 John J. Farmer III
John J. Farmer III
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr. , 27 November 2015
Sec. Pediatric Infectious Diseases
Volume 3 - 2015 | https://doi.org/10.3389/fped.2015.00084
This article is part of the Research Topic Current State of Invasive Pediatric Cronobacter Infection Research: Evidence vs. Conjecture View all 6 articles
Much has been learned about organism in the Cronobacter/Enterobacter sakazakii complex since I first named and described Enterobacter sakazakii in 1980. However, there are still wide knowledge gaps. One of the most serious is that are still many uncertainties associated with assessing the public health risk posed by these bacteria, particularly in neonatal meningitis. Over the last few decades, Cronobacter contamination of commercial powdered infant formula products has apparently been reduced, but it is still an ongoing problem. The powdered infant formula industry still cannot produce powdered formula that is free of bacterial contamination with Cronobacter, other Enterobacteriaceae, other pathogenic bacteria, and other microorganisms. Until this happens, infants and other will be at risk of becoming infected when they ingest contaminated formula.
“Those who don’t know history are destined to repeat it.” – Edmund Burke (1729–1797, British Statesman and Philosopher). In this review, I look at this familiar quotation in the context of my 40+ year-history with Cronobacter – Enterobacter sakazakii plus its sibling organisms that are now classified in the genus Cronobacter. There are now over 600 papers about this genus of Enterobacteriaceae; however, there are many myths and some knowledge gaps. There are also misconceptions and statements being made that simply are not supported by fact. Many of these are based on the lack of knowledge about the organism’s early history and the first few decades of research that laid the foundation for our current knowledge. The purpose of this review is to debunk, correct, clarify, and recommend. It is based on my long history and many different experiences with “Esak.”
Cronobacter researcher Stephen J. Forsythe wrote a paper in 2012 with an intriguing title – “Myths and legends of Cronobacter – a new bacterial pathogen of babies?” (1). In this short paper, he listed and described seven items that he called “myths.” I really like his idea and wish to expand the discussion he started. Each of my discussion items will be in the form of one of the followings: observation, fact, question, myth, or recommendation.
Facts: The first documented Cronobacter isolate dates back only to 1950. The first strain isolated from a human clinical specimen was in 1953. The first documented case of neonatal meningitis was in 1958 (see below).
The recorded history for Cronobacter organisms is short but they have certainly existed for millions of years (tens of millions of years? hundreds of millions of years?). It is only within the last few years that we have understood the complexity of the group and begun to use precise and accurate names in describing the species, subspecies, biogroups, and other subgroups, such as ribotypes, PFGE pattern types, and sequence types.
1890’s to the 1920’s: The bacteriological era was in its infancy. Bacteria were being described and named but with incomplete and imprecise descriptions. Many yellow-pigmented bacteria were described, given names, and classified in many different genera. A partial list includes: “coliform,” “yellow-pigmented coliform bacteria,” “pigmented cloacae A,” “Serratia species,” “Enterobacter species,” “Erwinia species,” “Chromobacterium typhiflavum,” “Chromobacterium species,” “unidentified Enterobacteriaceae,” and perhaps other names. The term “yellow pigmented coliform” was a vernacular term that appeared in the literature. It would include strains of Enterobacteriaceae that produce a yellow pigment and fermented lactose and produced gas during this fermentation. An organism described as a “yellow pigmented coliform” could be E. sakazakii or could be one of the other species or biogroups of Enterobacteriaceae that share these few phenotypic properties. When a culture with one of the above names exits in a culture collection, it can be tested with current methods to determine its correct identification and name. This was done with the cultures deposited in England’s National Collection of Type Cultures (NCTC) and several were determined to be in the Enterobacter sakazakii complex as described in Farmer et al. (2). Unless cultures were preserved, it is impossible to determine their correct identification based on today’s knowledge.
1929: A case of septicemia due to a “pigmented coliform” was described by Pangalos (3) who proposed the name Bacillus rubroluteus. However, some of the characteristics of this bacterium do not fit those of E. sakazakii: growth in broth was uniformly turbid (“Le bacille pousse sur bouillon en donnant un trouble homogené.”) in contrast to the growth of E. sakazakii, which characteristically settles to the bottom, leaving the upper layer clear; the pigment was yellow-brick rather than yellow “like Bacterium flavum.” The isolate was from a woman suffering from a febrile infection after curettage; not from a newborn. The organism was later renamed Serratia rubroluteum. No cultures of Serratia rubroluteum have apparently survived, so it is not possible to determine its true identity based on current knowledge.
1950: A strain of Enterobacteriaceae was isolated from a “tin of dried milk” and was sent to England’s National Collection of Type Cultures (NCTC). There it was given the designation NCTC 8155. It was re-characterized in the late 1970’s and identified as E. sakazakii biogroup 1 (2). This is the earliest date for a strain of this organism and is also the first documented isolate of Cronobacter from food and from a “dried milk” type of product. In 2011, Joseph and Forsyth (4) reported additional results for this strain, which they had obtained and then studied about 60 years after it was first isolated. They determined that is was “Cronobacter sakazakii sequence type 4,” which they found to be “a highly stable clone with a high propensity for neonatal meningitis.”
1953: A strain from abdominal pus was submitted to NCTC and given the designation NCTC 9238. It was later identified as E. sakazakii biogroup 1 (2). This is the earliest date of an isolate of Cronobacter from a human clinical specimen.
1954: A strain from water was submitted to NCTC and given the designation NCTC 9529. This isolate came from the Metropolitan Water Board. It is most likely was not isolated from drinking (potable) water, but may have come from the river water entering the treatment works rather than post-treatment (Barry Holmes, Director of NCTC, personal communication). It was identified as E. sakazakii, and then re-studied later. According to Joseph et al. (5) and to http://bacteria.ensembl.org/cronobacter_universalis_nctc_9529/Info/Annotation/# about this organism’s correct identification is Cronobacter universalis. This is the first documented water/environmental isolate of Cronobacter.
1958: This is the first documented neonatal meningitis case and the first documented outbreak (2 cases) due to E. sakazakii. It occurred at Osterhills Hospital (St. Albans City Hospital), England (6). The organism was identified as a “pigmented coliform bacterium.” Fortunately, these isolates were sent to M. T. Parker, of the Manchester (England) Public Health Laboratory who studied and preserved them.
1961: Urmenyi and White-Franklin publish their report about the Osterhills Hospital meningitis cases in The Lancet and used the term “pigmented coliform” in the title of the manuscript (6).
1965: The second documented case of meningitis due to E. sakazakii occurred at the city and county hospital of Odense, Denmark (7). This isolate was compared by M. T. Parker to the 1958 Osterhills Hospital isolates, and it was almost identical to the strains isolated in 1958. These organisms were again identified as a yellow-pigmented Enterobacter cloacae rather than as Enterobacter sakazakii.
1972 to 1976: DNA–DNA hybridization experiments showed that Enterobacter cloacae and yellow-pigmented E. cloacae were closely related, but the genetic relationship was not close enough to be classified as belonging to the same species (8, 9).
1977: The name Enterobacter sakazakii first appeared in print. This was in a widely distributed CDC publication (10). I also used this name in an oral presentation at the 1977 American Society for Microbiology national meeting.
1977–79: The name Enterobacter sakazakii was not validly published under the rules of the Bacteriological Code and should have appeared in parentheses and written as “Enterobacter sakazakii.”
1980: The name Enterobacter sakazakii was “officially published” according to the rules of the Bacteriological Code, and thus the name became a validly published species that can be written as – Enterobacter sakazakii, Farmer et al. (2). The species description included 15 subgroups, which were classified and named as 15 distinct biogroups. Biogroup 15 was very different in its biochemical properties from the other 14 biogroups. We speculated that this unusual biogroup might eventually be classified as a separate species, which indeed it was, 27 years later (11).
1980 onward: Once Enterobacter sakazakii was named and described, case reports of E. sakazakii neonatal meningitis and other papers about it began to appear in the literature.
1980 to 2007: From 1980 to 2007, Enterobacter sakazakii was considered to be a single well-defined bacterial species with 15 biogroups as named and described in the original paper (2). During this time, commercial and other identification systems and methods gave an identification of Enterobacter sakazakii (or Enterobacter cloacae). Each of these identifications needs to be reevaluated based on the establishment of Cronobacter in 2007 (see below).
1983: Muytjens et al. (12) summarize eight neonatal meningitis and sepsis cases of Enterobacter sakazakii from The Netherlands. This was the first large series of neonatal infections to be reported and the first outbreak with a thorough analysis. The cases were over a 4-year time period (1977–81) and comprised all the Enterobacter sakazakii cases detected in the entire country.
1987: Muytjens et al. (13) studied the contamination rate of commercial powdered formula products produced in 35 different countries. They found E. sakazakii and other Enterobacteriaceae were common contaminants. E. sakazakii was detected in powdered formula made in 13 different countries. This paper really marked the beginning of the association of E. sakazakii with powdered formula. This association and the danger of contaminated powdered formula was emphasized in an editorial by Muytjens and Kollée (14).
1988: This is the date of the first documented E. sakazakii outbreak in the United States (15). There were two bacteremia cases and two additional cases of colonization in a neonatal intensive care unit. All four infants had been fed a powdered protein hydrolyzate formula that had been mixed in a blender. The blender and an open can of the powdered protein hydrolyzate formula were cultured and found to be contaminated with Enterobacter sakazakii. This raised the question that does not have an answer – did the powdered formula contain Enterobacter sakazakii and contaminate the blender, or did the contaminated blender contaminate the formula?
2001: There was an outbreak of Enterobacter sakazakii at a Tennessee hospital with one case of meningitis and eight additional cases with Enterobacter sakazakii colonization. It was caused when infants were fed Portagen, a commercial powdered formula produced by Mead Johnson. This outbreak marked the beginning of the U. S. Food and Drug Administration’s interest in contamination of powdered infant formula products and especially contamination with Enterobacter sakazakii.
2002, April 11: In response to the Portagen outbreak, the U. S. Food and Drug Administration issued a letter to American health community: “Health Professionals Letter on Enterobacter sakazakii Infections Associated with Use of Powdered (Dry) Infant Formulas in Neonatal Intensive Care Units.” (16)
2002, July 26: In response to the Portagen outbreak, the U. S. Food and Drug Administration began a program to determine the degree of E. sakazakii contamination of powdered infant formula products (and associated raw ingredients) made by American companies (17). This FDA study determined that 5 of 22 (22.7%) of the batched samples of “finished product” were contaminated with E. sakazakii (18). Two of 69 samples of raw ingredients were contaminated with E. sakazakii (18).
2003, March 18–19: In further responses to the Portagen outbreak, the Food Advisory Committee of the U. S. Food and Drug Administration held a meeting of experts to discuss E. sakazakii infections in babies and infants with emphasis on contamination of powdered infant formula made by U. S. companies. At the meeting Dr. Don Zink presented the results from the FDA sampling and testing for E. sakazakii described above.
Ref (19) gives the complete set of slides for all eight presentations that were given.
2004: The World Health Organization published the first of three books on Cronobacter/Enterobacter sakazakii (20).
2006: The World Health Organization published the second of three books on Cronobacter/Enterobacter sakazakii (21).
2007: Cronobacter was proposed as a new genus to include the organisms formerly classified as Enterobacter sakazakii. Cronobacter Iverson et al. – had eight different organisms including four named species, one unnamed species, and five named subspecies:
Cronobacter sakazakii
Cronobacter sakazakii subspecies sakazakii
Cronobacter sakazakii subspecies malonaticus
Cronobacter dublinensis
Cronobacter dublinensis subspecies dublinensis
Cronobacter dublinensis subspecies lactaridi
Cronobacter dublinensis subspecies lausanensis
Cronobacter muytjensii
Cronobacter turicensis
Cronobacter genomospecies 1 (a distinct species, but unnamed)
2008: The World Health Organization published the third of three books on Cronobacter/Enterobacter sakazakii (22). The book Enterobacter sakazakii (23, 24) was published by the American Society for Microbiology in its series Emerging Issues in Food Safety.
2009, January 22–23: The First International Conference on Cronobacter (Enterobacter sakazakii) was held at O’Reilly Hall, University College, Dublin, Ireland1.
At this conference Dr. Angelica Lehner reported that Enterobacter sakazakii can be in a viable but non-culturable state and thus escape detection when only “normal” microbiological culturing methods are used.
2012–13: Three new species of Cronobacter were described – Cronobacter universalis, Cronobacter pulveris, and Cronobacter zurichensis.
2015: Ten species and three subspecies of Cronobacter have now been named, described, and have standing in nomenclature:
Cronobacter Iversen et al. (25)
Cronobacter condimenti Joseph et al. (5)
Cronobacter dublinensis Iversen et al. (25)
Cronobacter dublinensis subsp. dublinensis Iversen et al. (25)
Cronobacter dublinensis subsp. lactaridi Iversen et al. (25)
Cronobacter dublinensis subsp. lausannensis Iversen et al. (25)
Cronobacter helveticus Brady et al. (26)
Cronobacter malonaticus Iversen et al. (25)
Cronobacter muytjensii Iversen et al.
Cronobacter pulveris Brady et al. (26)
Cronobacter turicensis Iversen et al. (25)
Cronobacter universalis Joseph et al. (5)
Cronobacter zurichensis Brady et al. (26)
See http://www.bacterio.net/cronobacter.html and http://www.bacterio.net/-allnamesac.html for complete details for the above organisms and as a convenient way to find updates on new organisms in this genus and new organisms in other genera. Additional Cronobacter species probably exist but await discovery and description.
Two myths: Enterobacter sakazakii had been moved to a new genus Cronobacter. All strains originally known as Enterobacter sakazakii are now Cronobacter sakazakii.
Most scientists are not familiar with the Bacteriological Code whose principals and rules govern the naming and classifying bacteria. Accurate statements in relation to the myths above are:
(1) The original name and classification of this group of organisms now known as Cronobacter is “Enterobacter cloacae – yellow pigmented strains.” An even older name is “pigmented coliform.” However, most strains given the name “pigmented coliform” would probably not be Cronobacter if they could be re-studied and precisely identified.
(2) The “first proposed reclassification” was by Farmer et al. who named and described Enterobacter sakazakii. The name Enterobacter sakazakii was, and is, validly published and is available for those who might not agree with the proposed reclassification as the genus Cronobacter. A better and more precise term is “the Enterobacter sakazakii complex” which is equivalent to “Cronobacter species.”
(3) The “second proposed reclassification” was that of Iversen et al. who named and described Cronobacter with a total of 7 species/subspecies including Cronobacter sakazakii, the most important species.
(4) All strains originally classified as Enterobacter sakazakii need to be re-studied to see which Cronobacter species they belong to. Many will be Cronobacter sakazakii, but some will be other Cronobacter species.
For example, almost 40 years ago I isolated an organism from my dog’s water bowl and identified it as Enterobacter sakazakii. Today, this strain could be revived from a CDC freezer and retested with one or more sensitive identification methods now available. Its correct identification may be Cronobacter sakazakii or it may be one of the other Cronobacter species. When this is done a statement such as the following can be written:
“The organism that Farmer isolated in 1978 from his dog’s water bowl (CDC strain 1167-78) was originally identified as E. sakazakii. In 2015 it was removed from a CDC freezer and re-tested. The new identification was Cronobacter dublinensis subspecies lactaridi* based on the following criteria: PCR analysis, 16S r-RNA sequence analysis ….”
*Or whatever this revised identification turns out to be
The “Farmer” in “Cronobacter sakazakii (Farmer et al. 1980) Iversen et al. 2008” means that Farmer is “claiming credit” for this scientific finding. I saw a version of this statement in a rebuttal of a report that I had written. It was written by a well-known Cronobacter expert in a report he prepared for a legal case. He claimed that I was claiming credit for this organism, and seemed to imply that I did not have any right to do this. The term “Cronobacter sakazakii (Farmer et al. 1980) Iversen et al. 2008” is merely the correct way to cite this name under the rules of the Bacteriological Code. It has nothing to do with “claiming credit” as this expert incorrectly stated. His statement was based on a misunderstanding of the correct way to cite a species name when a new genus name is proposed. See the Bacteriological Code, and http://www.bacterio.net/cronobacter.html to verify the correctness of the above myth debunking.
Question: Are there other organisms in the family Enterobacteriaceae that can be confused with Cronobacter when they are being identified? Yes, strains in the “Enterobacter cloacae complex” can easily be confused. Strains typically identified as Enterobacter cloacae fall into at least five DNA-DNA hybridization groups depending on the operational definition used. The term “Enterobacter cloacae complex” might also include, or be confuses with, the organisms listed below (27):
Enterobacter cloacae DNA hybridization group 1
Enterobacter cloacae DNA hybridization group 2
Enterobacter cloacae DNA hybridization group 3
Enterobacter cloacae DNA hybridization group 4
Enterobacter cloacae DNA hybridization group 5
Enterobacter amnigenus
Enterobacter asburiae
Enterobacter cancerogenus
Enterobacter dissolvens
Enterobacter hormaechei
Enterobacter kobei
Enterobacter ludwigii
Enterobacter nimipressuralis
Enterobacter pyrinus
Enterobacter taylorae
Enteric Group 17
Others (depending on the operational definition used) such as some strains of Erwinia, Brenneria, Pantoea, Pectobacterium, Enterobacter ludwigii. For a more detailed analysis of this identification issue, see the discussions of Farmer et al. (27) in the Manual of Clinical Microbiology.
Question: Does the above discussions have anything to do with practical matters relating to Cronobacter? Yes. Every identification of a Cronobacter strain should be taken “with a grain of salt” or even better, the entire box of salt. The reader should critically examine the method(s) use in determining the identification. This is a particular problem if commercial biochemical identification methods (“commercial ID kits”) are used. They are not sensitive in distinguishing all of the organisms described in the preceding paragraphs.
Questions: I have seen the terms “Enterobacter sakazakii (sensu lato)” and “Enterobacter sakazakii (sensu stricto)” – What exactly do they mean and why are these terms necessary? These terms are used to clarify the meaning of the words/terms “Enterobacter sakazakii” and “Cronobacter sakazakii.” They became necessary when the new genus Cronobacter was proposed in 2007. Below is a listing that should clarify this.
The organisms/terms below have the same definition and meaning and it is different from the names/organisms in the next grouping:
• Enterobacter sakazakii (sensu lato)
• Enterobacter sakazakii (in a broad sense, those strains highly related to the type strain plus those less related but still now considered to be species of Cronobacter)
• Enterobacter sakazakii group
• Enterobacter sakazakii as defined by Farmer et al. (2)
• Cronobacter species
The organisms/terms below have the same definition and meaning and it is different from those in the previous grouping:
• Enterobacter sakazakii (sensu stricto)
• Enterobacter sakazakii (in a strict sense, only those strains highly related to the type strain of Enterobacter sakazakii)
• Cronobacter sakazakii (only those strains highly related to the type strain of Cronobacter sakazakii and excluding all of the other Cronobacter species)
Question: What are some correct and incorrect usages of “Enterobacter sakazakii” from the pre-2007 literature?
Correct:
• In 1978, Farmer isolated a strain of Enterobacter sakazakii from his dog’s water bowl.
• In 1978, Farmer isolated a strain of Enterobacter sakazakii (sensu lato) from his dog’s water bowl.
• In 1978, Farmer isolated a strain of the Enterobacter sakazakii group from his dog’s water bowl.
• In 1978 Farmer isolated a strain of the Enterobacter sakazakii complex from his dog’s water bowl.
• In 1978, Farmer isolated a strain of Cronobacter from his dog’s water bowl.
• In 1978, Farmer isolated a Cronobacter species from his dog’s water bowl.
Incorrect:
• In 1978, Farmer isolated a strain of Cronobacter sakazakii from his dog’s water bowl.
This last sentence would become correct if the strain isolated from his dog’s water bowl were re-studied and found to be Cronobacter sakazakii, rather than one of the other species of Cronobacter. Until this is done, it is best to refer to this organism as “Cronobacter species.”
Fact: Cronobacter is a typical member of the family Enterobacteriaceae in many ways. This is documented in original 1980 paper by Farmer et al. and further described in dozens of subsequent publications.
Fact: One simple way to recognize a strain of Cronobacter is to take advantage of the very unusual way that colonies of Cronobacter grow on microbiological plating media. I described these colonies on page 576 (2) as follows: “… either dry or mucoid, crenated (notched or scalloped), and rubbery when touched with a loop (very little growth was removed and the colony snapped back when touched).” I noted that the colonies were very different from the typical colonies produced by other members of the family Enterobacteriaceae which are smooth, moist, and non-rubbery.
Fact: Another simple way to recognize a strain of Cronobacter is that most strains produce a bright yellow pigment. The original study found that 97% of the stains studied did this and that pigment production was much stronger at room 25°C than 36°C (2). However, the ability to produce yellow pigment was sometimes lost upon storage and subculture, which is true of other Enterobacteriaceae that produce distinct pigments.
Fact: Strains of Cronobacter can grow as individual cells, pairs of cells, and large clumps which contain hundreds/thousands of connected cells. This was shown in the original study (2).
Fact: Strains of Cronobacter can also grow as large sheets of cells called biofilms. This has been documented in many published studies.
Fact: Strains of Cronobacter have phenotypic properties and genetic properties that can be used as “strain typing methods” in microbial forensic analysis. The use of these genetic properties in epidemiological studies and causation analysis is illustrated in Table 1.
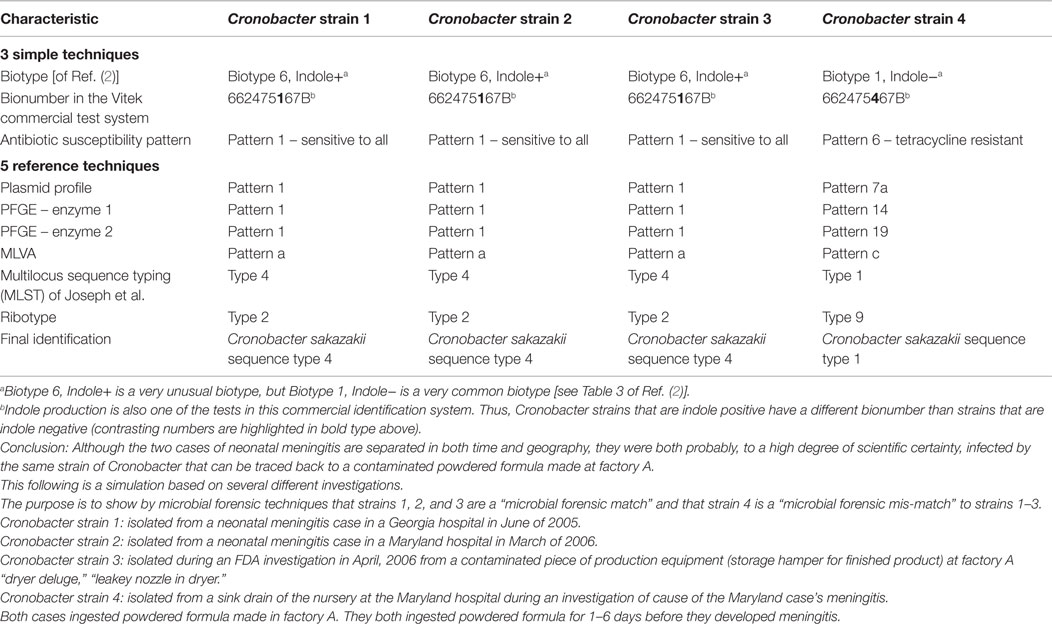
Table 1. Example of how microbial forensic analysis can be used to “trace back” Cronobacter strains to a powdered formula factory – use of simple and reference (more complex) techniques to compare strains.
Facts: Species/strains of Cronobacter have different pathogenic potentials for causing meningitis in infants and babies. Cronobacter sakazakii sequence type 4 (C. sakazakii ST 4) is extremely important as a cause of neonatal meningitis. Joseph and Forsythe (4) studied a collection of 41 Cronobacter strains and found that they could be defined in terms of different “sequence types.” They gave “sequence types designations” for these that went from 1 to 41 (ST1 – ST41) (see Table 1 in their paper). A summary of findings from the paper:
• Of the 20 C. sakazakii ST4 strains, ten were from neonates; seven were from infants; one was from a child and the source of the other was unknown.
• Seven of the C. sakazakii ST4 strains had been isolated from spinal fluid, two were from cases of necrotizing enterocolitis and one was from a case of bacteremia.
• Half (20 of 41) of the C. sakazakii strains were ST4, and 9 of 12 meningitis isolates were ST4.
• C. sakazakii ST4 appears to be a highly stable clone with a high propensity for neonatal meningitis.
• C. sakazakii ST4 appears to be a stable clone because strains have been isolated from 7 countries for > 50 years. The earliest non-clinical isolate was isolated in 1950 from a can of dried milk.
This illustrates the unique position of C. sakazakii ST4 in relation to other Cronobacter species and strains, and in relation to meningitis in neonates and babies. This is analogous to the unique position of Escherichia coli K1 as a cause of meningitis, which is in contrast to other species and strains in the genus Escherichia.
The importance of C. sakazakii ST4 is important in a critical analysis of the statement “Cronobacter is widely distributed in the environment.” This should be reframed to the question “Cronobacter/E. sakazakii strains have been found in several different kinds of environment specimens, but do any of these environmental strains have the capability of causing neonatal meningitis?”
Facts: Enterobacteriaceae strains including Cronobacter can become injured when they are subjected to stress such as heat and drying. Bacteria can respond to stress by entering a unique physiological state known as the “viable but non-culturable” (often abbreviated as the “VNC” state”). Many different studies indicate that pathogens in the family Enterobacteriaceae can enter this state. These include Escherichia coli O157:H7, Salmonella, Shigella, Enterobacter cloacae, Klebsiella, and many others. See the review by Oliver (28) for a complete listing and details.
Question: Can Cronobacter strains react to stress conditions and pass from a “viable and culturable state” to a “viable but non-culturable state?” Until recently Cronobacter had not been studied in regard to the viable but non-culturable state. Similarly, until recently laboratories had to resort to research procedures to look for this phenomenon. However, that there are now commercially available reagents and procedure for reviving, detecting and isolating strains of Cronobacter that are in the viable but non-culturable state.
Observation 1: At the International Conference on Cronobacter (Enterobacter sakazakii), Dublin, Ireland, January 22-23, 2009 the first data on the viable but non-culturable state for Cronobacter/E. sakazakii was presented. Dr. Angelica Lehner is one of the foremost Cronobacter researchers. She works at the Institute of Food Safety and Hygiene, University of Zurich, Zurich Switzerland and has done experiments using E. sakazakii strain E 601 (ATCC 29544), which is a non-capsule producer and E. sakazakii strain E 602 which produces capsules. She stated that “Cronobacter seems to enter a viable but non-culturable state” – see: http://crono09.tripod.com/lehner.pdf.
Observation 2: The commercial company Sigma Aldrich states: “Supplementing the pre-enrichment and enrichment broths with ferrioxamine E significantly improved the recovery of Salmonella, Cronobacter spp., Staphylococcus aureus and Yersinia enterocolitica from artificially or naturally contaminated foods [1–3]. A concentration of ferrioxamine E (available from Sigma, see Table 1) in the range of 5–200 ng/mL supports growth (see Table 2). … This leads to a reduced lag-phase in the medium and reactivates damaged bacteria. The ferrioxamine E is often used in Buffered Peptone Water the medium recommended by the ISO-Norms for Enterobacteriacea ….” (see Table 3)
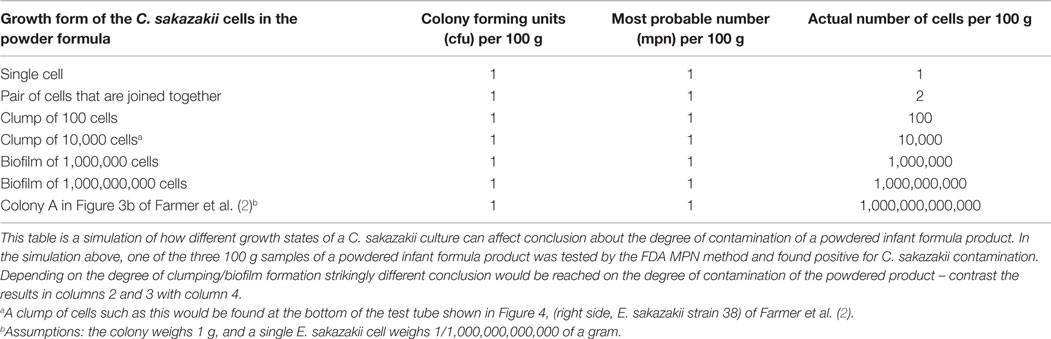
Table 2. Correlation between the number of Cronobacter sakazakii cells and colony forming units; must probable number values in a 100-g sample of a powdered formula product.
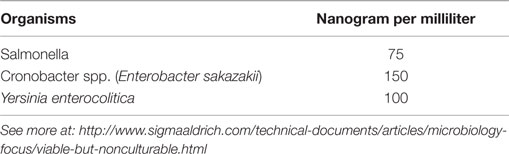
Table 3. Recommended end concentration of Ferrioxamine E.
Table 4 lists a few ways to “revive” Cronobacter and other bacteria from the non-culturable state to the culturable state.
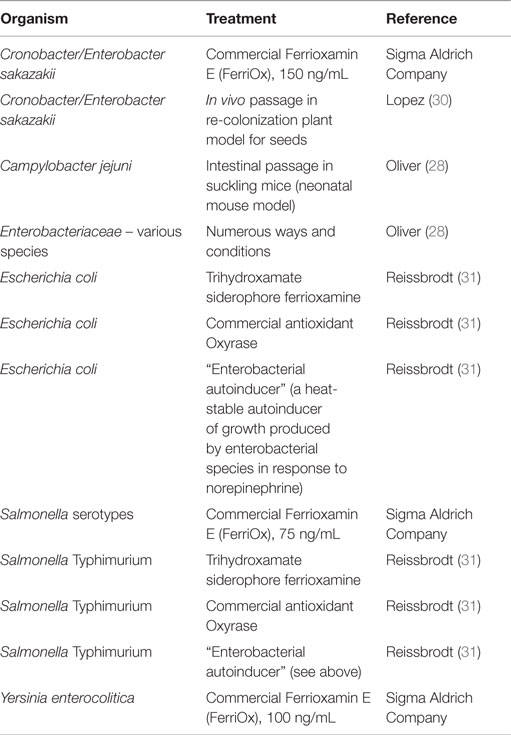
Table 4. Commercial and non-commercial treatments and reagents that have been used to change Cronobacter/E. sakazakii and other Enterobacteriaceae from the viable but non-culturable state to the culturable state.
The existence of Cronobacter strains in the “viable but non-culturable state” is a possible explanation for why a sample of powdered infant formula or other product can be tested and found “negative for Cronobacter contamination” but is actually contaminated with Cronobacter. This explanation would be that the lack of a sensitive testing method resulted in a false negative test result.
However, further studies are needed to provide a definitive answer to the above question. If Cronobacter strains can go from a “viable and culturable state” to a “viable but non-culturable state” work is needed to establish “frequency of occurrence” in different types of environments, particularly in the production of powdered infant formula products. It is essential for companies that produce these products to evaluate their procedures and final product for Cronobacter contaminants that are in the viable but non-culturable state. I have seen no evidence that powdered infant formula manufacturers have set this up as a general microbiological procedure or have done a specific evaluation in its causation analysis of a specific case of Cronobacter meningitis. These should be done as safety procedure.
The reader is urged to follow the development of this topic with frequent literature and internet searches.
Facts: Many different methods have been used to isolate and identify Cronobacter. Some isolation methods are good, but others give false negatives for the presence of Cronobacter. Each isolation method has its advantages and disadvantaged, and there is an extensive literature describing them. Many different methods have been used to identify Cronobacter. Some are good, but others give incorrect identifications. Each identification method has its advantages and disadvantaged, and there is an extensive literature describing them.
Facts: Not all strains identified as Cronobacter are really Cronobacter. Similarly, not all strains identified as, or referred to, as Enterobacter sakazakii are really Enterobacter sakazakii. These incorrect identifications are causing confusion in the literature.
Fact. The MPN method is a microbiological culturing method and is frequently used to determine the degree of Cronobacter contamination in a sample of powdered infant formula and in other foods. When the MPN method is used, the resulting report states the degree of contamination in terms of MPN per gram of the sample, or MPN per 10 g and/or MPN per 100 grams.
Myth: In the MPN method for Cronobacter, one colony forming unit (CFU) represents one viable cell of the Cronobacter contaminant. “Total viable counts” are often done by the MPN microbiological assay to determine contamination levels. This assay assumes that a positive result (positive tube) results from one cell of the contaminating bacterium. However, strains of Cronobacter can form large masses of adherent cells and can also form biofilms. Thus, a positive tube in the MPN assay may not have been caused by a single cell. This is illustrated in Table 2.
Myth: Two strains of Cronobacter that have the same PFGE pattern are the “same strain in a genetic/epidemiological sense.”
Myth: Two strains of Cronobacter that have different PFGE patterns cannot be the “same strain in a genetic/epidemiological sense.”
The reason for the two myths above is that there are too many variable in the PFGE laboratory technique to make precise statements such as these.
Fact: There are many good methods to preserve strains of Cronobacter once they have been isolated and identified.
Recommendation: Investigators should permanently preserve each Cronobacter strain that isolate and identify in order to allow for future study.
Unfortunately, investigators often destroy or discard strains of Cronobacter that they have so carefully isolated, identified and studied. An employee of the powdered infant formula industry stated that in his opinion it is not useful to preserve Cronobacter strains isolated from powdered infant formula, raw ingredients or from the factory environment. Perhaps he was thinking in terms of possible legal liability rather than in terms of helping an investigation of the causal role of the powdered formula in a case of neonatal meningitis following ingestion of powdered formula made in his production facility.
Fact: Cronobacter is a cause of neonatal meningitis. This is a well-documented fact. Cronobacter is also a well-known cause of hospital outbreaks and sporadic cases both in the home and hospital.
Myth: Cronobacter causes diarrhea and necrotizing enterocolitis (NEC). It is true that Cronobacter has been isolated from cases of diarrhea and necrotizing enterocolitis. There is an important adage “association does not prove causation,” and this is true for these two human illnesses. Additional studies are needed based on well-established causation criteria.
Recommendation: Use the wording “Cronobacter has an association with diarrhea and necrotizing enterocolitis rather than “Cronobacter causes diarrhea and necrotizing enterocolitis.”
Myth: Cronobacter causes a wide variety of other human infections.
Recommendations: I would reword this to: “Cronobacter has been isolated from a wide variety of other human infections, but in the vast majority of these it was not proven that the organism was actually causing an infection.” This is the “infection vs. colonization” problem. Investigators should use serodiagnostic testing to determine if the case had an antibody response to the Cronobacter strain that was isolated.
Myth: The incubation period for human neonatal meningitis caused by Cronobacter is 3–4 days. It is true that in outbreak investigations symptoms developed as soon as 3–4 days after the initial ingestion of the implicated formula product. However, because of the many variables involved this observation does not prove, or even imply, that the incubation period was 3–4 days for the cases studied.
Recommendation: I would use this wording: “The incubation period for human neonatal meningitis caused by Cronobacter is unknown. Because of technical difficulties it will be very hard to determine the range and average incubation period.”
Facts: The infectious dose is unknown for human neonatal meningitis caused by Cronobacter. The infectious dose and incubation period are also unknown for all other infections caused by Cronobacter.
Questions: What does it mean when a Cronobacter strain is isolated from a sink drain in the home of an infant who has been diagnosed with Cronobacter meningitis and the Cronobacter strain found in the sink drain is a “molecular match” to the strain isolated from the infant? Does this prove or imply that the home environment is the source/cause of the infant’s Cronobacter meningitis? No, there are several possible explanations. The following is taken from public documents in an actual legal case which is based on investigations by government agencies including CDC:
There are several possible explanations for the origin of the E. sakazakii strain in the left sink drain at the house where the infant lived:
(1) The strain was present in one of the implicated batches of powdered formula made by company A, and it was in a “viable and culturable” state. The unused formula was poured into the sink. This may have occurred as early as October 29 or 30, the date the mother first fed the infant formula made from powder. One or more E. sakazakii cells in the discarded liquid adhered to the sink drain, probably adhering to a biofilm that was already present the drain. The E. sakazakii strain from the formula then colonized the sink drain, probably as a stable biofilm. The sink drain was later tested by CDC and the strain of E. sakazakii was isolated.
(2) The facts are the same as in number 1 above except E. sakazakii in the formula was in a “viable and non-culturable.” The favorable environment of the sink allowed E. sakazakii to be “revived” and transformed into a “viable and culturable” state. It was later isolated and identified at CDC.
(3) The facts are the same as in number 1 above except E. sakazakii was in the feces of the infant in the days before his E. sakazakii infection began, i.e., he had intestinal colonization with E. sakazakii. It was then transferred to the sink/sink drain by one of many possible mechanisms. One mechanism would be the hands of someone who came in contact with his feces and then used the sink.
(4) Something or someone introduced the E. sakazakii into the sink. From the sink drain it may have been transferred to the infant in some way and then caused his infection. This explanation was given by one or more defense experts.
Fact: Not all species/strains of Cronobacter have the same pathogenic potential. This was emphasized in the previous discussion about the importance of Cronobacter sakazakii sequence type 4 (C. sakazakii ST 4) in neonatal meningitis.
Fact: There are no known animal infectious diseases caused by Cronobacter. Strains of Cronobacter have been isolated for animals, but these have been in the absence a naturally occurring disease process.
Fact: Animal models such as the neonatal rat model have been used to study the infectious process and possible virulence factors of Cronobacter.
Myth: Results from animal models accurately predict and can be extrapolated to the human disease processes to quantify items such as infectious dose and incubation period. Although animal models have been helpful in the absence of human data they have many limitations, and the results should be viewed with caution (29).
Fact or myth?: Cronobacter is widely distributed in the environment. This is myth or a fact depending on the definition of “widely distributed.” A safe way to avoid making this an unanswerable question is to stick to the facts and use precise and accurate wording, i.e., write precisely sentences and include references:
Strains of Cronobacter sakazakii have been isolated from the following sources: … (References).
Strains of Cronobacter sakazakii sequence type 4 have been isolated from the following sources: … (References).
Strains of Cronobacter condomentii have been isolated from the following sources: … (References).
Facts: The powdered infant formula industry and the IFC have played an important role in the current status of powdered infant formula in the United States in the following areas: manufacture, marketing, labeling, warnings, and instructions for preparation and use. They have influenced these in many different ways. However, it is beyond the scope of this paper to discuss these in detail. Several were discussed previously and additional one are listed in Tables 5 and 6.
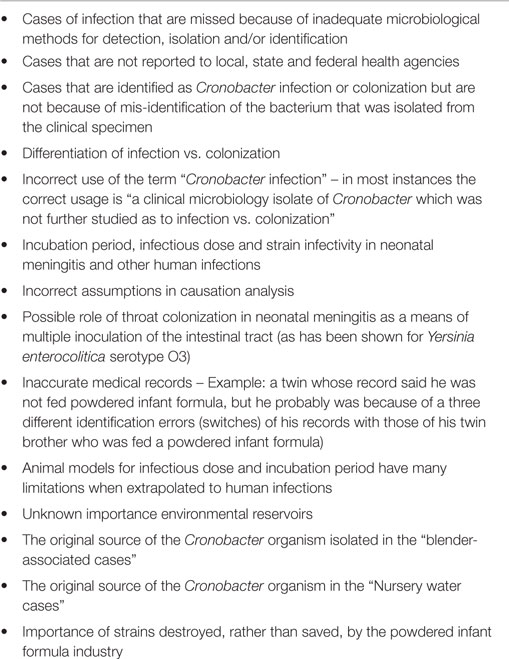
Table 5. Uncertainties associated with assessing the public health risk from Cronobacter.
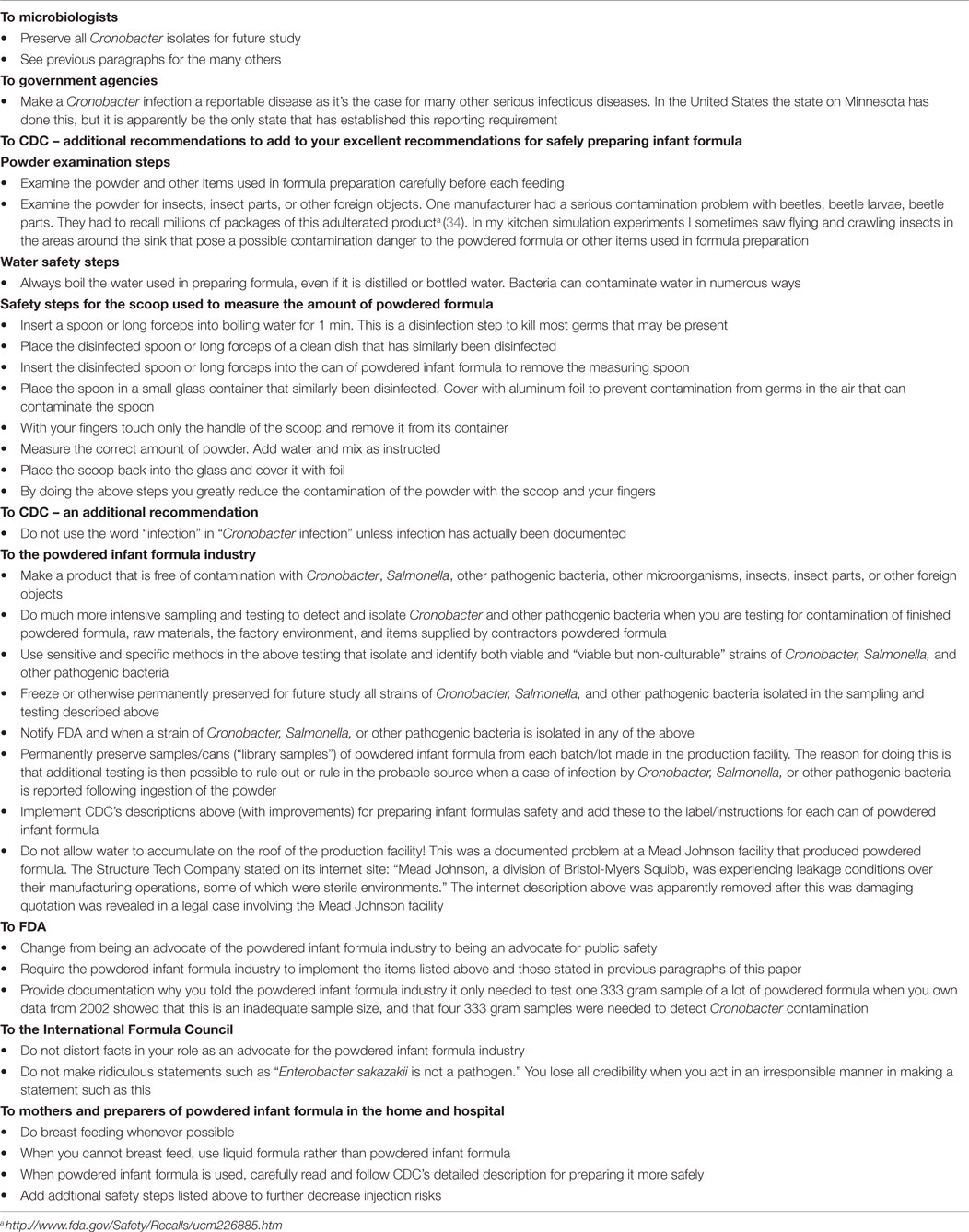
Table 6. Recommendations based on everything I have learned about Cronobacter over the last 40 years.
Myth: Manufacturer’s instructions for preparing powdered infant formula are complete and definitive in telling preparers how to avoid risks of infection by Cronobacter and other pathogens. There is there no universal standard or wording that commercial manufacturers of powdered infant formula are required to follow in this regard. The powdered infant formula industry and FDA have done a very poor job in providing complete information and instructions. Fortunately, CDC has taken the lead and has provided complete and specific instruction for preparing powdered infant formula which should greatly reduce the risk of Cronobacter infection and infection with other organisms. See: CDC’s information “Cronobacter Illness and Infant Formula” found at: http://www.cdc.gov/Features/Cronobacter/ and “Cronobacter Illness and Infant Formula” found at: http://www.cdc.gov/cronobacter/.
Recommendations: Based on published and unpublished information and on my personal experiences I have several recommendations for CDC to improve their excellent instructions/advice to reduce infection risks during preparation of powdered infant formula. These are listed in Table 6.
The REFERENCE section below is a recommended starting point to learn more about Cronobacter. The key point to remember is that beginning in 2007 there was a transition in the usage of names from Enterobacter sakazakii to Cronobacter. For this reason, a literature search should use the following terms to capture all of the possibilities: “yellow-pigmented Enterobacter cloacae” “Enterobacter sakazakii” “E. sakazakii” “Cronobacter sakazakii” “C. sakazakii” “sakazakii” and “Cronobacter.” A very simple alternative is to use just two terms: “sakazakii” and “Cronobacter,” which I have found is very effective. Several papers are highly recommended (32, 33, 35–42).
This paper expands on many of the topics and ideas in my Keynote Lecture “Cronobacter (Enterobacter) sakazakii – Reflections on the First 50 Years; Challenges and Unresolved Issues for the Next 50,” that I presented at the 1st International Conference on Cronobacter (Enterobacter sakazakii), Dublin, Ireland, January 22, 2009 (43).
The author declares that for over 10 years he has done expert witness work in legal cases that involved infants and babies who had ingested powdered formula products; became infected with Cronobacter/E. sakazakii; and suffered debilitating injury or death. This work included one or more of the following: detailed causation analysis, review of documents and procedures of the implicated manufacturer of the powdered formula product, written and oral reports, and testimony at deposition and trial. He was retained and received monetary compensation for this work regardless of the opinions and conclusions of his detailed causation analysis. Payments were from plaintiff attorney who represented the infant/baby who had suffered debilitating injury or death. The defendants in these cases were three U. S. manufacturers of the powdered formula product/products that were ingested by the injured infant or baby. Public records and non-sealed court documents describe some of the work/testimony described above. However, some work/testimony was “sealed by an order of the court,” or was covered by a “protective order” that I signed at the beginning of the cases. Thus, some of the above has been shielded from public view as a matter of law.
1. Forsythe SJ. Myths and legends of Cronobacter: a new bacterial pathogen of babies? Microbiol (2012) 1:30–3.
2. Farmer JJ, III, Asbury MA, Hickman FW, Brenner DJ, and the Enterobacteriaceae Study Group. Enterobacter sakazakii: a new species of “Enterobacteriaceae” isolated from clinical specimens. Int J Syst Bacteriol (1980) 30:569–84. doi: 10.1099/00207713-30-3-569
3. Pangalos G. Sur un bacille chromogène isolé par hémoculture. C R Soc Biol [Comptes Rendus Seances Soc Biol] (1929) 100:1097–8.
4. Joseph S, Forsythe SJ. Predominance of Cronobacter sakazakii sequence type 4 in neonatal infections. Emerg Infect Dis (2011) 17(9):1713–5. doi:10.3201/eid1709.110260
5. Joseph S, Desai P, Ji Y, Cummings CA, Shih R, Degoricija L, et al. Comparative analysis of genome sequences covering the seven Cronobacter species. PLoS One (2012) 7(11):e49455. doi:10.1371/journal.pone.0049455
6. Urmenyi AMC, White-Franklin AW. Neonatal death from pigmented coliform infection. Lancet (1961) 1:313–5. doi:10.1016/S0140-6736(61)91481-7
7. Jøker RN, Nørholm T, Siboni KE. A case of neonatal meningitis caused by a yellow Enterobacter. Dan Med Bull (1965) 12:128–30.
8. Brenner DJ. DNA reassociation for the clinical differentiation of enteric bacteria. Public Health Lab (1974) 32:118–30.
9. Steigerwalt AG, Fanning GR, Fife-Asbury MA, Brenner DJ. DNA relatedness among species of Enterobacter and Serratia. Can J Microbiol (1976) 22:121–37. doi:10.1139/m76-018
10. Brenner DJ, Farmer JJ III, Hickman FW, Asbury MA, Steigerwalt AG. Taxonomic and Nomenclatural Changes in Enterobacteriaceae. HEW Publication No. [CDC] 79-8356. Atlanta, GA: Center for Disease Control (1977).
11. Iversen C, Lehner A, Mullane N, Bidlas E, Cleenwerck I, Marugg J, et al. The taxonomy of Enterobacter sakazakii: proposal of a new genus Cronobacter gen. nov. and descriptions of Cronobacter sakazakii comb. nov. Cronobacter sakazakii subsp. sakazakii, comb. nov., Cronobacter sakazakii subsp. malonaticus subsp. nov., Cronobacter turicensis sp. nov., Cronobacter muytjensii sp. nov., Cronobacter dublinensis sp. nov. and Cronobacter genomospecies 1. BMC Evol Biol (2007) 7:64. doi:10.1186/1471-2148-7-64
12. Muytjens HL, Zanen HC, Sonderkamp HJ, Kollee LA, Wachsmuth IK, Farmer JJ III. Analysis of eight cases of neonatal meningitis and sepsis due to Enterobacter sakazakii. J Clin Microbiol (1983) 18:115–20.
13. Muytjens HL, Roelofs-Willemse H, Jaspar GH. Quality of powdered substitutes for breast milk with regard to members of the family Enterobacteriaceae. J Clin Microbiol (1988) 26:743–6.
14. Muytjens HL, Kollée LA. Enterobacter sakazakii in neonates: causative role of formula? Pediatr Infect Dis J (1990) 9:372–3. doi:10.1097/00006454-199005000-00016
15. Simmons BP, Gelfand MS, Haas M, Metts L, Ferguson J. Enterobacter sakazakii infections in neonates associated with intrinsic contamination of a powdered infant formula. Infect Control Hosp Epidemiol (1989) 10(9):398–401. doi:10.2307/30144207
16. FDA. U. S. Food and Drug Administration. Health Professionals Letter on Enterobacter sakazakii Infections Associated with Use of Powdered (Dry) Infant Formulas in Neonatal Intensive Care Units. Silver Spring, MD: U.S. Food and Drug Administration (2002).
17. FDA. U. S. Food and Drug Administration. “Inspection, Collection and to Analysis of Powdered Infant Formula for Enterobacter sakazakii (E. sakazakii)” – High Priority. (2002). (DOEP #02-18 – FACTS #33044”).
18. Zink D. FDA Field Survey of Powdered Formula Manufacturing, U. S. Food and Drug Administration, Food Advisory Committee, Meeting. (2003). Available from: http://www.fda.gov/ohrms/dockets/ac/03/slides/3939s1.htm
19. FDA. U. S. Food and Drug Administration. Food Advisory Committee, Meeting March 18-19, 2003. (2003). Available from: http://www.fda.gov/ohrms/dockets/ac/03/slides/3939s1.htm
20. World Health Organization (WHO) and Food and Agriculture Organization of the United Nations (FAO). Enterobacter sakazakii and Other Microorganisms in Powdered Infant Formula. Meeting Report, Microbiology Risk Assessment Series, Number 6. Geneva: World Health Organization (2004). 59 p. Available from: http://www.fao.org/3/a-y5502e.pdf
21. World Health Organization (WHO) and Food and Agriculture Organization of the United Nations (FAO). Enterobacter sakazakii and Salmonella in Powdered Infant Formula. Meeting Report, Microbiology Risk Assessment Series, Number 10. Geneva: World Health Organization (2006). 95 p. Available from: http://apps.who.int/iris/bitstream/10665/43547/1/9241563311_eng.pdf?ua=1
22. World Health Organization (WHO) and Food and Agriculture Organization of the United Nations (FAO). Enterobacter sakazakii (Cronobacter spp.) in Powdered Follow-up Formula. Meeting Report, Microbiology Risk Assessment Series, Number 15. Geneva: World Health Organization (2008). 86 p. Available from: http://www.who.int/foodsafety/publications/micro/MRA_followup.pdf
23. Farmer JJ III. Enterobacter sakazakii – Personal perspectives and reminiscences from a 32-year history. Chapter 10. In: Farber JM, Forsythe SJ, editors. Enterobacter sakazakii. Washington, DC: ASM Press (2008). p. 255–64.
24. Farber JM, Forsyth SJ, editors. Enterobacter sakazakii. Washington, DC: ASM Press (2008). 271 p.
25. Iversen C, Mullane N, McCardell B, Tall BD, Lehner A, Fanning S, et al. Cronobacter gen. nov., a new genus to accommodate the biogroups of Enterobacter sakazakii, and proposal of Cronobacter sakazakii gen. nov., comb. nov., Cronobacter malonaticus sp. nov., Cronobacter turicensis sp. nov., Cronobacter muytjensii sp. nov., Cronobacter dublinensis sp. nov., Cronobacter genomospecies 1, and of three subspecies, Cronobacter dublinensis subsp. dublinensis subsp. nov., Cronobacter dublinensis subsp. lausannensis subsp. nov. and Cronobacter dublinensis subsp. lactaridi subsp. nov. Int J Syst Evol Microbiol (2008) 58:1442–47. doi:10.1099/ijs.0.65577-0
26. Brady C, Cleenwerck I, Venter S, Coutinho T, De Vos P. Taxonomic evaluation of the genus Enterobacter based on multilocus sequence analysis (MLSA): proposal to reclassify E. nimipressuralis and E. amnigenus into Lelliottia gen. nov. as Lelliottia nimipressuralis comb. nov. and Lelliottia amnigena comb. nov., respectively, E. gergoviae and E. pyrinus into Pluralibacter gen. nov. as Pluralibacter gergoviae comb. nov. and Pluralibacter pyrinus comb. nov., respectively, E. cowanii, E. radicincitans, E. oryzae and E. arachidis into Kosakonia gen. nov. as Kosakonia cowanii comb. nov., Kosakonia radicincitans comb. nov., Kosakonia oryzae comb. nov. and Kosakonia arachidis comb. nov., respectively, and E. turicensis, E. helveticus and E. pulveris into Cronobacter as Cronobacter zurichensis nom. nov., Cronobacter helveticus comb. nov. and Cronobacter pulveris comb. nov., respectively, and emended description of the genera Enterobacter and Cronobacter. Syst Appl Microbiol (2013) 36:309–19.
27. Farmer JJ III, Boatwright KD, Janda JM. Enterobacteriaceae: Introduction and Identification, chapter 42. 9th ed. In: Murray PR, Baron EJ, Jorgensen JH, Landry ML, Pfaller MA, editors. Manual of Clinical Microbiology. Washington, DC: American Society for Microbiology (2007). p. 649–69.
28. Oliver JD. Recent findings on the viable but non-culturable state in pathogenic bacteria. FEMS Microbiol Rev (2009) 34:415–25. doi:10.1111/j.1574-6976.2009.00200.x
29. Farmer JJ III, Potter ME, Riley LW, Barrett TJ, Blake PA, Bopp CA, et al. Animal models to study Escherichia coli O157:H7 isolated from patients with haemorrhagic colitis. Lancet (1983) 1:702–703.
30. Lopez BR, Bashan Y, Bacilio M. Endophytic bacteria of Mammillaria fraileana, an endemic rock-colonizing cactus of the southern Sonoran Desert. Arch Microbiol (2011) 193:527–41. doi:10.1007/s00203-011-0695-8
31. Reissbrodt R, Rienaecker I, Romanova JM, Freestone PPE, Haigh RD, Lyte M, et al. Resuscitation of Salmonella enterica serovar Typhimurium and enterohemorrhagic Escherichia coli from the viable but nonculturable state by heat-stable enterobacterial autoinducer. Appl Environ Microbiol (2002) 68:4788–94. doi:10.1128/AEM.68.10.4788-4794.2002
32. Besse NG, Leclercq A, Maladen V, Tyburski C, Lombard B. Evaluation of the international organization for standardization-international dairy federation (ISO-IDF) draft standard method for detection of Enterobacter sakazakii in powdered infant food formulas. J AOAC Int (2006) 89(5):1309–16.
33. Bowen AB, Braden CR. Invasive Enterobacter sakazakii disease in infants. Emerg Infect Dis (2006) 12:1185–9. doi:10.3201/eid1208.051509
34. FDA. U. S. Food and Drug Administration. FDA Alerts Public Regarding Recall of Powdered Infant Formula. Georgia, VT: News Release P02-46 (2002). (29 different Wyeth products manufactured).
35. Chen Y, Lampel K, Hammack T. Cronobacter. In: Bacteriological Analytical Manual. Silver Spring, MD: U.S. Food and Drug Administration (2012). Chapter 29. Available from: http://www.fda.gov/Food/FoodScienceResearch/LaboratoryMethods/ucm289378.htm
36. Gurtler JB, Kornacki JL, Beuchat LR. Enterobacter sakazakii: a coliform of increased concern to infant health. Int J Food Microbiol (2005) 104:1–34. doi:10.1016/j.ijfoodmicro.2005.02.013
37. Himelright I, Harris E, Lorch V, Anderson M, Kuehnert M, Forster T, et al. Enterobacter sakazakii infections associated with the use of powdered infant formula – Tennessee, 2001. MMWR Morb Mortal Wkly Rep. (2002) 51:297–300.
39. Jason J. Prevention of invasive Cronobacter infections in young infants fed powdered infant formulas. Pediatrics (2012) 130(5):SI1–6. doi:10.1542/peds.2011-3855
40. Jones DM, Sutcliffe EM, Curry A. Recovery of viable but non-culturable Campylobacter jejuni. J Gen Microbiol (1991) 137:2477–82. doi:10.1099/00221287-137-10-2477
41. Năşcuţiu AM. Viable non-culturable bacteria. Bacteriol Virusol Parazitol Epidemiol (2010) 55:11–8 [Article in Romanian].
42. Patrick ME, Mahon BE, Greene SA, Rounds J, Cronquist A, Wymore K, et al. Incidence of Cronobacter spp. infections, United States, 2003-2009. Emerg Infect Dis (2014) 20(9):1520–3. doi:10.3201/eid2009.140545
Keywords: Cronobacter, Enterobacter sakazakii, powdered infant formula, safety, neonatal meningitis, risk assessment, government regulations, recommendations
Citation: Farmer JJ III (2015) My 40-year history with Cronobacter/Enterobacter sakazakii – lessons learned, myths debunked, and recommendations. Front. Pediatr. 3:84. doi: 10.3389/fped.2015.00084
Received: 22 April 2015; Accepted: 22 September 2015;
Published: 27 November 2015
Edited by:
Janine Jason, Jason and Jarvis Associates, LLC, USAReviewed by:
Masaaki Murakami, Hokkaido University, JapanCopyright: © 2015 Farmer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: John J. Farmer III, Silver Hill Associates, 1781 Silver Hill Road, Stone Mountain, GA 30087, USA, amltZmFybWVyODEyQGVhcnRobGluay5uZXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.