 Karin Nielsen-Saines
Karin Nielsen-Saines Erica Li
Erica Li Adriana Martinez Olivera3
Adriana Martinez Olivera3 Rachel Martin-Blais
Rachel Martin-Blais Yonca Bulut
Yonca Bulut
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Pediatr., 10 February 2021
Sec. Pediatric Infectious Diseases
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.628810
During the COVID pandemic, a surge in pediatric Type 1 Diabetes Mellitus (T1DM) cases appears to be occurring, potentially due to the presence of autoantibody-induced immune dysregulation triggered by COVID-19. We describe one such case in a previously healthy 7-year-old with asymptomatic COVID-19 presenting with a high nasopharyngeal SARS CoV-2 virus load, detectable COVID-19 IgG antibodies, diabetic keto-acidosis and islet cell autoantibodies. COVID-19 is not a trivial disease in children and adolescents and can lead to lifelong sequelae such as T1DM. Raising awareness about a possible association between COVID-19 and T1DM in children is critical.
During the COVID-19 pandemic, the number of cases of T1DM in youth spiked, with evidence suggesting an association between both conditions (1, 2). Studies have long implicated viruses, particularly respiratory infections, as potential triggers of T1DM in children and young adults (3). In a large prospective pediatric study, a temporal association was noted between respiratory infections and development of autoantibodies against insulin-producing pancreatic beta islet cells (3). Following a surge in COVID-19 cases, a prospective registry demonstrated a significant increase in pediatric diabetic ketoacidosis (DKA) diagnoses (1). Between March to May 2020, 532 children in Germany were diagnosed with T1DM, with 45% presenting with DKA. The incidence of DKA in children was nearly double of that reported in the prior year (24.5%) with the risk of DKA in 2020 being 1.85 times higher than in the 2 prior years (2.75 times higher in children <6 years of age as compared to 2019) (1). In the U.K., investigators reported an 80% increase in the number of cases of T1DM in children as compared to prior years (2). The reason for higher rates of DKA in youth could be multi-factorial and related to delayed medical care (4). Findings, however, parallel what was observed in adults with COVID-19 (5).
A 7-year-old previously healthy Hispanic male with no pre-existing co-morbidities presented to the UCLA emergency department with progressive anorexia and a 10-pound weight loss over 3 weeks in August 2020. Three days prior to presentation, the patient complained of acutely worsened anorexia with polydipsia, abdominal pain, nausea, and headache (Table 1). Both the patient and his mother denied any prior or concurrent presence of fever, cough, nasal congestion, shortness of breath, diarrhea, or dysuria. There was no history of recent illnesses or sick contacts. The child lived in a multigenerational family household in south Los Angeles, including both grandparents who worked as school janitors, his mother who was studying for her degree remotely, a young adolescent cousin and a 13-year-old healthy sister. No one in the household reported recent illnesses and the family history was overall unremarkable.
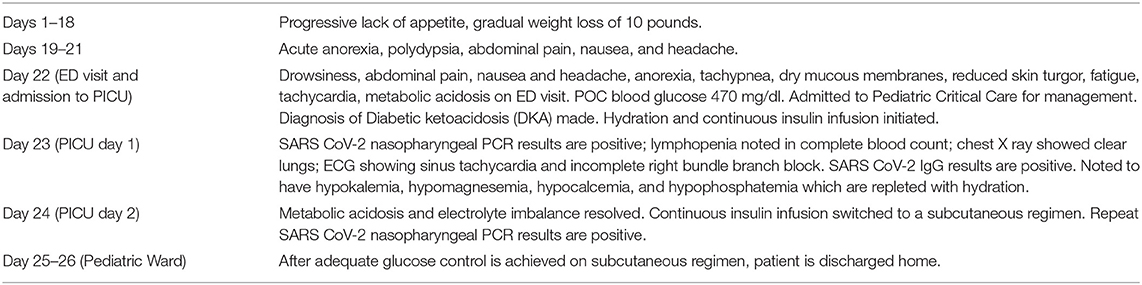
Table 1. Timeline.
In the emergency department, the patient's initial vital signs were a temperature of 36.8°C, heart rate of 131 beats per minute (BPM), blood pressure of 114/75 mmHg, respiratory rate of 37 breaths per minute and an oxygen saturation of 99% on room air. His weight was 25 kg, height 121.9 cm, and BMI was at the 75% percentile for age. On initial examination, he was drowsy but arousable. His exam was notable for dry mucous membranes, reduced skin turgor, tachypnea, clear lungs clear to auscultation, and soft, non-distended, non-tender abdomen. While he appeared fatigued, he had a non-focal neurological exam and responded appropriately to questions.
An initial point-of-care blood glucose was 470 mg/dL. A complete blood count (CBC) showed a normal white blood cell (WBC) count of 6.69 × 10 E3/uL, with an absolute neutrophil count (ANC) of 4,650 cells/uL, as well as a mild lymphopenia (1,420 lymphocytes/μL) (Table 2). The urinalysis was significant for a specific gravity of 1.024, 2+ ketones, 3+ glucose, 2+ protein. Chest X-ray did not show any pulmonary pathology. Clinical and laboratory findings were consistent with diabetic ketoacidosis (DKA). In the emergency department, the patient received a 10 mL/kg normal saline bolus and started on continuous insulin infusion. He was then transferred to the pediatric intensive care unit (PICU) for further care.
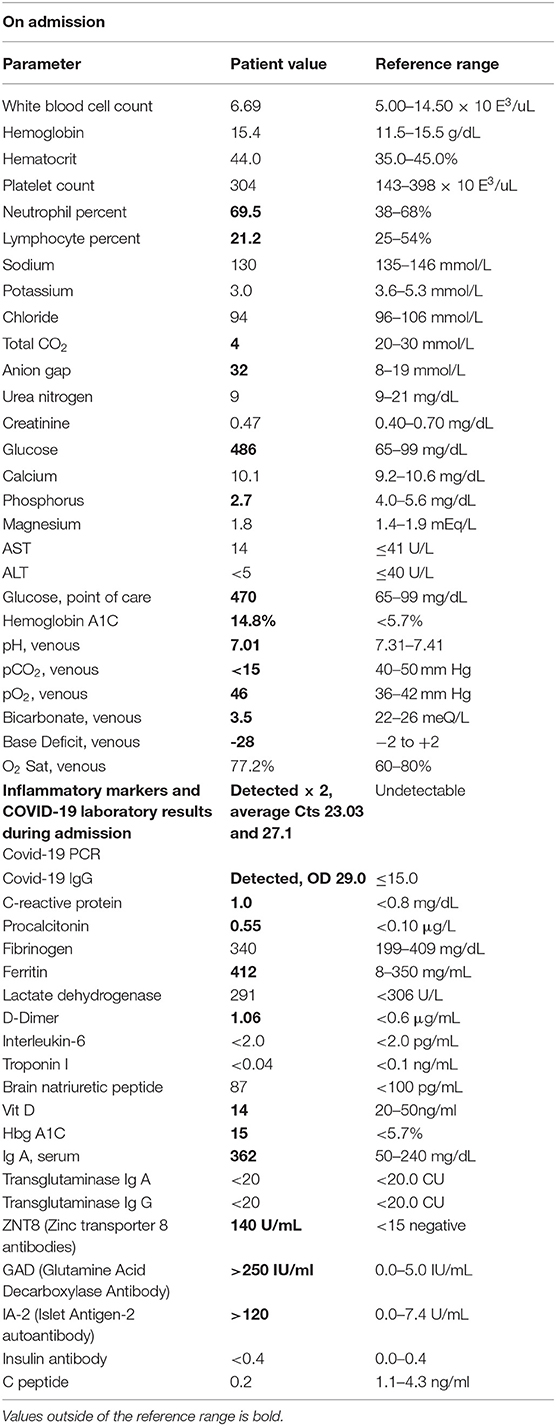
Table 2. Laboratory values on and during admission with abnormal results highlighted.
On arrival to the PICU, the patient was persistently tachycardic, with heart rates ranging from 100–140 BPM. He required a total of 40 mL/kg of normal saline fluid boluses over 24 h. An electrocardiogram was obtained, which revealed sinus tachycardia with incomplete right bundle branch block. His heart rate improved to 90–100 beats per minute over the next 2 days. A repeat CBC following hydration 24 h later showed a WBC count of 15.27 × 10 E3/μL with an ANC of 12,740 cells/μL, persistent lymphopenia (1,430 lymphocytes/μL) and 70 immature granulocytes/μL, hemoglobin of 16.1 g/dL, hematocrit of 46%, platelet count of 362 × 10 E3/μL. As the DKA was resolving on the two-bag system, the patient's hypokalemia, hypomagnesemia, hypocalcemia, and hypophosphatemia were repleted as appropriate.
On admission to the hospital, as per current hospital policy, a nasopharyngeal swab was tested for the presence of SARS-CoV-2 RNA using the Thermo Fisher TaqPath assay (Thermo Fisher Scientific, Waltham, MA). This returned positive the next morning, with cycle threshold (Ct) values of 23.25 for ORF1ab target, 23.12 for the N target, and 22.73 for the S target. A repeat upper respiratory specimen obtained 3 days later and evaluated using the BDMax assay (Beckon Dickinson and Company, Franklin Lakes, NJ) also returned positive, with Ct values of 26.7 for the N1 target and 27.5 for the N2 target. LIAISON® SARS-CoV-2 IgG assay targeting the spike protein (S1/S2) (Diasorin S.p.A., Saluggia (VC)—Italy) was also positive on admission (optical density of 29.0; positive ≥ 15.0, range 400 units/mL. The patient never had any fever, diarrhea, nor any respiratory symptoms during the admission. Additional laboratory evaluations for inflammatory markers potentially associated with COVID-19 Multi-Inflammatory Syndrome in Children (MIS-C) are shown in Table 2. Except for very mildly elevated procalcitonin, C-reactive protein, D-Dimer and ferritin levels, inflammatory markers were normal. Markers of type 1 diabetes, however, were grossly abnormal, with an islet antigen 2 (IA-2) autoantibody of >120.0 U/ml and the glutamic acid decarboxylase antibody >250.0 IU/ml. Hemoglobin A1C was elevated at 14.8%.
The patient remained on a continuous insulin infusion and the two-bag system for 2 days and then was switched to a subcutaneous insulin regimen once the acidosis resolved. Adequate glucose control on the new subcutaneous insulin regimen was achieved and he was discharged after a 4-day admission.
The patient responded well to usual DKA protocol, with somewhat interesting features of high insulin requirements and low potassium. After stabilization of the metabolic acidosis, a subcutaneous insulin regimen was started per endocrinology with the patient transferred to the pediatric ward. He continued on a Lantus insulin regimen for basal coverage with carb correction. A sliding scale with Humolog was initiated. Additional laboratory studies including IgA, IA-2 Ab, insulin Ab, transglutaminase Ab panel, ICA-512-HgbA1c, transglutaminase abs panel GAD 65, anti-insulin antibodies, c-peptide, and Zinc Transporter 8 were ordered (Table 2).
Both the patient and his mother received diabetes education for home regimens. He required electrolyte correction and was discharged home with oral potassium supplementation and 2,000 IU vit D per dietary recommendations. A repeat Covid PCR test was stil positive on 8/24. The patient was discharged home to quarantine with mother for 14 days from the first positive SARS CoV-2 PCR test.
The child was seen in the endocrine clinic 1 day after discharge and again 1 and 3 weeks after discharge, being found to have acceptable blood glucose levels. He was following a carbohydrate-controlled diet fairly well and thus no changes were made during the diabetic nutrition follow-up visits. The expected outcome for new onset T1DM is well-controlled DM care and dietary modification, however, we do not have enough information regarding the long term outcomes of simultaneous T1DM and Covid-19 infection in children.
Our pediatric patient illustrates the typical pattern of T1DM in children during the COVID-19 pandemic and differs from that of a published report in a 19 year old with new onset DKA following COVID-19 (6) as our patient had a classic presentation of autoantibody-mediated T1DM. The timing of SARS-CoV-2 infection in our patient coincided with development of indolent symptoms of diabetes, particularly anorexia and weight loss. Although T1DM is most commonly diagnosed in childhood, it is a relatively rare disease, occurring in about 1.5 in 1,000 children (7). COVID-19 is also infrequently identified in children as compared to adults, with pediatric cases mainly diagnosed during pandemic surges (7). For this reason, the magnitude of the association between T1DM, DKA, and COVID-19 in youth is difficult to quantify, but is, nonetheless, apparent. In a report of U.S. children hospitalized with COVID-19, 2.7% had a history of chronic diabetes, and 2.9% developed DKA during their hospital stay (8). Whether SARS CoV-2 itself or deferred medical care are responsible for a higher presentation of DKA cases in younger populations has been a matter of debate (4, 9).
ACE2 is expressed in multiple organs, including exocrine and endocrine tissues of the pancreas. SARS-CoV, responsible for the epidemic of 2003, was shown to bind to ACE2 receptors through its spike protein, similarly to SARS-CoV-2 (10). Diabetes has been recognized as a risk factor for increased COVID-19 morbidity and mortality in adults since the onset of the SARS-CoV-2 pandemic (11). More recently, data from adults suggest that COVID-19 may lead to worse outcomes in patients with pre-established diabetes, and may trigger diabetic ketoacidosis (12). New-onset diabetes during the course of COVID-19 infection is recognized in both adults and children, with a small number of case reports described to date (2, 13). A study of SARS patients with diabetes strongly suggested that the localization of ACE2 expression in the endocrine part of the pancreas allowed SARS coronavirus to enter and damage pancreatic islets, leading to acute diabetes (10). Both SARS-CoV and SARS-CoV-2 have been reported to trigger transient insulin resistance and hyperglycemia (10, 11).
A report of a 19 year-old male with autoantibody negative Type 1 diabetes mellitus (T1DM) following COVID-19 infection acquired following exposure to symptomatic parents highlights the important consideration of whether SARS-CoV-2 infection may directly damage pancreatic islet cells abundantly expressing ACE2 viral receptors (6). Another possibility is that immune dysregulation during the course of COVID-19 disease may induce development of autoantibodies against pancreatic beta cells. Potentially both circumstances may occur in parallel, with infection of cells expressing ACE2 receptors triggering a dysregulated humoral immune response resulting in the death of pancreatic islet cells. Deferred medical care which discourages patients and parents of children to seek help during lockdown situations may likely contribute to more patients with new onset T1DM present in DKA (9, 14). Decline in pediatric medical care occurs COVID-19 pandemic, where for example childhood immunization programs have suffered despite best efforts (15). In the case of our patient, symptoms went unrecognized for nearly 3 weeks, and upon diagnosis, off-scale levels of autoantibodies were present, a common finding in T1DM. Both mechanisms of pathogenesis and the underlying issues associated with pandemic situations and unavailability of hospital beds are likely leading to an unprecedented number of DKA cases in youth with COVID-19. Table 3 summarizes current pediatric studies on the topic to date.
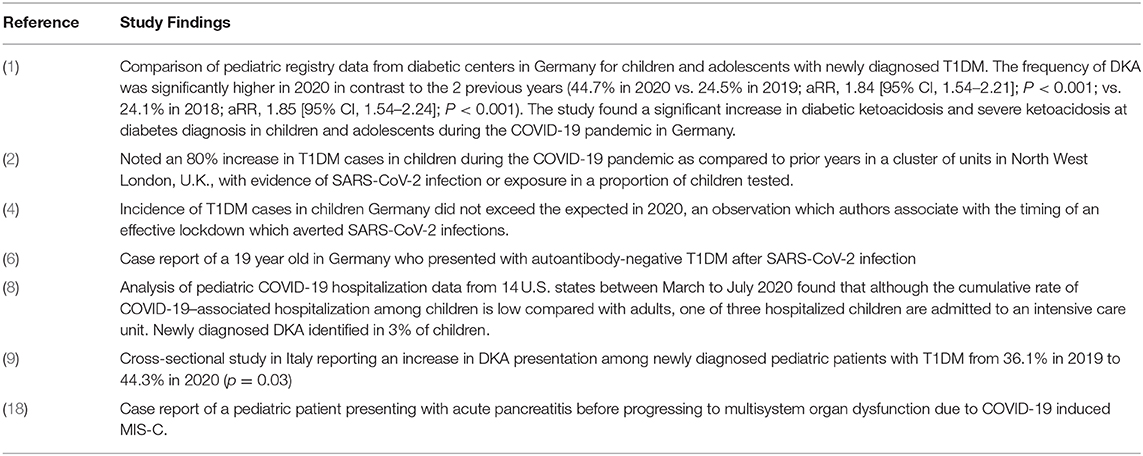
Table 3. Reports of DKA in children and youth during the COVID-19 pandemic.
Although SARS CoV-2 infection of pancreatic beta cells has not been yet demonstrated, there is enough evidence of direct viral damage leading to organ failure in different body compartments, as in the case of COVID-19 myocarditis (16). Cases of pancreatitis in patients with COVID-19 have been reported in both adults and children (17, 18). It is difficult to discern which cases of new onset T1DM are due to direct viral damage, and which are due to immune dysregulation induced by COVID-19. While DM is a risk factor for severe COVID-19, SARS-CoV-2 infection also triggers T1DM, a bidirectional relationship shown to occur in adults and now increasingly demonstrable in youth. It is critical that awareness regarding this specific complication of SARS-CoV-2 infection in children be heightened, not only to enable early identification of DM, but also to counteract the belief that COVID-19 poses no threat to young patients.
In summary, our intent with this case report was to raise awareness among pediatricians about the potential for a large increase in the number of COVID-19 associated T1DM and DKA cases in children and youth following pandemic surges. Other institutions might be witnessing the same phenomenon and through this publication we wished to share this unique presentation of COVID-19 in children. Because the number of COVID-19 cases have sky-rocketed in recent months globally (December 2020/ January 2021), it is very likely that we will be seeing a very sharp rise in the number of T1DM and DKA events in children exposed to the virus through their family members. These children often require admission to critical care, and it is very important to recognize this potential complication of this condition in pediatric populations.
Despite the difficult circumstances, the patient and his family are adapting to the diagnosis of T1DM and mother and child are now heavily engaged with our institution's pediatric diabetes clinic. The child continues to be closely monitored with bi-monthly in person and telehealth visits. Family support through pediatric diabetes networks has been instrumental.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The patient's mother provided informed consent for the publication of this case report.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2021.628810/full#supplementary-material
1. Kamrath C, Mönkemöller K, Biester T, Rohrer TR, Warncke K, Hammersen J, et al. Ketoacidosis in children and adolescents with newly diagnosed type 1 diabetes during the COVID-19 pandemic in Germany. JAMA. (2020) 324:801–4. doi: 10.1001/jama.2020.13445
2. Unsworth R, Wallace S, Oliver NS, Yeung S, Kshirsagar A, Naidu H, et al. New-onset Type 1 diabetes in children during COVID-19: multicenter regional findings in the U.K. Diab Care. (2020) 43:e170–e1. doi: 10.2337/dc20-1551
3. Lönnrot M, Lynch KF, Elding Larsson H, Lernmark Å, Rewers MJ, Törn C, et al. Respiratory infections are temporally associated with initiation of type 1 diabetes autoimmunity: the TEDDY study. Diabetologia. (2017) 60:1931–40. doi: 10.1007/s00125-017-4365-5
4. Tittel SR, Rosenbauer J, Kamrath C, Ziegler J, Reschke F, Hammersen J, et al. Did the COVID-19 lockdown affect the incidence of pediatric type 1 diabetes in Germany? Diabetes Care. (2020) 43:e172–e3. doi: 10.2337/dc20-1633
5. Rubino F, Amiel SA, Zimmet P, Alberti G, Bornstein S, Eckel RH, et al. New-onset diabetes in Covid-19. N Engl J Med. (2020) 383:789–90. doi: 10.1056/NEJMc2018688
6. Hollstein T, Schulte DM, Schulz J, Glück A, Ziegler AG, Bonifacio E, et al. Autoantibody-negative insulin-dependent diabetes mellitus after SARS-CoV-2 infection: a case report. Nat Metab. (2020) 2:1021–4. doi: 10.1038/s42255-020-00281-8
7. Rush T, McGeary M, Sicignano N, Buryk MA. A plateau in new onset type 1 diabetes: Incidence of pediatric diabetes in the United States Military Health System. Pediatr Diabetes. (2018) 19:917–22. doi: 10.1111/pedi.12659
8. Kim L, Whitaker M, O'Halloran A, Kambhampati A, Chai SJ, Reingold A, et al. Hospitalization rates and characteristics of children aged <18 years hospitalized with laboratory-confirmed COVID-19 - COVID-NET, 14 States, March 1-July 25, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:1081–88. doi: 10.15585/mmwr.mm6932e3
9. Rabbone I, Schiaffini R, Cherubini V, Maffeis C, Scaramuzza A, Diabetes Study Group of the Italian Society for Pediatric Endocrinology and Diabetes. Has COVID-19 delayed the diagnosis and worsened the presentation of Type 1 diabetes in children? Diab Care. (2020) 43:2870–2. doi: 10.2337/dc20-1321
10. Yang JK, Lin SS, Ji XJ, Guo LM. Binding of SARS coronavirus to its receptor damages islets and causes acute diabetes. Acta Diabetol. (2010) 47:193–9. doi: 10.1007/s00592-009-0109-4
11. Abdi A, Jalilian M, Sarbarzeh PA, Vlaisavljevic Z. Diabetes and COVID-19: a systematic review on the current evidences. Diab Res Clin Pract. (2020) 166:108347. doi: 10.1016/j.diabres.2020.108347
12. Goldman N, Fink D, Cai J, Lee YN, Davies Z. High prevalence of COVID-19-associated diabetic ketoacidosis in UK secondary care. Diab Res Clin Pract. (2020) 166:108291. doi: 10.1016/j.diabres.2020.108291
13. Reddy PK, Kuchay MS, Mehta Y, Mishra SK. Diabetic ketoacidosis precipitated by COVID-19: A report of two cases and review of literature. Diabetes Metab Syndr. (2020) 14:1459–62. doi: 10.1016/j.dsx.2020.07.050
14. DiMeglio LA, Albanese-O'Neill A, Muñoz CE, Maahs DM. COVID-19 and children with diabetes-updates, unknowns, and next steps: first, do no extrapolation. Diabetes Care. (2020) 43:2631–4. doi: 10.2337/dci20-0044
15. Khan A, Bibi A, Sheraz Khan K, Raza Butt A, Alvi HA, Zahra Naqvi A, Mushtaq S, et al. Routine pediatric vaccination in Pakistan during COVID-19: how can healthcare professionals help? Front Pediatr. (2020) 10:613433. doi: 10.3389/fped.2020.613433
16. Dolhnikoff M, Ferreira Ferranti J, de Almeida Monteiro RA, Duarte-Neto AN, Soares Gomes-Gouvêa M, Viu Degaspare N, et al. SARS-CoV-2 in cardiac tissue of a child with COVID-19-related multisystem inflammatory syndrome. Lancet Child Adolesc Health. (2020) 4:790–4. doi: 10.1016/S2352-4642(20)30257-1
17. Inamdar S, Benias PC, Liu Y, Sejpal DV, Satapathy SK, Trindade AJ, et al. Prevalence, risk factors, and outcomes of hospitalized patients with COVID-19 presenting as acute pancreatitis. Gastroenterology. (2020) 159:2226–8.e2. doi: 10.1053/j.gastro.2020.08.044
Keywords: COVID-19, children, type 1 diabetes mellitus (T1DM), diabetic keto-acidosis (DKA), SARS CoV-2, pediatric COVID-19
Citation: Nielsen-Saines K, Li E, Olivera AM, Martin-Blais R and Bulut Y (2021) Case Report: Insulin-Dependent Diabetes Mellitus and Diabetic Keto-Acidosis in a Child With COVID-19. Front. Pediatr. 9:628810. doi: 10.3389/fped.2021.628810
Received: 13 November 2020; Accepted: 12 January 2021;
Published: 10 February 2021.
Edited by:
Manuela Zlamy, Innsbruck Medical University, AustriaReviewed by:
Amjad Khan, Quaid-i-Azam University, PakistanCopyright © 2021 Nielsen-Saines, Li, Olivera, Martin-Blais and Bulut. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Erica Li, ZXJpY2FsaUBtZWRuZXQudWNsYS5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.