 Jaeyong Bae
Jaeyong Bae Jin-Mann S. Lin
Jin-Mann S. Lin- 1Chronic Viral Diseases Branch, Division of High-Consequence Pathogens and Pathology, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, GA, United States
- 2Department of Health Policy and Management, Rollins School of Public Health, Emory University, Atlanta, GA, United States
Background: ME/CFS is a complex and disabling illness with substantial economic burden and functional impairment comparable to heart disease and multiple sclerosis. Many patients with ME/CFS do not receive appropriate healthcare, partially due to lack of diagnostic tests, and knowledge/attitudes/beliefs about ME/CFS. This study was to assess the utility of US ambulatory healthcare data in profiling demographics, co-morbidities, and healthcare in ME/CFS.
Methods: Data came from the National Ambulatory Medical Care Survey (NAMCS) and the National Hospital Ambulatory Medical Care Survey (NHAMCS) in the U.S. Weighted analysis was performed. We examined 9.06 billion adult visits from 2000 to 2009 NAMCS/NHAMCS data. ME/CFS-related visits were identified by ICD-9-CM code, 780.71, up to tertiary diagnosis.
Results: We estimated 2.9 million (95% CI: 1.8–3.9 million) ME/CFS-related visits during 2000–2009, with no statistical evidence (p-trend = 0.31) for a decline or increase in ME/CFS-related visits. Internists, general and family practitioners combined provided 52.12% of these visits. Patients with ME/CFS-related visits were mostly in their 40 and 50 s (47.76%), female (66.07%), white (86.95%), metropolitan/urban residents (92.05%), and insured (87.26%). About 71% of ME/CFS patients had co-morbidities, including depression (35.79%), hypertension (31.14%), diabetes (20.30%), and arthritis (14.11%). As one quality indicator, physicians spent more time on ME/CFS-related visits than non-ME/CFS visits (23.62 vs. 19.38 min, p = 0.065). As additional quality indicators, the top three preventive counseling services provided to patients with ME/CFS-related visits were diet/nutrition (8.33%), exercise (8.21%), and smoking cessation (7.24%). Compared to non-ME/CFS visits, fewer ME/CFS-related visits included counseling for stress management (0.75 vs. 3.14%, p = 0.010), weight reduction (0.88 vs. 4.02%, p = 0.002), injury prevention (0.04 vs. 1.64%, p < 0.001), and family planning/contraception (0.17 vs. 1.45%, p = 0.037).
Conclusions: Visits coded with ME/CFS did not increase from 2000 to 2009. Almost three quarters of ME/CFS-related visits were made by ME/CFS patients with other co-morbid conditions, further adding to complexity in ME/CFS healthcare. While physicians spent more time with ME/CFS patients, a lower proportion of ME/CFS patients received preventive counseling for weight reduction, stress management, and injury prevention than other patients despite the complexity of ME/CFS. NAMCS/NHAMCS data are useful in evaluating co-morbidities, healthcare utilization, and quality indicators for healthcare in ME/CFS.
Background
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a multi-system illness characterized by reduced functioning associated with fatigue that is not due to ongoing exertion and not significantly improved by rest. Minimal mental or physical exertion may trigger relapse (termed post-exertional malaise). Additional core or common symptoms include unrefreshing sleep, cognitive problems, increased symptoms when standing, and pain, but patients may experience numerous other symptoms (1–4). Several different etiologies have been investigated for ME/CFS but so far the etiology cannot be fully explained (4, 5). Experts have noted that the terminology “chronic fatigue syndrome” can trivialize this illness and stigmatize persons who experience its symptoms (6). A variety of other names have been used, including myalgic encephalomyelitis (ME), ME/CFS, chronic fatigue immune dysfunction, and most recently, systemic exertion intolerance disease (4). In 2010, the Chronic Fatigue Syndrome Advisory Committee recommended use of ME/CFS across federal agencies within the Department of Health and Human Services. The term ME/CFS will be used in this paper.
Previous prevalence estimates of ME/CFS have varied from 0.007 to 8.34% (7–16). In the community-based studies (with or without clinical assessment), the prevalence of ME/CFS was estimated to be 0.007–8.34%, and in the clinical-based studies in primary care setting the prevalence was estimated to be 0.006–3.00%. The large variation in the ME/CFS prevalence estimates may be due to differences in study methodology, such as study population composition, heterogeneity of source populations, data collection procedures, limitations in case ascertainment, different case definitions, and operational application of case definition criteria. Moreover, most prior studies took place at a small number of hospitals or clinics, or used a population sample from one state (9, 11, 13, 17, 18).
The economic burden and functional impairment associated with ME/CFS is substantial and comparable to heart disease and multiple sclerosis. ME/CFS accounts for $18–51 billion of economic costs including $9–14 billion in medical costs and $9–37 billion in lost productivity annually (19–21). Patients with ME/CFS suffer from worse functional impairment compared to cancer, diabetes, heart disease, lung disease, multiple sclerosis, and rheumatoid arthritis (15, 22). Additionally, many patients with ME/CFS are found to have additional overlapping pain conditions such as fibromyalgia, multiple chemical sensitivity, and irritable bowel syndrome (23–27). Adjusting to a chronic, debilitating illness sometimes leads to other problems, including depression, stress, and anxiety. Like patients with other chronic illnesses, many patients with ME/CFS develop depression during their illness course (28, 29). ME/CFS patients with other co-morbid conditions have poor health and worse functioning status than those without co-morbid conditions. Co-morbid or co-existing conditions may also increase the frequency of healthcare utilization including office visits and laboratory tests (27, 30) and further complicate the management of ME/CFS symptoms. Many ME/CFS patients do not receive appropriate healthcare, partially due to constraints US healthcare systems face in addressing chronic illnesses but also due to healthcare providers lack of knowledge and misaligned attitudes, and beliefs concerning ME/CFS (31, 32).
In this study, we sought to use US national healthcare data from ambulatory visits to evaluate trends from 2000 to 2009 in ME/CFS. Additionally, we characterized demographics, co-morbidities, and healthcare services/quality indicators related to ME/CFS visits.
Methods
Data Sources
This analysis was based on the National Ambulatory Medical Care Survey (NAMCS) (33) and the National Hospital Ambulatory Medical Care Survey (NHAMCS) (34) from 2000 to 2009. Since 1992, both surveys have been administrated by the National Center for Health Statistics (NCHS), Centers for Disease Control and Prevention (CDC) (35–38). The NCHS Research Ethics Review Board approved the protocols for both the NAMCS and NHAMCS surveys, including a waiver of the requirement for informed consent of participating patients.
In brief, NAMCS collects healthcare data provided by non-federal office-based physicians whereas NHAMCS collects healthcare data provided by non-federal hospital outpatient departments (OPDs) and hospital emergency departments (EDs). Both surveys use multistage probability sampling procedures to allow for generating nationally representative estimates of ambulatory medical care services in the United States. The patient visit was the unit of this analysis. Between 2000 and 2009, response rates were 58.9–70.4% among physicians invited to participate in NAMCS, 68.3–91.0% among hospital OPDs, and 79.5–97.0% among EDs invited to participate in NHAMCS.
This analysis included the aggregated number of 748,464 adult visits (made by patients aged 18 years or older, 9.06 billion weighted visits) from the NAMCS and NHAMCS data during 2000–2009. This included 231,984 physician patient visits (7.49 billion weighted visits), 250,821 OPD visits (691 million weighted visits), and 265,659 ED visits (879 million weighted visits).
Measures
The US national ambulatory data includes up to three listed diagnoses (primary, secondary, and tertiary) for each visit. We classified all visits into two types: ME/CFS-related visits and non-ME/CFS-related visits. ME/CFS-related visits were identified using the International Classification of Diseases, 9th revision, Clinical Modification (ICD-9-CM) code, 780.71, up to tertiary diagnosis received in provider's diagnoses during visits. The primary outcomes of interest were: (1) co-morbidities, (2) healthcare services. We also examined the associations between types of visits and patient demographics.
Co-morbidities
In addition to the provider's diagnoses for patient visits, providers (for NAMCS and OPD only for NHAMCS) indicate the presence of 14 conditions even if the condition had been reported in the diagnosis box. The 14 conditions were arthritis, asthma, cancer, cerebrovascular disease, congestive heart failure, chronic renal failure, chronic obstructive pulmonary disease, depression, diabetes, hyperlipidemia, hypertension, ischemic heart disease, obesity, and osteoporosis. We considered these to be co-morbid conditions, and compared the percentages of ME/CFS and non-ME/CFS-related visits with these conditions.
Healthcare Services
Both NAMCS and NHAMCS surveys collected information on any service ordered or provided for patients during their visits. Our analysis included three categories of healthcare services: (1) preventive counseling/management services—asthma, diet/nutrition, exercise, family planning/contraception, growth/development, injury prevention, stress management, tobacco use/exposure, weight reduction, and other counseling, (2) diagnostic/screening services—complete blood count (CBC), glucose, glycohemoglobin (HgbA1c), lipid/cholesterol, and other blood tests, and (3) non-medication treatments—Complementary Alternative Medicine (CAM), physical therapy, psychotherapy, and other mental health counseling. We also examined the length of the patient's visit. These healthcare services have been constructed as quality indicators in other illnesses along with other illness-specific quality indicators based on the Institute of Medicine's broad criteria of clinical importance, scientific soundness, and feasibility for indicator selection (39, 40).
Other variables used in this study were: (1) patient demographics- age, sex, race/ethnicity, source of payment source including insurance type, and tobacco use (current or not), (2) vital signs—body mass index (BMI), and blood pressure (BP), and (3) physician/clinic information—geographic region (Northeast/Midwest/South/West), metropolitan statistical area (MSA or not), physician specialty (NAMCS only), clinic type (OPD only), physician practice characteristics (NAMCS only; solo practitioner physician practice characteristics employment status, ownership, office type), use of electronic medical records (EMRs), and referral status.
Statistical Analysis
Statistical analyses were performed using STATA version 12 (Stata Corporation, College Station, TX). To report national estimate, the “svy” command designed for multistage weighted probability surveys such as NAMCS and NHAMCS were utilized. The NCHS analytical guidelines establish the legitimacy of combining multiple years of data from the NAMCS and NHAMCS surveys. Comparisons of NAMCS and NHAMCS suggested limited differences in the percentage estimates of ME/CFS-related visits annually. We, therefore, combined the two surveys for subsequent analyses between ME/CFS-related and non-ME/CFS-related visits.
The Pearson correlation test was used to analyze the percentage trend of ME/CFS-related visits during 2000–2009. In addition to national estimate of ME/CFS-related visits, we examined bivariate associations of ME/CFS-related visits with the following health and healthcare outcomes: (1) co-morbidities, (2) quality of healthcare such as health education services and length of patient's visit, (3) other variables such as patient and physician/clinic information, and vital signs.
Results
Demographic Characteristics of ME/CFS-Related Visits
Table 1 shows the demographics for overall visits to physician offices, hospital outpatient departments, and emergency departments. Among 784,464 visits made by patients ≥18 years of age in the 2000–2009 NAMCS and NHAMCS datasets, we identified 130 visits (unweighted counts) indicating ICD-9-CM code, 780.71 for ME/CFS. After appropriate weighting, the estimated number of visits made by patients with ME/CFS in the United States over the 10 years period was 2.9 million [95% Confidence interval (CI): 1.8–3.9 million]. ME/CFS patient visits were mostly in the fourth and fifth decade age group (48.76%), female (66.07%), white (86.95%), metropolitan/urban residents (92.04%), and insured (87.26%). There were no statistically significant difference on the distribution of age, sex, race, residential area, and insurance between ME/CFS and non-ME/CFS related visits. Of the ME/CFS-related visits to office-based physicians, 52.12% were to general/family practitioners and internists. Obstetrics and gynecology, psychiatry, and neurology combined only accounted for <10% while all other specialties accounted for 38.13% ME/CFS patient visits. Among ME/CFS-related visits to hospital outpatient departments, general medicine clinics accounted for most of the visits (72.38%). Compared to non-ME/CFS visits, a slightly higher rate of adopting electronic health record (EHR) systems was observed in ME/CFS-related visits (35.91 vs. 42.95%).
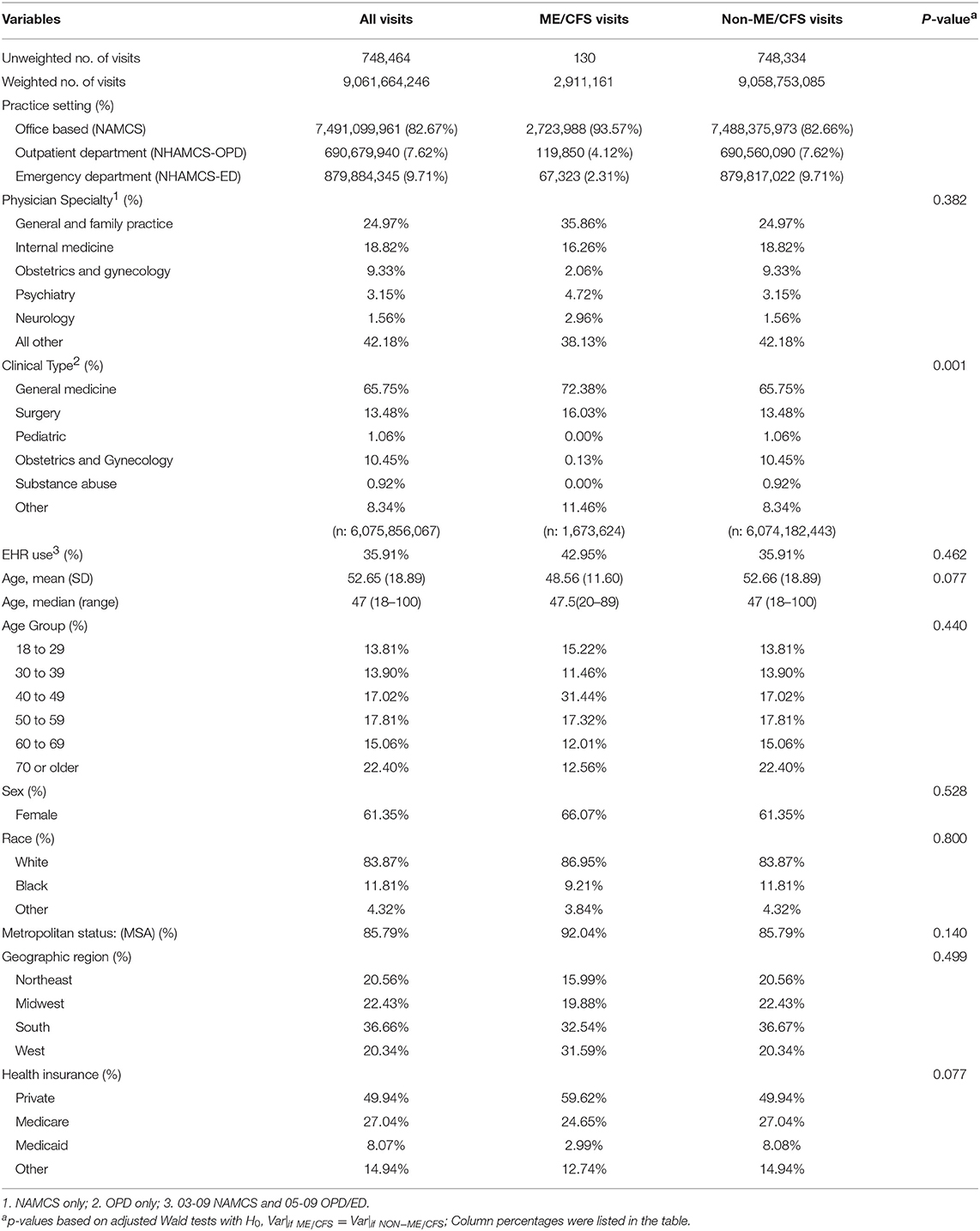
Table 1. Patient and practice demographic characteristics of ambulatory adult visits in USA, 2000–2009.
ME/CFS Patient Visit Trend, 2000–2009
Overall 0.03% of ambulatory visits by patients aged 18 years or older were made by ME/CFS patients. The percentage of ME/CFS-related visits was 0.04% for physician office visits, 0.02% for OPD visits, and 0.01% for ED visits. These proportions did not change significantly over time. The percentage of ME/CFS-related visits ranged from 0.02 to 0.08% during 2000–2009, and there was no statistical evidence for a linearly increasing trend across year (p-value for the linear trend: 0.31) (Figure 1).
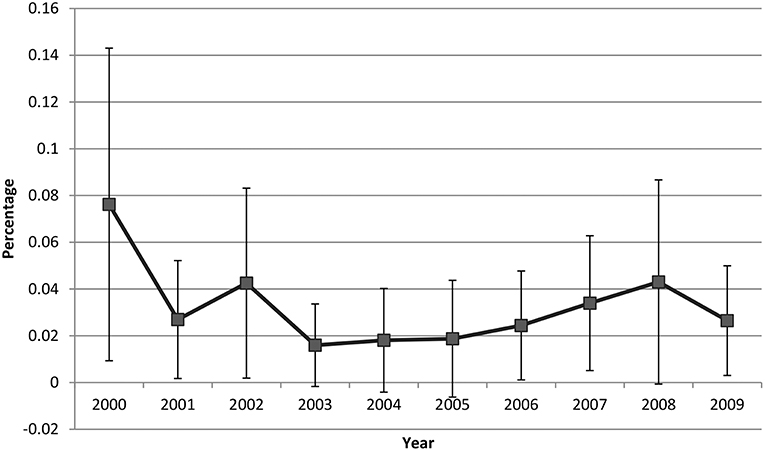
Figure 1. ME/CFS patient visit trend, 2000−2009.
Vital Signs, Continuity of Care, Providers Seen, and Visit Disposition
Table 2 summarizes the information on vital signs, continuity of care, major reason for visits, providers seen, and visit disposition of ME/CFS and non-ME/CFS patients. The vital signs of patients visiting for ME/CFS and all others did not differ significantly. The number of visits during the past 12 months made by established ME/CFS patients was greater than that by non-CFS patients (5.60 vs. 4.35, p = 0.202). Of ME/CFS-related visits, the top three reasons for visits were chronic/routine problems (60.85%), new problems (14.86%), and chronic/flare up problems (11.47%). Physicians provided care for over 90% of the patient visits for both ME/CFS-related and non-ME/CFS visits. The rates of referral to other physicians did not differ significantly between ME/CFS-related and non-ME/CFS visits.
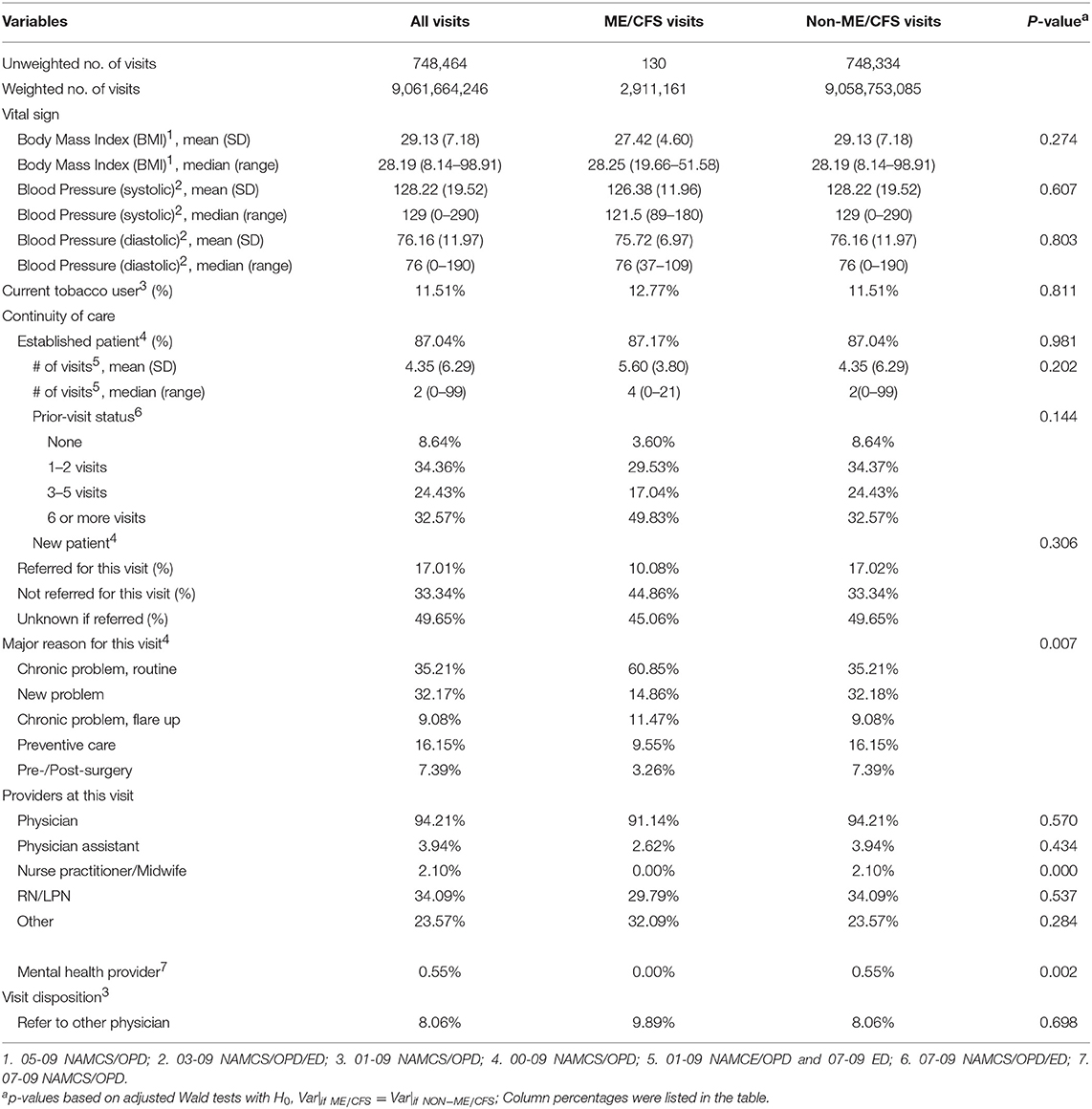
Table 2. Vital sign and continuity of care ambulatory adult visits in USA, 2000–2009.
ME/CFS and Other Chronic Conditions as Co-morbidities
Table 3 shows chronic conditions recorded at ME/CFS-related and non-ME/CFS visits. The co-morbidity rate was higher in visits by patients with ME/CFS than those by patients without ME/CFS (71.30 vs. 61.18%). The most frequent chronic conditions among ME/CFS-related visits were depression (35.79%), hypertension (31.14%), diabetes (20.30%), arthritis (14.11%), and asthma (13.79%).
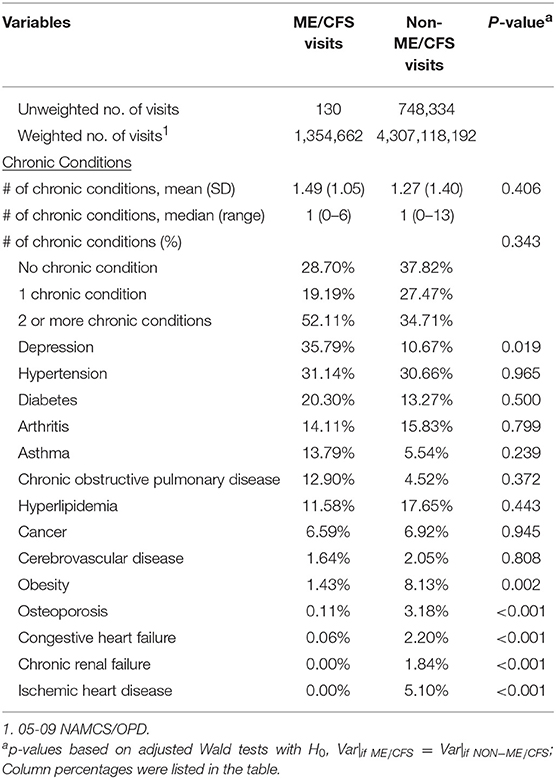
Table 3. ME/CFS and co-morbid conditions.
Healthcare Services and Quality
Table 4 compares quality of healthcare between ME/CFS-related visits and non-ME/CFS related visits. Physicians spent more time for ME/CFS-related visits than non-ME/CFS visits (23.62 vs. 19.38 min, p = 0.065). Fewer health counseling services were provided in ME/CFS-related visits than non-ME/CFS related visits (0.16 vs. 0.32 services per visit, p = 0.126). The most common counseling services provided during visits by ME/CFS patients were diet/nutrition (8.33%), exercise (8.21%), and smoking cessation (7.24%). Compared to non-ME/CFS visits, a lower proportion of ME/CFS-related visits was provided health education services on stress management (0.75 vs. 3.14%, p = 0.010), weight reduction (0.88 vs. 4.02%, p = 0.002), injury prevention (0.04 vs. 1.64%, p < 0.001), and family planning/contraception (0.17 vs. 1.45%, p = 0.037). Smoking cessation (tobacco use/expose) counseling was more prevalent in ME/CFS-related visits than non-ME/CFS visits (7.24 vs. 2.89%, p = 0.386). Contrary to health counseling services, more diagnostic/screening tests were provided in ME/CFS-related visits than non-ME/CFS visits (1.00 vs. 0.50 services per visit, p = 0.132). The most common diagnostic/screening tests provided during visits by ME/CFS patients were CBC (25.01%), glucose (19.05%), and lipids/cholesterol (12.84%), but did not reach any statistical significance level of 0.05. Non-medication treatment was more frequently provided at ME/CFS-related visits than non-ME/CFS visits (0.15 vs. 0.07 per visit, p = 0.244).
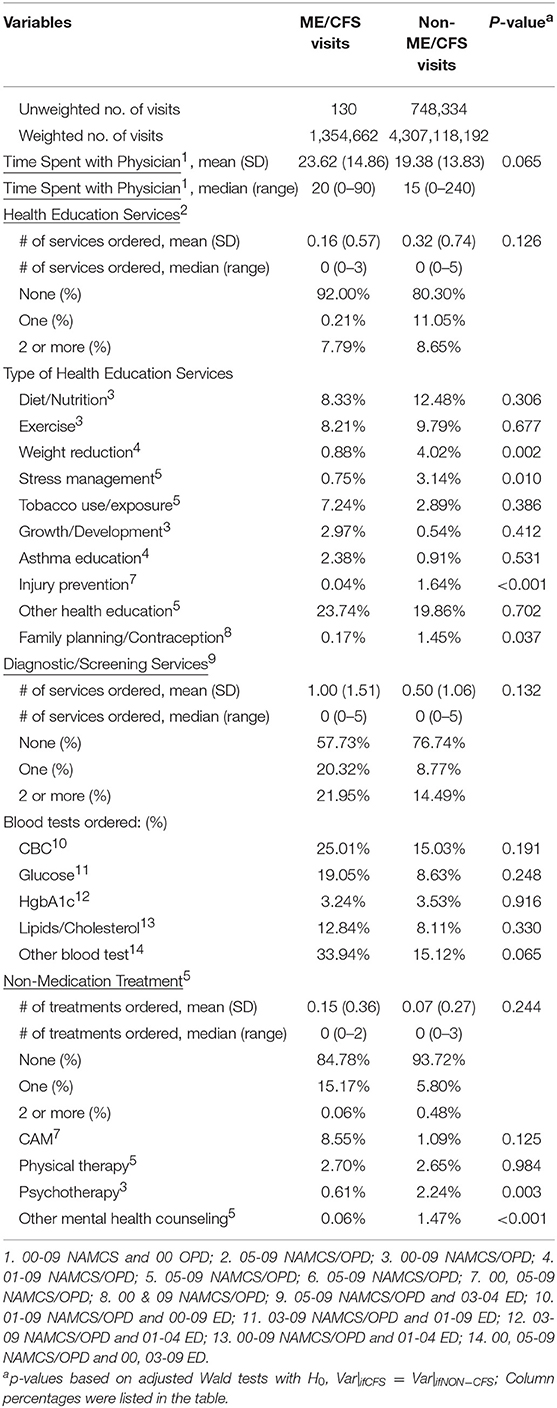
Table 4. Quality indicators of healthcare between ME/CFS-related and non-ME/CFS related visits.
Discussion
To our best knowledge, this is the first study that used a nationally representative healthcare sample of the U.S. to investigate the visit trend of diagnosing ME/CFS over years. This paper examined demographics, co-morbidities, and healthcare for visits by ME/CFS patients using a nationally representative sample of patient visits to physician offices, hospital outpatient departments, and emergency departments from 2000 to 2009. We found the overall estimated percentage of ME/CFS-related visits to be 0.03% with no statistical evidence (p-trend = 0.31) for a decline or increase from 2000 to 2009. Assuming no repeat visits by same patients, the percentage estimate of visits by ME/CFS patients would approximately reflect the prevalence estimates reported from previous studies in primary care settings.
Visits by ME/CFS patients report slightly more co-morbid conditions than visits by patients without ME/CFS. Over 70% of visits by ME/CFS patients report one or more co-morbid conditions, adding to complexity in ME/CFS healthcare. Our results on healthcare for visits by ME/CFS patients are mixed. While physicians spent more time during visits by ME/CFS patients than that by patients without ME/CFS, a lower portion of visits by ME/CFS patients was provided counseling for diet/nutrition, exercise, and weight reduction. On the other hand, a higher portion of visits by ME/CFS patients were provided diagnostic/screening tests and non-medication treatment twice as often as visits by non-ME/CFS patients.
Conclusion
In conclusion, we found that there is no increasing or decreasing trend in the percentage of ME/CFS-related visits during 2000–2009. Compared to visits by non-ME/CFS patients, visits by ME/CFS patients are provided more direct care time by physicians, more diagnostic/screening tests, and more non-medication treatments but less health counseling services. Future research should consider developing basic guidelines or recommendations for appropriate healthcare in ME/CFS-diagnosed visits such as providing weight reduction or nutrient/diet counseling for ME/CFS patients with greater BMI. When providing exercise counseling, one should be cautious of the impact of exercise. An individualized exercise or activity management plan should be emphasized to balance rest and activity to avoid post-exertional malaise flare-ups. Before starting any individualized exercise or activity management program, one should be carefully assessed and monitored periodically on their muscle strength and functional status for any physical activity.
It will also allow for identifying the potential interrupted time series that might be resulted from future ICD coding transition/change and the impact of the 2015 IOM recommendation on ME/CFS. Future investigation on this topic is warranted.
Study Limitation
Several limitations of this study should be mentioned. First, NAMCS, and NHAMCS do not include identifiers for individual patients; therefore, some patients who made visits more than once may have had their visits counted independently, which would yield inaccurate estimates of the variance. The surveys used a randomly selected sampling unit (a physician or facility) with a reporting period of the randomly assigned 1-week for NAMCS and 4-week for NHAMCS. Although our results showed that on average ME/CFS patients made about 5.6 visits per year and that translated into one visit every 2 months, it's less likely that the same patient would visit to the same selected physician or facility during the randomly assigned 1-week reporting period. Therefore, we believe that this limitation might affect our conclusion only to a small degree. Second, the NAMCS and NHAMCS included at most only three diagnosis codes and chief complaints. A greater number of listed diagnosis codes was associated with a higher likelihood of identifying ME/CFS. Thus, we may not have been able to identify some ME/CFS patients who were diagnosed as ME/CFS in 4th or later diagnosis. There is an ICD-9-CM code 780.79 for “Other malaise and fatigue” which converts approximately to ICD-10-CM G93.3 for Postviral fatigue syndrome ([Benign] myalgic encephalomyelitis) but 780.79 was not commonly documented in this data source. Therefore, in our analysis we focused on visits with ICD-9-CM code, 780.71 for chronic fatigue syndrome. One should also be aware that the ME/CFS related visits might be under-reported due to the possibility of a substantial level of omissions by healthcare providers. Finally, due to the small number of cases identified one should be cautious of generalizing the results beyond the general healthcare setting.
Ethics Statement
This is a secondary analysis using publicly available data. This analysis was based on the National Ambulatory Medical Care Survey (NAMCS) (33) and the National Hospital Ambulatory Medical Care Survey (NHAMCS) (34) from 2000 to 2009. Since 1992, both surveys have been administrated by the National Center for Health Statistics (NCHS), Centers for Disease Control and Prevention (CDC) (35–38). The NCHS Research Ethics Review Board approved the protocols for both the NAMCS and NHAMCS surveys, including a waiver of the requirement for informed consent of participating patients.
Author Contributions
JML had the original idea for the study. JML developed the analysis plan and JB performed all statistical analyses with guidance and support from JML. JB and JML drafted the paper and contributed to the interpretation and the final manuscript.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This work was conducted primarily while JB was supported in part by an appointment to the Research Participation Program at the Centers for Disease Control and Prevention administered by the Oak Ridge Institute for Science and Education through an inter-agency agreement between the U.S. Department of Energy and the Centers for Disease Control and Prevention.
References
1. Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A. The chronic fatigue syndrome: a comprehensive approach to its definition and study. Ann Intern Med. (1994) 121:953–9. doi: 10.7326/0003-4819-121-12-199412150-00009
2. Whiting P, Bagnall AM, Sowden AJ, Cornell JE, Mulrow CD, Ramírez G. Interventions for the treatment and management of chronic fatigue syndrome. JAMA. (2001) 286:1360–8. doi: 10.1001/jama.286.11.1360
3. Afari N, Buchwald D. Chronic fatigue syndrome: a review. Am J Psychiatry. (2003) 160:221–36. doi: 10.1176/appi.ajp.160.2.221
4. Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Washington, DC: The National Academies Press (2015). Available online at: http://www.nationalacademies.org/hmd/reports/2015/me-cfs.aspx
5. Rowe PC, Underhill RA, Friedman KJ, Gurwitt A, Medow MS, Schwartz MS, et al. Myalgic encephalomyelitis/chronic fatigue syndrome diagnosis and management in young people: a primer. Front Pediatr. (2017) 5:121. doi: 10.3389/fped.2017.00121
6. Komaroff AL. Myalgic encephalomyelitis/chronic fatigue syndrome: a real illness. Ann Intern Med. (2015) 162:871–2. doi: 10.7326/M15-0647
7. Price RK, North CS, Wessely S, Fraser VJ. Estimating the prevalence of chronic fatigue syndrome and associated symptoms in the community. Public Health Rep. (1992) 107:514–22.
8. Lawrie SM, Pelosi AJ. Chronic fatigue syndrome in the community. Prevalence and associations. Br J Psychiatry. (1995) 166:793–7. doi: 10.1192/bjp.166.6.793
9. Jason LA, Jordan KM, Richman JA, Rademaker AW, Huang CF, Mccready W, et al. A community-based study of prolonged fatigue and chronic fatigue. J Health Psychol. (1999) 4:9–26. doi: 10.1177/135910539900400103
10. Bates DW, Schmitt W, Buchwald D, Ware NC, Lee J, Thoyer E, et al. Prevalence of fatigue and chronic fatigue syndrome in a primary care practice. Arch Intern Med. (1993) 153:2759–65. doi: 10.1001/archinte.153.24.2759
11. Wessely S, Chalder T, Hirsch S, Wallace P, Wright D. The prevalence and morbidity of chronic fatigue and chronic fatigue syndrome: a prospective primary care study. Am J Public Health. (1997) 87:1449–55. doi: 10.2105/AJPH.87.9.1449
12. Ranjith G. Epidemiology of chronic fatigue syndrome. Occup Med. (2005) 55:13–9. doi: 10.1093/occmed/kqi012
13. Reeves W, Jones JF, Maloney E, Heim C, Hoaglin DC, Boneva RS, et al. Prevalence of chronic fatigue syndrome in metropolitan, urban, and rural Georgia. Popul Health Metr. (2007) 5:5 doi: 10.1186/1478-7954-5-5
14. Dinos S, Khoshaba B, Ashby D, White PD, Nazroo J, Wessely S, et al. A systematic review of chronic fatigue, its syndromes and ethnicity: prevalence, severity, co-morbidity and coping. Int J Epidemiol. (2009) 38:1554–70. doi: 10.1093/ije/dyp147
15. Nacul LC, Lacerda EM, Campion P, Pheby D, Drachler MDL, Leite JC, et al. The functional status and well being of people with myalgic encephalomyelitis/chronic fatigue syndrome and their carers. BMC Public Health. (2011) 11:402. doi: 10.1186/1471-2458-11-402
16. Johnston S, Brenu EW, Staines D, Marshall-Gradisnik S, Johnston S, Brenu EW, et al. The prevalence of chronic fatigue syndrome/myalgic encephalomyelitis: a meta-analysis. Clin Epidemiol. (2013) 5:105–10. doi: 10.2147/CLEP.S39876
17. Steele L, Dobbins J, Fukuda K, Reyes M, Randall B, Koppelman M, et al. The epidemiology of chronic fatigue in San Francisco. Am J Med. (1998) 105:83S−90S. doi: 10.1016/S0002-9343(98)00158-2
18. Vincent A, Brimmer DJ, Whipple MO, Jones JF, Boneva R, Lahr BD, et al. Prevalence, incidence, and classification of chronic fatigue syndrome in olmsted county, minnesota, as estimated using the rochester epidemiology project. Mayo Clin Proc. (2012) 87:1145–52. doi: 10.1016/j.mayocp.2012.08.015
19. Reynolds KJ, Vernon SD, Bouchery E, Reeves WC. The economic impact of chronic fatigue syndrome. Cost Effect Resource Allocation. (2004) 2:4. doi: 10.1186/1478-7547-2-4
20. Jason LA, Benton MC, Valentine L, Johnson A, Torres-Harding S. The economic impact of ME/CFS: individual and societal costs. Dynamic Med. (2008) 7:6. doi: 10.1186/1476-5918-7-6
21. Lin JMS, Resch SC, Brimmer DJ, Johnson A, Kennedy S, Burstein N, et al. The economic impact of chronic fatigue syndrome in Georgia: direct and indirect costs. Cost Effect Resource Allocation. (2011) 9:1. doi: 10.1186/1478-7547-9-1
22. Komaroff AL, Fagioli LR, Geiger AM, Doolittle TH, Lee J, Kornish RJ, et al. An examination of the working case definition of chronic fatigue syndrome. Am J Med. (1996) 100:56–4. doi: 10.1016/S0002-9343(96)90012-1
23. Goldenberg DL, Simms RW, Geiger A, Komaroff AL. High frequency of fibromyalgia in patients with chronic fatigue seen in a primary care practice. Arthritis Rheum. (1990) 33:381–7. doi: 10.1002/art.1780330311
24. Buchwald D, Garrity D. Comparison of patients with chronic fatigue syndrome, fibromyalgia, and multiple chemical sensitivities. Arch Intern Med. (1994) 154:2049–53. doi: 10.1001/archinte.1994.00420180053007
25. Jason LA, Taylor RR, Kennedy CL. Chronic fatigue syndrome, fibromyalgia, and multiple chemical sensitivities in a community-based sample of persons with chronic fatigue syndrome-like symptoms. Psychosom Med. (2000) 62:655–63. doi: 10.1097/00006842-200009000-00009
26. Warren JW, Langenberg P, Clauw DJ. The number of existing functional somatic syndromes (FSSs) is an important risk factor for new, different FSSs. J Psychosom Res. (2013) 74:12–7. doi: 10.1016/j.jpsychores.2012.09.002
27. Rusu C, Gee ME, Lagacé C, Parlor M. Chronic fatigue syndrome and fibromyalgia in Canada: prevalence and associations with six health status indicators. Health Promot Chronic Dis Prev Can. (2015) 35:3–11. doi: 10.24095/hpcdp.35.1.02
28. DeJean D, Giacomini M, Vanstone M, Brundisini F. Patient experiences of depression and anxiety with chronic disease: a systematic review and qualitative meta-synthesis. Ont Health Technol Assess Ser. (2013) 13:1–33.
29. Nater UM, Lin JM, Maloney EM, Jones JF, Tian H, Boneva RS, et al. Psychiatric comorbidity in persons with chronic fatigue syndrome identified from the Georgia population. Psychosom Med. (2009) 71:557–65. doi: 10.1097/PSY.0b013e31819ea179
30. Aaron LA, Herrell R, Ashton S, Belcourt M, Schmaling K, Goldberg J, et al. Comorbid clinical conditions in chronic fatigue: a co-twin control study. J Gen Intern Med. (2001) 16:24–31. doi: 10.1046/j.1525-1497.2001.03419.x
31. Lin JMS, Brimmer DJ, Boneva RS, Jones JF, Reeves WC. Barriers to healthcare utilization in fatiguing illness: a population-based study in Georgia. BMC Health Serv Res. (2009) 9:13. doi: 10.1186/1472-6963-9-13
32. Brimmer DJ, Fridinger F, Lin JMS, Reeves WC. US healthcare providers' knowledge, attitudes, beliefs, and perceptions concerning Chronic Fatigue Syndrome. BMC Family Pract. (2010) 11:28. doi: 10.1186/1471-2296-11-28
33. National Center for Health Statistics: The National Ambulatory Medical Care Survey. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. Available online at: http://www.cdc.gov/nchs/ahcd/about_ahcd.htm
34. National Center for Health Statistics: The National Hospital Ambulatory Medical Care Survey. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. Available online at: http://www.cdc.gov/nchs/ahcd/about_ahcd.htm
35. Schappert SM, Rechtsteiner EA. Ambulatory medical care utilization estimates for 2007. Vital and Health Stat. (2011) 169:1–38.
36. Hing E, Hall MJ, Ashman JJ, XU J. National hospital ambulatory medical care survey: 2007 outpatient department summary. National Health Stat Rep. (2010) 28:1–32.
37. Hsiao CJ, Cherry DK, Beatty PC, Rechtsteiner EA. National ambulatory medical care survey: 2007 summary. National Health Stat Rep. (2010) 27:1–32.
38. Niska R, Bhuiya F, Xu J. National hospital ambulatory medical care survey: 2007 emergency department summary. Natl Health Stat Rep. (2010) 386:1–31. doi: 10.1037/e587172010-001
39. Ma J, Stafford RS. Quality of US outpatient care: temporal changes and racial/ethnic disparities. Arch Intern Med. (2005) 165:1354–61. doi: 10.1001/archinte.165.12.1354
Keywords: myalgic encephalomyelitis/chronic fatigue syndrome, National Ambulatory Medical Care Survey (NAMCS), co-morbidities, healthcare utilization, quality indicators of healthcare
Citation: Bae J and Lin JM (2019) Healthcare Utilization in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): Analysis of US Ambulatory Healthcare Data, 2000–2009. Front. Pediatr. 7:185. doi: 10.3389/fped.2019.00185
Received: 05 September 2018; Accepted: 23 April 2019;
Published: 14 May 2019.
Edited by:
Kenneth Joseph Friedman, Rutgers, The State University of New Jersey, United StatesReviewed by:
Salvatore Savasta, University of Pavia, ItalyDerek Francis Henry Pheby, Buckinghamshire New University, United Kingdom
Copyright © 2019 Bae and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jin-Mann S. Lin, ZHdlM0BjZGMuZ292
†Present Address: Jaeyong Bae, Korea Institute for Health and Social Affairs, Sejong City, South Korea