 Annastasia Ediati1,2Gijsbert H. W. Verrips3Achmad Zulfa Juniarto2,4Sultana M. H. Faradz2,4Stenvert L. S. Drop5
Annastasia Ediati1,2Gijsbert H. W. Verrips3Achmad Zulfa Juniarto2,4Sultana M. H. Faradz2,4Stenvert L. S. Drop5 Arianne B. Dessens6*
Arianne B. Dessens6*- 1Faculty of Psychology, Diponegoro University, Semarang, Indonesia
- 2Faculty of Medicine, Center for Biomedical Research, Diponegoro University, Semarang, Indonesia
- 3Healthy Living, Child Health, Netherlands Organisation for Applied Scientific Research TNO, Leiden, Netherlands
- 4Dr. Kariadi Hospital, Semarang, Indonesia
- 5Department of Pediatrics, Erasmus Medical Center Rotterdam, Sophia Children's Hospital, Rotterdam, Netherlands
- 6Department of Child and Adolescent Psychiatry and Psychology, Erasmus Medical Center Rotterdam, Sophia Children's Hospital, Rotterdam, Netherlands
Background: Patients with a disorder of sex development (DSD) are born with atypical genitals or may develop atypical genitals and atypical body appearance, if left untreated. Health related quality of life (HRQoL) was assessed in Indonesian patients to whom diagnostic procedures and medical intervention had been delayed.
Method: Comparison of 118 patients born with DSD, aged 6–41 years (60 children, 24 adolescents, and 34 adults) and 118 healthy control subjects matched for gender, age, and residential setting. HRQoL was measured using a translation of the TACQOL/TAAQOL.
Results: According to parental and children's report, children with DSD reported more problems in social functioning and had less positive moods. Girls, in particular, reported problems in cognitive functioning. Adult patients reported more depressive moods, especially women, who reported more anger. No differences were found between in the adolescent groups.
Conclusion: The data suggest that Indonesian children with DSD experienced more problems in social contact than non-affected Indonesian children, whereas Indonesian adults with DSD suffered from negative emotions more often than non-affected Indonesians. These findings on HRQoL are in line with findings on emotional functioning.
Introduction
In patients with a disorder of sex development (DSD), the internal and external sex organs are developed atypically. As a consequence, patients may be born with an atypical external genital and/or may develop an ambiguous physical appearance later in life. The sexual ambiguity puts patients in a delicate social position (1, 2). In the past 20 years, several studies on quality of life in patients with DSD have been conducted (3–9). Studies performed in Western patients revealed inconclusive outcomes, from a significantly reduced quality of life to a reported quality of life not different from, or, even better than the reference populations (6), probably due to differences in sample size, outcome measures, and cultural context (5, 10–13). Studies performed among Asian patients focused on poverty, ignorance, poor basic medical knowledge, inadequate laboratory support, lack of appropriate and affordable medications, understanding the medical condition and future social opportunities in relationships due to reduced fertility (8).
In Indonesia, DSD is largely unknown and clinical management is comparable to care provided in neighbor countries (8). By providing clinical management and by international collaboration, the Dr. Kariadi Hospital became an Indonesian center of expertise. Before they consulted this team, many patients had not or had received insufficient medical care. They were born with ambiguous external genitalia, developed an ambiguous physical appearance in puberty and had been raised with doubts about their gender (14–20).
We aimed to investigate health related quality of life (HRQoL) in Indonesian patients with DSD who recently came under clinical management. This study was part of a larger study conducted jointly with a clinical investigation on the etiology of DSD in these Indonesian patients (18–20). As no Indonesian measure for HRQoL was available, an internationally applied HRQoL measure, the TNO-AZL Children Quality of Life Questionnaire Parent Form [TACQOL-PF, (21)], the TNO-AZL Children Quality of Life Questionnaire Child Form [TACQOL-CF, (22)], and the TNO-AZL Adult Quality of Life Questionnaire [TAAQOL, (23)] were translated. Psychometric properties of this Indonesian version of the TACQOL/TAAQOL were assessed prior to the study and are reported as well in the Instruments section.
Materials and Methods
Study Design and Setting
Comparison of Indonesian children, adolescent, and adult patients with DSD to healthy control subjects matched by age, gender, and residential setting (rural, suburban, or urban area) on HRQoL. All patients consulted the DSD team of the Dr. Kariadi Hospital.
Participants
Patients With DSD
This group included 118 patients diagnosed with DSD: 60 children (42 boys, 18 girls; 6–11 years), 24 adolescents (15 boys, 9 girls; 12–17 years), and 34 adults (20 men, 14 women; 18–41 years). At inclusion, sixty-one (52%) patients had received some treatment (hormonal medication and/or genital surgery), 57 (48%) never had undergone diagnostic evaluation or received any treatment (18). Excluded were individuals with a genital anomaly and dysmorphic features suggestive of malformation syndromes (24), patients with a sex chromosome DSD without mosaicism and patients with DSD and intellectual disabilities (indicated from the child's academic achievements and/or observed by the medical doctor in interaction with the patient). Of 168 patients eligible for evaluation of their psychosocial well-being, 21 (12%) were lost to follow-up and 29 (17%) declined participation. Detailed information on patients and diagnoses is summarized in Table 1.
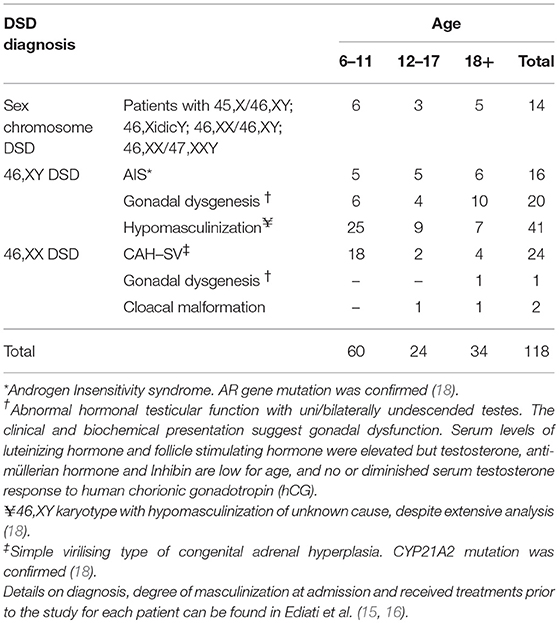
Table 1. DSD diagnoses of participants in the study (N = 118).
Matched Controls
For each patient, a healthy control subject matched for age, gender, and residential settings was included. Matched control subjects were approached through local leaders or midwives. After a potential matched control subject was identified, information about the study and an invitation to join were given.
Instruments
To measure health related quality of life, a generic measure of HRQoL was selected: the TACQOL-PF (21), TACQOL-CF (22), and the TAAQOL (23). In the TACQOL/TAAQOL, HRQoL is determined as a functional status weighted by the emotional reaction. Functional status items inform about the incidence of physical, psychological and social problems on different subscales. Each item is scored on a 3 point Likert scale. If a problem in functional status is reported, the emotional reaction to the problem is determined, by asking the subject how (s)he experiences the reported problem. Experience is scored on a 4 point Likert scale, except for the scales Negative and Positive emotions that only include a 0–2 scale (21–23). For all scales, higher scores indicate a better HRQoL. For the purpose of the study, Indonesian translations of TACQOL and TAAQOL had been provided and evaluated based on a standardized guideline for validating health-related quality of life measures across cultures (25). To assess psychometric quality, data were obtained from 667 healthy subjects: 216 children aged 8–11; 68 adolescents aged 12–15; 57 parents of children aged 6–15; and 326 adults aged 16–34. Principal component analysis (PCA) was performed to analyze the factor structures. The original construct validity was replicated for the Indonesian version of measures. Reliability was tested using internal consistency indicated by Cronbach's alpha coefficients. The results of PCA, number of items used in the Indonesian versions of measures, and the Cronbach's alphas were reported as follows.
TACQOL-PF measure parent-reported HRQoL in children and adolescents aged 6–15 years (26, 27). Four scales were applied: Cognitive functioning (8 items; α = 0.87), Social functioning (8 items; α = 0.53), Positive Emotions (8 items; α = 0.84) and Negative Emotions (8 items; α = 0.61). PCA generated two components (Cognition and Social scales) that explained 42% of the total variance, and another two components of emotions (Positive and Negative emotion scales) that explained 44% of the total variance. TACQOL-CF is a self-report instrument to assess HRQoL in children and adolescents aged 8–15 years. There are different versions: for children aged 8–11 (26) and for adolescents aged 12–15 (27). The Indonesian TACQOL CF 8–11 comprised four scales: Cognitive functioning (6 items; α = 0.56), Social functioning (8 items; α = 0.55), Positive Emotions, (8 items; α = 0.63), and Negative Emotions (7 items; α = 0.67). PCA generated two components (Cognition and Social scales) that explained 31% of the total variance and two components of emotions (Positive and Negative emotion scales) that explained 31.3% of the total variance. TACQOL CF 12–15 comprised four scales: Cognitive functioning (8 items; α = 0.75), Social functioning with peers (4 items; α = 0.49), Positive Emotions, (7 items; α = 0.72), and Negative Emotions (8 items; α = 0.81). PCA generated two components (Cognition and Peers scales) that explained 43.5% of the total variance and two components of emotions (Positive and Negative emotion scales) that explained 35.4% of the total variance. TAAQOL is a self-report instrument for adolescents and adults aged 16 years or older (23). PCA generated nine components with 63.1% of the total variance explained. The Indonesian TAAQOL comprised nine scales with the following number of items and Cronbach's alphas: Cognition functioning (4 items; α = 0.74), Sleep problems (4 items; α = 0.81), Social functioning (3 items; α = 0.55), Limitation in daily activities (4 items; α = 0.73), Problems in sexual functioning (2 items; α = 0.83), Vitality (4 items; α = 0.64), Happiness (4 items; α = 0.86), Depressive moods (4 items; α = 0.50), and Anger (3 items; α = 0.72).
Procedures
Parents and patients were informed orally and received written study information by the medical doctor (AZJ), who coordinated diagnostic evaluation and clinical management (18, 19). After parents and patients had given their written informed consent, psychological assessment including data on patients' socioeconomic and ethnic-cultural background was collected in the hospital or at the patient's home, by a trained psychologist (AE).
Statistical Analysis
Differences in continuous data with skewed distributions between patients and controls were summarized as median values (Mdn) and tested with the Mann-Whitney U test. Differences in categorical data between groups were compared using the Fisher's Exact test. Differences between groups were considered significant at p < 0.05 (two sided). Due to the small sample size, comparisons of subgroups based on diagnoses or different medical/surgical treatments were not conducted.
Results
Participant Characteristics
Comparison between patients and matched control subjects revealed that the majority of participants were male, lived in rural areas, came from the Central Java province, were Javanese, and Muslim. The parents' educational background varied from illiterate to university level, the majority had attended high school. Most parents, particularly parents of patients with DSD, worked in the low-income sector or were unemployed. Socio-cultural-economic characteristics are displayed in Table 2.
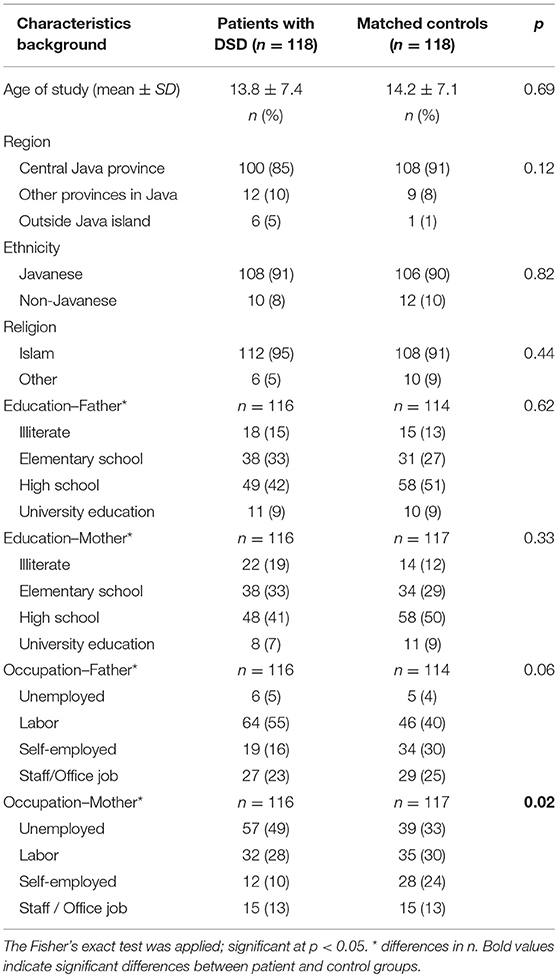
Table 2. Socio-economic and cultural background of study participants.
HRQoL in Children, Adolescents, and Adults With DSD
Table 3 summarizes the findings in children with DSD on TACQOL PF 6–11 and TACQOL CF 8–11. Compared to control children and parents, children with DSD and their parents reported reduced HRQoL on several scales. Boys with DSD and their parents reported a reduction in social contacts (respectively p = 0.03 and p = 0.001). Boys with DSD also reported less positive moods (p = 0.03). Girls with DSD and their parents reported problems in cognitive functioning and school performance (p = 0.008 and p = 0.02, respectively). Parents reported that their daughters had less positive moods (p = 0.003); their daughters reported more negative moods (p = 0.047).
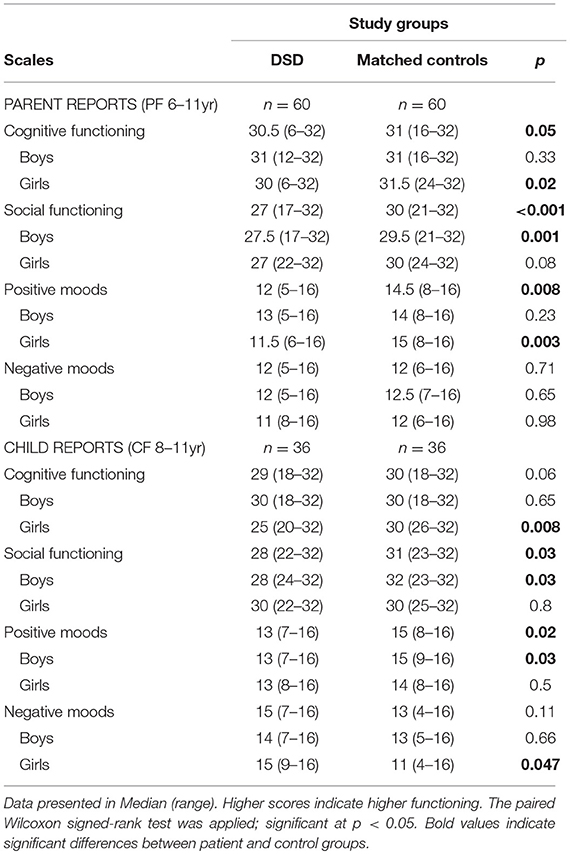
Table 3. HRQoL in children: data from TACQOL PF 6–11 and TACQOL CF 8–11.
Table 4 displays the comparison on TACQOL PF 12–15 and TACQOL CF 12–15 data. There were no differences found between patient and matched control groups on both parental and adolescent reports.
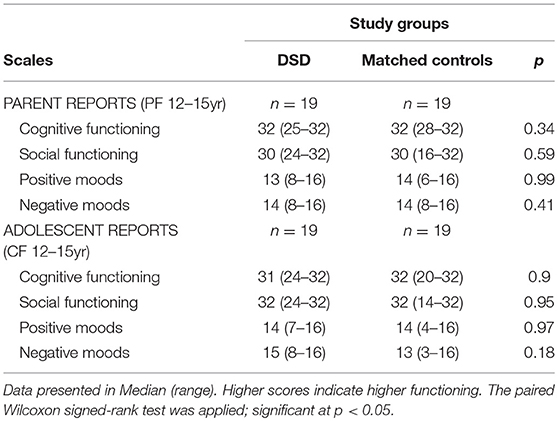
Table 4. HRQoL in adolescents: data from TACQOL 12–15.
Table 5 presents the comparison on data from the TAAQOL. Men and women with DSD reported more depressive moods (p = 0.05), women reported more angry moods too (p = 0.003).
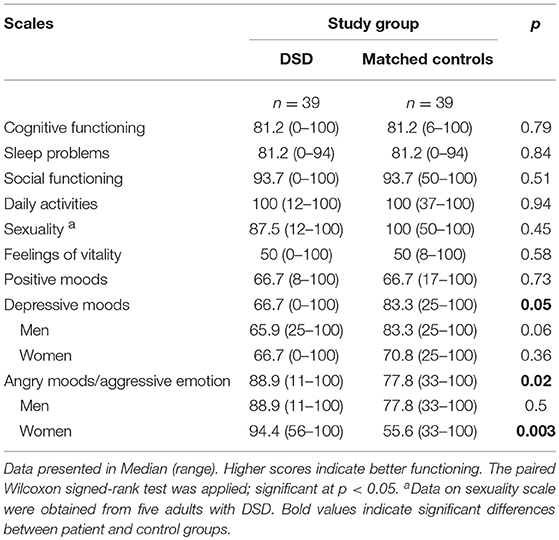
Table 5. HRQoL in adults: data from TAAQOL (16 years or older).
Discussion
Comparison with matched healthy control subjects indicated that DSD impairs social and emotional functioning, particularly in children and adults. Parents of boys and girls with DSD reported different types of problems: a reduction in social contacts was more prominent among boys, whereas girls were less happy and experienced problems in cognitive functioning and school performance. The majority (15 of 18) of young girls in this study had 46,XX CAH-simple virilizing type. Although prior studies revealed that CAH does not affect intelligence (28), recent studies showed an affected working memory and spatial ability in children and adolescents with CAH that might be related to insufficient or fluctuating levels of glucocorticoids in the brain (29–31). Due to limited availability, these Indonesian girls also experienced repeated interruption of cortisone-treatment. Adults reported more depressive emotions, women also reported more angry moods and aggressive emotions. Difficulties in connecting with peers, social isolation, attention problems, mood disturbances, depression, anger and aggression were also reported on other measures in this study (14–17). Many patients felt they were not accepted and feared, or experienced, exclusion (17). Infertility made it difficult for women to meet social expectations with respect to marriage and procreation (14, 17). Our findings match with findings in Chinese patients with DSD who also experienced social limitations (32). Our findings on impaired QoL and elevated distress also correspond with observations in patients from Northern Europe (6, 33, 34). Our patients differed from Western patients as they never had received or only had received minimal medical care. Many of our patients have been raised with an ambiguous physical appearance (18, 19), in doubts about their gender (15), and ignorance about their condition (14–18, 20). It was difficult for them to understand their physical development (8). They also had to cope with the ignorance of their families and villagers (14–17). This makes coping difficult, mood disturbances may easily emerge. Among Indonesians, the terms of hermaphrodite and “kelamin ganda,” meaning “double genitals,” are known. However, patients often reported they were perceived and stigmatized as transgender persons, particularly patients with an ambiguous physical appearance (16, 17).
This study had several limitations: (a) the entire study group of 118 patients falls in three different age groups. Each age group included patients with different DSD diagnoses. The number of patients in each subgroup is small; (b) because the past clinical management had been minimal, there were considerable variation between patients, therefore detailed comparisons between subgroups of patients could not be conducted; (c) We collected data in a reference population of 667 subjects; large enough to perform validity and reliability analyses. The construct validity and reliability found in the original version could be replicated best for the Indonesian TACQOL PF 6–15, but the child versions and TAAQOL showed imperfections. The imperfections on the child forms may be explained by the unfamiliarity of Indonesian children and adolescents with self-evaluation and rating scales.
In order to perform a quantitative study and to compare the HRQoL of Indonesian patients with the HRQoL of patients from other countries, we translated a generic measure originally developed for Western patients. Western measures may only consist domains of HRQoL important for Western patients. Here is another limitation of our study; specific Indonesian socio-cultural factors related to HRQoL have not been studied. For example, Western culture is individual centered, Indonesia is a collective society. Compared to Western countries, Indonesians are strongly demanded to follow social norms and expectancies from childhood onwards (35, 36). Failure to meet social demands is considered shameful for individuals as well as their families (37). In our studies on gender development and sexuality, we learned that being infertile had a great impact on the lives of our patients (14–17). In addition to the domains measured in the present HRQoL measures, cultural specific domains measuring the impact of being infertile, restricted medical knowledge among medical personal, lack of resources, not understanding one's own condition well, lack of affordable and available medication should be added to turn a Western HRQoL measure into a measure more suitable for Asian countries.
In conclusion, this study reported on the HRQoL of Indonesian children, adolescents, and adults with DSD who received medical care late in life. Compared to healthy control subjects, patients reported learning problems, reduction in social relationships and negative moods. The delicate position in the communities is an important contributing factor in the development of mood swings. HRQoL can be improved by early identification and establishment of a diagnosis, medical care, patient education and empowerment to facilitate coping with DSD in daily life and in the community. Such interventions should be integrated into clinical management, can be offered by specialized teams and, along with the popularity of cellphones, can be made widely available by broadcasting via podcasts or on YouTube.
Ethics Statement
The study protocol was carried out in accordance with the recommendations of the Declaration of Helsinki and was approved by the board of the ethical committee at the Faculty of Medicine, Diponegoro University, Semarang, Indonesia. All subjects gave their written informed consent in accordance with the Declaration of Helsinki.
Author Contributions
AE was involved in the study design, scale adaptation, data collection and analysis and drafting of the manuscript. SF and SD supervised the study and revised the manuscript for intellectual content. GV developed the original HRQoL-scales and was involved in analysis and interpretation of data. AJ informed patients about the study and invited them for participation and collected the clinical data. AD conceptualized the study and design, supervised the study, coordinated the data collection, was involved in drafting of the manuscript. All authors approved the final manuscript as submitted.
Funding
AE and AJ received DIKTI scholarships from the Ministry of National Education and Culture, the Republic of Indonesia.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We sincerely thank all participants in this study. We are grateful to Dr. Saskia E. Wieringa (Department of Sociology and Anthropology, University of Amsterdam) for advices during preparation of the Indonesian version of measures utilized in this study; Nani Maharani MD, Ph.D. and Muflihatul Muniroh MD, Ph.D. (Faculty of Medicine, Diponegoro University), Costrie G. Widayanti, MSc (Faculty of Psychology, Diponegoro University) for arranging the interviews; Ir. Kris A. Sieradzan (Department of Medical Informatics, Erasmus MC) and Widagdo MD, MSc for their assistance in data entry. We thank Amy Wisniewski, Ph.D. (Genitourinary Institute, Cook Children's Hospital, Fort Worth, USA) for grammatical review on the earlier version of this manuscript.
References
1. Lee PA, Houk CP, Ahmed SF, Hughes IA. Consensus statement on management of intersex disorders. Pediatrics (2006) 118:e488–500.doi: 10.1542/peds.2006-0738
2. Lee PA, Nordenström A, Houk CP, Ahmed SF, Auchus R, Baratz A et al. Global disorders of sex development update since 2006: Perceptions, approach and care. Horm Res Paediatr. (2016) 85:158–80. doi: 10.1159/000442975
3. Cassia Amaral RC, Inacio M, Brito VN, Bachega TASS, Oliveira AA, Domenice, S et al. Quality of life in a large cohort of adult brazilian patients with 46,XX and 46,XY disorders of sex development from a single tertiary centre. Clin Endocrinol. (2015) 82:274–9. doi: 10.1111/cen.12572
4. D'Alberton F, Assante MT, Foresti M, Balsamo A, Bertelloni S, Dati E et al. Quality of life and psychological adjustment of women living with 46,XY differences of sex development. J Sex Med. (2015) 12:1440–9. doi: 10.1111/jsm.12884
5. de Neve-Enthoven NGM, Callens N, van Kuyk M, van Kuppenveld JH, Drop SLS, Cohen-Kettenis PT et al. Psychosocial well-being in dutch adults with disorders of sex development. J Psychosom Res. (2016) 83:57–64. doi: 10.1016/j.jpsychores.2016.03.005
6. Nordenström A. Psychosocial factors in disorders of sex development in a long-term perspective : what clinical opportunities are there to intervene? Horm Metab Res. (2015) 47:351–6. doi: 10.1055/s-0034-1398562
7. Selveindran, NM, Syed Zakaria SZ, Jalaludin M, Rasat R. Quality of life in children with disorders of sex development. Horm Res Paediatr. (2017) 88:324–30. doi: 10.1159/000478780
8. Zainuddin AA, Grover SR, Shamsuddin K, Mahdy ZA. Research on quality of life in female patients with congenital adrenal hyperplasia and issues in developing nations. J Pediatr Adolesc Gynecol. (2013) 26:296–304. doi: 10.1016/j.jpag.2012.08.004
9. Rapp M, Mueller-Godeffroy E, Lee P, Roehle R, Kreukels BPC, Köhler B, et al. Multicentre cross-sectional clinical evaluation study about quality of life in adults with disorders/differences of sex development (DSD) compared ot country specific reference populations (dsd-LIFE). Health Qual Life Outcomes (2018) 16:54. doi: 10.1186/s12955-018-0881-3
10. Hines M, Ahmed SF, Hughes IA. Psychological outcomes and gender-related development in complete androgen insensitivity syndrome. Arch Sex Behav. (2003) 32:93–101. doi: 10.1023/A:1022492106974
11. Jürgensen M, Lux A, Wien SB, Kleinemeier E, Hiort O, Thyen U. Health-related quality of life in children with disorders of sex development (DSD). Eur J Pediatr. (2014) 173:893–903. doi: 10.1007/s00431-014-2264-z
12. Morgan JF, Murphy H, Lacey JH, Conway G. Long term psychological outcome for women with congenital adrenal hyperplasia: cross sectional survey. BMJ (2005) 330:340–1. doi: 10.1136/bmj.38334.427361.D3
13. Han TS, Krone N, Willis DS, Conway GS, Hahner S, Rees DA, et al. Quality of life in adults with congenital adrenal hyperplasia relates to glucocorticoid treatment, adiposity and insulin resistance: united kingdom congenital adrenal hyperplasia adult study executive (CaHASE). Eur J Endocrinol. (2013) 168:887–93. doi: 10.1530/EJE-13-0128
14. Ediati A, Juniarto AZ, Birnie E, Drop SLS, Faradz SMH, Dessens AB. Body image and sexuality in indonesian adults with a disorder of sex development (DSD). J. Sex Res. (2015) 52:15–29. doi: 10.1080/00224499.2013.816260
15. Ediati A, Juniarto AZ, Birnie E, Drop SLS, Faradz SMH, Dessens AB. Gender development in indonesian children, adolescents, and adults with disorders of sex development. Arch Sex Behav. (2015) 44:1339–61. doi: 10.1007/s10508-015-0493-5
16. Ediati A, Faradz SMH, Juniarto AZ, van der Ende J, Drop SLS, Dessens AB. Emotional and behavioral problems in late-identified indonesian patients with disorders of sex development. J Psychosom Res. (2015) 79:76–84. doi: 10.1016/j.jpsychores.2014.12.007
17. Ediati A, Juniarto AZ, Birnie E, Okkerse J, Wisniewski A, Drop S. et al. Social stigmatisation in late identified patients with disorders of sex development in indonesia. BMJ Paediatr Open (2017) 30:e000130. doi: 10.1136/bmjpo-2017-000130
18. Juniarto AZ, van der Zwan YG, Santosa A, Ariani MD, Eggers S, Hersmus R, et al. Hormonal evaluation in relation to phenotype and genotype in 286 patients with a disorder of sex development from indonesia. Clin Endocrinol. (2016) 85:247–57. doi: 10.1111/cen.13051
19. Juniarto AZ, Setyawati BA, Miranti IP, Santosa A, Hersmus R, Stoop H, et al. (2013). Gonadal malignancy in 13 consecutive collected patients with disorders of sex development (DSD) from semarang (Indonesia). J Clin Pathol. (2013) 66:198–204. doi: 10.1136/jclinpath-2012-201062
20. Juniarto AZ, van der Zwan YG, Santosa A, Hersmus R, de Jong FH, Olmer R, et al. Application of the new classification on patients with a disorder of sex development in indonesia. Int J Endocrinol. (2012) 2012:237084. doi: 10.1155/2012/237084
21. Vogels T, Verrips GH, Verloove-Vanhorick SP, Fekkes M, Kamphuis RP, Koopman HM, et al. Measuring health-related quality of life in children: the development of the TACQOL parent form. Qual Life Res. (1998) 7:457–65.
22. Verrips GHW, Vogels TGC, Koopman HM, Theunissen NCM, Kamphuis RP, Fekkes M, et al. Measuring health-related quality of life in a child population. Eur. J. Public Health (1999) 9:188–93.
23. Fekkes M, Kamphuis RP, Ottenkamp J, Verrips E, Vogels T, Kamphuis, M, et al. Health-related quality of life in young adults with minor congenital heart disease. Psychol Health (2001) 16:239–50. doi: 10.1080/08870440108405502
24. Hutson JM, Grover SR, O'Connell M. Pennell SD. Malformation syndromes associated with disorders of sex development. Nat Rev Endocrinol. (2014) 10:476–87. doi: 10.1038/nrendo.2014.83
25. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. (1993) 46:1417–32.
26. Vogels TC, Verrips GHW, Koopman HM, Theunissen NCM, Fekkes M, Kamphuis RP. TACQOL Manual: Parent Form and Child Form 6–11 years. Leiden Center for Child Health and Pediatrics LUMC-TNO. Leiden (2004).
27. Vogels TC, Bruil J, Koopman HM, Fekkes M, Verrips GHW. TACQOL 12–15 Manual; Leiden Center for Child Health and Pediatrics LUMC-TNO. Leiden (2004).
28. Berenbaum, SA, Bryk KK, Duck SC. Normal intelligence in female and male patients with congenital adrenal hyperplasia. Int J Pediatr Endocrinol. (2010) 2010:853103. doi: 10.1155/2010/853103
29. Browne WV, Hindmarsh PC, Pasterski V, Hughes IA, Acerini CL, Spencer D, et al. Working memory performance is reduced in children with congenital adrenal hyperplasia. Horm Behav. (2015) 67:83–8. doi: 10.1016/j.yhbeh.2014.11.014
30. Collaer ML, Hindmarsh PC, Pastersk V, Fane BA, Hines M. Reduced short term memory in congenital adrenal hyperplasia (CAH) and its relationship to spatial and quantitative performance. Psychoneuroendocrinology (2016) 64:164–73. doi: 10.1016/j.psyneuen.2015.11.010
31. Hampson E, Rovet JF. Spatial function in adolescents and young adults with congenital adrenal hyperplasia: clinical phenotype and implications for the androgen hypothesis. Psychoneuroendocrinology (2015) 54:60–70. doi: 10.1016/j.psyneuen.2015.01.022
32. Zhu D, Hu L, Wan X, Li H, You Q, Gao L, et al. J. Quality of life evaluation in juveniles with disorders of sexual development. Pediatr Surg Int. (2012) 28:1119–23. doi: 10.1007/s00383-012-3182-7
33. Johannsen TH, Ripa CP, Mortensen EL, Main KM. Quality of life in 70 women with disorders of sex development. Eur J Endocrinol. (2006) 155:877–85.doi: 10.1530/eje.1.02294
34. Schützmann K, Brinkmann L, Schacht M, Richter-Appelt H. Psychological distress, self-harming behavior, and suicidal tendencies in adults with disorders of sex development. Arch Sex Behav. (2009) 38:16–33. doi: 10.1007/s10508-007-9241-9
35. Hofstede G. Culture's consequences: Comparing values, behavior, institutions. and organizations across nation. Thousands Oak, CA: SAGE Publication (2001).
36. Mulder N. Individual and society in Java: A cultural analysis. Yogyakarta: Gadjah Mada University Press (1992)
Keywords: disorders of sex development, quality of life, survey, questionnaires, observational study
Citation: Ediati A, Verrips GHW, Juniarto AZ, Faradz SMH, Drop SLS and Dessens AB (2019) Quality of Life in Late-Treated Patients With Disorders of Sex Development: Insights for Patient-Centered Care. Front. Pediatr. 6:434. doi: 10.3389/fped.2018.00434
Received: 09 August 2018; Accepted: 28 December 2018;
Published: 30 January 2019.
Edited by:
Alexander Springer, Medical University of Vienna, AustriaReviewed by:
Matthieu Peycelon, Indiana University, United StatesMaximilian Stehr, Klinik Hallerwiese und Cnopfsche Kinderkrankenhaus, Germany
Martin Kaefer, Indiana University Bloomington, United States
Copyright © 2019 Ediati, Verrips, Juniarto, Faradz, Drop and Dessens. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Arianne B. Dessens, YS5iLmRlc3NlbnNAZXJhc211c21jLm5s