
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pain Res. , 19 March 2025
Sec. Musculoskeletal Pain
Volume 6 - 2025 | https://doi.org/10.3389/fpain.2025.1489293
 David Mauricio Parra-Fernandez1
David Mauricio Parra-Fernandez1 Margareth Lorena Alfonso-Mora1*
Margareth Lorena Alfonso-Mora1* María Alejandra Sánchez-Vera1
María Alejandra Sánchez-Vera1 Paola Sarmiento-Gonzalez2
Paola Sarmiento-Gonzalez2 Andrea Milena García Becerra3
Andrea Milena García Becerra3 Miriam Guerra-Balic4
Miriam Guerra-Balic4
Objective: To investigate the association between adolescents' mobile phone dependence (MPD) and musculoskeletal pain.
Methods: A cross-sectional study was conducted among 622 adolescents aged 10–18 in Tabio, Colombia. Participants completed an online survey that included the MPD and the Nordic Musculoskeletal Questionnaire, which assessed musculoskeletal pain symptoms.
Results: 56.3% (n = 350) participants reported experiencing musculoskeletal pain, with the upper back being the most affected area (30.4%, n = 193). Adolescents reporting pain had significantly higher MPD scores compared to those without pain (mean 29 vs. 24, p < 0.001). Additionally, females exhibited higher MPD scores than males (mean 29 vs. 25, p < 0.001) and had a higher prevalence of pain (32% vs. 24%). Furthermore, older adolescents in the 11th grade had higher MPD scores than younger adolescents in the 5th grade (mean 31 vs. 21, p < 0.019). Logistic regression analysis indicated that specific MPD dimensions, namely “abuse” and “difficulty regulating use,” were significantly associated with general pain and neck pain, but no association was observed with upper back pain. Furthermore, female sex was linked to both neck and upper back pain.
Conclusion: This study found that the MPD dimensions of “abuse” and “difficulty regulating use” were significantly associated with neck pain, regardless of the adolescents' sex.
The widespread adoption of mobile phones has resulted in significantly increased screen time and sedentary behaviors among adolescents (1, 2). This trend raises concerns about the potential burden on the musculoskeletal system. Globally, mobile phone usage is growing, with 5.44 billion users representing 68% of the world's population (1). Among adolescents, usage has dramatically increased, with a 17% rise observed between 2019 and 2021 (2), with approximately 70% of Latino youth owning a mobile phone. Adolescents frequently use these devices for social media, video streaming, and gaming, with a weekly average usage increasing from 8 to 10 h (2). In Colombia, the prevalence of mobile phone ownership among adolescents is approximately 61.7%, with 30.6% reporting daily use ranging from 30 min to 1 h (3).
While mobile phones offer adolescents numerous benefits, including increased autonomy, improved academic performance, and enhanced social interaction (4, 5), excessive use is associated with considerable risks to physical, mental, and psychosocial well-being (6, 7). Problematic mobile phone use is particularly prevalent among 15- to 16-year-olds, as it is considered the most common way of dependency disorder during adolescence (8–12). This is characterized by excessive and frequent use (13), academic disruption, and emotional distress (14).
Emerging evidence strongly suggests a link between problematic mobile phone use and musculoskeletal disorders (MSKDs) in adolescents (15–18). MSKDs include a range of conditions affecting bones, muscles, joints, and connective tissues. Representing a major contributor to the global disease burden in individuals aged 15–65, MSKDs affect an estimated 1.7 billion people worldwide (19). The prevalence of MSKDs in adolescents is estimated at 47.4%, with pain being the primary reported symptom (20). Studies indicate a higher incidence of MSKDs associated with excessive mobile phone use among females compared to males (18, 20), particularly among those aged 15–17 years (21).
The most reported pain sites include the neck, shoulders, wrists/hands, upper back, and lower back; some adolescents also report vision-related symptoms (7, 8, 15–17, 20–23). Prolonged mobile phone use (more than 10 h per week) significantly increases the risk of neck and lower back pain. Furthermore, lifestyle factors such as physical inactivity, poor sleep, inadequate fruit and vegetable consumption, and substance use have been identified as predictors of persistent MSKDs (24), in addition to the posture adopted during mobile phone use (25).
Given these concerns, this study investigated the association between MPD and MSKDs in adolescents residents of the Sabana Centro region of Colombia. It is the first to assess the prevalence of pain associated with problematic mobile phone use within the Colombian population. Its relevance is heightened by the substantial increase in screen time following the COVID-19 pandemic, impacting both educational and non-educational settings. A comprehensive understanding of problematic screen use, particularly concerning mobile phones, is crucial for developing effective interventions to improve adolescents' health and well-being.
A cross-sectional design was applied to investigate the association between MPD and musculoskeletal pain among adolescents. Data were collected from two educational institutions in Tabio, Colombia, during September and October 2022. Ethical approval was received by the ethics committee of the University of La Sabana (Minute 021-18 Nov 2020). Before participation, all students provided informed assent, and their parents/guardians signed informed consent forms.
The sample size was calculated using R Studio 4.3.2.1 and the pwr package. A binomial statistical test was employed, assuming a small effect size [Cohen's h = 0.03 (8)], with a significance level (α) set to 0.05 and a power of 0.80. Based on these parameters, the required sample size was 622 participants (11).
For the recruitment process, 1,183 students from the two schools were invited to volunteer after receiving information about the study's objectives. A researcher administered the survey in their classrooms, and consent forms were sent to parents to obtain their signed approval. Participants were included if they were school-aged (10–18 years), enrolled in grades 5–11th, and had access to a mobile phone. Exclusion criteria were a pre-existing medical diagnosis of a disability. Of the 1,183 invited students, 685 consented to participate; after applying inclusion/exclusion criteria, 63 participants were excluded, resulting in a final sample of 622 adolescents.
Participants completed an online questionnaire comprising three sections:
1. Sociodemographic data: age, sex, and grade level.
2. Mobile phone dependence MPD: the MPD scale was used to assess MPD. This scale, designed for adolescents consisted of 22 items grouped into four factors: withdrawal (36 points), abuse and difficulty (36 points), problems arising from use (16 points), and tolerance/interference (16 points). Items are rated on a 5-point Likert scale (0 = never to 4 = always), with a total score ranging from 0 to 88. Higher scores reflect greater dependency. The validated Spanish version of the MPD scale (Cronbach's alpha = 0.89) was used (5).
3. Musculoskeletal pain assessment: musculoskeletal pain experienced in the previous 6 months was assessed using a Spanish-validated version of the Nordic Musculoskeletal Questionnaire (NMQ) (26). The reliability of this version demonstrated an intraclass correlation coefficient (ICC) exceeding 0.9. Participants responded “yes” or “no” to five questions regarding pain in the following five specific body regions: (1) neck, (2) head and neck, (3) shoulders, (4) upper back, and (5) lower back. Each question included a visual diagram of the corresponding body region. General pain was defined as pain in any of these five regions.
Data analysis was done using SPSS version 26. Descriptive statistics (frequencies, percentages, means, median standard deviations, interquartile ranges) were obtained. The Shapiro–Wilk test was applied to assess the normality of data distribution. Given the non-normal distribution of mobile phone dependency scores, non-parametric tests (Spearman correlation for correlations, Mann–Whitney U test for group comparisons) were used. A Spearman correlation coefficient (ρ) of 0.76–1.00 was considered a strong relationship (27). The χ2 test was used to identify the association between sex and pain prevalence. A p-value ≤0.05 was considered statistically significant. Logistic regression analysis was used to model the relationship between general pain, neck pain, and upper back pain (dichotomous outcome: yes/no), with the independent variables of sex, age, and MPD factors.
Of the 1,183 students invited, 622 (52%) participated in the study, including pupils from grades 5–11th, of which 54.5% were females and 45.5% were males, with a median age of 14 years. Musculoskeletal pain (in at least one of five specified body regions) was reported by 56.3% (n = 350) participants within the past 6 months. The upper back was the most frequently affected region (30.4%, n = 193), followed by the neck (29.3%) and shoulders (21.1%). The median MPD score was 27 [interquartile range (IQR): 17–37] (Table 1).
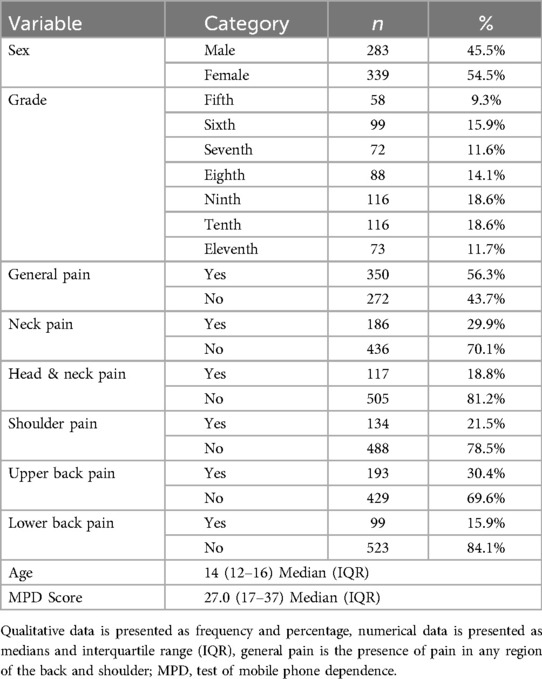
Table 1. Sociodemographic characteristics and prevalence of musculoskeletal pain.
Female adolescents reported significantly higher MPD scores than males in all dimensions except for Excessive Use (median difference in total MPD: 4 points; p < 0.001). MPD scores increased significantly with the grade level (p = 0.019). Participants reporting pain in any body region exhibited significantly higher MPD scores (median difference: 5 points; p < 0.001) compared to those without pain, except for those with low back pain (p = 0.055) (Table 2).
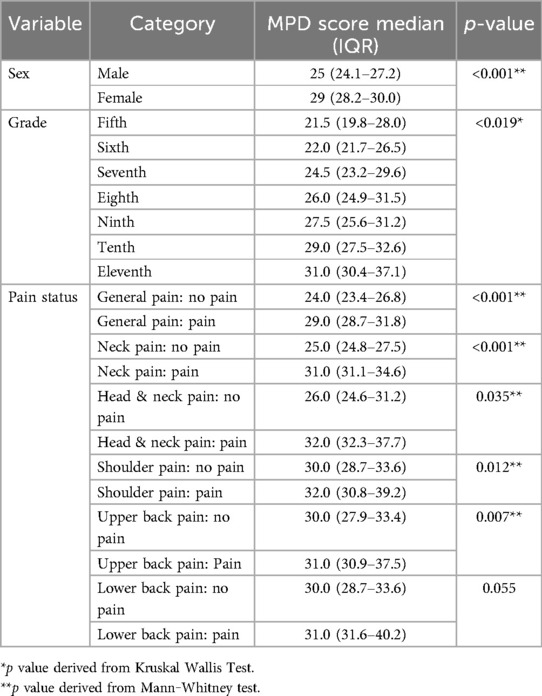
Table 2. MPD scores by demographic factors and pain status.
The analysis of MPD dimensions by gender revealed consistently higher female scores across all dimensions except “problems arising from use” (Table 3). Among participants with back pain, those experiencing pain in the neck, shoulders, or upper back had significantly higher scores on three of the four MPD dimensions; however, no significant difference was observed for low back pain (Table 4).
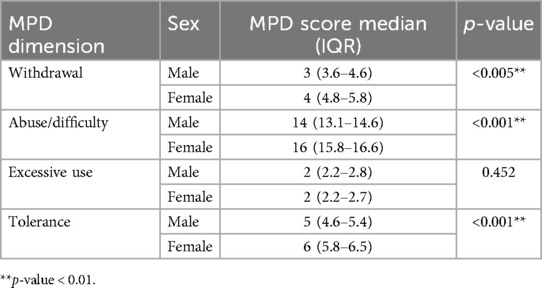
Table 3. MPD dimension scores by sex.
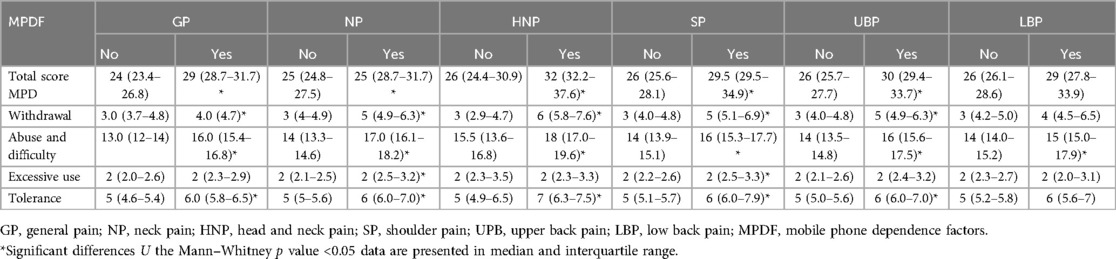
Table 4. The median difference between mobile phone dependence factors and pain.
A weak positive correlation was found between age and total MPD scores (Rho = 0.19, p < 0.01). This association was particularly pronounced for the “withdrawal” (Rho = 0.15, p < 0.01), “abuse/difficulty” (Rho ρ = 0.16, p < 0.01), and “tolerance” (Rho = 0.25, p < 0.01) dimensions of the MPD scale. Females reported a significantly higher prevalence of pain (approximately 10% greater than males) across most body regions, except for the low back and shoulders (χ2 test, p < 0.001). Furthermore, adolescents reporting pain were significantly older (mean difference of 1 year, p < 0.001) than those without pain (Table 5).
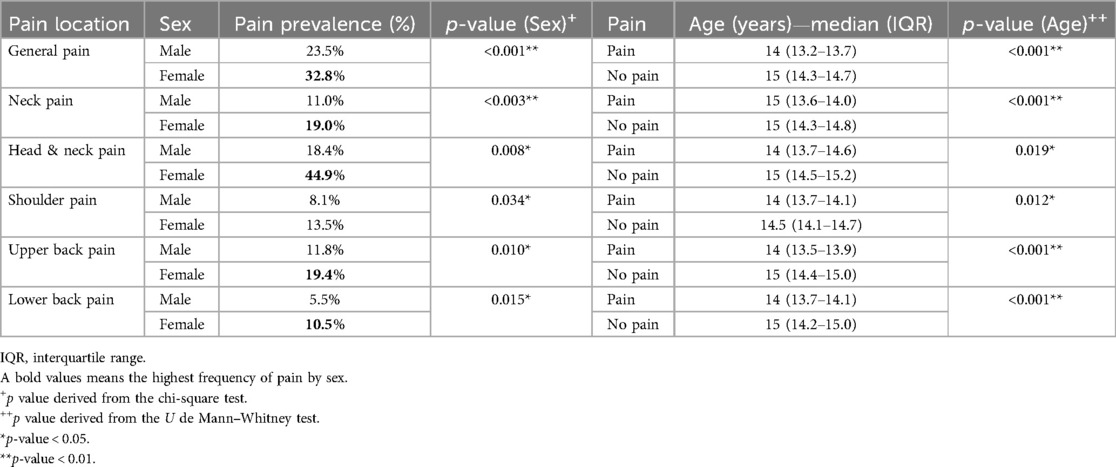
Table 5. Prevalence of musculoskeletal pain by sex and age.
Three logistic regression models were developed to examine the association between general pain, neck pain, and upper back pain, as these were the most prevalent pain areas reported among the participants. These models included sex, age, and the four dimensions of the MPD scale (withdrawal, abuse/difficulty, problems arising from use, and tolerance/interference) as independent variables. Significant associations were found between the “abuse/difficulty” dimension of the MPD and general and neck pain. Furthermore, female sex was identified as associated variable for neck and upper back pain (Appendix 1).
This study revealed a high prevalence of musculoskeletal pain among adolescents, particularly affecting the upper back and neck. Higher MPD scores were significantly associated with pain and were more prevalent among female and older adolescents. A positive correlation was found between age and MPD scores and between sex and pain prevalence.
The observed prevalence of musculoskeletal pain aligns with previous research. Martins et al. (20) reported a 47.4% prevalence in a similar adolescent population, consistent with our findings of 56.3%. Straker et al. (18) found neck and shoulder pain in 50% of participants, with lower back pain in 34% and upper limb pain in 30%, supporting the high prevalence of upper body pain found in our study. Mustafaoğlu et al. (22) also reported high prevalence rates of upper back, neck, and wrist/hand pain, and similar observations regarding neck, shoulder, and eye discomfort have been reported by Ahmed et al. (17) and Mokhtarinia et al. (8).
Previous studies on mobile phone dependency have shown varying prevalence rates. Mokhtarinia et al. (8) reported a 53.3% prevalence in Iran, with slightly higher rates among males (54.5%) than females (52.7%), although no significant difference in average dependency scores was found. Gangadharan et al. (7) reported a lower prevalence (33%) in India, with slightly higher rates among males (33.6%) than females (32.3%). Alsalameh et al. (15) also observed higher rates in males. In contrast, our findings are consistent with Straker et al. (18), who reported higher mobile phone use among older adolescents and females.
The observed discrepancies regarding sex and MPD between our study and prior research might be attributable to several factors. Our study included a wider age range, which may have influenced the results. Furthermore, our larger sample size allowed for greater statistical power to detect significant differences. The observed higher mobile phone dependency among females supports further investigation into potential gender-specific patterns of mobile phone usage.
Our findings showed a significant association between higher MPD scores and musculoskeletal pain, primarily in the neck, shoulders, and upper back, but not in the lower back. This is consistent with Alsalameh et al. (15), who also found higher MPD scores among participants with pain (except those with elbow or lower back pain). However, our study only revealed a significant correlation between MPD and age. The gender differences in pain prevalence align with Sirajudeen et al. (28) who observed an association between sex and shoulder pain, although Walankar et al. (29) did not report a similar relationship. These variations may reflect differences in study populations, cultural contexts, or methodological approaches.
This cross-sectional study has several limitations. Its design does not allow for establishing causality between MPD and musculoskeletal pain. Additionally, other forms of screen time potentially associated with pain, such as the use of computers and tablets, were not assessed. Self-reported pain data are subject to bias, which could lead to underreporting or overreporting of results. Finally, selection bias should be considered, as the study included only pupils who returned signed informed assents and whose parents or legal guardians provided signed consent.
Extensive literature links risk mobile phone use to various negative health outcomes, affecting both physical and mental health. The rising prevalence of musculoskeletal pain in adolescents is likely multifactorial, involving excessive mobile device use, sedentary behavior, poor posture (e.g., forward head posture), and sleep disturbances. Muscular fatigue, chronic pain, and reduced quality of life are common consequences (30). Based on this evidence, interventions promoting increased physical activity, sports participation, and limiting screen time (to no more than 2 h daily) are strongly recommended (30).
The prevalence of musculoskeletal pain is a significant contributor to the global burden of disease, which is increasing among children and adolescents. Lifestyle habits are a risk factor for these conditions in this population. This study found not only a prevalence of 58% for pain but also an association with mobile dependency, particularly among females, with the incidence increasing with age. These findings emphasize the need for public health interventions aimed at adolescents to promote healthier mobile phone use, encourage physical activity, and improve posture, particularly among females. Future research should assess the effectiveness of these interventions, with a specific focus on addressing the “abuse” and “difficulty regulating use” dimensions of MPD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Comite de etica Universidad de La Sabana. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
DP-F: Data curation, Formal analysis, Writing – original draft, Project administration. MA-M: Conceptualization, Data curation, Formal analysis, Writing – original draft. MS-V: Conceptualization, Data curation, Formal analysis, Validation, Writing – original draft. PS-G: Conceptualization, Writing – review & editing. AGB: Conceptualization, Writing – review & editing. MG-B: Conceptualization, Writing – review & editing, Supervision.
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by the Universidad de La Sabana (2020) (Convocatoria Interna Para La Financiación De Proyectos De Investigación, Creación, Desarrollo Tecnologico E Innovación). Project ID: ENF-59-2020.
The authors thank public schools' participants for this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that Generative AI was used in the creation of this manuscript. While preparing this work, the authors used Chat GPT 4.0 to correct style and grammar mistakes. After using this tool/service, the authors reviewed and edited the content as needed and took full responsibility for the content of the published article.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2025.1489293/full#supplementary-material
1. Girela-Serrano BM, Spiers ADV, Ruotong L, Gangadia S, Toledano MB, Di Simplicio M. Impact of mobile phones and wireless devices use on children and adolescents’ mental health: a systematic review. Eur Child Adolesc Psychiatry. (2022) 33(6):1621–51. doi: 10.1007/s00787-022-02012-8
2. O’Reilly M. Social media and adolescent mental health: the good, the bad and the ugly. J Ment Health. (2020) 29(2):200–6. doi: 10.1080/09638237.2020.1714007
3. Marín-Díaz V, Muñoz-González JM, Sampedro-Requena BE. Problematic relationships with smartphones of Spanish and Colombian university students. Int J Environ Res Public Health. (2020) 17(15):5370. doi: 10.3390/ijerph17155370
4. Mettathamrong J. Factors that affect the behavior of adolescents in Thailand due to the use of mobile phones in their daily life. Utop Prax Latinoam. (2021) 26(2):212–26. doi: 10.5281/zenodo.4678884
5. Chóliz M, Pinto L, Phansalkar SS, Corr E, Mujjahid A, Flores C, et al. Development of a brief multicultural version of the test of mobile phone dependence (TMDbrief) questionnaire. Front Psychol. (2016) 7:650. doi: 10.3389/fpsyg.2016.00650
6. Gupta DS. Impact of mobile phone on youth: a psycho-social study. Int J Res Educ. (2016) 30(4):50–6.
7. Gangadharan N, Borle AL, Basu S. Mobile phone addiction as an emerging behavioral form of addiction among adolescents in India. Cureus. (2022) 14(4):e23798. doi: 10.7759/cureus.23798
8. Mokhtarinia HR, Torkamani MH, Farmani O, Biglarian A, Gabel CP. Smartphone addiction in children: patterns of use and musculoskeletal discomfort during the COVID-19 pandemic in Iran. BMC Pediatr. (2022) 22(1):681. doi: 10.1186/s12887-022-03748-7
9. Kliesener T, Meigen C, Kiess W, Poulain T. Associations between problematic smartphone use and behavioural difficulties, quality of life, and school performance among children and adolescents. BMC Psychiatry. (2022) 22(1):195. doi: 10.1186/s12888-022-03815-4
10. Muñoz-Miralles R, Ortega-González R, López-Morón MR, Batalla-Martínez C, Manresa JM, Montellà-Jordana N, et al. The problematic use of information and communication technologies (ICT) in adolescents by the cross sectional JOITIC study. BMC Pediatr. (2016) 16(1):140. doi: 10.1186/s12887-016-0674-y
11. Azadvari M, Sarzaeim M, Rajabi S, Yahyaee A, Razavi SZE, Haghparast A, et al. Associations between exposure to common technology devices and reported neck pain among Iranian school-age adolescents: a cross sectional study. BMC Musculoskelet Disord. (2023) 24(1):883. doi: 10.1186/s12891-023-07010-8
12. Haug S, Castro RP, Kwon M, Filler A, Kowatsch T, Schaub MP. Smartphone use and smartphone addiction among young people in Switzerland. J Behav Addict. (2015) 4(4):299–307. doi: 10.1556/2006.4.2015.037
13. Pérez de Albéniz Garrote G, Rubio L, Medina Gómez B, Buedo-Guirado C. Smartphone abuse amongst adolescents: the role of impulsivity and sensation seeking. Front Psychol. (2021) 12:746626. doi: 10.3389/fpsyg.2021.746626
14. Yoon M, Yun H. Relationships between adolescent smartphone usage patterns, achievement goals, and academic achievement. Asia Pac Educ Rev. (2023) 24(1):13–23. doi: 10.1007/s12564-021-09718-5
15. Alsalameh A, Harisi M, Alduayji M, Almutham A, Mahmood F. Evaluating the relationship between smartphone addiction/overuse and musculoskeletal pain among medical students at Qassim University. J Family Med Prim Care. (2019) 8(9):2953–9. doi: 10.4103/jfmpc.jfmpc_665_19
16. Yang G, Cao J, Li Y, Cheng P, Liu B, Hao Z, et al. Association between internet addiction and the risk of musculoskeletal pain in Chinese college freshmen: a cross-sectional study. Front Psychol. (2019) 10:1959. doi: 10.3389/fpsyg.2019.01959
17. Ahmed S, Mishra A, Akter R, Shah MH, Sadia AA. Smartphone addiction and its impact on musculoskeletal pain in neck, shoulder, elbow, and hand among college going students: a cross-sectional study. Bull Fac Phys Ther. (2022) 27(1):1–15. doi: 10.1186/s43161-021-00067-3
18. Straker L, Harris C, Joosten J, Howie EK. Mobile technology dominates school children’s IT use in an advantaged school community and is associated with musculoskeletal and visual symptoms. Ergonomics. (2018) 61(5):658–69. doi: 10.1080/00140139.2017.1401671
19. Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the global burden of disease study 2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396(10267):2006–17. doi: 10.1016/S0140-6736(20)32340-0
20. Martins RL, Carvalho N, Albuquerque C, Andrade A, Martins C, Campos S, et al. Musculoskeletal disorders in adolescents: a study on prevalence and determining factors. Acta Paul Enferm. (2020) 33:1–8. doi: 10.37689/acta-ape/2020AO0173
21. Minghelli B. Musculoskeletal spine pain in adolescents: epidemiology of non-specific neck and low back pain and risk factors. J Orthop Sci. (2020) 25(5):776–80. doi: 10.1016/j.jos.2019.10.008
22. Mustafaoglu R, Yasaci Z, Zirek E, Griffiths MD, Ozdincler AR. The relationship between smartphone addiction and musculoskeletal pain prevalence among young population: a cross-sectional study. Korean J Pain. (2021) 34(1):72–81. doi: 10.3344/kjp.2021.34.1.72
23. Toh SH, Coenen P, Howie EK, Mukherjee S, Mackey DA, Straker LM. Mobile touch screen device use and associations with musculoskeletal symptoms and visual health in a nationally representative sample of Singaporean adolescents. Ergonomics. (2019) 62(6):778–93. doi: 10.1080/00140139.2018.1562107
24. Smedbråten K, Grotle M, Jahre H, Richardsen KR, Småstuen MC, Skillgate E, et al. Lifestyle behaviour in adolescence and musculoskeletal pain 11 years later: the Trøndelag health study. Eur J Pain. (2022) 26(9):1910–22. doi: 10.1002/ejp.2012
25. Mongkonkansai J, Veerasakul S, Tamrin SBM, Madardam U. Predictors of musculoskeletal pain among primary school students using smartphones in Nakhon Si Thammarat, Thailand. Int J Environ Res Public Health. (2022) 19(17):10530. doi: 10.3390/ijerph191710530
26. Mateos-González L, Rodríguez-Suárez J, Llosa JA, Agulló-Tomás E. Spanish version of the nordic musculoskeletal questionnaire: cross-cultural adaptation and validation in nursing aides. An Sist Sanit Navar. (2024) 47(1):e1066. doi: 10.23938/ASSN.1066
27. de Winter JC, Gosling SD, Potter J. Comparing the Pearson and Spearman correlation coefficients across distributions and sample sizes: a tutorial using simulations and empirical data. Psychol Methods. (2016) 21(3):273–90. doi: 10.1037/met0000079
28. Sirajudeen MS, Alzhrani M, Alanazi A, Alqahtani M, Waly M, Manzar MD, et al. Prevalence of upper limb musculoskeletal disorders and their association with smartphone addiction and smartphone usage among university students in the kingdom of Saudi Arabia during the COVID-19 pandemic—a cross-sectional study. Healthcare. (2022) 10(12):2373. doi: 10.3390/healthcare10122373
29. Walankar PP, Kemkar M, Govekar A, Dhanwada A. Musculoskeletal pain and risk factors associated with smartphone use in university students. Indian J Occup Environ Med. (2021) 25(4):220–4. doi: 10.4103/ijoem.ijoem_351_20
30. Rodríguez-Cáceres A, Sánchez-Vera MA, Alfonso-Mora M, Sarmiento-Gonzalez P, Lever Méndez J, Milena A, et al. Relación entre la exposición a pantallas, el comportamiento sedentario y el dolor musculoesquelético en adolescentes: revisión sistemática. Retos. (2023) 50:1064–70. doi: 10.47197/retos.v50.99865
Keywords: musculoskeletal pain, mobile phone use, adolescent, physiotherapy, low back pain, neck pain
Citation: Parra-Fernandez DM, Alfonso-Mora ML, Sánchez-Vera MA, Sarmiento-Gonzalez P, García Becerra AM and Guerra-Balic M (2025) Mobile phone dependence and musculoskeletal pain prevalence in adolescents: a cross-sectional study. Front. Pain Res. 6:1489293. doi: 10.3389/fpain.2025.1489293
Received: 31 August 2024; Accepted: 28 February 2025;
Published: 19 March 2025.
Edited by:
Adérito Ricardo Duarte Seixas, Escola Superior de Saúde Fernando Pessoa, PortugalReviewed by:
Ana Velly, McGill University, CanadaCopyright: © 2025 Parra-Fernandez, Alfonso-Mora, Sánchez-Vera, Sarmiento-Gonzalez, García Becerra and Guerra-Balic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Margareth Lorena Alfonso-Mora, bWFyZ2FyZXRoYWxtb0B1bmlzYWJhbmEuZWR1LmNv
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.