
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pediatr. , 30 October 2020
Sec. Pediatric Cardiology
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.596840
This article is part of the Research Topic Heart Failure in Pediatrics and Congenital Heart Disease View all 17 articles
 Emmi Helle1,2*
Emmi Helle1,2* Jaana Pihkala1Riitta Turunen1Hanna Ruotsalainen3Sari Tuupanen4,5Juha Koskenvuo4,5
Jaana Pihkala1Riitta Turunen1Hanna Ruotsalainen3Sari Tuupanen4,5Juha Koskenvuo4,5 Tiina Ojala1
Tiina Ojala1Myocardial dysfunction is a known risk factor for morbidity and mortality in hypoplastic left heart syndrome (HLHS). Variants in some transcription factor and contractility genes, which are known to cause cardiomyopathy, have previously been associated with impaired right ventricular function in some HLHS patients. The care of HLHS patients is resource demanding. Identifying genetic variants associated with myocardial dysfunction would be helpful in tailoring the follow-up and therapeutic strategies. We tested whether a commercial cardiomyopathy gene panel could serve as a diagnostic tool in a Finnish cohort of HLHS patients with impaired right ventricular function to identify potentially pathogenic variants associated with poor prognosis. None of the patients had pathogenic or likely pathogenic variants in the studied cardiomyopathy-associated genes. Thus, our approach of performing a cardiomyopathy gene panel to identify pathogenic variants as directly causal or as modifiers for worse outcomes in hypoplastic left heart syndrome is not useful in clinical practice at the moment.
Congenital heart defects (CHD), structural defects of the heart and great vessels, are the most common congenital malformations affecting nearly 1% of the population (1, 2). Hypoplastic left heart syndrome (HLHS) is a severe form of CHD where there is atrioventricular and ventriculoarterial (AV/VA) concordance with mitral and aortic stenosis or atresia and left ventricular hypoplasia rendering the left side unable to support the systemic circulation. The palliative treatment strategy for HLHS consists of three operations: (1) the Norwood procedure shortly after birth, (2) the Bi-directional Glenn operation, which is usually performed at 4–6 months of age, and (3) the Fontan procedure usually performed at 2–4 years of age. In HLHS, the right ventricle acts as the systemic ventricle. Myocardial dysfunction is a known risk factor for morbidity and mortality in HLHS patients throughout the treatment protocol (3, 4). The etiology of myocardial dysfunction is poorly understood. Potential risk factors include changes in hemodynamic stress during the different palliation stages, residual anatomic obstructions, arrhythmias, valve insufficiencies, myocardial ischemia, and genetic predisposition (5). In addition, the right ventricular myocardial microarchitecture is not optimized to serve the systemic circulation, which might contribute to pathogenesis (6).
While impaired chamber flow due to outflow tract obstruction and primary deficiencies in myocardial growth during early cardiac development are potential etiologic contributors to HLHS, a genetic component plays a role in disease development. Identifying gene variants associated with HLHS has been challenging. According to previous studies, about 10% of non-syndromic HLHS is likely monogenic (7), NOTCH1 being the predominant monogenic cause (8–12). However, in most cases, the inheritance pattern is complex. Potentially pathogenic variants in a handful of genes associated with cardiomyopathy, especially MYH6, have been associated with both the development of congenital heart defects and the disease course in the form of impaired myocardial dysfunction in these patients (13–15).
Identifying genetic variants that increase the risk for poor ventricular function in HLHS would lead to optimized follow-up and care. To identify such variants, we performed a commercial cardiomyopathy gene panel sequencing in a cohort of HLHS patients with impaired right ventricle function.
The study was conducted at Children's Hospital, Helsinki University Hospital, Finland. The study protocol was approved by the Ethics Board of Helsinki and Uusimaa Hospital District (Biomedicum Helsinki 2, Tukholmankatu 8, 00290 Helsinki, Finland). Written informed consent was obtained from the legal guardians of the participants and also directly from all participants aged over 6 years.
From a national cohort of all 134 hypoplastic left heart syndrome patients born in Finland between 1/1998 and 9/2012, we identified 10 non-syndromic patients with impaired right ventricular function, but no clear anatomic problem explaining the impairment (Table 1). The patients did not have extra-cardiac anomalies. All patients were of self-reported Finnish origin. Clinical data were collected from hospital records. Right ventricle ejection fraction was reported from cardiac magnetic resonance imaging data, when available, otherwise as Simpson's Biplane ejection fraction calculated from echocardiography data. Three patients did not have numeric data on the ejection fraction, but the right ventricle dysfunction was described qualitatively. Four patients underwent heart transplantation.
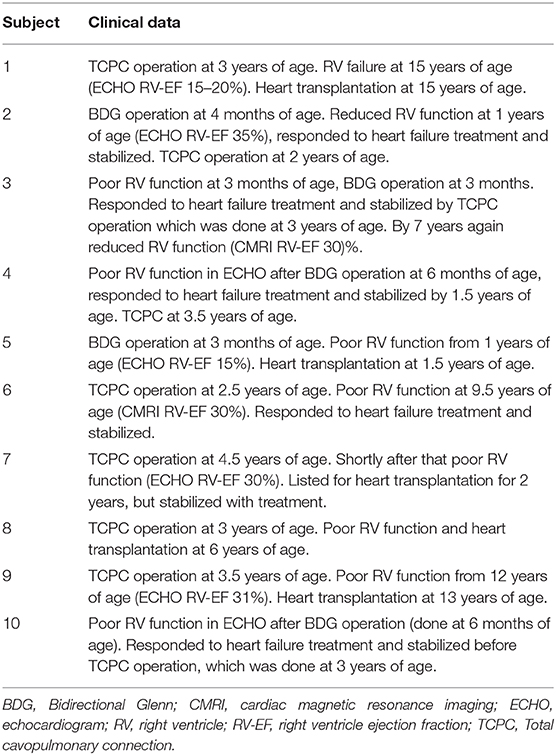
Table 1. Clinical characteristics of HLHS study subjects.
DNA was extracted from peripheral blood or saliva samples. DNA was analyzed by next-generation sequencing using a targeted commercial cardiomyopathy panel including 103 genes by Blueprint Genetics Ltd. (listed in Supplementary Table 1). The gene panel includes well-known disease genes based on curated gene reviews and variant databases [Clinical Genomic Database (CGD; National Human Genome Research Institute/NIH), ClinGen—Clinical Genome Resource, DECIPHER/DD2GP, BabySeq Project (G2P), HGMD, and ClinVar], and newly identified disease-causing genes from peer-reviewed publications with functional evidence of pathogenicity. Synonymous variants and variants with a minor allele frequency over 0.01 in any subpopulation of gnomAD (16) were excluded. Variants were evaluated for their pathogenicity using in silico tools (Mutation Taster, SIFT, and PolyPhen-2), amino acid conservation in species and existing public and private mutation databases.
None of the gene variants found in the study subjects could be classified as pathogenic or likely pathogenic according to the American College of Medical Genetics and Genomics Guidelines (17). The variants are presented in Supplementary Table 2. Nine missense variants were classified as variants of uncertain significance. There were no loss-of-function variants in the genes investigated. Two study subjects had two missense variants in TTN.
Identifying genetic variants contributing to disease course is a major objective in the precision medicine era. As variants in the cardiomyopathy associated contractility gene MYH6 have been associated with poor prognosis in HLHS and other CHD patients (7, 13, 14), we hypothesized that a cardiomyopathy gene panel could function as a prognostic tool in HLHS. However, none of the studied HLHS patients with impaired right ventricular function had pathogenic or likely pathogenic variants included in a large cardiomyopathy gene panel. This suggests that conducting a cardiomyopathy gene panel is not useful in predicting the disease course in these patients in a clinical setting.
The genetic etiology in CHD is complex. One tenth of non-syndromic HLHS is thought to be monogenic, and the only variants that are repeatedly found in HLHS patients are NOTCH1 loss of function variants (8–12). Variants in GJA1 (18), NKX2.5 (19), and MYH6 (13), genes have been suggested as causal for HLHS in certain sporadic families. In addition, syndromic or rare copy number variants in cardiogenic genes have been associated with HLHS and other left sided defects, such as coarctation of the aorta, bicuspid aortic valve, and congenital aortic stenosis, and are estimated be the cause in 10% of cases (20–24). Syndromes associated with HLHS include Turner syndrome (loss of part or all of an X chromosome in females), 22q11.2 deletion syndrome, Jacobsen Syndrome (11q terminal deletion disorder), Kabuki syndrome (single gene variants in KMT2D and KDM6A), VACTERL association (genetic origin unknown), Rubinstein-Taybi (single gene variants in CBP and EP300), Adams-Oliver syndrome (single gene variants in ARHGAP31, DOCK6, RBPJ, EOGT, NOTCH1, DLL4), and Beckwith-Wiedemann syndrome (single gene variants in CDKNIC) (25).
Interestingly, variants in some cardiomyopathy associated genes have been suspected as pathogenic also in CHD. Damaging, recessive MYH6 variants were enriched in a large cohort of CHD individuals where most of the MYH6 variant carriers were left ventricular outflow tract obstruction patients (7). MYH7 variants have been found in left ventricular non-compaction associated with bicuspid aortic valve (26) and Ebstein anomaly (27). Also variants in transcription factor genes, such as GATA4 and TBX20, have been associated with both CHD and dilated cardiomyopathy (28–30). Recently, a homozygous truncating variant in PKP2, a gene previously associated with arrhythmogenic right ventricular cardiomyopathy, was evaluated as causal in two siblings diagnosed with severe HLHS with prominently trabeculated abnormal myocardium and reduced contractility of both ventricles (31).
In addition to causing CHD, variants in cardiomyopathy associated genes have been suspected to worsen the disease course in HLHS and other CHD. Dominant (14) and recessive (13) damaging variants in MYH6 have been related to poor ventricular function and need for cardiac transplantation in HLHS patients, and recessive damaging variants in MYH6 were associated with abnormal ventricular function in a study of a wide range of CHD (7), although no segregation of MYH6 variants has thus far been demonstrated. In a study of five HLHS individuals who developed reduced right ventricular function, two were found to have rare compound heterozygous mutations in MYH6 that were assessed as pathogenic (13). In another study of a wide range of CHD, recessive MYH6 variants were identified in 7/2,871 individuals, five of whom had left ventricular outflow tract obstruction defects (7). Four of the seven individuals had abnormal ventricular function. A weakness of these studies was the lack of functional data—the pathogenicity was assessed by in silico modeling only. In the third study of 190 HLHS individuals, 20 (10.5%) had MYH6 variants in contrast to 2.9% of controls (14). Of these, 19 individuals were heterozygous carriers, and 10 of the variants were novel. Variants were observed across all functional domains of α-MHC. Those with MYH6 variants were overrepresented in the group needing a cardiac transplant. Transcriptome and protein expression analyses from patient-derived cardiac tissue and induced pluripotent stem cell-derived cardiomyocytes indicated differential expression in some contractility genes in patients with MYH6 variants and controls. However, the MYH6 transcript levels themselves were not different between cases and controls.
The disease course of HLHS is variable. Identifying genetic variants associated with poor prognosis would be helpful in tailoring the follow-up and therapeutic strategies. Contrary to our hypothesis, pathogenic variants in MYH6 or other cardiomyopathy genes were not found in this Finnish cohort of HLHS patients with poor ventricular function. A limitation of this study is the small cohort size, however, HLHS is a rare disease and these patients represent those with the most unfavorable outcome in a national cohort.
It is certainly likely that in most cases congenital heart defects are of multifactorial origin—a combination of one or more predisposing genetic variants and adverse environmental exposure—and only a small number of cases are explained by monogenic causes. In addition, it is probable that the causative or additional genetic variants modify the disease course. While variants in genes associated with cardiomyopathy might contribute to HLHS outcome in some patients, our finding does not support this as a significant predisposing factor at the patient cohort level. Thus, our approach of performing a cardiomyopathy gene panel to identify pathogenic variants as directly causal or as modifiers for worse outcomes in HLHS is not useful in clinical practice at the moment.
Data cannot be shared publicly because the data consists of individual clinical data and individual genotypes for young children. Data are available from the Helsinki University Hospital's Institutional Data Access/Ethics Committee for researchers who meet the criteria for access to confidential data. Data availability contact: Emmi Helle.
The study protocol was reviewed and approved by the Ethics Board of Helsinki and Uusimaa Hospital District. Written informed consent was obtained from the legal guardians of the participants and also directly from all participants aged over 6 years.
EH, JP, and TO: study design. EH, RT, HR, and TO: data collection. EH, ST, JK, and TO: data analysis and data interpretation. EH, JP, JK, and TO: drafting of manuscript. All authors: reviewed manuscript content and approved the final version.
This study was funded by the Finnish Medical Foundation (EH), the Finnish Foundation for Pediatric Research (EH, JP, and TO), Finnish Foundation for Cardiovascular Research (EH), and Finnish state funding for university-level health research (JP and TO) (these funders do not provide specific grant numbers).
JK: Full-time Laboratory Director at Blueprint Genetics (paid salary from BpG); ST: Full-time geneticist at BpG (paid salary from BpG).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank all the patients and their family members for participating in the study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.596840/full#supplementary-material
1. Reller MD, Strickland MJ, Riehle-Colarusso T, Mahle WT, Correa A. Prevalence of congenital heart defects in metropolitan Atlanta, 1998-2005. J Pediatr. (2008) 153:807–13.
2. Hoffman JIE, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. (2002) 39:1890–900.
3. Altmann K, Printz BF, Solowiejczky DE, Gersony WM, Quaegebeur J, Apfel HD. Two-dimensional echocardiographic assessment of right ventricular function as a predictor of outcome in hypoplastic left heart syndrome. Am J Cardiol. (2000) 86:964–8. doi: 10.1016/S0002-9149(00)01131-0
4. Piran S, Veldtman G, Siu S, Webb GD, Liu PP. Heart failure and ventricular dysfunction in patients with single or systemic right ventricles. Circulation. (2002) 105:1189–94. doi: 10.1161/hc1002.105182
5. Stout KK, Broberg CS, Book WM, Cecchin F, Chen JM, Dimopoulos K, et al. Chronic heart failure in congenital heart disease: a scientific statement from the American Heart Association. Circulation. (2016) 133:770–801. doi: 10.1161/CIR.0000000000000352
6. Taverne YJHJ, Yannick JH, Sadeghi A, Bartelds B, Ad JJ, Merkus D. Right ventricular phenotype, function, and failure: a journey from evolution to clinics. Heart Failure Rev. (2020). doi: 10.1007/s10741-020-09982-4
7. Jin SC, Homsy J, Zaidi S, Lu Q, Morton S, DePalma SR, et al. Contribution of rare inherited and de novo variants in 2,871 congenital heart disease probands. Nat Genet. (2017) 49:1593–601. doi: 10.1038/ng.3970
8. McBride KL, Riley MF, Zender GA, Fitzgerald-Butt SM, Towbin JA, Belmont JW, et al. NOTCH1 mutations in individuals with left ventricular outflow tract malformations reduce ligand-induced signaling. Hum Mol Genet. (2008) 17:2886–93. doi: 10.1093/hmg/ddn187
9. Iascone M, Ciccone R, Galletti L, Marchetti D, Seddio F, Lincesso AR, et al. Identification of de novo mutations and rare variants in hypoplastic left heart syndrome. Clin Genet. (2012) 81:542–54. doi: 10.1111/j.1399-0004.2011.01674.x
10. Theis JL, Hrstka SC, Evans JM, O'Byrne MM, de Andrade M, O'Leary PW, et al. Compound heterozygous NOTCH1 mutations underlie impaired cardiogenesis in a patient with hypoplastic left heart syndrome. Hum Genet. (2015) 134:1003–11. doi: 10.1007/s00439-015-1582-1
11. Kerstjens-Frederikse WS, van de Laar IMBH, Vos YJ, Verhagen JMA, Berger RMF, Lichtenbelt KD, et al. Cardiovascular malformations caused by NOTCH1 mutations do not keep left: data on 428 probands with left-sided CHD and their families. Genet Med. (2016) 18:914–23. doi: 10.1038/gim.2015.193
12. Helle E, Córdova-Palomera A, Ojala T, Saha P, Potiny P, Gustafsson S, et al. Loss of function, missense, and intronic variants in NOTCH1 confer different risks for left ventricular outflow tract obstructive heart defects in two European cohorts. Genet Epidemiol. (2019) 43:215–26. doi: 10.1002/gepi.22176
13. Theis JL, Zimmermann MT, Evans JM, Eckloff BW, Wieben ED, Qureshi MY, et al. Recessive MYH6 mutations in hypoplastic left heart with reduced ejection fraction. Circ Cardiovasc Genet. (2015) 8:564–71. doi: 10.1161/CIRCGENETICS.115.001070
14. Tomita-Mitchell A, Stamm KD, Mahnke DK, Kim M-S, Hidestrand PM, Liang HL, et al. Impact of MYH6 variants in hypoplastic left heart syndrome. Physiol Genomics. (2016) 48:912–21. doi: 10.1152/physiolgenomics.00091.2016
15. Kim M-S, Fleres B, Lovett J, Anfinson M, Samudrala SSK, Kelly LJ, et al. Contractility of induced pluripotent stem cell-cardiomyocytes with an MYH6 head domain variant associated with hypoplastic left heart syndrome. Front Cell Dev Biol. (2020) 8:440. doi: 10.3389/fcell.2020.00440
16. Karczewski KJ, Francioli LC, Tiao G, Cummings BB, Alföldi J, Wang Q, et al. The mutational constraint spectrum quantified from variation in 141,456 humans. Nature. (2020) 581:434–43. doi: 10.1038/s41586-020-2308-7
17. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. (2015) 17:405–24. doi: 10.1038/gim.2015.30
18. Dasgupta C, Martinez AM, Zuppan CW, Shah MM, Bailey LL, Fletcher WH. Identification of connexin43 (alpha1) gap junction gene mutations in patients with hypoplastic left heart syndrome by denaturing gradient gel electrophoresis (DGGE). Mutat Res. (2001) 479:173–86. doi: 10.1016/S0027-5107(01)00160-9
19. Elliott DA, Kirk EP, Yeoh T, Chandar S, McKenzie F, Taylor P, et al. Cardiac homeobox gene NKX2-5 mutations and congenital heart disease: associations with atrial septal defect and hypoplastic left heart syndrome. J Am Coll Cardiol. (2003) 41:2072–6. doi: 10.1016/S0735-1097(03)00420-0
20. Grossfeld P, Ye M, Harvey R. Hypoplastic left heart syndrome: new genetic insights. J Am Coll Cardiol. (2009) 53:1072–4. doi: 10.1016/j.jacc.2008.12.024
21. Hitz M-P, Lemieux-Perreault L-P, Marshall C, Feroz-Zada Y, Davies R, Yang SW, et al. Rare copy number variants contribute to congenital left-sided heart disease. PLoS Genet. (2012) 8:e1002903. doi: 10.1371/journal.pgen.1002903
22. Tomita-Mitchell A, Mahnke DK, Struble CA, Tuffnell ME, Stamm KD, Hidestrand M, et al. Human gene copy number spectra analysis in congenital heart malformations. Physiol Genomics. (2012) 44:518–41. doi: 10.1152/physiolgenomics.00013.2012
23. Warburton D, Ronemus M, Kline J, Jobanputra V, Williams I, Anyane-Yeboa K, et al. The contribution of de novo and rare inherited copy number changes to congenital heart disease in an unselected sample of children with conotruncal defects or hypoplastic left heart disease. Hum Genet. (2014) 133:11–27. doi: 10.1007/s00439-013-1353-9
24. Hanchard NA, Umana LA, D'Alessandro L, Azamian M, Poopola M, Morris SA, et al. Assessment of large copy number variants in patients with apparently isolated congenital left-sided cardiac lesions reveals clinically relevant genomic events. Am J Med Genet A. (2017) 173:2176–88. doi: 10.1002/ajmg.a.38309
25. Pierpont ME, Brueckner M, Chung WK, Garg V, Lacro RV, McGuire AL, et al. Genetic basis for congenital heart disease: revisited: a scientific statement from the american heart association. Circulation. (2018) 138:e653–e711. doi: 10.1161/CIR.0000000000000606
26. Basu R, Hazra S, Shanks M, Paterson DI, Oudit GY. Novel mutation in exon 14 of the sarcomere gene MYH7 in familial left ventricular noncompaction with bicuspid aortic valve. Circ Heart Fail. (2014) 7:1059–62. doi: 10.1161/CIRCHEARTFAILURE.114.001666
27. Vermeer AMC, van Engelen K, Postma AV, Baars MJH, Christiaans I, De Haij S, et al. Ebstein anomaly associated with left ventricular noncompaction: an autosomal dominant condition that can be caused by mutations in MYH7. Am J Med Genet C Semin Med Genet. (2013) 163C:178–84. doi: 10.1002/ajmg.c.31365
28. Garg V, Kathiriya IS, Barnes R, Schluterman MK, King IN, Butler CA. GATA4 mutations cause human congenital heart defects and reveal an interaction with TBX5. Nature. (2003) 424:443–7. doi: 10.1038/nature01827
29. Kirk EP, Sunde M, Costa MW, Rankin SA, Wolstein O, Castro ML, et al. Mutations in cardiac T-box factor gene TBX20 are associated with diverse cardiac pathologies, including defects of septation and valvulogenesis and cardiomyopathy. Am J Hum Genet. (2007) 81:280–91. doi: 10.1086/519530
30. Li J, Liu W-D, Yang Z-L, Yuan F, Xu L, Li R-G, et al. Prevalence and spectrum of GATA4 mutations associated with sporadic dilated cardiomyopathy. Gene. (2014) 548:174–81. doi: 10.1016/j.gene.2014.07.022
Keywords: hypoplastic left heart syndrome, congenital heart defects, genetics, precision medicine, heart failure, right ventricle dysfunction, right heart failure, myocardial dysfunction
Citation: Helle E, Pihkala J, Turunen R, Ruotsalainen H, Tuupanen S, Koskenvuo J and Ojala T (2020) Rare Variants in Genes Associated With Cardiomyopathy Are Not Common in Hypoplastic Left Heart Syndrome Patients With Myocardial Dysfunction. Front. Pediatr. 8:596840. doi: 10.3389/fped.2020.596840
Received: 20 August 2020; Accepted: 13 October 2020;
Published: 30 October 2020.
Edited by:
Estela Azeka, University of São Paulo, BrazilReviewed by:
Hannah Bellsham-Revell, Evelina London Children's Hospital, United KingdomCopyright © 2020 Helle, Pihkala, Turunen, Ruotsalainen, Tuupanen, Koskenvuo and Ojala. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emmi Helle, ZW1taS5oZWxsZUBoZWxzaW5raS5maQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.