
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 26 July 2019
Sec. Neonatology
Volume 7 - 2019 | https://doi.org/10.3389/fped.2019.00309
 Silvia Corti1
Silvia Corti1 Paola Pileri1Martina I. Mazzocco1
Paola Pileri1Martina I. Mazzocco1 Chiara Mandò1Anna F. Moscatiello1Dario Cattaneo2Stefania Cheli2Sara Baldelli2Laura Pogliani1Emilio Clementi2,3
Chiara Mandò1Anna F. Moscatiello1Dario Cattaneo2Stefania Cheli2Sara Baldelli2Laura Pogliani1Emilio Clementi2,3 Irene Cetin1*
Irene Cetin1*Background: SSRIs (Selective Serotonin Reuptake Inhibitors) are the most useful drugs to treat depression during pregnancy. Intrauterine exposure to SSRIs may increase the risk of growth restriction, preterm birth and neonatal complications. However, advantages in treating depression seem to exceed potential drug side effects in respect un-treated depression. SSRIs undergo extensive hepatic first-pass metabolism with the involvement of several cytochrome P450 (CYPs) enzymes. Genetic polymorphisms may influence the expression and activity of CYPs genes. The first aim of this study was to evaluate neonatal outcomes in depressed mothers exposed to SSRIs during pregnancy. SSRIs pharmacogenetics was also evaluated in a subset of mothers and fetuses.
Methods: In this case-control study, cases (n = 42) were Caucasian women with a diagnosis of depression and/or anxiety, treated with SSRIs for the whole pregnancy. Controls (n = 85) were Caucasian women without a psychiatric diagnosis and not exposed to SSRIs during pregnancy. Exclusion criteria for both groups were other psychotropic drugs, anti-epileptics, drug of abuse, alcohol addiction, maternal or fetal infectious diseases, fetal/neonatal chromosomal genetic abnormalities. Maternal and fetal blood samples were obtained at delivery to analyze genotype in 33 cases.
Results: The population was homogenous for demographic, anthropometric, socio-economic and obstetric variables except for smoking and mean hemoglobin values before delivery. Obstetric features were comparable. Newborns exposed to SSRIs during fetal life were significantly more likely to be Low Birth Weight (LBW) (birth weight <2,500 g) (p = 0.01), had significantly lower mean Apgar scores at 1' (p = 0.006) and at 5' (p = 0.023) and worse Apgar distribution at 1' (p = 0.017) and at 5' (p = 0.013). Fifty-six percent of newborns presented one or more symptoms consistent with poor neonatal adaptation syndrome (PNAS). Pharmacogenetic analysis at delivery did not show significant differences in the frequencies of obstetric or neonatal complications in relation to polymorphisms.
Conclusions: We found that newborns exposed to SSRIs are at increased risk of poor neonatal outcomes in terms of low birth weight, low Apgar scores and, clinically, poor neonatal adaptation syndrome. Preliminary pharmacogenetic analysis showed that the degree of CYPs alterations, that depends on polymorphisms, may influence neonatal outcomes.
Recent studies have shown that 2–9% of women in the Western world are prescribed antidepressants (AD) during pregnancy (1). Intrauterine exposure to antidepressant drugs may have adverse consequences for birth outcome and child development (2, 3). Antidepressants use during pregnancy can lead to increased risk of miscarriage, congenital cardiac malformations, preterm birth (PTB), persistent pulmonary hypertension of the newborn (PPHN), and poor neonatal adjustment syndrome (PNAS) (4, 5). Multiple studies have reported an increased risk of PTB (OR ranging from 1.5 to 2) with prenatal exposure to antidepressants (6). It has been reported a possible increased risk of delayed neurobehavioral development in children (7). Several recent systematic reviews and meta-analyses emphasize that there are minimal definitive conclusions to guide treatment (8). In this view it is important to evaluate potential neonatal risks such that pregnant women can be provided with better counseling and midwives and pediatricians alerted at delivery.
Exposure to untreated depression and stress during pregnancy may have negative consequences for birth outcome and child development (9). Suicidal ideation also can be elevated in pregnant women with depression, representing a real risk for the life of both the mother and the fetus (10, 11).
Selective serotonin reuptake inhibitors (SSRIs) are the drug of choice, for their safety profile, in terms of fewer metabolites, higher protein binding to decrease placental passage, and fewer interactions with other medications (12). Sertraline, paroxetine, fluoxetine, fluvoxamine citalopram, and escitalopram are included in this group.
Results of studies examining the effects of antidepressants exposure on birth outcomes and child development have been inconsistent, since the contribution from the underlying mood disorder and the associated behaviors (e.g., poor prenatal health behaviors, concomitant medications, smoking, substance abuse, and obesity) may be confounding variables (6).
In pregnancy there are changes in drugs absorption, distribution, metabolism, and elimination. Therefore, antidepressants dosage should be increased to maintain a therapeutic effect (13, 14). Fetal exposure to antidepressants occurs through umbilical cord blood flow, placental transport, and absorption from amniotic fluid. This is influenced by the cord-to-maternal ratio of the antidepressant level, their half-life and peak levels, genetic polymorphisms of drug metabolism enzymes and transporter proteins, and the unbound fraction of antidepressant in the fetus (15).
SSRIs undergo extensive hepatic first-pass metabolism with the involvement of several cytochrome P450 (CYPs) enzymes. Expression of CYPs genes is influenced by a combination of factors including genetic polymorphisms, drug-drug interactions, patients' age. Distinct CYPs pharmacogenetic phenotypes, derived from polyallelic mechanisms, have been associated to the dose requirement, drug efficacy and occurrence of severe toxicities (16, 17).
We recently reported preliminary observations on the contribution of individual pharmacogenetics of SSRIs on infants' outcome. We also estimated the umbilical/maternal plasma SSRI concentration ratio at delivery (18).
The primary aim of this study was to evaluate neonatal outcomes in depressed mothers exposed to SSRIs during pregnancy. We also evaluated SSRIs pharmacogenetics in a subset of mothers and fetuses.
This was a prospective, observational, and experimental case-control study. It was performed from January 2011 to May 2016 in the Unit of Obstetrics-Gynecology, Sacco Hospital, Milan in collaboration with the Units of Neonatology and Pharmacology. The Medical Ethics Committee of Sacco Hospital approved the study protocol and the consent procedure. All women gave their written informed consent for their own and on behalf of their newborns.
Forty-nine cases and 100 controls were prospectively enrolled. Cases were Caucasian women with a diagnosis of depression and/or anxiety in treatment with selective serotonin reuptake inhibitors (SSRIs) before conception. Venlafaxine was considered as an SSRI if being dosed <200. We also included in the study women taking anxiolytics such as benzodiazepines, if needed.
The control group included Caucasian women, not exposed to psychotropic medications before and during pregnancy. Two unexposed subjects per one SSRI-exposed subject were randomly selected from the delivery register of the hospital, by taking the first two deliveries immediately after each SSRI case.
The exclusion criteria were the use of other psychotropic drugs (besides SSRIs or sporadic benzodiazepines), anti-epileptic drugs, drug of abuse or alcohol addiction, maternal or fetal infectious diseases, fetal/neonatal chromosomal genetic abnormalities. Women who stopped taking medication before or during labor were excluded from the study.
Out of the 48 enrolled cases, two were lost to follow-up, two were excluded because in treatment with antipsychotics or antidepressants other than SSRI, and two had not yet delivered at the end of the study, leaving 42 cases with 42 newborns.
All cases were followed in a prospective way by our multidisciplinary team, that checked drug compliance, psychologic clinical control and maternal and fetal well-being at each visit during the whole pregnancy up to delivery.
Maternal and fetal data of the control group were collected from the registers and databases of Sacco Hospital. Forty-two cases were compared to 85 controls for neonatal outcomes.
We evaluated and compared pregnancy complications such as Gestational Diabetes, Intrauterine Growth Restriction (IUGR), Pregnancy Induced Hypertension, Cholestasis of pregnancy, Preterm Premature Rupture of Membranes (pPROM), Hyperemesis Gravidarum, Polyhydramnios, Oligohydramnios, Anhydramnios, and delivery outcomes in the two groups, including variables such as mode of delivery, urgent cesarean section, vacuum-assisted vaginal delivery, induction of labor, epidural anesthesia, meconium-stained amniotic fluid third degree.
We evaluated neonatal anthropometric characteristics such as birthweight, neonatal sex, gestational age at birth, Apgar score at 1 and 5 min, umbilical artery pH and base excess (BE) at blood gas analysis on cord blood. Neonatal complications considered in this study were Intrauterine Growth Restriction (IUGR), preterm birth, low birth weight (LBW), Small for Gestational Age (SGA), Apgar scores at 1' and 5' lower than 7, neurologic symptoms, Respiratory Distress Syndrome (RDS), Hypoglycemia, malformations, access to Neonatal Intensive Care Unit, and Poor Neonatal Adjustment Syndrome (PNAS).
SSRI's pharmacogenetics were evaluated by analyzing cases' maternal and blood samples that were collected at delivery. Fetal samples were collected from cord blood. Immediately after withdrawal, each blood sample was collected in a vial with sodium citrate and kept on ice until centrifugation. Samples were stored at −20°C for further genotyping at the centralized pharmacogenetics laboratory of the Pharmacology Unit of Sacco Hospital.
Of 42 cases, 35/42 valid samples were collected for genotyping, and 32 maternal and neonatal samples were included in the pharmacogenetic analysis focused at the time of delivery. Two mothers had some missing data (nd) relatively to genotype (Figure 1).
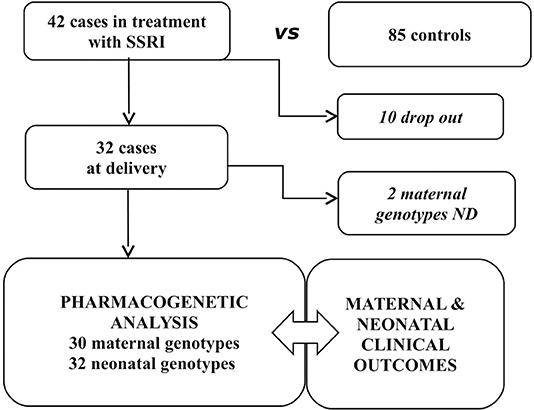
Figure 1. Study population.
Genomic DNA was isolated from peripheral blood cells using an automatic DNA extraction system (Maxwell® 16 System, Promega, Madison, WI, USA) according to the manufacturer's instructions. Polymorphisms were determined by Real-Time PCR using LightSNiP® (TIB-MolBiol, Berlin) or TaqMan® assay (Thermo Fisher Scientific, Waltham, MA, USA) according the manufacturer's instructions. We selected and evaluated the functional variants mapping in CYP2D6 (*3,*4,*5,*6, rs1080985 promoter variant, gene duplication) for paroxetine, venlafaxine and citalopram, CYP2C19 (*2, *3, *17) for sertraline and citalopram, CYP2B6*6 for sertraline, CYP3A4*22 and CYP3A5*3 for citalopram (19).
Results are reported as mean values ± standard deviation (SD).
Maternal and fetal characteristics were compared between groups using independent-samples t-test. Levene's test for equality of variances was performed to assess whether data were obtained from populations of equal/unequal variances. Chi-square analyses were performed to compare characteristics expressed as frequencies. Analyses were considered significant when p < 0.05. Tests were performed by statistical package SPSS (IBM-SPSS-Statistics 21.00, Armonk, NY).
One hundred twenty-seven pregnant women were studied 42 of whom in treatment with SSRIs (cases) and 85 without (controls). The control population showed similar demographic, anthropometric and socio-economic features, except for smoking (Table 1); higher rates of smoking among depressed women compared to women without a psychiatric diagnosis were previously reported. We did not find relevant differences in major comorbidities prevalence, such as hypertension or diabetes mellitus.
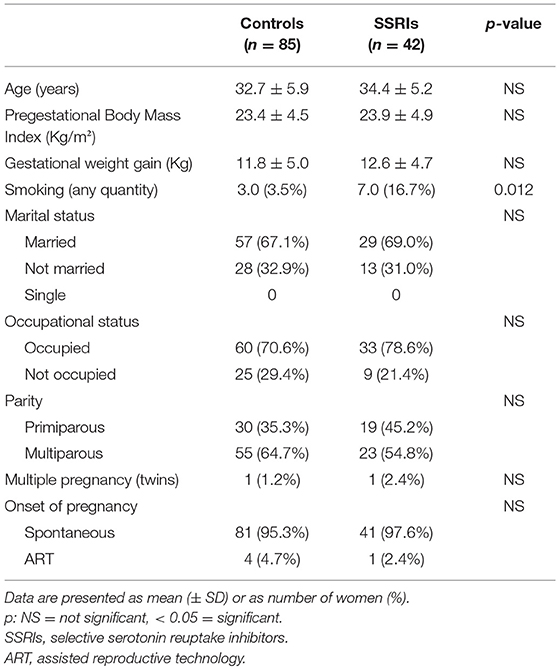
Table 1. Characteristics of the population.
In the SSRIs population depressive disorder, including both major and minor ones, accounted for 43% of the cases, anxiety disorders, including generalized anxiety, panic and obsessive-compulsive disorders for 26%, mixed anxiety-depressive disorder for 26%, and bipolar ones for 5%. Sertraline (40%) and paroxetine (31%) were the two most used molecules accounting together for more than 80%. Nineteen percent of patients had also received prescription for an anxiolytic drug belonging to the family of benzodiazepines for sporadic use.
Pregnancy complications and obstetric outcomes were similar in the two groups, as shown in Table 2 and Figure 2.
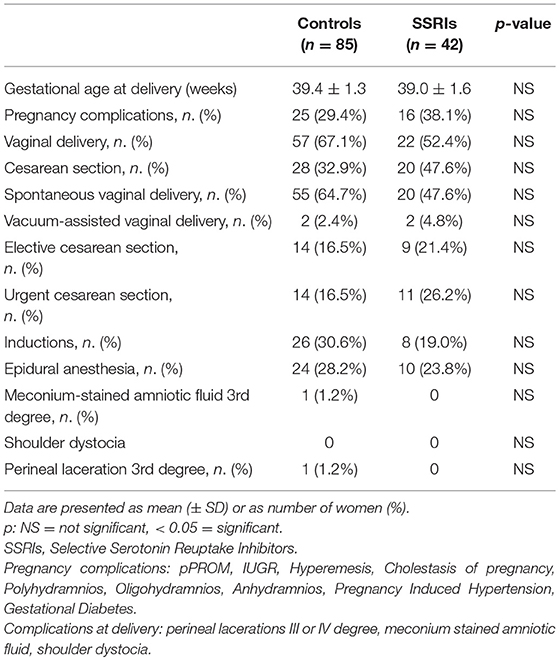
Table 2. Pregnancy and obstetric outcomes.
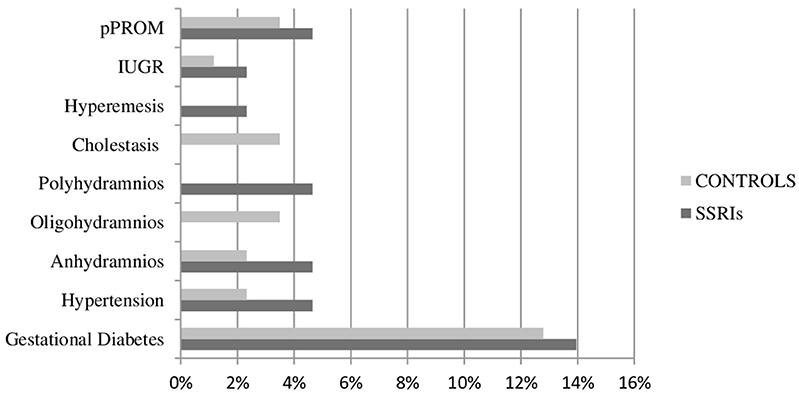
Figure 2. Pregnancy complications in the study population. Data are presented as percentage of women (%) on the population. SSRIs, selective serotonin reuptake inhibitors; IUGR, intrauterine growth restriction; pPROM, preterm premature rupture of membranes.
The SSRIs group presented statistically relevant higher rates of low birth weight newborns (14.3%, p = 0.01) and significantly lower Apgar scores at 1 and 5 min after delivery (p = 0.00 and p = 0.02). Higher scores were more prevalent in controls than in cases, whereas the lowest scores were registered only in cases (p = 0.01). Neonatal sex was not a discriminant factor (Table 3). Incidence of other neonatal complications in the two groups was not statistically relevant.
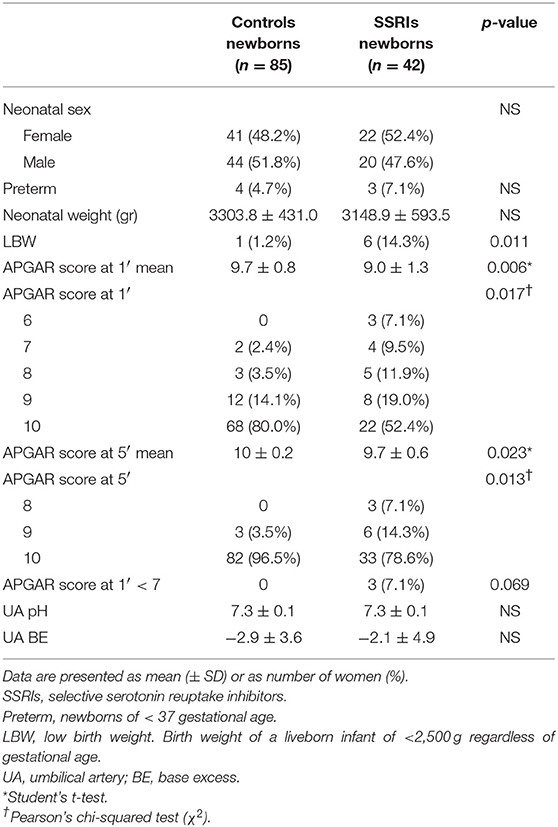
Table 3. Neonatal outcomes.
Table 4 presents neonatal outcomes in relation to the maternal and fetal genotypes. No significant difference was observed in neonatal outcomes in relation to either genotype.
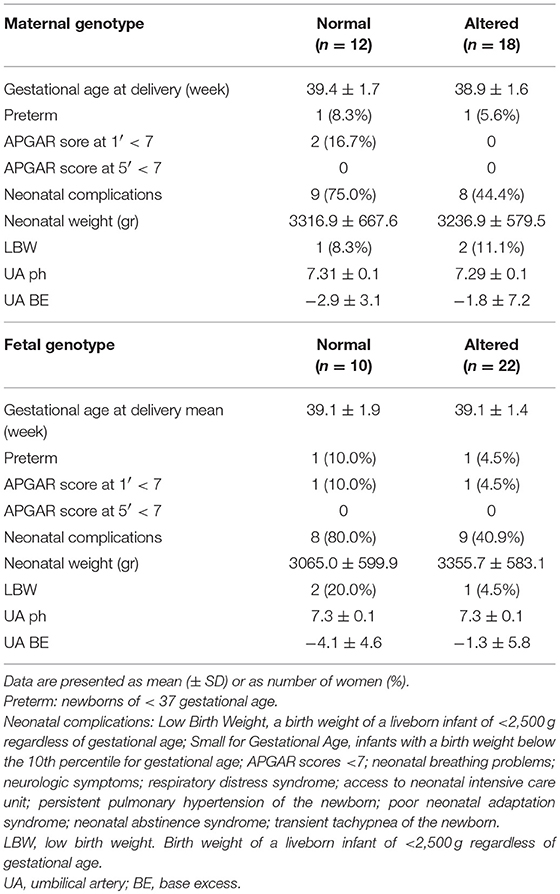
Table 4. Neonatal outcomes considering maternal and fetal genotype.
This study shows that newborns exposed to SSRIs during fetal life are at increased risk of poor neonatal outcomes, in terms of low birth weight, low Apgar scores, and poor neonatal adaptation syndrome. The case-control population showed similar demographic, anthropometric and socio-economic features, except for smoking. Higher rates of smoking among depressed women, compared to women without a psychiatric diagnosis, were reported in previous studies (20–23). It is not clear if smoking may be related with depression. Levels of dopamine are often low in people with depression, and these individuals may then use cigarettes as a way of temporarily increasing their dopamine supply, in order to increase pleasurable feelings (24).
The distribution of the psychiatric diagnosis in this study was in line with epidemiological data (25). Depressive disorders accounted for 43% of the diagnosis, followed by anxiety disorders (26%) and mixed anxiety-depressive disorder (26%). Only 5% of patients had a bipolar diagnosis. Also the use of drugs was in line with epidemiological data with sertraline as the most frequent drug (26). This is because of its short half-life and consequent easier use and safer profile in pregnancy.
Neonatal sex was not a discriminant factor nor a bias for the results. Low birth weight newborns were significantly more frequent in the SSRIs group compared to the control (14.3 vs. 1.2%). These findings are in line with previous studies, reporting a significant association between antidepressant use in pregnancy and LBW and PTB (5, 27–29). Both PTB and LBW can also be a consequence of the underlying psychiatric disorder (4, 7, 20–22, 30). However, most studies used prescription and pharmacy dispensation data to classify exposed and not exposed, but the adherence to the prescribed treatment was unknown (30). Moreover, most studied retrospective data from national registers (20, 21, 30) and others did not consider the degree of the underlying psychiatric disorder (30). These limitations are not present in this study.
Smoking may be a confounder of this result, since it can cause LBW (31, 32) and in this study smoking rates were relevantly different between groups.
In this study, Apgar scores at 1 and 5 min after delivery were significantly lower in the SSRIs group. Besides averages, differences in APGAR score distribution were more significant: higher scores were more prevalent in controls than in cases, whereas the lowest scores were registered only in cases (p = 0.01). Clinically, these newborns experienced symptoms related to poor neonatal adjustment syndrome (PNAS), respiratory distress syndrome (RDS) or transient tachypnea of the newborn (TTN). PNAS was clinically defined as Finnegan score ≥ 8 in three consecutive measurements in newborns with suggestive clinical presentation (i.e., jitteriness, poor muscle tone, weak cry, respiratory distress, hypoglycemia, low Apgar scores, and seizures) (33). It accounted for 56% of newborns and was the most represented adverse outcome. The most represented symptoms (47%) were the neurological ones including: tremors, irritability, hyper-hypotonus, hyperreflexia, jitteriness, restlessness. Respiratory distress requiring oxygen supplementation was present in 5 newborns, none manifested pulmonary hypertension or seizures. All these side effects were transient and resolved within a couple of months. Seven newborns required admission in the neonatal ward.
It is unclear what causes PNAS. The fact that SSRIs cross the placenta may be an underlying pathophysiologic mechanism through possible increases in serotonin concentrations in the developing fetus. Increased serotonin concentrations may in turn impact on fetal cardiovascular, respiratory and neurological development. Accumulation of the antidepressant in the neonate could lead to serotonergic toxicity. Finally, the abrupt discontinuation of neonate exposure to the antidepressant occurring at delivery may cause withdrawal signs (34).
These findings are in agreement with recent studies showing that treatment of maternal psychiatric disorders with SSRIs during pregnancy is related to higher risk of respiratory distress or neonatal maladaptation. In particular, higher risk of neonatal problems, low Apgar scores, breathing problems, access to neonatal care unit, and longer hospital staying have been reported (21, 34–41). However, some of these studies had a number of limitations in the study design and in the selection of the included population: most studies were retrospective (38) or drew data from several national registers (36); others collected data from different hospitals (36, 38) and considered a not homogenous population (38). Finally, some studies did not take into account confounding variables, as the underlying maternal psychiatric condition, potentially leading to misclassification bias (40), or maternal Body Mass Index (BMI) (36).
These limitations were not present in this study, since data were prospectively collected in one single hospital with the same procedures and the same multidisciplinary medical team. Moreover, the population of this study was homogeneous and evaluated for confounding variables, as the underlying psychiatric diagnosis and maternal BMI. These were main strengths of this study. Another point of strength of this study was that the analysis of neonatal outcomes included anthropometric and short-term clinical outcomes, and their relation with maternal and fetal pharmacogenetic variables.
Indeed, maternal and fetal genotypes of genes involved in SSRIs metabolism were evaluated in relation to neonatal outcomes. Due to little sample size, we did not find significant differences. However, as we previously reported, we observed three cases with an altered polymorphism that was associated to an altered pharmacokinetic resulting in neonatal toxicity (18). Our hypothesis is that maternal and fetal functional polymorphisms in genes involved in SSRIs metabolism could affect their pharmacokinetics—how much drug is transferred to the fetus throughout the whole pregnancy and at delivery according to umbilical/plasma ratio—resulting in different drug exposure, clinical SSRI maternal responsiveness, and neonatal adverse outcomes. Given the high number of polymorphisms involved in SSRIs metabolism, a study with a larger sample size and adequate power is needed to draw conclusions that may be relevant in clinical practice.
Several limitations do exist in this study. First, the low sample size, but, on the other hand the main strength of this study is the prospective approach. Than, the presence of major confounders such as smoking, that was a relevant variable in this case-control population. Nevertheless, it is well-known that smoking is much more prevalent in women with depressive disorders in respect to not depressed ones.
With regard to the pharmacogenetic aspect, only the major causal variants in CYPs gene were taken into account, without considering other genetic variants described to influence CYPs expression and activity. Also, the genetic variability was not explored, due to the differences in transporter-dependent SSRI reuptake efficiency. Moreover, a control group of depressed-not-treated women was not considered. In a causal discussion, we could not ascertain that the differences found were due to SSRI treatment and not to the underlying psychiatric illness. Finally, drug compliance was evaluated during obstetric and psychiatric visits every month, but real compliance could not be determined in all cases.
This study confirms and expands previous data that correlate SSRIs use during pregnancy to poor neonatal outcomes in terms of LBW, low Apgar scores and, clinically, to PNAS. However, poor neonatal outcome may also be related to untreated psychiatric diseases. Therefore, identification of infants at risk of PNAS is critical to child management since it could significantly influence neonatal outcomes.
This study was carried out in accordance with the recommendations of the Medical Ethics Committee of Sacco Hospital, Milan, Italy, with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Medical Ethics Committee of Sacco Hospital, Milan, Italy.
SCo and MM: patients' enrollment and follow up, maternal data and specimen collection, maternal and neonatal data analysis and interpretation, manuscript draft elaboration. PP: maternal and fetal data analysis and interpretation, manuscript revision. CM: statistical data analysis and interpretation. AM: neonatal data collection, evaluation, and interpretation. DC, SCh, and SB: genotyping. LP: neonatal data evaluation and interpretation, manuscript revision, and approval of final version. EC: manuscript revision and approval of final version. IC: study conception and design, manuscript revision, and approval of final version.
This work has been financially supported by grants from Fondazione Giorgio Pardi, by ASM (Associazione Italiana per lo Studio delle Malformazioni).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Results of this study were partially presented at the 19th National Congress of the Italian Society of Perinatal Medicine (Società Italiana di Medicina Perinatale, SIMP), in Naples (Italy), January 19-21, 2017. Published in Journal of Pediatric and Neonatal Individualized Medicine 2017;6(1):e060125; doi: 10.7363/060125; www.jpnim.com; Open Access eISSN: 2281-0692. Published online: 2017 Jan 18.
Results of this study were partially presented at the SRI Society for Reproductive Investigations 64st Annual Scientific Meeting (March 15-18, Orlando, FL, USA). Published in REPRODUCTIVE SCIENCES-ISSN 1933-7191-24:suppl. 1 (2017 Mar 15), pp. 1–1.
BMI, Body Mass Index; CYP, cytochrome P; LBW, low birth weight; OR, odds ratio; PNAS, poor neonatal adaptation syndrome; PPHN, Persistent Pulmonary Hypertension of the Newborn; PTB, preterm baby; RDS, respiratory distress syndrome; SD: standard deviation; SGA, small for gestational age; SSRIs, selective serotonine inhibitors; TDM, therapeutic drug monitoring; TTN, Transient Tachypnea of the Newborn.
1. Ververs T, Kaasenbrood H, Visser G, Schobben F, de Jong-van den Berg L, Egberts T. Prevalence and patterns of antidepressant drug use during pregnancy. Eur J Clin Pharmacol. (2006) 62:863–70. doi: 10.1007/s00228-006-0177-0
2. El Marroun H, White T, Verhulst FC, Tiemeier H. Maternal use of antidepressant or anxiolytic medication during pregnancy and childhood neurodevelopmental outcomes: a systematic review. Eur Child Adolesc Psychiatry. (2014) 23:973–92. doi: 10.1007/s00787-014-0558-3
3. El Marroun H, White TJ, van der Knaap NJ, Homberg JR, Fernández G, Schoemaker NK, et al. Prenatal exposure to selective serotonin reuptake inhibitors and social responsiveness symptoms of autism: population-based study of young children. Br J Psychiatry. (2014) 205:95–102. doi: 10.1192/bjp.bp.113.127746
4. Grote NK, Bridge JA, Gavin AR, Melville JL, Iyengar S, Katon WJ. A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Arch Gen Psychiatry. (2010) 67:1012–24. doi: 10.1001/archgenpsychiatry.2010.111
5. Glover V. Maternal depression, anxiety and stress during pregnancy and child outcome; what needs to be done. Best Pract Res Clin Obstet Gynaecol. (2014) 28:25–35. doi: 10.1016/j.bpobgyn.2013.08.017
6. Yonkers KA, Blackwell KA, Glover J, Forray A. Antidepressant use in pregnant and postpartum women. Annu Rev Clin Psychol. (2014) 10:369–92. doi: 10.1146/annurev-clinpsy-032813-153626
7. Salisbury AL, O'Grady KE, Battle CL, Wisner KL, Anderson GM, Stroud LR, et al. The roles of maternal depression, serotonin reuptake inhibitor treatment, and concomitant benzodiazepine use on infant neurobehavioral functioning over the first postnatal month. Am J Psychiatry. (2016) 173:147–57. doi: 10.1176/appi.ajp.2015.14080989
8. Szegda K, Markenson G, Bertone-Johnson ER, Chasan-Taber L. Depression during pregnancy: a risk factor for adverse neonatal outcomes? A critical review of the literature. J Matern Fetal Neonatal Med. (2014) 27:960–7. doi: 10.3109/14767058.2013.845157
9. Pearlstein T. Depression during pregnancy. Best Pract Res Clin Obstetr Gynaecol. (2015) 29:754–764. doi: 10.1016/j.bpobgyn.2015.04.004
10. Mauri M, Oppo A, Borri C, PND-ReScU group. SUICIDALITY in the perinatal period: comparison of two self-report instruments. Results from PND-ReScU. Arch Womens Ment Health. (2012) 15:39–47. doi: 10.1007/s00737-011-0246-y
11. Newport DJ, Levey LC, Pennell PB, Ragan K, Stowe ZN. Suicidal ideation in pregnancy: assessment and clinical implications. Arch Womens Ment Health. (2007) 10:181–7. doi: 10.1007/s00737-007-0192-x
12. ACOG Committee on Practice Bulletins–Obstetrics. ACOG Practice Bulletin: clinical management guidelines for obstetrician-gynecologists number 92, April 2008 (replaces practice bulletin number 87, November 2007). Use of psychiatric medications during pregnancy and lactation. Obstet Gynecol. (2008) 111:1001–20. doi: 10.1097/AOG.0b013e31816fd910
13. Deligiannidis KM, Byatt N, Freeman MP. Pharmacotherapy for mood disorders in pregnancy: a review of pharmacokinetic changes and clinical recommendations for therapeutic drug monitoring. J Clin Psychopharmacol. (2014) 34:244–55. doi: 10.1097/JCP.0000000000000087
14. Westin AA, Brekke M, Molden E, Skogvoll E, Spigset O. Selective serotonin reuptake inhibitors and venlafaxine in pregnancy: changes in drug disposition. PLoS ONE. (2017) 12:e0181082. doi: 10.1371/journal.pone.0181082
15. Sit D, Perel JM, Wisniewski SR, Helsel JC, Luther JF, Wisner KL. Mother-infant antidepressant concentrations, maternal depression, and perinatal events. J Clin Psychiatry. (2011) 72:994–1001. doi: 10.4088/JCP.10m06461
16. Zanger UM, Schwab M. Cytochrome P450 enzymes in drug metabolism: regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol Ther. (2013) 138:103–41. doi: 10.1016/j.pharmthera.2012.12.007
17. Hiemke C, Baumann P, Bergemann N, Conca A, Dietmaier O, Egberts K, et al. AGNP consensus guidelines for therapeutic drug monitoring in psychiatry: update 2011. Pharmacopsychiatry. (2011) 44:195–235. doi: 10.1055/s-0031-1286287
18. Pogliani L, Falvella FS, Cattaneo D, Pileri P, Moscatiello AF, Cheli S, et al. Pharmacokinetics and pharmacogenetics of selective serotonin reuptake inhibitors during pregnancy: an observational study. Ther Drug Monit. (2017) 39:197–201. doi: 10.1097/FTD.0000000000000370
19. Baldelli S, Fucile S, Cattaneo D, Clementi E. Development of a LC-MS/MS method for therapeutic drug monitoring of antidepressants and antipsychotics in human plasma. Ther Drug Monit. (2011) 33:528.
20. Grigoriadis S, VonderPorten EH, Mamisashvili L, Roerecke M, Rehm J, Dennis CL, et al. Antidepressant exposure during pregnancy and congenital malformations: is there an association? A systematic review and meta-analysis of the best evidence. J Clin Psychiatry. (2013) 74:e293–308. doi: 10.4088/JCP.12r07966
21. Grigoriadis S, VonderPorten EH, Mamisashvili L, Eady A, Tomlinson G, Dennis CL, et al. The effect of prenatal antidepressant exposure on neonatal adaptation: a systematic review and meta-analysis. J Clin Psychiatry. (2013) 74:e309–20. doi: 10.4088/JCP.12r07967
22. Grigoriadis S, VonderPorten EH, Mamisashvili L, Tomlinson G, Dennis CL, Koren G, et al. The impact of maternal depression during pregnancy on perinatal outcomes: a systematic review and meta-analysis. J Clin Psychiatry. (2013) 74:e321–41. doi: 10.4088/JCP.12r07968
23. Skurtveit S, Selmer R, Roth C, Hernandez-Diaz S, Handal M. Prenatal exposure to antidepressants and language competence at age three: results from a large population-based pregnancy cohort in Norway. BJOG. (2014) 121:1621–31. doi: 10.1111/1471-0528.12821
25. RCOG. Prevention and Management of Postpartum Haemorrhage (Green-top No. 52). London: RCOG (2016). Available online at: https://obgyn.onlinelibrary.wiley.com/doi/epdf/10.1111/1471-0528.14178
26. Sanchez SE, Puente GC, Atentico G, Qiu C, Yanez D, Gelaye B, et al. Risk of spontaneous preterm birth in relation to maternal depressive, anxiety and stress symptoms. J Reprod Med. (2013) 58:25–33.
27. Huang H, Coleman S, Bridge JA, Yonkers K, Katon W. A meta-analysis of the relationship between antidepressant use in pregnancy and the risk of preterm birth and low birth weight. Gen Hosp Psychiatry. (2014)36:13–8. doi: 10.1016/j.genhosppsych.2013.08.002
28. Huybrechts KF, Palmsten K, Avorn J, Cohen LS, Holmes LB, Franklin JM, et al. Antidepressant use in pregnancy and the risk of cardiac defects. New Engl J Med. (2014) 370:2397–407. doi: 10.1056/NEJMoa1312828
29. Huybrechts KF, Sanghani RS, Avorn J, Urato AC. Preterm birth and antidepressant medication use during pregnancy: a systematic review and meta-analysis. PLoS ONE. (2014) 9:e92778. doi: 10.1371/journal.pone.0092778
30. Viktorin A, Lichtenstein P, Lundholm C, Almqvist C, D'Onofrio BM, Larsson H, et al. Selective serotonin re-uptake inhibitor use during pregnancy: association with offspring birth size and gestational age. Int J Epidemiol. (2016) 45:170–7. doi: 10.1093/ije/dyv351
31. Inoue S, Naruse H, Yorifuji T, Kato T, Murakoshi T, Doi H, Subramanian SV. Impact of maternal and paternal smoking on birth outcomes. J Public Health. (2017) 39:1–10. doi: 10.1093/pubmed/fdw050
32. Chiolero A, Bovet P, Paccaud F. Association between maternal smoking and low birth weight in Switzerland: the EDEN study. Swiss Med Wkly. (2005) 135:525–30.
33. Koren G, Finkelstein Y, Matsui D, Berkovich M. Diagnosis and management of poor neonatal adaptation syndrome in newborns exposed in utero to selective seretonin/norepinephrine reuptake inhibitors. J Obstet Gynaecol Can. (2009) 31:348–350. doi: 10.1016/S1701-2163(16)34157-3
34. Moses-Kolko EL, Bogen D, Perel J, Bregar A, Uhl K, Levin B, et al. Neonatal signs after late in utero exposure to serotonin reuptake inhibitors: literature review and implications for clinical applications. JAMA. (2005) 293:2372–83. doi: 10.1001/jama.293.19.2372
35. McDonagh M, Matthews A, Phillipi C, Romm J, Peterson K, Thakurta S, et al. Antidepressant Treatment of Depression During Pregnancy and the Postpartum Period. Evidence Report/Technology Assessment No. 216. Pacific Northwest Evidence-based Practice Center. Report No. 14-E003 (2014). doi: 10.23970/AHRQEPCERTA216
36. Malm H, Sourander A, Gissler M, Gyllenberg D, Hinkka-Yli-Salomäki S, McKeague IW, et al. Pregnancy complications following prenatal exposure to SSRIs or maternal psychiatric disorders: results from population-based national register data. Am J Psychiatry. (2015) 172:1224–32. doi: 10.1176/appi.ajp.2015.14121575
37. Byatt N, Deligiannidis KM, Freeman MP. Antidepressant use in pregnancy: a critical review focused on risks and controversies. Acta Psychiatr Scand. (2013) 127:94–114. doi: 10.1111/acps.12042
38. Wen SW, Yang Q, Garner P, Fraser W, Olatunbosun O, Nimrod C, et al. Selective serotonin reuptake inhibitors and adverse pregnancy outcomes. Am J ObstetGynecol. (2006) 194:961–6. doi: 10.1016/j.ajog.2006.02.019
39. Lattimore KA, Donn SM, Kaciroti N, Kemper AR, Neal CR Jr, Vazquez DM. Selective serotonin reuptake inhibitor (SSRI) use during pregnancy and effects on the fetus and newborn: a meta-analysis. J Perinatol. (2005) 25:595–604. doi: 10.1038/sj.jp.7211352
40. Salisbury AL, Wisner KL, Pearlstein T, Battle CL, Stroud L, Lester BM. Newborn neurobehavioral patterns are differentially related to prenatal maternal major depressive disorder and serotonin reuptake inhibitor treatment. Depress Anxiety. (2011) 28:1008–19. doi: 10.1002/da.20883
41. Oberlander TF, Papsdorf M, Brain UM, Misri S, Ross C, Grunau RE, et al. Prenatal effects of selective serotonin reuptake inhibitor antidepressants, serotonin transporter promoter genotype (SLC6A4), and maternal mood on child behavior at 3 years of age. Arch Pediatr Adolesc Med. (2010) 164:444–51. doi: 10.1001/archpediatrics.2010.51
Keywords: SSRI, pharmacogenetics, poor neonatal adaptation syndrome, newborns, pregnancy, depression
Citation: Corti S, Pileri P, Mazzocco MI, Mandò C, Moscatiello AF, Cattaneo D, Cheli S, Baldelli S, Pogliani L, Clementi E and Cetin I (2019) Neonatal Outcomes in Maternal Depression in Relation to Intrauterine Drug Exposure. Front. Pediatr. 7:309. doi: 10.3389/fped.2019.00309
Received: 06 December 2018; Accepted: 09 July 2019;
Published: 26 July 2019.
Edited by:
Alessandro Favilli, Department of Surgical and Biomedical Sciences, University of Perugia, ItalyReviewed by:
Jonathan Michael Davis, Tufts University, United StatesCopyright © 2019 Corti, Pileri, Mazzocco, Mandò, Moscatiello, Cattaneo, Cheli, Baldelli, Pogliani, Clementi and Cetin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Irene Cetin, aXJlbmUuY2V0aW5AdW5pbWkuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.