 Cristina Sanchez-Castañeda1,2
Cristina Sanchez-Castañeda1,2 Sandra Luis-Ruiz1,2Marta Ramon-Krauel2,3
Sandra Luis-Ruiz1,2Marta Ramon-Krauel2,3 Carles Lerin2,3Consuelo Sanchez4Núria Miró5Sònia Martínez6Maite Garolera7
Carles Lerin2,3Consuelo Sanchez4Núria Miró5Sònia Martínez6Maite Garolera7 Maria Angeles Jurado1,2*
Maria Angeles Jurado1,2*- 1Department of Clinical Psychology and Psychobiology, Institut de Neurociències, Universitat de Barcelona, Barcelona, Spain
- 2Institut de Recerca Sant Joan de Déu, Barcelona, Spain
- 3Endocrinology Department, Hospital Sant Joan de Déu, Barcelona, Spain
- 4Paediatric Endocrinology Unit, Consorci Sanitari de Terrassa, Terrassa, Spain
- 5Diabetes Education Unit, Consorci Sanitari de Terrassa, Terrassa, Spain
- 6Pharmacy and Nutrition Unit, Consorci Sanitari de Terrassa, Terrassa, Spain
- 7Neuropsychology Unit, Consorci Sanitari de Terrassa, Terrassa, Spain
Background: Individuals with obesity are known to present cognitive deficits, especially in executive functions. Executive functions play an important role in health and success throughout the whole life and have been related to food decision-making and to the ability to maintain energy balance. It is possible to improve executive functions through targeted training. This would involve brain plasticity changes that could be studied through connectivity MRI. The general hypothesis of this study is that executive functions training in children with obesity can improve food choices and produce cognitive and neuroimaging changes (structural and functional connectivity), as well as improve emotional state and quality of life.
Methods: Randomized controlled double-blind trial with 12-month follow-up. Thirty children with obesity will be randomly allocated into “executive training” (Cognifit with adaptive difficulty + Cogmed) or “control task” group (Cognifit without adaptive difficulty). Both groups will attend 30–45 min of individual gamified training (Cogmed and/or Cognifit systems) by iPad, five times per week during 6 weeks. Cogmed and Cognifit software are commercially available from Pearson and Cognifit, respectively. Participants will receive an iPad with both apps installed for a 6-week use. Participants will also receive counseling diet information via presentations sent to the iPad and will wear a Fitbit Flex 2 tracker to monitor daily activity and sleep patterns. Main outcomes will be cognitive, emotional, food decision, and quality-of-life measures, as well as neuroimaging measures. Participants are evaluated at baseline (T0), after treatment (T1), and 12 months since baseline (T2).
Discussion: Longitudinal study with active control group and 3 time points: baseline, immediately after treatment, and 1 year after baseline. Threefold treatment: executive function training, psychoeducation, and feedback on activity/sleep tracking. We will evaluate the transfer effects of the intervention, including emotional and functional outcomes, as well as the effects on neural plasticity by connectivity MRI.
Trial registration: This project has been registered in ClinicalTrials.gov (trial registration number NCT03615274), August 3, 2018.
Introduction
Childhood obesity is one of the most serious public health challenges of the 21st century. Its prevalence has increased at an alarming rate. Globally, in 2016 the number of children with overweight under the age of 5 was estimated to be over 41 million (1). Children with overweight or obesity are likely to stay obese into adulthood and more likely to develop noncommunicable diseases like type 2 diabetes and cardiovascular diseases at a younger age. Overweight and obesity, as well as their related diseases, are largely preventable. Prevention of childhood obesity, therefore, needs high priority (1). Furthermore, childhood obesity has long-term complications such as psychosocial and psychological problems (i.e., depression and low self-esteem) (2, 3).
Weight-loss programs in children have shown limited success, especially at long term (4). A better comprehension of vulnerability factors related to weight gain should provide valuable information for designing more effective treatments (5). In obesity, there is an imbalance between ingested and expended calories (6). On one hand, there is increased availability of energy-dense food that is high in fat; on the other hand, there is a decrease in physical activity. Therefore, novel interventions addressing both aspects of the problem are needed. Guidelines state that “treatment should focus on reducing caloric intake, increasing physical activity, modifying behavior (motivation and readiness to make behavioral and dietary changes), and including family members as active treatment participants” (2).
In addition, individuals with obesity have significant cognitive deficits, especially in executive functions (7). Executive functions are neuropsychological processes including decision-making, inhibitory control, and working memory. All of them are highly implicated in the cognitive control of eating impulses and in the ability to maintain energy balance, as well as in the motivation and adherence to a reduced-energy diet (8, 9). Inhibitory control is the most consistently reported to be impaired, although there is also impairment in reward sensitivity, attention/set-shifting, and working memory (10). Executive impairment also seems to be on the basis of some of the behaviors characteristic of obesity (i.e., increased food intake, disinhibited eating, and less physical activity). Therefore, it is a relevant factor to be considered in weight-loss interventions (11).
The mechanism by which obesity is associated with cognitive function is not clear yet. Smith et al. (12) suggested a bidirectional relationship, where obesity impairs executive functions by affecting cerebral tissue/mechanisms (such as brain inflammation and/or glucose abnormalities), and this impairment in executive functions has an influence in turn on obesity by causing an inability to regulate food intake, plan ahead, and inhibit responses and by promoting impulsive behavior (13, 14). If obesity exerts a detrimental effect on the brain, it is important to prevent obesity during brain development, particularly during the development of executive functions (10) that begins in early childhood and continues in adolescence, and has been attributed to the maturation of the prefrontal cortex (15).
It is possible to improve executive functions through targeted training. This targeted intensive cognitive training induces more effective neural system operations, providing cerebral plasticity (16). Executive functions and working memory training with game elements significantly improved working memory, but also motivation, training performance, and school performance in low-attending children (17, 18).
MRI can be used to assess changes in brain activity induced by training. Several weeks of daily executive function training enhanced working memory–related activity in middle frontal and intraparietal areas (19) and also produced changes in cortical thickness in young adults (20), thus showing that the neural systems underlying executive functions are plastic (21). Brain connectivity changes after training have also been reported in children (17) and adults (22, 23), and could predict body mass index (BMI) (24). However, even if neuroimaging could be a potential biomarker of responsiveness to treatment, changes in connectivity after obesity treatment (including cognitive training) have not been explored yet.
Lastly, children with obesity may experience more psychological disorders (self-concept, anxiety, and depression) (3) and reduced scores in quality of life (QoL) measures than normal-weight children (25). Treating executive deficits while fostering physical activity and promoting healthy nutritional habits may also help to improve QoL and emotional state.
This project has the purpose of evaluating the impact of executive functions training in BMI, food choice, and cognition in children with obesity as well as in their emotional state and QoL. These changes are expected to induce cerebral plasticity that will be measured by MRI connectivity. We hypothesize that children with obesity undergoing the cognitive training program will perform better than active controls in cognitive measures, take better food-related decisions, and consequently, show changes in brain connectivity, emotional state, and QoL measures at the end of the intervention and during the follow-up at 12 months. We also expect them to maintain BMI.
Materials and Methods
Study Design
The design is a randomized controlled double-blind trial with 12 months of follow-up. Patients meeting study criteria are randomly allocated according to a sequential number into the “executive functions training” or “control task training” groups after given written informed consent to the coordinator of the project (C.S.C). A sample of the informed consent can be found in Supplementary Material 1. Randomization is stratified by sex, age (9–12 years), and manual dominance. The same person is the one in charge of monitoring training compliance, so the rest of the team is blind to group allocation. All neuropsychological assessments are performed by an independent psychologist (S.L), blinded to group allocation. Patients and families are also blind to the study-group allocation. Because the intervention has no possible side effects, there are no circumstances under which unblinding is permissible. This protocol report follows the SPIRIT and CONSORT reporting guidelines (26, 27).
Trial Registration Dataset and Protocol Version
The trial has been retrospectively registered in ClinicalTrials.gov (https://clinicaltrials.gov/) on August 3, 2018. The last version of the protocol is the fourth version (March 25, 2020). Table 1 shows the study version history and a summary of the dataset information.
Table 1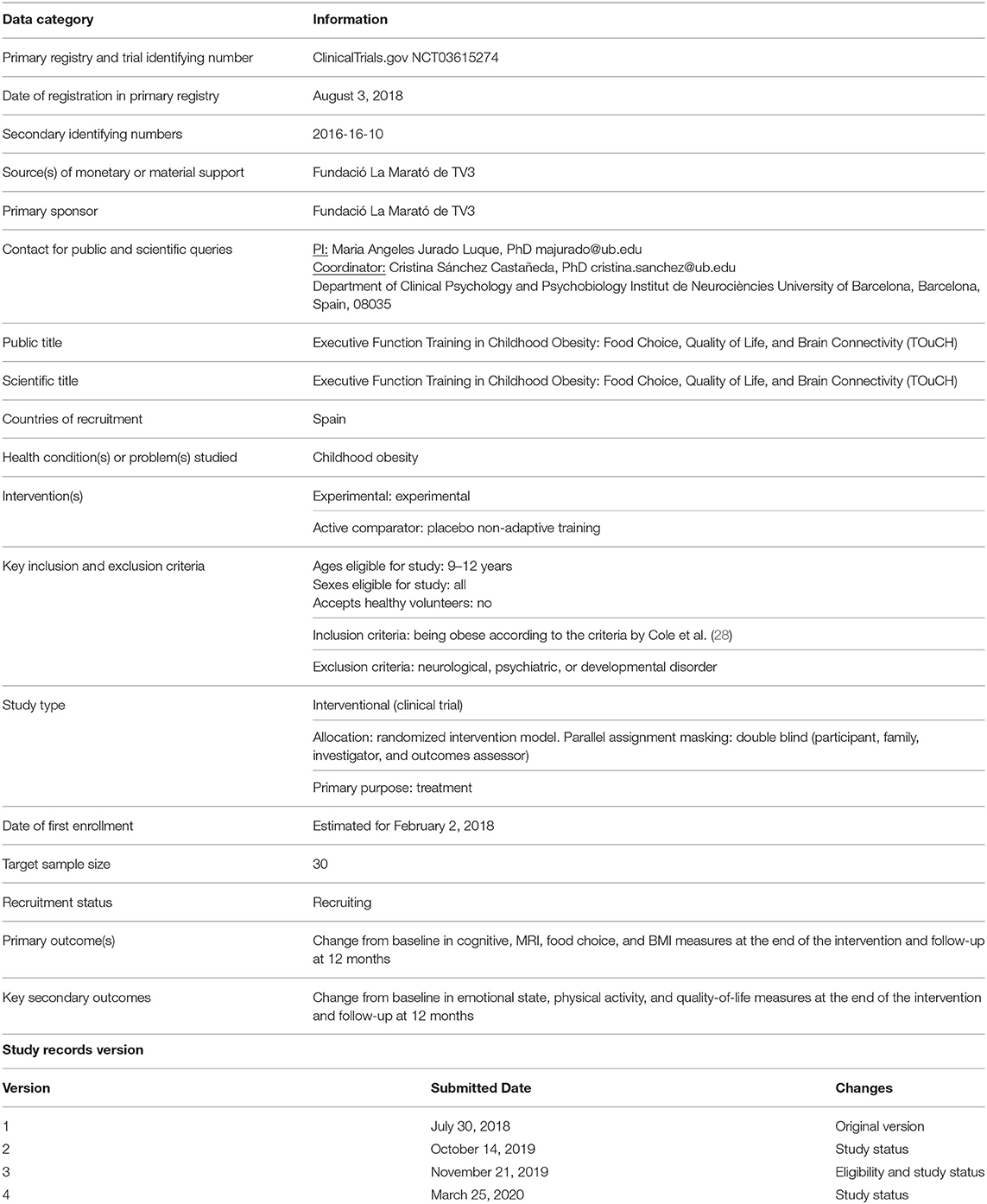
Table 1. Trial registration dataset.
Ethics Approval and Consent to Participate
Ethics approval was provided by the University of Barcelona Institutional Review Board (IRB00003099 protocol 122/V/2016), and by the Consorci Sanitari de Terrassa (02-17-503-039) and Sant Joan de Deu Hospital (PIC-02-19) Review Boards. The parents or legal tutors of all participants (in the presence of the children) gave written informed consent in accordance with the Declaration of Helsinki before enrollment. The trial has minimal risk because it has no adverse effects and it is based on commercially available training programs. Cogmed and Cognifit are commercially available from Pearson and Cognifit, respectively. Both programs have previous publications guaranteeing their efficacy (see next point). Furthermore, the IRB protocol (IRB00003099) from the University of Barcelona ensures that participation is voluntary, that participants could quit at any time they chose, that signed informed consent is obtained, that confidentiality is maintained, and that data security is rigorous. Participants will receive 20every time they come to the MRI to cover the travel expenses.
Any modifications to the protocol, which may impact on the conduct of the study, potential benefit of the patient or may affect patient safety, including changes of study objectives, study design, patient population, sample sizes, study procedures, or significant administrative aspects, will require a formal amendment to the protocol. Such amendment will be approved by the Ethics Committee/Institutional review board before implementation and notified to the participants and families.
Cogmed and Cognifit Evidence of Efficacy
According to Simons et al. (29) (pp. 143–148), “Cogmed Working Memory Training has been classified as one of the five commercial cognitive-training programs whose effectiveness had been assessed by several publications. The studies investigating the effects of Cogmed working memory training were undoubtedly the most numerous and best designed (e.g., often including active controls).” In addition, a recent independent meta-analysis by Aksayli et al. (30) evaluated the impact of Cogmed on people's cognitive and academic skills as a function of the type of transfer (near- or far-transfer). They used stricter inclusion criteria than previous meta-analysis (i.e., including a control group and excluding studies with subjective measures of cognitive/academic skills) to ensure a minimum standard of quality. They reviewed 50 independent studies, from a total of 2,761 records examined, and concluded that the training program increased performance on memory tasks immediately post-test (Hedge's g = 0.444) and this improvement remained significant after several months, although it slightly decreased (g = 0.365 at follow-up). Participants improved the most in those memory tasks whose demands and visual stimuli were very similar to the trained tasks (very-near-transfer; g = 0.566 and 0.487 immediately post-test and at follow-up, respectively), while there was a moderate effect on the participants' performance on those memory tasks not included in the training program (lesser-near-transfer; g = 0.246, p = 0.002 and g = 0.176, p = 0.005 at post-test and follow-up, respectively).
The Cognifit software has been however less studied. There are no independent studies to date including a sample of children. Therefore, we have assessed its efficacy according to independent studies on adult population. In a study by Siberski et al. (31), the effect of cognitive training vs. computer gaming was evaluated, and results showed that Cognifit significantly improved monitoring, planning, recognition, response time, shifting, spatial perception, visual memory, and visual scanning with medium-sized effects (Cohen's d ranged from 0.58 to 0.72) and naming, visual perception, and working memory with small effect sizes (d = 0.44, 0.37, and 0.41, respectively). However, the computer games group also showed an improvement in divided attention (Cohen's d = 0.85), inhibition (d = 0.67), recognition (d = 0.64), and updating (d = 0.44). In a study by Verghese et al. (32), assessing the effect of cognitive training on physical activity (concretely on gait speed), participants who underwent Cognifit training had an improvement in gait velocity during normal walking (p = 0.05; calculated Cohen's d = 0.65) and in walking while talking condition (p = 0.002; calculated Cohen's d = 1.15). Finally, an independent review by Shah et al. (33) classified Cognifit training program as delivering Level I evidence (at least two well-designed randomized control trials or quasi-randomized studies, one with high quality and the other at least of moderate quality as rated on a risk of bias score (PEDro score) and Cogmed as Level II evidence (at least one well-designed randomized control trials of high quality as rated on the PEDro score).
Study Sample and Setting
Participants will be children with obesity aged 9–12 years followed by an endocrinologist pediatrician at two hospitals located in the area of Barcelona: Consorci Sanitari de Terrassa and Hospital Sant Joan de Déu. We attempt to include children until we have a sample of 30 children with a complete training and post-training visit. The pediatric assessment will consist of height, weight, waist circumference, blood pressure, puberal state, and personal and familial history. Height and weight will be converted into BMI.
Inclusion and exclusion criteria are detailed in Figure 1. Participants should also have a stable wifi connection at home to be able to perform the training. Figure 2 shows the flow diagram of the study recruitment with the sample recruited to date.
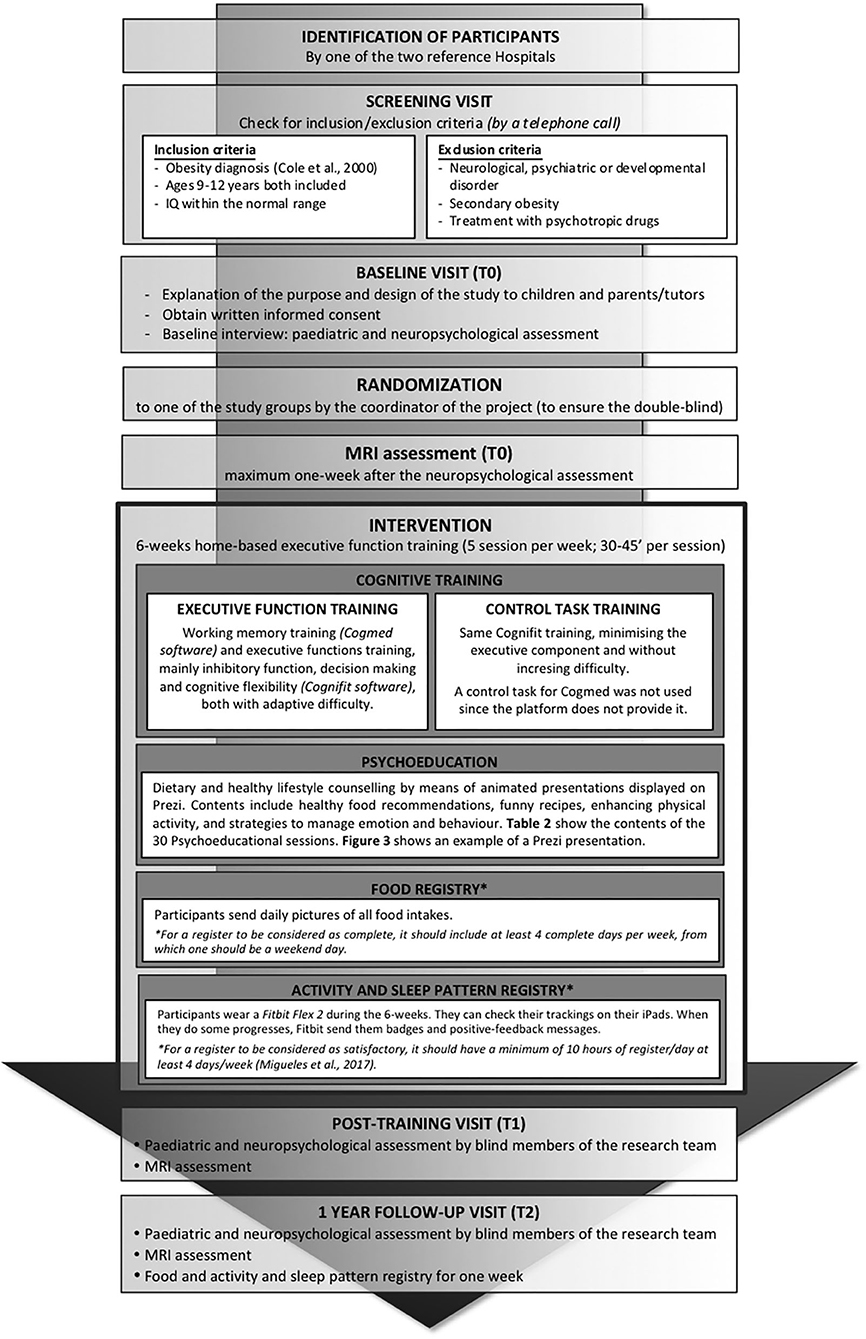
Figure 1. Diagram of the study protocol methods.
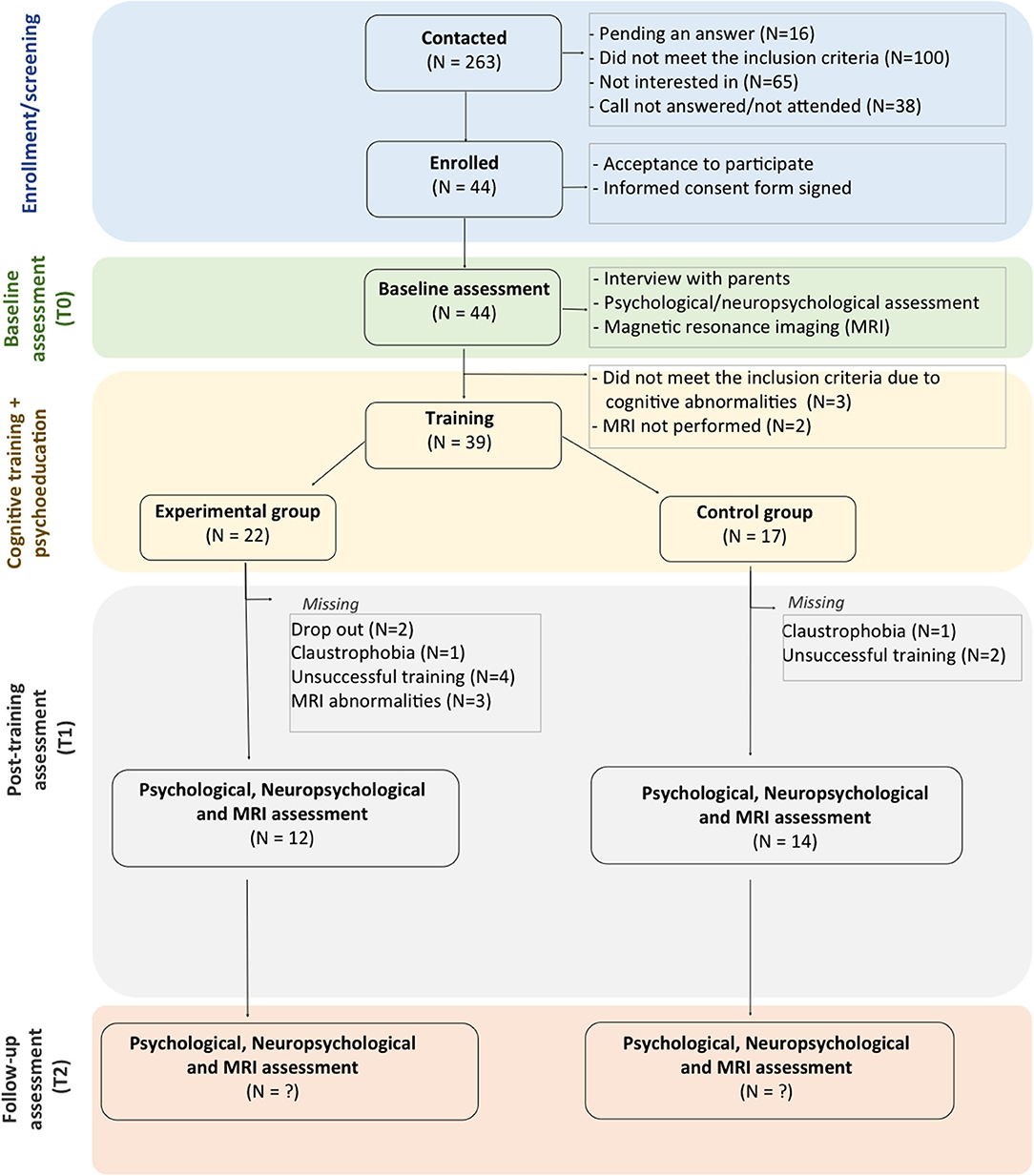
Figure 2. CONSORT flow diagram of study recruitment.
Sample Size
We attempt to achieve a total sample size of 30 subjects who have completed the treatment (training rate >70% of the days) and with a complete neuropsychological and MRI post-treatment assessment, 15 children per group. Previous literature on the field has shown significant results with similar sample sizes. Boutelle et al. (34) described a significant decrease in the percentage of eating (dppc2 = 0.6, medium effect size) and ingested kcal (dppc2 = 0.64, medium size), after training attention in a sample of 14 children (vs. 15 children doing a control task), showing far-transfer effect. Also, Verbeken et al. (35) reported a reduction in BMI (at 2-month follow-up; ηp2 = 0.16, dppc2 = 0.20, small effect) and improvement in short-term visual memory (Corsi block tapping task-forward; ηp2 = 0.13, dppc2 = 0.75, large effect), visual working memory (Corsi block-backwards; ηp2 = 0.14, dppc2 = 0.53, medium effect; BRIEF working memory; ηp2 = 0.10, dppc2 = 0.22), and meta-cognition (BRIEF; ηp2 = 0.12, dppc2 = 0.71) after training 22 children with obesity in visual working memory (vs. 22 children in passive control group). Also, Verbeken et al. (36) showed that an inhibition control and attentional training could significantly reduce inhibition problems (BRIEF; ηp2 = 0.26, dppc2 = 1.91, large effect) in a sample of 22 children with obesity (vs. 15 children in the passive control group).
In addition, multidisciplinary behavioral interventions have shown to produce significant decreases in BMI with similar sample sizes. Delgado-Rico et al. (37) showed a decrease in BMI (Cohen's d = 0.5, medium effect size) related with a decrease in impulsivity and inhibitory control in 42 adolescents. Also, Melnyk et al. (38) have shown a significant decrease in weight and BMI (large positive effect size, d = 1.5; p = 0.05) in a sample of 13 adolescents. Vignolo et al. (39) showed a significant reduction in standardized BMI (calculated Cohen's d = 1.75, large effect) and adjusted BMI (calculated Cohen's d = 0.66, medium effect) after a hospital-based multidisciplinary program, together with a reduction in waist circumference and improved family habits, emotional and social aspects, and motor skills in a sample of 20 children. Moens and Braet (40) showed a reduction in BMI after 6 months of parent-led cognitive-behavioral training in a sample of 31 children vs. 19 at waiting list [t(30) = 2.44, p = 0.021]. Finally, Gao et al. (41) assessed the effect of home-based exergaming (exercise with videogames) in 18 children compared with an active control group (n = 16), showing that cognitive flexibility improved (ηp2 = 0.19, medium effect size).
Regarding computerized cognitive training, especially those targeting working memory, executive function, and inhibitory control (which are the goal of this study), it may exert a positive effect on cognition assessed with similar sample sizes, concretely in visual, and/or verbal working memory at post-treatment (ηp2 = 0.21; dppc2 = 2.43, large effect size) (17, 42) and at follow-up [ηp2 = 0.18; dppc2 = 3.39, large effect size (42); dppc2 = 1.51, large effect (43)], in word fluency (dppc2 = 0.57, medium effect), in visuospatial complex memory (dppc2 = 0.97–1.08, large effect size) (44), in decision-making (healthy food, hypothetical shopping task) (ηp2 = 0.118, dppc2 = 0.65 and 0.44, medium effect), and in healthy food choice (real food task) (dppc2 = 0.65, medium effect) (45).
Interventions
Participants are provided with an iPad (5th generation, wifi) with all the apps needed for the training installed and a mail to contact the study coordinator (who is the only one aware of group allocation) if they have problems. The display of apps and contents in the iPads are remotedly controlled by Zuludesk (now Jamf SCHOOL; https://www.jamfschool.com/). Participants are also provided with a Fitbit Flex 2 (https://www.fitbit.com/flex2) to monitor physical activity and sleep patterns during the weeks of training. Figure 3 shows the materials given to the participants to undergo the training period: an iPad (5th generation) enrolled in the study with all the apps installed and a Fitbit Flex 2.

Figure 3. Materials provided to participants to follow the home-based training.
The coordinator of the study follows the adherence to the training on a daily basis, as well as ensures that participants send and synchronize the required information (pictures of the food intake and Fitbit synchronization). The intervention is threefold (see details in Figure 1).
Cognitive Training
All participants undergo a 6-week period of home-based executive function training, five sessions per week, with a duration of 30–45 min per session.
The executive functions training consists of working memory training by the Cogmed software (http://www.cogmed.com) and executive functions training (mainly inhibitory function, decision-making, and cognitive flexibility training) by Cognifit software (https://www.cognifit.com), both with adaptive difficulty. These apps are installed in the iPads provided to participants.
The control task training will consist of the same training by Cognifit software with non-adaptive difficulty, minimizing the executive component and without increasing difficulty. A control task training for Cogmed was not used because the platform does not provide it anymore.
Participants are asked to perform the training from Monday to Friday. If they cannot perform one or two sessions during the week, they are allowed to make up these sessions during the weekend. In the case of an occasional unfulfillment of the training, we offer the participants to rest 1 week more in training, so they can finish it satisfactorily. In any case, we will extend the training more than 1 week. In the baseline visit with the participants and families, we will also register the number of hours per day/week subjects use to play to other videogames to control for concomitant interventions.
The rest of the procedure will be the same for both groups.
Psychoeducation and Food Registry
During the 6 weeks of training, participants are required to send daily pictures of the food intakes to evaluate if the training exerts a change in the eating patterns. We will consider a weekly register as complete, when we have at least 4 days in a week complete, from which one should be a weekend day.
In addition, participants receive dietary and healthy lifestyle counseling by means of animated presentations displayed on Prezi (www.prezi.com). The purpose of those presentations are to encourage participants and their families to learn basic healthy habits by sending them daily presentations with a variety of contents that include healthy food recommendations, funny recipes, enhancing physical activity, and strategies to manage emotion and behavior. Table 2 show the contents of the 30 psychoeducational sessions. Figure 4 shows an example of a Prezi presentation.
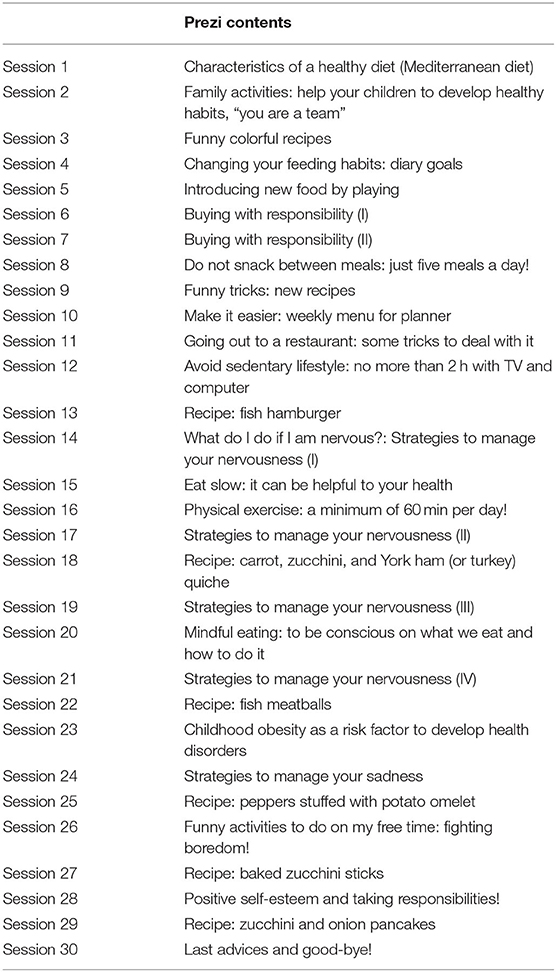
Table 2. Prezi contents.
Figure 4. Screenshots of a Prezi daily presentation.
Activity and Sleep Pattern Registry
Furthermore, to control for the effect that physical activity and sleep patterns may have on food decisions and BMI, we will register them over the training period by a Fitbit Flex 2. Participants can check their trackings on their iPads. When they do some progresses, Fitbit sends them badges and positive-feedback messages (https://blog.fitbit.com/fitbit-badges/). We consider a register as complete when it has at least 10 h of register/day at least 4 days/week (46).
Outcomes
We will assess the effect of the intervention on BMI, food choice, global cognition, and neural plasticity. Secondary measures will be emotion/behavior, QoL, and physical activity (see details of the registered protocols in Table 1). There will be three evaluation timepoints: (1) baseline assessment (T0); (2) post-training assessment (T1), which will be performed after the 6-week training period; and (3) 1-year follow-up assessment (T2), which will be done 12 months after T0, with a leeway of 1 month.
We will collect cognitive, psychological (emotional and quality of life measures), and MRI data in all three time points. Participants' parents will also be interviewed in T0 and T2. Socio-economical data from family, school information, and habits of nutrition and physical exercise from children will be obtained to characterize the sample.
Food, activity, and sleep hours registries will be collected during the 6 weeks of training and for a week at 12-month follow-up.
Anthropometric Measures
The pediatric assessment will consist of height, weight, waist circumference, blood pressure, puberal state, and personal and familial history. Height and weight will be converted into BMI.
BMI will be considered a primary measure.
Cognitive Assessment
The estimated verbal and visual IQ will be evaluated by the vocabulary and the matrix reasoning subtests of the Wechsler Intelligence Scale for Children—fifth edition (WISC-V Spanish version) (47) to control for potential differences in IQ between groups at baseline.
Attention and speed will be measured by the forward digit span and forward picture span (WISC-V), Children's Color Trail Test (CCTT) (48), the Five Digits Test (49), and Conners' Continuous Performance Test 3 (CPT3) (50).
The main subdomains comprising executive functions proposed by Diamond (2013) will be assessed. Cognitive flexibility will be evaluated by the Five Digits Test and the Children's Color Trail test (CCTT-2). Working memory will be assessed by the backward digit span (WISC-V), the backward picture span of the Weschler Non-verbal Scale (WNV) (51), and by an N-back task. Inhibitory control will be assessed by the Five Digits Test and a Go-no-go task. Planning will be measured by the Tower of London (52). Moreover, the Behavior Rating Inventory of Executive Function (BRIEF) will be administered (53).
We will consider global cognition as a primary measure. Attention and executive function subdomains will be further analyzed by a post-hoc analysis with Bonferroni correction for multiple comparisons.
Food Choice Registry
During the training period and for 1 week at 12 months' follow-up, participants will send pictures of the daily intake of food and drinks. These will be collected in tables quantifying the type of food per day and week. We will also administer the Kidmed questionnaire (54) at T0, T1, and T2.
A change in food choice will also be considered a primary measure.
QoL and Behavioral Measures
We will assess QoL by the Pediatric Quality of Life Inventory (PedsQL v4.0) (55) that includes parent- and self-reported scales of physical, emotional, social, and school functioning. Children's self-esteem and support perceived from classmates, parents, teachers, and friends is assessed by the Self-Perception and Social Support Profile for Children (56), and anxiety and depression by the Child Behavior Checklist (CBCL), a rating scale assessing behavioral and emotional symptoms in children (57) (www.aseba.org).
Changes in these measures will be considered secondary outcomes, resulting from a significant change in the previous ones (anthropometric and cognitive measures).
Connectivity Changes: MRI Assessment
All participants will undergo a 3T brain-MRI acquisition at baseline (T0), after treatment (T1), and after 12 months (T2). The scanning protocol will include structural and functional acquisitions. The MRI sequences will be the following: (1) high-resolution three-dimensional T1-weighted images acquired in the sagittal plane (MPRAGE sequence: TR = 2,400 ms, TE = 3.32 ms, TI = 1,000 ms, 256 slices, FOV = 224 mm; flip angle = 8°; 0.8 mm isotropic voxel); (2) 3D T2-weighted images in sagittal orientation (TR = 3,200 ms, TE = 298 ms, 256 slices, FOV = 224 mm; 0.9 mm isotropic voxel); (3) diffusion tensor imaging sequence (DTI) (single-shot diffusion-weighted EPI, b = 1,000 mm2/s, 30 directions, TR = 7,700 ms, TE = 89 ms, FOV = 244 mm; 2 mm isotropic voxel). Each direction will be acquired twice (AP and PA) and images will be averaged, improving signal-to-noise ratio; (4) resting state fMRI sequence (gradient-echo echo-planar imaging–EPI sequence) (240 volumes; 40 axial slices; TR = 2,500 ms; TE = 28 ms; FOV = 240 mm; flip angle = 80°; 3 mm isotropic voxel); (5) clinical sequences: a gradient T2 sequence (TR = 518 ms; TE = 20 ms; FOV = 240 mm; flip angle = 20°, voxel = 0.8 mm × 0.8 mm × 3 mm) and an axial FLAIR sequence (TR = 9,000 ms; TE = 96 ms; TI = 2,500 ms, FOV = 240 mm; flip angle = 150°, voxel = 0.9 mm × 0.9 mm × 3mm).
Brain plasticity will be assessed by computing brain connectivity through the analysis of DTI and resting-state fMRI sequences. It will be considered a primary measure. However, its analysis needs to be performed post-hoc with multiple comparisons' correction (FEW, FDR). Structural and clinical imaging (T1-, T2-weighted, and clinical sequences) are acquired to ensure that there are no significant baseline differences in brain structure between groups.
Data Analysis Plan
Demographic, Neuropsychological, and QoL Variables
For demographic variables, we will use a descriptive analysis of the variables and a comparative analysis between the training and control groups at baseline. We will use the χ2 test (and if this is not applicable, Fisher's exact) for categorical variables and Student's t-test (if not applicable, the Mann–Whitney U-test) for quantitative variables to check that randomization has successfully distributed the possible confounding variables (age, sex, IQ, manual dominance, socioeconomic, and educational status).
For the evaluation of the effectiveness of treatment on BMI and cognition, we will perform a general linear model for repeated measures analysis including these two variables as primary outcomes. We will perform further post-hoc analysis evaluating the effects on cognitive domains and emotional and QoL measures if appropriate. Means comparisons will be performed by Student's t-test, if the conditions of application are met and confounding variables have been well-controlled (otherwise, adjusted analyses will be performed by multiple regression). Multiple comparisons will be tested by Bonferroni correction. Effect size will also be calculated according to Hunter and Schmidt (58). All statistical tests will be carried using a two-sided test with the significance level set at 5% with the software Statistical Package for the Social Sciences (SPSS, version 24.0) or R (version 3.6.3).
Food Choice
To test our hypothesis that along the training weeks participants will make healthier and more balanced food choices, we will compute the content of the tables and analyze them by linear mixed models for longitudinal data. Multiple comparisons will be tested by Bonferroni correction. We will also assess the difference between groups at 12-month follow-up.
Imaging Data
To compute brain connectivity and perform graph-theoretical analysis, we need to preprocess MPRAGE, fMRI, and DTI data sets altogether. Thus, we can perform structural (by probabilistic or deterministic tractography) and functional connectivity analyses, i.e., parcellating the brain into functionally related areas using an atlas [i.e., the AAL atlas by (59)]. The mean time series of the obtained regions' voxels can be used to calculate cross-correlations between them, thus obtaining an n × n correlation matrix that represents each subject's connectivity profile.
To do that, we will segment the MPRAGE images by the automated FreeSurfer stream (version 5.3; available at https://surfer.nmr.mgh.harvard.edu/) into different cortical regions. With FSL [FMRIB's Software Library, http://www.fmrib.ox.ac.uk/fsl/; tract-based spatial statistics (TBSS) and tractography Diffusion Toolbox (FDT)], we will analyze the DTI dataset. After individual FA map extraction, a probabilistic tracking algorithm is used to estimate white matter pathways connecting different regions of interest. Again, a general linear model, correcting for multiple comparisons across space, will be used to compare differences among groups. Finally, we will preprocess functional images (fMRI) using FSL and AFNI (Analysis of Functional NeuroImages, https://afni.nimh.nih.gov/). An independent component analysis (ICA) can be carried out using tensorial independent component analysis as implemented in MELODIC part of FSL. This enables to obtain a set of independent components and identify the common resting-state functional networks (60).
Brain plasticity will be assessed by post hoc analysis with a correction for multiple comparisons (FWE, FDR).
Additional Analysis: Non-adherence or Missing Data
We will further analyze if discontinuation affects more one of the experimental groups, and we will also evaluate the baseline properties of the subjects that discontinue or perform the intervention at a non-successful level (reaching a number of essays/training days). Missing behavioral data can be handled by multiple imputation. However, in the case of missing, uncompleted, or artifacted MRI data, we will discard these subjects from the group analysis.
Missed trainings will be addressed by an intention-to-treat (ITT) approach to evaluate if they affect the results. Thus, we will analyze the available data by list-wise deletion without imputing the unknown values.
Details of the Sample Enrollment to Date
A total of 263 children and their families were contacted to participate in the study from the two areas covered by the two participating hospitals. From those, a total of 44 children and their families (16.73%) consented to participate in the study and underwent the first neuropsychological assessment. A total of 16 families are still pending on taking a decision regarding if participating or not; 100 did not meet the inclusion criteria, 65 families refused to participate in the study, and 38 families did not answer to our calls. From the 44 subjects assessed neuropsychologically, 3 children did not meet inclusion criteria for cognitive impairment, and 2 did not perform the MRI assessment. A total of 39 children were therefore randomly assigned to one of the training groups (88.6% of the ones who consented). To date, there are 22 children with a baseline visit in the experimental group and 17 in the control group. From those, 26 children to date completed the training (task completion more than 70%) and have both neuropsychological and MRI post-treatment assessments (66.6%). Five children more underwent only neuropsychological assessment (a total of 79.5%) due to claustrophobia or because of MRI abnormalities. A total of eight children (20.5%) dropped out or did not reach the minimum training requirements (at least a 70% of completion), six in the experimental group and two in the control group. We explain this higher dropout rate in the experimental group due to the increasing difficulty in the training tasks. This results in a 79.5% retention rate with a training completion of at least 70%.
Discussion
Confidentiality and Data Management
Personal information about potential and enrolled participants will only be stored at the trial site and be subject to privacy policy. All data will be treated anonymously (with a trial code) and introduced in a database stored in an institutional server that requires accreditation and password to be accessed. Personal information will not be shared and will be deleted after the trial.
A second blind researcher will ensure accuracy of data in the database and will perform a preliminary analysis of data to ensure it distributes on a normal range. All missing data or outliers will be double checked with the original source of information. Data analysis will only be performed with anonymized data by accredited researchers. After trial publication, trial data will be shared in anonymized form on justified request.
Discontinuation
A patient may withdraw from the study at any time, at his or her parents' request, for any reason without penalty or loss of benefits. In any case, all patients will be followed up at each assessment time point after discontinuation according to the intention-to-treat principle. In the event of withdrawal of consent, data will be deleted if requested.
Patient and Public Involvement
A pool of patients and families were involved in the design of psychoeducation materials by participating in an assessment of information needs assessment previous to the development of the study. The results of the needs assessment were used to build the psychoeducation sessions contents. Furthermore, during the training period, children are asked on a daily basis about their satisfaction with the training and the level of compliance and burden of it. Motivation pre-intervention and satisfaction post-intervention are also assessed.
Dissemination Policy
We will disseminate the results from this study via conference presentations and journal publications. The results of the project will be also presented in a Symposium organized by La Marató de TV3 that the Foundation organizes every year (https://www.ccma.cat/tv3/marato/en/recerca/) addressed to the general audience. Article journal will focus on (1) the post-training effects on the cognitive, emotional, and QoL measures; (2) the post-training effects on MRI connectivity; (3) the post-training effect on food choice; and (4) the 1-year effect on the previous measures. We would expect to find a post-training effect that hopefully will maintain at 1-year follow-up. In case we find that the treatment is effective, we will analyze which elements are the most effective to design further interventional studies and to transfer the effect to the clinics.
Ethics Statement
The studies involving human participants were reviewed and approved by University of Barcelona Institutional Review Board (IRB00003099 protocol 122/V/2016), Consorci Sanitari de Terrassa Review Board (02-17-503-039), and Sant Joan de Deu Hospital Review Board (PIC-02-19). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
CS-C, SL-R, MAJ, and MG contributed to the conception and acquisition of data and will analyze and interpret data. MR-K, CL, CS, NM, and SM contributed to the patients' selection. CS-C contributed to drafting the work and the rest of co-authors to revising it critically. All authors approved the final version of the paper and agreed to be accountable for all aspects of the work and ensure the accuracy and integrity of it.
Funding
This work was supported by the Marató de TV3 Foundation grant number 201616-10 (https://www.ccma.cat/tv3/marato/en/recerca/), by the Agència de Gestió d'Ajuts Universitaris i de Recerca (AGAUR) from Generalitat de Catalunya grant number 2017SGR0748, and by a predoctoral grant from AGAUR grant number FI-DGR 2018 to SL-R. These funding sources have no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results. This study was possible thanks to the collaboration of patients with obesity and families.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2021.551869/full#supplementary-material
Abbreviations
AAL, automated anatomical labeling; AFNI, analysis of functional neuroimages; BMI, body mass index; BRIEF, Behavior Rating Inventory of Executive Function; CBCL, Child Behavior Checklist; CCTT, Children's Color Trail Test; CPT3, Continuous Performance Test, 3rd version; DTI, diffusion tensor imaging; EPI, echo-planar imaging; FA, fractional anisotropy; FDT, FMRIB's diffusion toolbox; FLAIR, fluid attenuation inversion recovery; fMRI, functional magnetic resonance imaging; FSL, FMRIB's software library; ICA, independent component analysis; IQ, intelligence quotient; IRB, institutional review board; MD, mean diffusivity; MELODIC, Multivariate Exploratory Linear Optimized Decomposition into Independent Components; MPRAGE, magnetization-prepared rapid acquisition with gradient echo; PedsQL, Pediatric quality of life; QoL, quality of life; SPSS, Statistical Package for the Social Sciences; T0, baseline assessment; T1, post-training assessment; T2, 12-month follow-up assessment; TBSS, tract-based spatial statistics; WISC-V, Weschler Intelligence Scale for Children, fifth edition; WNV, Weschler Non-verbal Scale.
References
1. World Health Organization. Child Overweight and Obesity. (2020). Available online at: https://www.who.int/dietphysicalactivity/childhood/en/ (accessed February 25, 2020).
2. Acosta MC, Manubay J, Levin FR. Pediatric obesity: parallels with addiction and treatment recommendations. Harv Rev Psychiatry. (2008) 16:80–96. doi: 10.1080/10673220802069764
3. Topçu S, Orhon FS, Tayfun M, Uçaktürk SA, Demirel F. Anxiety, depression and self-esteem levels in obese children: a case-control study. J Pediatr Endocrinol Metab. (2016) 29:357–61. doi: 10.1515/jpem-2015-0254
4. Turk MW, Yang K, Hravnak M, Sereika SM, Ewing LJ, Burke LE. Randomized clinical trials of weight loss maintenance: a review. J Cardiovasc Nurs. (2009) 24:58–80. doi: 10.1097/01.JCN.0000317471.58048.32
5. Stice E, Burger KS, Yokum S. Reward region responsivity predicts future weight gain and moderating effects of the TaqIA allele. J Neurosci. (2015) 35:10316–24. doi: 10.1523/JNEUROSCI.3607-14.2015
6. Townshend T, Lake A. Obesogenic environments: current evidence of the built and food environments. Perspect Public Health. (2017) 137:38–44. doi: 10.1177/1757913916679860
7. Yang Y, Shields GS, Guo C, Liu Y. Executive function performance in obesity and overweight individuals: a meta-analysis and review. Neurosci Biobehav Rev. (2018) 84:225–44. doi: 10.1016/j.neubiorev.2017.11.020
8. Appelhans BM, French SA, Pagoto SL, Sherwood NE. Managing temptation in obesity treatment: a neurobehavioral model of intervention strategies. Appetite. (2016) 96:268–79. doi: 10.1016/j.appet.2015.09.035
9. Stingl KT, Kullmann S, Ketterer C, Heni M, Häring HU, Fritsche A, et al. Neuronal correlates of reduced memory performance in overweight subjects. Neuroimage. (2012) 60:362–9. doi: 10.1016/j.neuroimage.2011.12.012
10. Reinert KR, Poe EK, Barkin SL. The relationship between executive function and obesity in children and adolescents: a systematic literature review. J Obes. (2013) 2013:820956. doi: 10.1155/2013/820956
11. Liang J, Matheson BE, Kaye WH, Boutelle KN. Neurocognitive correlates of obesity and obesity-related behaviors in children and adolescents. Int J Obes. (2014) 38:494–506. doi: 10.1038/ijo.2013.142
12. Smith E, Hay P, Campbell L, Trollor JN. A review of the association between obesity and cognitive function across the lifespan: implications for novel approaches to prevention and treatment. Obes Rev. (2011) 12:740–55. doi: 10.1111/j.1467-789X.2011.00920.x
13. Ottino-González J, Jurado MA, García-García I, Caldú X, Prats-Soteras X, Tor E, et al. Allostatic load and executive functions in overweight adults. Psychoneuroendocrinology. (2019) 106:165–70. doi: 10.1016/j.psyneuen.2019.04.009
14. Cortese S, Comencini E, Vincenci B, Speranza M, Angriman M. Attention- deficit/hyperactivity disorder and impairment in executive functions: a barrier to weight loss in individuals with obesity?. BMC Psychiatry. (2013) 13:286. doi: 10.1186/1471-244X-13-286
15. Diamond A. Executive functions. Annu Rev Psychol. (2013) 64:135–68. doi: 10.1146/annurev-psych-113011-143750
16. Brooks SJ. A debate on working memory and cognitive control: can we learn about the treatment of substance use disorders from the neural correlates of anorexia nervosa?. BMC Psychiatry. (2016) 16:10. doi: 10.1186/s12888-016-0714-z
17. Astle DE, Barnes JJ, Baker K, Colclough GL, Woolrich MW. Cognitive training enhances intrinsic brain connectivity in childhood. J Neurosci. (2015) 35:6277–83. doi: 10.1523/JNEUROSCI.4517-14.2015
18. Cardoso CDO, Dias N, Senger J, Colling APC, Seabra AG, Fonseca RP. Neuropsychological stimulation of executive functions in children with typical development: a systematic review. Appl Neuropsychol Child. (2018) 7:61–81. doi: 10.1080/21622965.2016.1241950
19. Olesen PJ, Westerberg H, Klingberg T. Increased prefrontal and parietal activity after training of working memory. Nat Neurosci. (2004) 7:75–9. doi: 10.1038/nn1165
20. Román FJ, Lewis LB, Chen CH, Karama S, Burgaleta M, Martínez K, et al. Gray matter responsiveness to adaptive working memory training: a surface-based morphometry study. Brain Struct Funct. (2016) 221:4369–82. doi: 10.1007/s00429-015-1168-7
21. Klingberg T. Development of a superior frontal-intraparietal network for visuo-spatial working memory. Neuropsychologia. (2006) 44:2171–7. doi: 10.1016/j.neuropsychologia.2005.11.019
22. Takeuchi H, Taki Y, Nouchi R, Hashizume H, Sekiguchi A, Kotozaki Y, et al. Effects of working memory training on functional connectivity and cerebral blood flow during rest. Cortex. (2013) 49:2106–25. doi: 10.1016/j.cortex.2012.09.007
23. Thompson TW, Waskom ML, Gabrieli JD. Intensive working memory training produces functional changes in large-scale frontoparietal networks. J Cogn Neurosci. (2016) 28:575–88. doi: 10.1162/jocn_a_00916
24. Park BY, Seo J, Yi J, Park H. Structural and functional brain connectivity of people with obesity and prediction of body mass index using connectivity. PLoS One. (2015) 10:e0141376. doi: 10.1371/journal.pone.0141376
25. Varni JW. The PedsQL: Measurement Model for the Pediatric Quality of Life Inventory. Mapi Research Trust (2007) (Spanish Version).
26. Chan A-W, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, KrleŽa-Jerić K, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. (2013) 158:200–7. doi: 10.7326/0003-4819-158-3-201302050-00583
27. Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c332. doi: 10.1136/bmj.c332
28. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. (2000) 320:1240–3. doi: 10.1136/bmj.320.7244.1240
29. Simons DJ, Boot WR, Charness N, Gathercole SE, Chabris CF, Hambrick DZ, et al. Do “Brain-Training” Programs Work? Psychol Sci Public Interest. (2016) 17:103–86. doi: 10.1177/1529100616661983
30. Aksayli N, Sala G, Gobet F. The cognitive and academic benefits of Cogmed: a meta-analysis. Educ Res Rev. (2019) 27:229–43. doi: 10.1016/j.edurev.2019.04.003
31. Siberski J, Shatil E, Siberski C, Eckroth-Bucher M, French A, Horton S, et al. Computer-based cognitive training for individuals with intellectual and developmental disabilities: pilot study. Am J Alzheimers Dis Other Demen. (2015) 30:41–8. doi: 10.1177/1533317514539376
32. Verghese J, Mahoney J, Ambrose AF, Wang C, Holtzer R. Effect of cognitive remediation on gait in sedentary seniors. J Gerontol A Biol Sci Med Sci. (2010) 65:1338–43. doi: 10.1093/gerona/glq127
33. Shah TM, Weinborn M, Verdile G, Sohrabi HR, Martins RN. Enhancing cognitive functioning in healthy older adults: a systematic review of the clinical significance of commercially available computerized cognitive training in preventing cognitive decline. Neuropsychol Rev. (2017) 27:62–80. doi: 10.1007/s11065-016-9338-9
34. Boutelle KN, Kuckertz JM, Carlson J, Amir N. A pilot study evaluating a one session attention modification training to decrease overeating in obese children. Appetite. (2014) 76:180–5. doi: 10.1016/j.appet.2014.01.075
35. Verbeken S, Braet C, Goossens L, van der Oord S. Executive function training with game elements for obese children: a novel treatment to enhance self-regulatory abilities for weight-control. Behav Res Ther. (2013) 51:290–9. doi: 10.1016/j.brat.2013.02.006
36. Verbeken S, Braet C, Naets T, Houben K, Boendermaker W. Computer training of attention and inhibition for youngsters with obesity: a pilot study. Appetite. (2018) 123:439–47. doi: 10.1016/j.appet.2017.12.029
37. Delgado-Rico E, Río-Valle JS, Albein-Urios N, Caracuel A, González-Jiménez E, Piqueras MJ, et al. Effects of a multicomponent behavioral intervention on impulsivity and cognitive deficits in adolescents with excess weight. Behav Pharmacol. (2012) 23:609–15. doi: 10.1097/FBP.0b013e328356c3ac
38. Melnyk BM, Small L, Morrison-Beedy D, Strasser A, Spath L, Kreipe R, et al. The COPE Healthy Lifestyles TEEN program: feasibility, preliminary efficacy, and lessons learned from an after school group intervention with overweight adolescents. J Pediatr Health Care. (2007) 21:315–22. doi: 10.1016/j.pedhc.2007.02.009
39. Vignolo M, Rossi F, Bardazza G, Pistorio A, Parodi A, Spigno S, et al. Five-year follow-up of a cognitive-behavioural lifestyle multidisciplinary programme for childhood obesity outpatient treatment. Eur J Clin Nutr. (2008) 62:1047–57. doi: 10.1038/sj.ejcn.1602819
40. Moens E, Braet C. Training parents of overweight children in parenting skills: a 12-month evaluation. Behav Cogn Psychother. (2012) 40:1–18. doi: 10.1017/S1352465811000403
41. Gao Z, Lee JE, Zeng N, Pope ZC, Zhang Y, Li X. Home-based exergaming on preschoolers' energy expenditure, cardiovascular fitness, body mass index and cognitive flexibility: a randomized controlled trial. J Clin Med. (2019) 8:1745. doi: 10.3390/jcm8101745
42. Karbach J, Strobach T, Schubert T. Adaptive working-memory training benefits reading, but not mathematics in middle childhood. Child Neuropsychol. (2015) 21:285–301. doi: 10.1080/09297049.2014.899336
43. Pugin F, Metz AJ, Stauffer M, Wolf M, Jenni OG, Huber R. Working memory training shows immediate and long-term effects on cognitive performance in children. F1000Res. (2015) 3:82. doi: 10.12688/f1000research.3665.3
44. Nevo E, Breznitz Z. Effects of working memory and reading acceleration training on improving working memory abilities and reading skills among third graders. Child Neuropsychol. (2014) 20:752–65. doi: 10.1080/09297049.2013.863272
45. Porter L, Bailey-Jones C, Priudokaite G, Allen S, Wood K, Stiles K, et al. From cookies to carrots; the effect of inhibitory control training on children's snack selections. Appetite. (2018) 124:111–23. doi: 10.1016/j.appet.2017.05.010
46. Migueles JH, Cadenas-Sanchez C, Ekelund U, Nyström CD, Mora-Gonzalez J, Löf M, et al. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: a systematic review and practical considerations. Sports Med. (2017) 47:1821–45. doi: 10.1007/s40279-017-0716-0
47. Weschler D. Wechsler Intelligence Scale for Children, 5th edn. Madrid: Pearson SA (2015) (Spanish Version).
48. Llorente AM, Williams J, Satz P, D'Elia LF. (2003). Children's Color Trails Test. PAR, Psychological Assessment Resources Inc.
52. Shallice T. Specific impairments of planning. Philos Trans R Soc Lond B Biol Sci. (1982) 298:199–209. doi: 10.1098/rstb.1982.0082
54. Serra Majem L, Ribas Barba L, Ngo de la Cruz J, Ortega Anta RM, Pérez Rodrigo C, Aranceta Bartrina J. Alimentación, jóvenes y dieta mediterránea enEspaña. In: Serra Majem L, Aranceta Bartrina J, editors. Desarrollo del KIDMED, Índice de Calidad de la Dieta Mediterráena en la Infancia y la Adolescencia, Alimentación Infantil y Juvenil. Barcelona: Masson (2004). p. 51–9.
55. Varni JW, Seid M, Rode CA. The PedsQL: measurement model for the pediatric quality of life inventory. Med Care. (1999) 37:126–39. doi: 10.1097/00005650-199902000-00003
56. Harter S, Broc MA. Perfil de Autoconcepto, Autoestima, y Apoyo Social Para Adolescentes. (2000). Madrid: COSPA (Spanish Version).
57. Achenbach TM. Child Behaviour Checklist (CBCL). (2001). Available online at: www.aseba.org (accessed February 25, 2020) (Spanish Version).
58. Hunter JE, Schmidt FL. Methods of Meta-Analysis: Correcting Error and Bias in Research Findings. California, CA: Sage Publications, Inc.; Teller Road Thousand Oaks (2004).
59. Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage. (2002) 15:273–89. doi: 10.1006/nimg.2001.0978
Keywords: childhood obesity, cognitive training, executive function, quality of life, neuroimaging, magnetic resonance, connectivity, decision making
Citation: Sanchez-Castañeda C, Luis-Ruiz S, Ramon-Krauel M, Lerin C, Sanchez C, Miró N, Martínez S, Garolera M and Jurado MA (2021) Executive Function Training in Childhood Obesity: Food Choice, Quality of Life, and Brain Connectivity (TOuCH): A Randomized Control Trial Protocol. Front. Pediatr. 9:551869. doi: 10.3389/fped.2021.551869
Received: 14 April 2020; Accepted: 19 January 2021;
Published: 24 February 2021.
Edited by:
Madhusmita Misra, Massachusetts General Hospital and Harvard Medical School, United StatesReviewed by:
Anita Morandi, Integrated University Hospital Verona, ItalyJordan Sherwood, Massachusetts General Hospital and Harvard Medical School, United States
Copyright © 2021 Sanchez-Castañeda, Luis-Ruiz, Ramon-Krauel, Lerin, Sanchez, Miró, Martínez, Garolera and Jurado. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Angeles Jurado, bWFqdXJhZG9AdWIuZWR1