 Jun-Yi Wang
Jun-Yi Wang Pei-Jin Hu
Pei-Jin Hu Dong-Mei Luo1
Dong-Mei Luo1 Yi Song
Yi Song Jun Ma
Jun Ma Patrick W. C. Lau
Patrick W. C. Lau- 1Institute of Child and Adolescent Health, Peking University School of Public Health, National Health Commission Key Laboratory of Reproductive Health, Beijing, China
- 2Department of Sport and Physical Education, Hong Kong Baptist University, Kowloon Tong, China
Background: The aim of this study was to assess the geographic disparity in anemia and whether stunting was associated with anemia in different geographic groups among school-aged children in China.
Methods: 71,129 Han children aged 7, 9, 12, and 14 years old were extracted from the 2014 cycle of Chinese National Surveys on Children Constitution and Health. Anemia, anemia severity, and stunting were defined according to WHO definitions. Binary logistic regression models were used to estimate the association between anemia and stunting in different geographic groups.
Results: The prevalence of anemia was significantly higher in girls (10.8%) than boys (7.0%). The highest anemia prevalence was in Group VII (lower class/rural, 12.0%). A moderate/severe prevalence of anemia was concentrated in Group VII and Group VIII (western/lower class/rural) for both sexes. The prevalence of anemia was higher in stunting boys than non-stunting boys in Group IV (lower class/city, χ2 = 12.78, P = 0.002) and Group VII (χ2 = 6.21, P = 0.018), while for girls, it was higher in stunting girls than their non-stunting peers only in Group II (upper class/large city, χ2 = 4.57, P = 0.046). Logistic regression showed that the stunting children have 30% higher risk of anemia than non-stunting children after adjustment for age, sex and school (OR = 1.30, 95% CI: 1.05–1.60).
Conclusion: A significant geographic disparity and an association between anemia and stunting among specific groups of school-aged children in China was demonstrated. Consequently, eliminating the geographic disparity and ameliorating stunting might contribute to the improvement of Chinese children's anemia. Specific guidelines and interventions are needed, especially for adolescent girls and the groups with serious anemia burden.
Introduction
Anemia, or low concentrations of hemoglobin (Hb), adversely affects cognitive and motor development and study capacity, and increases susceptibility to infection, which also exerts a substantial economic burden on the government (1, 2). Globally, 1.62 billion people suffer with anemia and the prevalence among children was 25.4%, according to a World Health Organization (WHO) (3) report. Asia is the hardest hit, especially in South Asia (4, 5), where an improvement in children's hemoglobin status may lead to a modest global increase in mean hemoglobin and a reduction in anemia prevalence. Globally, anemia is affecting people in both developed and developing countries with different health risks, and almost all age groups and both sexes are susceptible. Even for developed countries, such as Sweden, France, Australia, Denmark, Belgium, and Ireland, anemia prevalence has changed little during past two decades (6). Although iron deficiency anemia is the true indicator of poor nutritional status, considering that 90–95% of anemia cases in China are due to iron deficiency (7), anemia remains useful as an indicator of undernutrition and is particularly relevant for adolescents in the context of rapid growth and menstruation. Compared with children under five and pregnant women, adolescents have not been paid much attention. In 2016, 333 million adolescents with anemia lived in multi-burden settings, of which 194 million lived in India and China according to GBD (Global Burden of Disease study) data (6). Although the prevalence of anemia in China has declined in the past two decades at the national level (8), it was as high as 14.8% in some rural regions like Shanxi (9, 10). Nationwide, more than 19.2 million Chinese children were anemic and 389,198 had severe anemia in 2010, based on a total number of children aged 7–18 years (194,599,052). Nevertheless, updated information of geographic disparity on anemia among Chinese children is unclear. This information is urgently needed as it may provide a solid foundation to alleviate the geographic disparity of anemia among Chinese children.
In China, most anemia is due to prolonged iron deficiency, which impairs hemoglobin production and limits the amount of oxygen that red blood cells carry throughout the body and to the brain (11). Stunting is also a big issue in China and warrants monitoring because it is an undervalued indicator which reflects the cumulative effect of undernutrition with socioeconomic and other factors. These factors may contribute to anemia. Studies in Haiti and Angola confirmed that stunting increased the risks of developing anemia (12, 13). The question is still uncertain as to whether stunting is associated with anemia in China, especially in school-aged children who have been largely under-investigated. Moreover, if the association exists, does it vary or remain similar in different settings and populations?
Hemoglobin data from children aged 7 to 14 of both sexes across China was collected in the 2014 Chinese National Surveys on Students' Constitution and Health (CNSSCH). It provided a valuable opportunity to update the available information on anemia among school-aged children who have been largely neglected in research in China, compared with numerous publications on children under five and pregnant women (14). The objectives of the present study were to: (1) delineate the geographic disparity of anemia; (2) identify the most susceptible population with the heaviest burden of anemia; and (3) examine the association between anemia and stunting, and the relationships across different geographic groups.
Materials and Methods
Data was extracted from the 2014 cycle of CNSSCH, which was a large-scale cross-sectional survey of school-aged children conducted by six relevant ministries including the Ministries of Education, Health, Science and Technology, the State Ethnic Affairs Commission, and the State Sports General Administration, China. It spanned 31 provinces, excluding Hong Kong, Macau, and Taiwan. The sampling procedure, as previously described in detail (14), was the same in all CNSSCH survey sites. In brief, this survey was to investigate children's health status in China and used a multistage stratified cluster sampling design (14). In the first stage of sampling, in order to achieve better representation within the 30 provinces, populations were stratified by three socioeconomic indicator groups or three sets of prefecture-level cities (i.e., upper, moderate, low) at the regional level, defined by regional gross domestic product, total yearly income per capita, average food consumption per capita, natural growth rate of the population, and the regional social welfare index. In each group of three sub-provincial levels, one city was selected randomly and remained constant from the first survey in 1985. Within these sub-province regions, populations were also stratified by urban and rural area of residence. Within these stratified areas, a random selection of schools, including primary school, middle school, and high school, was conducted according to the established procedures. In the second stage, sampling took place in classes (primary sampling units or clusters) selected randomly from each grade in these schools, and all students in the selected class were included and listed in the investigation after meeting the inclusion criteria and after obtaining verbally informed consent from both students and their parents. Finally, within the primary sampling units, namely every age from 7 to 18 years for boys and girls, at least 50 Han ethnicity students, the minimum sample size, were included in the survey and sampling yielded equal numbers of the three socioeconomic indicator groups. Thus, the sample weight remained consistent in each age, sex, region (urban/rural), city (three socioeconomic indicators' groups at sub-province level), and province for students aged 7–18 years in each survey year. The participants in this study were Han children aged 7, 9, 12, and 14 years old from 26 provinces and four municipalities, except for Tibet (where the Han ethnicity is a minority). The children were recruited in this study if their parents and themselves had lived in their local regions more than a year.
Participants underwent a medical examination prior to the national survey and were excluded if they had one or more of the following conditions: (1) serious organ disease (e.g., heart, lung, liver, kidney); (2) abnormal physical development (e.g., pygmyism, gigantism); (3) physical impairment or deformity (e.g., severe scoliosis, pectus carinatum, limp, genu valgum, and gunu varum); or (4) acute disease symptoms (e.g., diarrhea, fever) during the past month and not yet recovered. Consequently, 71,129 children with complete data records on age, sex, urban/rural groups, height, weight and hemoglobin concentration were included in the analysis. Moreover, the ratio of boys/girls or urban/rural groups was approximately equal to 1:1 of each sex- and age-specific subgroup. The project was approved by the Medical Research Ethics Committee of Peking University Health Science Center (IRB00001052-18002). With data collected from schools across China, the school principals were able to determine the process for gaining informed consent from children's parents or guardians. All participants' information was anonymized and de-identified prior to analysis to protect their privacy.
Measures
Participants were required to wear light clothing and stand straight, barefoot, and at ease when height was measured. The heel, humerus, and shoulders were contacted to form a “three-point, one-line” standing position. Measurements were conducted by a team of trained field professionals who were required to pass a training course in anthropometric measurements. Height was measured to the nearest 0.1 cm with a portable stadiometer. The stadiometers were calibrated before use. The measurements were carried out at the same time of the day during the survey (better to be specific, e.g., morning, afternoon, during school recess, etc.). Height-for-age Z-score (HAZ) was calculated by using WHO 2007 references with the fixed population. Stunting was defined using the growth references of HAZ: stunting: < −2SD (15, 16).
Hemoglobin concentration was measured by laboratory technicians for the participants in the selected school. Hemoglobin concentration was measured by HemoCue201+ (Origin: Sweden, Model: HemoCue201+, Manufacturer: HemoCue AB) (17). Data collection was supervised as follows by well-trained on-site investigators: (a) the capillary blood sample was collected from the fingertip after discarding the first drop, and a small amount of blood was pressed out onto the fingertips. The blood was taken continuously with a micro cuvette, (b) the micro cuvette was inserted into the cuvette tank and reacted for 15s to 60s, (c) the score was determined and recorded on site (18). Age specific cut-off values of hemoglobin concentration were used to define anemia. Hemoglobin concentration was defined by using WHO criteria (19, 20) and categorized as: (1) for children aged 5 to 11 year: ≥115 g/L normal, <115 g/L anemia, 110–114 g/L mild anemia, ≤ 109 moderate/severe prevalence anemia; (2) for children aged 12–14 year: ≥120 g/L normal, <120 g/L anemia, 110–119 g/L mild anemia, ≤ 109 g/L moderate/severe prevalence anemia.
In order to compare the prevalence of anemia in different geographic groups with different socioeconomic status (SES), all subgroups were further divided into eight categories (21): Group I (large coastal city), Group II (upper class/large city), Group III (middle class/city), Group IV (lower class/city), Group V (upper class/rural), Group VI (middle class/rural), Group VII (lower class/rural), and Group VIII (western/lower class/rural). Group I included the nine largest cities (Beijing, Shanghai, Tianjin, Shijiazhuang, Shenyang, Dalian, Jinan, Qingdao, and Nanjing) and Group II represented the upper urban class. Group VIII constituted the other extreme: rural regions in western provinces, home to the lowest SES class (data was shown in Figure 1).
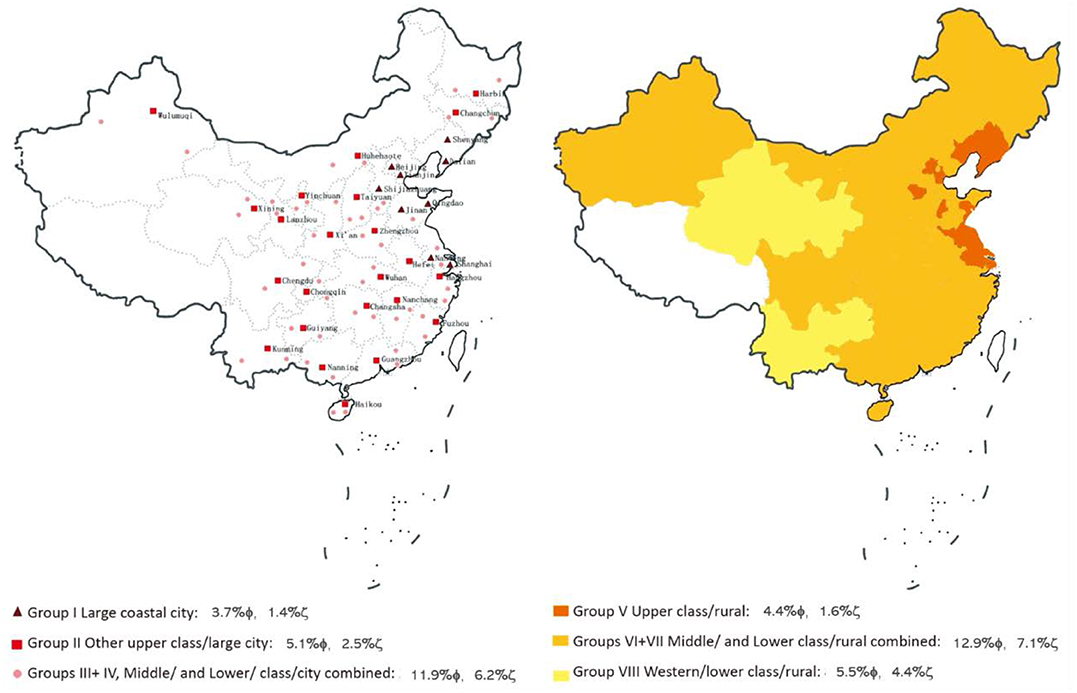
Figure 1. The distribution of different geographic groups with different socioeconomic status (SES); note: ϕ the prevalence of mild anemia in 2014, ζ the prevalence of moderate/severe anemia in 2014.
Statistical Analyses
The prevalence of anemia in the Han children was described by sex, age, and geographic groups. Chi-square test was used to assess the difference of the prevalence and categories of anemia among different subgroups, while the inspection level was adjusted by Bonferroni method [α′=2α/k(k−1), k = 7]. To assess the geographic difference of association between anemia and stunting, binary logistic regression analyses were conducted with adjustments for sex and age. The design effect of cluster sampling by school was also added in the model. All analyses were conducted using Stata 12.1 (Stata Corp, College Station, Texas). A 2-sided P-value of <0.05 was considered significant.
Results
The Prevalence of Anemia in Different Geographic Groups
As shown in Table S1, the prevalence of anemia was significantly higher in girls (10.8%) than boys (7.0%). The highest anemia prevalence was in Group VII (12.0%). The lowest prevalence of anemia was observed in Group I (5.2%), Group V (6.0%), and Group II (7.6%). The prevalence of anemia in Group I was more than twice that of Group VII. Table S2 demonstrates that the moderate/severe prevalence of anemia was concentrated in Group VII and Group VIII for both sexes. The prevalence of anemia at each age group was similar to the total sample and the highest prevalence of anemia was found in the age 7 group, followed by 12 years, and the lowest prevalence was the 14-year-old boys group. For girls, those aged 12 and 14 years had significantly higher anemia prevalence than those of 7 and 9 years (data was shown in Table S3).
The Prevalence of Anemia in Susceptible Population
Girls had a higher prevalence of anemia than boys across different groups. The prevalence of anemia among girls in Group VII was 4–5 times higher than boys in Group I (Table S1). Table 1 and Table S4 indicate that the prevalence of anemia among stunting children was higher than their non-stunting counterparts. When stratified by sex, the prevalence of anemia was higher in stunting boys than non-stunting boys in Group IV (χ2 = 12.78, P = 0.002) and Group VII (ψ2 = 6.21, P = 0.018), while for girls, the anemia prevalence was higher in stunting girls than their non-stunting peers only in Group II (χ2 = 4.57, P = 0.046).
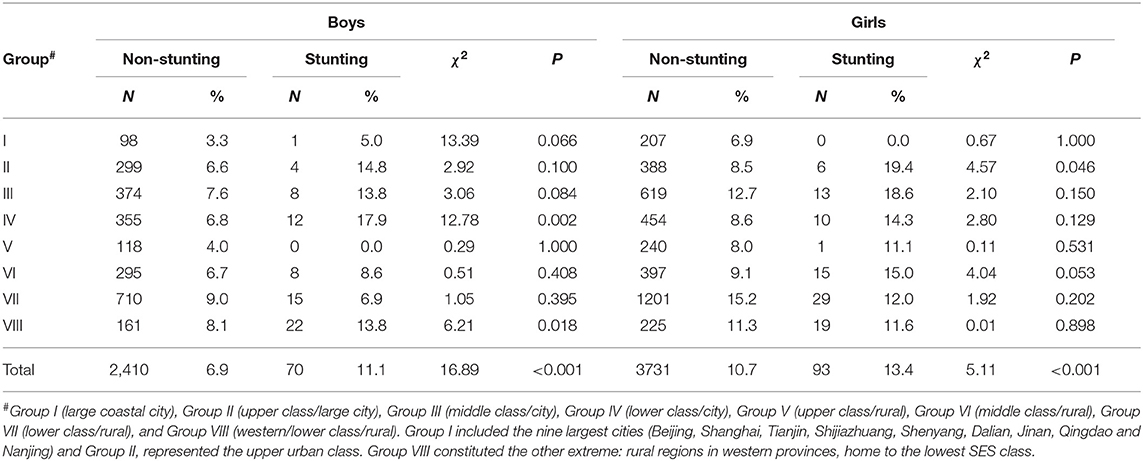
Table 1. The prevalence of anemia stratified by stunting status, geographic group, and sex among Chinese school-aged children.
The Association Between Anemia and Stunting Stratified by Geographic Groups and Sex
As shown in Table 2, the stunting children have a 30% higher risk of anemia than non-stunting children (OR = 1.30, 95% CI: 1.05–1.60). When stratified by geographic group, the association strengths ranged from 1.41 to 2.34 in Group II, III, IV, VI, and VIII but with 95% CI overlap, while there was no significant association between anemia and stunting in Group I, V, and VII. After stratifying by sex, stunting boys were 1.74 times more likely to be anemic than non-stunting boys while there was no significant association between stunting and anemia among girls. The results of the associations by age stratification were consistent with total sample (data not shown).
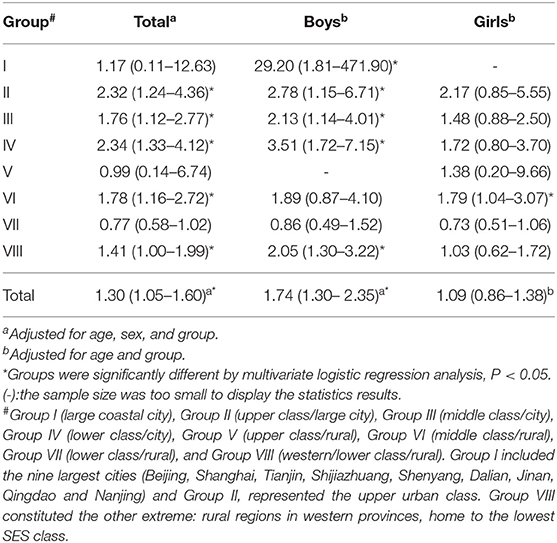
Table 2. Association between anemia and stunting stratified by geographic group and sex among Chinese school-aged children.
Discussion
In the present study, by using data from the 2014 CNSSCH covering 26 provinces and four municipalities in China, not only were the differences in the prevalence of anemia among school-aged children by geographic groups, sex, and stunting status documented, but also the major associations between anemia and stunting in school-aged children. On the whole, the prevalence of anemia was significantly higher in girls than in boys, and in addition there was low prevalence of anemia in areas with good economic conditions. However, some regions, such as the poorer rural setting of Group VII and middle-class cities of Group III might be overlooked.
Researchers have pointed out that geographic disparity was related inversely to SES, to wealth at a household level, and to income and education at an individual level (2, 22, 23). Areas with SES were often geographically good, and also had better health care facilities and services (24). Compared to rural areas, individuals living in better SES have a greater availability of food and better housing, electricity, piped water, sanitation, and transportation. Moreover, these populations usually have a higher educational level, economic status, and employment opportunities. Studies in Indonesia have found child stunting to be associated with poor health care practices, inadequate sanitation and water supply, food insecurity, and low caregiver education (25). Sankar Goswmai's study used the wealth index to reflect the state of SES and the results indicated that, relatively, the poorest area had the highest prevalence of anemia (OR = 2.033, 95% CI:1.71–2.22), while the richer area had lowest prevalence of anemia (OR = 1.183, 95% CI:1.14–1.32) (26). In groups with these good economic development indicators, the prevalence of anemia was low; the study mentioned that a child living in a household in the lowest wealth quintile was 21% more likely to be anemic than were those in the highest wealth quintile (27), which is consistent with the present study. In Group I (large coastal city) and Group II (other upper class/large city), the economic development is relatively high and anemia prevalence is relatively lower than other groups. High quality living environments and facilities due to advanced economic development can contribute to anemia reduction among Chinese children (2). A previous study conducted in 32 selected low-income and middle-income countries showed that a child living in a household in the lowest wealth quintile was 21% more likely to be anemic than those in the highest wealth quintile (2). However, the prevalence of anemia did not disappear in Group I and Group II, which indicated that improving the monitoring of anemia, scaling up coverage of prevention, and developing anemia prevention interventions were still needed in China (28, 29).
China has long been concerned about the imbalance of geographic disparity, thus, improving the health of children in rural western China remains a critical health priority (30). The national anemia prevention intervention policy was mainly implemented in the area of Group VIII, i.e., “National Nutrition Improvement Program for Rural Compulsory Education Students (NNIPRCES)” released by the general office of the State Council of China (2011) (31). Even though the prevalence of anemia in Group VIII has been significantly reduced after the implementation of the above policy (32), it is still serious due to its high baseline. Currently, Group VII has replaced Group VIII as the most serious burden of anemia because no extra attention has been given to this group. Other than continuing investment in anemia improvement in rural regions of western provinces, it is recommended that attention should be paid to other areas such as poorer rural settings in China. For example, nutritional education and improvement of diet quality should be included in the content of anemia intervention, to ensure the daily Recommended Dietary Allowance (RDA) of iron-containing foods (meat, milk, etc.) (33). These additional measures may play a more important role in decreasing anemia for vulnerable groups such as children living in western regions, boys with stunting issues, and adolescent girls (14).
Besides Group VII, Group III also had a surprisingly high prevalence of anemia. The higher prevalence of anemia in Group VII indicated that lower economic groups are susceptible and intervention needs to be focused here first, and as such it might be helpful to improve the anemic status by eliminating the geographic disparity. Considering the serious disparity, the government should reconsider the priorities around the anemic burden across the country and develop new strategies and interventions not only to the groups with serious burden, but also those at high risk like Group III.
In the present study, the association between anemia and stunting exists only in boys, but not in girls. Therefore, non-targeted anemia interventions, such as general nutrition improvement, may only work for boys. Ramachandran (34) pointed out that adolescent girls form a crucial segment of the population and constitute the vital “bridge” between the present generation and the next generation. The main reasons for this consequence among girls may be the menstrual bleeding during their puberty and weight loss (35, 36). In order to pursue a slim figure, adolescent girls deliberately lose their body weight by dieting, which may lead to insufficient iron intake (37). Iron deficiency may be a routine consequence of growth and skeletal development (38). Sex differences should be taken into account when implementing anemia interventions. Consequently, it is suggested that all children, especially adolescent girls, need health education due to their vulnerability to anemia (39). Furthermore, reliable measures on the causes of anemia are needed to guide interventions (40).
China, with its significant economic development in recent decades, has experienced epidemiological and demographic transitions which have affected its population's nutritional conditions and produced environments that have contributed to a change in anemia (41). Despite the nutritional transition and improved nutritional status, stunting and anemia remain a major public health problem in China (42). There were some common factors in the occurrence of anemia and stunting. As we all know, the main risk factor for anemia among children is low iron intake at a stage of life in which iron requirement is high. Iron, as an essential trace mineral, is necessary for linear growth and body tissue proliferation (43). Meanwhile, stunting is an indicator of long-term chronic malnutrition, which is primarily caused by insufficient nutrition supply (44). The supply of nutrients includes not only macro-nutrients, but also micronutrients, such as iron (45). One reason why stunting may be related to anemia is that stunting may pick up deficiencies in iron, which are also known to boost the risk of anemia through impaired erythropoiesis and oxidative stress pathways (44). Especially for children in groups with high prevalence of stunting, all age-groups of children were vulnerable groups for anemia (46). In addition, it is worth noting that school-aged children in Group III (middle class/city) in China have been facing the double burden of anemia and stunting. Therefore, “the child- and adolescent- specific dietary guidance” is able to guide children to a reasonable quality diet, which refers to the “recommended daily dietary allowances for children and adolescents” established by the Chinese Nutrition Society (47). WHO recommends that a diet containing adequate amounts of bioavailable iron could prevent and control anemia (48). In addition, community-based platforms for nutrition education and government commitment and focus on equity are also important factors that may lead to the implementation of interventions that prevent and treat child stunting (49–51).
There are limitations in the present study. Firstly, it was a cross-sectional study and it cannot infer causality between anemia and stunting. Secondly, samples of capillary blood from the fingertip of each child were collected after discarding the first drop. Capillary blood can't distinguish the type and cause of anemia. Thirdly, iron deficiency and other nutrient indicators were not assessed directly.
Conclusions
The present study demonstrated a large geographic disparity in anemia in China. Lower anemia is found in better SES groups, while the higher prevalence is shown in poorer SES groups. The prevalence of anemia in Group VIII was not only due to SES, but also stunting. In addition to focusing on the rural western regions, the government should also pay more attention and provide more resources to the population in middle class cities and lower-class rural areas. The present findings imply that previous measures aimed at improving anemia, regardless of sex and with a limited focus on school-aged children in poor groups, may not be comprehensive enough to tackle the anemia problem in China. Specific strategies and interventions should be developed for children in susceptible groups, and especially for girls.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The project was approved by the Medical Research Ethics Committee of Peking University Health Science Center (IRB00001052-18002).
Author Contributions
J-YW and YS conceptualized and designed the study and completed the statistical analyses. J-YW drafted the initial manuscript and reviewed and revised the manuscript. YS and YM designed the study and collected the data. D-ML and YS assisted with the statistical analyses. YM, JM, PL, BD, P-JH, D-ML, JD, and YS critically reviewed and revised the manuscript. All authors were involved in writing the paper and had final approval of the submitted and published versions.
Funding
This present study was supported by the National Natural Science Foundation (81673192, 81302442).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We acknowledge the revision suggestions from Lain Kiloughery, and also appreciate the investigators and students who participated in the surveys.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.00193/full#supplementary-material
References
1. Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR, Branca F, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Global Health. (2013) 1:e16–25. doi: 10.1016/S2214-109X(13)70001-9
2. Balarajan Y, Ramakrishnan U, Ozaltin E, Shankar AH, Subramanian SV. Anaemia in low-income and middle-income countries. Lancet. (2011) 378:2123–35. doi: 10.1016/S0140-6736(10)62304-5
3. Antwi-Bafour S, Hammond S, Adjei JK, Kyeremeh R, Martin-Odoom A, Ekem I. A case-control study of prevalence of anemia among patients with type 2 diabetes. J Med Case Rep. (2016) 10:110. doi: 10.1186/s13256-016-0889-4
4. Kojima S. Why is the incidence of aplastic anemia higher in Asia? Exp Rev Hematol. (2017) 10:277–79. doi: 10.1080/17474086.2017.1302797
5. WHO. Worldwide Prevalence of Anaemia 1993-2005 - WHO Global Database on Anaemia. Geneva: World Health Organization (2008). Available online at: http://www.who.int/iris/handle/10665/43894 (accessed May 2, 2019).
6. Azzopardi PS, Hearps SJC, Francis KL, Kennedy EC, Mokdad AH, Kassebaum NJ, et al. Progress in adolescent health and wellbeing: tracking 12 headline indicators for 195 countries and territories, 1990–2016. Lancet. (2019) 393:1101–18. doi: 10.1016/S0140-6736(18)32427-9
8. China NBoSo. Tabulation on the 2010 Population Census of the People's Republic of China. (2011). Available online at: http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm (accessed May 5, 2019).
9. Zhan Y, Chen R, Zheng W, Guo C, Lu L, Ji X, et al. Association between serum magnesium and anemia: china health and nutrition survey. Biol Trace Elem Res. (2014) 159:39–45. doi: 10.1007/s12011-014-9967-x
10. Gan QL, Chen J, Yang T, Li L, Xu P, Pan H, et al. Prevalence of anemia among students from National Improvement Program for Rural Compulsory Students in 2013. Chin J Sch Health. (2016) 37:674–75. doi: 10.16835/j.cnki.1000-9817.2016.05.011
11. Luo R K-WM, Rozelle S, Zhang L, Liu C, Sharbono B, Shi Y, et al. Anemia in Rural China's elementary schools- prevalence and correlates in Shaanxi Province's Poor Counties. Ecol Food Nutr. (2010) 49:357–72. doi: 10.1080/03670244.2010.507437
12. Iannotti L, Delnatus JR, John ARO, Eaton JC, Griggs JJ, Brown S. Determinants of anemia and haemoglobin concentration in haitian school-aged children. PLoS ONE. (2015) 93:1092–98. doi: 10.4269/ajtmh.15-0073
13. Oliveira D, Ferreira FS, Atouguia J, Fortes F, Guerra A, Centeno-Lima S. Infection by intestinal parasites, stunting and anemia in school-aged children from Southern Angola. PLoS ONE. (2015) 10:e0137327. doi: 10.1371/journal.pone.0137327
14. Song Y, Wang HJ, Dong B, Wang Z, Ma J, Agardh A. National trends in haemoglobin concentration and prevalence of anemia among Chinese School-Aged Children, 1995-2010. J Pediatr. (2017) 183:164–69.e2. doi: 10.1016/j.jpeds.2017.01.012
15. Organization WH. WHO Reference 2007 SPSS Macro Package. (2007). Available online at: http://www.who.int/entity/growthref/tools/readme_spss.pdf (accessed May 4, 2019).
16. Onis MD, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Org. (2007) 85:660–7. doi: 10.2471/BLT.07.043497
17. Nkrumah B, Nguah SB, Sarpong N, Dekker D, Idriss A, May J, et al. Haemoglobin estimation by the HemoCue(R) portable haemoglobin photometer in a resource poor setting. BMC Clin Pathol. (2011) 11:5. doi: 10.1186/1472-6890-11-5
18. World Health Organization (WHO). Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. (2011). Available online at: http://apps.who.int/iris/bitstream/10665/85839/3/WHO_NMH_NHD_MNM_11.1_eng.pdf (accessed May 4, 2019).
19. World Health Organization (WHO) U, UNU. Iron Deficiency Anaemia Assessment, Prevention, and Control, A Guide for Programme Managers. Geneva: World Health Organization (2001).
20. Chan M. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. China: World Health Organization (2011). p. 1–6.
21. Ji CY, Chen TJ, Working Group on Obesity in C. Empirical changes in the prevalence of overweight and obesity among Chinese students from 1985 to 2010 and corresponding preventive strategies. Biomed Environ Sci. (2013) 26:1–12.
22. Melku M, Addis Z, Alem M, Enawgaw B. Prevalence and predictors of maternal anemia during pregnancy in Gondar, Northwest Ethiopia: an Institutional Based Cross-Sectional Study. Anemia. (2014) 2014:108593. doi: 10.1155/2014/108593
23. Adamu AL, Crampin A, Kayuni N, Amberbir A, Koole O, Phiri A, et al. Prevalence and risk factors for anemia severity and type in Malawian men and women: urban and rural differences. Popul Health Metr. (2017) 15:12. doi: 10.1186/s12963-017-0128-2
24. Alexis J, Comber CB, Robert Radburn. A spatial analysis of variations in health access- linking geography, socio-economic status and access perceptions. Int J Health Geogr. (2011) 10:1–11. doi: 10.1186/1476-072X-10-44
25. Beal T, Tumilowicz A, Sutrisna A, Izwardy D, Neufeld LM. A review of child stunting determinants in Indonesia. Matern Child Nutr. (2018) 14:e12617. doi: 10.1111/mcn.12617
26. World Health Organization (WHO). Reducing Stunting in Children- Equity Considerations for Achieving the Global Targets 2025. (2018). Available online at: https://apps.who.int/iris/handle/10665/260202 (accessed May 11, 2019).
27. Goswmai S, Das KK. Socio-economic and demographic determinants of childhood anemia. J Pediatr. (2015) 91:471–7. doi: 10.1016/j.jped.2014.09.009
28. Okumura MJ, Knauer HA, Calvin KE, Takayama JI. Caring for children with special health care needs: profiling pediatricians and their health care resources. Matern Child Health J. (2018) 22:1042–50. doi: 10.1007/s10995-018-2484-3
29. Dreshaj HNA. Global challenges for the environment, water clean and economic advantages. Int J Eng Trends Technol. (2013) 4:1–5. Available online at: https://ssrn.com/abstract=2835964
30. Huo YJ, Zhou H, Wang Y. Status of underweight and it's relative factors for children under 3 years old in 14 counties in the western areas of China. Chin Journal Child Health Care. (2017) 25:552−5. doi: 10.11852/zgetbjzz2017-25-06-04
31. Cardoso MA, Augusto RA, Bortolini GA, Oliveira CS, Tietzman DC, Sequeira LA, et al. Effect of providing multiple micronutrients in powder through primary healthcare on anemia in young Brazilian children: a multicentre pragmatic controlled trial. PLoS ONE. (2016) 11:e0151097. doi: 10.1371/journal.pone.0151097
33. de Souza Queiroz S, de A. Torres M. Iron deficiency anemia in children. J Pediatr. (2000) 76:298–304. doi: 10.2223/JPED.167
34. Ramachandran P. Health and nutrition in adolescents and young women: preparing for the next generation. J Health Med Nurs. (2017) 145:256–57. doi: 10.1016/j.ijhydene.2013.08.087
35. Choi JLMSS. Attempts to lose weight among US children- importance of weight perceptions from self, parents, and health professionals. Obesity. (2018) 26:597–605. doi: 10.1002/oby.22106
36. Powers J M, Stanek J R, Lakshmi S, Haamid FW, O'Brien SH. Hematologic considerations and management of adolescent girls with heavy menstrual bleeding and anemia in U.S. Children's Hospitals. J Pediatr Adolesc Gynecol. (2018) 31:446–50. doi: 10.1016/j.jpag.2018.06.008
37. Zhang CX, Chen YM, Chen WQ, Su YX, Wang CL, Wu JN. Food group intake among adolescents in guangzhou city compared with the Chinese Dietary Guidelines. Asia Pac J Clin Nutr. (2012) 21:450–6. doi: 10.6133/apjcn.2012.21.3.18
38. Verma A, Rawal VS, Kedia G, Kumar D, Chauhan J. Factors influencing anemia among girls of school going age (6–18 years) from the slums of Ahmedabad City. Ind J Comm Med. (2004) 29:25−6.
39. Thummakomma K, Meda P, Jayashankar T. Impact of change in dietary behavior and iron supplemention for reduction of iron deficiency anemia in rural adolescent girls. Int J f Agric. (2017) 7:525–28. doi: 10.24247/ijasraug201768
40. Patton GC, Sawyer SM, Santelli JS, Ross DA, Afifi R, Allen NB, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. (2016) 387:2423–78. doi: 10.1016/S0140-6736(16)00579-1
41. Mikki N, Abdul-Rahim HF, Awartani F, Holmboe-Ottesen G. Prevalence and sociodemographic correlates of stunting, underweight, and overweight among Palestinian school adolescents (13-15 years) in two major governorates in the West Bank. BMC Public Health. (2009) 9:485. doi: 10.1186/1471-2458-9-485
42. Zou Y, Zhang R-H, Xia S-C, Huang LC, Fang YQ, Meng J, et al. The rural-urban difference in BMI and anemia among children and adolescents. Int J Environ Res Public Health. (2016) 13:1020. doi: 10.3390/ijerph13101020
43. Bruce BR. Modern nutrition in health and disease (tenth edition). Crit Care Med. (2006) 34:529–32. doi: 10.1097/01.CCM.0000236502.51400.9F
44. Fatimah APS. Iron intake and haemoglobin levels in stunting in adolescent. Althea Med J. (2016) 3:175–80. doi: 10.15850/amj.v3n2.782
45. Ramakrishnan U, Nguyen P, Martorell R. Effects of micronutrients on growth of children under 5 y of age: meta-analyses of single and multiple nutrient interventions. Am J Clin Nutr. (2008) 89:191–203. doi: 10.3945/ajcn.2008.26862
46. Assefa S, Mossie A, Hamza L. Prevalence and severity of anemia among school children in Jimma Town, Southwest Ethiopia. BMC Hematol. (2014) 14:1–9. doi: 10.1186/2052-1839-14-3
47. Ge KY. Chinese Nutrition Scientific Encyclopedia. Beijing: People's Medical Publishing House (2004). p. 1521–44.
48. World Health Organization (WHO). Global Nutrition Targets 2025: Anaemia Policy Brief. (2014). Available online at: https://www.who.int/nutrition/publications/ (accessed June 22, 2019)
49. Smith LC KF, Frankenberger TR, Wadud A. Admissible evidence in the court of development evaluation? The Impact of CARE's SHOUHARDO project on child stunting in Bangladesh. IDS Working Papers. (2011) 41:196–216. doi: 10.1111/j.2040-0209.2011.00376_2.x
50. Bhutta ZA, Das JK, Rizvi A, Gaffey MF, Walker N, Horton S, et al. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet. (2013) 382:452–77. doi: 10.1016/S0140-6736(13)60996-4
Keywords: anemia, geographic disparity, stunting, children, China
Citation: Wang J-Y, Hu P-J, Luo D-M, Dong B, Ma Y, Dai J, Song Y, Ma J and Lau PWC (2020) Reducing Anemia Among School-Aged Children in China by Eliminating the Geographic Disparity and Ameliorating Stunting: Evidence From a National Survey. Front. Pediatr. 8:193. doi: 10.3389/fped.2020.00193
Received: 09 October 2019; Accepted: 31 March 2020;
Published: 12 May 2020.
Edited by:
Kristine G. Koski, McGill University, CanadaReviewed by:
Satinder Aneja, Sharda University, IndiaSelda Rizalar, Istanbul Medipol University, Turkey
Copyright © 2020 Wang, Hu, Luo, Dong, Ma, Dai, Song, Ma and Lau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yinghua Ma, eWluZ2h1YW1hQGJqbXUuZWR1LmNu; Yi Song, c29uZ3lpQGJqbXUuZWR1LmNu