphi process, we did not specifically examine the outcome domains of families of children with disabilities. However, the literature identifies themes of child physical functioning, quality of life, and feeding/swallowing as important (25, 26). Many of the instruments presented in this manuscript address the identified child-focused outcome domains. However, they do not fully explore important outcomes such as care coordination, satisfaction with care, family finances, or parental outcomes. These are areas for potential further instrument development to ensure meaningful attention to patient- and family-centered outcomes whether children have disabilities or not, and we would encourage consideration of parent/family assessment of instrument utility in the development process. Additionally, little is known about how results of these instruments may be used to trigger educational or other forms of child or family support services. Ideally, these instruments would serve a dual purpose of allowing for monitoring of a patient's recovery from critical illness while also directing access to supportive and rehabilitative services.
In sum, our current ability to measure long-term outcomes for children with disabilities who experience critical illness is complicated by instruments which do not allow comparison to pre-PICU baseline and disability-specific administration concerns. Development of measures that are specifically designed for this population is important in an era where these children increasingly experience critical illness and repeated PICU admissions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
JAH and RJG conceived of and designed the project. JAH, SAS, and RJG drafted the manuscript and analyzed and interpreted data. All authors participated in data collection and critical revision of the article and approved the final version of the manuscript.
Institutional support was provided from the University of Minnesota Clinical and Translational Science Institute (UL1TR002494 from the National Institutes of Health's National Center for Advancing Translational Sciences).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We acknowledge Daniel Notterman, MD (Princeton University); J. Michael Dean, MD (University of Utah); Joseph A. Carcillo, MD (UPMC Children's Hospital of Pittsburgh); Robert A. Berg, MD (Children's Hospital of Philadelphia); Athena Zuppa, MD (Children's Hospital of Philadelphia); Murray M. Pollack, MD (Children's National Hospital); Kathleen L. Meert, MD (Children's Hospital of Michigan); Mark W. Hall, MD (Nationwide Children's Hospital); Anil Sapru, MD (Mattel Children's Hospital, University of California Los Angeles); Patrick S. McQuillen, MD (Benioff Children's Hospital, University of California); Peter M. Mourani, MD (Children's Hospital Colorado, University of Colorado); David Wessel, MD (Children's National Hospital); Samuel Sorenson, BS (University of Utah); Lenora Olson, PhD (University of Utah) of the PICU-COS Investigators of the Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network and Tammara L. Jenkins, MSN, RN, PCNS-BC, FCCM (Program Officer, Pediatric Trauma and Critical Illness Branch) and Robert Tamburro, MD, MSc (Medical Officer, Pediatric Trauma and Critical Illness Branch) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. We additionally acknowledge the work of the PALISI POST-PICU Scoping Review Investigators (Supplementary Table 1). More information about the PICU COS and associated tools can be found at: https://www.cpccrn.org/network-projects/network-projects-picucoscoreoutcome-set/.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2021.689485/full#supplementary-material
1. Manning JC, Pinto NP, Rennick JE, Colville G, Curley MAQ. Conceptualizing post intensive care syndrome in children-the PICS-p framework. Pediatr Crit Care Med. (2018) 19:298–300. doi: 10.1097/PCC.0000000000001476
2. Feldman HM, Ploof DL, Hofkosh D, Goehring EL Jr. Developmental needs of infants and toddlers who require lengthy hospitalization. Am J Dis Child. (1993) 147:211–5. doi: 10.1001/archpedi.1993.02160260101034
3. Petersen MC, Kube DA, Whitaker TM, Graff JC, Palmer FB. Prevalence of developmental and behavioral disorders in a pediatric hospital. Pediatrics. (2009) 123:e490–5. doi: 10.1542/peds.2008-2750
4. Sobotka SA, Peters S, Pinto NP. Neurodevelopmental disorders in the PICU population. Clin Pediatr. (2018) 57:913–9. doi: 10.1177/0009922817737080
5. Heneghan JA, Reeder RW, Dean JM, Meert KL, Berg RA, Carcillo J, et al. Characteristics and outcomes of critical illness in children with feeding and respiratory technology dependence. Pediatr Crit Care Med. (2019) 20:417–25. doi: 10.1097/PCC.0000000000001868
6. Edwards JD, Houtrow AJ, Vasilevskis EE, Rehm RS, Markovitz BP, Graham RJ, et al. Chronic conditions among children admitted to U.S. pediatric intensive care units: their prevalence and impact on risk for mortality and prolonged length of stay. Crit Care Med. (2012) 40:2196–203. doi: 10.1097/CCM.0b013e31824e68cf
7. O'Brien S, Nadel S, Almossawi O, Inwald DP. The impact of chronic health conditions on length of stay and mortality in a general PICU. Pediatr Crit Care Med. (2017) 18:1–7. doi: 10.1097/PCC.0000000000000976
8. Chan T, Rodean J, Richardson T, Farris RW, Bratton SL, Di Gennaro JL, et al. Pediatric critical care resource use by children with medical complexity. J Pediatr. (2016) 177:197–203.e1. doi: 10.1016/j.jpeds.2016.06.035
9. Kane JM, Hall M, Cecil C, Montgomery VL, Rakes LC, Rogerson C, et al. Resources and costs associated with repeated admissions to PICUs. Crit Care Explor. (2021) 3:e0347. doi: 10.1097/CCE.0000000000000347
10. Maddux AB, Pinto N, Fink EL, Hartman ME, Nett S, Biagas K, et al. Postdischarge outcome domains in pediatric critical care and the instruments used to evaluate them: a scoping review. Crit Care Med. (2020) 48:e1313–21. doi: 10.1097/CCM.0000000000004595
11. Fink EL, Maddux AB, Pinto N, Sorenson S, Notterman D, Dean JM, et al. A core outcome set for pediatric critical care. Crit Care Med. (2020) 48:1819–28. doi: 10.1097/CCM.0000000000004660
12. Newacheck PW, Strickland B, Shonkoff JP, Perrin JM, McPherson M, McManus M, et al. An epidemiologic profile of children with special health care needs. Pediatrics. (1998) 102 (1 Pt 1):117–23. doi: 10.1542/peds.102.1.117
13. Bethell CD, Blumberg SJ, Stein RE, Strickland B, Robertson J, Newacheck PW. Taking stock of the CSHCN screener: a review of common questions and current reflections. Acad Pediatr. (2015) 15:165–76. doi: 10.1016/j.acap.2014.10.003
14. Feudtner C, Feinstein JA, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr. (2014) 14:199. Published 2014 Aug 8. doi: 10.1186/1471-2431-14-199
15. Simon TD, Haaland W, Hawley K, Lambka K, Mangione-Smith R. Development and validation of the pediatric medical complexity algorithm (PMCA) version 3.0. Acad Pediatr. (2018) 18:577–80. doi: 10.1016/j.acap.2018.02.010
16. Shapiro MC, Henderson CM, Hutton N, Boss RD. Defining pediatric chronic critical illness for clinical care, research, and policy. Hosp Pediatr. (2017) 7:236–44. doi: 10.1542/hpeds.2016-0107
17. Cohen E, Kuo DZ, Agrawal R, Berry JG, Bhagat SK, Simon TD, et al. Children with medical complexity: an emerging population for clinical and research initiatives. Pediatrics. (2011) 127:529–38. doi: 10.1542/peds.2010-0910
18. Hagerman TK, Houtrow AJ. Variability in prevalence estimates of disability among children in the national survey of children's health. JAMA Pediatr. (2021) 175:307–10. doi: 10.1001/jamapediatrics.2020.5073
19. Meert KL, Reeder RW, Maddux AB, Banks R, Berg RA, Newth CJ, et al. Health-related quality of life after community-acquired septic shock in children with preexisting severe developmental disabilities. Pediatr Crit Care Med. (2020) 22:e302–13. doi: 10.1097/PCC.0000000000002374
20. Varni JW, Limbers CA, Burwinkle TM. Impaired health-related quality of life in children and adolescents with chronic conditions: a comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the PedsQL 4.0 generic core scales. Health Qual Life Outcomes. (2007) 5:43. doi: 10.1186/1477-7525-5-43
21. Graham RJ, Rodday AM, Parsons SK. Family-centered assessment and function for children with chronic mechanical respiratory support. J Pediatr Health Care. (2014) 28:295–304. doi: 10.1016/j.pedhc.2013.06.006
22. Rodday AM, Graham RJ, Weidner RA, Terrin N, Leslie LK, Parsons SK. Predicting health care utilization for children with respiratory insufficiency using parent-proxy ratings of children's health-related quality of life. J Pediatr Health Care. (2017) 31:654–62. doi: 10.1016/j.pedhc.2017.04.021
23. Jenkinson J, Roberts S, Dennehy S, Tellegen P. Validation of the Snijders-Oomen nonverbal intelligence test - revised 2½-7 for Australian children with disabilities. J Psychoeduc Assess. (1996) 14:276–86. doi: 10.1177/073428299601400307
24. Ratcliffe KJ, Ratcliffe MW. The Leiter scales: a review of validity findings. Am Ann Deaf. (1979) 124:38–45.
25. Fayed N, Guttmann A, Chiu A, Gardecki M, Orkin J, Hamid JS, et al. Family-provider consensus outcomes for children with medical complexity. Dev Med Child Neurol. (2019) 61:1093–100. doi: 10.1111/dmcn.14110
Keywords: intensive care, pediatrics, disabilities, children with medical complexity, outcomes
Citation: Heneghan JA, Sobotka SA, Hallman M, Pinto N, Killien EY, Palumbo K, Murphy Salem S, Mann K, Smith B, Steuart R, Akande M and Graham RJ (2021) Outcome Measures Following Critical Illness in Children With Disabilities: A Scoping Review. Front. Pediatr. 9:689485. doi: 10.3389/fped.2021.689485
Received: 01 April 2021; Accepted: 08 June 2021;
Published: 02 July 2021.
Edited by:
Courtney Rowan, Indiana University, United StatesReviewed by:
Ali Ertug Arslankoylu, Mersin University, TurkeyCopyright © 2021 Heneghan, Sobotka, Hallman, Pinto, Killien, Palumbo, Murphy Salem, Mann, Smith, Steuart, Akande and Graham. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia A. Heneghan, aGVuZWcwMTNAdW1uLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.