 Xiaohua Ye1†
Xiaohua Ye1† Shangqin Chen
Shangqin Chen Jianghu Zhu
Jianghu Zhu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr. , 16 April 2019
Sec. Pediatric Surgery
Volume 7 - 2019 | https://doi.org/10.3389/fped.2019.00145
Background: Intussusception is a common abdominal emergency in infancy and childhood, and the recurrence rate is reported to be up to 20%. Numerous potential risk factors for recurrence have been reported, although some of them are still controversial.
Objective: The present study was conducted to identify the risk factors or predictive symptoms for recurrent intussusception in children who successfully recovered via enema reduction.
Methods: The databases of PUBMED, EMBASE, and Cochrane were searched up to August 2018. The primary outcome was the odds ratio involving the following potential risk factors: sex, the presence of blood in stool, fever, abdominal pain, right abdominal mass, pathological lead point, and vomiting.
Results: A total of 12,008 participants from 10 studies included in the abovementioned databases were enrolled in this meta-analysis. The correlation strength with each risk factor was as follows: Sex (OR = 0.87 [0.69, 1.09], P = 0.22); fever (OR = 1.85 [1.29, 2.65], P = 0.0008); blood in stool (OR = 0.93 [0.52, 1.67], P = 0.25); abdominal pain (OR = 0.82 [0.49, 1.37], P = 0.46); vomiting (OR = 0.55 [0.37, 0.80], P = 0.002); pathological lead point (PLP) (OR = 7.71 [1.96,30.29], P = 0.003); location of the mass (OR = 0.51 [0.03, 8.28], P = 0.64). Besides, children who were relatively older (over 1–2 years of age) were seen to have a higher risk of recurrence.
Conclusion: The main conclusion of this meta-analysis was that children with the presence of fever and PLP may have a higher risk of recurrence following enema reduction for intussusception. The prevalence of vomiting was found to be lower in RI (Recurrent Intussusception) patients than in the non-RI patients (control group).
Intussusception is defined as the invagination of a portion of the intestine into itself and is one of the most common causes of abdominal emergencies in infancy and childhood (1), with an incidence of 74 per 100,000 among children <1 year of age (2).
The main methods of treatment for intussusception are enema reduction and operation (3). The surgical method is usually employed as the second line treatment and rarely causes recurrence following successful restitution of the intestine, whereas enema reduction, the primary treatment, has an ~12.7% incidence of recurrence according to a recent meta-analysis (4).
Several studies have reported on numerous potential risk factors, although some of them are still controversial (5–13). Symptoms such as fever and blood in stool and the absence of vomiting have been reportedly associated with recurrent intussusception (RI) in some studies, whereas other studies either did not find any associations or presented a contrary conclusion. Pathological lead point (PLP) was also regarded as a risk factor for RI in some studies (14–18); however, the majority of cases of intussusception were idiopathic, leading to a difficulty in collecting adequate samples from RI patients to verify it with convincing research data.
As the risk factors for RI have not been clearly defined, most hospitals admit patients for 24–48 h of observation (19). However, there is a growing body of literature supporting outpatient management of patients following successful enema reduction (4, 5, 19). Therefore, this meta-analysis was conducted to identify the risk factors or predictive symptoms for RI in children who were successfully treated by enema reduction, and to recognize the children with low risk factors who can be discharged from the hospital.
This meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (20).
The RI group included children who had been treated for intussusception successfully by enema reduction and then experienced recurrence. The control group included children who had been treated for intussusception successfully by enema reduction without any recurrence.
The PUBMED, EMBASE, and Cochrane databases were searched for articles without restriction of language until January 2019. For extending the range of retrieve, we only set two keywords as the limitation in case of some unexpected missing of any qualified studies. The final strategy is “(intussusception[Title/Abstract]) AND recurren*[Title/Abstract]).” It is of note that the reference list of each of the initially included studies was checked to avoid missing any data.
The included studies met the following criteria: (1) All participants enrolled were children below 14 years of age. (2) The study groups were clearly defined based on the presence or absence of RI in the participants. (3) Adequate information could be obtained either from full-text screening or was provided by the authors. (4) Participants who received enema reduction did not expose to surgical intervention before the recurrence.
Data such as the first author's name, year of publication, region, potential risk factor assessed in the study, the number of participants, and other useful information were elicited from full-text screening and recorded in Excel tables.
Literature quality evaluation was conducted by means of the Newcastle-Ottawa Quality Assessment Scale (21). Two reviewers accomplished this process independently, and disagreements were resolved by discussion between them. The presence of publication bias was assessed by visual inspection of the funnel graph.
Odds ratio (OR) was calculated for the outcome involving sex, the presence of blood in stool, fever, abdominal pain, right abdomen mass, PLP, and vomiting. The reason for the choice of OR was the retrospective design of the meta-analysis based on published studies that varied in design, subjects' population, primary outcome measure, and research quality (22).
Forest plot was depicted to present the pooled OR value and heterogeneity was evaluated using I2 statistic. Due to the potential statistical heterogeneity, a random effect model was chosen to synthesize data instead of a fixed-effect model when assessing the role of sex, blood in stool, vomiting, PLP, and right abdominal mass in developing RI. Heterogeneity was considered significant if I2 value was over 25%. All reported test results were two-tailed and P-value < 0.05 was considered significant. Data analysis was performed with Revman 5.3.
The flow-chart of this meta-analysis is shown in Figure 1. Initially, studies from three databases (PubMed, Cochrane, and Embase) were retrieved and a total of 1,126 articles were screened based on the title and abstracts after eliminating the duplicates. Further, 24 studies were assessed for eligibility by reviewing full-text articles. Among these articles, seven studies did not compare the outcome of RI patients with a control group whose enema reduction was successful and did not show recurrence (unsuitable setting of group); two did not focus on the pediatric population alone; and five did not provide useful information. Finally, 10 studies were included in this meta-analysis.
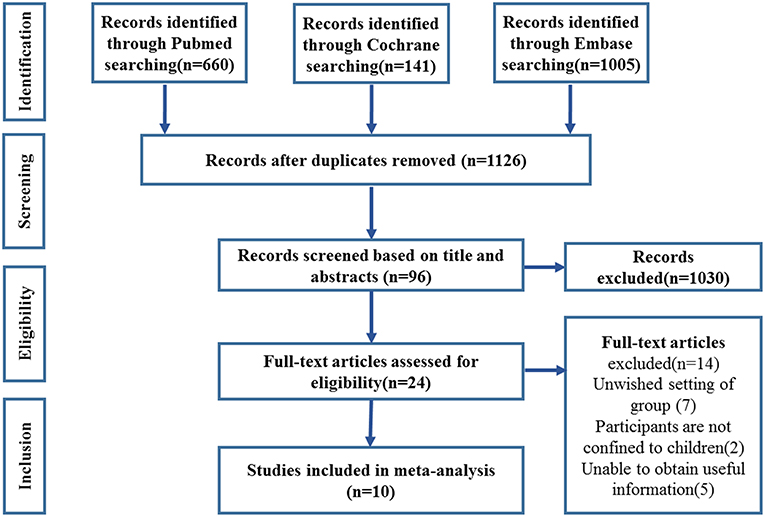
Figure 1. Study selection flow chart.
The characteristics of the nine enrolled studies are presented in Table 1. First, except for two American studies, all the others were on the Asian population, which slightly lessened the ethnic confounding factor naturally. Second, the methods for reduction used in these studies were all non-operative; one study used Altrasound-guided saline enema, three studies used barium enema, five studies chose pneumatic enema reduction, and Chen et al. (11) simply mentioned that the method they performed was non-surgical. Third, statistically, all the nine studies chose P = 0.05 as the cut-off value for the significance test. Based on that, four studies did not find any significant determinants to predict the presence of RI. Five studies provided the information about how age influences the onset of RI and two reported that the absence of vomiting happens more frequently in RI. Both Guo et al. (6) and Xie et al. (12) investigated the association between blood in stool and RI, but their conclusions were found to be inconsistent, both in the duration of symptoms and location of the mass. However, the presence of an association between PLP and RI was reported in both their studies. Besides, Vo et al. (8) reported that the presence of fever and the sex of the child were prominent factors associated with RI.
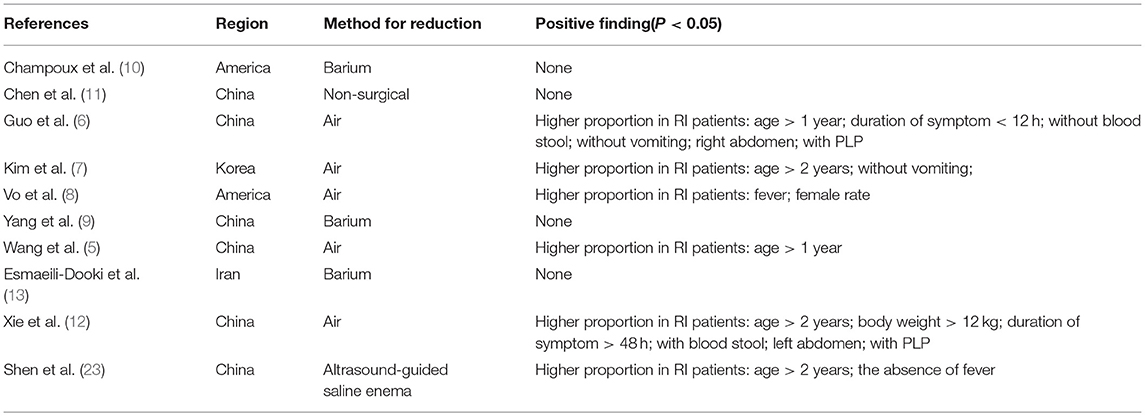
Table 1. Characteristic table of included studies.
Nine included studies were evaluated by the Newcastle-Ottawa Quality Assessment Scale, which is shown in Table 2. All the included studies had a seven-plus score, which guaranteed the eligibility for meta-analysis.
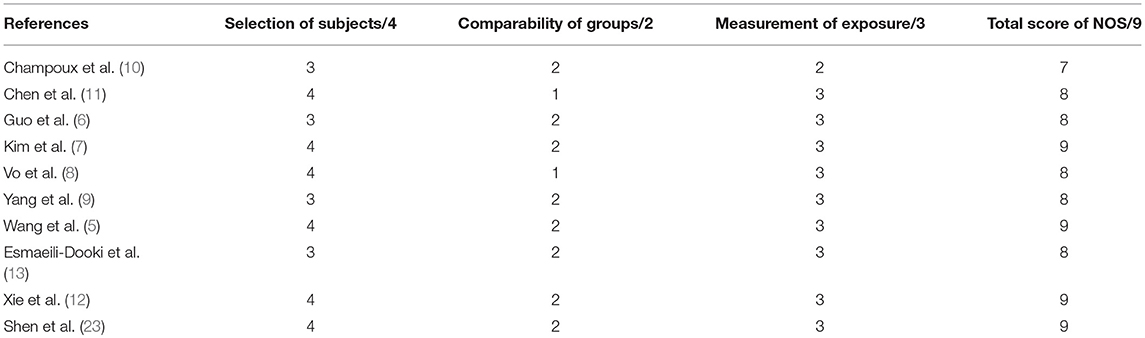
Table 2. Quality evaluation of included studies by Newcastle-Ottawa Scale.
Publication bias was assessed via funnel graphs. Based on the symmetry of the funnel graphs, it was less likely that this meta-analysis had publication bias in the models for abdominal pain, blood in stool, and sex, although it showed a high susceptibility for publication bias in the other models.
Data pertaining to the female/male ratio were extracted from seven studies and presented as the incidence rate in males. Only Vo et al. (8) reported a higher incidence of RI in female patients, while other studies did not show any differences. This meta-analysis showed that there was no association between sex and the presence of RI, statistically (OR = 0.87 [0.69, 1.09], P = 0.22) (Figure 2).
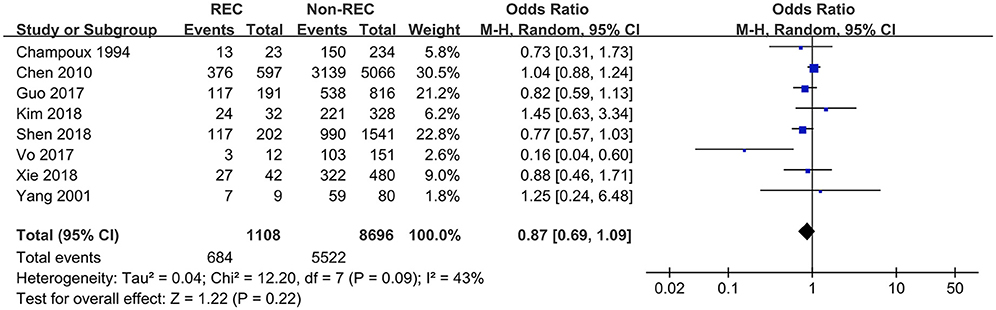
Figure 2. Forest plot showing pooled analyses of sex and RI.
Information about the presence of fever in the participants was extracted from three studies. Both Champoux et al. (10) and Vo et al. (8) chose 38°C (100.4°F) as the cut-off value for fever, which facilitated the integration of data without heterogeneity. Although Xie et al. (12) considered 37.8°C as the cut-off value for fever, the present study still pooled their data because it would not affect the outcome. Kim et al. (7) processed their data by comparing the mean value of body temperature, which hindered the statistic combination with the dichotomous variable in the other studies. Finally, this meta-analysis showed the presence of fever was a valuable risk factor to predict the RI (OR = 1.85 [1.29, 2.65], P = 0.0008) (Figure 3).
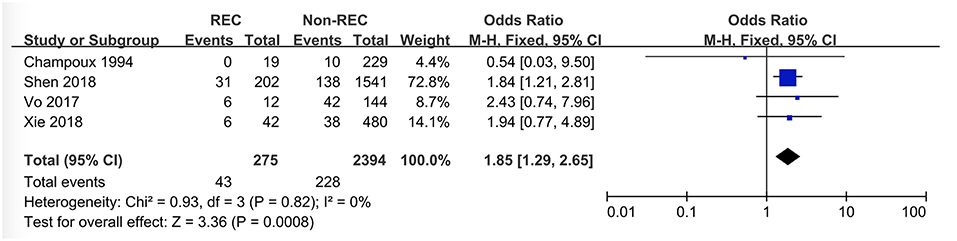
Figure 3. Forest plot showing pooled analyses of fever and RI.
Data pertaining to blood in stool were collected from six studies. Guo et al. (6) found the prevalence of blood in stool to be higher in the control group, while Xie et al. (12) reported a contrary conclusion. The other four studies did not find any relationship. This meta-analysis showed that blood in stool was not a predictive symptom of RI (OR = 0.93 [0.52, 1.67], P = 0.25) (Figure 4).
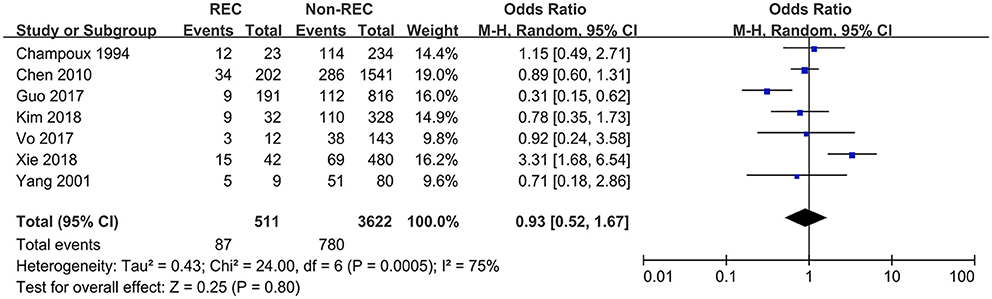
Figure 4. Forest plot showing pooled analyses of blood stool and RI.
Detailed data about the abdominal pain were extracted from four studies, and all of them did not present a positive finding. Accordingly, this meta-analysis showed that abdominal pain was not a key symptom in distinguishing RI patients from Non-RI patients (OR = 0.82 [0.49, 1.37], P = 0.46) (Figure 5).
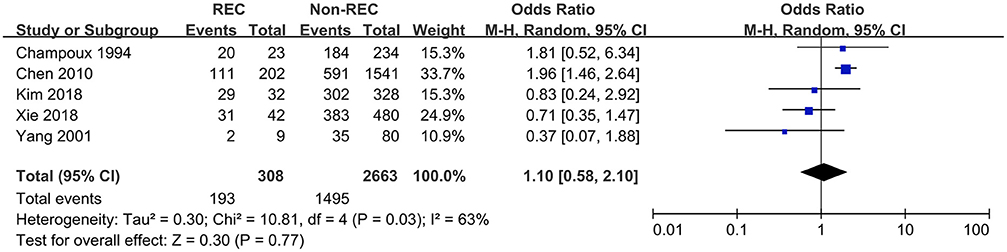
Figure 5. Forest plot showing pooled analyses of abdominal pain and RI.
Data related to the presence of vomiting in the participants were extracted from five studies. Guo et al. (6) and Kim et al. (7) reported a lower prevalence of vomiting in RI patients, while the other studies did not find any statistic association. The synthesized endpoint of this meta-analysis showed that the prevalence of vomiting was lower in RI patients compared with that in the control group (OR = 0.55 [0.37, 0.80], P = 0.002) (Figure 6).
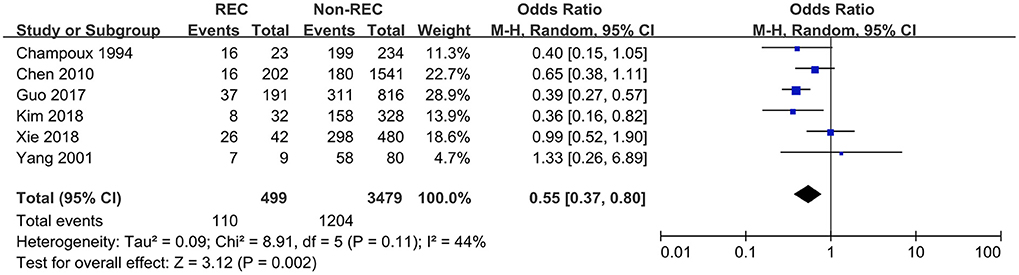
Figure 6. Forest plot showing pooled analyses of vomiting and RI.
Data regarding the presence of PLP in participants were extracted from four studies. Among these, Guo et al. (6) and Xie et al. (12) reported a higher prevalence of PLP in RI patients, while the other two did not. This meta-analysis demonstrated that PLP may influence the presence of RI in a way, but it was not statistically significant (OR = 7.71 [1.96,30.29], P = 0.003) (Figure 7).
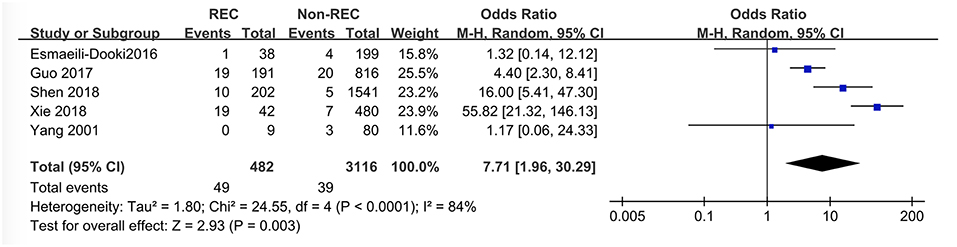
Figure 7. Forest plot showing pooled analyses of PLP and RI.
Data about location of the mass were extracted from only two studies and “right abdominal mass” was defined as “mass located in the right abdominal portion.” It is of interest that the conclusions in the two studies were contrary; Guo et al. (6) thought right abdominal mass was more likely to occur in RI patients, while Xie et al. (12) did not. This meta-analysis pooled their data and presented that there was no association between the presence of RI and location of the mass (OR = 0.51 [0.03, 8.28], P = 0.64) (Figure 8).
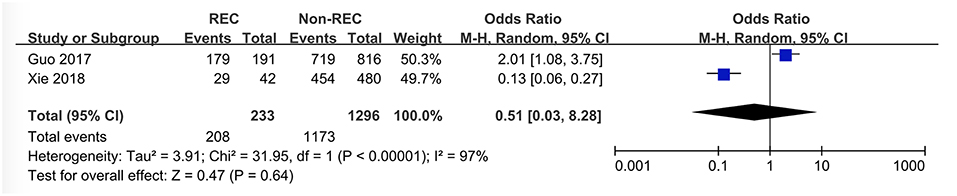
Figure 8. Forest plot showing pooled analyses of right abdominal mass and RI.
Because of the heterogeneity of the data, age in each of the studies could not be statistically pooled; thus, qualitative evaluation based on six related studies was taken. Both Guo et al. (6) and Wang et al. (5) reported that RI was more likely to occur in children aged above 1 year. Similarly, Kim et al. (7) and Xie et al. (12) thought children aged above 2 years were more susceptible to develop RI. Vo et al. (8) observed that there was no significant association between the presence of RI and atypical age, which was defined as either <6 months or >36 months.
This meta-analysis included ten studies in which 1,273 children who recovered from intussusception with a recurrence and 10,685 without recurrence were enrolled. The following potential risk factors of RI were investigated: sex, fever, blood in stool, abdominal pain, vomiting, pathological lead point (PLP), and location of the mass. The predictive risk factors of RI identified were age and the prevalence of vomiting.
Of the five studies reviewed to investigate the influence of age in RI, two studies (5, 6) reported that RI was more likely to occur in children aged above 1 year, and the other two studies (7, 12) concluded that children aged above 2 years were more susceptible to develop RI. However, one study (8) observed that there was no significant association between the presence of RI and atypical age (<6 months or >36 months), but this finding is not contradictory to that in previous studies. Children aged <6 months showed a lower prevalence of RI, while those aged above 36 months showed a definitely higher prevalence, according to the findings in the other four studies. Thus, the average prevalence of RI in the atypical age groups would likely be neutral and children who were relatively older (over 1 or 2 years of age) may have a higher risk of recurrence.
The prevalence of vomiting was found to be lower in RI patients compared with patients in the control group. The other potential risk factors, including sex, the presence of blood in stool, fever, abdominal pain, right abdominal mass, and PLP failed to show significant association with RI in this meta-analysis. However, PLP may still be one of the potential risk factors of RI as it shows a result very close to statistical point (P = 0.06).
In addition to what has been presented here, this study also provided some other information that could not be systematically reviewed. Imaging was a widely-used method in the diagnosis of intussusception. However, whether there is a role of imaging in distinguishing RI children from those without recurrence was unclear. Xie et al. (12) reported that the poor prognosis sign shown by ultrasonography could distinguish between the RI participants and the controls (P = 0.048), while Kim et al. (7) did not think that ultrasonography had any predictive function after assessing all the measurements such as thickness of bowel ≥10 mm (P = 0.07), number of entrapped lymph nodes ≥2 (P = 0.71), and size of entrapped lymph nodes ≥1 mm (P = 1.0). Besides, radiological risk factors were also proved to be irrelevant with RI in the study performed by Vo et al. (8).
Although Reijnen et al. (24) had reported that duration of symptoms >48 h was a significant predictor of failure of hydrostatic reduction, few studies stated that the duration of symptoms was associated with the recurrence of intussusception in children. In this meta-analysis, conflicting conclusions were drawn in terms of how duration of symptoms influenced the presence of RI: Guo et al. (6) stated that a higher proportion of children with RI had symptoms for <12 h, whereas Xie et al. (12) showed that more recurrences occurred with >48 h duration of symptoms. Therefore, large-scale studies are needed in the future to address this problem.
This study has some limitations: (1) While the majority of the included studies are from Asia, ethnic confounding factors still exist because of the other American studies. (2) Certain factors such as body temperature were recorded in different formats, which hinders statistical analysis. (3) The cause of RI in some patients is still unknown. Although 12,008 participants were enrolled in the study, the number of overlapped risk factors or predictive symptoms in each of the studies were too less to be analyzed statistically in a comprehensive way. However, it is the first meta-analysis to investigate the risk factors of RI after successful enema reduction in children, to the best of our knowledge, which will certainly have some practical clinical implications.
The main conclusion of this meta-analysis was that children with the presence of fever and PLP may have a higher risk of recurrence following enema reduction for intussusception and the prevalence of vomiting was found to be lower in RI patients than in the control group. Therefore, older age, absence of vomiting, the presence of fever and PLP may not be good factors, at least in terms of the probability for the occurrence of RI, a fact which deserves the attention of clinicians.
XY, RT, SC, ZL, and JZ contributed to the study conception and design. XY, RT, SC, and ZL performed data acquisition. XY, RT, SC, ZL, and JZ performed analysis and data interpretation. XY and RT drafted the manuscript. JZ performed critical revision.
This work was supported by the following grants from the National Natural Science Foundation of China (No. 81701489 and 81771624) and Wenzhou Municipal Science & Technology Bureau (No. Y20160020).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Charles T, Penninga L, Reurings JC, Berry MC. Intussusception in children: a clinical review. Acta Chir Belg. (2015) 115:327–33. doi: 10.1080/00015458.2015.11681124
2. Jiang J, Jiang B, Parashar U, Nguyen T, Bines J, Patel MM. Childhood intussusception: a literature review. PLoS ONE. (2013) 8:e68482. doi: 10.1371/journal.pone.0068482
3. Hannon EJ, Allan RA, Negus AS, Murphy F, Okoye BO. Air enema reduction of intussusception: a registrar-led, protocol-driven service is safe and effective. Pediatr Surg Int. (2013) 29:805–9. doi: 10.1007/s00383-013-3328-2
4. Gray MP, Li SH, Hoffmann RG, Gorelick MH. Recurrence rates after intussusception enema reduction: a meta-analysis. Pediatrics. (2014) 134:110–9. doi: 10.1542/peds.2013-3102
5. Wang Z, He QM, Zhang H, Zhong W, Xiao WQ, Lu LW, et al. Intussusception patients older than 1 year tend to have early recurrence after pneumatic enema reduction. Pediatr Surg Int. (2015) 31:855–8. doi: 10.1007/s00383-015-3726-8
6. Guo WL, Hu ZC, Tan YL, Sheng M, Wang J. Risk factors for recurrent intussusception in children: a retrospective cohort study. BMJ open. (2017) 7:e018604. doi: 10.1136/bmjopen-2017-018604
7. Kim JH, Lee JS, Ryu JM, Lim KS, Kim WY. Risk factors for recurrent intussusception after fluoroscopy-guided air enema. Pediatr Emerg Care. (2018) 34:484–7. doi: 10.1097/PEC.0000000000001071
8. Vo A, Levin TL, Taragin B, Khine H. Management of intussusception in the pediatric emergency department: risk factors for recurrence. Pediatr Emerg Care. (2017). doi: 10.1097/PEC.0000000000001382. [Epub ahead of print].
9. Yang CM, Hsu HY, Tsao PN, Chang MH, Lin FY. Recurrence of intussusception in childhood. Acta Paediatr Taiwan. (2001) 42:158–61.
10. Champoux AN, Del Beccaro MA, Nazar-Stewart V. Recurrent intussusception. risks and features. Arch Pediatr Adolesc Med. (1994) 148:474–8. doi: 10.1001/archpedi.1994.02170050032006
11. Chen SC, Wang JD, Hsu HY, Leong MM, Tok TS, Chin YY. Epidemiology of childhood intussusception and determinants of recurrence and operation: analysis of national health insurance data between 1998 and 2007 in Taiwan. Pediatr Neonatol. (2010) 51:285–91. doi: 10.1016/S1875-9572(10)60055-1
12. Xie X, Wu Y, Wang Q, Zhao Y, Xiang B. Risk factors for recurrence of intussusception in pediatric patients: a retrospective study. J Pediatr Surg. (2018) 53:2307–11. doi: 10.1016/j.jpedsurg.2018.03.023
13. Esmaeili-Dooki MR, Moslemi L, Hadipoor A, Osia S, Fatemi SA. Pediatric intussusception in Northern Iran: comparison of recurrent with non-recurrent cases. Iran J Pediatr. (2016) 26:e3898. doi: 10.5812/ijp.3898
14. Saka R, Sasaki T, Matsuda I, Nose S, Onishi M, Fujino T, et al. Chronic ileocolic intussusception due to transmural infiltration of diffuse large B cell lymphoma in a 14-year-old boy: a case report. SpringerPlus. (2015) 4:366. doi: 10.1186/s40064-015-1157-6
15. Dias AR, Lopes RI, do Couto RC, Bonafe WW, D'Angelo L, Salvestro ML. Ileal duplication causing recurrent intussusception. J Surg Educ. (2007) 64:51–3. doi: 10.1016/j.cursur.2006.09.003
16. Kim KH, Kang KA, Lim JH, Lee KG, Kwon TJ. Inverted meckel diverticulum as a lead point of small bowel intussusception: misinterpreting case as a lipoma. Clin Imaging. (2016) 40:840–2. doi: 10.1016/j.clinimag.2016.03.009
17. Basara I, Canda AE, Sagol O, Obuz F, Secil M. Intussusception and perforation due to an inflammatory fibroid polyp located in the ileum. Wien Klin Wochenschr. (2016) 128:731–4. doi: 10.1007/s00508-016-1073-y
18. Siminas S, Qasem E, Shukla R, Turnock R. Inflammatory fibroid polyp: a rare benign tumor of the alimentary tract in children presenting as intussusception-case report and review of literature. Eur J Pediatr Surg Rep. (2014) 2:16–9. doi: 10.1055/s-0033-1354746
19. Whitehouse JS, Gourlay DM, Winthrop AL, Cassidy LD, Arca MJ. Is it safe to discharge intussusception patients after successful hydrostatic reduction? J Pediatr Surg. (2010) 45:1182–6. doi: 10.1016/j.jpedsurg.2010.02.085
20. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. (2015) 350:g7647. doi: 10.1136/bmj.g7647
21. Wells GA, Shea B, Higgins JP, Sterne J, Tugwell P, Reeves BC. Checklists of methodological issues for review authors to consider when including non-randomized studies in systematic reviews. Res Synth Methods. (2013) 4:63–77. doi: 10.1002/jrsm.1077
23. Shen G, Zhang C, Li J, Zhang J, Liu Y, Guan Z, et al. Risk factors for short-term recurrent intussusception and reduction failure after ultrasound-guided saline enema. Pediatr Surg Int. (2018) 34:1225–31. doi: 10.1007/s00383-018-4340-3
Keywords: intussusception, recurrence, reduction, risk factor, vomiting
Citation: Ye X, Tang R, Chen S, Lin Z and Zhu J (2019) Risk Factors for Recurrent Intussusception in Children: A Systematic Review and Meta-Analysis. Front. Pediatr. 7:145. doi: 10.3389/fped.2019.00145
Received: 20 November 2018; Accepted: 26 March 2019;
Published: 16 April 2019.
Edited by:
Kenneth K. Y. Wong, The University of Hong Kong, Hong KongReviewed by:
Go Miyano, Juntendo University, JapanCopyright © 2019 Ye, Tang, Chen, Lin and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianghu Zhu, emh1amlhbmdodTIwMDVAMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.