
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 09 July 2020
Sec. Genetics of Common and Rare Diseases
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.00317
 Helena Donath1*
Helena Donath1* Ursula Hess1Matthias Kieslich2
Ursula Hess1Matthias Kieslich2 Marius Theis2Ute Ohlenschläger2
Marius Theis2Ute Ohlenschläger2 Ralf Schubert1
Ralf Schubert1 Sandra Woelke1
Sandra Woelke1 Stefan Zielen1
Stefan Zielen1Background: Ataxia telangiectasia (A-T) is a rare autosomal-recessive multisystem disorder characterized by pronounced cerebellar ataxia, telangiectasia, cancer predisposition and altered body composition. In addition, evidence is rising for endocrine dysfunction.
Objectives: To determine the evolution of diabetes and its prevalence in a larger A-T cohort.
Methods: A retrospective analysis of the patient charts of 39 subjects from the Frankfurt A-T cohort was performed between August 2002 and 2018 concerning HbA1c and oral glucose tolerance (OGTT). The median follow-up period was 4 years (1–16 years). In addition, in 31 A-T patients aged 1 to 38 years HbA1c and fasting glucose were studied prospectively from 2018 to 2019.
Results: In the retrospective analysis, we could demonstrate a longitudinal increase of HbA1c. The prospective analysis showed a significant increase of HbA1c and fasting glucose with age (r = 0.79, p ≤ 0.0001). OGTT has a good sensitivity for insulin resistance screening, whereas HbA1c can be used to evaluate individual courses and therapy response. Seven out of 39 (17.9%) patients suffered from diabetes. Metformin did not always lead to sufficient diabetes control; one patient was treated successfully with repaglinide.
Conclusion: Diabetes is a common finding in older A-T patients and often starts in puberty. Our data clearly demonstrate the need for an annual diabetes screening in patients > 12 years.
Ataxia telangiectasia (A-T) is a rare autosomal recessive multisystem disorder characterized by pronounced cerebellar ataxia, telangiectasia, cancer predisposition, and altered body composition (1–3). The incidence is estimated at 1:40.000–1:200.000 (4).
The sequence of the Ataxia Telangiectasia Mutated (ATM) gene has been known since 1995. It is located in the region q22-23 of chromosome 11 and encodes a 370 kDa serine/threonine kinase called ATM belonging to the family of signal transduction molecules (5, 6) and is activated in response to DNA double-strand breaks. ATM has over 700 interaction partners, including the tumor suppressor p53 (7, 8). In this way, a large number of processes such as cell cycle checkpoints, DNA repair systems or apoptosis are controlled. Due to the multitude of tasks, the failure of the kinase results in a complex clinical appearance that manifests in various organ systems (9). Many of the clinical alterations observed in A-T patients may be related to the dysfunctional control of reactive oxygen species (ROS) observed when ATM is deficient (10, 11).
Medical care for A-T patients has improved significantly during the last years and new treatment options rise hope to patients and physicians (4). With increasing life expectancy evolving morbidities like liver disease (12), insulin resistance (IR) (13), lipid alterations (14, 15), and cardiovascular disease (16) are coming to the fore as a typical signs of premature aging (17).
While gastrointestinal involvement, mainly dysphagia, poor weight gain, and failure to thrive have been characterized well (2, 3, 18–21), hepatic and metabolic disease is an entity taken into consideration only recently, with the clinical improvement and increased survival of A-T patients (12, 15). Recently, it was shown that ATM is also involved in metabolic and cardiovascular complications when disrupted (13, 15, 22, 23). ATM is a critical player in a multitude of cellular pathways for glucose metabolism (24–26). In vitro hyperglycemia led to increased activation of the ATM protein in pancreatic β-cells (27). The absence of ATM leads to dysglycemia and IR with lower Matsuda index when compared to controls while performing an oral glucose tolerance test (OGTT) (28).
ATM protein is involved in glucose transport, and lack of ATM can cause IR (24). Cytoplasmic ATM is a major upstream activator of Akt thus contributes to the translocation of cell surface glucose transporter 4 (GLUT4) to cell membrane (24). Early IR and a high prevalence of diabetes type 2 in older A-T patients as well as their family members are well known (23, 29–32). In the last years, it became evident that ATM gene polymorphisms are associated with higher risk of type 2 diabetes (33) and poorer response to metformin treatment (34).
The aim of this retrospective and in part prospective study was to evaluate our patient cohort for the incidence of IR and diabetes. In addition, we evaluated the therapy efficaciousness of diabetes treatment in seven patients.
Between August 2002 and August 2018 we studied data of 39 classical A-T patients aged 1 to 38 years from the Frankfurt A-T cohort regarding HbA1c and outcome of OGTT. The parameters were taken from the available patient charts. In addition, 31 A-T patients were investigated for HbA1c and fasting glucose prospectively. The parameters were determined in the serum of whole blood.
(Pre-)Diabetes was defined according to recent International Society for Pediatric and Adolescent Diabetes (ISPAD) guidelines as pathological 2 h-postchallenge glucose, fasting glucose ≥ 126 mg/dL or HbA1c ≥ 5.7% (35).
All patients were clinically and/or genetically diagnosed with A-T according to recent World Health Organization (WHO) recommendations (36). We compared patients <12 years of age (group 1) to patients ≥ 12 years (group 2).
The data presented were collected from two non-interventional clinical trials at the children's hospital Frankfurt. Both trials were registered at clinicaltrials.gov 2012 (Susceptibility to infections in ataxia telangiectasia; NCT02345135) and 2017 (Susceptibility to Infections, tumor risk, and liver disease in patients with ataxia telangiectasia; NCT03357978). The studies were approved by the responsible ethics committee in Frankfurt (application number 121/12 and 504/15) and conducted following the ethical principles of the Declaration of Helsinki, regulatory requirements and the code of Good Clinical Practice.
For statistical analysis GraphPad Prism 5.01 (GraphPad Software, Inc.) was used. Values are presented as arithmetic means with standard deviations (SDs). For comparisons between the two study groups, two-tailed Mann-Whitney-U test was applied. Correlations were analyzed by Spearman's correlation coefficient. P ≤ 0.05 were considered significant.
From our database, we collected HbA1c of 39 A-T patients who presented in our clinic within this period of time (2002–2018) and had at least one measurement of HbA1c; a total of 73 HbA1c measurements were performed. HbA1c was significantly higher in group 2 compared to group 1 (4.85 ± 0.14 vs. 5.65 ± 0.08%, p ≤ 0.0001). We could show a significant correlation between age and increased HbA1c (r = 0.59, p ≤ 0.0001). Figure 1 shows the progression of HbA1c with age. We evaluated the results of OGTT in 13 older patients (Median age: 17.5 years). As shown in Table 1, 7 out of 13 patients had IR or diabetes. OGTT was more sensitive to detect disturbed glucose metabolism than the corresponding HbA1c. All diabetic patients were ≥ 12 years of age at diagnosis (median age at diagnosis: 21 years). Figure 2 shows OGTT results in six patients who had or developed diabetes. None of the patients had auto antibodies, the family history of diabetes was unremarkable in all cases. None of the patients had systemic steroid intake documented in the patient charts.
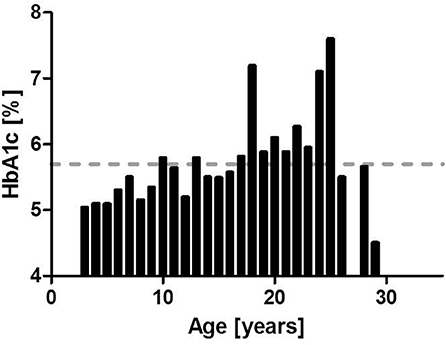
Figure 1. HbA1c (n = 3) and age. As depicted here HbA1c is increasing with age. Normal range is up to 5.7% (hatched line).
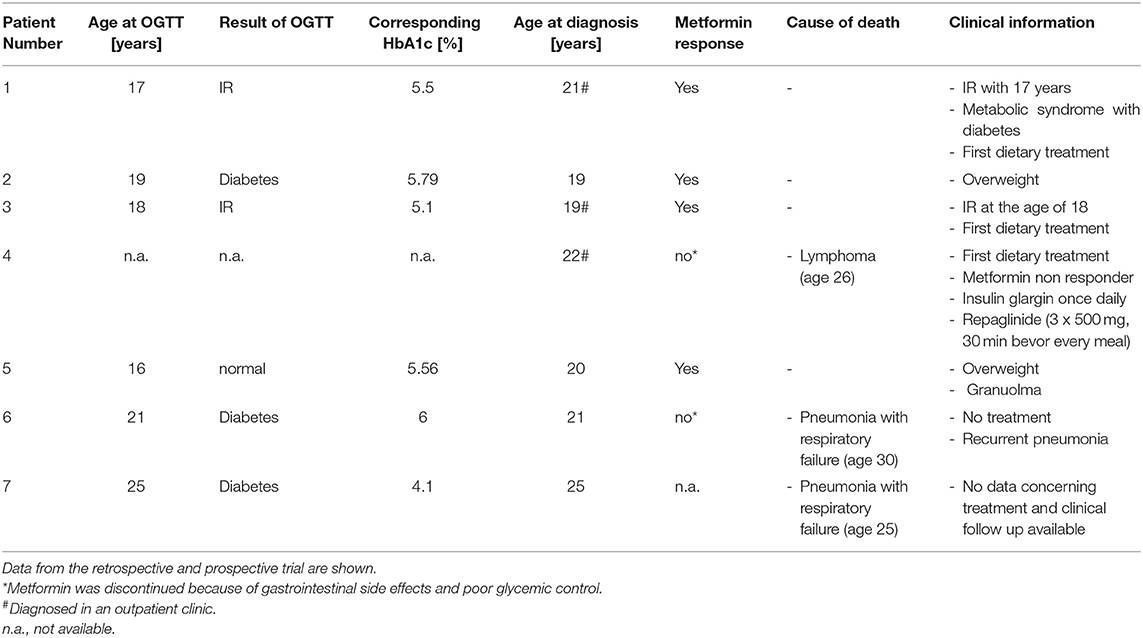
Table 1. Overview about seven diabetic patient from the Frankfurt A-T cohort.
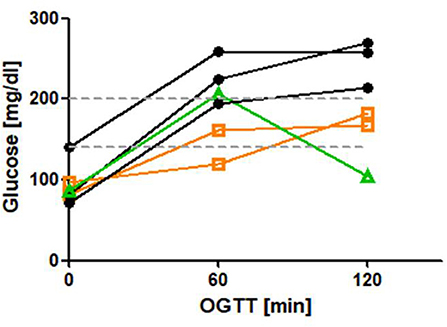
Figure 2. OGTT in 6 patient with diabetes. IR is defined as 120 min glucose > mg/dl, diabetes is defined as 120 min glucose > 200 mg/dl (hatched lines). N = 3 patients were diagnosed with diabetes (black curves). N = 2 had an IR and developed diabetes (orange curves). N = 1 had a normal OGTT and developed diabetes (green curve).
Patient characteristics are shown in Table 2. HbA1c and fasting glucose were significantly increased in group 2 compared to group 1 (HbA1c: group 1: 4.84 ± 0.35, group 2: 5.72 ± 0.6%; p ≤ 0.0001, fasting glucose: group 1: 84.2 ± 10.13 mg/dL, group 2: 103.7 ± 16.8 mg/dL, p ≤ 0.0001). Pathologically increased HbA1c levels were found in 30% (3/10) of older A-T patients. We could establish a significant correlation of HbA1c (r = 0.79, p ≤ 0.0001) and fasting glucose (r = 0.51, p ≤ 0.001) with age. The correlations are shown in Figures 3, 4. 30 % (3/10) of group 2 suffered from diabetes type 2 whereas no patient in group 1 was affected.
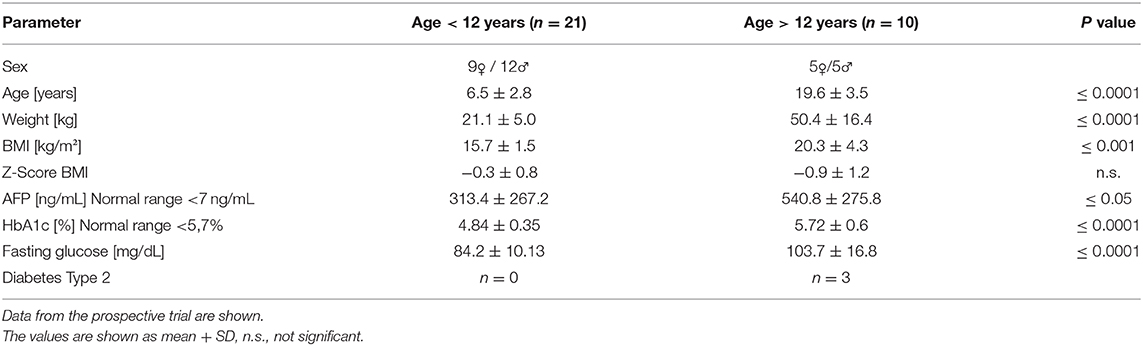
Table 2. Patient characteristics.
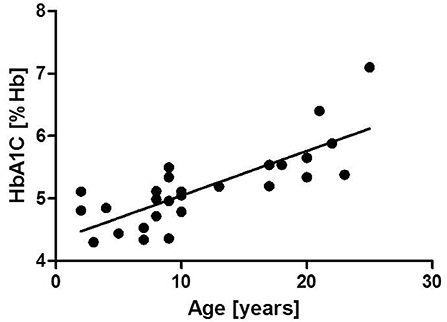
Figure 3. Correlation of HbA1c and age r = 0.79, p ≤ 0.0001.
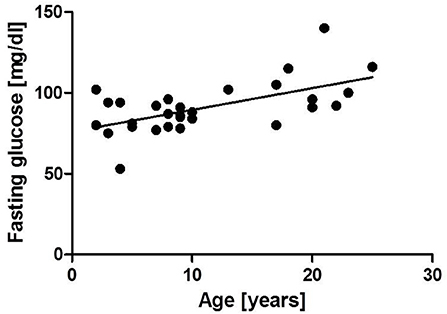
Figure 4. Correlation of fasting glucose and age r = 0.51, p ≤ 0.0001.
All diabetic patients received treatment with metformin (Table 1). Response to metformin was favorable 4/7 patients (57.1%). 2/7 patients did not respond to metformin monotherapy. Due to gastrointestinal side effects, one of these patients discontinued the metformin treatment. After a short period without any treatment, subcutaneous injections of insulin glargin were started. Still, the patient suffered from poorly controlled diabetes marked by a fasting glucose of 250 mg/dL and HbA1c of 7.6% at presentation in our clinic. Due to an advanced neurological deficit we were hesitant to initiate an intensified subcutaneous insulin therapy and therefore decided to treat him with repaglinide orally. Within 8 weeks, HbA1c dropped to 6.2%. The individual course of HbA1c of this patient is shown in Figure 5.
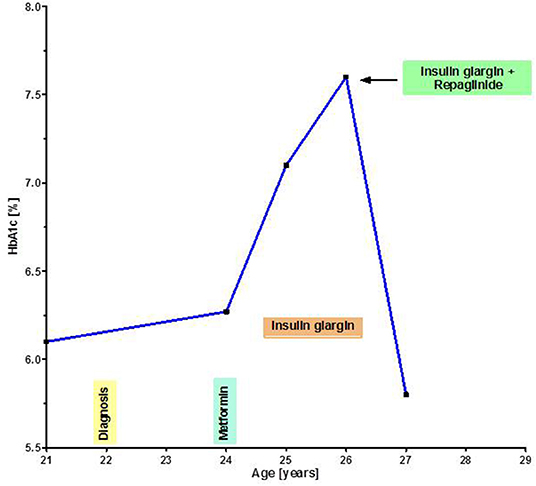
Figure 5. Individual course of HbA1c in a diabetic patient under different treatments. Repaglinide led to an efficacious glycaemia control.
A-T is a lethal, chronic degenerative disease. Due to the improved treatment options in the recent years, hitherto largely unknown disease features such as endocrine dysfunction, liver disease and cardiovascular diseases are gaining in importance (12, 15, 37, 38). The present work clearly demonstrates the high rate of type 2 diabetes (17.9%) among post-pubertal patients.
Diabetes is one of the leading causes of death worldwide (39). It leads to a high cardiovascular risk, micro-angiopathy, dyslipidemia, nephropathy, neuropathy, and repressed immune system (39). HbA1c values in the upper normal range indicate a high risk for later diabetes (40). In condition of A-T, IR and diabetes have rarely been investigated in clinical settings. In view of the comorbidities (e.g., malnutrition, neurological deficit, and immunodeficiency), consistent diabetes therapy is of particular importance.
In the cytoplasm of the cells, ATM causes activation of the serine/threonine-specific protein kinase Akt in response to insulin. Akt is an important protein which participates in the signaling cascade for the inhibition of apoptotic signals (41). In response to insulin, protein translation is stimulated, and glucose uptake is controlled by GLUT 4 (24). Mice with a muscle-specific deletion in the GLUT 4 gene develop IR and glucose intolerance (42). Low ATM levels will therefore contribute to the development of IR and glucose intolerance in A-T via the down-regulation of Akt activity in muscle cells (24).
In 2000, the insulin signaling induced ATM-dependent phosphorylation of 4E-BP1 was reported (46). Ever since, the deficiency in the insulin and insulin-like growth factor 1 (IGF-1) axes has been demonstrated in the absence of ATM (20, 26). Apo E knockout mice without ATM protein showed increased IR and were prone to develop a metabolic syndrome (22).
Additionally, ATM is a regulator of adipocyte differentiation. In Atm-deficient mice lack of induction of C/EBPα and PPARγ, central transcription factors for adipocyte differentiation, as well a reduced fat mass were reported (43). Of course, fat mass is of particular importance for glucose metabolism and homeostasis. There was no significant difference when comparing fat mass of A-T patients to sex and age matched healthy controls in humans (2). Apparently, the significantly decreased lean mass is a major contributor to the disturbed glycemic control in A-T patients.
Apart from that, there have been few reports on endocrine abnormalities in A-T patients (38). While poor weight gain, stunting and delayed pubertal development have been characterized as a typical findings in A-T (2, 3, 19, 20, 38), abnormalities in glucose metabolism, also if known since long time, are hardly described as clinical manifestation (30–32). We have recently reported about liver involvement in A-T and dyslipidemia (12). In synopsis of lipid metabolism disorder and IR, A-T patients suffer from an incomplete metabolic syndrome with increased risk for cardiovascular events (15, 16, 44).
Due to better care, life expectancy of A-T patients has emerged over the last decades (45). Especially in the light of new treatment options such as bone marrow transplantation (46–48), dexamethasone treatment (49–51), and gene therapy (52–54) disease facets with manifestation in the later disease course should be screened and treated. According to our data, diabetes screening is indicated starting for the age of 12 years. HbA1c is an easy to obtain, inexpensive marker that can be used to evaluate individual courses and therapy response. However, OGTT is more sensitive in diagnosing IR than HbA1c and fasting glucose. This shows that the OGTT is still of value and confirms the current recommendation of the English CF society: HbA1c reflects glycemic control over a period of time. The statement about the long-term course of blood glucose has some advantages, but the values of HbA1c in CF patients may still be within the normal range when the OGTT already shows an IR or even diabetes (55). Taken these information into account, we truly believe that both measurements, HbA1c and OGTT, should be applied in A-T patients.
First line treatment for insulin-resistant diabetes is metformin (39). However, to our clinical experience, not all A-T patients respond to treatment with metformin. As has been shown in 2011, inhibition of ATM in rat hepatoma cell lines diminished the effect of metformin by reduced phosphorylation and activation of AMP-activated protein kinase (25). Additionally, the gene variant SNP rs11212617 at a locus that includes the ATM was proved to influence the glycemic response to metformin in type 2 diabetes (56). In line with these studies, Connelly et al. reported that the absence of ATM leads to dysglycaemia and IR with lower Matsuda index when compared to controls while performing an OGTT (28). Nevertheless, they could not show altered fasting glucose levels, insulin concentrations or insulinogenic index measurements (28).
In addition to that, it is important to consider the general condition of the patient with particular attention to the neurological status, body composition, and independence in the patients' everyday life. For instance, subcutaneous injections often present an insurmountable barrier to self-administration due neurological impairment [unpublished clinical observation]. Apart from clinical experience, research on endocrine, and metabolic alterations in A-T is rare (15, 22, 37, 57). No guidelines for treatment of diabetes in this challenging patient group are available.
In case a patient does not respond adequately to metformin therapy, insulin treatment is recommended. The beneficial effects of insulin as anabolic hormone should be taken into consideration when escalating diabetes therapy (58). Especially in malnourished patients, an amelioration of the nutritional status with weight gain could be achieved with insulin injections. The insulin/IGF-1 axis increases muscle mass and bone density and improves insulin sensitivity as well as enhancement of free fatty acid oxidations in the muscles. Also, it was shown recently that the IGF-1 pathway has beneficial effect on cardiovascular and cerebrovascular disease (59). On the other hand, insulin as anabolic hormone and growth factor may possibly increase the cancer risk in A-T patients (60).
However, self-administration of subcutaneous insulin injections are not feasible for older A-T patients with considerable neurological deficit. In case an insulin therapy is initiated, they are dependent on their caregiver. There is a dilemma between the autonomy of patients and the necessary treatment. To improve compliance, a different treatment regimen with oral antidiabetic drugs such as repaglinide may be used in special cases (61). In the Frankfurt A-T cohort, one of our A-T patients with diabetes had poorly controlled serum glucose levels under treatment with insulin glargin. We initiated a treatment with repaglinide. Hereunder, with a very favorable side-effect profile, a good therapeutic success and at the same time excellent compliance was achieved.
This study has some limitations. Due to the retrospective design, we cannot provide a complete data set for the diagnosis of type 2 diabetes, since many patients of our national cohort are admitted to our center for routine care annually or even every second year only. Still, to our best knowledge, this is the first prospective study on diabetes in 31 A-T patients and seems to confirm our retrospective analysis of longitudinal data sets of our national cohort. Due to the large number of cases, we think we have delivered reliable data that clearly demonstrate the need for an annual diabetes screening in patients ≥ 12 years.
Especially with advancing age, a diabetes screening should be conducted regularly in A-T patients. IR and diabetes have to be treated in order to stabilize the nutritional status and avert further complications. OGTT has a good sensitivity for IR screening, whereas HbA1c is an inexpensive marker that can be used to evaluate individual courses and therapy response. Metformin should be administered as first line treatment and in non-responders repaglinide was shown to be safe and efficacious for glycemic control.
Scientific knowledge on the subject: Little is known about the natural course of diabetes in ataxia telangiectasia (A-T). This is the first longitudinal retrospective and prospective surveillance of diabetes in a larger A-T cohort.
What This Study Adds to the Field: Diabetes is a common finding in older A-T patients and normally starts after puberty. There was a significant correlation of HbA1c and fasting glucose with age. OGTT has a good sensitivity for IR screening, whereas HbA1c can be used to evaluate individual courses and therapy response.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethikkommitee des Universitätsklinikums Frankfurt. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
This manuscript has been released as a pre-print at Research Square, Donath et al. (62).
HD, SW, UH, SZ, and RS did the study design, data collection and interpreted, and did statistical analysis. MT, MK, UO, HD, SW, UH, and SZ conducted visits. HD and SZ wrote the manuscript. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank our patients and their families who share and support our research.
A-T, Ataxia telangiectasia; ATM, Ataxia telangiectasia mutated; ROS, Reactive oxygen species; IR, Insulin resistance; OGTT, Oral glucose tolerance test; GLUT4, Cell surface glucose transporter 4; ISPAD, International Society For Pediatric And Adolescent Diabetes; WHO, World Health Organization; SD, Standard deviation; IGF-1, Insulin-Like Growth Factor 1; SNP, Single nucleotide polymorphism.
1. Boder E, Sedwick RP. Ataxia-telangiectasia; a familial syndrome of progressive cerebellar ataxia, oculocutaneous telangiectasia and frequent pulmonary infection. Pediatrics. (1958) 21:526–54.
2. Pommerening H, van Dullemen S, Kieslich M, Schubert R, Zielen S, Voss S. Body composition, muscle strength and hormonal status in patients with ataxia telangiectasia: a cohort study. Orphanet J Rare Dis. (2015) 10:155. doi: 10.1186/s13023-015-0373-z
3. Woelke S, Pommerening H, Kieslich M, Schubert R, Zielen S. Growth hormone treatment in patients with ataxia telangiectasia. Growth Factors. (2017) 35:125–30. doi: 10.1080/08977194.2017.1367681
4. Rothblum-Oviatt C, Wright J, Lefton-Greif MA, McGrath-Morrow SA, Crawford TO, Lederman HM. Ataxia telangiectasia: a review. Orphanet J Rare Dis. (2016) 11:159. doi: 10.1186/s13023-016-0543-7
5. Gatti RA, Berkel I, BODER E, Braedt G, Charmley P, Concannon P, et al. Localization of an ataxia-telangiectasia gene to chromosome 11q22-23. Nature. (1988) 336:577–80. doi: 10.1038/336577a0
6. Vanagaite L, James MR, Rotman G, Savitsky K, Bar-Shira A, Gilad S, et al. A high-density microsatellite map of the ataxia-telangiectasia locus. Hum Genet. (1995) 95:451–4. doi: 10.1007/BF00208975
7. Savitsky K, Bar-Shira A, Gilad S, Rotman G, Ziv Y, Vanagaite L, et al. A single ataxia telangiectasia gene with a product similar to pI-3 kinase. Science. (1995) 268:1749–53. doi: 10.1126/science.7792600
8. Ambrose M, Gatti RA. Pathogenesis of ataxia-telangiectasia: the next generation of aTM functions. Blood. (2013) 16:4036–45. doi: 10.1182/blood-2012-09-456897
9. Lavin MF. Ataxia-telangiectasia: from a rare disorder to a paradigm for cell signalling and cancer. Nat Rev Mol Cell Biol. (2008) 9:759–69. doi: 10.1038/nrm2514
10. Yang Y, Hui CW, Li J, Herrup K. Correction: the interaction of the atm genotype with inflammation and oxidative stress. PLoS ONE. (2015) 10:e0130645. doi: 10.1371/journal.pone.0130645
11. Reichenbach J, Schubert R, Schindler D, Müller K, Böhles H, Zielen S. Elevated oxidative stress in patients with ataxia telangiectasia. Antioxid Redox Signal. (2002) 4:465–9. doi: 10.1089/15230860260196254
12. Donath H, Woelke S, Theis M, Heß U, Knop V, Herrmann E, et al. Progressive liver disease in patients with ataxia telangiectasia. Front Pediatr. (2019) 7:458. doi: 10.3389/fped.2019.00458
13. Espach Y, Lochner A, Strijdom H, Huisamen B. ATM protein kinase signaling, type 2 diabetes and cardiovascular disease. Cardiovasc Drugs Ther. (2015) 29:51–8. doi: 10.1007/s10557-015-6571-z
14. Mercer JR, Cheng K-K, Figg N, Gorenne I, Mahmoudi M, Griffin J, et al. DNA damage links mitochondrial dysfunction to atherosclerosis and the metabolic syndrome. Circ Res. (2010) 15:1021–31. doi: 10.1161/CIRCRESAHA.110.218966
15. Paulino TL, Rafael MN, Hix S, Shigueoka DC, Ajzen SA, Kochi C, et al. Is age a risk factor for liver disease and metabolic alterations in ataxia telangiectasia patients? Orphanet J Rare Dis. (2017) 12:136. doi: 10.1186/s13023-017-0689-y
16. Andrade IGA, Costa-Carvalho BT, da Silva R, Hix S, Kochi C, Suano-Souza FI, et al. Risk of atherosclerosis in patients with ataxia telangiectasia. Ann Nutr Metab. (2015) 66:196–201. doi: 10.1159/000430790
17. Shiloh Y, Lederman HM. Ataxia-telangiectasia (A-T): an emerging dimension of premature ageing. Ageing Res Rev. (2017) 33:76–88. doi: 10.1016/j.arr.2016.05.002
18. Lefton-Greif MA, Crawford TO, Winkelstein JA, Loughlin GM, Koerner CB, Zahurak M, et al. Oropharyngeal dysphagia and aspiration in patients with ataxia-telangiectasia. J Pediatr. (2000) 136:225–31. doi: 10.1016/S0022-3476(00)70106-5
19. Ross LJ, Capra S, Baguley B, Sinclair K, Munro K, Lewindon P, et al. Nutritional status of patients with ataxia-telangiectasia: a case for early and ongoing nutrition support and intervention. J Paediatr Child Health. (2015) 51:802–7. doi: 10.1111/jpc.12828
20. Voss S, Pietzner J, Hoche F, Taylor AMR, Last JI, Schubert R, et al. Growth retardation and growth hormone deficiency in patients with ataxia telangiectasia. Growth Factors. (2014) 32:123–9. doi: 10.3109/08977194.2014.939805
21. Stewart E, Prayle AP, Tooke A, Pasalodos S, Suri M, Bush A, et al. Growth and nutrition in children with ataxia telangiectasia. Arch Dis Child. (2016) 101:1137–41. doi: 10.1136/archdischild-2015-310373
22. Schneider JG, Finck BN, Ren J, Standley KN, Takagi M, Maclean KH, et al. ATM-dependent suppression of stress signaling reduces vascular disease in metabolic syndrome. Cell Metab. (2006) 4:377–89. doi: 10.1016/j.cmet.2006.10.002
23. van Os NJH, Roeleveld N, Weemaes CMR, Jongmans MCJ, Janssens GO, Taylor AMR, et al. Health risks for ataxia-telangiectasia mutated heterozygotes: a systematic review, meta-analysis and evidence-based guideline. Clin Genet. (2016) 90:105–17. doi: 10.1111/cge.12710
24. Halaby M-J, Hibma JC, He J, Yang D-Q. ATM protein kinase mediates full activation of akt and regulates glucose transporter 4 translocation by insulin in muscle cells. Cell Signal. (2008) 20:1555–63. doi: 10.1016/j.cellsig.2008.04.011
25. Zhou K, Bellenguez C, Spencer CCA, Bennett AJ, Coleman RL, Tavendale R, et al. Common variants near aTM are associated with glycemic response to metformin in type 2 diabetes. Nat Genet. (2011) 43:117–20. doi: 10.1038/ng.735
26. Yang D-Q, Halaby M-J, Li Y, Hibma JC, Burn P. Cytoplasmic aTM protein kinase: an emerging therapeutic target for diabetes, cancer and neuronal degeneration. Drug Discov Today. (2011) 16:332–8. doi: 10.1016/j.drudis.2011.02.001
27. Sidarala V, Kowluru A. Exposure to chronic hyperglycemic conditions results in ras-related c3 botulinum toxin substrate 1 (Rac1)-mediated activation of p53 and aTM kinase in pancreatic β-cells. Apoptosis. (2017) 22:597–607. doi: 10.1007/s10495-017-1354-6
28. Connelly PJ, Smith N, Chadwick R, Exley AR, Shneerson JM, Pearson ER. Recessive mutations in the cancer gene ataxia telangiectasia mutated (ATM), at a locus previously associated with metformin response, cause dysglycaemia and insulin resistance. Diabet Med. (2016) 33:371–5. doi: 10.1111/dme.13037
30. Morrell D, Chase CL, Kupper LL, Swift M. Diabetes mellitus in ataxia-telangiectasia, fanconi anemia, xeroderma pigmentosum, common variable immune deficiency, and severe combined immune deficiency families. Diabetes. (1986) 35:143–7. doi: 10.2337/diabetes.35.2.143
31. Bar RS, Levis WR, Rechler MM, Harrison LC, Siebert C, Podskalny J, et al. Extreme insulin resistance in ataxia telangiectasia: defect in affinity of insulin receptors. N Engl J Med. (1978) 298:1164–71. doi: 10.1056/NEJM197805252982103
32. Blevins LS, Gebhart SS. Insulin-resistant diabetes mellitus in a black woman with ataxia-telangiectasia. South Med J. (1996) 89:619–21. doi: 10.1097/00007611-199606000-00013
33. Altall RM, Qusti SY, Filimban N, Alhozali AM, Alotaibi NA, Dallol A, et al. SLC22A1 and ATM genes polymorphisms are associated with the risk of type 2 diabetes mellitus in western saudi arabia: a case-control study. Appl Clin Genet. (2019) 15:213–9. doi: 10.2147/TACG.S229952
34. Out M, Becker ML, van Schaik RH, Lehert P, Stehouwer CD, Kooy A. A gene variant near ATM affects the response to metformin and metformin plasma levels: a post hoc analysis of an RCT. Pharmacogenomics. (2018) 19:715–26. doi: 10.2217/pgs-2018-0010
35. Zeitler P, Fu J, Tandon N, Nadeau K, Urakami T, Barrett T, et al. ISPAD clinical practice consensus guidelines 2014. Type 2 diabetes in the child and adolescent. Pediatr Diabetes. (2014) 15 Suppl 20:26–46. doi: 10.1111/pedi.12179
36. Gathmann B, Goldacker S, Klima M, Belohradsky BH, Notheis G, Ehl S„, et al. The german national registry for primary immunodeficiencies (PID). Clin Exp Immunol. (2013) 173:372–80. doi: 10.1111/cei.12105
37. Weiss B, Krauthammer A, Soudack M, Lahad A, Sarouk I, Somech R, et al. Liver disease in pediatric patients with ataxia telangiectasia: a Novel report. J Pediatr Gastroenterol Nutr. (2016) 62:550–5. doi: 10.1097/MPG.0000000000001036
38. Nissenkorn A, Levy-Shraga Y, Banet-Levi Y, Lahad A, Sarouk I, Modan-Moses D. Endocrine abnormalities in ataxia telangiectasia: findings from a national cohort. Pediatr Res. (2016) 79:889–94. doi: 10.1038/pr.2016.19
39. Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV) Arbeitsgemeinschaft der Wis-senschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie Therapie des Typ-2-Diabetes - Langfassung, 1. Auflage. Version 4. 2013. Zuletzt Geändert (2014). Available online at: www.dm-therapie.versorgungsleitlinien.de
40. Pradhan AD, Rifai N, Buring JE, Ridker PM. Hemoglobin a1c predicts diabetes but not cardiovascular disease in nondiabetic women. Am J Med. (2007) 120:720–7. doi: 10.1016/j.amjmed.2007.03.022
41. Viniegra JG, Martínez N, Modirassari P, Hernández Losa J, Parada Cobo C, Sánchez-Arévalo Lobo VJ, et al. Full activation of pKB/Akt in response to insulin or ionizing radiation is mediated through aTM. J Biol Chem. (2005) 280:4029–36. doi: 10.1074/jbc.M410344200
42. Zisman A, Peroni OD, Abel ED, Michael MD, Mauvais-Jarvis F, Lowell BB, et al. Targeted disruption of the glucose transporter 4 selectively in muscle causes insulin resistance and glucose intolerance. Nat Med. (2000) 6:924–8. doi: 10.1038/78693
43. Takagi M, Uno H, Nishi R, Sugimoto M, Hasegawa S, Piao J, et al. ATM regulates adipocyte differentiation and contributes to glucose homeostasis. Cell Rep. (2015) 10:957–67. doi: 10.1016/j.celrep.2015.01.027
44. Micol R, Ben Slama L, Suarez F, Le Mignot L, Beauté J, Mahlaoui N, et al. Morbidity and mortality from ataxia-telangiectasia are associated with aTM genotype. J Allergy Clin Immunol. (2011) 128:382–9.e1. doi: 10.1016/j.jaci.2011.03.052
45. Crawford TO, Skolasky RL, Fernandez R, Rosquist KJ, Lederman HM. Survival probability in ataxia telangiectasia. Arch Dis Child. (2006) 91:610–1.
46. Duecker R, Baer PC, Buecker A, Huenecke S, Pfeffermann L-M, Modlich U, et al. Hematopoietic stem cell transplantation restores naïve t-Cell populations in atm-Deficient mice and in preemptively treated patients with ataxia-Telangiectasia. Front Immunol. (2019) 10:2785. doi: 10.3389/fimmu.2019.02785
47. Pietzner J, Baer PC, Duecker RP, Merscher MB, Satzger-Prodinger C, Bechmann I, et al. Bone marrow transplantation improves the outcome of atm-deficient mice through the migration of ATM-competent cells. Hum Mol Genet. (2013) 22:493–507. doi: 10.1093/hmg/dds448
48. Bakhtiar S, Woelke S, Huenecke S, Kieslich M, Taylor AM, Schubert R, et al. Pre-emptive allogeneic hematopoietic stem cell transplantation in ataxia telangiectasia. Front Immunol. (2018) 9:2495. doi: 10.3389/fimmu.2018.02495
49. Menotta M, Orazi S, Gioacchini AM, Spapperi C, Ricci A, Chessa L, et al. Proteomics and transcriptomics analyses of ataxia telangiectasia cells treated with dexamethasone. PLoS ONE. (2018) 13:e0195388. doi: 10.1371/journal.pone.0195388
50. Coker SA, Szczepiorkowski ZM, Siegel AH, Ferrari A, Mambrini G, Anand R, et al. A study of the pharmacokinetic properties and the in vivo kinetics of erythrocytes loaded with dexamethasone sodium phosphate in healthy volunteers. Transfus Med Rev. (2018) 32:102–10. doi: 10.1016/j.tmrv.2017.09.001
51. Menotta M, Biagiotti S, Orazi S, Rossi L, Chessa L, Leuzzi V, et al. In vivo effects of dexamethasone on blood gene expression in ataxia telangiectasia. Mol Cell Biochem. (2018) 438:153–66. doi: 10.1007/s11010-017-3122-x
52. Carranza D, Torres-Rusillo S, Ceballos-Pérez G, Blanco-Jimenez E, Muñoz-López M, García-Pérez JL, et al. Reconstitution of the ataxia-Telangiectasia cellular phenotype with lentiviral vectors. Front Immunol. (2018) 9:2703. doi: 10.3389/fimmu.2018.02703
53. Cortés ML, Oehmig A, Saydam O, Sanford JD, Perry KF, Fraefel C, et al. Targeted integration of functional human aTM cDNA into genome mediated by hSV/AAV hybrid amplicon vector. Mol Ther. (2008) 16:81–8. doi: 10.1038/sj.mt.6300338
54. Pineda de las Infantas MJ, Torres-Rusillo S, Unciti-Broceta JD, Fernandez-Rubio P, Luque-Gonzalez MA, Gallo MA, et al. Synthesis of 6,8,9 poly-substituted purine analogue libraries as pro-apoptotic inducers of human leukemic lymphocytes and dAPK-1 inhibitors. Org Biomol Chem. (2015) 13:5224–34. doi: 10.1039/C5OB00230C
55. Tommerdahl KL, Brinton JT, Vigers T, Nadeau KJ, Zeitler PS, Chan CL. Screening for cystic fibrosis-related diabetes and prediabetes: evaluating 1,5-anhydroglucitol, fructosamine, glycated albumin, and hemoglobin a1c. Pediatr Diabetes. (2019) 20:1080–6. doi: 10.1111/pedi.12914
56. van Leeuwen N, Nijpels G, Becker ML, Deshmukh H, Zhou K, Stricker BHC, et al. A gene variant near aTM is significantly associated with metformin treatment response in type 2 diabetes: a replication and meta-analysis of five cohorts. Diabetologia. (2012) 55:1971–7. doi: 10.1007/s00125-012-2537-x
57. Ehlayel M, Soliman A, Sanctis V de. Linear growth and endocrine function in children with ataxia telangiectasia. Indian J Endocrinol Metab. (2014). 18(Suppl 1):S93-6. doi: 10.4103/2230-8210.145079
58. Steiner DF, Chan SJ, Terris S, Hofmann C. Insulin as a cellular growth regulator. Ciba Found Symp. (1977) 217–28. doi: 10.1002/9780470720363.ch11
59. Obradovic M, Zafirovic S, Soskic S, Stanimirovic J, Trpkovic A, Jevremovic D, et al. Effects of iGF-1 on the cardiovascular system. Curr Pharm Des. (2019) 25:3715–25. doi: 10.2174/1381612825666191106091507
60. Iqbal MA, Siddiqui FA, Gupta V, Chattopadhyay S, Gopinath P, Kumar B, et al. Insulin enhances metabolic capacities of cancer cells by dual regulation of glycolytic enzyme pyruvate kinase m2. Mol Cancer. (2013) 12:72. doi: 10.1186/1476-4598-12-72
61. Dimic D, Velojic Golubovic M, Antic S, Radenkovic S. Evaluation of the repaglinide efficiency in comparison to the glimepiride in the type 2 diabetes patients poorly regulated by the metmorfine administration. Bratisl Lek Listy. (2009) 110:335–9.
62. Donath H, Hess U, Kieslich M, et al. Diabetes in Patients with Ataxia telangiectasia: A National Cohort Study. PREPRINT (Version 1). Available online at: https://doi.org/10.21203/rs.3.rs-21121/v1 (accessed April 08, 2020).
Keywords: ataxia telangiectasia, diabetes, HbA1c, OGTT, diabetes therapy
Citation: Donath H, Hess U, Kieslich M, Theis M, Ohlenschläger U, Schubert R, Woelke S and Zielen S (2020) Diabetes in Patients With Ataxia Telangiectasia: A National Cohort Study. Front. Pediatr. 8:317. doi: 10.3389/fped.2020.00317
Received: 13 April 2020; Accepted: 18 May 2020;
Published: 09 July 2020.
Edited by:
Prashant Kumar Verma, All India Institute of Medical Sciences, Rishikesh, IndiaReviewed by:
Luciana Chessa, Sapienza University of Rome, ItalyCopyright © 2020 Donath, Hess, Kieslich, Theis, Ohlenschläger, Schubert, Woelke and Zielen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helena Donath, aGVsZW5hLmRvbmF0aEBrZ3UuZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.