
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 14 February 2019
Sec. General Pediatrics and Pediatric Emergency Care
Volume 7 - 2019 | https://doi.org/10.3389/fped.2019.00010
 Michael Buyck1*
Michael Buyck1* Sergio Manzano1,2Kevin Haddad2Anne-Catherine Moncousin2Annick Galetto-Lacour1
Sergio Manzano1,2Kevin Haddad2Anne-Catherine Moncousin2Annick Galetto-Lacour1 Katherine Blondon3,4
Katherine Blondon3,4 Oliver Karam2,5,6†
Oliver Karam2,5,6†Background: Pediatric resuscitations are rare events. Simulation-based training improves clinical and non-clinical skills, as well as survival rate. We assessed the effectiveness of using blindfolds to further improve leadership skills in pediatric simulation-based training.
Methods: Twelve teams, each composed of 1 pediatric emergency fellow, 1 pediatric resident, and 2 pediatric emergency nurses, were randomly assigned to the blindfold group (BG) or to the control group (CG). All groups participated in one session of five simulation-based resuscitation scenarios. The intervention was using a blindfold for the BG leader for the scenarios B, C, and D. Three evaluators, who were blinded to the allocation, assessed leadership skills on the first and last video-recorded scenarios (A and E). Questionnaires assessed self-reported changes in stress and satisfaction about skills after the first and the last scenarios.
Results: Improvement in leadership skills doubled in the BG compared with the CG (11.4 vs. 5.4%, p = 0.04), whereas there was no increase in stress or decrease in satisfaction.
Conclusion: Blindfold could be an efficient method for leadership training during pediatric resuscitation simulated scenarios. Future studies should further assess its effect at a follow-up and on clinical outcomes after pediatric resuscitation.
• As pediatric resuscitations are rare events, simulation-based training have been developed to train the teams who respond to these situations.
• Most teaching techniques focus on improving clinical skills.
• There is very little evidence on how to improve non-clinical skills, such as leadership skills.
• Our study suggests that blindfolding the leader during simulation sessions might improve leadership skills training.
• Our study has identified an innovative way of improving leadership skills.
Pediatric cardiac arrests are rare events in the out-of-hospital (8 events per 100,000 person year) and in-hospital pediatric population (20 events per 100,000 person year) (1, 2). These low incidences do not provide sufficient exposure to allow teams to master these situations. Simon and Sullivan suggested a correlation between emergency physicians' degree of comfort with potentially life-saving skills and frequency of critical situations (3). Similarly, 50% of residents felt inadequately trained to lead cardiac arrest teams in an internal medicine study because such events were too rare (4). Pediatric residents, who are less exposed to resuscitation than internal medicine residents (5), also report a lack of clinical skills when confronted to pediatric cardiac arrest (6).
To improve exposure to these situations, experts have recommended in-hospital simulation-based trainings (7). Simulation-based trainings have been shown to be effective in teaching clinical skills, improving pediatric residents confidence (8), and improving pediatric survival rate (9).
However, according to the European Resuscitation Council, non-clinical skills, which include team communication and leadership, are as important as clinical skills for patient outcomes (10, 11). Team communication, interdisciplinary collaboration, and good leadership have shown a favorable impact on resuscitation outcome (11–15). TeamSTEPPS defines leadership as the “ability to direct and coordinate the activities of other team members, assess team performance, assign tasks, develop team skills and attitudes, motivate team members, plan and organize, and establish a positive atmosphere” (16). These abilities imply a hands-off position for the leader described as a benefit for resuscitation (17). Grant et al. defined 12 non-clinical skills in their Evaluation Score (18), which cover four concepts: physical and verbal leader's position; communication and delegating skills; ability to reassess, adapt and anticipate; and ability to ask for internal and external help.
Non-clinical skills are taught during advanced life support certification (19), but might have been less frequently applied in simulation-based trainings (6). Initiatives to improve this situation, such as leadership-oriented feedbacks after simulation-based trainings and specific leadership workshops have been shown to improve non-clinical skills (20–22). To further bolster leadership skills, other techniques have been evaluated. Some authors have evaluated the effect of blindfolding the leader, although not in a randomized controlled trial (23, 24). Our objective is to evaluate the effect of blindfolding the team leader on leadership skills, using a randomized controlled trial design.
The study is a randomized controlled trial, which took place in the Pediatric Simulation Center of the Geneva University Hospital, the second biggest pediatric tertiary university hospital of Switzerland. As no patient was enrolled, this study evaluating teaching strategies, our local institutional review board (Commission d'Ethique de la Recherche de Genève) waived the need to submit our protocol. However, each participant signed a written informed consent.
Eligible participants were all pediatric emergency fellows, residents and nurses. Exclusion criteria were 1) inability to participate in the full 4-h session, or 2) prior knowledge of the simulations scenarios. Participants were recruited among the staff of the pediatric emergency department. They were assigned to 12 resuscitation teams of four members: one emergency fellow, one emergency resident, and two pediatric registered nurses. These 12 teams were randomly allocated following simple randomization procedure (sealed envelopes with a 50% chance) to the experimental blindfold group (BG) and the control group (CG).
Participants were given a $100 gift-card.
All participants took part in a 4-h session of five high-fidelity simulation-based scenarios, labeled A, B, C, D, and E (Table 1 and Figure 1). All the scenarios were designed by advanced pediatric simulation specialists, trained by EuSim (www.EuSim.org), and were intended to be easily managed when following the Pediatric Advanced Life Support (PALS) algorithms.
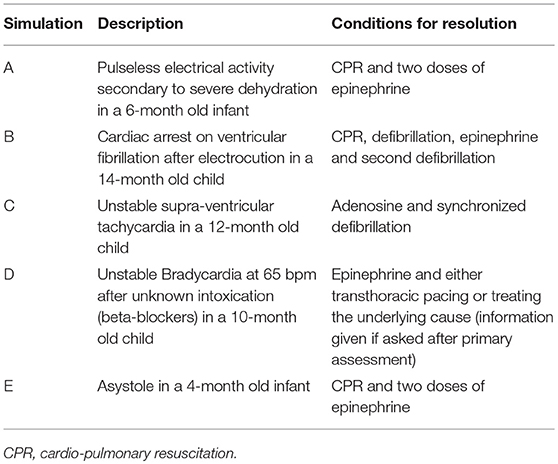
Table 1. Description of the simulation scenarios.
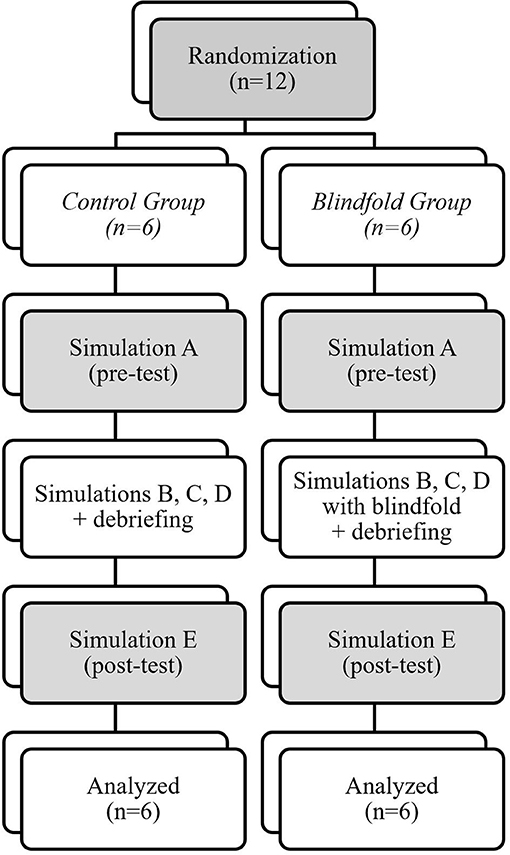
Figure 1. Randomization.
Simulations A and E were the pre-test and the post-test simulations for both groups and was not followed by a debrief (Figure 1). These scenarios were comparable to avoid additional difficulties, which could have affected the non-clinical skills. Immediately after these simulations, each team member was asked to answer two questionnaires on their perceived stress and their satisfaction of the quality of the resuscitation (Data sheets 1 and 2).
Scenarios B, C, and D were identical for both groups. The intervention was using a blindfold for the BG leader for the scenarios B, C, and D. The blindfold was a commercial sleep mask blocking out light. There was no blindfold use in the CG. Each simulation was followed by a standardized debrief lasting a maximum of 20 min, provided by 2 senior Advanced EuSim Instructors, without video feedback. The debrief focused on the team leader's non-clinical skills, in particular the team leader's spatial and verbal position, his communication and delegation skills, and his ability to reevaluate, adapt, anticipate and to ask for help. Every topics were discussed in each group after these three training simulations (Figure 1).
The primary outcome was the progression of the Resuscitation Team Leader Evaluation score between pre-test (simulation A) and post-test (simulation E). For the purpose of this study, we removed the items 1 and 12 from the score described by Grant et al. (18), as the leader was clearly defined from the beginning of the study and teams did not have the possibility to ask for external help. Therefore, the non-clinical skills were assessed on a scale of 0 to 30 points.
Simulations A and E video recordings were scored by three simulation-based training experts who did not take part to the simulations. The experts were blinded to the team allocations to CG or BG.
Secondary outcomes assessed by the experts were: time to CPR from cardiac arrest (measured from the circulatory arrest to CPR initiation), number of pertinent “huddles” (or reassessments), and number of complete and incomplete communication loops. We defined a communication loop as complete when three elements were present: the leader identifies a team member by name, they respond with an audible confirmation of the order, and finally verbally confirm when the task is completed. Finally, we evaluated the difference between pre- and post-test perceived stress (25) and the pre- and post-test satisfaction questionnaires.
We collected the participants' demographic data (number of years of pediatric emergency experience, number of participated sessions of pediatric high-fidelity simulation, number of years from the last PALS certification) to assess for comparability among groups.
The sample size was based on a study that used the Resuscitation Team Leader Evaluation (20), where the mean non-clinical score was 15.6 ± 2.0 points (out of a maximum of 30 points). Based on an estimated 25% improvement from baseline (3.9 points) in the CG and a 50% improvement (7.8 points) in the BG, with a 90% power and an alpha of 0.05, the sample size was six teams in each group.
Results are presented using medians and interquartile ranges (IQR), or numbers and proportions. Differences between the two groups were assessed using Mann-Whitney U-tests or Fisher's exact tests, as appropriate.
All tests were two-sided, with a level of 0.05. We used SPSS version 22 for Mac (SPSS, Chicago, IL) for all statistical analyses.
From December 2016 to March 2017, we recruited 48 participants (12 pediatric emergency fellows, 12 pediatric emergency residents and 24 pediatric emergency registered nurses), who were assigned to 12 teams. There were no statistically significant differences between the BG and CG characteristics at baseline (Table 2).
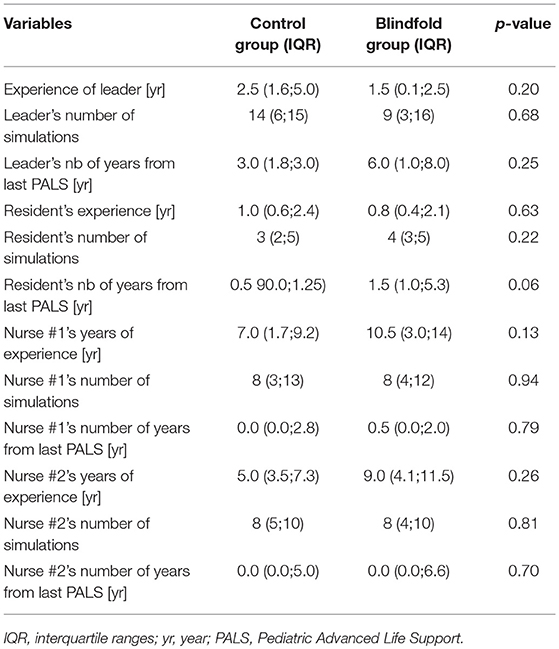
Table 2. Demographic comparison between groups.
The Calgary score did not differ significantly between the two groups at baseline: BG 19 points (IQR 13;27) vs. CG 24 points (IQR 18;27), p = 0.57. The change in Calgary score was significantly greater in the BG than the CG at the end of the session: 11.4% (IQR 8.0;18.9) vs. 5.4% (IQR 0.0;8.6), p = 0.04 (Tables 3, 4, and Figure 2).
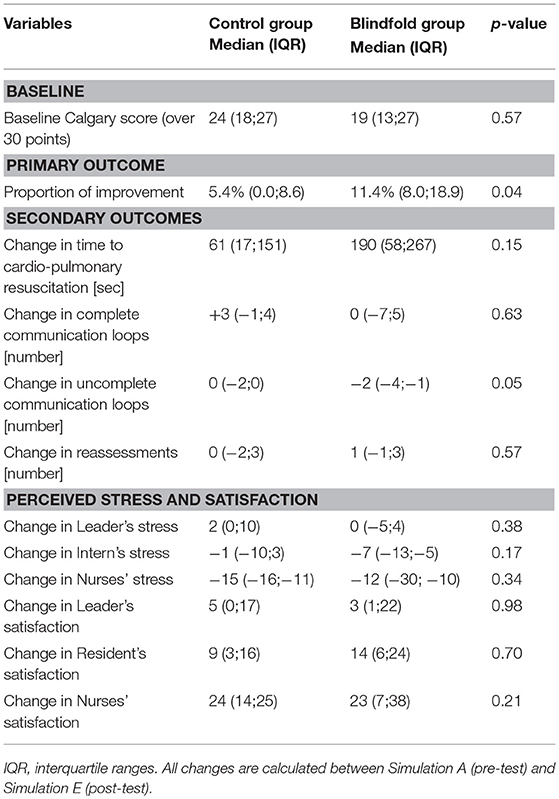
Table 3. Outcomes for blindfolded and control groups.
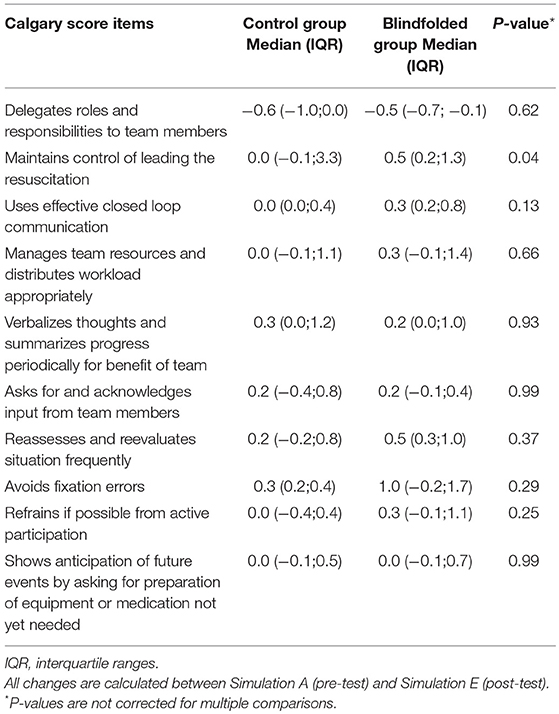
Table 4. Changes in the calgary score for blindfolded and control groups.
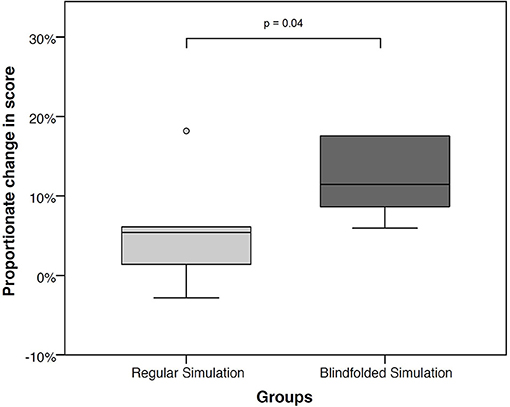
Figure 2. Proportional change in Calgary score from baseline, between regular and blindfolded simulation.
Although there were no differences in the number of complete communication loops, there was a significant decrease in the number of incomplete communication loops in the BG (p = 0.05). There were no statistically significant differences in time to CPR between the two groups (p = 0.15) (Table 3).
There was no significant change in the leaders' and teams' stress nor in the self-reported satisfaction score (p = 0.98; Table 3).
The improvement in leadership skills after the three blindfolded simulations corroborates with the findings from previous non-randomized observations (23, 24). This might be explained by an overall enhancement of teamwork skills, in particular for leadership. Blindfolding the leader might help improve leadership skills by helping keep a distance, instead of focusing on details or taking part in the actions, such as performing chest compressions. Although sometimes unavoidable due to lack of resources, taking part in the actions as a leader can lead to delays in responsiveness to changes to new information such as a change in the patient's state. Furthermore, emergent situations are often noisy with lots of distractors. Wearing a blindfold might help the leader avoid distractions, and can help him focus on the “numbers” or on following the right algorithms. Future studies could help to specify why blindfolded simulations seem to improve leadership skills. For example, it might be interesting to use eye-tracking techniques to analyze the leader's gaze (26). This could allow us to study the time the leader spends focusing on the monitor screen or micromanaging other team members' tasks.
Having a blindfolded leader also requires other team members to improve their communication skills overall. First, all the important data need to be verbalized to keep the leader informed about the current events. Basically, this is calling out a selection of pertinent events or data. Second, team members need to take turns when communicating, because the leader will not be able to follow if they all speak at once. Finally, team members need to acknowledge requests for action, since the leader cannot see if his instructions have been heard. All of these communication tools are important for collaborative teamwork (16). In our study, we found a significant improvement for incomplete communication loops.
We also studied the effect of blindfold on stress. Stress is known to be a major cause of cognitive impairment (27), and one could hypothesize that having to lead a situation, and bear responsibility for the outcome, without being able to see may engender additional stress. However, in light of the discussion above about blindfolds helping to be more focused on the CPR algorithms, and less distracted by the surrounding noise and activity, the leader's perception of stress may in fact benefit from wearing a blindfold. For the other members of the team, stress may be affected by the trust placed in a blindfolded leader's instructions. In our sample, neither the leader's or other team members' stress was increased by the use of a blindfold.
Some limitations for our study must be recognized. First of all, the leadership progression isn't as high as expected. Even if our results are statistically significant, one might question its clinical significance. Also, the two groups had different baseline scores. Nevertheless, we believe that this should not have impacted our results, as the effect of the intervention was calculated as a change from baseline. The debriefing sessions might also have been influenced by the allocation to one arm or the other, because the simulation instructor was not blinded to the allocation as he had to observe the simulations. To address this potential bias, our debriefings were strictly scripted and monitored by the primary investigator who was present for all simulations and debriefings. Another limitation is the variability in the resuscitation team, as the junior physician and the two nurses had heterogeneous levels of experience and training. Other studies have standardized the team, using the same team for all simulations (20). However, heterogeneous teams are more pragmatic and improve the generalizability of our results. Furthermore, as debriefings were aimed at leadership skills, results might be influenced by this consecutive effect. However, this effect should have been minimized by the fact that both groups had similar standardized debriefings addressing leadership issues. Additionally, a more homogeneous team would have increased the statistical power, as it would have reduced the “noise” in the statistical analysis. Our study was also limited by the fact that blindfolded simulation does not represent reality. However, blindfolded simulation seems to be efficient even if it not realistic, as is the case of other teaching technics, such as serious games. Moreover, our sample size was calculated based on an anticipated effect of the intervention that was higher than the one observed. This might explain why most of our secondary outcomes are not statistically significant. We must also acknowledge that the satisfaction was measured with a non-validated tool. Finally, post-training assessment took place just after training; it would have been interesting to propose a follow-up assessment at 3 or 6 months.
Blindfold might be an efficient method for leadership training during pediatric resuscitation simulated scenarios. Future studies should further assess the effect of blindfolded training on communication skills and on clinical outcomes after pediatric resuscitation.
MB and OK initiated the study. MB and OK have full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors contributed to design the study, organization of data acquisition and to interpretation of the results. The first draft of the manuscript was written by MB and OK. All authors contributed to amend it and approved the final version.
This study was supported by internal research funds from Geneva University Hospital.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2019.00010/full#supplementary-material
1. Michelson KA, Hudgins JD, Monuteaux MC, Bachur RG, Finkelstein JA. Cardiac arrest survival in pediatric and general emergency departments. Pediatrics (2018) 141:e20172741. doi: 10.1542/peds.2017-2741
2. Tibballs J, Kinney S. A prospective study of outcome of in-patient paediatric cardiopulmonary arrest. Resuscitation (2006) 71:310–8. doi: 10.1016/j.resuscitation.2006.05.009
3. Simon HK, Sullivan F. Confidence in performance of pediatric emergency medicine procedures by community emergency practitioners. Pediatr Emerg Care (1996) 12:336–9. doi: 10.1097/00006565-199610000-00003
4. Hayes CW, Rhee A, Detsky ME, Leblanc VR, Wax RS. Residents feel unprepared and unsupervised as leaders of cardiac arrest teams in teaching hospitals: a survey of internal medicine residents. Crit Care Med. (2007) 35:1668–72. doi: 10.1097/01.CCM.0000268059.42429.39
5. Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke statistics-−2018 update: a report from the American heart association. Circulation (2018) 137:e67–492. doi: 10.1161/CIR.000000000000055
6. Hunt EA, Walker AR, Shaffner DH, Miller MR, Pronovost PJ. Simulation of in-hospital pediatric medical emergencies and cardiopulmonary arrests: highlighting the importance of the first 5 minutes. Pediatrics (2008) 121:e34–43. doi: 10.1542/peds.2007-0029
7. Weinstock PH, Kappus LJ, Kleinman ME, Grenier B, Hickey P, Burns JP. Toward a new paradigm in hospital-based pediatric education: The development of an onsite simulator program. Pediatr Crit Care Med. (2005) 6:635–41. doi: 10.1097/01.PCC.0000185489.07469.AF
8. Bank I, Snell L, Bhanji F. Pediatric crisis resource management training improves emergency medicine trainees' perceived ability to manage emergencies and ability to identify teamwork errors. Pediatr Emerg Care (2014) 30:879–83. doi: 10.1097/PEC.0000000000000302
9. Andreatta P, Saxton E, Thompson M, Annich G. Simulation-based mock codes significantly correlate with improved pediatric patient cardiopulmonary arrest survival rates. Pediatr Crit Care Med. (2011) 12:33–8. doi: 10.1097/PCC.0b013e3181e89270
10. Monsieurs KG, Nolan JP, Bossaert LL, Greif R, Maconochie IK, Nikolaou NI, et al. European resuscitation council guidelines for resuscitation 2015: section 1. Executive summary. Resuscitation (2015) 95:1–80. doi: 10.1016/j.resuscitation.2015.07.038
11. Marsch SC, Müller C, Marquardt K, Conrad G, Tschan F, Hunziker PR. Human factors affect the quality of cardiopulmonary resuscitation in simulated cardiac arrests. Resuscitation (2004) 60:51–6. doi: 10.1016/j.resuscitation.2003.08.004
12. Cooper S, Wakelam A. Leadership of resuscitation teams: 'lighthouse leadership.' Resuscitation (1999) 42:27–45. doi: 10.1016/S0300-9572(99)00080-5
13. Brett-Fleegler MB, Vinci RJ, Weiner DL, Harris SK, Shih MC, Kleinman ME. A simulator-based tool that assesses pediatric resident resuscitation competency. Pediatrics (2008) 121:e597–603. doi: 10.1542/peds.2005-1259
14. Capella J, Smith S, Philp A, Putnam T, Gilbert C, Fry W, et al. Teamwork training improves the clinical care of trauma patients. J Surg Educ. (2010) 67:439–43. doi: 10.1016/j.jsurg.2010.06.006
15. Hicks CM, Bandiera GW, Denny CJ. Building a simulation-based crisis resource management course for emergency medicine, phase 1: results from an interdisciplinary needs assessment survey. Acad Emerg Med. (2008) 15:1136–43. doi: 10.1111/j.1553-2712.2008.00185.x
16. King HB, Battles J, Baker DP, Alonso A, Salas E, Webster J, et al. TeamSTEPPS™: team strategies and tools to enhance performance and patient safety. In: Henriksen K, Battles JB, Keyes MA, et al., editors. Advances in Patient Safety: New Directions and Alternative Approaches, Volume 3: Performance and Tools. Rockville, MD: Agency for Healthcare Research and Quality (US) (2008) 5–20.
17. Andersen PO, Jensen MK, Lippert A, Østergaard D. Identifying non-technical skills and barriers for improvement of teamwork in cardiac arrest teams. Resuscitation (2010) 81:695–702. doi: 10.1016/j.resuscitation.2010.01.024
18. Grant EC, Grant VJ, Bhanji F, Duff JP, Cheng A, Lockyer JM. The development and assessment of an evaluation tool for pediatric resident competence in leading simulated pediatric resuscitations. Resuscitation (2012) 83:887–93. doi: 10.1016/j.resuscitation.2012.01.015
19. Chameides L, American Heart Association, American Academy of Pediatrics. Pediatric Advanced Life Support Provider Manual. Dallas, TX: American Heart Association (2011).
20. Bragard I, Farhat N, Seghaye MC, Karam O, Neuschwander A, Shayan Y, et al. Effectiveness of a high-fidelity simulation-based training program in managing cardiac arrhythmias in children: a randomized pilot study. Pediatr Emerg Care (2016). doi: 10.1097/PEC.0000000000000931. [Epub ahead of print].
21. Hunziker S, Bühlmann C, Tschan F, Balestra G, Legeret C, Schumacher C, et al. Brief leadership instructions improve cardiopulmonary resuscitation in a high-fidelity simulation: a randomized controlled trial. Crit Care Med. (2010) 38:1086–91. doi: 10.1097/CCM.0b013e3181cf7383
22. Gilfoyle DE, Gottesman R, Razack S. Development of a leadership skills workshop in paediatric advanced resuscitation. Med Teach. (2007) 29:e276–83. doi: 10.1080/01421590701663287
23. Brindley PG, Hudson D, Lord JA. The blindfolded learner—a simple intervention to improve crisis resource management skills. J Crit Care (2008) 23:253–4. doi: 10.1016/j.jcrc.2007.10.036
24. Hughes PG, Ahmed RA. Blindfolded trauma team resuscitation: a strategy for improved leadership and communication. BMJ Simul Technol Enhanc Learn (2017). doi: 10.1136/bmjstel-2017-000277
25. Cohen S, Williamson GM. Perceived stress in a probability sample in the United States. In: Spacapan S, Oskamp S, editors. The Social Psychology of Health. Newbury Park: Sage (1988) 31–67.
26. Williams B, Quested A, Cooper S. Can eye-tracking technology improve situational awareness in paramedic clinical education? Open Access Emerg Med. (2013) 5:23–8. doi: 10.2147/OAEM.S53021
Keywords: pediatric, emergency medicine, simulation-based training, non-clinical skills, leadership
Citation: Buyck M, Manzano S, Haddad K, Moncousin A-C, Galetto-Lacour A, Blondon K and Karam O (2019) Effects of Blindfold on Leadership in Pediatric Resuscitation Simulation: A Randomized Trial. Front. Pediatr. 7:10. doi: 10.3389/fped.2019.00010
Received: 07 November 2018; Accepted: 14 January 2019;
Published: 14 February 2019.
Edited by:
Enitan Carrol, University of Liverpool, United KingdomReviewed by:
Antonio Rodriguez-Nunez, University of Santiago de Compostela, SpainCopyright © 2019 Buyck, Manzano, Haddad, Moncousin, Galetto-Lacour, Blondon and Karam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael Buyck, TWljaGFlbC5CdXlja0BoY3VnZS5jaA== orcid.org/0000-0001-6847-1800
†Oliver Karam orcid.org/0000-0001-6606-1736
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.