
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pediatr., 29 March 2021
Sec. Pediatric Pulmonology
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.622240
This article is part of the Research TopicEmerging Pneumonia in ChildrenView all 11 articles
 Jenny Libeth Jurado Hernández1*
Jenny Libeth Jurado Hernández1* Iván Francisco Álvarez Orozco2
Iván Francisco Álvarez Orozco2The coronavirus disease 2019 (COVID-19) represents a health problem with multidimensional impacts and heterogeneous respiratory involvement in children, probably due to the interaction between different and complex mechanisms that could explain its variable degrees of severity. Although the majority of reports reveal that children develop less severe cases, the number of patients is increasing with more morbidity. Most serious respiratory manifestations are acute respiratory distress syndrome (ARDS) and pneumonia. By understanding the key aspects that can be used to differentiate between pediatric and adult respiratory compromise by COVID-19, we can improve our knowledge, and thus decrease the negative impact of the disease in the pediatric population. In this mini review, we summarize some of the mechanisms and findings that distinguish between adult and pediatric COVID-19 and respiratory involvement, taking into account some issues related to the physiopathology, diagnosis, clinical and paraclinical presentation, severity, treatment, and control of the disease.
The coronavirus disease 2019 (COVID-19) is the result of infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (1, 2). This coronavirus is characterized by its high level of transmissibility and pathogenicity, resulting in a pandemic, and its multidimensional impact (3–5). SARS-CoV-2 produces heterogeneous respiratory involvement, especially in children (6, 7). Some vascular, immunological, and molecular mechanisms probably explain its variable degrees of severity or atypical presentations compared to adults (8) and, consequently, some differences in diagnosis, severity, treatment, and control of the disease. Currently, pediatric patients with severe manifestations of the disease are increasing (9); pneumonia is the most common respiratory entity, and acute respiratory distress syndrome (ARDS) is the critical form (7).
With the aim of summarizing the mechanisms and findings that can be used to differentiate respiratory involvement between pediatric and adult COVID-19, taking into account issues related to the physiopathology, diagnosis, severity, treatment, and control of the disease, this paper elaborates on the characteristics of the SARS-CoV-2 pathophysiology, clinical and paraclinical presentation, diagnostic and therapeutic approach, and follow-up of COVID-19 in both populations. Using the Scopus and PubMed databases, the keywords SARS-CoV-2, COVID-19, respiratory involvement, respiratory system, pneumonia, and ARDS were searched. This review includes the differences in COVID-19 manifestations between children and adults.
COVID-19 occurs in children of all ages (10); however, the pediatric disease represents <5% of total cases (11). In this population, the infection predominates in school children and adolescents (12); the Center of Disease Control and Prevention (CDC) reports 386,329 cases in the United States (13). The percentage of cases is slightly higher in females compared with males (50.5 vs. 49.5%), and the rate of mortality is extremely low in both populations (<0.1%; 62 deaths) with a greater percentage of deaths in males (52.5%) (14). Despite these statistics, global data about morbidity in children may be understated because they have less frequent exposure to some sources of transmission, and the clinical course includes milder respiratory symptoms compared with adults (15–18). These situations may explain why children are less often tested (18, 19). For them, transmission of infection through familial clusters predominates (10).
The Figure 1 shows the basic structure of SARS-CoV-2 and pathophysiology of COVID-19. SARS-CoV-2 infection causes heterogeneous respiratory involvement ranging from mild to severe respiratory failure. In pediatric and adult patients, this compromise can occur in three phases. In the first phase, the virus binds to epithelial cells of the respiratory tract to commence primary replication; most patients are able to contain the infection in this stage and thus present mild disease. In the second phase, SARS-CoV-2 migrates down the airways and enters alveolar epithelial cells facilitating pulmonary viral replication and localized inflammation (7, 20); most patients need hospitalization due to pneumonia. In the third phase, the rapid replicative process of the virus at the lung level may trigger apoptosis of cells with vascular leakage and the release of pro-inflammatory proteins (5). The simultaneous downregulation of ACE2 expression can alter the renin-angiotensin system with elevation of angiotensin-2, which increases inflammation and vascular permeability, causing pulmonary edema. Patients can develop a strong immune response (21, 22) with subsequent cytokine storm [e.g., release of IL-2, IL-6, IL-7, IL-10, GCSF, IP-10, MCP-1, MIP-1, and TNF-α; (5)] which causes ARDS and respiratory failure (23–25). The proportion of T cells (helper T cells and memory helper T cells) is diminished, and naïve helper T cell levels are elevated in the severe disease (5, 14). To date, pediatric moderate and critical respiratory cases are less frequent than those presented in adults.
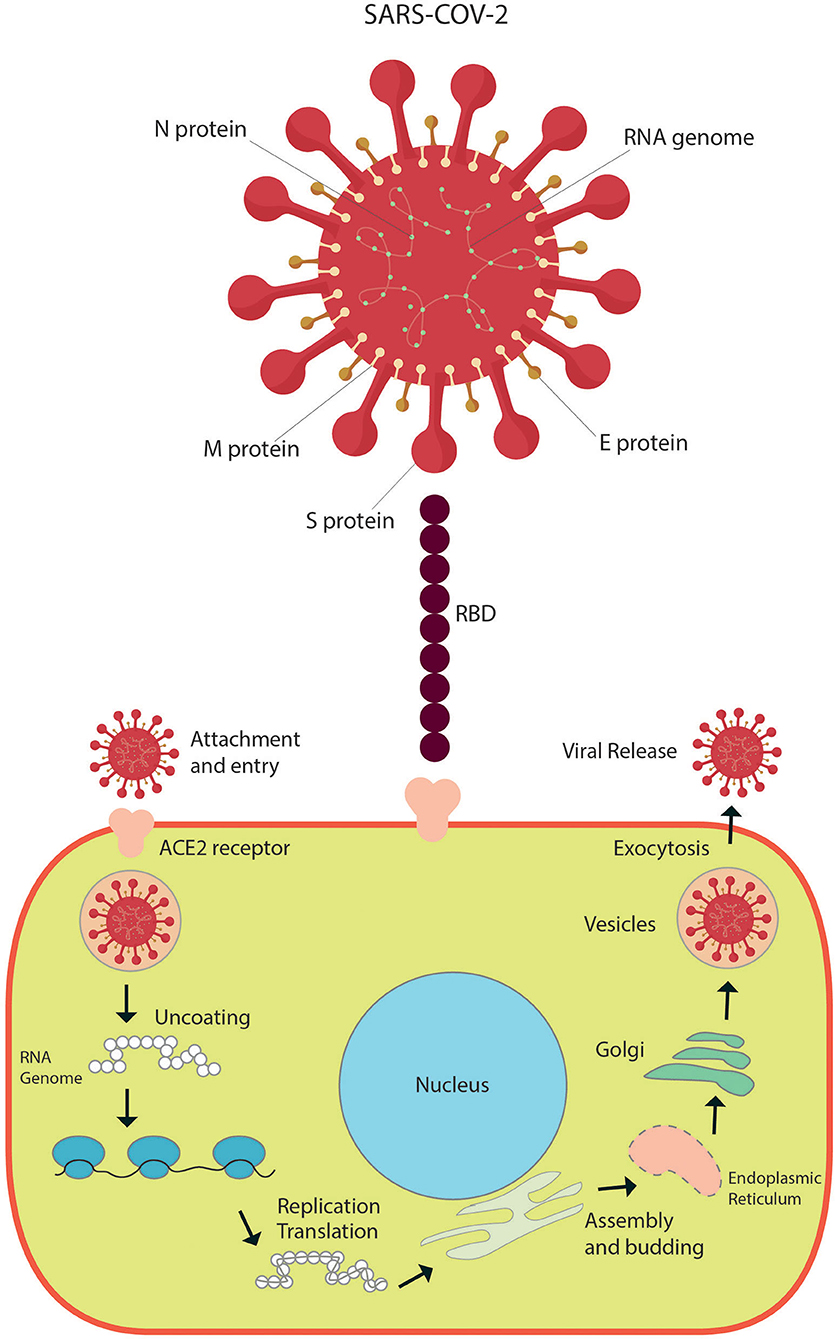
Figure 1. Basic structure of SARS-CoV-2 and pathophysiology of infection.
Generally, the SARS-CoV-2 viral load is elevated in the first week of clinical presentation, gradually reducing afterward (26). However, after 4–7 days of COVID-19, some patients present a critical evolution concurrent with a decrease in viral load and deterioration of inflammatory parameters. Among the more severe clinical cases, some patients can have a less steep and prolonged decline in the SARS-CoV-2 load (5). Around days 7–10 of symptoms, an elevation in IgG and IgM levels against antigens of the virus appears, and there is a progressive decrease in the viral load (5, 27, 28). The persistence of high viral load and exaggerated inflammatory response in severe lung involvement and multi-organ dysfunction is explained by the combination of virus-mediated cytopathic effects and immunologically mediated injury. Patients can gradually improve, or they do not recover (29).
Mechanisms have been proposed to explain the lower severity of respiratory involvement by COVID-19 in children compared to adults (30). From an immunological standpoint, the function of innate immunity with a predominance of natural killer cells and the previous development of immunological memory against other respiratory infectious processes seem to influence the response capacity against this beta coronavirus, minimizing its clinical impact (5, 31, 32). Likewise, the availability of a greater number of B and T lymphocytes observed in children can prevent an excessive inflammatory response, conferring a less severe course of illness (33), especially in pneumonia (34). In this way, another potential route that can provide clinical benefit is constant immunological training secondary to frequent exposure to early childhood vaccines, including immunization against HiB and pneumococcus (35).
At the vascular level, endothelial function, and coagulation are more preserved in children, reducing the possibility of vasculitic alterations or pulmonary thrombotic phenomena (36).
From a microbiological context, the presence of additional viral infections concomitant to SARS-CoV-2 occurs more frequently in children than in adults and seems to play a protective role by inhibiting the replicative process (37–40). Furthermore, the competitive effect of normal airway microbiota can decrease colonization and growth of the virus (41, 42) and interfere with the appearance or infection severity. Previous infection with other coronaviruses may influence development of cross-protection against the novel coronavirus (43).
In children, exposure to SARS-CoV-2 is usually less frequent and has a lower intensity due to adopted precautionary measures, favoring a milder clinical presentation of COVID-19 (44).
From a molecular perspective, in the pediatric and adolescent population with COVID-19, increased ACE2 activity is observed. This characteristic appears to have a protective function due to its participation in anti-inflammatory signaling (43, 45), leading to less severe disease in children compared to that in the elderly (29). However, Sharif-Askari et al. reported a low expression level of TMPRSS2 and ACE2 in the upper and the lower respiratory tract of children and adolescents in comparison to adults with COPD or who smoked, suggesting the negative impact of some clinical conditions on the severity of COVID-19 in adults (46).
The demonstration of SARS-CoV-2 through the reverse transcription polymerase chain reaction (RT-PCR) test confirms diagnosis (15, 19, 28, 47); it is particularly useful in children given their heterogeneity in presentation of COVID-19 (12). In some cases, it is possible to find patients with a high index of suspicion for this viral infection with suggestive symptoms and/or a history of exposure and a negative test result in whom it can be necessary to repeat (48).
Moreover, the serology is available to recognize the population with prior or recent SARS-CoV-2 infection (6). However, this test is not considered the only tool to support diagnosis of acute infection because of the variability in the time for the seroconversion or the detection of antibodies against SARS-CoV-2 (6, 43). The serological assay may be helpful in the case of an individual with a high likelihood of infection whose molecular diagnosis and antigen test show false-negative results (6, 49, 50). Unlike adults, the seroconversion rate can be lower among infected children (51, 52), which suggests a weaker seroconversion in asymptomatic cases and slight forms of COVID-19 (43). Rostad et al. found IgG antibodies to the virus in all children with multisystem inflammatory syndrome in children (MIS-C) and in more than 90% of those with severe or moderate COVID-19 by clinic and inflammatory parameters; however, antibody responses in children with a mild form were not detected (53). With these findings, a prognostic and diagnostic role of antibodies specifically for pediatric COVID-19 is suggested.
In about two thirds of pediatric cases of COVID-19, the child had physical contact with a confirmed case (54), and the exposure, different from adults, usually occurred at home (55). In children, most described symptoms are fever (47.5–51.6%) and cough (41.5–47.3%) (7, 10, 18, 21, 22, 36, 56, 57); however, dyspnea (40%) is the most common respiratory signal in more severe presentations, such as pneumonia and ARDS (7, 18). Relative to adults, pediatric cases present other concomitant symptomatology (e.g., fatigue and muscle pain) and more co-morbid conditions even in different systems in a representative proportion (55, 58).
The progression to severe or critical forms is infrequent in pediatric cases (10): 2% are severe cases, and <2% correspond to critical evolutions (7). Some cases are classified as moderate disease due to radiological findings, although the symptoms are few (2, 7, 59). The recovery is faster probably due to lower affectation and a better immune response (60), but complications in the presence of co-morbidities are more likely (10, 61, 62). Although mortality in cases requiring pediatric intensive care units (PICU) is low (12, 63), an increase is being observed.
Götzinger et al. explored various risk factors for admission to intensive care. Age below 1 month, male sex, clinical evolution with lower airway infectious compromise, and a history of co-morbidities showed relevance. They also identified a heterogeneity of previous diseases, including pulmonary entities, cardiac disturbances, malignant diseases, or nervous system disorders. Some patients received antivirals or immunomodulators due to a serious clinical course (64); however, the role of these agents in pediatric COVID-19 is not fully established.
The American College of Radiology suggests performing chest x-rays (CXR) in pediatric patients with moderate or severe symptomatology, and in those with antecedents and previous risk factors (18) because they can need hospitalization and greater care (65). Peribronchial cuffing in both lung fields and central and peripheral ground-glass opacities (GGOs) are present in this group. However, these patterns are still non-specific. Another finding is bilateral or unilateral consolidation. Less common presentations include pleural effusion and mediastinal widening. During follow-up, radiological control depends on clinical evolution with rapid resolution of involvement in most of the cases. If patients worsen, a persistence of symptom exacerbation in findings or new consolidations can be observed (66).
Palabiyik et al. observed alterations in CXR in about half of children evaluated for pneumonia, particularly in the lower areas. The most frequent abnormality was unilateral increased density (67). Unlike adults, radiological compromise is less described in children possibly because the cases are mostly mild, the disease goes unnoticed, or it is poorly evaluated (68). Some authors emphasize atypical manifestations in pediatric pneumonia, including unilateral lobar or segmental consolidation, central bilateral or unilateral GGOs, and/or consolidation, single-round consolidation, pleural effusion, or lymphadenopathy (65, 69).
The COVID-19 alterations most recognized on a chest computerized tomography (CT) scan in pediatrics are GGOs and patchy shadowing (7). Although, this imaging study is not recommended for systematic use, it has shown utility mainly in the evaluation of children when the acute clinical course includes hypoxemia or dyspnea, deterioration in clinical or laboratory parameters (for example, a higher D-dimer), or there is a poor response to support therapy (9, 65, 66). Unlike adults, CT indications are more specific, such as in clinical worsening or suspicion of pulmonary embolism (30, 65), because the avoidance of radiation is necessary. Typical features more reported in pneumonia are bilateral, peripheral, and/or sub-pleural GGOs and/or consolidation, especially in the lower lobe—and the “halo” sign. In relation to the indeterminate pattern, the CT scan reveals similar findings to those previously described in CXR and in “crazy paving” signs. Discrete small nodules (tree-in-bud, centrilobular) and lung cavitation can be observed in atypical presentations as well as other alterations mentioned in the radiography. In cases of indeterminate or atypical patterns, it is recommended that additional investigations of differential diagnoses occur according to each case (61, 69).
In comparison to adults, children have a generalized peripheral distribution of lesions (68) and a lower percentage of cases with GGOs, consolidation, crazy paving pattern, pleural effusion, and bilateral compromise (70). The more pronounced difference between the groups corresponds to a higher frequency of unilateral lesions (30% of cases) and nodules (15%) in children (70, 71); this implies that atypical presentations should be considered more often in pediatrics (67). Also, ~20% of the pediatric population have normal CT, which reinforces the importance of its performance in selected cases (70).
Most children with COVID-19 have normal laboratory findings compared with adults; however, a variability in features is recognized (18). In a review that included 655 pediatric patients, 17.1% showed low leucocyte levels, and 13.3% had lymphopenia or neutropenia (18). In other publications that summarize various studies, high levels of ferritin in 26% of children (12), elevation of C-reactive protein in 19%, and procalcitonin in 25–31% have been reported (5, 12). All these alterations present possibly in the context of greater severity secondary to a more inflammatory response. In contrast, a lower presence of marked inflammatory changes and lymphopenia is possible (72). In relation to co-infection, the prevalence of other common respiratory pathogens is high in children; therefore, concomitant evaluation (37) in the peak season for viral respiratory illness is suggested (73).
In a study of 70 adolescents admitted to PICUs, 21 (30%) developed ARDS even in the first 2 weeks of admission with a prolonged hospital stay; most patients had bilateral infiltrates. The platelet counts were significantly lower, and levels of IL-6 were more elevated compared to those without ARDS. Although other markers (lactate, pro-B-type natriuretic peptide) were high, the results did not have statistical relevance (74). The overall mortality was 2.8% (74); however, in adults the percentage of mortality with this condition is higher.
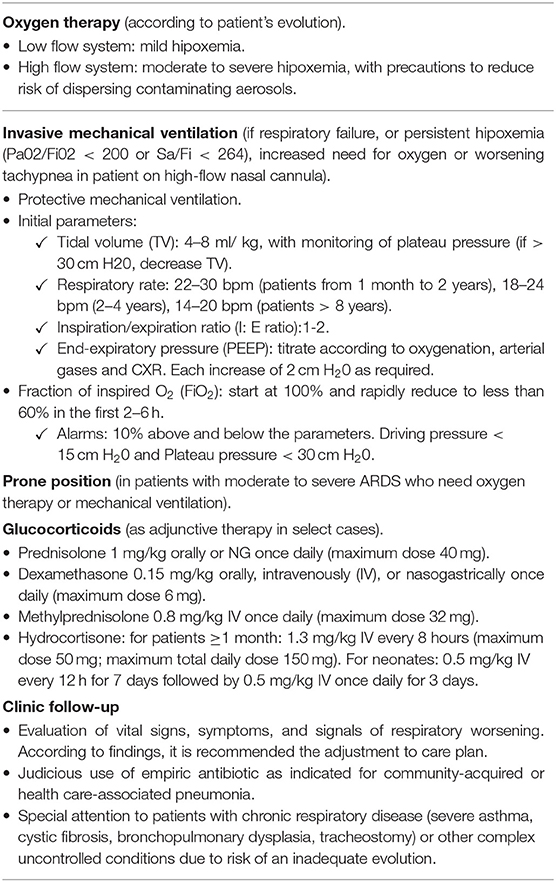
Generally, children with severe and critical presentations of COVID-19 require hospitalization. In addition, patients with non-severe forms and risk of severe disease due to pre-existing conditions can need hospital admission. Pediatric treatment focuses on supportive care by respiratory support with supplemental oxygen and invasive or non-invasive ventilation, fluid and electrolyte support, judicious use of empiric antibiotics as indicated for community-acquired or healthcare-associated pneumonia, systematic clinical follow-up, and laboratory monitoring (75). Unlike adults, anticoagulation seems to be less frequent in children, shown by lower presentation of embolic events. Evaluation of inflammation with C-reactive protein, D-dimer, LDH, ferritin, and IL-6 can be considered two to three times per week or if there is clinical worsening (75, 76). Other laboratory or imaging studies can be required according to each case. Special attention must be given to adequate nutritional support and temperature control. Table 1 summarizes respiratory management in children (49, 77).
There is no specific treatment for adult and pediatric COVID-19, and pharmacotherapy is controversial (64, 78). Therefore, clinical trials have been developed to investigate the use of antivirals, antimalarials, and adjunct therapies especially in adult patients with severe or non-severe manifestations. Other investigations have evaluated the impact of using different forms of oxygen therapy and prevention measures (79, 80). Few studies have included children. The main limitation in the research on antiviral therapy and other strategies has been the big difference in the number of pediatric and adult events in COVID-19 and asymptomatic infection or with minimal symptoms among children (81).
There are some conditional suggestions for the utilization of antiviral agents in pediatric COVID-19 given the lack of demonstrated efficacy. This therapy should be reserved for children with severe involvement secondary to confirmed disease. Remdesivir, a nucleotide analog prodrug that inhibits viral RNA polymerases (82), has been considered in pediatrics because randomized trials in adults suggest a potential benefit; however, the use of this agent must be individualized and, preferably, in the context of a clinical trial (75, 77, 81, 83). At this time, remdesivir is approved by the FDA for the treatment of COVID-19 in hospitalized patients aged >12 years and >40 kg in weight (84). Lopinavir/ritonavir is not recommended for routine use in children due to unfavorable pharmacodynamics and the absence of evidence for efficacy (77, 85, 86). Hydroxychloroquine and chloroquine are considered only in clinical trials and in hospitalization (77, 87–90).
As part of adjunctive therapy, low-dose glucocorticoids are suggested for select children with severe or critical disease who cannot participate in a clinical trial: the efficacy is uncertain given children have been underrepresented in the clinical trials (75, 79–81, 90–93). The use of other adjunctive treatment must be discussed case by case according to disease severity and in agreement with multidisciplinary teams as indicated (90). IL-6 inhibitors, interferon-beta 1b, and convalescent plasma from recovered COVID-19 patients are not recommended for routine use because the benefits/risks are uncertain in children (83, 84, 90, 94). Moreover, the clinical potential of other immunomodulators or passive immunization therapies must be elucidated with prospective, randomized, placebo-controlled trials in the pediatric group. Recently, evidence of potential therapeutic options in COVID-19 has been updated; however, it is necessary to develop high-quality trials to improve disease management (95).
Preventive measures to reduce viral spread utilize personal hygiene maintenance, including frequent hand washing, use of a face mask, disinfection of surfaces, social and physical distancing, home isolation, voluntary home quarantine, and operation adjustments in educative centers (77, 96).
Vaccination seems be the most effective method to avoid and control the illness (97, 98). Strategies include recombinant vectors, DNA, mRNA in lipid nanoparticles, protein subunits, inactivated viruses, and live attenuated viruses (7, 97, 99). Recently, the FDA approved the emergency use of two vaccines to prevent SARS-CoV-2 infection in individuals >16 years, generating profound worldwide expectation (100).
Various mechanisms and findings can be used to differentiate between adult and pediatric COVID-19, especially with respiratory involvement; however, children are less often tested. They have lower seroconversion and less exposure to some sources of transmission, although infection through familial clusters predominates. Adaptive and innate immune responses, previous or concomitant infection with other viruses, microbiota effects, increased ACE2 activity, and more preserved coagulation and endothelial function confer clinical advantages that contribute to the presentation of milder forms of the disease and a better prognosis. Fever and cough are more common manifestations, and dyspnea occurs in the context of pneumonia and ARDS. Co-morbidities can affect evolution. Most children show normal laboratory findings; however, there is certain variability and a lower prevalence of lymphopenia or marked inflammatory parameters. They can present atypical or normal images in a representative proportion of cases. CXR is preferred over CT. A CT scan is performed if there is clinical worsening or suspicion of pulmonary embolism. Pediatric treatment focuses on supportive care as there is less research into vaccines and specific treatments and thus a more conditioned use of pharmacotherapy.
Although there are still knowledge gaps in pediatric COVID-19 discussion, it is necessary to continue comprehensive and specific investigations to mitigate its consequences.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
This mini review was financed with own resources.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
ACE2, angiotensin-converting enzyme 2; ARDS, acute respiratory distress syndrome; CDC, Center of Disease Control and Prevention; COPD, chronic obstructive pulmonary disease; GGOs, ground-glass opacities; COVID-19, coronavirus disease 2019; RBD, receptor-binding domains; CT, computerized tomography; CXR, chest x-ray; FDA, Food and Drugs Administration; HDL, lactate dehydrogenase; HiB, Haemophilus influenzae B; IgG, immunoglobulin G; IgM, immunoglobulin M; IL-2, interleukin 2; IL-6, interleukin 6; IL-7, interleukin 7; IL-10, interleukin 10; GCSF, granulocyte colony-stimulating factor; IP-10, interferon-inducible protein; MCP-1, monocyte chemoattractant protein-1; MIS-C, multisystem inflammatory syndrome in children; MIP-1, macrophage inflammatory protein 1 alpha; PICU, pediatric intensive care unit; RNA, ribonucleic acid; RT-PCR, reverse transcription polymerase chain reaction; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TMPRSS2, transmembrane protease serin 2; TNF-α, tumor necrosis factor alpha.
1. Coutard B, Valle C, de Lamballerie X, Canard B, Seidah NG, Decroly E. The spike glycoprotein of the new coronavirus 2019-nCoV contains a furin-like cleavage site absent in CoV of the same clade. Antiviral Res. (2020) 176:104742. doi: 10.3389/fped.2021.579922/abstract
2. Min Z, Jun C, Fu F, Shu Q, Hu Y, Chun C, et al. Diagnosis and treatment recommendations for pediatric respiratory infection caused by the 2019 novel coronavirus. World J Pediatr. (2020) 16:240–6. doi: 10.1007/s12519-020-00345-5
3. Hu B, Guo H, Zhou P, Shi ZL. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol. (2020) 19:141–54. doi: 10.1038/s41579-020-00459-7
4. Cui J, Li F, Shi ZL. Origin and evolution of pathogenic coronaviruses. Nat Rev Microbiol. (2019) 17:181–92. doi: 10.1038/s41579-018-0118-9
5. Zimmermann P, Curtis N. Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections. Arch Dis Child. (2020) 1–11. doi: 10.1136/archdischild-2020-320338
6. World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report - 64. (2020). Available online at: www.who.int (accessed February 25, 2021).
7. de Souza TH, Nadal JA, Nogueira RJN, Pereira RM, Brandão MB. Clinical manifestations of children with COVID-19: A systematic review. Pediatr Pulmonol. (2020) 55:1892–9. doi: 10.1002/ppul.24885
8. Kaul D. An overview of coronaviruses including the SARS-2 coronavirus – molecular biology, epidemiology and clinical implications. Curr Med Res Pract. (2020) 10:54–64. doi: 10.1016/j.cmrp.2020.04.001
9. Yuki K, Fujiogi M, Koutsogiannaki S. COVID-19 pathophysiology: a review. Clin Immunol. (2020) 215:108427. doi: 10.1016/j.clim.2020.108427
10. Ali AS, Al-Hakami AM, Shati AA, Asseri AA, Al-Qahatani SM. Salient conclusive remarks on epidemiology and clinical manifestations of pediatric COVID-19: narrative review. Front Pediatr. (2020) 8:584694. doi: 10.3389/fped.2020.584694
11. Meena J, Yadav J, Saini L, Yadav A, Kumar J. Clinical features and outcome of SARS-CoV-2 infection in children: a systematic review and meta- analysis. Indian Pediatr. (2020) 57:820–6. doi: 10.1007/s13312-020-1961-0
12. Badal S, Thapa Bajgain K, Badal S, Thapa R, Bajgain BB, Santana MJ. Prevalence, clinical characteristics, and outcomes of pediatric COVID-19: A systematic review and meta-analysis. J Clin Virol. (2021) 135:104715. doi: 10.1016/j.jcv.2020.104715
14. Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao Y, et al. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin Infect Dis. (2020) 71:762–8. doi: 10.1093/cid/ciaa248
15. Sanche S, Lin YT, Xu C, Romero-Severson E, Hengartner N, Ke R. High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 2. Emerg Infect Dis. (2020) 26:1470–77. doi: 10.3201/eid2607.200282
16. Robinson J, Freire D. COVID-19 – what does a paediatrician need to know? Paediatr Respir Rev. (2020) 35:3–8. doi: 10.1016/j.prrv.2020.05.001
17. Zeng L, Xia S, Yuan W, Yan K, Xiao F, Shao J, et al. Neonatal early-onset infection with SARS-CoV-2 in 33 neonates born to mothers with COVID-19 in Wuhan, China. JAMA Pediatr. (2020) 174:722–25. doi: 10.1001/jamapediatrics.2020.0878
18. Liguoro I, Pilotto C, Bonanni M, Ferrari ME, Pusiol A, Nocerino A, et al. SARS-COV-2 infection in children and newborns: a systematic review. Eur J Pediatr. (2020) 179:1029–46. doi: 10.1007/s00431-020-03684-7
19. Zimmermann P, Curtis N. Coronavirus infections in children including COVID-19: an overview of the epidemiology, clinical features, diagnosis, treatment and prevention options in children. Pediatr Infect Dis J. (2020) 39:355–68. doi: 10.1097/INF.0000000000002660
20. Shang J, Wan Y, Luo C, Ye G, Geng Q, Auerbach A, et al. Cell entry mechanisms of SARS-CoV-2. Proc Natl Acad Sci USA. (2020) 117:11727–34. doi: 10.1073/pnas.2003138117
21. Teo JTR, Abidin NH, Cheah FC. Severe acute respiratory syndrome-Coronavirus-2 infection: a review of the clinical pathological correlations of Coronavirus disease-19 in children. Malays J Pathol. (2020) 42:349–61.
22. Dhama K, Patel SK, Pathak M, Yatoo MI, Tiwari R, Malik YS, et al. An update on SARS-CoV-2/COVID-19 with particular reference to its clinical pathology, pathogenesis, immunopathology and mitigation strategies. Travel Med Infect Dis. (2020) 37:101755. doi: 10.1016/j.tmaid.2020.101755
23. Jin Y, Yang H, Ji W, Wu W, Chen S, Zhang W, et al. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses. (2020) 12:372. doi: 10.3390/v12040372
24. Fu Y, Cheng Y, Wu Y. Understanding SARS-CoV-2-mediated inflammatory responses: from mechanisms to potential therapeutic tools. Virol Sin. (2020) 35:266–71. doi: 10.1007/s12250-020-00207-4
25. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
26. Cevik M, Tate M, Lloyd O, Maraolo AE, Schafers J, Ho A. SARS-CoV-2, SARS-CoV, and MERS-CoV viral load dynamics, duration of viral shedding, and infectiousness: a systematic review and meta-analysis. Lancet Microbe. (2020) 2:e13–22. doi: 10.1016/S2666-5247(20)30172-5
27. To KKW, Tsang OTY, Leung WS, Tam AR, Wu TC, Lung DC, et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis. (2020) 20:P565–74. doi: 10.1016/S1473-3099(20)30196-1
28. Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. (2020) 581:465–9. doi: 10.1038/s41586-020-2196-x
29. Dhochak N, Singhal T, Kabra SK, Lodha R. Pathophysiology of COVID-19: why children fare better than adults. Indian J Pediatr. (2020) 87:537–46. doi: 10.1007/s12098-020-03322-y
30. Parisi GF, Indolfi C, Decimo F, Leonardi S, Miraglia del Giudice M. COVID-19 pneumonia in children: from etiology to management. Front Pediatr. (2020) 8:616622. doi: 10.3389/fped.2020.616622
31. Lau CM, Adams NM, Geary CD, Weizman O-E, Rapp M, Pritykin Y, et al. Epigenetic control of innate and adaptive immune memory. Nat Immunol. (2018) 19:963–72. doi: 10.1038/s41590-018-0176-1
32. Netea MG, Domínguez-Andrés J, Barreiro LB, Chavakis T, Divangahi M, Fuchs E, et al. Defining trained immunity and its role in health and disease. Nat Rev Immunol. (2020) 20:375–88. doi: 10.1038/s41577-020-0285-6
33. Valiathan R, Ashman M, Asthana D. Effects of ageing on the immune system: infants to elderly. Scand J Immunol. (2016) 83:255–66. doi: 10.1111/sji.12413
34. Rahimi B, Vesal A, Edalatifard M. Coronavirus and its effect on the respiratory system: is there any association between pneumonia and immune cells. J Fam Med Prim care. (2020) 30:4729–35. doi: 10.4103/jfmpc.jfmpc_763_20
35. Root-Bernstein R. Age and location in severity of COVID-19 pathology: do lactoferrin and pneumococcal vaccination explain low infant mortality and regional differences? Bioessays. (2020) 42:e2000076. doi: 10.1002/bies.202000076
36. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. (2020) 323:1061–9. doi: 10.1001/jama.2020.1585
37. Wu Q, Xing Y, Shi L, Li W, Gao Y, Pan S, et al. Coinfection and other clinical characteristics of COVID-19 in children. Pediatrics. (2020) 146:e20200961. doi: 10.1542/peds.2020-0961
38. Zimmermann P, Curtis N. COVID-19 in children, pregnancy and neonates: a review of epidemiologic and clinical features. Pediatr Infect Dis J. (2020) 39:469–77. doi: 10.1097/INF.0000000000002700
39. Kim D, Quinn J, Pinsky B, Shah NH, Brown I. Rates of co-infection between SARS-CoV-2 and other respiratory pathogens. JAMA. (2020) 323:2085–6. doi: 10.1001/jama.2020.6266
40. Kumar N, Sharma S, Barua S, Tripathi BN, Rouse BT. Virological and immunological outcomes of coinfections. Clin Microbiol Rev. (2018) 31:e00111–17. doi: 10.1128/CMR.00111-17
41. Gonzalez AJ, Ijezie EC, Balemba OB, Miura TA. Attenuation of influenza A virus disease severity by viral coinfection in a mouse model. J Virol. (2018) 92:e00881–18. doi: 10.1128/JVI.00881-18
42. Nickbakhsh S, Mair C, Matthews L, Reeve R, Johnson PCD, Thorburn F, et al. Virus-virus interactions impact the population dynamics of influenza and the common cold. Proc Natl Acad Sci USA. (2019) 116:27142–50. doi: 10.1073/pnas.1911083116
43. Felsenstein S, Hedrich CM. SARS-CoV-2 infections in children and young people. Clin Immunol. (2020) 220:108588. doi: 10.1016/j.clim.2020.108588
44. Dalton CB, Corbett SJ, Katelaris AL. COVID-19: implementing sustainable low cost physical distancing and enhanced hygiene. Med J Aust. (2020) 212:443–46.e1. doi: 10.5694/mja2.50602
45. Chen J, Jiang Q, Xia X, Liu K, Yu Z. Individual variation of the SARS-CoV2 receptor ACE2 gene expression and regulation. Ageing Cell. (2020) 19:e13168. doi: 10.1111/acel.13168
46. Sharif-askari NS, Sharif-askari FS, Alabed M, Temsah M, Heialy S Al, Hamid Q, et al. Airways Expression of SARS-CoV-2 receptor, ACE2, and TMPRSS2 Is lower in children than adults and increases with smoking and COPD. Mol Ther Methods Clin Dev. (2020) 18:1–6. doi: 10.1016/j.omtm.2020.05.013
47. Sankar J, Dhochak N, Kabra SK, Lodha R. COVID-19 in children: clinical approach and management. Indian J Pediatr. (2020) 87:433–442. doi: 10.1007/s12098-020-03292-1
48. COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institute of Health (2020).
49. Fernández-Sarmiento J, Acevedo L, Mulett H, Bastidas S, Sarta M, Durán N, et al. Severe SARS-CoV-2 infection in critical care. Trends Anaesth Crit Care. (2020) 34:28–37. doi: 10.1016/j.tacc.2020.07.002
50. Yongchen Z, Shen H, Wang X, Shi X, Li Y, Yan J, et al. Different longitudinal patterns of nucleic acid and serology testing results based on disease severity of COVID-19 patients. Emerg Microbes Infect. (2020) 9:833–6. doi: 10.1080/22221751.2020.1756699
51. Stringhini S, Wisniak A, Piumatti G, Azman AS, Lauer SA, Baysson H, et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): a population-based study. Lancet. (2020) 396:313–9. doi: 10.1016/S0140-6736(20)31304-0
52. Long QX, Liu BZ, Deng HJ, Wu GC, Deng K, Chen YK, et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nature Med. (2020) 26:845–8. doi: 10.1038/s41591-020-0897-1
53. Rostad CA, Chahroudi A, Mantus G, Lapp SA, Teherani M, Macoy L, et al. Quantitative SARS-CoV-2 serology in children with Multisystem Inflammatory Syndrome (MIS-C). Pediatrics. (2020) 146:e2020018242. doi: 10.1542/peds.2020-018242
54. Lok C, Ho T, Oligbu P, Ojubolamo O, Pervaiz M. Clinical characteristics of children with COVID-19. AIMS Public Heal. (2020) 7:258–73. doi: 10.3934/publichealth.2020022
55. Pei Y, Liu W, Bilal I, Li F, Xie S. Comparing Chinese children and adults with RT-PCR positive COVID-19: a systematic review. J Infect Public Health. (2020) 13:1424–31. doi: 10.1016/j.jiph.2020.06.036
56. Patel NA. Pediatric COVID-19: Systematic review of the literature. Am J Otolaryngol Head Neck Med Surg. (2020) 41:102573. doi: 10.1016/j.amjoto.2020.102573
57. Castagnoli R, Votto M, Licari A, Brambilla I, Bruno R, Perlini S, et al. Severe Acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children and adolescents: a systematic review. JAMA Pediatr. (2020) 174:882–9. doi: 10.1001/jamapediatrics.2020.1467
58. Luo H, Liu S, Wang Y, Phillips- PA. Age differences in clinical features and outcomes in patients with COVID-19, Jiangsu, China: a retrospective, multicentre cohort study. BMJ Open. (2020) 10:e039887. doi: 10.1136/bmjopen-2020-039887
59. Chinese Medical Association. Recommendations for the diagnosis, prevention and control of the 2019 novel coronavirus infection in children (first interim edition). Chinese J Pediatr. (2020) 58:169–74. doi: 10.3760/cma.j.issn.0578-1310.2020.0004
60. Fialkowski A, Gernez Y, Arya P, Weinacht KG, Kinane TB, Yonker LM. Insight into the pediatric and adult dichotomy of COVID-19: Age-related differences in the immune response to SARS - CoV - 2 infection. Pediatr Pulmonol. (2020) 55:2556–64. doi: 10.1002/ppul.24981
61. Foust AM, Phillips GS, Chu WC, Daltro P, Das KM, Kilborn T, et al. International expert consensus statement on chest imaging in pediatric COVID-19 patient management: imaging findings, imaging study reporting and imaging study recommendations. Radiol Cardiothorac Imaging. (2020) 2:e200214. doi: 10.1148/ryct.2020200214
62. Das BB. Covid-19 and pulmonary hypertension in children: what do we know so far? Medicina. (2020) 56:716. doi: 10.3390/medicina56120716
63. Shekerdemian LS, Mahmood NR, Wolfe KK, Riggs BJ, Ross CE, Mckiernan CA, et al. Characteristics and outcomes of children with coronavirus disease 2019 (COVID-19) infection admitted to us and Canadian pediatric intensive care units. JAMA Pediatr. (2020) 174:868–73. doi: 10.1001/jamapediatrics.2020.1948
64. Götzinger F, Santiago-García B, Noguera-Julián A, Lanaspa M, Lancella L, Calò Carducci FI, et al. COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study. Lancet Child Adolesc Heal. (2020) 4:653–61. doi: 10.1016/S2352-4642(20)30177-2
65. Foust A, McAdam A, Chu W, Garcia-Peña P, Phillips G, Plut D, et al. Practical guide for pediatric pulmonologists on imaging management of pediatric patients with COVID-19. Pediatric Pulmonology. (2020) 55:2213–24. doi: 10.1002/ppul.24870
66. Oterino C, Alonso E, Andrés M, Buitrago N, Pérez A, Parrón M, et al. Pediatric chest x-ray in covid-19 infection. Eur J Radiol. (2020) 131:109236. doi: 10.1016/j.ejrad.2020.109236
67. Palabiyik F, Kokurcan SO, Hatipoglu N, Cebeci SO, Inci E. Imaging of COVID-19 pneumonia in children. Br J Radiol. (2020) 93:20200647. doi: 10.1259/bjr.20200647
68. Xia W, Shao J, Guo Y, Peng X, Li Z, Hu D. Clinical and CT features in pediatric patients with COVID-19 infection: different points from adults. Pediatr Pulmonol. (2020) 55:1169–74. doi: 10.1002/ppul.24718
69. Simpson S, Kay F, Abbara S, Bhalla S, Chung J, Chung M, et al. Radiological Society of North America expert consensus document on reporting chest CT findings related to COVID-19: endorsed by the society of thoracic radiology, the american college of radiology, and RSNA. Radiol Cardiothoracic Imaging. (2020) 2:e200152. doi: 10.1148/ryct.2020200152
70. Azadbakht J, Haghi-aminjan H, Farhood B. Chest CT findings of COVID-19-infected patients, are there differences between pediatric and adult patients? A systematic review. Egypt J Radiol Nucl Med. (2020) 51:145. doi 10.1186/s43055-020-00261-8
71. Chen Z, Fan H, Cai J, Li Y, Wu B, Hou Y, et al. High-resolution computed tomography manifestations of COVID-19 infections in patients of different ages. Eur J Radiol. (2020) 126:108972. doi: 10.1016/j.ejrad.2020.108972
72. Ludvigsson JF. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. (2020) 109:1088–95. doi: 10.1111/apa.15270
73. Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell. (2020) 181:281–92.e6. doi: 10.1016/j.cell.2020.02.058
74. Derespina KR, Kaushik S, Plichta A, Conway EE, Bercow A, Choi J, et al. Clinical manifestations and outcomes of critically ill children and adolescents with coronavirus disease 2019 in New York city. J Pediatr. (2020) 226:55–63. doi: 10.1016/j.jpeds.2020.07.039
75. Dequin P.-F, Heming N, Meziani F, Plantefève G, Voiriot G. Effect of hydrocortisone on 21-day mortality or respiratory support among critically Ill patients with COVID-19: a randomized clinical trial. JAMA. (2020) 324:1298–306. doi: 10.1001/jama.2020.16761
76. Zhou P, Yang X.-L, Wang XG, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. (2020) 579:270–3. doi: 10.1038/s41586-020-2012-7
77. Deville JG, Song E, Ouellette CP. Coronavirus Disease 2019 (COVID-19): Management in Children. UpToDate. (2020). Available online at: https://www.uptodate.com/contents/coronavirus-disease-2019-covid-19-management-in-children (accessed February 25, 2021).
78. Singh T, Heston SM, Langel SN, Blasi M, Hurst JH, Fouda GG, et al. Lessons from COVID-19 in children: key hypotheses to guide preventative and therapeutic strategies. Clin Infect Dis. (2020) 71:2006–13. doi: 10.1093/cid/ciaa547
79. RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. (2021) 384:693–704. doi: 10.1056/NEJMoa2021436
80. REMAP-CAP Investigators. Effect of hydrocortisone on mortality and organ support in patients with severe COVID-19 - The REMAP-CAP COVID-19 corticosteroid domain randomized clinical Trial. JAMA. (2020) 324:1317–29. doi: 10.1001/jama.2020.17022
81. Tomazini B, Maia I, Cavalcanti A, Berwanger O, Rosa R, Viega V. Effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19 - the CoDEX randomized clinical trial. JAMA. (2020) 324:1307–16. doi: 10.1001/jama.2020.17021
82. Lu R, Zhao X, Li J, Niu P, Yang B, Wu H, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. (2020) 395:565–74.doi: 10.1016/S0140-6736(20)30251-8
83. Zhikang Y, Rochwerg B, Mpharm YW, Adhikari N, Murthy S, Lamontagne F, et al. Treatment of patients with nonsevere and severe coronavirus disease 2019: an evidence-based guideline. CMAJ. (2020) 192:E536–45. doi: 10.1503/cmaj.200648
84. Piechotta V, Kl C, Sj V, Doree C, Monsef I, Em W, et al. Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: a living systematic review (Review). Cochrane Database Syst Rev. (2020) 7:CD013600. doi: 10.1002/14651858.CD013600.pub2
85. RECOVERY Collaborative Group. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet. (2020) 396:1345–52. doi: 10.1016/S0140-6736(20)32013-4
86. Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A trial of lopinavir–ritonavir in adults hospitalized with severe covid-19. N Engl J Med. (2020) 382:1787–99. doi: 10.1056/NEJMoa2001282
87. RECOVERY Collaborative Group. Effect of hydroxychloroquine in hospitalized patients with Covid-19. N Engl J Med. (2020) 383:2030–40. doi: 10.1056/NEJMoa2022926
88. Chowdhury S, Rathod J, Gernsheimer J. A rapid systematic review of clinical trials utilizing chloroquine and hydroxychloroquine as a treatment for COVID-19. Acad Emerg Med. (2020) 27:493–504. doi: 10.1111/acem.14005
89. Hernandez AV, Roman YM, Pasupuleti V, Barboza JJ, White CM. Hydroxychloroquine or chloroquine for treatment or prophylaxis of COVID-19. Ann Intern Med. (2020) 173:287–96. doi: 10.7326/M20-2496
90. Dulek DE, Fuhlbrigge RC, Tribble AC, Connelly JA, Loi MM, El Chebib H, et al. Multidisciplinary guidance regarding the use of immunomodulatory therapies for acute COVID-19 in pediatric patients. J Pediatr Infect Dis. Soc. (2020) 18: piaa098. doi: 10.1093/jpids/piaa098
91. REACT Working Group. Association between administration of systemic corticosteroids and mortality among critically Ill patients with COVID-19: a meta-analysis. JAMA. (2020) 324:1330–41. doi: 10.1001/jama.2020.17023
92. World Health Organization. Corticosteroids for COVID-19. 2020. Available online at: https://www.who.int/publications/i/item/WHO-2019-nCoV-Corticosteroids-2020.1 (accessed February 25, 2021).
93. Lamontagne F, Agoritsas T, Macdonald H, Leo Y, Diaz J, Agarwal A, et al. A living WHO guideline on drugs for covid-19. BMJ. (2020) 370:m3379. doi: 10.1136/bmj.m3379
94. Mair-Jenkins J, Saavedra-Campos M, Baillie JK, Cleary P, Khaw F, Lim WS, et al. The effectiveness of convalescent plasma and hyperimmune immunoglobulin for the treatment of severe acute respiratory infections of viral etiology: a systematic review and exploratory meta-analysis. J Infect Dis. (2015) 211:80–90. doi: 10.1093/infdis/jiu396
95. Organización Panamericana de la Salud/Organización Mundial de la Salud (OPS/OMS). Ongoing Living Update of COVID-19 Therapeutic Options: Summary of Evidence. (2020). Available online at: https://iris.paho.org/bitstream/handle/10665.2/52719/PAHOIMSEIHCOVID-19200030_eng.pdf?sequence=17&isAllowed=y (accessed January 27, 2021).
96. Ortiz-Prado E, Simbaña-Rivera K, Barreno LG-, Rubio-Neira M, Cevallos-Robalino D, Sanches-Sanmiguel H, et al. Clinical, molecular, and epidemiological characterization of the SARS-CoV-2 virus and the Coronavirus Disease 2019 (COVID-19), a comprehensive literature review. Diagn Microbiol Infect Dis. (2020) 98:115094. doi: 10.1016/j.diagmicrobio.2020.115094
97. Rabaan AA, Al-Ahmed SH, Sah R, Tiwari R, Yatoo MI, Patel SK, et al. SARS-CoV-2/COVID-19 and advances in developing potential therapeutics and vaccines to counter this emerging pandemic. Ann Clin Microbiol Antimicrob. (2020) 19:1–37. doi: 10.1186/s12941-020-00384-w
98. Korber B, Fischer WM, Gnanakaran S, Labranche CC, Saphire EO, Montefiori DC, et al. Tracking Changes in SARS-CoV-2 Spike: Evidencethat D614G Increases Infectivity of the COVID-19 virus. Cell. (2020) 812–27. doi: 10.1016/j.cell.2020.06.043
99. Kaur SP, Gupta V. COVID-19 vaccine: a comprehensive status report. Virus Res. (2020) 288:198114. doi: 10.1016/j.virusres.2020.198114
100. Food and Drugs Administration. Fact Sheet for Healthcare Providers: Emergency Use Authorization (EUA) of Veklury® (remdesivir). (2020). Available online at: https://www.accessdata.fda.gov/scripts/medwatch/index.cfm?action=reporting.home (accessed February 25, 2021).
Keywords: SARS-CoV-2, COVID-19, respiratory system, respiratory involvement, pneumonia, ARDS, children
Citation: Jurado Hernández JL and Álvarez Orozco IF (2021) COVID-19 in Children: Respiratory Involvement and Some Differences With the Adults. Front. Pediatr. 9:622240. doi: 10.3389/fped.2021.622240
Received: 28 October 2020; Accepted: 28 January 2021;
Published: 29 March 2021.
Edited by:
Mario Barreto, Sapienza University of Rome, ItalyReviewed by:
Ozgur Kasapcopur, Istanbul University-Cerrahpasa, TurkeyCopyright © 2021 Jurado Hernández and Álvarez Orozco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jenny Libeth Jurado Hernández, amp1cmFkb0BuZXVtb2xvZ2ljYS5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.