
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Parasitol. , 05 September 2023
Sec. Parasite Diagnostics
Volume 2 - 2023 | https://doi.org/10.3389/fpara.2023.1235925
This article is part of the Research Topic Polymerase Chain Reaction technique for Chagas Disease: challenges and limitations View all 6 articles
 Carlos Henrique Valente Moreira1,2
Carlos Henrique Valente Moreira1,2 Ana Luiza Bierrenbach3Cesar Augusto Taconeli4
Ana Luiza Bierrenbach3Cesar Augusto Taconeli4 Léa Campos de Oliveira-da Silva5Lewis F. Buss5,6Sheila M. Keating7
Léa Campos de Oliveira-da Silva5Lewis F. Buss5,6Sheila M. Keating7 Erika Regina Manuli5,8,9Noemia Barbosa Carvalho9Cristina Guastini9Sonia Bakkour Coco10,11
Erika Regina Manuli5,8,9Noemia Barbosa Carvalho9Cristina Guastini9Sonia Bakkour Coco10,11 José Ângelo Lauletta Lindoso1,8
José Ângelo Lauletta Lindoso1,8 Lucas Augusto Moyses Franco5,8Fabio Ghilardi5Flavia Cristina da Silva Sales5,8Paul Contestable12Clara Di Germanio10Michael P. Busch10,13†
Lucas Augusto Moyses Franco5,8Fabio Ghilardi5Flavia Cristina da Silva Sales5,8Paul Contestable12Clara Di Germanio10Michael P. Busch10,13† Ester Cerdeira Sabino5,8*†
Ester Cerdeira Sabino5,8*†Background: Evaluating the effectiveness of Chagas disease treatment poses challenges due to the lack of biomarkers for disease progression and therapeutic response. In this study, we aimed to assess the clearance of Trypanosoma cruzi (T. cruzi) parasites in a group of benznidazole (BNZ)-treated chronic Chagas disease patients using high-sensitivity quantitative PCR (qPCR) and track T. cruzi antibody levels through a semiquantitative chemiluminescent assay.
Methods: A total of 102 T. cruzi seropositive patients with previous PCR-positive results were enrolled in the study. We collected samples 30 days before treatment (T-30d), on the day before initiating BNZ treatment (T0d), and at follow-up visits 60 days (T60d), 6 months (T6M), 12 months (T12M), and 36 months (T36M) after treatment initiation. Treatment efficacy was assessed by testing of serial samples using a target-capture qPCR assay specific to satellite T. cruzi DNA and the ORTHO T. cruzi ELISA Test System for antibody quantitation.
Results: Of the enrolled individuals, 87 completed at least 50% of the treatment course, and 86 had PCR results at follow-up visits T6M, T12M, and T36M. PCR results exhibited fluctuations before and after treatment, but levels were significantly lower post-treatment. Only 15 cases consistently tested PCR-negative across all post-treatment visits. Notably, nearly all participants demonstrated a declining antibody trajectory, with patients who tested PCR-negative at T36M exhibiting an earlier and more pronounced decline compared to PCR-positive cases at the same visit.
Conclusion: Our study suggests that serial PCR results pose challenges in interpretation. In contrast, serial antibody levels may serve as an ancillary, or even a more reliable indicator of parasite decline following BNZ treatment. Monitoring antibody levels can provide valuable insights into the efficacy of treatment and the persistence of parasites in Chagas disease patients.
More than 100 years after its discovery (Chagas, 1909), Chagas disease remains a major public health problem in South and Central America. Despite effective vector control, there are still hotspots of endemicity in countries such as Brazil, where one million people are estimated to be living with Trypanosoma cruzi (T. cruzi) infection (Brazilian Ministry of Health, 2022). Furthermore, due to human migration, around 400,000 people infected with T. cruzi live in non-endemic countries (Pinazo et al., 2011; Requena-Méndez et al., 2015). For most patients, T. cruzi infection is generally lifelong, and end-organ damage, such as progression to cardiac damage and other clinically significant sequelae, may occur over decades (Sabino et al., 2013). Therefore, millions of infected individuals could benefit from parasiticidal treatment to decrease this evolving process (Cardoso et al., 2018; Hasslocher-Moreno et al., 2021).
Benznidazole (BNZ) is the primary treatment available for Chagas disease worldwide. The evidence base supporting treatment with BNZ comes primarily from retrospective observational studies that have documented a reduced rate of progression to cardiomyopathy and lower mortality in BNZ-treated patients (Cardoso et al., 2018; Hasslocher-Moreno et al., 2021).
Surrogate markers of therapeutic success are urgently needed to allow more reasonable evaluation of existing treatments and routine clinical follow-up of BNZ-treated patients and support novel drug discovery and drug repurposing (Molina et al., 2014; Torrico et al., 2018; Pandey et al., 2022; Torrico et al., 2022). As evidenced by persistently negative polymerase chain reaction (PCR) test results, long-term sterilizing parasite clearance has previously been suggested as a surrogate for treatment success (Sulleiro et al., 2020). However, parasitemia is low-level, near the detection limit in untreated and chronically infected individuals, and may fluctuate in the absence of treatment (Morillo et al., 2015; De Salazar et al., 2022).
Consequently, persistently or intermittently negative results may not indicate parasite clearance after treatment. The presence of chronic parasitemia is linked to levels of anti-T cruzi antibodies, which are associated with the occurrence of abnormal electrocardiogram (ECG) results, positive results in quantitative polymerase chain reaction (qPCR) tests, as well as an increased risk of developing cardiomyopathy and long-term mortality. These findings highlight the potential value of measuring antibody quantities as an indicator of persistent parasite presence (Buss et al., 2020).
We present the three-year follow-up results of a prospective cohort of BNZ-treated chronic Chagas disease patients. We aimed to characterize the parasite clearance rate using a high-sensitivity quantitative qPCR assay and describe the trajectory of anti-T. cruzi antibody levels throughout early treatment and long-term follow-up relative to parasite persistence by PCR as a marker of therapeutic response.
This is a prospective study, conducted from 2013 to 2015, of a cohort of chronic Chagas patients treated in outpatient services at two specialized centers in São Paulo, Brazil: Instituto de Infectologia “Emílio Ribas” and Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo. Patients were enrolled before and followed up for three years after BNZ treatment. All individuals were PCR-positive before the treatment (Figure 1), and most were followed for three years following treatment with longitudinal clinical assessments and characterization of persistence and levels of T. cruzi parasitemia and antibodies.
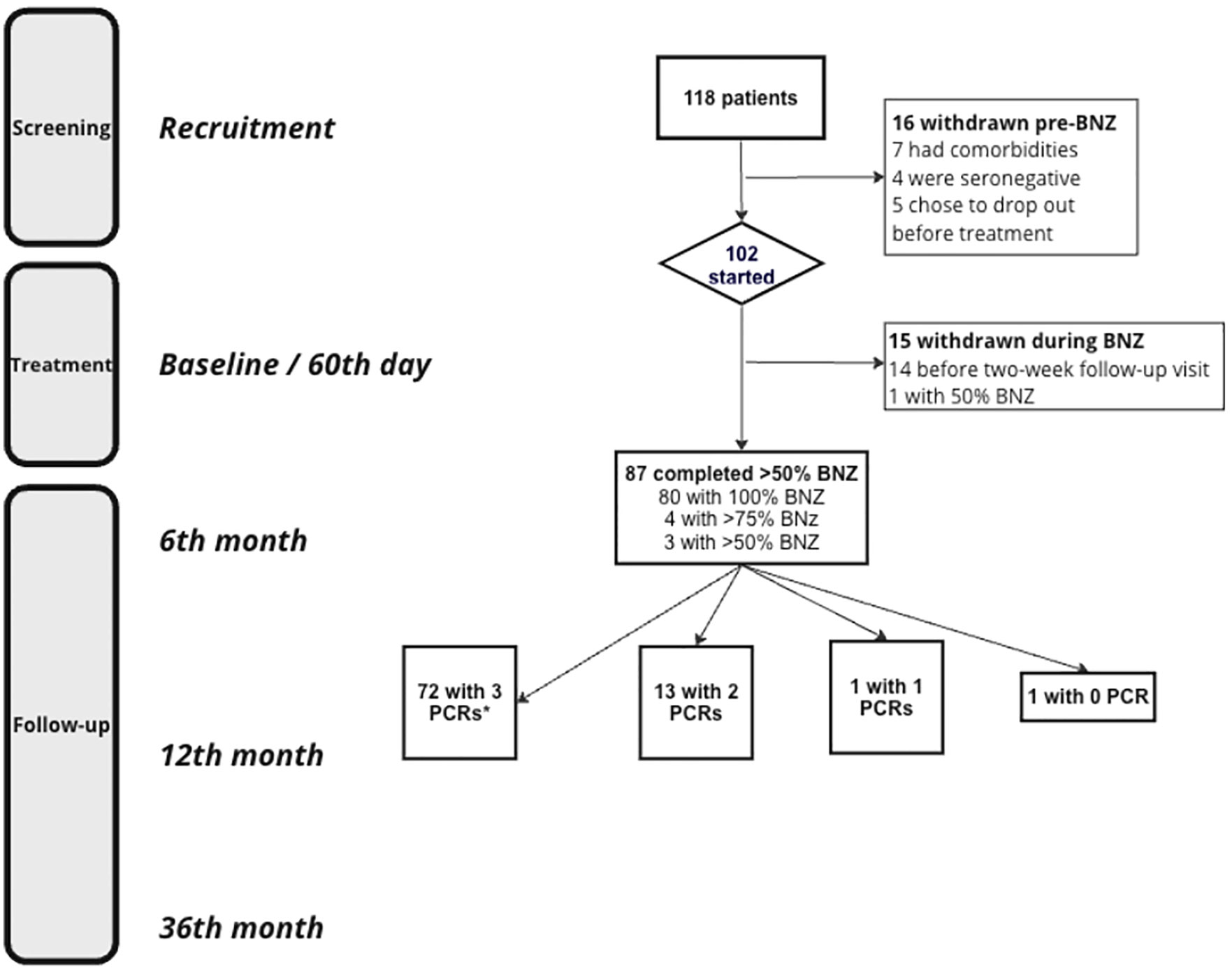
Figure 1 Study flowchart. *All follow-up PCRs are depicting those drawn after BZN treatment. BNZ, Benznidazole.
We enrolled 102 individuals aged between 18 and 65 diagnosed with chronic Chagas disease and previously tested PCR-positive for T. cruzi. At different stages of the disease, these patients, ranging from indeterminate to mild cardiac or digestive involvement, self-reported and had their physicians confirm any comorbidities. They were then treated with BNZ at a standard dose of 5 mg/kg/day orally, up to a maximum of 300mg/day, split into two or three daily doses over 60 days (Dias et al., 2016).
We collected medical data and blood samples at multiple intervals. The first round, 30 days prior to the BNZ treatment (T-30d), included a detailed medical history, physical examination, and blood tests for T. cruzi qPCR and antibody quantitation. Another round of data collection occurred on the day before treatment initiation (T0d). We then gathered follow-up data at 60 days (T60d), six months (T6M), twelve months (T12M), and thirty-six months (T36M) post-treatment initiation, using the same data collection procedures.
At the enrollment interview and follow-up visits, 12mL of blood anticoagulated with ethylenediaminetetraacetic acid (EDTA) was collected and immediately mixed with an equal volume of 6M guanidine/HCl-0.2M EDTA solution for PCR. These samples were boiled, aliquoted, and frozen at −20°C in Brazil. Serum separator tubes (SST) were also collected at each visit and centrifuged at 3000G for 15 min, and serum aliquots were frozen at -20°C. Aliquots of guanidine-lysed blood and serum were shipped to the US Central Laboratory (VRI; previously BSRI) for qPCR and serology, respectively.
The qPCR assay used in this study was developed based on a PCR method that targets satellite T. cruzi DNA (DNAsat) (Sabino et al., 2015). Four replicate qPCR assays were performed from each of two DNA-extracted aliquots in eight replicates. For each assay, 500uL of guanidine-lysed blood was processed for DNA extraction using a target-capture (TC) step that employed magnetic beads coated with a T.cruzi-specific 20-mer capture oligonucleotides (Sabino et al., 2015). A qPCR cycle threshold (CT) of 45 was used as the cut-off. For qualitative interpretation, results were considered positive if at least two of four replicates were positive. Quantifying parasitemia was based on a standard curve derived from cultured parasites spiked into whole blood samples before lysis, with a quantitation range of 0.1 to 10,000 parasites/mL (Sabino et al., 2015).
The serological test (ORTHO T. cruzi VITROS ELISA Test System) is based on a whole parasite lysate antigen ELISA (Buss et al., 2020). The test utilizes microwells coated with T. cruzi antigens as the solid phase with chemiluminescent detection. Results are reported as signal-to-cutoff (S/CO) ratios representing the relative amount of anti-T. cruzi antibody present in test samples. Testing was performed according to the manufacturer’s instructions (Buss et al., 2020).
Data from each patient were uploaded into REDCap (Research Electronic Data) (Harris et al., 2009; Harris et al., 2019), and results were then de-identified from specific patient-sensitive information.
We assessed changes in parasite loads measured through qPCR and serology levels by comparing the differences between the levels at multiple time points (T0d, T60d, T6M, T12M, and T36M) and the levels at T-30d. Our defined outcomes were as follows: “Negative” indicated a negative PCR result at T6M, T12M, and T36M; “Positive” indicated a positive result on the T36M visit, regardless of the earlier results; and “Inconclusive” referred to patterns that were negative on the T36M visit but had at least one PCR positive result at T6M or T12M visits. If the T6M or T12M PCR result was missing, we classified them as “Inconclusive”.
To analyze the data, we conducted a multinomial logistic regression with the Negative group as the reference, considering the age at study initiation and sex. We presented these outcomes graphically using a serial boxplot to show the trend across visits regarding the antibody levels between these groups.
To predict the likelihood of experiencing a “Non-Positive PCR outcome,” which includes the Negative and Inconclusive groups, we conducted a logistic regression with “Positive” as the reference category. The models were adjusted for the same variables as in the multinomial analysis. We presented the associations between predictor variables and the outcomes using odds ratios (OR) with 95% confidence intervals (CI 95%).
For qPCR and serology levels, we employed paired Wilcoxon rank-sum tests, paired t-tests, and Chi-squared tests with Bonferroni adjustment post-hoc for comparison across visits and the T0d visit. We used the Kruskal-Wallis test to analyze the differences in antibody levels across visit time points and outcomes for T. cruzi-infected patients treated with benznidazole. Continuous variables were reported as medians and interquartile ranges or mean and standard deviations based on their distribution, while categorical variables were reported as frequencies and percentages.
Our conclusions are based on a two-tailed hypothesis test with an alpha error probability of 0.05. We performed the statistical analysis and generated graphics using R Studio software (version 4.2) (RStudio, 2022).
This study protocol was approved by the local ethics committee of the Hospital of Clinics, University of São Paulo, and Institute of Infectology “Emilio Ribas” (CAAE00580612.8.0000.0065). All patients provided written informed consent at the time of recruitment.
From the total of 102 patients treated for Chagas disease, a subset of 87 patients who completed at least 50% of the BNZ treatments were considered for the initial analysis. A more detailed breakdown of this subset was further assessed for informative data: out of these 87 patients, 86 had both qPCR and antibody results available from their follow-up visits at six months (T6M), twelve months (T12M), and thirty-six months (T36M). These 86 patients were included in the final data analysis (Figure 1). The cohort was predominantly male (62%) with a median age of 53 years (interquartile range of 47 to 59 years). Among these patients, 34 (39.1%) were diagnosed with a mild cardiac form of Chagas disease (Table 1).
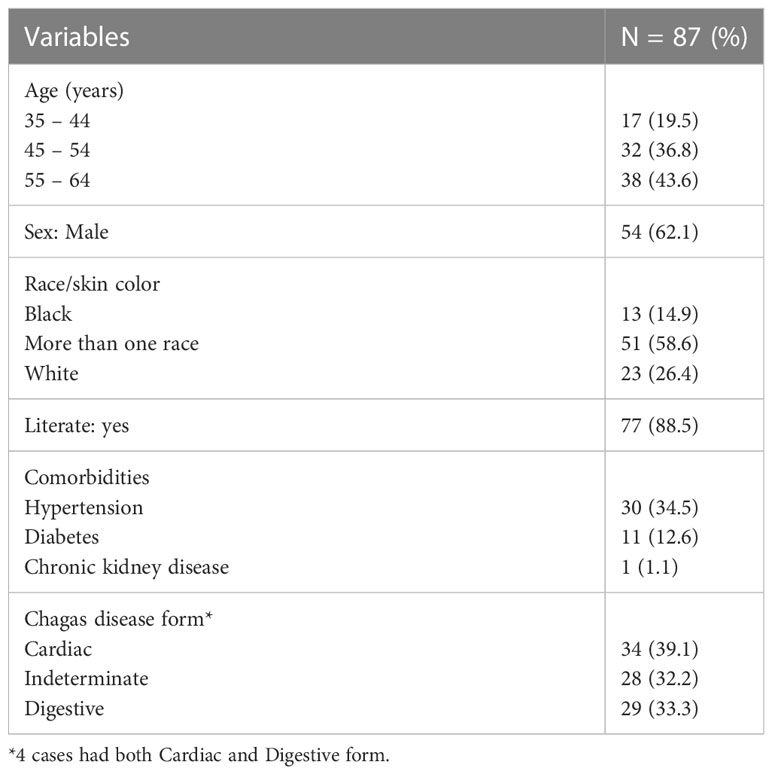
Table 1 Clinical characteristics of the subjects that completed at least 50% of the BZN course.
qPCR levels fluctuated during the two pre-treatment visits, with approximately 30% of the patients having parasitemia levels higher than one parasite equivalent/mL and 45% having PCR-negative results at one of these two visits on post-study batch testing at the Central Lab. Following treatment, the qPCR levels continued to fluctuate, particularly at T6M and T12M, but were significantly lower than pre-treatment levels and the T60d visits, as shown in Table 2. Our study found that qPCR levels showed a statistically significant decrease compared to baseline (T0d) measurements, starting from T60d in patients with a non-positive outcome. This significant decrease persisted over time. On the other hand, patients with a positive outcome experienced a statistically significant drop in qPCR levels only at their final follow-up visit (T36M) compared to their T0d levels. Only 15 patients had negative PCR results on all their ≥T6M post-treatment follow-up visits. The proportion of patients with PCR positivity across the follow-up visits varied, with a significant difference from the initial visit (T0d) at the T60d but not the T6M and T12M visits, and only regaining significance at the last visit (T36M). The fluctuation of the PCR results made it difficult to determine which patients had achieved parasite suppression. Interestingly, on the T36M visit, 90% of the patients had negative PCR results (Table 2; Figure 2).
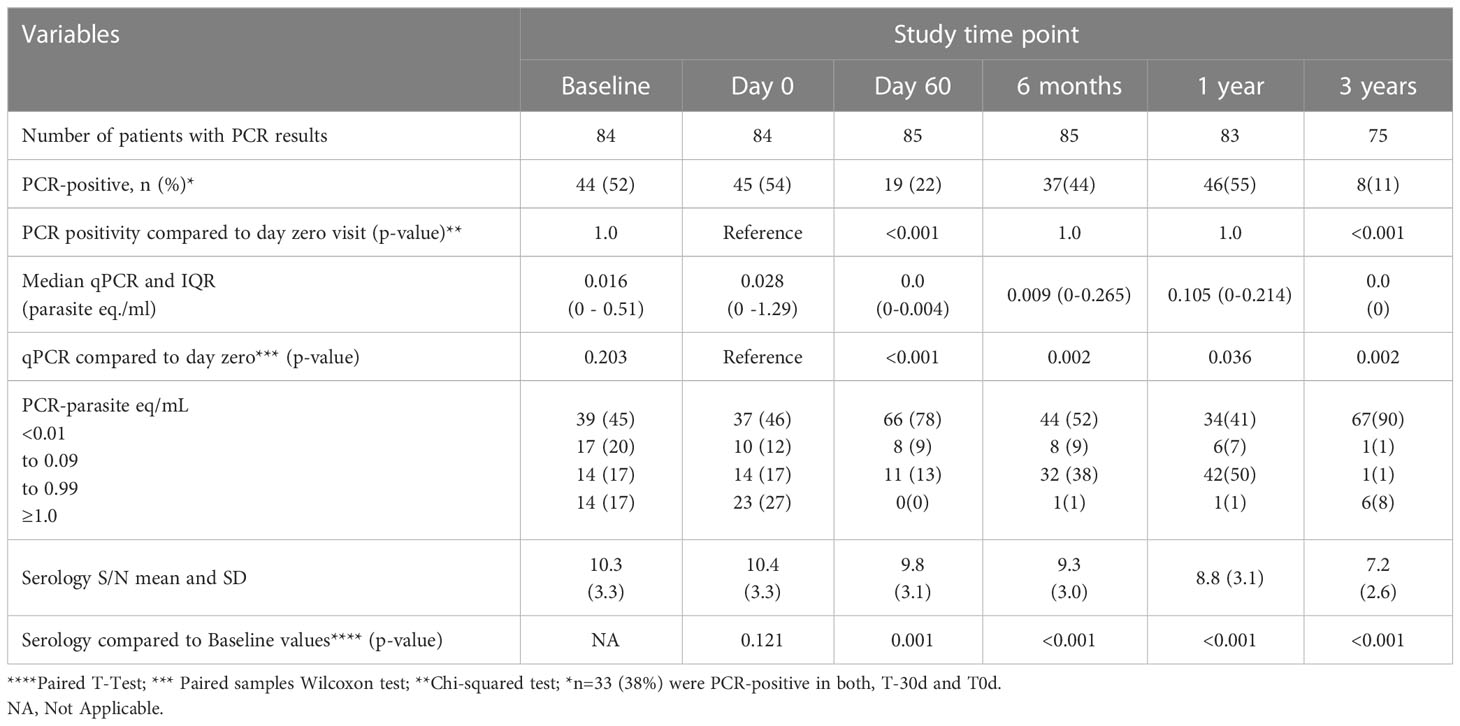
Table 2 PCR and serological results of Chagas patients completing at least 50% of the treatment course with benznidazole.

Figure 2 Dotplot representing individual Polymerase Chain Reaction (qPCR) measurements for 85 subjects treated with benznidazole, with at least three follow-up PCR measurements. The red dots represent the mean values, while the red bars indicate the 95% confidence interval around the mean. Note the different scales in the two segments of the y-axis.
Our multinomial logistic regression analysis revealed that the difference in antibody (Ab) levels after treatment, compared to baseline levels, could predict the odds of not belonging to the Positive outcome category. Specifically, at the T36M visit, a 1-unit decrease in Ab values was significantly associated with a reduced likelihood of being classified as part of the Positive outcome group relative to the Negative reference category. The odds decreased by a factor of 0.36, indicating that each unit decrease in Ab levels was associated with a 64% decrease in the likelihood of belonging to the Positive outcome category (Figure 3). Similar trends were observed at the T12M and T6M visits. At the T12M visit, a 1-unit decrease in Ab levels, compared to the T-30d visit, was associated with a 60% reduction in the odds of being classified as part of the Positive outcome group, compared to the Negative group. Similarly, at the T6M visit, a 1-unit decrease in Ab levels resulted in approximately a 51% decrease in the odds of being classified as part of the Positive outcome group. Interestingly, the drop in S/CO between T-30d and T60d is predictive of the outcome at the T36M visit. However, the CI95% was too large to rule out the possibility of no effect.
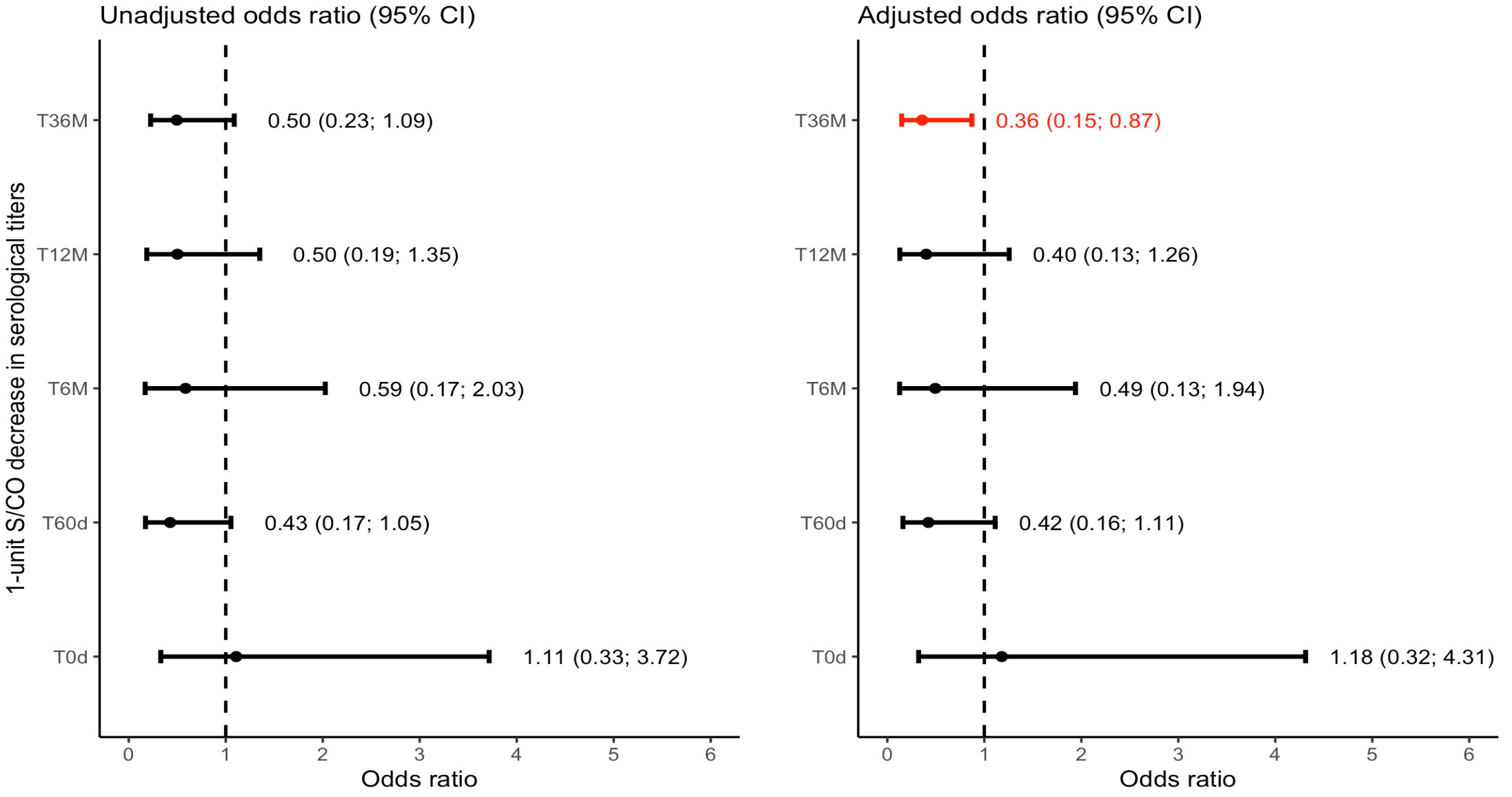
Figure 3 Forest plot depicting the Multinomial Logistic Odds Ratio for the positive outcome group with negative as the reference category. CI: Confidence Interval; S/CO: Signal-to-Cutoff.T0d: Time 0 day; on the day at benznidazole treatment initiation. T60d: Time 60 days; follow-up visit 60 days after initiating benznidazole treatment. T6M: Time 6 Months; follow-up visit 6 months after initiating benznidazole treatment; T12M: Time 12 Months; follow-up visit 12 months after initiating benznidazole treatment. T36M: Time 36 Months; follow-up visit 36 months after initiating benznidazole treatment.
Our study also investigated the association between qPCR results, antibody levels, and the probability of attaining a Non-Positive outcome comprising Negative or Inconclusive results. The results revealed a consistent trend of higher success rates in parasite suppression over time, with the likelihood more than doubling at the T36M visit compared to earlier time points among those presenting the reference category as “Positive” (Figure 4).
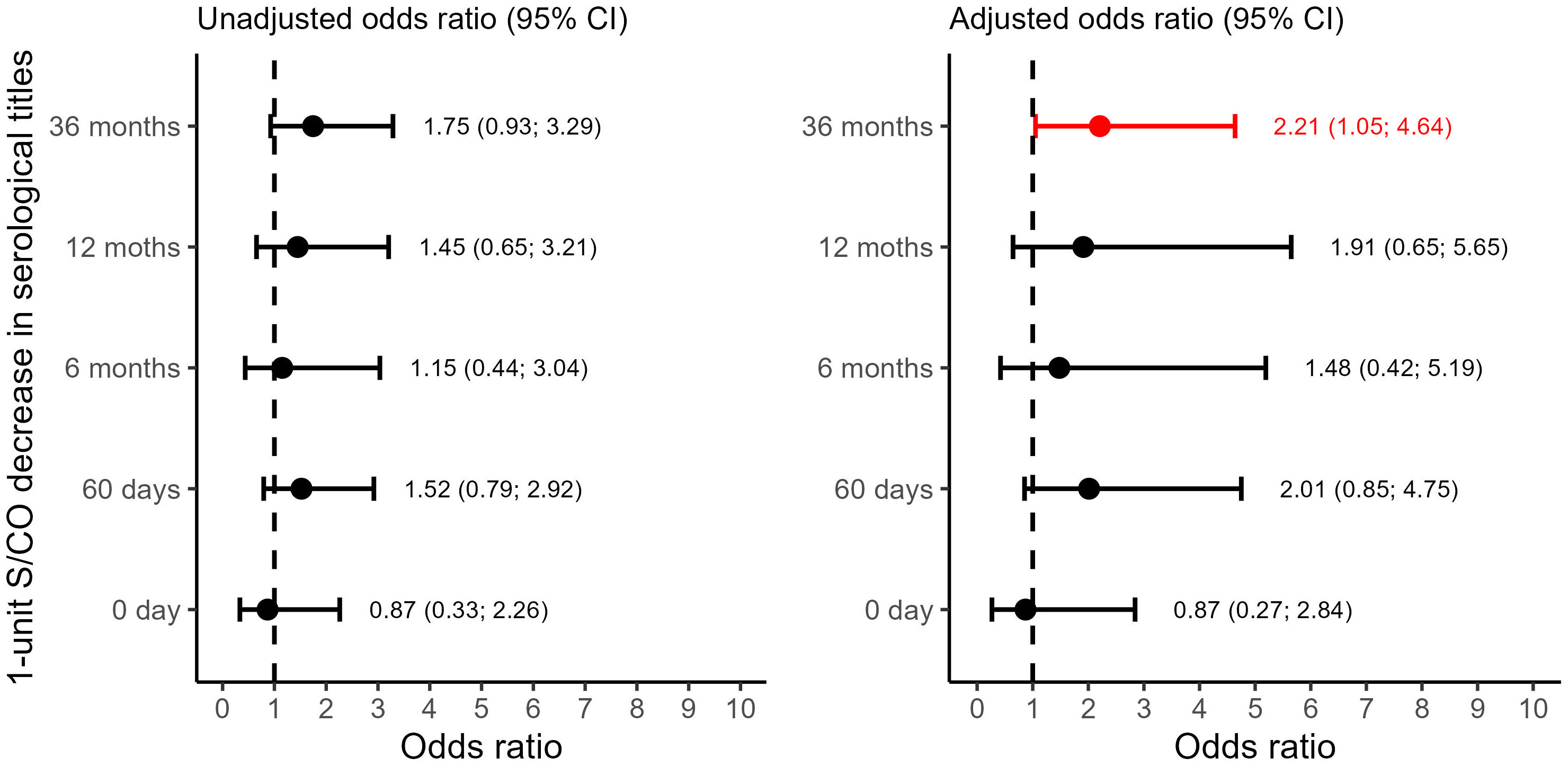
Figure 4 Forest plot depicting the Binomial Logistic Odds Ratio for the non-positive result (negative or inconclusive) outcome group with positive as the reference category. CI: Confidence Interval. S/CO: Signal-to-Cutoff. T0d: Time 0 day; on the day at benznidazole treatment initiation. T60d: Time 60 days; follow-up visit 60 days after initiating benznidazole treatment. T6M: Time 6 Months; follow-up visit 6 months after initiating benznidazole treatment; T12M: Time 12 Months; follow-up visit 12 months after initiating benznidazole treatment. T36M: Time 36 Months; follow-up visit 36 months after initiating benznidazole treatment.
However, it is important to consider the wider confidence intervals observed in most of the observations, which make it challenging to rule out the possibility of no effect conclusively. These wider intervals can be attributed to the limited number of data points and observations across the Positive outcome group. Despite this limitation, we consistently observed a significant decline in antibody levels among patients who were classified within the Negative group. This trend was observable in both approaches for grouping the outcomes, even when we split the patients into a third group, the Inconclusive. This trend was noticeable as early as the T6M visit (Figures 5–8).
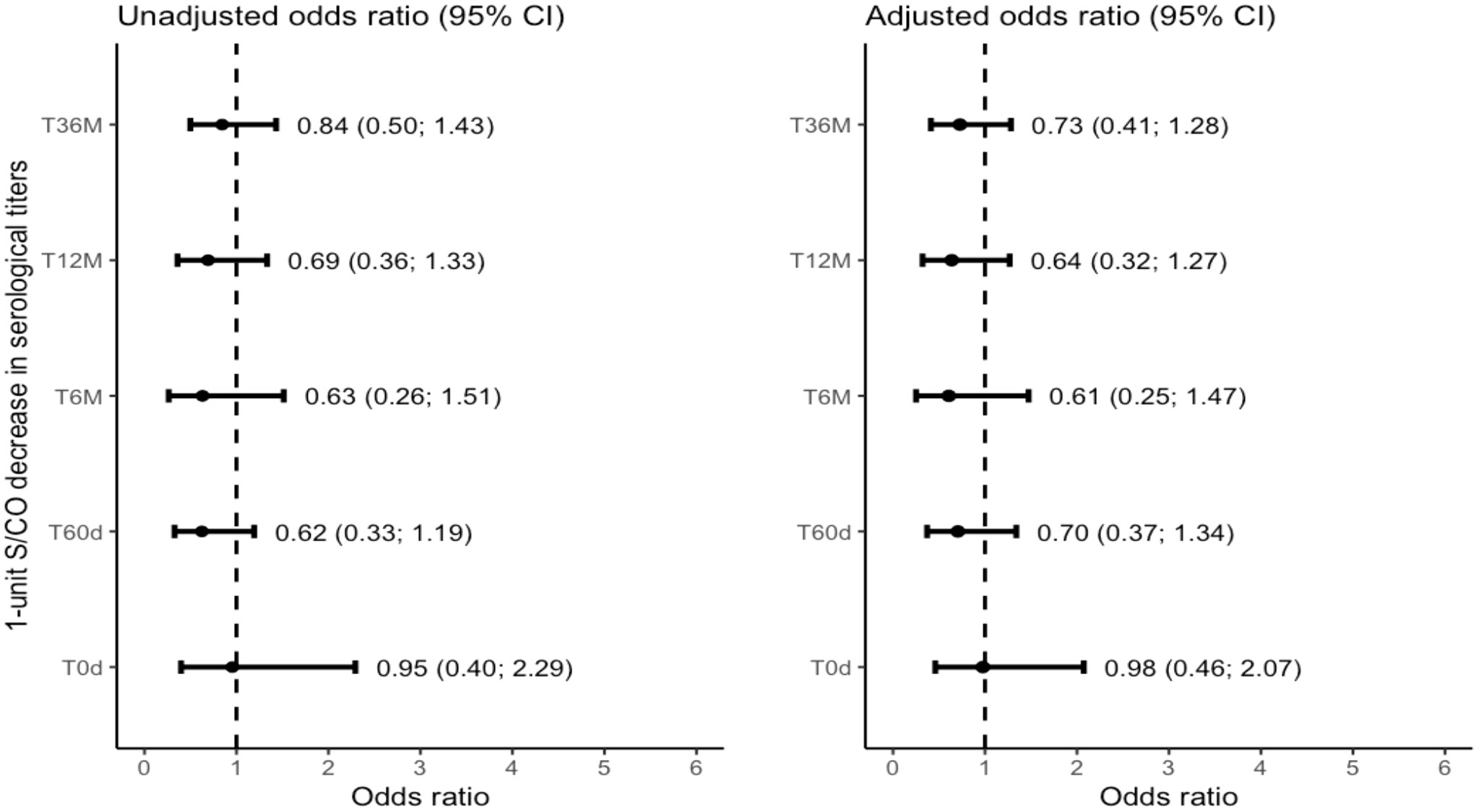
Figure 5 Forest plot depicting the Multinomial Logistic Odds Ratio for the inconclusive outcome group with negative as the reference category. CI: Confidence Interval. S/CO: Signal-to-Cutoff. T0d: Time 0 day; on the day at benznidazole treatment initiation. T60d: Time 60 days; follow-up visit 60 days after initiating benznidazole treatment. T6M: Time 6 Months; follow-up visit 6 months after initiating benznidazole treatment; T12M: Time 12 Months; follow-up visit 12 months after initiating benznidazole treatment. T36M: Time 36 Months; follow-up visit 36 months after initiating benznidazole treatment.
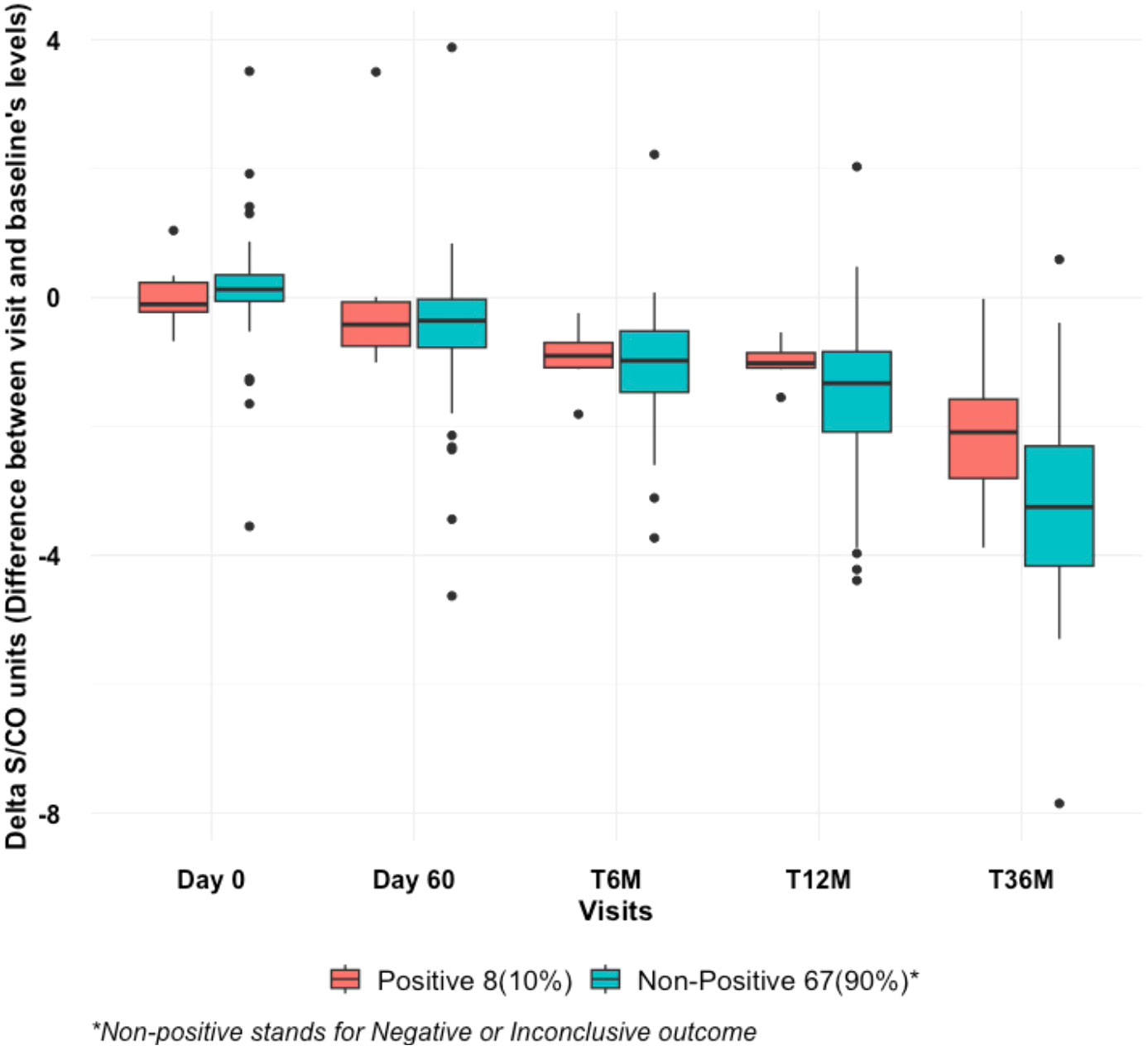
Figure 6 Serial boxplot over visits depicting Decaying Serological Values (S/CO): from Baseline across follow-up visits between defined outcomes. Positive vs. Non-Positive Outcomes (negative or inconclusive). S/CO: Signal-to-CutOff; T0d: Time 0 day; on the day at benznidazole treatment initiation. T60d: Time 60 days; follow-up visit 60 days after initiating benznidazole treatment. T6M: Time 6 Months; follow-up visit 6 months after initiating benznidazole treatment. T12M: Time 12 Months; follow-up visit 12 months after initiating benznidazole treatment. T36M: Time 36 Months; follow-up visit 36 months after initiating benznidazole treatment.
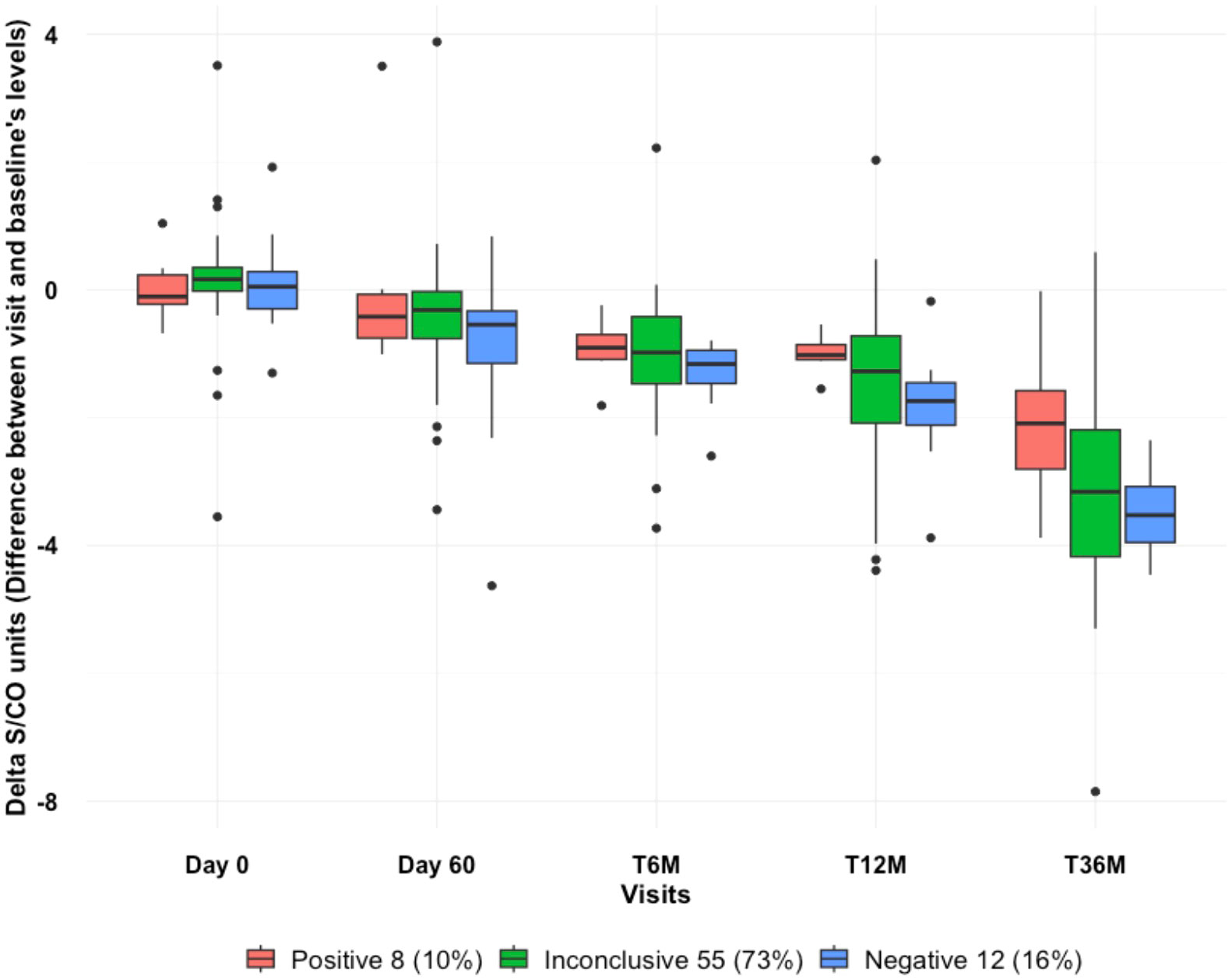
Figure 7 Serial boxplot over visits depicting Decaying Serological Values (S/CO): from Baseline across follow-up visits between defined outcomes: Combined PCR outcome (T6M, T12M, T36M), respectively: Negative (negative result in all visits); Positive (positive result at the T36M visit, regardless of the previous results); Inconclusive (negative result at the T36M visit, and at least one positive result at T6M or T12M).
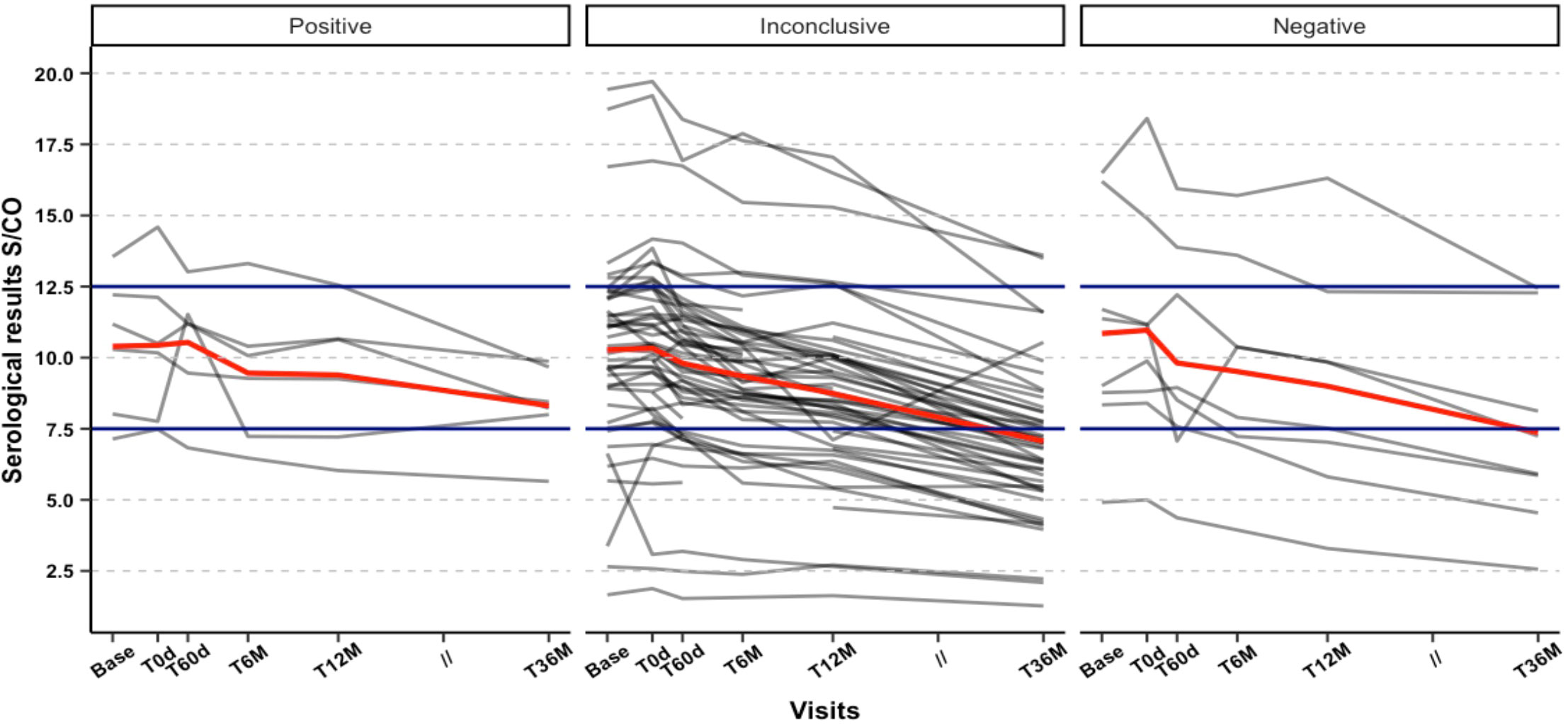
Figure 8 Individual Serological values (S/CO) trajectories from Baseline across follow-up visits between defined outcomes: Combined PCR outcome (T6M, T12M, T36M), respectively: Negative (negative result in all visits); Positive (positive result at the T36M visit, regardless of the previous results); Inconclusive (negative result at the T36M visit, and at least one positive result at T6M or T12M).
In our study, we tracked 87 patients infected with T. cruzi, all of whom were treated with BZN. The PCR results we obtained were challenging to interpret, primarily when used to determine complete parasite elimination. Most patients still showed detectable levels of PCR at least once post-treatment, even though these levels were significantly lower than before treatment. Interestingly, we observed a consistent and early decrease in antibody levels, especially in those patients classified as the ‘Negative’ group.
Our PCR methodology incorporated several steps to enhance sensitivity, including a larger whole blood volume for extraction of 500uL (2 x 250uL) extraction, target capture assay, and eight replicates per sample. This may explain why our study differs from other clinical trials that did detect higher BZN responses defined by earlier and sustained PCR results (Morillo et al., 2015; Morillo et al., 2017). Another plausible explanation is that the older age of our cohort could have contributed to the lower efficacy of BZN. Immunosenescence may play a role in unbalanced parasite clearance since it can interfere with developing protective humoral immunity in response to infectious pathogens in older people (Crooke et al., 2019). Also, we can speculate that the strains present in this population were more resistant to the drug. However, we can not corroborate this since our study did not aim to perform parasite typing or check BNZ resistance. However, interestingly, recent studies have challenged the parasite resistance to the BNZ concept and its association with unsuccessful parasitological outcomes by proposing that this resistance is relative, incomplete, and not associated with specific genetic parasite lineages or host genetics and that the unpredictable treatment outcomes may be due to a transiently dormant amastigote phase (Sánchez-Valdéz et al., 2018).
Interpreting the PCR results posed challenges, but after three years, an encouraging 90% of patients tested negative, indicating that some may have achieved parasite suppression. The proportion of positive results varied significantly between the initial visit (T0d) and subsequent visits, particularly at T60d, which coincided with the end of treatment and the anticipated peak of benznidazole’s trypanocidal effect. However, this significant difference was not consistently observed during the T6M and T12M visits, suggesting potential fluctuations in detectable parasitemia by PCR. Nevertheless, statistical significance was regained at the final follow-up visit (T36M), indicating likely parasite clearance in certain patients (refer to Table 2). While qPCR levels showed a decline across all treatment time points, we agree that these levels should not be regarded as a standalone marker for treatment effectiveness. This is because the qPCR levels did not differentiate between the treatment groups at individual time points. Notably, our study revealed that participants with a >1 S/CO drop at T12M were all negative on PCR at the three-year mark, indicating that an early decrease in antibody titers may be an early predictor of long-term parasite clearance and treatment success.
One limitation of our study is the lack of a non-treated control group, as it would have been ethically challenging to maintain such a group for an extended period. Studies have shown spontaneous antibody decline may occur in untreated patients, however, only in a small proportion of the patients and after a more extended time (Buss et al., 2020). Therefore, the observed antibody decline was likely due to BZN treatment rather than natural variation. Secondly, we didn’t include those patients who had taken less than 50% of the prescribed drug in our analysis, decreasing the study sample. However, we should have included them since recent studies have proposed a shorter BNZ trend compared with the standard treatment (Torrico et al., 2021) and a better adverse effects profile.
In conclusion, our study highlights the challenges of interpreting T. cruzi PCR results. It suggests that antibody decline detected by chemiluminescent assay may be a valuable marker for BZN therapeutic response. Further follow-up visits are necessary to fully understand the long-term response to BZN treatment considering the association of such parasitological outcomes and antibody dynamics.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics committee of the Hospital of Clinics, University of São Paulo, and Institute of Infectology “Emilio Ribas” (CAAE00580612.8.0000.0065). The patients/participants provided their written informed consent to participate in this study.
Conceptualization: ES, AB, CM, MB. Data Curation: CM, CT, LB, SK, CDG, PC. Formal Analysis: CM, CT, AB, LB, CT, SC. Funding Acquisition: ES, MB. Investigation: CM, FG, CG, NC, JL, LS, FS, EM, LF, FG. Methodology: LS, FS, EM, LB, CM, CT, CDG, FG, PC. Project Administration: ES, LS, MB, SK. Resources: ES, LS, MB, EM, PC. Software: CM, CT, LF, FG, LB. Validation: LS, LF, FG, AB. Visualization: CM, ES, AB, MB, LB. Writing – Original Draft Preparation: CM, LB. Writing – Review & Editing: all authors. All authors contributed to the article and approved the submitted version.
This project has received funding from Bill and Melinda Gates´ foundation under grant n° OPP1071295/Subagreement 7636, Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) N° 467043/2014-0, and NIH - 1R01A1AI25738-01.
We acknowledge the patient volunteers, the Institute of Infectology “Emilio Ribas,” and HCFMUSP employees, especially the nurses and laboratory staff: Aparecido Braz, Cleide Guerra, and their teams.
Author SM was employed by the company GigaGen - A Grifols Company. Author SC was employed by the company Grifols Diagnostic Solutions. Author PC was employed by the company Ortho-Clinical Diagnostics, Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received funding from Bill and Melinda Gates Foundation. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpara.2023.1235925/full#supplementary-material
Brazilian Ministry of Health (2022). Available at: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/d/doenca-de-chagas/situacao-epidemiologica (Accessed July 13, 2023).
Buss L. F., Campos de Oliveira-da Silva L., Moreira C. H. V., Manuli E. R., Sales F. C., Morales I., et al. (2020). Declining antibody levels to Trypanosoma cruzi correlate with polymerase chain reaction positivity and electrocardiographic changes in a retrospective cohort of untreated Brazilian blood donors. PloS Negl. Trop. Dis. 14, e0008787. doi: 10.1371/journal.pntd.0008787
Cardoso C. S., Ribeiro A. L. P., Oliveira C. D. L., Oliveira L. C., Ferreira A. M., Bierrenbach A. L., et al. (2018). Beneficial effects of benznidazole in Chagas disease: NIH SaMi-Trop cohort study. PloS Negl. Trop. Dis. 12, e0006814. doi: 10.1371/journal.pntd.0006814
Chagas C. (1909). Nova tripanozomiaze humana: estudos sobre a morfolojia e o ciclo evolutivo do Schizotrypanum cruzi n. gen., n. sp., ajente etiolojico de nova entidade morbida do homem. Memórias do Instituto Oswaldo Cruz 1, 159–218. doi: 10.1590/s0074-02761909000200008
Crooke S. N., Ovsyannikova I. G., Poland G. A., Kennedy R. B. (2019). Immunosenescence: A systems-level overview of immune cell biology and strategies for improving vaccine responses. Exp. Gerontol 124, 110632. doi: 10.1016/j.exger.2019.110632
De Salazar P. M., Sosa-Estani S., Salvador F., Sulleiro E., Sánchez-Montalvá A., Ribeiro I., et al. (2022). Human Trypanosoma cruzi chronic infection leads to individual level steady-state parasitemia: Implications for drug-trial optimization in Chagas disease. PloS Negl. Trop. Dis. 16, e0010828. doi: 10.1371/journal.pntd.0010828
Dias J. C. P., Ramos A. N. Jr, Gontijo E. D., Luquetti A., Shikanai-Yasuda M. A., Coura J. R., et al. (2016). 2nd Brazilian consensus on chagas disease, 2015. Rev. Soc. Bras. Med. Trop. 49Suppl 1, 3–60. doi: 10.1590/0037-8682-0505-2016
Harris P. A., Taylor R., Minor B. L., Elliott V., Fernandez M., O’Neal L., et al. (2019). The REDCap consortium: Building an international community of software platform partners. J. BioMed. Inform 95, 103208. doi: 10.1016/j.jbi.2019.103208
Harris P. A., Taylor R., Thielke R., Payne J., Gonzalez N., Conde J. G. (2009). Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J. BioMed. Inform 42, 377–381. doi: 10.1016/j.jbi.2008.08.010
Hasslocher-Moreno A. M., Saraiva R. M., Sangenis L. H. C., Xavier S. S., de Sousa A. S., Costa A. R., et al. (2021). Benznidazole decreases the risk of chronic Chagas disease progression and cardiovascular events: A long-term follow up study. EClinicalMedicine 31, 100694. doi: 10.1016/j.eclinm.2020.100694
Molina I., Gómez i Prat J., Salvador F., Treviño B., Sulleiro E., Serre N., et al. (2014). Randomized trial of posaconazole and benznidazole for chronic Chagas’ disease. N Engl. J. Med. 370, 1899–1908. doi: 10.1056/NEJMoa1313122
Morillo C. A., Marin-Neto J. A., Avezum A., Sosa-Estani S., Rassi A. Jr, Rosas F., et al. (2015). Randomized trial of benznidazole for chronic chagas’ Cardiomyopathy. N Engl. J. Med. 373, 1295–1306. doi: 10.1056/NEJMoa1507574
Morillo C. A., Waskin H., Sosa-Estani S., Del Carmen Bangher M., Cuneo C., Milesi R., et al. (2017). Benznidazole and posaconazole in eliminating parasites in asymptomatic T. Cruzi carriers: the STOP-CHAGAS trial. J. Am. Coll. Cardiol. 69, 939–947. doi: 10.1016/j.jacc.2016.12.023
Pandey R. P., Nascimento M. S., Franco C. H., Bortoluci K., Silva M. N., Zingales B., et al. (2022). Drug repurposing in chagas disease: chloroquine potentiates benznidazole activity against Trypanosoma cruzi in vitro in vivo. Antimicrob. Agents Chemother. 66, e0028422. doi: 10.1128/aac.00284-22
Pinazo M.-J., MIranda B., Rodríguez-Villar C., Altclas J., Brunet Serra M., García-Otero E. C., et al. (2011). Recommendations for management of Chagas disease in organ and hematopoietic tissue transplantation programs in nonendemic areas. Transplant. Rev. 25, 91–101. doi: 10.1016/j.trre.2010.12.002
Requena-Méndez A., Aldasoro E., de Lazzari E., Sicuri E., Brown M., Moore D. A. J., et al. (2015). Prevalence of Chagas disease in Latin-American migrants living in Europe: a systematic review and meta-analysis. PloS Negl. Trop. Dis. 9, e0003540. doi: 10.1371/journal.pntd.0003540
Sabino E. C., Ribeiro A. L., Lee T. H., Oliveira C. L., Carneiro-Proietti A. B., Antunes A. P., et al. (2015). Detection of Trypanosoma cruziDNA in blood by PCR is associated with Chagas cardiomyopathy and disease severity. Eur. J. Heart Failure 17, 416–423. doi: 10.1002/ejhf.220
Sabino E. C., Ribeiro A. L., Salemi V. M. C., Di Lorenzo Oliveira C., Antunes A. P., Menezes M. M., et al. (2013). Ten-year incidence of chagas cardiomyopathy among asymptomatic trypanosoma cruzi–seropositive former blood donors. Circulation 127, 1105–1115. doi: 10.1161/CIRCULATIONAHA.112.123612
Sánchez-Valdéz F. J., Padilla A., Wang W., Orr D., Tarleton R. L. (2018). Spontaneous dormancy protects Trypanosoma cruzi during extended drug exposure. Elife 7. doi: 10.7554/eLife.34039
Sulleiro E., Silgado A., Serre-Delcor N., Salvador F., Tavares de Oliveira M., Moure Z., et al. (2020). Usefulness of real-time PCR during follow-up of patients treated with Benznidazole for chronic Chagas disease: Experience in two referral centers in Barcelona. PloS Negl. Trop. Dis. 14, e0008067. doi: 10.1371/journal.pntd.0008067
Torrico F., Gascón J., Barreira F., Blum B., Almeida I. C., Alonso-Vega C., et al. (2021). New regimens of benznidazole monotherapy and in combination with fosravuconazole for treatment of Chagas disease (BENDITA): a phase 2, double-blind, randomised trial. Lancet Infect. Dis. 21, 1129–1140. doi: 10.1016/S1473-3099(20)30844-6
Torrico F., Gascon J., Ortiz L., Alonso-Vega C., Pinazo M.-J., Schijman A., et al. (2018). Treatment of adult chronic indeterminate Chagas disease with benznidazole and three E1224 dosing regimens: a proof-of-concept, randomised, placebo-controlled trial. Lancet Infect. Dis. 18, 419–430. doi: 10.1016/S1473-3099(17)30538-8
Keywords: Chagas, Trypanossoma cruzi, benznidazole, serology, PCR, biomarker
Citation: Moreira CHV, Bierrenbach AL, Taconeli CA, de Oliveira-da Silva LC, Buss LF, Keating SM, Manuli ER, Carvalho NB, Guastini C, Coco SB, Lindoso JÂL, Franco LAM, Ghilardi F, Sales FCdS, Contestable P, Di Germanio C, Busch MP and Sabino EC (2023) Parasitemia and antibody response to benznidazole treatment in a cohort of patients with chronic Chagas disease. Front. Parasitol. 2:1235925. doi: 10.3389/fpara.2023.1235925
Received: 06 June 2023; Accepted: 01 August 2023;
Published: 05 September 2023.
Edited by:
Ivan Scandale, Drugs for Neglected Diseases Initiative, SwitzerlandReviewed by:
Alicia Ponte-Sucre, Central University of Venezuela, VenezuelaCopyright © 2023 Moreira, Bierrenbach, Taconeli, de Oliveira-da Silva, Buss, Keating, Manuli, Carvalho, Guastini, Coco, Lindoso, Franco, Ghilardi, Sales, Contestable, Di Germanio, Busch and Sabino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ester Cerdeira Sabino, c2FiaW5vZWNAZ21haWwuY29t
†These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.