
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 18 February 2020
Sec. Genetics of Common and Rare Diseases
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.00045
This article is part of the Research Topic Genetic Testing in Pediatric Disorders View all 35 articles
 Rob M. Moonen1,2
Rob M. Moonen1,2 Maurice J. Huizing2
Maurice J. Huizing2 Gema E. González-Luis3
Gema E. González-Luis3 Giacomo Cavallaro4
Giacomo Cavallaro4 Fabio Mosca4
Fabio Mosca4 Eduardo Villamor2*
Eduardo Villamor2*The etiology of necrotizing enterocolitis (NEC) is multifactorial and an underlying genetic predisposition to NEC is increasingly being recognized. A growing number of studies identified single nucleotide polymorphisms (SNPs) of selected genes with potential biological relevance in the development of NEC. However, few of these genetic studies have been replicated in validation cohorts. We aimed to confirm in a cohort of 358 preterm newborns (gestational age <30 weeks, 26 cases of NEC ≥ Bell stage II) the association with NEC of three candidate SNPs: the vascular endothelium growth factor (VEGF) C-2578A polymorphism (rs699947), the interleukin (IL)-18 C-607A polymorphism (rs1946518), and the IL-4 receptor α-chain (IL-4Rα) A-1902G polymorphism (rs1801275). We observed that allele and genotype frequencies of the three SNPs did not significantly differ between the infants with and without NEC. In contrast, the minor G-allele of the IL-4Rα A-1902G polymorphism was significantly less frequent in the group of 51 infants with the combined outcome NEC or death before 34 weeks postmenstrual age than in the infants without the outcome (0.206 vs. 0.331, P = 0.01). In addition, a significant negative association of the G-allele with the combined outcome NEC or death was found using the dominant (adjusted odds ratio, aOR: 0.44, 95% CI 0.21–0.92), recessive (aOR 0.15, 95% CI 0.03–0.74), and additive (aOR 0.46, 95% CI 0.26–0.80) genetic models. In conclusion our study provides further evidence that a genetic variant of the IL-4Rα gene may contribute to NEC.
Necrotizing enterocolitis (NEC) is the leading cause of morbidity and mortality from gastrointestinal disease in very and extremely preterm infants (1, 2). As extensively discussed in several exhaustive reviews, the etiology of NEC is multifactorial and largely related to immaturity of the gastrointestinal tract (1–9). Besides low gestational age (GA), a complex interplay of other factors, such as type of feeding, gut dysbiosis, the high susceptibility of intestinal mucosal surface to inflammatory processes, or intestinal hypoperfusion may contribute to the pathogenesis of NEC (1–9). Nevertheless, NEC affects a minority of (very) preterm infants and clinical risk factors provide a limited explanation of the inter-individual variability in NEC susceptibility (3, 10). In the last years, an underlying genetic predisposition to NEC is increasingly being recognized (3, 10, 11).
As recently reviewed by Cuna et al., the candidate gene approach has been used in most studies on the genetics of NEC (3). Using this approach, a growing number of studies investigated single nucleotide polymorphisms (SNPs) of selected genes based on a-priori hypothesis of relevance to NEC. These studies particularly focused on mediators involved in the regulation of immune/inflammatory responses, such as toll like receptors, interleukins (ILs), tumor necrosis factor, or nuclear factor-kappa beta, and in the control of intestinal microcirculation, such as nitric oxide synthase, or vascular endothelium growth factor (VEGF) (3). However, few of these genetic studies have been replicated in validation cohorts (3). In the present study we aimed to confirm the association with NEC of three candidate SNPs: the VEGF C-2578A polymorphism (rs699947) (12, 13), the IL-18 C-607A polymorphism (rs1946518) (14), and the IL-4 receptor α-chain (IL-4Rα) A-1902G polymorphism (rs1801275) (15). We performed our investigation in a cohort of preterm infants from four neonatal intensive care units located in three different European countries (Spain, Italy, and the Netherlands) (16, 17).
The present study was performed on DNA samples collected during a previous study on carbamoyl phosphate synthetase SNPs as risk factor for NEC (16). The protocol of the above study was reviewed and approved by the institutional review board (IRB) for each participating center (see names below) and we obtained written informed consent from the parents. The consent also allowed, after anonymization of the DNA samples, the investigation of other SNPs potentially involved in NEC development. The protocol is registered in ClinicalTrials.gov Protocol Registration System (NCT00554866). Additional approval was obtained for the present analysis. All infants with a GA ≤30 weeks and birth weight (BW) ≤1,500 g born between July 2007 and July 2012 and admitted to the level III neonatal intensive care unit of the Maastricht University Medical Center (the Netherlands, IRB number MEC-07-2-018), Hospital Universitario Materno-Infantil de Canarias (Las Palmas de Gran Canaria, Spain, IRB number CEIC- 276), Carlo Poma Hospital (Mantova, Italy, inclusion until December 2011, IRB number 21366/2007), and Ospedale Maggiore Policlinico (Milan, Italy, inclusion from January 2012, IRB number 220211b) were eligible for participation in the study. As reported in a previous study, buccal cell samples were obtained from 96 healthy term infants (25 in Maastricht, 31 in Las Palmas de Gran Canaria and 40 in Mantova) (18).
Definitions were identical to those used in our previous study (16) and are therefore literally reproduced here. Data on clinical characteristics and outcomes were obtained from the medical records. GA was determined by the last menstrual period and early ultrasounds (before 20 weeks of gestation). Small for GA was defined as BW for GA below the sex-specific 10th percentile. Chorioamnionitis was defined as every clinical suspicion of infection of the chorion, amnion, amniotic fluid, placenta, or a combination as judged by the obstetrician. Prolonged rupture of membranes was defined as rupture of membranes >24 h before delivery. Prenatal exposure to a single course of antenatal steroids was defined as two doses of betamethasone administered 24 h apart and exposure to a partial course of antenatal steroids was defined as administration of a single dose of betamethasone <24 h prior to delivery.
NEC was defined as Bell stage II disease or greater. Cases of NEC stage III were also separately analyzed. At the conclusion of the study, all cases of NEC were reviewed in a blinded fashion by a panel of 4 investigators of the study. Cases of spontaneous intestinal perforation (i.e., without pathologic evidence of NEC) were excluded from the NEC group. The control group for NEC was formed by the infants without the condition who survived until 34 weeks postmenstrual age (PMA). In another analysis, we investigated the combined outcome NEC or death before 34 weeks PMA.
Arterial hypotension was defined as the need for volume expansion or inotropic support. A diagnosis of sepsis required signs of generalized infection, a positive blood culture, and antibiotic therapy. Respiratory distress syndrome (RDS) was defined as requirement for oxygen supplementation or respiratory support due to tachypnea, grunting, nasal flaring, retractions, or cyanosis. Bronchopulmonary dysplasia (BPD) was defined as a supplemental oxygen requirement at 36 weeks PMA to maintain oxygen saturation >90% (19). Retinopathy of prematurity (ROP) was defined as stage II or higher. Persistent ductus arteriosus (PDA) was defined as a requirement for indomethacin or ibuprofen and/or surgical ligation. Intraventricular hemorrhage (IVH) was classified by using the 4-level grading system (20). Grade <2 IVHs were not included in the analysis.
Buccal cell samples for DNA testing were obtained with a sterile OmniSwab (Whatman) and collected in Eppendorf sterile PCR tubes and stored at −80°C until further analysis. The samples obtained in Spain and Italy were transported on dry ice to Maastricht where all the analyses were performed. DNA was extracted using standard methods and stored at −20°C until genotyping. Discrimination of the VEGF rs699947, the IL-18 rs1946518, and the IL-4Rα rs1801275 alleles was performed with TaqMan® SNP genotyping assays (Applied Biosystems, Foster City, CA, USA) ID C_8311602_10 (rs699947), C_2898460_10 (rs1946518), and C_2351160_20 (rs1801275), following the manufacturer's instructions. The TaqMan technique combines DNA amplification and genotype detection in a single assay (21). Probe sequences are depicted in Supplementary Table 1. Genotyping assays were performed on an ABI PRISM 7900 Sequence Detection System for allelic discrimination (Applied Biosystems).
Methods for statistical analysis were identical to those used in our previous study (16) and are therefore literally reproduced here. Categorical variables were expressed as counts or percentages and compared using the chi-square test. Continuous variables were expressed as mean (SD) if they followed a normal distribution and compared using unpaired, two-sided t-test. If not normally distributed, continuous variables were expressed as median values (interquartile range, IQR; 25th−75th percentile) and compared using the using the Mann–Whitney U-test. The Kolmogorov-Smirnov test was used to test for normal distribution of continuous data.
Differences in allelic frequencies and genotype distributions between the investigated populations, as well as Hardy–Weinberg equilibrium (HWE) for genotype distribution were assessed using a chi-square test. The Hardy–Weinberg law states that q2 + 2pq + p2 = 1, where p and q are allele frequencies in a two-allele system. Logistic regression analysis was used to compute the odds ratios (ORs) and their 95% confidence intervals (CI) for NEC and the combined outcome NEC or death before 34 weeks of PMA based on genotype after accounting for the covariates which were significantly different between the groups and are known risk factors for developing NEC. Different genetic models were used to analyze the effect of the risk allele including the general allelic (multiplicative or codominant model), dominant, recessive, and additive models. Assuming a genetic penetrance parameter γ (γ>1), a multiplicative model indicates that the risk of disease is increased γ-fold with each additional copy of the risk allele; an additive model indicates that risk of disease is increased γ-fold for the genotype with one copy of the risk allele and 2 γ-fold for the genotype with two copies of the risk allele; a common recessive model indicates that two copies of the risk allele are required for a γ-fold increase in disease risk, and a common dominant model indicates that either one or two copies of the risk allele are required for a γ-fold increase in disease risk (22). The major allele was considered as a reference and the interactions were tested in the different models by multivariable logistic regression model. All the statistical analyses were performed using IBM SPSS Statistics for Windows, Version 22.0. (IBM Corporation, Armonk, NY, USA) and conducted at the P < 0.05 level of significance.
A total number of 358 preterm infants (26 NEC cases) were genotyped for the three SNPs, but genotype of VEGF C-2578A SNP failed in 9 infants (1 from the NEC group) and genotype of IL-18 C-607A SNP failed in 1 infant without NEC. Demographic and clinical characteristics of the infants with and without NEC are shown and compared in Table 1. Mean GA and mean BW of infants with NEC were significantly lower than in infants without NEC. In addition, infants with NEC showed a higher incidence of vaginal delivery, mechanical ventilation, BPD, hypotension, IVH, ROP, and mortality. We adjusted for GA, BW, mechanical ventilation, hypotension, and death before 34 weeks PMA in the subsequent logistic regression analysis.
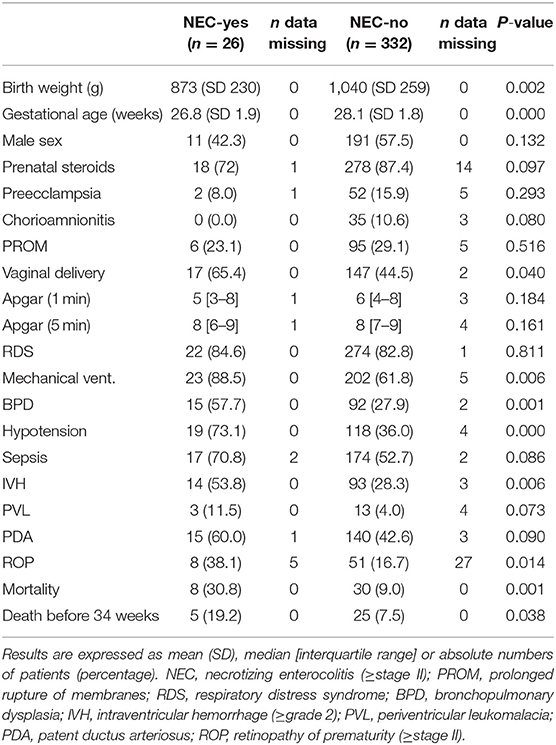
Table 1. Baseline characteristics and neonatal complications in preterm infants with and without NEC.
The demographic and clinical characteristics of the infants with and without the combined outcome NEC or death before 34 weeks PMA are shown and compared in Table 2. Mean GA, mean BW and median Apgar score at 1 and 5 min of infants with NEC or death were significantly lower than in infants without the combined outcome. In addition, infants with the combined outcome NEC or death showed a higher incidence of vaginal delivery, mechanical ventilation, hypotension, IVH, and PDA. We adjusted for GA, BW, Apgar score after at 1 and 5 min, mechanical ventilation, hypotension, and PDA in the subsequent logistic regression analysis. We did not observe a significant difference between the NEC and the control group in the rate of exposure to antenatal steroids and therefore we did not control for this exposure.
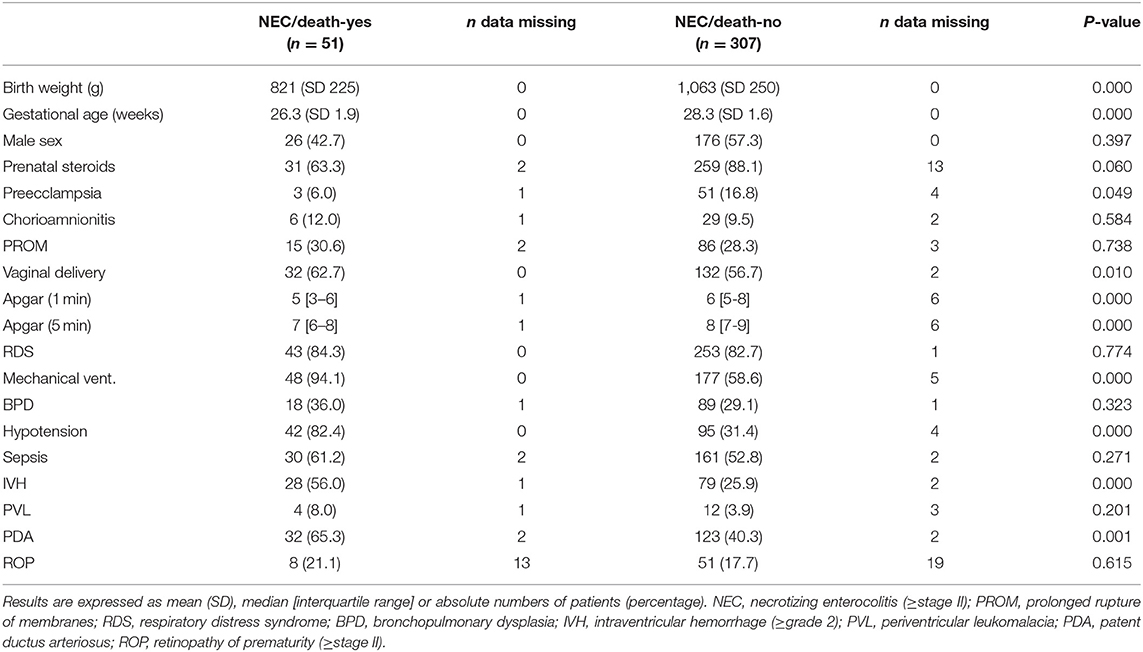
Table 2. Baseline characteristics and neonatal complications in preterm infants with and without the combined outcome NEC or death before 34 weeks of corrected gestational age.
Allele and genotype frequencies of the VEGF C-2578A, IL-18 C-607A, and IL-4Rα A-1902G polymorphisms in the total preterm population did not significantly differ from the allele and genotype frequencies observed in the population of 96 healthy term infants (Table 3) (18). The distribution of the genotypes of the VEGF C-2578A- and the IL-4Rα A-1902G polymorphisms in the preterm population and the IL-4Rα A-1902G polymorphism in the term population did not fulfill Hardy-Weinberg criteria (Table 3). The minor allele frequencies (MAFs) of the studied polymorphisms in the NEC ≥ stage II, and NEC stage III groups were not significantly different from the MAFs observed in the infants without NEC (Table 4). The MAF of the IL-4Rα A-1902G polymorphism was significantly lower (0.206 vs. 0.331, P = 0.01) in the group of infants with the combined outcome NEC or death before 34 weeks PMA than in the infants without the outcome (Table 4). The MAFs of the VEGF C-2578A, and IL-18 C-607A SNPS were not significantly different in the group of infants with the combined outcome NEC or death before 34 weeks PMA than in the infants without the outcome (Table 4). The distribution of the genotypes of the VEGF C-2578A- and the IL-4Rα A-1902G polymorphisms in the population of preterm infants without NEC or without the combined outcome NEC/death did not fulfill Hardy-Weinberg criteria (Table 4).
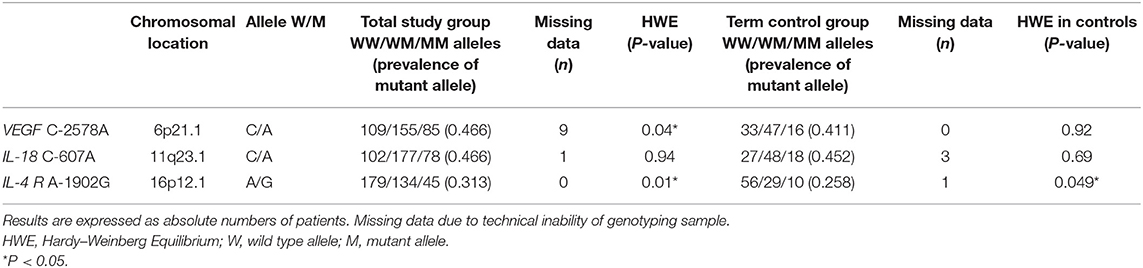
Table 3. Genotype characteristics of the VEGF C-2578A, IL-18 C-607A, and IL-4 receptor α-chain A-1902G polymorphism in total preterm study group (n = 358) and term control group (n = 96).
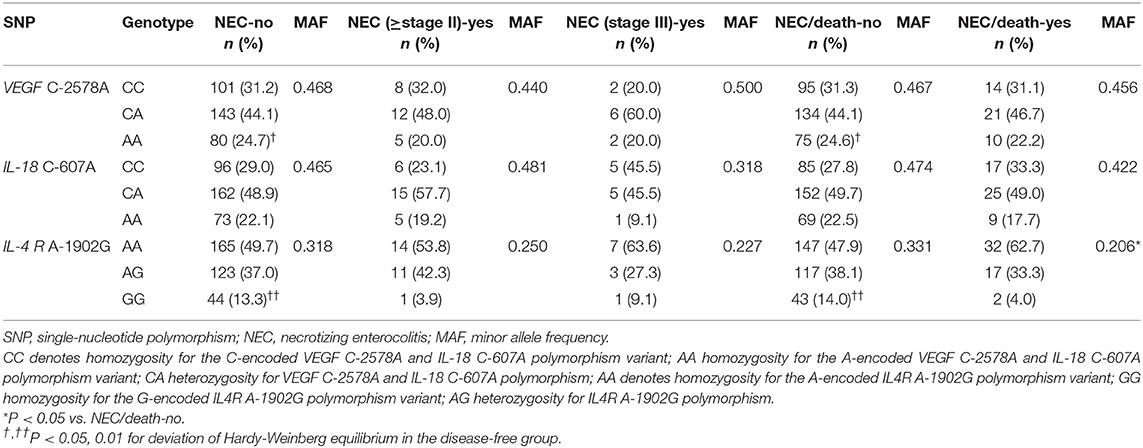
Table 4. Genotype distribution and minor allele frequency of the VEGF C-2578A, IL-18 C-607A, and IL-4 R A-1902G polymorphisms for NEC ≥stage II, NEC stage III and the combined outcome NEC or death before 34 weeks of corrected gestational age.
We further analyzed the effect of the VEGF C-2578A-, IL-18 C-607A- and IL-4Rα A-1902G polymorphism on the occurrence of NEC and NEC or death under different genetic models. Logistic regression analysis could not detect any significant association between the studied polymorphisms and NEC ≥ stage II (Table 5), or NEC stage III (Table 6) in any of the genetic models. In contrast, the co-dominant, dominant, recessive, and additive model showed a negative significant association of the G-allele of the IL-4Rα A-1902G polymorphism with the combined outcome NEC or death before 34 weeks of corrected gestational age (Table 7).
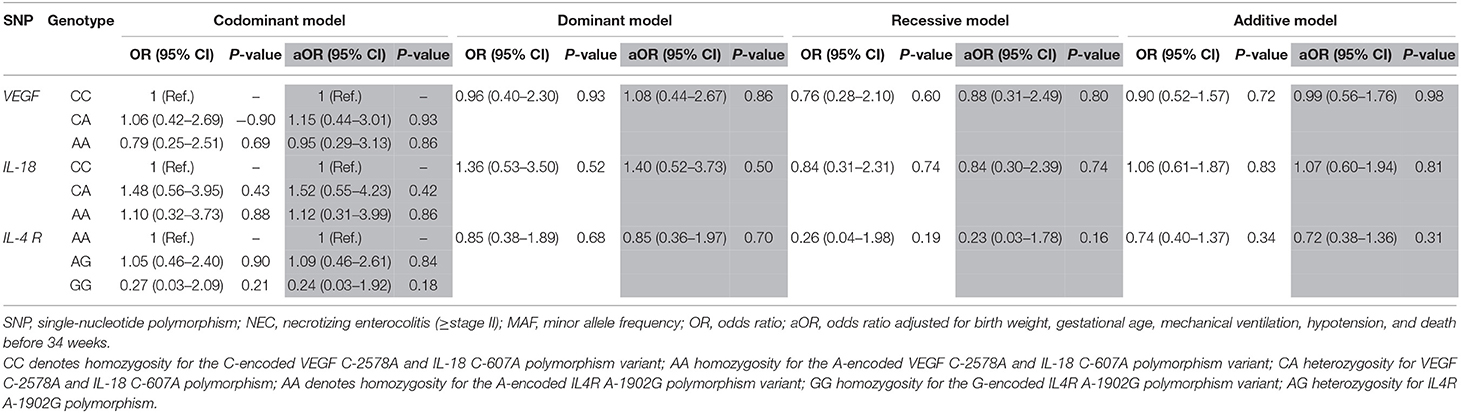
Table 5. Effects of VEGF C-2578A, IL-18 C-607A, and IL-4 R A-1902G polymorphisms on the risk of NEC (≥ stage II) under different genetic models.
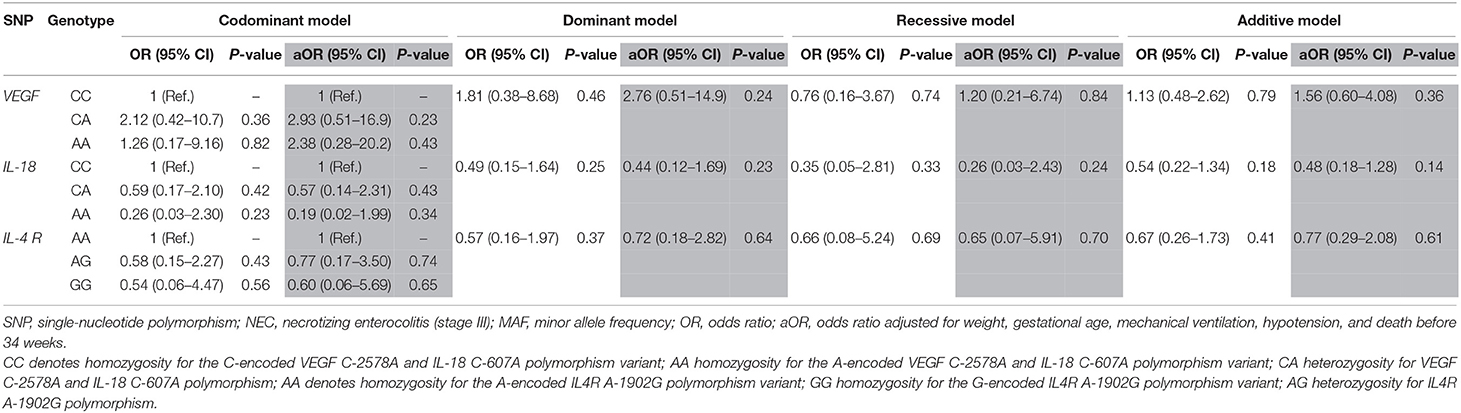
Table 6. Effects of VEGF C-2578A, IL-18 C-607A, and IL-4 R A-1902G polymorphisms on the risk of NEC stage III under different genetic models.
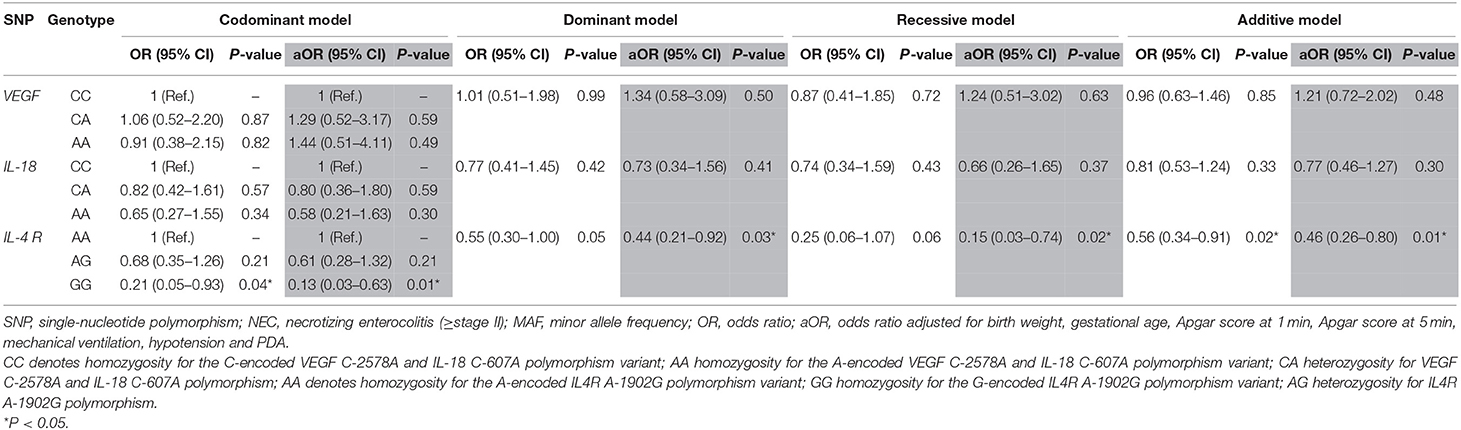
Table 7. Effects of VEGF C-2578A, IL-18 C-607A and IL-4 R A-1902G polymorphisms on the risk of the combined outcome NEC or death before 34 weeks of corrected gestational age under different genetic models.
Given that NEC remains a leading cause of morbidity and mortality, identifying preterm infants at increased risk for developing the condition remains an important but elusive objective. Previous studies suggested an association between the risk of NEC and the SNPs VEGF C-2578A, IL-18 C-607A (14), and IL-4Rα A-1902G (15). In the present cohort we could not confirm the association between the VEGF C-2578A and IL-18 C-607A SNPs and the risk of NEC or the combined outcome NEC or death before 34 weeks of corrected gestation. However, the co-dominant, dominant, recessive, and additive models showed a significant negative association of the G-allele of the IL-4Rα A-1902G polymorphism with the combined outcome NEC or death before 34 weeks of corrected gestation.
This study has some limitations that need to be considered. First, we did not investigate the functional consequences of the SNPs. Second, the distribution of the genotypes of the VEGF C-2578A- and the IL-4Rα A-1902G polymorphisms in the preterm control population and the IL-4Rα A-1902G polymorphism in the term population did not fulfill Hardy-Weinberg criteria. Theoretically, disease-free control groups from outbred populations should not deviate from HWE (23). Deviation from HWE may be related to non-random mating, population stratification, selection bias, limited sample size, or genotyping error (23). Of note, deviation from HWE in the control group may increase the chance of detecting a false-positive association, particularly when ORs did not show a strong association (23). This points to the need for caution in interpreting our findings.
VEGF is an angiogenic protein that couples hypoxia sensing to angiogenesis and is necessary for the development and maintenance of capillary networks (9). It is suggested that VEGF-mediated alterations of the intestinal mucosal microvasculature play an important role in NEC pathogenesis (9, 13, 24, 25). In fact, intestinal VEGF protein expression is reduced in human and experimental NEC (9, 26). The VEGF gene is highly polymorphic, especially in the promoter, 5′-untranslated and 3′-untranslated regions (27). Some of these SNPs, including the C-2578A, have been related to varying VEGF protein expression and serum VEGFA levels and proposed to be involved in the pathogenesis of various adult diseases (27–30).
As mentioned in the introduction, two previous studies showed that the A allele of the VEGF C-2578A SNP increased the risk of NEC in preterm infants (12, 13). Moreover, one of the studies showed that plasma VEGFA levels were significantly lower in carriers of the A allele (13). In contrast, our study could not confirm the association between the VEGF C-2578A SNP and NEC. Differences in the inclusion criteria and the ethnic background of the studied populations may account for these different results. The study of Banyasz et al. included infants with all stages of NEC (12), whereas our study and the study of Gao et al. (13) only included infants with confirmed NEC (Bell stage II disease or greater). As highlighted by Cuna et al., a precise phenotypic definition of NEC is essential in the design of genetic studies and only confirmed cases of NEC in preterm infants should be included. The study of Gao et al. (13) involved a Chinese Han population and a simple association may not translate to a population of different ethnic backgrounds (31). An important point of consideration is that the Chinese population has a lower prevalence of the A allele of the VEGF C-2578A SNP (32–34) than the Caucasian population (28).
Excessive inflammation is a hallmark in the pathogenesis of NEC and, therefore, many investigators have examined the potential association between several SNPs of pro-and anti-inflammatory cytokine genes and NEC (3, 10). Altered IL-18 levels are present in patients with inflammatory bowel disease (35) and IL-18 deficient mice are showed decreased intestinal damage following experimental NEC (36). Alterations of IL-18 production have been associated with the C-607A SNP of the IL-18 gene (37). Heninger et al. showed in a case-control studies including 136 preterm newborns (46 NEC, 90 control) that the frequency of the AA genotype of the C-607A SNP was higher in infants with stage III NEC compared to those with stages I–II and those without NEC (14). We could not replicate their results in our cohort.
IL-4 is another cytokine with powerful anti-inflammatory actions. Th1-cell proliferation is inhibited by IL-4 and IL-4 opposes the effects of pro-inflammatory cytokines on macrophages. Isolated lamina propria mononuclear cells from inflamed intestine expressed IL-4 mRNA and secreted this cytokine in lower amounts than control cells (38, 39). The IL-4Rα A-1902G polymorphism has been shown to affect receptor signaling and the anti-inflammatory effect of IL-4 is more pronounced in peripheral blood mononuclear cells from adults carrying the G-variant of the SNP (40). Trezl et al. showed that carriers of the mutant allele of the IL-4Rα A-1902G polymorphism had a lower risk of all stages of NEC (15). In contrast, our study could not demonstrate an association between the IL-4Rα A-1902G SNP and the risk of NEC (≥ Bell stage II). Nevertheless, we found a significant negative association of the G-allele of the IL-4Rα A-1902G polymorphism with the combined outcome NEC or death before 34 weeks of corrected gestation in all genetic models. We analyzed this combined outcome because epidemiological studies indicate that the time to onset of NEC follows a bimodal distribution with a first peak around at 1 week of age and a second peak around at the end of the third week of life (41, 42). Therefore, early death is a competing outcome for NEC.
As reported by Treszl et al. (15, 38), the IL-4Rα G1902 variant does not influence IL-4 levels, but its presence is associated with enhanced transduction of IL-4 signals. This enhanced IL-4 transduction is known to shift the development of lymphocytes to a more pronounced Th2 proliferation. They speculate that the elevated number of Th2 cells in carriers of this genetic polymorphism is a protective factor against the development of NEC (15, 38). Accordingly, our data suggest that the minor G variant of the IL-4RαA-1902G SNP might protect against the combined outcome NEC/early death. However, there is still a need for further studies to determine the mechanisms of the protective role of the IL-4Rα G1902 variant in NEC.
This is one of the largest cohort studies investigating the association of SNPs involved in the homeostasis of intestinal microcirculation and inflammatory response with NEC. We observed that the IL-4Rα A-1902G genotype was associated with the risk of developing the combined outcome of NEC or death before 34 weeks PMA. Nevertheless, NEC is a condition with a complex and multifactorial pathogenesis and, therefore, an isolated genetic derangement may not be sufficient to account for the entire complexity of the disease. Many genetic variations associated to prematurity, intestinal function, microcirculatory regulation, inflammatory signaling, or immune defense could protect or increase the susceptibility of preterm infants to NEC (3, 43). The future challenge resides in identifying the haplotypes that confer increased risk for NEC and in understanding their interaction with environmental risk factors. In addition, further investigation is required to determine functional consequences of each SNP.
This article contains previously unpublished data. Data are available upon request to the authors.
The present study was performed on DNA samples collected during a previous study on carbamoyl phosphate synthetase SNPs as risk factor for NEC. The protocol of the above study was reviewed and approved by the Research Ethics Committees of the participating centers and we obtained written informed consent from the parents. The protocol is registered in ClinicalTrials.gov Protocol Registration System (NCT00554866). Additional approval was obtained for the present analysis.
RM participated in the design of the study, collection of data, analysis and interpretation of data, and drafted the first version of the manuscript. MH, GG-L, GC, and FM collected data, participated in the design of the study and the interpretation of the data, and helped to draft the manuscript. EV conceived the study, participated in the design of the study, collection of data, analysis and interpretation of data, and drafted the final version of the manuscript. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank the investigators of the department of Clinical Genetics, Maastricht University Medical Center, for providing polymorphisms analysis.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.00045/full#supplementary-material
1. Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med. (2011) 364:255–64. doi: 10.1056/NEJMra1005408
2. Neu J. Necrotizing enterocolitis: the mystery goes on. Neonatology. (2014) 106:289–95. doi: 10.1159/000365130
3. Cuna A, George L, Sampath V. Genetic predisposition to necrotizing enterocolitis in premature infants: current knowledge, challenges, and future directions. Semin Fetal Neonatal Med. (2018) 23:387–93. doi: 10.1016/j.siny.2018.08.006
4. Neu J, Pammi M. Necrotizing enterocolitis: the intestinal microbiome, metabolome and inflammatory mediators. Semin Fetal Neonatal Med. (2018) 23:400–5. doi: 10.1016/j.siny.2018.08.001
5. Mai V, Young CM, Ukhanova M, Wang X, Sun Y, Casella G, et al. Fecal microbiota in premature infants prior to necrotizing enterocolitis. PLoS ONE. (2011) 6:e20647. doi: 10.1371/journal.pone.0020647
6. Wu SF, Caplan M, Lin HC. Necrotizing enterocolitis: old problem with new hope. Pediatr Neonatol. (2012) 53:158–63. doi: 10.1016/j.pedneo.2012.04.001
7. Lim JC, Golden JM, Ford HR. Pathogenesis of neonatal necrotizing enterocolitis. Pediatr Surg Int. (2015) 31:509–18. doi: 10.1007/s00383-015-3697-9
8. Rose AT, Patel RM. A critical analysis of risk factors for necrotizing enterocolitis. Semin Fetal Neonatal Med. (2018) 23:374–9. doi: 10.1016/j.siny.2018.07.005
9. Bowker RM, Yan X, De Plaen IG. Intestinal microcirculation and necrotizing enterocolitis: the vascular endothelial growth factor system. Semin Fetal Neonatal Med. (2018) 23:411–5. doi: 10.1016/j.siny.2018.08.008
10. Cuna A, Sampath V. Genetic alterations in necrotizing enterocolitis. Semin Perinatol. (2017) 41:61–9. doi: 10.1053/j.semperi.2016.09.019
11. Bhandari V, Bizzarro MJ, Shetty A, Zhong X, Page GP, Zhang H, et al. Familial and genetic susceptibility to major neonatal morbidities in preterm twins. Pediatrics. (2006) 117:1901–6. doi: 10.1542/peds.2005-1414
12. Bányász I, Bokodi G, Vásárhelyi B, Treszl A, Derzbach L, Szabó A, et al. Genetic polymorphisms for vascular endothelial growth factor in perinatal complications. Eur Cytokine Netw. (2006) 17:266–70. doi: 10.1684/ecn.2006.0041
13. Gao X, Ma F, Hao H, Dai Y, Liu W, Xiao X, et al. Association of VEGFA polymorphisms with necrotizing enterocolitis in Chinese Han population. Pediatr Neonatol. (2018) 60:129–34. doi: 10.1016/j.pedneo.2018.07.002
14. Héninger E, Treszl A, Kocsis I, Dérfalvi B, Tulassay T, Vásárhelyi B. Genetic variants of the interleukin-18 promoter region (-607) influence the course of necrotising enterocolitis in very low birth weight neonates. Eur J Pediatr. (2002) 161:410–1. doi: 10.1007/s00431-002-0968-y
15. Treszl A, Héninger E, Kálmán A, Schuler A, Tulassay T, Vásárhelyi B. Lower prevalence of IL-4 receptor alpha-chain gene G variant in very-low-birth-weight infants with necrotizing enterocolitis. J Pediatr Surg. (2003) 38:1374–8. doi: 10.1016/S0022-3468(03)00399-3
16. Moonen RM, Cavallaro G, Huizing MJ, González-Luis GE, Mosca F, Villamor E. Association between the p.Thr1406Asn polymorphism of the carbamoyl-phosphate synthetase 1 gene and necrotizing enterocolitis: a prospective multicenter study. Sci Rep. (2016) 6:36999. doi: 10.1038/srep36999
17. Huizing MJ, Cavallaro G, Moonen RM, González-Luis GE, Mosca F, Vento M, et al. Is the C242T polymorphism of the CYBA gene linked with oxidative stress-associated complications of prematurity? Antioxid Redox Signal. (2017) 27:1432–8. doi: 10.1089/ars.2017.7042
18. Moonen RM, Reyes I, Cavallaro G, González-Luis G, Bakker JA, Villamor E. The T1405N carbamoyl phosphate synthetase polymorphism does not affect plasma arginine concentrations in preterm infants. PLoS ONE. (2010) 5:e10792. doi: 10.1371/journal.pone.0010792
19. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. (2001) 163:1723–9. doi: 10.1164/ajrccm.163.7.2011060
20. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. (1978) 92:529–34. doi: 10.1016/S0022-3476(78)80282-0
21. Koch W, Ehrenhaft A, Griesser K, Pfeufer A, Müller J, Schömig A, et al. TaqMan systems for genotyping of disease-related polymorphisms present in the gene encoding apolipoprotein E. Clin Chem Lab Med. (2002) 40:1123–31. doi: 10.1515/cclm.2002.197
22. Clarke GM, Anderson CA, Pettersson FH, Cardon LR, Morris AP, Zondervan KT. Basic statistical analysis in genetic case-control studies. Nat Protoc. (2011) 6:121–33. doi: 10.1038/nprot.2010.182
23. Salanti G, Amountza G, Ntzani EE, Ioannidis JP. Hardy-Weinberg equilibrium in genetic association studies: an empirical evaluation of reporting, deviations, and power. Eur J Hum Genet. (2005) 13:840–8. doi: 10.1038/sj.ejhg.5201410
24. Watkins DJ, Besner GE. The role of the intestinal microcirculation in necrotizing enterocolitis. Semin Pediatr Surg. (2013) 22:83–7. doi: 10.1053/j.sempedsurg.2013.01.004
25. Bowker RM, Yan X, Managlia E, Liu SXL, Marek C, Tan XD, et al. Dimethyloxalylglycine preserves the intestinal microvasculature and protects against intestinal injury in a neonatal mouse NEC model: role of VEGF signaling. Pediatr Res. (2018) 83:545–53. doi: 10.1038/pr.2017.219
26. Sabnis A, Carrasco R, Liu SX, Yan X, Managlia E, Chou PM, et al. Intestinal vascular endothelial growth factor is decreased in necrotizing enterocolitis. Neonatology. (2015) 107:191–8. doi: 10.1159/000368879
27. Langsenlehner U, Hofmann G, Renner W, Gerger A, Krenn-Pilko S, Thurner EM, et al. Association of vascular endothelial growth factor–a gene polymorphisms and haplotypes with breast cancer metastases. Acta Oncol. (2015) 54:368–76. doi: 10.3109/0284186X.2014.948056
28. Schneider BP, Radovich M, Sledge GW, Robarge JD, Li L. Association of polymorphisms of angiogenesis genes with breast 375 cancer. Breast Cancer Res Treat. (2008) 111:157–63. 29. doi: 10.1007/s10549-007-9755-9
29. Howell WM, Ali S, Rose-Zerilli MJ, Ye S. VEGF polymorphisms and severity of atherosclerosis. J Med Genet. (2005) 42:485–90. doi: 10.1136/jmg.2004.025734
30. Watson CJ, Webb NJ, Bottomley MJ, Brenchley PE. Identification of polymorphisms within the vascular endothelial growth factor (VEGF) gene: correlation with variation in VEGF protein production. Cytokine. (2000) 12:1232–5. doi: 10.1006/cyto.2000.0692
31. Hanchard NA. Genetic susceptibility and single-nucleotide polymorphisms. Semin Fetal Neonatal Med. (2005) 10:283–9. doi: 10.1016/j.siny.2005.01.001
32. Fan X, Wu Q, Li Y, Hao Y, Ning N, Kang Z, et al. Association of polymorphisms in the vascular endothelial growth factor gene and its serum levels with diabetic retinopathy in Chinese patients with type 2 diabetes: a cross-sectional study. Chin Med J. (2014) 127:651–7. doi: 10.3760/cma.j.issn.0366-6999.20132656
33. Lin TH, Su HM, Wang CL, Voon WC, Shin SJ, Lai WT, et al. Vascular endothelial growth factor polymorphisms and extent of coronary atherosclerosis in Chinese population with advanced coronary artery disease. Am J Hypertens. (2010) 23:960–6. doi: 10.1038/ajh.2010.104
34. Li Y, Liang J, Liu X, Liu H, Yin B, Xiao J, et al. Correlation of polymorphisms of the vascular endothelial growth factor gene and the risk of lung cancer in an ethnic Han group of North China. Exp Ther Med. (2012) 3:673–6. doi: 10.3892/etm.2012.453
35. Pages F, Berger A, Lebel-Binay S, Zinzindohoue F, Danel C, Piqueras B, et al. Proinflammatory and antitumor properties of interleukin-18 in the gastrointestinal tract. Immunol Lett. (2000) 75:9–14. doi: 10.1016/S0165-2478(00)00285-6
36. Halpern MD, Khailova L, Molla-Hosseini D, Arganbright K, Reynolds C, Yajima M, et al. Decreased development of necrotizing enterocolitis in IL-18-deficient mice. Am J Physiol Gastrointest Liver Physiol. (2008) 294:G20–6. doi: 10.1152/ajpgi.00168.2007
37. Giedraitis V, He B, Huang WX, Hillert J. Cloning and mutation analysis of the human IL-18 promoter: a possible role of polymorphisms in expression regulation. J Neuroimmunol. (2001) 112:146–52. doi: 10.1016/S0165-5728(00)00407-0
38. Treszl A, Tulassay T, Vasarhelyi B. Genetic basis for necrotizing enterocolitis–risk factors and their relations to genetic polymorphisms. Front Biosci. (2006) 11:570–80. doi: 10.2741/1819
39. Cho SX, Berger PJ, Nold-Petry CA, Nold MF. The immunological landscape in necrotising enterocolitis. Expert Rev Mol Med. (2016) 18:e12. doi: 10.1017/erm.2016.13
40. Hershey GK, Friedrich MF, Esswein LA, Thomas ML, Chatila TA. The association of atopy with a gain-of-function mutation in the alpha subunit of the interleukin-4 receptor. N Engl J Med. (1997) 337:1720–5. doi: 10.1056/NEJM199712113372403
41. Yee WH, Soraisham AS, Shah VS, Aziz K, Yoon W, Lee SK, et al. Incidence and timing of presentation of necrotizing enterocolitis in preterm infants. Pediatrics. (2012) 129:e298–304. doi: 10.1542/peds.2011-2022
42. Llanos AR, Moss ME, Pinzòn MC, Dye T, Sinkin RA, Kendig JW. Epidemiology of neonatal necrotising enterocolitis: a population-based study. Paediatr Perinat Epidemiol. (2002) 16:342–9. doi: 10.1046/j.1365-3016.2002.00445.x
Keywords: VEGF, IL-18, IL-4 receptor α-chain, polymorphisms, necrotizing enterocolitis, preterm
Citation: Moonen RM, Huizing MJ, González-Luis GE, Cavallaro G, Mosca F and Villamor E (2020) Risk of Necrotizing Enterocolitis Associated With the Single Nucleotide Polymorphisms VEGF C-2578A, IL-18 C-607A, and IL-4 Receptor α-Chain A-1902G: A Validation Study in a Prospective Multicenter Cohort. Front. Pediatr. 8:45. doi: 10.3389/fped.2020.00045
Received: 14 April 2019; Accepted: 28 January 2020;
Published: 18 February 2020.
Edited by:
Merlin G. Butler, University of Kansas Medical Center, United StatesReviewed by:
Asma Sultana, King Saud University Medical City, Saudi ArabiaCopyright © 2020 Moonen, Huizing, González-Luis, Cavallaro, Mosca and Villamor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduardo Villamor, ZS52aWxsYW1vckBtdW1jLm5s
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.