 Marimar Saez-de-Ocariz1
Marimar Saez-de-Ocariz1 María José Pecero-Hidalgo2Francisco Rivas-Larrauri3
María José Pecero-Hidalgo2Francisco Rivas-Larrauri3 Miguel García-Domínguez3Edna Venegas-Montoya3
Miguel García-Domínguez3Edna Venegas-Montoya3 Martín Garrido-García4
Martín Garrido-García4 Marco Antonio Yamazaki-Nakashimada3*
Marco Antonio Yamazaki-Nakashimada3*- 1Department of Dermatology, Instituto Nacional de Pediatría, Mexico City, Mexico
- 2Department of Pediatrics, Instituto Nacional de Pediatría, Mexico City, Mexico
- 3Department of Clinical Immunology, Instituto Nacional de Pediatría, Mexico City, Mexico
- 4Department of Cardiology, Instituto Nacional de Pediatría, Mexico City, Mexico
Rationale: Kawasaki disease (KD) is an acute vasculitis of small and medium vessels; whereas systemic lupus erythematosus (SLE) is a chronic systemic autoimmune disease. Their presentation is varied and not always straightforward, leading to misdiagnosis. There have been case reports of lupus onset mimicking KD and KD presenting as lupus-like. Coexistence of both diseases is also possible.
Patient concerns: We present three adolescents, one with fever, rash, arthritis, nephritis, lymphopenia, and coronary aneurysms, a second patient with rash, fever, aseptic meningitis, and seizures, and a third patient with fever, rash, and pleural effusion.
Diagnoses: The first patient was finally diagnosed with SLE and KD, the second patient initially diagnosed as KD but eventually SLE and the third patient was diagnosed at onset as lupus but finally diagnosed as KD.
Interventions: The first patient was treated with IVIG, corticosteroids, aspirin, coumadin and mycophenolate mofetil. The second patient was treated with IVIG, corticosteroids and methotrexate and the third patient with IVIG, aspirin and corticosteroids.
Lessons: Both diseases may mimic each other's clinical presentation. KD in adolescence presents with atypical signs, incomplete presentation, and develop coronary complications more commonly. An adolescent with fever and rash should include KD and SLE in the differential diagnosis.
Introduction
Kawasaki disease (KD) and systemic lupus erythematosus (SLE) are immune mediated diseases characterized by varied clinical features that may include vasculitis (1–3). Vasculitis in lupus is most commonly due to the local deposition of immune complexes, but some patients have an inflammatory vasculopathy in the absence of local immune complex deposition (3). SLE can present coronary arteritis with aneurysm formation (4). We present three patients with overlapping features of KD and SLE. All patients and/or parents provided informed consent for publication of the cases.
Case 1
A 16-year-old-male presented with a history of fever, weakness, headache with photophobia, abdominal pain, vomiting, and axillar lymphadenopathy. On physical examination he had persistent fever, conjunctival injection, malar erythema, erythematous and cracked lips, bilateral parotid enlargement, cervical lymphadenopathy and a diffuse photosensitive rash. Sicca symptoms were not present. KD was diagnosed, and intravenous immunoglobulins were started at 2 g/kg in addition to aspirin. The echocardiogram was within normal limits. After treatment, he was afebrile for 24 h, after which he presented seizures and neurological deterioration. Cranial computed tomography revealed changes suggestive of aseptic meningitis. A skin biopsy demonstrated an atrophic epidermis, necrotic keratinocytes, hydropic degeneration of the basal layer, basal membrane thickening and periadnexal and perivascular lymphocytic infiltration. Anti-Ro and IgM anti-β2-glycoprotein-1 antibodies were positive, antinuclear antibodies were negative. The diagnosis of systemic lupus erythematosus was made based on the presence of seizures, malar rash, photosensitivity and, positive anti-β2-glycoprotein-1 and anti-Ro antibodies. Corticosteroids, hydroxychloroquine, and methotrexate were started. He has been followed for more than 2 years, and the corticosteroids have been tapered with good evolution.
Case 2
A 12-year-old male was transferred to our hospital with the diagnosis of lupus. He had a history of 20 days of fever, arthralgias, alopecia, a thoracic and abdominal rash, vomiting, oral ulcers, pleural effusion, pancytopenia, lymphopenia, and positive antinuclear antibodies (1:320). On physical examination the patient had palmoplantar erythema with desquamation and perineal erythema. Work-up showed a complete blood cell count within normal limits, increased AST (70 UI/l), ALT (59 UI/l) and bilirrubin (total 8.1 mg/dl, direct 5.5 mg/dl), and negative anti-dsDNA and anti-Sm antibodies. The echocardiogram revealed cardiomegaly and pericardial effusion. The presence of fever, palmoplantar erythema with desquamation, perineal erythema, elevated transaminases, gallbladder hydrops and pericardial effusion led to a diagnosis of incomplete KD and intravenous immunoglobulins, aspirin and corticosteroids were administered. On follow up, cardiac and liver abnormalities resolved.
Case 3
An 11 year-old-female presented with a history of cervical adenopathy, followed 2 months later by left knee arthritis, malar rash, photosensitivity, dark urine and fever. On physical examination malar rash and intense Raynaud's phenomenon were noted (Figure 1). The diagnosis of lupus was made based on acute cutaneous lupus - malar erythema and photosensitivity -, arthritis, renal disease - cylindruria and proteinuria -, autoimmune hemolytic anemia, lymphopenia, positive antinuclear antibodies and anti-dsDNA antibodies. During her hospitalization fever continued and she presented erythematous crusted lips and a generalized rash with palmoplantar erythema. Intravenous immunoglobulins were administered with a presumptive diagnosis of Parvovirus-B19 infection. Methylprednisolone pulses were started, and improvement was observed. She was discharged with hydroxycloroquine, prednisone and mycophenolate mofetil. She presented periungueal desquamation while at home. One month later, she was readmitted to the hospital due to headache, seizures and persistent hypertension. Echocardiogram and heart MRI revealed large ectasia of the main left coronary artery (z-score + 6.12), large ectasia of the circumflex artery (z-score + 5.19), with normal proximal right coronary artery and large ectasia of the mid right coronary artery (z-score + 7.35) with mild mitral regurgitation (Figure 2).

Figure 1. Erythema in palms accompanied by intense Raynaud's phenomenon.
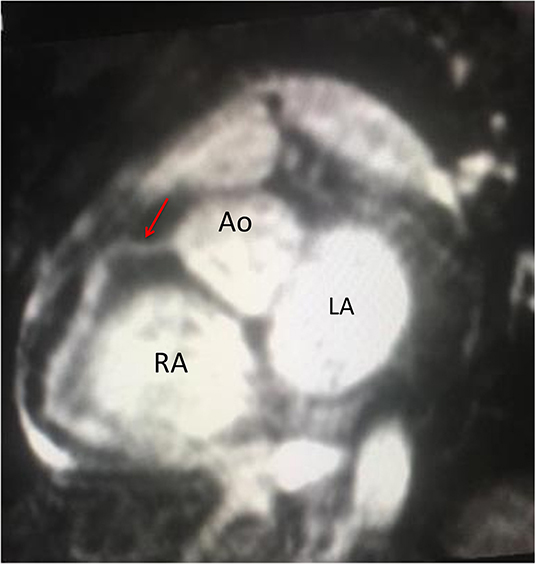
Figure 2. Magnetic resonance coronary angiography in a Whole-Heart iPAT sequence in a short axis view. Red Arrow: normal proximal right coronary artery 3 mm (z-score + 054), with dilated mid right coronary artery 6 mm (z-score + 7.35) and dilated distal right coronary artery 6 mm (z-score + 8.07). Ao, aorta; RA, Right atrium; LA, Left atrium (Courtesy of Dr. Roberto Cano).
Discussion
Clinical criteria are used to diagnose KD with the presence of fever and principal clinical features involving the mouth, eyes, skin, hands and feet and cervical lymphadenopathy (Table 1). SLE is a complex autoimmune disease with variable clinical features. In the absence of SLE diagnostic criteria, SLE classification criteria are often used by clinicians to help identify some of the salient clinical features when making the diagnosis. Children who fulfill the ACR criteria, SLICC criteria or the new EULAR/ACR criteria are considered to have definitive SLE (Table 2). Of note is that in the recent EULAR/ACR criteria, fever is considered a criterion suggestive of SLE.
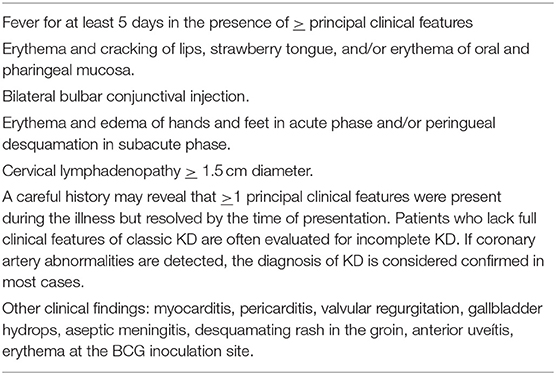
Table 1. Kawasaki disease classification criteria (AHA 2017 Guidelines).
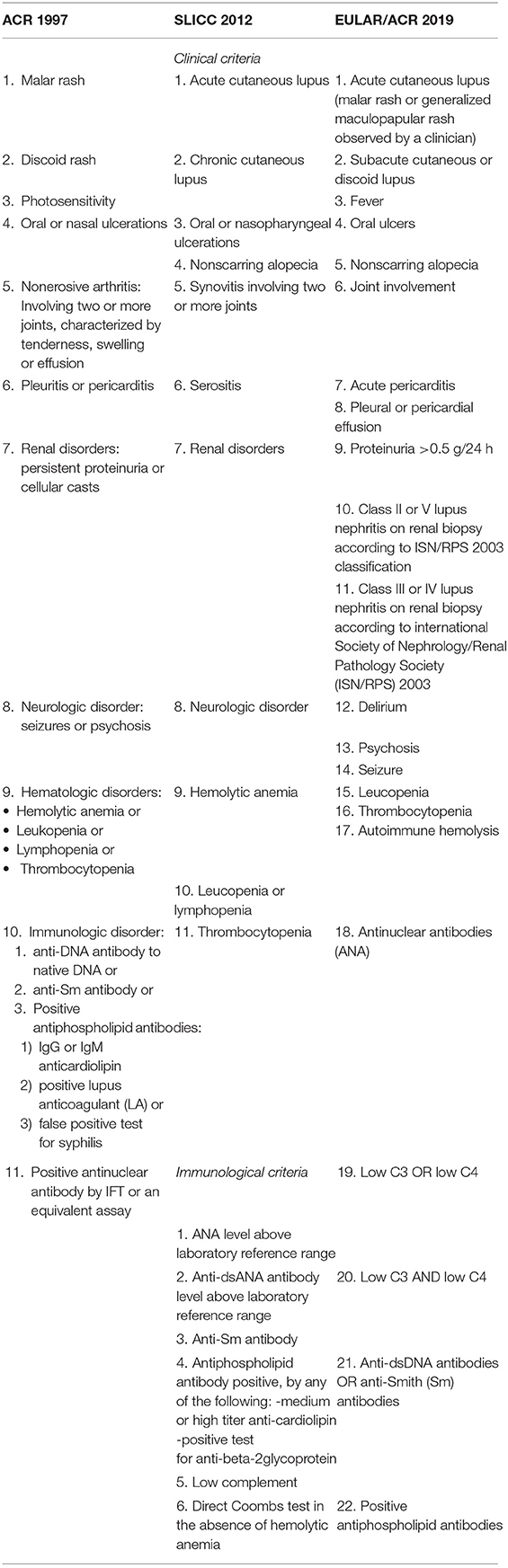
Table 2. Definitions of SLE classification criteria.
KD and SLE share several clinical manifestations: both diseases can present with fever, lymphadenopathy, arthritis or arthralgia, ocular and mucosal manifestations, rash and multisystemic involvement. However, the coexistence of both or misdiagnosis among them has seldom been reported (5–9). There are two previously reported cases of lupus-onset mimicking Kawasaki disease and vice versa and another three reported cases of the coexistence of both diseases (5–9) (Table 3).
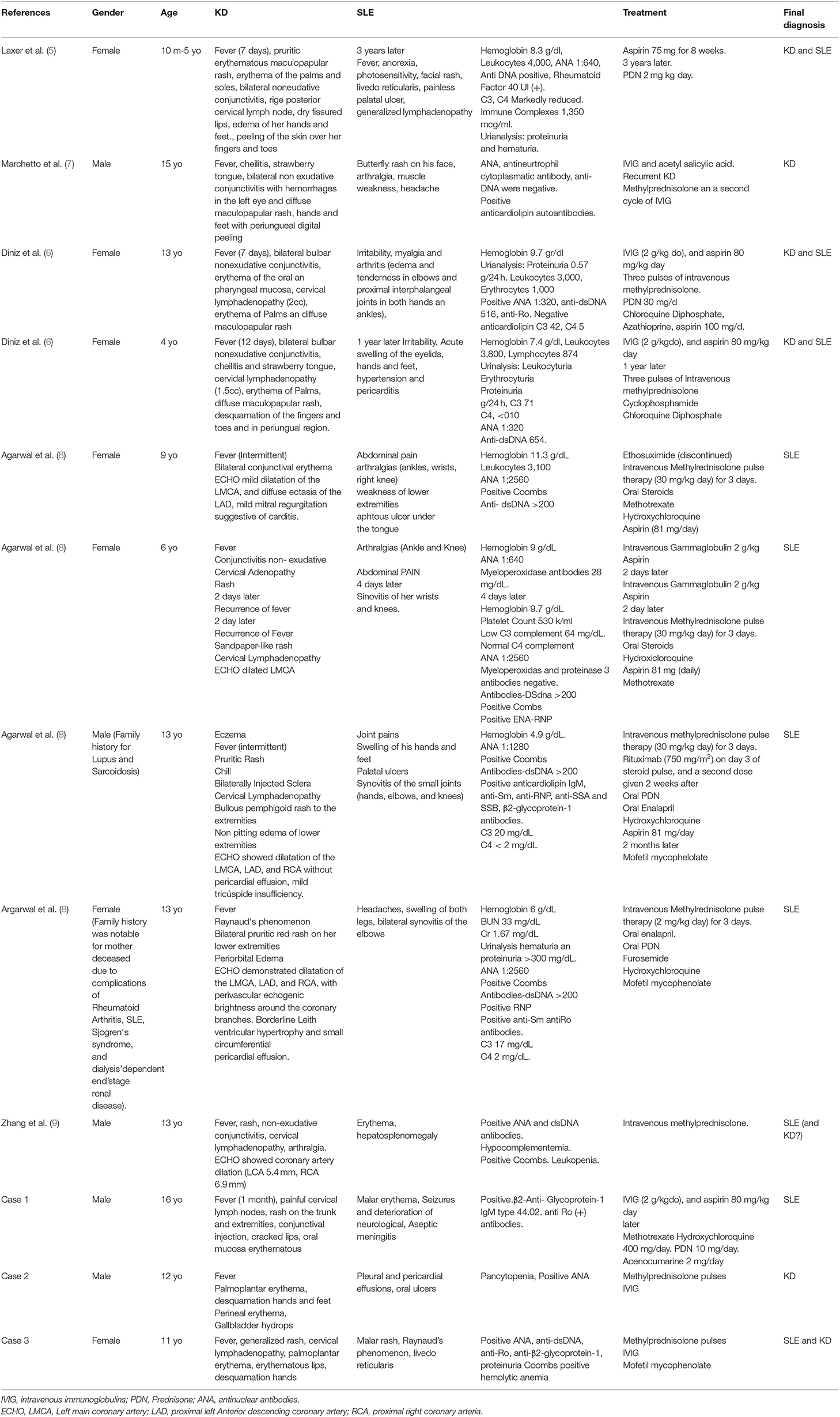
Table 3. Cases with overlapping features of KD and SLE.
The first patient was diagnosed with SLE and KD in an almost concurrent presentation, since she presented diagnostic criteria for both diseases. It can be discussed whether this case could only correspond to lupus with carditis, as the ones reported by Agarwal et al., however it is important to note that none of the four patients described by this author completed diagnostic criteria for KD (8). Recently, Zhang et al. (9) report a 13 year-old male who presented fever, rash, non-exudative conjunctivitis with cervical lymphadenopathy and an echocardiogram presenting coronary artery dilation. He was eventually diagnosed as SLE since he presented autoimmune hemolytic anemia, positive ANA, dsDNA and hypocomplementemia (9). As can be seen from previous reports (Table 3), both diseases can present simultaneously or with years of difference (5, 6, 9).
Coronary arteritis is not an exclusive feature of KD as other diseases like lupus and other vasculitis present this complication. In fact, coronary artery lesions have been documented in asymptomatic patients with microscopic polyangiitis, polyarteritis nodosa, and Wegener granulomatosis with MRI (10). Children with systemic onset juvenile idiopathic arthritis may present coronary artery dilation on echocardiograms similar to that observed for children with KD (11).
In our second patient the initial clinical picture made KD a diagnostic possibility; the skin biopsy was useful, as features were unequivocal for lupus. Parotitis was an unusual manifestation and can be present in both KD and lupus (12, 13). The third case was initially diagnosed as SLE, but eventually the clinical picture - despite atypical features such as pleural effusion, the response to treatment and the current health status under no medication, are more compatible with atypical KD (14).
Both KD and SLE share common features in terms of mechanisms of vascular inflammation and both may present with coronary artery dilatation. The two of them have been associated with the presence of anti-peroxiredoxin antibodies and the elevation of IL-17 (15, 16).
At this point, with the previously reported cases and our own it can be said that both diseases may mimic each other's clinical presentation. Interestingly, the majority of the patients that often present with the clinical challenge were tweens and teenagers (an unusual age for KD). KD in adolescence presents with atypical signs, incomplete presentation, and develop coronary complications more commonly (17). An adolescent with fever and rash should include KD and SLE in the differential diagnosis. As always in medicine, an accurate diagnosis is necessary to give appropriate treatment and reduce complications.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
Ethics Statement
Signed informed consent was obtained from the parents and the patients.
Author Contributions
MY-N, MS, and MP-H conceptualized and designed the study, reviewed, and revised the manuscript. MS and MY-N carried out the initial analyses and drafted the initial manuscript. FR-L and MG-G critically reviewed the manuscript. MP-H, EV-M, and MG-D recollected the data. All the authors were responsible for the treatment of the patient and read and approved the final manuscript.
Conflict of Interest
MY-N has received lecture fees from Shire, CSL Behring and Octapharma.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
KD, Kawasaki disease; SLE, systemic lupus erythematosus; IVIG, intravenous immunoglobulins; AST-Aspartate aminotransferase, ALT-Alanine transaminase.
References
1. McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Cardiovascular Surgery and Anesthesia; and Council on Epidemiology and Prevention. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. (2017) 135:e927–99. doi: 10.1161/CIR.0000000000000484
2. Petri M, Orbai AM, Alarcón GS, Gordon C, Merrill JT, Fortin PR, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. (2012) 64:2677–86. doi: 10.1002/art.34473
3. Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann Rheum Dis. (2019) 78:1151–9. doi: 10.1136/annrheumdis-2019-216700
4. Heibel RH, O'Toole JD, Curtiss EI, Medsger TA Jr, Reddy SP, Shaver JA, et al. Coronary arteritis in systemic lupus erythematosus. Chest. (1976) 69:700–3. doi: 10.1378/chest.69.5.700
5. Laxer RM, Cameron BJ, Silverman ED. Occurrence of Kawasaki disease and systemic lupus erythematosus in a single patient. J Rheumatol. (1988) 15:515–6.
6. Diniz JC, Almeida RT, Aikawa NE, Sallum AM, Sakane PT, Silva CA. Kawasaki disease and juvenile systemic lupus erythematosus. Lupus. (2012) 21:89–92. doi: 10.1177/0961203311414097
7. Marchetto S, Chiappini E, Simonini G, Falcini F, de Martino M. Lupus-like onset of recurrent Kawasaki disease in an adolescent boy. Clin Exp Rheumatol. (2004) 22:377.
8. Agarwal A, Medical Student SB, Lim-Stavros S, Votava-Smith JK, Ramanathan A. Pediatric systemic lupus erythematosus presenting with coronary arteritis: a case series and review of the literature. Semin Arthritis Rheum. (2015) 45:42–7. doi: 10.1016/j.semarthrit.2015.02.013
9. Zhang H, Zhang L, Guo N. Pediatric-onset systemic lupus erythematosus with coronary artery dilation: a case report. Medicine. (2020) 99:e18946. doi: 10.1097/MD.0000000000018946
10. Mavrogeni S, Manoussakis MN, Karagiorga TC, Douskou M, Panagiotakos D, Bournia V, et al. Detection of coronary artery lesions and myocardial necrosis by magnetic resonance in systemic necrotizing vasculitides. Arthritis Rheum. (2009) 61:1121–9. doi: 10.1002/art.24695
11. Binstadt BA, Levine JC, Nigrovic PA, Gauvreau K, Dedeoglu F, Fuhlbrigge RC, et al. Coronary artery dilation among patients presenting with systemic-onset juvenile idiopathic arthritis. Pediatrics. (2005) 116:e89–93. doi: 10.1542/peds.2004-2190
12. Seyedabadi KS, Howes RF, Yazdi M. Parotitis associated with Kawasaki syndrome. Pediatr Infect Dis J. (1987) 6:223. doi: 10.1097/00006454-198702000-00022
13. Azarisman SM, Heselynn H. Systemic lupus erythematosus presenting as parotitis and secondary Sjogren's syndrome. Singapore Med J. (2007) 48:e60–1.
14. Yavuz T, Nisli K, Yilmaz C, Dindar A. Large pleural effusion necessitates chest tube drainage in a patient with Kawasaki disease. J Paediatr Child Health. (2007) 43:191–2. doi: 10.1111/j.1440-1754.2007.01043.x
15. Karasawa R, Ozaki S, Nishioka K, Kato T. Autoantibodies to peroxiredoxin I and IV in patients with systemic autoimmune diseases. Microbiol Immunol. (2005) 49:57–65. doi: 10.1111/j.1348-0421.2005.tb03640.x
16. Park SJ, Shin JI. Interleukin-17 and B cell-activating factor in Kawasaki disease and juvenile systemic lupus erythematosus. Lupus. (2012) 21:1260. doi: 10.1177/0961203312457211
Keywords: Kawasaki disease, juvenile systemic lupus erythematosus, intravenous immunoglobulins, adolescent, atypical Kawasaki disease
Citation: Saez-de-Ocariz M, Pecero-Hidalgo MJ, Rivas-Larrauri F, García-Domínguez M, Venegas-Montoya E, Garrido-García M and Yamazaki-Nakashimada MA (2020) A Teenager With Rash and Fever: Juvenile Systemic Lupus Erythematosus or Kawasaki Disease? Front. Pediatr. 8:149. doi: 10.3389/fped.2020.00149
Received: 26 December 2019; Accepted: 17 March 2020;
Published: 07 April 2020.
Edited by:
Mamoru Ayusawa, Nihon University Itabashi Hospital, JapanReviewed by:
Surjit Singh, Post Graduate Institute of Medical Education and Research (PGIMER), IndiaAntonio Condino-Neto, University of São Paulo, Brazil
Copyright © 2020 Saez-de-Ocariz, Pecero-Hidalgo, Rivas-Larrauri, García-Domínguez, Venegas-Montoya, Garrido-García and Yamazaki-Nakashimada. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Antonio Yamazaki-Nakashimada, eXpraTcxQHlhaG9vLmNvbS5teA==