
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 21 December 2018
Sec. Obstetric and Pediatric Pharmacology
Volume 6 - 2018 | https://doi.org/10.3389/fped.2018.00393
 Patricia Khashayar1,2Amir Kasaeian3,4Ramin Heshmat1Mohammad Esmaeil Motlagh5Armita Mahdavi Gorabi6
Patricia Khashayar1,2Amir Kasaeian3,4Ramin Heshmat1Mohammad Esmaeil Motlagh5Armita Mahdavi Gorabi6 Mehdi Noroozi7
Mehdi Noroozi7 Mostafa Qorbani8,9*Roya Kelishadi10*
Mostafa Qorbani8,9*Roya Kelishadi10*Objective: The purpose of this paper is to explore multidimensional factors related to childhood obesity and overweight based on the data gathered on different aspects of the general health status were assessed among a large number of Iranian children and adolescents in the fourth phase of the “Childhood and Adolescence Surveillance and Prevention of Adult Non-communicable disease” survey. It also aims to determine the degree to which each ecological context contributes to childhood overweight/obesity.
Method: A total of 14,880 students and their parents were recruited. They filled out a questionnaire on their relationship with peers, body image, and psychosocial environment of school, dietary habits, life-style habits, physical activity pattern and socioeconomic status (SES). Their height, weight, was measured and body mass index (BMI) was calculated. Obesity and overweight was defined based on the WHO growth chart. Multilevel modeling using three-level random intercept logistic regression models were used to assess predictors of overweight and obesity. In our hierarchical models, children (first level) were conceptualized as being nested within provinces (second level) and provinces within quad regions (third level).
Result: From among the 13,486 recruited students, 9.7% were overweight and 11.9% were obese. In multivariate model (adjusted model), being boy (OR:1.58), living in urban area (OR:1.58), having positive family history of obesity (OR = 2.04), breakfast skipping (OR: 1.46), socioeconomic status (OR moderateSES/lowSES = 1.44 and OR highSES/lowSES = 1.89), and birth weight (BW) (OR normalBW/lowBW = 1.33 and OR highBW/lowBW = 1.8) were associated with childhood obesity. Increasing age was the only factor in the obesity model that had a significant preventive effect on the odds of becoming obese (OR = 0.96, P < 0.001). In multivariate model, living in urban area, increasing age, high and moderate SES, high BW and family history of obesity were the significant predictors of overweight.
Conclusion: Our findings show that high BW, sociodemographic characteristics, breakfast skipping, and family history of obesity are associated with childhood obesity and overweight. Therefore, developing strategies that consider the effects of diverse sociodemographic and environmental factors on childhood overweight and obesity would be the most effective way to prevent and manage this multifactorial health concern.
Over the past decade, a considerable surge is noted in the prevalence of childhood obesity in different parts of the world, raising concerns about the negative health consequences of the condition in the long run (1–3).
According to the reports released by WHO European childhood obesity surveillance initiative 2008, the prevalence of obesity ranged from 6.0 to 26.6% among boys and from 4.6 to 17.3% among girls (3).
Many studies have identified the influential factors for childhood obesity through examining simple relationships between childhood obesity and the predictors such as polygenic, metabolic, psychosocial, behavioral, and environmental (obesogenic) factors with focus on leisure time activity, food intake (4, 5). This is while it is well-known that childhood obesity is the result of a multifactorial etiology involving individuals and environmental factors, adding that effective interventions for prevention and control of childhood obesity should be considered for different factors (6). In other words, childhood obesity could only be tackled through a multidisciplinary approach in three levels: family, school and community but there is a need to identify the elements which are amenable to measurement and interventions in each level (1, 7).
On the other hand, most of the studies on obesity determinants have been conducted in North America where obesity was first described as a social problem. This is while obesity has recently been recognized as an emerging public health concern worldwide (8). Based on the Centers for Disease Control and Prevention's (CDC) criteria, a recent systematic review estimated the overall prevalence of obesity and overweight in Iran to be about 5.1% [95% confidence interval [CI], 4.4–5.8] and 10.8% (95% CI, 10.2–11.4), respectively (9). It suggested that despite the fact that the prevalence of childhood obesity in the Iranian children is not considerably high, but the escalating trend of excess weight among young children is alarming and thus more interventional programs are needed in this regard.
In the fourth phase of the “Childhood and Adolescence Surveillance and Prevention of Adult Non-communicable disease” (CASPIAN) survey, different aspects of the general health status were assessed among a large number of Iranian children and adolescents (10). The purpose of this paper, therefore, is to explore multidimensional factors related to childhood overweight and obesity based on this data, and to determine the degree to which each ecological context contributes to childhood overweight/obesity.
This information will be useful for the design and planning of intervention program through facilitating the identification of areas requiring analysis, major issues and priorities for tackling the obesity epidemic in the country.
The fourth phase of the CASPIAN was conducted in 2011–2012 among a national representative sample of Iranian students from both urban and rural areas. Similar to previous phases, this national school-based surveillance aimed to study the risk behaviors and risk factors of chronic non-communicable diseases using global school-based health survey (GSHS). The study protocol has been published elsewhere (10).
In brief, students from different grades were selected through multistage, cluster sampling method from 31 Iranian provinces. Clusters were determined at the level of schools, resulting in 10 sample units (students and their parents) in each cluster and 48 clusters in each province. The maximum sample size that could give a good estimate of the risk factors of interest was selected. Thus, a total of 14,880 students and their parents were recruited.
The CASPIAN study questionnaires (student and parent questionnaire) were based on the GSHS and was prepared in Persian. The validity and reliability of these questionnaires were confirmed previously (11). The students' questionnaire included questions about demographic characteristics (age, sex, and living area), food and meal consumption habits, life-style habits, physical activity, screen time pattern, and genetic determinants (family history of hypertension, diabetes, obesity). Past history of the student birth weight (BW) and family dietary habits to the student were included in the parents' questionnaire.
Oral assent was obtained from participants, and written informed consent was obtained from their parents and the study was approved by ethic committee of Isfahan University of Medical Sciences (Project code: 294176).
Breakfast consumption was assessed using a single question, “usually on how many days of the week do you eat breakfast?. Breakfast frequency was defined as skippers (eating breakfast 0–4 days/week), and non-skippers (eating breakfast 5–7 days/week) (12). Food habits including fruit intake, vegetable intake, and sweetened beverages were assessed using a single questions, “how many times do you eat each of these food groups?.” Response options were daily, weekly, seldom and never. For statistical analysis food habits considered as daily and non-daily consumption.
Screen time was assessed using a single item, “how long students spent their time on watching television, video and using computer in weekdays and weekends.” According to the international screen time recommendations, screen time <2 h/day was considered as low, and 2 h/day or more was considered high (13). Physical activity was assessed using two questions. (1) During the past week, on how many days you have physically activity for 30 min per day? (2) How many hours do you spend in sport class in school per week? Physical activity was categorized into tertiles. The first tertile was defined as low, second tertile as moderate and third tertile as high.
The methods and variables used for calculating socioeconomic status (SES) were based on the categories approved in the Progress International Reading Literacy Study (PIRLS) for Iran (14, 15). Socioeconomic status (SES) was calculated using principal component analysis (PCA). Using this method, variables such as parental education, parental occupation, possessing private car, school type (public/private), and having personal computer in home were summarized in one main component. This main component was then categorized into tertiles (low, intermediate, and high SES).
Students' BW was asked from parents and was categorized as low BW (LBW) (BW <2,500 g), normal BW (NBW) (BW: 2,500–4,000 g) and high BW (HBW) (BW > 4,000 g).
The height, weight of the students were measured under standard protocols and by using calibrated instruments. Body mass index (BMI) was calculated by dividing weight (kg) to height squared (m2) and then categorized based on the WHO growth charts (16). Childhood overweight and obesity is defined as a BMI between 85th and 95th and ≥ 95th percentile for children of same age and sex, respectively (17).
As the data of one of the provinces was not available, the analysis was performed on information from the other 30 provinces. Mean of continuous variables was reported with 95% of the confidence interval (CI). Categorical variables were expressed as numbers and percentages. Continuous variables such as age, and BMI across regions were compared using ANOVA test. The homogeneity of categorical variables such as SES, sex, and residency area across quad regions were examined by Chi-square test.
Multilevel modeling was also used for data analysis as it adequately represents the unexplained variability of the nested structure, which is often hard to depict in the single-level approach (18). Taking into account the hierarchical structure of our dataset and the possible correlation within and between clusters, we used a three-level random intercept logistic regression models for overweight and obesity. In our hierarchical models, children (first level) were conceptualized as being nested within provinces (second level) and provinces within quad regions (third level).
We assessed the evidence for the effects of several predictors on overweight and obesity. First, the unadjusted effects of the predictors on overweight and obesity were studied in the univariate model. Thereafter those with effects at the 0.2 level of significance were entered to enter the multivariate model. This information helped us study and compare their adjusted effects and effect size on the outcomes of interest.
The results of logistic regression models were presented as odd ratio (OR) and 95% CI. All statistical measures were estimated using survey data analysis methods.
All data management procedures were done using Stata 11.2 (19). Univariate and multivariate modeling were performed using hierarchical modeling methods using Package “lme4” in R software version 3.3.1 (20, 21). All the variables with a p-value at or below 0.2 in the univariate analysis were included in the multivariate analysis. P < 0.05 was considered as statistically significant.
Overall, 13,486 students aged 6–18 years-old out of the 14,880 invited ones participated in this study. The participation rate of the study was 90.6%. Totally 6,846 (50.76%) of them were boys and about 75.6% of them were from urban areas. Mean age (SD) of all participants were 12.46 (3.35) years. Overall, 8.89 and 7.64% of them were categorized in low and high BW group. Family history of obesity was reported by 45.47% of the participants. Being involved in regular physical activity was reported by 24% of the boys and 13% of the girls. Only 9% of the participants did not report being engaged in any physical activity. Overall, 32.8 % (28.39% of boys and 35.89% of girls) of students were breakfast skipper (eating breakfast <5 days/week. Daily consumption of fruits, vegetables and sweetened beverages was reported by 55.74% (58.07% of girls and 53.47% of boys), 35.84% (37.36% of girls and 34.35% of boys), and 20.12% (17.60% of girls and 22.57% of boys) of students, respectively.
The demographic characteristics of the students according to study regions is outlined in Table 1. The distribution of all demographic characteristics (age, sex, living area, and SES) was statistically different between regions (p < 0.05). Table 2 shows the anthropometric indices of study population according to study regions. Overall, 9.7% of the students (10.1% of girls vs. 9.3% of boys) were overweight and 11.9% (10.1% of girls vs. 13.6% of boys) were obese. Mean of BMI and prevalence of overweight and obesity in the second highest SES region was significantly higher than other regions (p < 0.01).
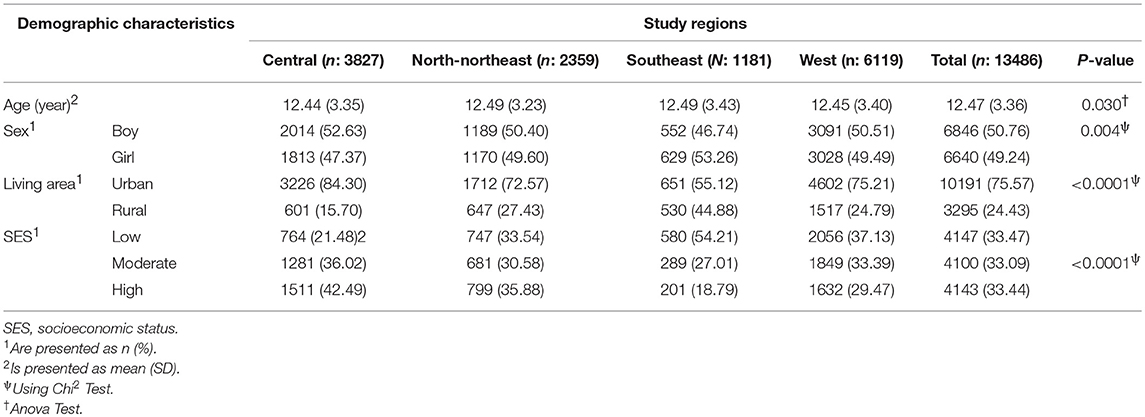
Table 1. Individual level characteristics among population by regions.
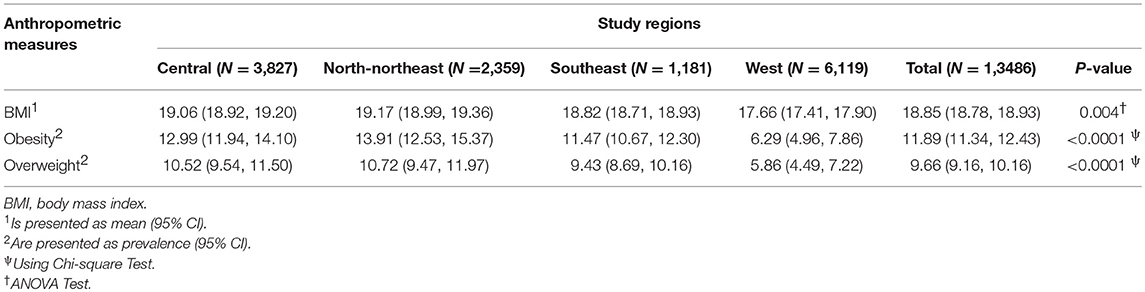
Table 2. Anthropometric measures of study population according to study region.
The associated factors of childhood obesity in univariate and multivariate hierarchical models is presented in Table 3. In the obesity univariate modeling, all the predictors, except for consumption of sweetened beverage and physical activity met the criteria (P < 0.2) and were included in the multivariate model. In the multivariate model, being boy (OR: 1.58), living in urban area (OR: 1.58), having positive family history of obesity (OR = 2.04), breakfast skipping (OR: 1.46), SES (OR moderate SES /low SES = 1.44 and OR high SES/low SES = 1.89), and BW (OR NBW/LBW = 1.33 and OR HBW /LBW = 1.8) were associated with childhood obesity. Increasing age was the only factor in the obesity multivariate model that had a significant preventive effect on the odds of becoming obese (OR = 0.96, P < 0.001).
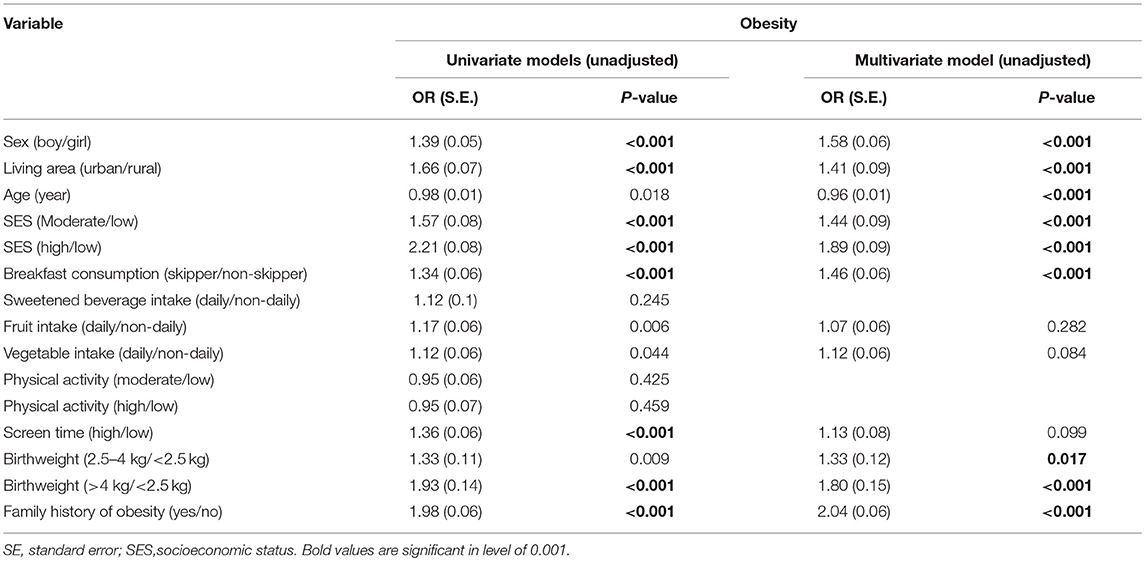
Table 3. Associated factors of childhood obesity in hierarchical multilevel models.
In the overweight univariate hierarchical modeling, all the predictors, except for daily consumption of sweetened beverage, vegetable intake and physical activity met the criteria (P < 0.2) and were included in the multivariate model. In the adjusted model, living in urban area (OR: 1.5), increasing age (OR: 1.04), high and moderate SES (OR moderate SES /low SES = 1.23 and OR high SES/low SES = 1.70), HBW (OR HBW /LBW = 1.39) and family history of obesity (OR: 1.17) were the significant predictors of overweight (Table 4).
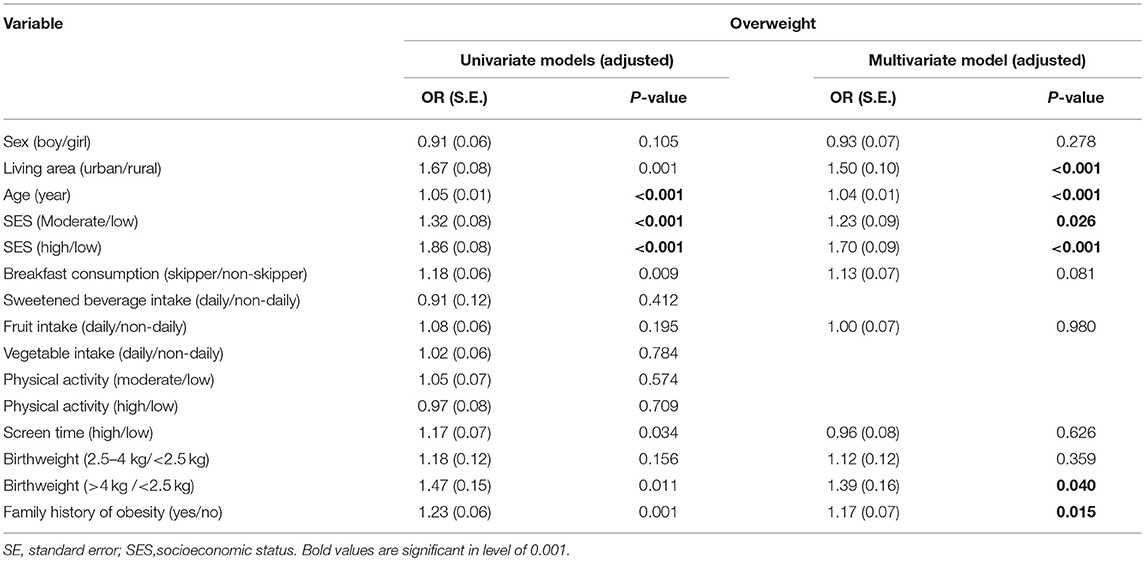
Table 4. Associated factors of childhood overweight in hierarchical multilevel models.
The worrying upward trend in childhood obesity is changing it into a serious and urgent health issue, and thus policymakers in different parts of the world are concentrating on various educational, medical and public health interventions designed to attenuate its growth (22, 23). The best way however to develop and implement an effective strategy is to really understand the condition.
While most of the existing literature focuses on single-component interventions, more recent studies suggest defining the “toxic environment” in which the children live in, and determining an intervention model that integrates activities in more than one setting to ultimately reduce obesity and its complications more effectively (7, 24).
Health behaviors associated with childhood obesity are shaped by multiple factors; as family and school are considered as the main ecological environment surrounding children, adopting health initiatives through a multi-level approach that connects parents and care givers in schools would help fight the multifactorial nature of childhood obesity (25). Mohammadpour-Ahranjani et al. similarly reported that the causes of childhood obesity, which is growing in Iran likewise many other countries, are perceived to relate to macro-level policy influences, the school environment, sociocultural factors, and family and individual behavioral factors, acting in combination (8).
In line with previous studies, especially those from Iran, this study showed high prevalence of childhood obesity in Iran (26, 27). Our results also suggested that the factors that explained the variation in children's weight status were mainly consistent with those reported in previous research on childhood obesity and generally with theoretical reviews on weight gain and its pathways (5, 28). Having higher BW and being born to overweight or obese parents are both considered to increase the risk of childhood obesity (29–31). Moreover, in line with previous studies, breakfast skipping was associated with childhood obesity in our study (32, 33)
As for the influence of the living area, controversial results are reported. Several studies have reported a higher prevalence of obesity among rural children compared with their urban counterparts (34, 35). It is plausible that lower levels of awareness on nutrition and health, lesser access to healthier food and the availability of fewer exercise facilities in rural regions and probably due to lower income levels is the cause. Our study, surprisingly, reported students from urban areas to be at a higher risk of the condition. In our case, the current shift to the westernized lifestyle, especially the intake of attractive energy dense food with undesirable composition, increased consumption of animal fats and sugars and reduced consumption of dietary fiber, along with lack of sufficient physical activity, happening mainly in the urban areas may be the reason (36, 37). This trend has been responsible for the significant increase in the number of overweight and obese children in the past two decades.
Similarly, the relation between SES status and the higher risk of obesity varies according to social environments and context. In developing countries children from lower SES families are reported to be at significantly greater risk of becoming overweight/obese (38–40). Many researchers consider intake of high-calorie and low-nutrition foods such as consuming junk foods or unhealthy foods or limited time and access to resources for physical activity as the main determinants of childhood obesity (41–44). This is while our results, similar to other studies in developing countries showed higher SES status to be associated with higher risks of obesity (45, 46). This again could be because of the rapid growth of the westernized lifestyle in our country. Our results also failed to show any link between following a diet rich in nutritional foods, such as fruit/vegetables, adequate intake of beverages such as milk and fruit and vegetable juice, and engagement in physical activity to decreased risk of childhood overweight/obesity (47, 48).
The present study managed to identify various factors influencing childhood weight during school when children start to be exposed to an environment other than their family. However, we did not take into account the school grade in which the students were studying in and thus the effect of duration of exposure to these external factors is missing. Moreover, all the ecological contexts and parameters that could somehow influence childhood obesity, such as quantity and quality of physical education at school level and home, school nutrition program, and school resources (e.g., playgrounds), were not studied. The influence of contextual factors at the community level, such as the availability and accessibility of a safe park or playground, accessibility to healthy food in the community, and also walkability was not studied either. As a result, the current study was mainly focused on individualized and family factors and failed to identify school and community factors linked with childhood obesity.
Our findings show a high prevalence of childhood overweight and obesity in Iranian children and adolescents and high BW, sociodemographic characteristics, breakfast skipping, and family history of obesity are associated with this health concern. Therefore, developing strategies that consider the effects of diverse sociodemographic and environmental factors on childhood overweight and obesity would be the most effective way to prevent and manage this multifactorial health concern. The results of the present study thus may help policymakers to provide a theoretical basis and model childhood obesity as a function of both individual and external factors deriving from both family and school.
MQ, RK, and RH designed the research. MM and AM conducted the research. AK and MN analyzed the data. PK, AK and MQ wrote the paper. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Karnik S, Kanekar A. Childhood obesity: a global public health crisis. Int J Prev Med. (2012) 3:1–7.
2. Cunningham SA, Kramer MR, Narayan KMV. Incidence of childhood obesity in the United States. N Engl J Med. (2014) 370:403–11. doi: 10.1056/NEJMoa1309753
3. Wijnhoven TMA, van Raaij JMA, Spinelli A, Rito AI, Hovengen R, Kunesova M, et al. WHO European childhood obesity surveillance initiative 2008: weight, height and body mass index in 6-9-year-old children. Pediatr Obes. (2013) 8:79–97. doi: 10.1111/j.2047-6310.2012.00090.x
4. Sherburne Hawkins S, Law C. A review of risk factors for overweight in preschool children: a policy perspective. Int J Pediatr Obes. (2006) 1:195–209. doi: 10.1080/17477160600943351
5. Stafford M, Ellaway A, Sacker A, Wiggins RD, Macintyre S. Pathways to obesity: identifying local, modifiable determinants of physical activity and diet. Soc Sci Med. (2007) 65:1882–97. doi: 10.1016/j.socscimed.2007.05.042
6. Childhood Obesity: Causes and Consequences. (2016). Available online at: https://www.cdc.gov/obesity/childhood/causes.html
7. Kelishadi R, Azizi-Soleiman F. Controlling childhood obesity: a systematic review on strategies and challenges effective interventions for prevention and control of childhood obesity should be considered for different aspects. J Res Med Sci. (2014) 19:993–1008.
8. Mohammadpour-Ahranjani B, Pallan MJ, Rashidi A, Adab P. Contributors to childhood obesity in Iran: the views of parents and school staff. Public Health (2014) 128:83–90. doi: 10.1016/j.puhe.2013.10.005
9. Kelishadi R, Haghdoost AA, Sadeghirad B, Khajehkazemi R. Trend in the prevalence of obesity and overweight among Iranian children and adolescents: a systematic review and meta-analysis. Nutrition (2014) 30:393–400. doi: 10.1016/j.nut.2013.08.011
10. Kelishadi R, Ardalan G, Qorbani M, Ataie-Jafari A, Bahreynian M, Taslimi M, et al. Methodology and early findings of the fourth survey of childhood and adolescence surveillance and prevention of adult non-communicable disease in Iran: the CASPIAN-IV study. Int J Prev Med. (2013) 4:1451–60.
11. Kelishadi R, Majdzadeh R, Motlagh ME, Heshmat R, Aminaee T, Ardalan G, et al. Development and evaluation of a questionnaire for assessment of determinants of weight disorders among children and adolescents: the Caspian-IV study. Int J Prev Med. (2012) 3:699–705.
12. Ahadi Z, Kelishadi R, Qorbani M, Zahedi H, Aram M, Motlagh ME, et al. Association of breakfast intake with psychiatric distress and violent behaviors in Iranian children and adolescents: the CASPIAN-IV study. Indian J Pediatr. (2016) 83:922–9. doi: 10.1007/s12098-016-2049-7
13. American Academy of Pediatrics, Committee on Public Education. American Academy of Pediatrics: children, adolescents, and television. Pediatrics (2001) 107:423–6. doi: 10.1542/peds.107.2.423 Ogle, Laurence T.; Sen, Anindita; Pahlke, Erin;
14. Ogle LT, Sen A, Pahlke E, Jocelyn L, Kastberg D, Roey S, et al. International Comparisons in Fourth-Grade Reading Literacy: Findings from the Progress in International Reading Literacy Study (PIRLS) of 2001. Washington, DC: ERIC (2003). p. 1–42.
15. Heshmat R, Qorbani M, Ghoreshi B, Djalalinia S, Tabatabaie OR, Safiri S, et al. Association of socioeconomic status with psychiatric problems and violent behaviours in a nationally representative sample of Iranian children and adolescents: the CASPIAN-IV study. BMJ Open (2016) 6:e011615. doi: 10.1136/bmjopen-2016-011615
16. WHO Multicentre Growth Reference Study Group. WHO child growth standards based on length/height, weight and age. Acta Paediatr Suppl. (2006) 450:76–85. doi: 10.1080/08035320500495548
17. Li C, Ford ES, Mokdad AH, Cook S. Recent trends in waist circumference and waist-height ratio among US children and adolescents. Pediatrics (2006) 118:e1390-8. doi: 10.1542/peds.2006-1062
20. R Core Team. R: a Language And Environment For Statistical Computing. R Foundation for Statistical Computing, Vienna (2013). Available online at: www.R-project.org (Accessed Oct 18, 2017).
21. Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. (2015) 67:1–48. doi: 10.18637/jss.v067.i01
22. Bass R, Eneli I. Severe childhood obesity: an under-recognised and growing health problem. Postgrad Med J. (2015) 91:639–45. doi: 10.1136/postgradmedj-2014-133033
23. Kelsey MM, Zaepfel A, Bjornstad P, Nadeau KJ. Age-related consequences of childhood obesity. Gerontology (2014) 60:222–8. doi: 10.1159/000356023
24. Kelishadi R, De Ferranti SD, Majdzadeh R, O 'dea JA, Gupta AK, Adeli K. Childhood obesity: today and tomorrow's health challenge. J Obes. (2013) 2013:208392. doi: 10.1155/2013/208392
25. Dooyema CA, Belay B, Foltz JL, Williams N, Blanck HM. The childhood obesity research demonstration project: a comprehensive community approach to reduce childhood obesity. Child Obes. (2013) 9:454–9. doi: 10.1089/chi.2013.0060
26. Khashayar P, Heshmat R, Qorbani M, Motlagh ME, Aminaee T, Ardalan G, et al. Metabolic syndrome and cardiovascular risk factors in a national sample of adolescent population in the middle east and north africa: the CASPIAN III study. Int J Endocrinol. (2013) 2013:702095. doi: 10.1155/2013/702095
27. Mehrkash M, Kelishadi R, Mohammadian S, Mousavinasab F, Qorbani M, Hashemi ME, et al. Obesity and metabolic syndrome among a representative sample of Iranian adolescents. Southeast Asian J Trop Med Public Health (2012) 43:756–63.
28. Baygi F, Dorosty AR, Kelishadi R, Qorbani M, Asayesh H, Mansourian M, et al. Determinants of childhood obesity in representative sample of children in North East of Iran. Cholesterol (2012) 2012: 875163. doi: 10.1155/2012/875163
29. Azadbakht L, Kelishadi R, Saraf-Bank S, Qorbani M, Ardalan G, Heshmat R, et al. The association of birth weight with cardiovascular risk factors and mental problems among Iranian school-aged children: the CASPIAN-III study. Nutrition (2014) 30:150–8. doi: 10.1016/j.nut.2013.06.005
30. Djalalinia S, Qorbani M, Heshmat R, Motlagh ME, Ardalan G, Bazyar N, et al. Association of breast feeding and birth weight with anthropometric measures and blood pressure in children and adolescents: the CASPIAN-IV study. Pediatr Neonatol. (2015) 56:324–33. doi: 10.1016/j.pedneo.2015.01.004
31. Ejtahed HS, Heshmat R, Motlagh ME, Hasani-Ranjbar S, Ziaodini H, Taheri M, et al. Association of parental obesity with cardiometabolic risk factors in their children: the CASPIAN-V study. PloS ONE. (2018) 13:e0193978. doi: 10.1371/journal.pone.0193978
32. Shafiee G, Kelishadi R, Qorbani M, Motlagh ME, Taheri M, Ardalan G, et al. Association of breakfast intake with cardiometabolic risk factors. J Pediatr. (2013) 89:575–82. doi: 10.1016/j.jped.2013.03.020
33. Ahadi Z, Qorbani M, Kelishadi R, Ardalan G, Motlagh ME, Asayesh H, et al. Association between breakfast intake with anthropometric measurements, blood pressure and food consumption behaviors among Iranian children and adolescents: the CASPIAN-IV study. Public Health (2015) 129:740–7. doi: 10.1016/j.puhe.2015.03.019
34. Johnson JA, Johnson AM. Urban-rural differences in childhood and adolescent obesity in the United States: a systematic review and meta-analysis. Child Obes. (2015) 11:233–41. doi: 10.1089/chi.2014.0085
35. Liu J, Bennett KJ, Harun N, Probst JC. Urban-Rural Differences in overweight status and physical inactivity among US children aged 10-17 Years. J Rural Health (2008) 24:407–15. doi: 10.1111/j.1748-0361.2008.00188.x
36. Kelishadi R, Hashemi Pour M, Sarraf-Zadegan N, Sadry G hossein, Ansari R, Alikhassy H, et al. Obesity and associated modifiable environmental factors in Iranian adolescents: Isfahan Healthy Heart Program - heart health promotion from childhood. Pediatr Int. (2003) 45:435–42.
37. Kelishadi R. Childhood overweight, obesity, and the metabolic syndrome in developing countries. Epidemiol Rev. (2007)1:62–76. doi: 10.1093/epirev/mxm003
38. Bahreynian M, Motlagh ME, Qorbani M, Heshmat R, Ardalan G, Kelishadi R. Prevalence of growth disorders in a nationally representative sample of Iranian adolescents according to socioeconomic status: the CASPIAN-III Study. Pediatr Neonatol. (2015) 56:242–7. doi: 10.1016/j.pedneo.2014.12.001
39. Bahreynian M, Kelishadi R, Qorbani M, Motlagh ME, Kasaeian A, Ardalan G, et al. Weight disorders and anthropometric indices according to socioeconomic status of living place in Iranian children and adolescents: the CASPIAN-IV study. J Res Med Sci. (2015) 20:440. doi: 10.4103/1735-1995.163960
40. Rahmanian M, Kelishadi R, Qorbani M, Motlagh ME, Shafiee G, Aminaee T, et al. Dual burden of body weight among Iranian children and adolescents in 2003 and 2010: the CASPIAN-III study. Arch Med Sci. (2014) 10:96–103. doi: 10.5114/aoms.2014.40735
41. Martikainen PT, Marmot MG. Socioeconomic differences in weight gain and determinants and consequences of coronary risk factors. Am J Clin Nutr. (1999) 69:719–26. doi: 10.1093/ajcn/69.4.719
42. Yoon NH, Kwon S. The effects of community environmental factors on obesity among Korean adults: a multilevel analysis. Epidemiol Health (2014) 36:e2014036. doi: 10.4178/epih/e2014036
43. Baygi F, Qorbani M, Dorosty AR, Kelishadi R, Asayesh H, Rezapour A, et al. Dietary predictors of childhood obesity in a representative sample of children in north east of Iran. Zhongguo Dang Dai Er Ke Za Zhi (2013) 15:501–8. doi: 10.7499/j.issn.1008-8830.2013.07.001
44. Payab M, Kelishadi R, Qorbani M, Motlagh ME, Ranjbar SH, Ardalan G, et al. Association of junk food consumption with high blood pressure and obesity in Iranian children and adolescents: the CASPIAN-IV study. J Pediatr. (2014) 35:582–90. doi: 10.1016/j.jped.2014.07.006
45. Monteiro CA, Conde WL, Popkin BM. Independent effects of income and education on the risk of obesity in the brazilian adult population. J Nutr. (2001) 131:881S−6S. doi: 10.1093/jn/131.3.881S
46. Boonpleng W, Park CG, Gallo AM, Corte C, Mccreary L, Bergren MD. Ecological influences of early childhood obesity: a multilevel analysis. West J Nurs Res. 35:742–59. doi: 10.1177/0193945913480275.
47. Pate RR, O'Neill JR, Brown WH, Pfeiffer KA, Dowda M, Addy CL. Prevalence of compliance with a new physical activity guideline for preschool-age children. Child Obes. (2015) 11:415–20. doi: 10.1089/chi.2014.0143
Keywords: obesity, overweight, body mass index, multilevel analysis, socioeconomic status
Citation: Khashayar P, Kasaeian A, Heshmat R, Motlagh ME, Mahdavi Gorabi A, Noroozi M, Qorbani M and Kelishadi R (2018) Childhood Overweight and Obesity and Associated Factors in Iranian Children and Adolescents: A Multilevel Analysis; the CASPIAN-IV Study. Front. Pediatr. 6:393. doi: 10.3389/fped.2018.00393
Received: 11 November 2017; Accepted: 28 November 2018;
Published: 21 December 2018.
Edited by:
Angie Jelin, Johns Hopkins University, United StatesReviewed by:
Geert 't Jong, University of Manitoba, CanadaCopyright © 2018 Khashayar, Kasaeian, Heshmat, Motlagh, Mahdavi Gorabi, Noroozi, Qorbani and Kelishadi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mostafa Qorbani, bXFvcmJhbmkxMzc5QHlhaG9vLmNvbQ==
Roya Kelishadi, cm95YS5rZWxpc2hhZGlAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.