
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pediatr., 27 July 2021
Sec. Pediatric Immunology
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.666423
This article is part of the Research TopicDietary Interventions and Nutritional Factors in the Prevention of Allergic Diseases in InfantsView all 16 articles
 Francesco Savino1*
Francesco Savino1* Francesco Pellegrino2
Francesco Pellegrino2 Valentina Daprà3
Valentina Daprà3 Cristina Calvi3Carla Alliaudi3Paola Montanari3Ilaria Galliano3
Cristina Calvi3Carla Alliaudi3Paola Montanari3Ilaria Galliano3 Massimiliano Bergallo3
Massimiliano Bergallo3Background: Recurrent wheezing is a common clinical manifestation in childhood, and respiratory syncytial virus infection is a well-known risk factor. However, the genetic background favoring the development of recurrent wheezing is not fully understood. A possible role of macrophage receptor with collagenous gene (MARCO) polymorphism has been recently proposed.
Objective: To investigate a correlation between MARCO rs1318645 polymorphisms and susceptibility to recurrent wheezing during childhood.
Methods: We prospectively recruited 116 infants, of which 58 with respiratory syncytial virus bronchiolitis and 58 controls hospitalized at Regina Margherita Children's Hospital, Turin, Italy, between November 2014 and April 2015. All subjects were investigated for MARCO rs1318645 polymorphisms in the first period of life. Genotyping of rs1318645 was carried out by TaqMan mismatch amplification mutation assay real-time polymerase chain reaction procedure. Subjects were then enrolled in a 5-year follow-up study to monitor the occurrence of wheezing and respiratory infections.
Results: The analysis of MARCO rs1318645 of allelic frequencies shows an increasingly significant risk to develop recurrent infection (p = 0.00065) and recurrent wheezing (p = 0.000084) with a wild-type C allele compared with a G allele. No correlation was found between wheezing and past respiratory syncytial virus infection (p = 0.057) and for a history of atopy in the family (p = 0.859).
Conclusion: Our finding showed that subjects with C allelic MARCO rs1318645 polymorphism are at higher risk for recurrent infection and wheezing episodes during the first 5 years of life. Future studies of genetic associations should also consider other types of polymorphisms.
Recurrent wheezing and consequently associated asthma are common respiratory disorders during childhood. A rise in prevalence and severity has been observed in recent years, contributing to increased health system costs (1). Historically, respiratory syncytial virus (RSV) has long been considered the most common trigger of recurrent wheezing (2), particularly in preterm infants (3). A recent meta-analysis performed by Liu et al. (4) also suggests an association between early life rhinovirus infections and the subsequent development of wheezing and asthma.
The variation in response to RSV infection suggests that host intrinsic factors influence susceptibility mechanisms and severity of symptoms. Recently, candidate gene single-nucleotide polymorphisms (SNPs) have been associated with RSV disease severity in infants (5).
We recognized macrophage receptor with collagenous structure (MARCO), an innate immunity scavenger receptor, as a possible gene candidate to RSV disease susceptibility. In the MARCO promoter, we identify a polymorphic region, the SNP rs1318645, −156 C/G (C is the wild type), which influences the transcriptional activity of the gene.
MARCO is a class A scavenger receptor, expressed on macrophages membrane, where it recognizes pathogen-associated molecular patterns and environmental or un-opsonized particles. Studies have demonstrated that MARCO and other scavenger receptors decrease the proinflammatory environment in infections, mediating the clearance of lung pathogens (6).
MARCO promoter contains a polymorphic region that, when deleted, reduced transcriptional activity. In enrolled children, we study SNPs rs1318645. The mutation from C (wild type) to G at the −156 sites has been associated with a deletion of an antioxidant response element of the MARCO promoter. That is a binding site for a transcription factor named “nuclear factor erythroid-derived 2-like 2,” also known as NRF2.
TaqMan mismatch amplification mutation assay (TaqMAMA) combines the quantitative strengths of TaqMan with the allele-specific polymerase chain reaction (PCR) of mismatch amplification mutation assay (MAMA). This technique is used for screening human DNA samples for known genetic polymorphisms and may be suitable for broad and cost-effective genotyping applications in all types of laboratories.
Using the MARCO rs1318645 TaqMAMA-specific real-time PCR (7), the outcome of this study is to determine a correlation between MARCO rs1318645 SNP and incidence of bronchiolitis, RSV susceptibility. Consequently, as respiratory infections during infancy, especially by RSV, constitute a significant risk factor for the development of recurrent wheezing and asthma in childhood (8), with a 5-year follow-up, we tried to verify the potential correlation of MARCO rs1318645 SNP and the onset of recurrent infection and wheezing during childhood.
This case–control study was conducted in Turin Children Hospital Regina Margherita, Italy, between November 2014, April 2015, and December 2020. Study participants were full-term infants with age younger than 12 months. In the control group, we enrolled at term infants, adequate for gestational age (birth weight: 2,500–4,000 g), exclusively or predominant breast milk feeding, who were visited during outpatient control (follow-up visit and routine check) in our Department of Pediatrics at Regina Margherita Children Hospital, Turin, Italy. In the case group, we enrolled infants with a diagnosis of bronchiolitis made by trained pediatricians, hospitalized, and clinically monitored every day.
The parents of the enrolled infants were informed about the purpose, benefits, and possible risks of the study, and written informed consent was obtained. Exclusion criteria included known or suspected impairment of immunological function, major known congenital airway malformations, chronic lung disease, cardiac disease, prematurity (gestational age younger than 37 weeks), neuromuscular disorders affecting swallowing, and known or suspected coagulation disorders or bleeding tendency. Baseline population characteristics (age, sex, breastfeeding history, smoke exposition, family history of atopy, like atopic dermatitis, recurrent wheezing, asthma, and food allergy) reported by parents were collected by investigators. A pediatrician investigator monitored the clinical evolution of the participants by visiting them 5 years after enrollment.
The parents of the enrolled infants were informed about the purpose of the study to obtain written consent, and a standardized questionnaire was administered to investigate the onset of symptoms associated with recurrent wheezing and history of recurrent infections. The pediatrician investigators also asked for information about the development of allergic symptoms, discovering of food allergy, or execution of allergy test (e.g., Patch test or Prick test). The data reported by parents were collected and classified in the previous database.
The study was conducted in accordance with the International Council for Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use guidelines protocol, applicable regulations and guidelines governing clinical study conduct, and the ethical principles that have their origin in the Declaration of Helsinki1.
A MARCO rs1318645 SNP (GenBank access number NT_005403.18)2 on chromosome 2 showing a C/G transition in position 24445994 was chosen.
Infants were subjected to a venous blood sample from 7:30 to 8:30 AM during the routine clinical blood sampling to reduce the stress of infants.
Genomic DNA was extracted from blood using the Maxwell16 LEV Blood DNA kit with automatic extractor Maxwell16 System (Promega, Madison, Wisconsin, USA) following the manufacturer's instructions.
Genotyping of rs1318645 was carried out by TaqMAMA real-time PCR procedure (MARCO rs1318645 cod. PP-036) (BioMole, Turin, Italy) (7).
The work described was carried out in accordance with the code of ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans1.
MAMA allele-specific forward primers were designed. The last nucleotide at 3′ region gives the specificity of the primers. An additional deliberate mismatch in the third last from the 3′ end improves the specificity of MAMA primers. The established assays use the same probe and reverse primer and probe mix PP-036 (BioMole, Turin, Italy). The Probe is a TaqMan labeled at the 5′ end with 6-carboxyfluorescein and at the 3′ with 5-carboxytetramethylrhodamine.
PCR was set up in a volume of 20 μl, containing 5 μl of DNA and 15 μl of reaction mix (PP-036, BioMole, Turin, Italy). Assays were performed with 7500 Real-Time PCR System (Thermo Fisher Scientific, Waltham, Massachusetts, USA), following the standard Life Technologies profiles and subsequently analyzed using ABI Prism 7500 SDS software version 2.0 (Life Technologies, Thermo Fisher Scientific, Waltham, Massachusetts, USA).
For statistical analysis, the chi-square test was performed using commercial software (GraphPad Prism 5 San Diego, California, USA); a p < 0.05 was considered statistically significant. The P-value was calculated for each allele in the control group and in patients with recurrent infections and wheezing. A P-value of <0.05 was considered significant with 95% confidence intervals.
A total of 116 infants were enrolled. According to the criteria described in section Materials and Methods, 58 infants with bronchiolitis were identified in the case group and tested for MARCO. Bronchiolitis group includes 29 (50%) male patients and 29 (50%) female patients as shown in Figure 1.

Figure 1. Enrollment process and follow-up.
Fifty-eight children were enrolled in the control group, including 30 (51.7%) male patients and 28 (48.3%) female patients, at term, adequate for gestational age (birth weight: 2,500–4,000 g), exclusively or predominant breast milk feeding.
As shown in Table 1, both groups were similar (p > 0.05 indicates that no statistical effect was observed) for age at enrollment, sex, and type of feeding (breastfeeding). The mean duration of hospitalization in the bronchiolitis group was 6.87 days (range 5–21).
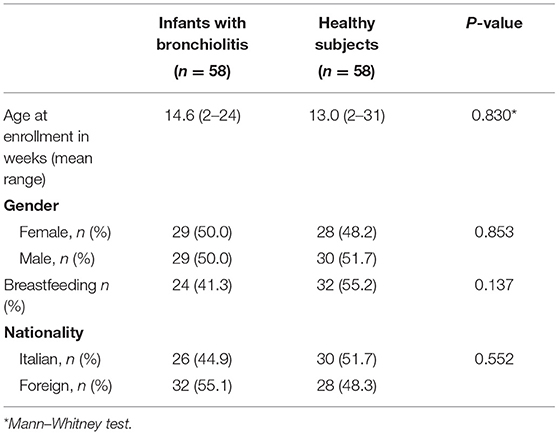
Table 1. Epidemiological characteristics of enrolled subjects.
In the bronchiolitis group, we executed nasopharyngeal swabs for respiratory viruses. We study RSV susceptibility in 53 (91.4%) infants with bronchiolitis. A total of 27 (51%) tested positive for RSV. Five of 27 were also positive in nasopharyngeal pathogen detection for other viruses (rhinovirus and coronavirus NL63).
Infants with RSV-positive bronchiolitis (51%) and RSV-negative bronchiolitis (49%) have shown the same allelic and genotype frequencies: χ2 analysis of genotypes (p = 0.373) and allelic (p = 0.250); frequencies showed no association between MARCO rs1318645 and RSV susceptibility.
In bronchiolitis cohort follow-up, we contacted families of bronchiolitis-group infants to organize a visit to our hospital. A team of pediatricians performed a medical examination of enrolled children and interviewed parents using a structured questionnaire.
The follow-up aimed to verify the possible association between MARCO rs1318645 SNP and the onset of recurrent respiratory infections, defined as one or more admissions to the pediatric emergency department for acute respiratory symptoms or three or more visits to general pediatricians for clinical respiratory infections and/or the development of recurrent wheezing [three or more episodes, which requires one or more accesses to the pediatric emergency department or pneumology or allergology specialistic visit and leading to bronchodilator drug (β2 agonist) or inhaled corticosteroids prescription].
Families who referred a history of recurrent wheezing focused on the necessity to access to the emergency department or consult an allergology or pneumology specialist and leading to bronchodilator drug (β2 agonist) or inhaled corticosteroids prescription.
We asked parents about smoke exposition and the development of airway malformations. We excluded two infants who developed airway complex chirurgical conditions. We correctly reenrolled 47 patients, in which we researched family history of atopy (atopic dermatitis, recurrent wheezing, history of asthma, and food allergy in parents).
A total of 19 (40.4%) infants were exposed to passive smoke during infancy. Eleven (57.9%) of these smoke-exposed children developed recurrent airway infections, but also 15 (54%) of 28 nonexposed children developed recurrent respiratory infections. No correlation between cigarette smoke exposition and recurrent infections resulted.
Nine (47.4%) of smoke-exposed children and 15 (54%) of nonexposed children developed recurrent wheezing. No correlation between cigarette smoke exposition and recurrent infections (p-value 0.770) or wheezing (p-value 0.676) resulted.
Nineteen children (40.4%) referred a history of atopy in their family (e.g., atopic dermatitis, recurrent wheezing, history of asthma, and food allergy). A total of 12 (63.2%) of these presented recurrent infections (p-value 0.373) and 10 (52.6%) referred recurrent wheezing (p-value 0.859).
Twenty-four children with past RSV-positive tampons were correctly enrolled in the follow-up. A total of 15 (62.5%) children referred recurrent airway infection, and the same number referred recurrent wheezing. No correlation between RSV infection during infancy and recurrent infections (p-value 0.191) or wheezing (p-value 0.057) resulted.
We defined recurrent infections as one or more admissions to the pediatric emergency department for acute respiratory symptoms or three or more visits to general pediatricians for the same symptoms. Allelic and genotype frequencies in an infant with recurrent infections are shown in Table 2. The analysis of allelic frequencies shows a significant risk of C allele to develop recurrent infection compared with G (p-value = 0.001).
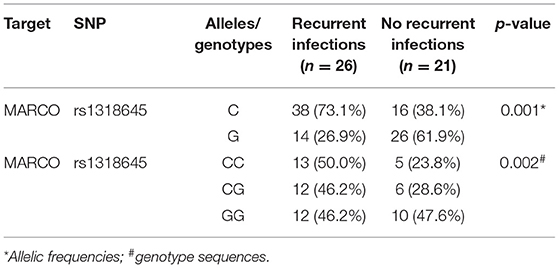
Table 2. MARCO rs1318645 and recurrent airway infections susceptibility.
We define recurrent wheezing as three or more episodes that require one or more access to the pediatric emergency department or pneumology or allergology specialistic visit and leading to bronchodilator drug (β2 agonist) or inhaled corticosteroids prescription. Allelic and genotype frequencies in an infant with recurrent wheezing are shown in Table 3. The analysis of allelic frequencies shows a significant risk of C allele to develop recurrent wheezing episodes compared with G (p-value = 0.001). χ2 analysis of genotypes frequencies are significant (p-value = 0.002).
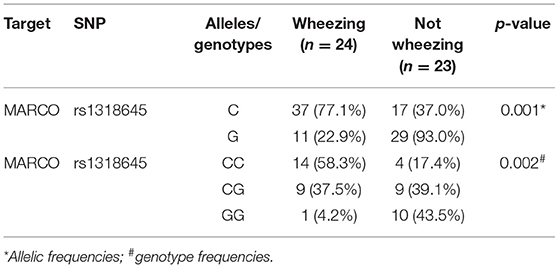
Table 3. MARCO rs1318645 and recurrent wheezing during childhood.
Respiratory viruses are one of the causes of early life wheezing that may contribute to the development of childhood asthma. Several epidemiological studies reported that respiratory virus-associated wheezing during early life, particularly during infancy, contributes to the development of asthma during childhood (9–12).
Growing data have associated specific SNPs in several immune-related genes with altered susceptibility to infectious diseases, but despite their potential role, there are few data about SNPs associated with RSV and other respiratory infections; a systematic literature review has been performed by Drysdale et al. (13).
SNPs in genes coding for interleukin (IL)-8, IL-19, IL-20, IL-13 mannose-binding lectin, interferon-gamma, and a regulated on activation, normal T cell expressed and secreted polymorphism have been associated with subsequent wheeze after RSV lower respiratory tract infection in term-born infants (14). Utilizing the inpatient database of severe RSV infection or without, we compared MARCO rs1318645 [GenBank access number NT_005403.182] polymorphism and risk of recurrent wheezing or recurrent airway infections during childhood. Our finding allowed us to identify a biologically plausible bronchiolitis susceptibility gene candidate: MARCO. Unexpectedly, we identified the wild-type C allele frequency as an increased risk of recurrent infection and wheezing incidence in an infant. We did not show genotypic or allelic different susceptibility in bronchiolitis RSV positive vs. RSV negative, and, in contrast to what High et al. (15) reported, this research did not find evidence supporting a causative role of C/C genotype o G allele for RSV disease severity. In fact, they determined that G allele and G/G genotypes were more likely to have severe RSV disease than children who were heterozygous or wild type for the C allele, showing a missense loss of function polymorphism in the human MARCO homolog associated with severe RSV disease in two populations of infected infants (15). Demonstrating a correlation between the wild-type C allele and increased susceptibility to bronchiolitis, we can speculate an important role of MARCO in the pathogenesis of airway infection, but our results about RSV disease severity differ from those of High et al. suggesting that the C allele increases the risk of bronchiolitis but in a mild presentation, whereas G allele is associated with severe clinical form of the disease. The precise role of MARCO is still not clear in our study, as well as the utility of more studies for understanding human RSV disease.
Although RSV infection is very common, a minority of infected children develop wheezing during childhood. The genetic factors that increase the risk of wheezing have not been clarified yet.
Respiratory viruses replicate in cells, damaging airway epithelium that is a chemical, physical, and immunological barrier. They cause loss of cilia, decreasing mucociliary clearance and promoting the sensibilization to allergens and environmental irritants. Causing sustained airway inflammation, recurrent infections of the respiratory tract play a major role in the pathogenesis of wheezing (16), and one wheezing episode or more during the first years of life are confirmed risk factors for the development of asthma (2, 17, 18).
Also, the atopic clinical history and the early-life wheezing episodes synergistically contribute to asthma pathogenesis (19, 20).
We hypothesize the immune system impairment on the epithelial barrier, in which MARCO is involved, predisposing to respiratory tract infections and recurrent wheezing in the first years of life. For this reason, we established a follow-up of children affected by bronchiolitis to study wheezing development as a risk of future asthma. As shown in our results, we identified the wild-type C allele frequency and C/C genotypes as increased risk of recurrent infections and wheezing 5 years after the bronchiolitis episode rather than the G allele. This confirms that, unexpectedly, the wild-type allele in SNP rs1318645 is correlated with an increased susceptibility to respiratory sequelae of bronchiolitis. We also observed a trend in our results that describe a major susceptibility to recurrent wheezing in children with previous RSV + bronchiolitis. This is confirmed by literature from years (21), although the link between RSV infection and the development of wheezing is still partially unclear. At the basis of this phenomenon, it would seem to be involved not only in the remodeling of the respiratory tract after the inflammatory process. For this reason, researchers are focusing on SNPs, speculating about their genetic predisposition to atopy, wheezing, and asthma. For example, SNPs s8076131, rs12603332, and rs3744246 of gene ORMDL3, which has been reported to be involved in the lung epithelial defense pathway, have been associated with the development of asthma such as GSDMB SNPs rs7216389 (22, 23). Also, the SNPs rs1889570 (C/T), IL-17A rs4711998 (A/G), and IL-17A rs3819024 (A/G) of THE IL17F gene have recently emerged as associated with more post- bronchiolitis asthma development (24). ILs are also associated with allergic sensibilization, such as polymorphisms of the genes that code for IL-4 and IL-13 (25–27), such as a correlation between toll-like receptor 9 rs187084 gene polymorphism and wheezing has been described (28). From our study, apparently, the genetic predisposition seems to affect the airway infection susceptibility and the recurrent wheezing more than the previous RSV infection. As we can see, candidate gene SNPs are the vanguard for the future study of genetic contributions to complex, multifactorial diseases, specifically examining common variants and eventually making it possible to identify determinants of disease.
We admit that there are some limitations to our study. First, our research is focused on a single SNP (MARCO rs1318645 polymorphism), although nowadays, it is possible to investigate more polymorphisms, such as IL-4 rs2243250, ADRB2 rs1042713, and FCER1B rs569108 and IL-13 rs20541 (29, 30).
Besides, our methods of data collection do not include a respiratory function test, such as spirometry, to define the grade of bronchoconstriction in patients with wheezing.
A small number of subjects have been enrolled, and for this reason, it is necessary to explore the effects of other variables that might result in misleading interpretations of causality.
Nevertheless, our work remains relevant, as our findings contribute to the emerging global picture of recurrent wheezing and childhood-onset asthma and because it outlines the roots for future, more integrated studies.
In summary, we describe an association between MARCO rs1318645 polymorphisms and susceptibility to recurrent airway infection and recurrent wheezing in children, but mechanisms through which MARCO modulates the inflammatory response to RSV and the disease severity are not completely understood. As innate immunity receptors seem to play a critical role in host defense, as well as allergy, nutritional factors, and asthma, the genetic risk factors involved in susceptibility to RSV infections are needed to eventually prevent RSV disease and associated sequelae in children.
Future studies of genetic associations should consider the different wheezing phenotypes in infancy. In addition, stratified genetic analyses for subjects with atopy can be useful for elucidating the background mechanisms of recurrent wheezing.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethical approval was not provided for this study on human participants because the work described was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans, http://www.wma.net/en/20activities/10ethics/10helsinki/index.html. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
The guarantors of the study are FS and MB, from conception and design to conduct of the study and acquisition of data, data analysis, and interpretation of data. FS, FP, and MB have written the first draft of the manuscript. FP has performed follow-up, tables, and searched references. VD, CC, CA, PM, and IG have performed genetic investigations. All co-authors have provided important intellectual input and contributed considerably to the analyses and interpretation of the data. All authors guarantee that the accuracy and integrity of any part of the work have been appropriately investigated and resolved, and all have read, edited, and approved the final version of the manuscript. The corresponding author had full access to the data and had final responsibility for the decision to submit for publication. No honorarium or other forms of payment was given to any of the authors to produce this manuscript.
The partial funding was provided by the BERM_RILO_17_04 University of Turin program and research grant.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^Available online at: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/
2. ^Available online at: https://ftp.ncbi.nlm.nih.gov/genbank/
1. Asher I, Pearce N. Global burden of asthma among children. Int J Tuberc Lung Dis. (2014) 18:1269–78. doi: 10.5588/ijtld.14.0170
2. Sigurs N, Aljassim F, Kjellman B, Robinson PD, Sigurbergsson F, Bjarnason R, et al. Asthma and allergy patterns over 18 years after severe RSV bronchiolitis in the first year of life. Thorax. (2010) 65:1045–52. doi: 10.1136/thx.2009.121582
3. Scheltema NM, Nibbelke EE, Pouw J, Blanken MO, Rovers MM, Naaktgeboren CA, et al. Respiratory syncytial virus prevention and asthma in healthy preterm infants: a randomised controlled trial. Lancet Respir Med. (2018) 6:257–64. doi: 10.1016/S2213-2600(18)30055-9
4. Liu L, Pan Y, Zhu Y, Song Y, Su X, Yang L, et al. Association between rhinovirus wheezing illness and the development of childhood asthma: a meta-analysis. BMJ Open. (2017) 7:e013034. doi: 10.1136/bmjopen-2016-013034
5. Miyairi I, DeVincenzo JP. Human genetic factors and respiratory syncytial virus disease severity. Clin Microbiol Rev. (2008) 21:686–703. doi: 10.1128/CMR.00017-08
6. Zani IA, Stephen SL, Mughal NA, Russell D, Homer-Vanniasinkam S, Wheatcroft SB, et al. Scavenger receptor structure and function in health and disease. Cells. (2015) 4:178–201. doi: 10.3390/cells4020178
7. Galliano I, Dapra V, Ciferri F, Mqntanari P, Calvi C, Alliaudi C, et al. TaqMAMA assay polymerase chain reaction real time for allelic discrimination of Macrophage receptor with collagenous structure rs1318645 polymorphism. Minerva Biotecnol. (2020) 32:1–5. doi: 10.23736/S1120-4826.19.02567-9
8. O'Brien KL. To wheeze or not to wheeze: the question of RSV prevention. Lancet Respir Med. (2018) 6:232–3. doi: 10.1016/S2213-2600(18)30048-1
9. Stensballe LG, Simonsen J, Breindahl M, Winding L, Kofoed P-E. Wheeze after hospitalization for respiratory syncytial virus infection in children. J Pediatr Infect Dis. (2018) 13:046–50. doi: 10.1055/s-0037-1606565
10. Gern JE, Rosenthal LA, Sorkness RL, Lemanske RF Jr. Effects of viral respiratory infections on lung development and childhood asthma. J Allergy Clin Immunol. (2005) 115:668–74; quiz 675. doi: 10.1016/j.jaci.2005.01.057
11. Kusel MM, de Klerk NH, Kebadze T, Vohma V, Holt PG, Johnston SL, et al. Early-life respiratory viral infections, atopic sensitization, and risk of subsequent development of persistent asthma. J Allergy Clin Immunol. (2007) 119:1105–10. doi: 10.1016/j.jaci.2006.12.669
12. Nafstad P, Magnus P, Jaakkola JJ. Early respiratory infections and childhood asthma. Pediatrics. (2000) 106:E38. doi: 10.1542/peds.106.3.e38
13. Drysdale SB, Milner AD, Greenough A. Respiratory syncytial virus infection and chronic respiratory morbidity - is there a functional or genetic predisposition? Acta Paediatr. (2012) 101:1114–20. doi: 10.1111/j.1651-2227.2012.02825.x
14. Pinto LA, Stein RT, Ribeiro JD. Genetic associations with asthma and virus- induced wheezing: a systematic review. J Bras Pneumol. (2009) 35:1220–6. doi: 10.1590/S1806-37132009001200010
15. High M, Cho HY, Marzec J, Wiltshire T, Verhein KC, Caballero MT, et al. Determinants of host susceptibility to murine respiratory syncytial virus (RSV) disease identify a role for the innate immunity scavenger receptor MARCO gene in human infants. EBioMedicine. (2016) 11:73–84. doi: 10.1016/j.ebiom.2016.08.011
16. Mertsola J, Ziegler T, Ruuskanen O, Vanto T, Koivikko A, Halonen P. Recurrent wheezy bronchitis, and viral respiratory infections. Arch Dis Child. (1991) 66:124–9. doi: 10.1136/adc.66.1.124
17. Thomsen SF, van der Sluis S, Stensballe LG, Posthuma D, Skytthe A, Kyvik KO, et al. Exploring the association between severe respiratory syncytial virus infection and asthma: a registry-based twin study. Am J Respir Crit Care Med. (2009) 179:1091–7. doi: 10.1164/rccm.200809-1471OC
18. Beasley R, Semprini A, Mitchell EA. Risk factors for asthma: is prevention possible? Lancet. (2015) 386:1075–85. doi: 10.1016/S0140-6736(15)00156-7
19. Oliver BG, Robinson P, Peters M, Black J. Viral infections, and asthma: an inflammatory interface? Eur Respir J. (2014) 44:1666–81. doi: 10.1183/09031936.00047714
20. Jackson DJ, Gangnon RE, Evans MD, Roberg KA, Anderson EL, Pappas TE, et al. Wheezing rhinovirus illnesses in early life predict asthma development in high-risk children. Am J Respir Crit Care Med. (2008) 178:667–72. doi: 10.1164/rccm.200802-309OC
21. Mummidi PS, Tripathy R, Dwibedi B, Mahapatra A, Baraha S. Viral aetiology of wheezing in children under five. Indian J Med Res. (2017) 145:189–93. doi: 10.4103/ijmr.IJMR_840_15
22. James B, Milstien S, Spiegel S. ORMDL3 and allergic asthma: from physiology to pathology. J Allergy Clin Immunol. (2019) 144:634–40. doi: 10.1016/j.jaci.2019.07.023
23. Zhao CN, Fan Y, Huang JJ, Zhang HX, Gao T, Wang C, et al. The association of GSDMB and ORMDL3 gene polymorphisms with asthma: a meta-analysis. Allergy Asthma Immunol Res. (2015) 7:175–85. doi: 10.4168/aair.2015.7.2.175
24. Jin Y, Deng Z, Cao C, Li L. IL-17 polymorphisms and asthma risk: a meta-analysis of 11 single nucleotide polymorphisms. J Asthma. (2015) 52:981–8. doi: 10.3109/02770903.2015.1044251
25. Zhang JH, Zhang M, Wang YN, Zhang XY. Correlation between IL-4 and IL-13 gene polymorphisms and asthma in Uygur children in Xinjiang. Exp Ther Med. (2019) 17:1374–82. doi: 10.3892/etm.2018.7096
26. Shirking A, Mansoura A, Farid Hosseini R, Jabbari Azad F, Al-Sadat Mahmoud Ian R, Montage M, et al. The role of interleukin-4 and 13 gene polymorphisms in allergic rhinitis: a case control study. Rep Biochem Mol Biol. (2019) 8:111–8.
27. Narozna B, Hoffmann A, Sobkowiak P, Schoneich N, Breborowicz A, Szczepankiewicz A. Polymorphisms in the interleukin 4, interleukin 4 receptor and interleukin 13 genes and allergic phenotype: a case control study. Adv Med Sci. (2016) 61:40–5. doi: 10.1016/j.advms.2015.07.003
28. Nuolivirta K, Törmänen S, Teräsjärvi J, Vuononvirta J, Koponen P, Korppi M, et al. Post-bronchiolitis wheezing is associated with toll-like receptor 9 rs187084 gene polymorphism. Sci Rep. (2016) 6:31165. doi: 10.1038/srep31165
29. Hua L, Yang F, Chen Q, Liu Q, Ji R, Liu H, et al. Association of a four-gene model with allergic diseases: two-year follow-up of a birth cohort study. Immun Inflamm Dis. (2021) 9:239–45. doi: 10.1002/iid3.385
Keywords: atopy, MARCO polymorphisms, SNPs, rs1318645, recurrent wheezing
Citation: Savino F, Pellegrino F, Daprà V, Calvi C, Alliaudi C, Montanari P, Galliano I and Bergallo M (2021) Macrophage Receptor With Collagenous Structure Polymorphism and Recurrent Respiratory Infections and Wheezing During Infancy: A 5-Years Follow-Up Study. Front. Pediatr. 9:666423. doi: 10.3389/fped.2021.666423
Received: 10 February 2021; Accepted: 21 June 2021;
Published: 27 July 2021.
Edited by:
Gianvincenzo Zuccotti, University of Milan, ItalyReviewed by:
Roberto Miniero, Università Magna Grecia di Catanzaro, ItalyCopyright © 2021 Savino, Pellegrino, Daprà, Calvi, Alliaudi, Montanari, Galliano and Bergallo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Savino, ZnJhbmNlc2NvLnNhdmlub0B1bml0by5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.