
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pain Res. , 07 January 2025
Sec. Pharmacological Treatment of Pain
Volume 5 - 2024 | https://doi.org/10.3389/fpain.2024.1484948
 Mosadoluwa Afolabi1Jensy Rodriguez-Silva1
Mosadoluwa Afolabi1Jensy Rodriguez-Silva1 Ishveen Chopra1
Ishveen Chopra1 Ines Macias-Perez2Jason Makii2
Ines Macias-Perez2Jason Makii2 Emily Durr2Theresa Human2*
Emily Durr2Theresa Human2*
Introduction: Intravenous non-steroidal anti-inflammatory drugs (NSAIDs) are commonly used in healthcare settings, but their comparative safety and resource utilization impacts remain understudied. This study aimed to compare adverse drug reactions (ADRs) and healthcare resource utilization (HCRU) between patients receiving IV-ibuprofen versus IV/IM ketorolac.
Methods: A retrospective, longitudinal analysis was conducted using an all-payer database, examining records from January 1, 2014, to June 3, 2023. The study included both adult (≥18 years) and pediatric (<18 years) populations who received one or more doses of either medication. Propensity score matching was applied to both populations, and HCRU was tracked for 29 days post-final dose. The adult cohort included 31,046 IV-ibuprofen and 124,184 ketorolac records, while the pediatric cohort had 5,579 patients per treatment arm.
Results: Both adult and pediatric patients receiving IV-ibuprofen demonstrated lower ADR incidence and reduced HCRU compared to those receiving ketorolac.
Discussion: The findings suggest IV-ibuprofen may be a safer alternative to ketorolac, potentially improving patient care outcomes while reducing healthcare system burden. These results have implications for clinical practice and healthcare resource management.
Adverse drug reactions (ADRs) are unintended injuries or complications that arise from administration of a medication. These unwanted drug effects have considerable clinical costs as they can lead to emergency department visits, hospital admission, prolongation of hospital stays and can result in disability or even death (1–4). A recent study estimated that the annual impact of serious ADRs, among hospitalized adult and pediatric patients in the United States (US), results in 2.2 million hospitalizations and 106,000 deaths (5). The economic burden of ADRs is also substantial, with estimates of up to $30.1 billion annually in the US alone (6). Additionally, ADRs can have a significant effect on a patients’ quality of life, including physical and emotional suffering, social isolation, and impaired daily functioning (7). Choosing the most appropriate medication is of the utmost importance to minimize harm, improve outcomes, and reduce medical costs and resources.
Currently there are two intravenous (IV) nonsteroidal anti-inflammatory drugs (NSAID) on the US market, ketorolac injection and IV ibuprofen (Caldolor®, Cumberland Pharmaceuticals Inc., Nashville, TN, USA). Only the parental formulation of ketorolac will be considered in this study. Ketorolac was approved in 1989 for the short-term management of moderately severe, acute pain requiring opioid analgesia (8). Although ketorolac is the most frequently administered IV NSAID, it has several limitations including multiple contraindications. Ketorolac is contraindicated for: use in excess of 5 days due to increased potential for frequency and severity of ADRs; use in pediatric patients; administration preoperatively due to increased risk of bleeding; use in patients with active or history of gastrointestinal (GI) bleeding or peptic ulcer disease; use in patients at high risk of bleeding and those with advanced renal impairment; and use in labor and delivery due to adverse effects on fetal circulation, inhibition of uterine contractions, and increased risk of uterine hemorrhage (8–11). Intravenous (IV) ibuprofen was first approved in 2009 for the management of mild to moderate pain, moderate to severe pain in combination with narcotics, and for the reduction of fever in adults and pediatric patients ≥3 months of age (12, 13). Additionally, IV ibuprofen has demonstrated efficacy and safety when administered pre-surgically (14, 15).
The mechanism of action of non-selective NSAIDs include inhibition of cyclooxygenase 1 (COX-1) and COX-2 pathways which decrease the expression of prostaglandin precursors, including thromboxane and prostacyclin, and is how they derive their analgesic, antipyretic, and anti-inflammatory properties (16). While all IV NSAIDs are non-selective in their COX-1 and COX-2 inhibition, they differ in their degree of inhibition of COX-1 relative to COX-2. Warner et al. evaluated the COX isoenzyme inhibitory capacity of multiple NSAIDs and reported ketorolac as the most COX-1 selective, which aligns with studies that signal ketorolac to be the most gastro- and nephrotoxic of all NSAIDs (9, 17, 18). Ibuprofen inhibits COX-1 2.5 times more than COX-2 and would be considered slightly more neutral than the other NSAIDs (19). A meta-analysis of 28 studies evaluating the relative risk (RR) of GI adverse reactions in several NSAIDs, demonstrated ibuprofen had one of the most favorable risk profiles (RR 1.84; 95% CI 1.54, 2.20) and significantly safer than ketorolac (RR 11.50; 95% CI 5.56, 23.78) (20).
Although these medications have been extensively studied, there are no studies that describe the difference in adverse reactions between agents. The objective of this study is to describe and compare ADRs after exposure to IV ibuprofen vs. IV or intramuscular (IM) ketorolac, in both adult and pediatric populations. The economic impact of the difference will also be described through all-cause and ADR-related health care resource utilization (HCRU) within 29 days after the last dose of medication administration.
This is a retrospective, longitudinal, observational database study evaluating an all-payer database assessing patients that received one or more doses of IV ibuprofen or IV/IM ketorolac between January 1, 2014 to June 30, 2023.
Real World Data (RWD) Insights data was utilized for this study. RWD Insights includes comprehensive coverage at the patient level across the US health care system, as well as all provider types. Data are de-identified and complies with the requirements of the Health Insurance Portability and Accountability Act (HIPAA).
Eligible patients were classified into 2 age groups: <18 years and ≥18 years old. Patients had at least ≥1 pharmacy or medical claim for IV ibuprofen or IV/IM ketorolac and ≥12-months pre/post-index date administration data records. Patients were excluded if they had a pre-index ICD-9/ICD-10 claim for renal dysfunction, GI or general bleeding disorders, low back pain, headache, abdominal pain, nausea/vomiting, or throat pain. Patients that received oral/ophthalmic/nasal formulations or received both medications were also excluded. The first dose administered is considered the index dose (Figure 1).
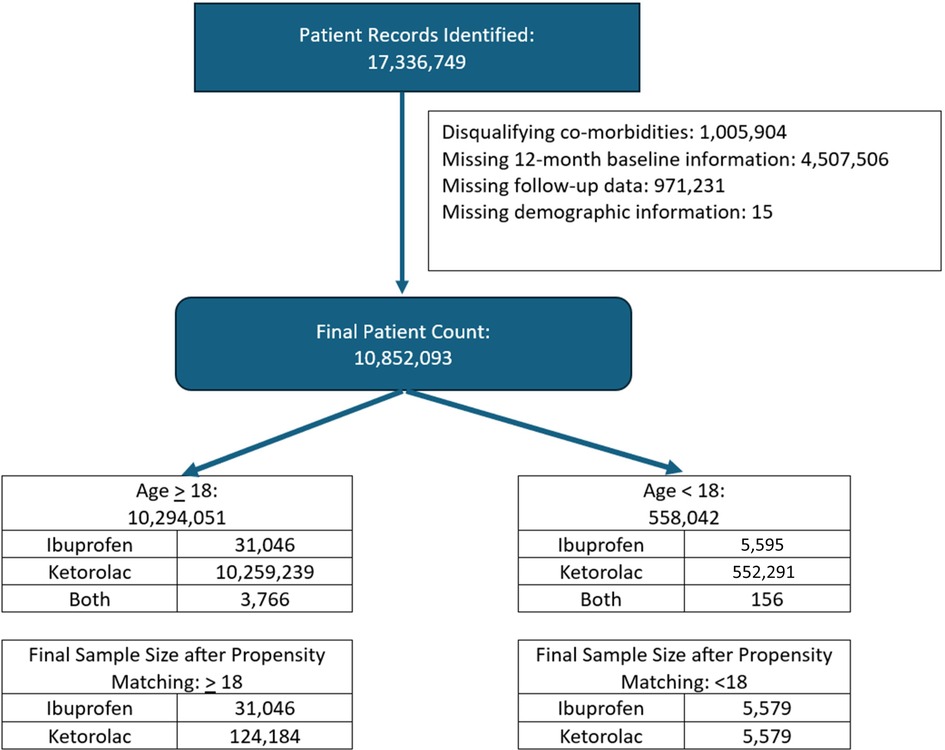
Figure 1. Patient selection.
Key baseline patient characteristics included demographics, dose, number of doses administered, diagnoses (ICD-9/ICD-10 codes), physician characteristics, setting of drug administration, reason for drug administration (surgical, fever, non-surgical), payer channel, concurrent medication use (ACEI, ARB, calcineurin inhibitors, antiplatelet, anticoagulants, NSAIDs, IIb/IIIa inhibitors, aminoglycoside, vancomycin, acyclovir), Charlson Comorbidity Index (CCI) Score, CCI comorbidities, and Pediatric Comorbidity Index (PCI) (age <18 years).
Safety with these medications was assessed during the post-index period. Common ADRs for both parenteral ibuprofen and ketorolac were identified a priori and included renal dysfunction, GI bleeding disorders, general bleeding disorders, low back pain, headache, abdominal pain, nausea/vomiting, and throat pain. These ADRs were identified using ICD-9/ICD-10 codes. The incidence of ADRs post parenteral ibuprofen and ketorolac dose was identified 72 h after the last dose administered (maximum of 5 days). As previously described, patients with a claim for any of the targeted side effects 12-month prior to the index dose were excluded.
Healthcare resource utilization (HCRU) were evaluated out to 29 days after last dose of treatment. All-cause HCRU during the follow-up period across all healthcare settings [hospitalizations/inpatient visits, outpatient visits, emergency department (ED) visits, and pharmacy] was assessed. All-cause visits were defined as any inpatient or outpatient visit related to any diagnosis.
Descriptive analysis was performed on both demographic and outcome variables. Propensity score matching (PSM) was employed to account for observable baseline differences between the two groups of interest, with a matching ratio of 1:4 (ibuprofen: ketorolac) for adult patients and 1:1 (ibuprofen: ketorolac) for pediatric patients. The variables used in the logistic regression model included age group, sex, reason for administration (categorized as surgical, fever, or other), and the number of index drug administrations (ranging from 1 to 5+).
A total of 31,046 IV Ibuprofen and 124,184 parenteral ketorolac adult patients were identified and matched (1:4). In adults the mean dose was 784 ± 445 mg and 30 ± 16 mg for parenteral ibuprofen and ketorolac, respectively. One dose was administered to 93% of adult patients. Among adults, most patients were female, greater than 65 years of age, received the index drug for surgical pain, and had few to no comorbidities (Table 1, Supplementary Table S1). A significant portion of adults that received ketorolac had Medicare or Medicaid.
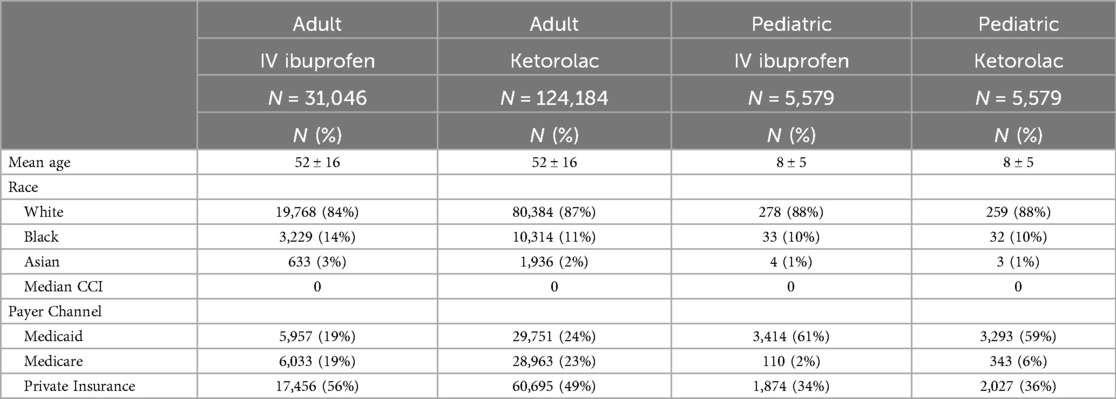
Table 1. Demographics adult and pediatric after matching.
In the pediatric population, 5,579 patients were identified in the IV ibuprofen group and matched (1:1). The mean dose was 429 ± 340 mg and 25 ± 12 mg for parenteral ibuprofen and ketorolac, respectively in the pediatric population. One dose was administered to 98% of pediatric patients. The pediatric population was slightly more male than females, aged 0–5 years old, received the index drug primarily for pain (both surgical and non-surgical), and had few to no comorbidities (Table 1, Supplementary Table S1).
Within three days of the last dose administered, claims for renal dysfunction events were reduced by 45% (0.34% vs. 0.62%; p < 0.001) in patients that received IV ibuprofen compared to IV/IM ketorolac. GI bleeding events were numerically lower in patients that received IV ibuprofen compared to ketorolac, although no difference statistically. Patients that received IV ibuprofen had a 78% reduction in hematuria (0.28% vs. 1.24%; p < 0.001), 77% reduction in abdominal/pelvic pain claims (2.6% vs. 11%; p < 0.001), 90% reduction in headache claims (0.38% vs. 4%; p < 0.001) and 80% reduction in nausea and vomiting (0.98% vs. 4.9%; p < 0.001) compared to ketorolac (Table 2).

Table 2. Adult incidence of common NSAID ADRs comparing IV ibuprofen to ketorolac.
There were no differences in gastrointestinal bleeding, renal toxicity or lower back pain events. Claims for hematuria were lower by 64% (0.16% vs. 0.47%; p < 0.001). However, claims for abdominal/pelvic pain were lower by 67% (3.5% vs. 10%; p < 0.001), headache by 61% (2.2% vs. 5.7%; p < 0.001), and nausea/vomiting by 51% (4.6% vs. 9.4%; p < 0.001) in patients that received IV ibuprofen compared to IV/IM ketorolac (Table 3).
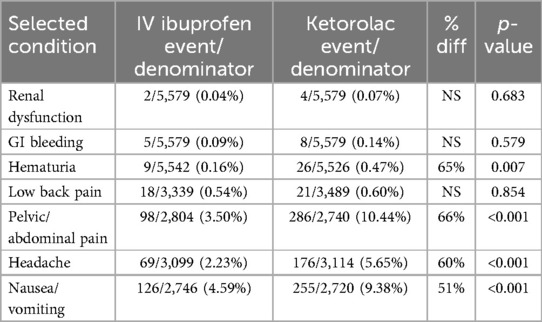
Table 3. Pediatric incidence of common NSAID ADRs comparing IV ibuprofen to ketorolac.
In adult patients, the total HCRU within 29 days following the last dose of drug administration were significantly lower overall in the group that received IV ibuprofen when compared to those that received ketorolac. Length of stay (LOS) decreased by approximately one day (3.1 ± 4.8 vs. 3.8 ± 5.37; p < 0.001) in the IV Ibuprofen arm compared to ketorolac. Hospital visits (81% vs. 83%; p < 0.001), emergency room (ER) visits (7.5% vs. 25%; p < 0.001), and outpatient office visits (29% vs. 38%; p < 0.001) were significantly different among patients that received IV ibuprofen compared to ketorolac. Any inpatient admission however was slightly higher in the IV ibuprofen arm compared to ketorolac (9.1% vs. 8.5%; p = 0.001). There were no significant differences between the two groups in claims for hemodialysis, endoscopy, or transfusion of red blood cells in the 29 day follow up. (Table 4)
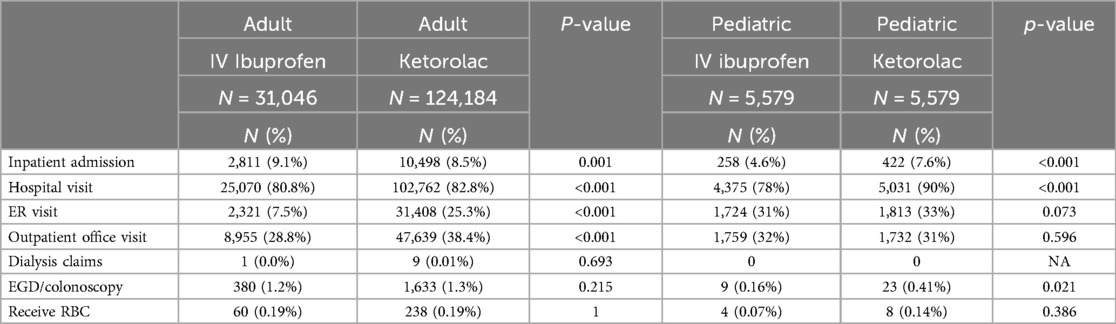
Table 4. HCRU in adult and pediatric patients.
Total HCRU was lower in the IV-ibuprofen arm compared to the ketorolac group among the pediatric patients and was demonstrated by decreased LOS (2.1 ± 2.6 vs. 3.3 ± 4.4;<0.001), fewer hospital visits (78% vs. 90%; p < 0.001) and fewer ER visits (31% vs. 33%; p = 0.005). Significantly more claims for EGDs/colonoscopies were found among those that received ketorolac compared to IV ibuprofen (Table 4).
This retrospective, observational, payer-based database study shows a reduction in major ADRs in both the adult and pediatric groups. Among the adult population, nephrotoxicity was meaningfully reduced in patients that received IV ibuprofen compared to ketorolac, when undergoing a surgical procedure. Other common ADRs that are associated with NSAIDs were also significantly less reported. Reducing ADRs encountered by patients contributes substantially to patient satisfaction, recovery time, and minimizes healthcare resources (1–4).
As described previously, the mechanism of action of non-selective NSAIDs is inhibition of COX-1 and COX-2 pathways which decreases the expression of prostaglandin precursors, including thromboxane and prostacyclin, producing anti-inflammatory and analgesia properties. COX-1 acts primarily in the control of renal glomerular filtration rate (GFR) while COX-2 plays a role in sodium and water excretion. Prostaglandins, particularly PGE2 and PGD2, act as vasodilators in the afferent arterioles, increasing renal perfusion. By inhibiting this pathway, NSAIDs can result in acute vasoconstriction, reduce GFR, and ultimately lead to acute renal injury (21). Risk factors for acute kidney injury associated with NSAIDs include advanced age, systemic arterial hypertension, comorbidities that reduce renal profusion, and dehydration. Although it is anticipated that all NSAIDs carry some risk for acute renal dysfunction, short-term (<5 days) administration of ketorolac has been reported to carry an incidence of 1.1% and longer durations and higher doses at 2.1% (22). Ketorolac also has the highest number of reported cases in the literature and are likely secondary to greater COX-1 inhibition than all other NSAIDs (18, 23–29). It was withdrawn from the market in many countries following association with hemorrhage and renal failure (30). The reported incidence in this study, although lower than previously reported, are still statistically different, favoring fewer renal events with IV ibuprofen than ketorolac. Additionally, although the incidence appears nominal, the costs associated are expected significant. Lastly, there were no differences in claims for hemodialysis suggesting that either the renal dysfunction is reversible or not severe enough to require dialysis.
GI bleeding is one of the adverse effects reported among NSAIDs. Similarly, to renal adverse events, the etiology is secondary to inhibition of the COX isoenzymes, particularly COX-1 inhibition. Gastrointestinal injury ranges from dyspepsia to fatal GI bleeding and perforation. Risk factors for GI bleeding due to NSAIDs include age ≥65, history of previous GI bleed or peptic ulcer disease, concomitant use of aspirin, anticoagulants or corticosteroids, and elevated NSAID dose (31). There is debate as to whether individual NSAIDs carry a greater risk. Ketorolac has attracted attention lately with reports of increased incidence of GI bleeding. Rodrigez et al. compared the relative risk of GI bleeding among individual agents and reported a RR 24.7(9.6–63.5) with ketorolac compared to RR 2.1 (0.6–7.1) with ibuprofen (17). When evaluating doses, ketorolac doses ≤20 mg revealed RR 20.0 (4.3–93.6) and doses >20 mg RR 28.1 (8.7–90.9). Ibuprofen was not considered to carry a statistically significant risk, therefore individual doses were not assessed. In our study however, there was a numerically higher risk of GI bleeding with ketorolac compared to IV ibuprofen in both populations, though not statistically nor probably clinically significant. There were however a statistically higher rate of EGDs/colonoscopy claims in pediatric patients that received ketorolac. Potential reasons may be that clinicians are identifying and monitoring for these ADRs when NSAIDs are administrered, particularly when prescribing ketorolac. Additionally, most pharmacies have employed dose guidance for ketorolac due to the numerous warnings and contraindications, including dose, duration of therapy based on age, renal function. Lastly, clinicians may not be informed about the contraindication of ketorolac in the pediatric population and perhaps utilization in this population is resulting in more GI follow up.
As gastrointestinal toxicity and nephrotoxicity are the most feared ADRs, other side effects must be considered. Both ketorolac and IV ibuprofen demonstrate similar ADRs in >1% of patients (excluding those related to GI bleeding and renal toxicity) including abdominal pain, nausea, vomiting, headache, and prolonged bleeding (8, 12). Therefore each of these were identified through extraction of ICD-9/ICD-10 codes in the post-dose 72-hour timeframe. As prolonged bleeding is not a straightforward payer code, hematuria was identified as a surrogate marker for minor bleeding. Results demonstrated all ADRs identified a priori were statistically reduced in adult patients and in four of the five categories in pediatrics, when IV ibuprofen was compared to ketorolac. It is unclear if these results are based on the direct comparison of ADRs between agents, or due to secondary benefits. For example, if IV ibuprofen reduced opioids in the post-surgical phase vs. ketorolac, this could account for the reduction in nausea, vomiting, and abdominal pain.
Multiple doses, particularly with ketorolac, have been linked with worse side effects. However, given that most patients had 1 dose, we believe dose may not impact ADRs in this study. This is something that can by further explored in futures studies. Prevention of in ADRs is not only important to minimize harm, improve patient satisfaction, and improve outcomes but also to reduce the need for healthcare resources. The resource utilization comparison revealed shorter LOS, reduced outpatient follow up, and fewer ED visits in IV Ibuprofen arm compared to ketorolac.
Specific costs could not be evaluated accurately due to the disparity in payer types. It is well known that negotiated payments are significantly lower in patients with government backed insurers compared to private providers (32). As a significantly higher proportion of adult patients that received ketorolac had Medicare or Medicaid, and more that received IV Ibuprofen had private commercial plans, the costs could not be accurately calculated.
Surgical bleeding is another concern when utilizing NSAIDs, particularly when administered pre- or intra-operatively. Both ketorolac and IV ibuprofen appear to be safe when administered post-operatively (14, 33–41). Only IV ibuprofen has demonstrated safety when administered pre-operatively (14, 15, 42–44). Pre-emptive ketorolac resulted in increased bleeding post-operatively and therefore is contraindicated to be administered in this manner (8, 45). The majority of the patients identified in this cohort were administered either ketorolac or IV ibuprofen for surgical pain. Post-surgical bleeding would naturally be a safety end point to evaluate; however, collecting payer data that could determine if the agent was given pre or post-procedure proved to be not possible. Also, determining the incidence of post-operative bleeding is not based on predetermined or clear ICD-9/ICP-10 coding. If there were a difference in post-operative bleeding among groups, they did not require a difference in transfusions of RBCs, indicating either bleeding was not different and/or was not serious or life-threatening.
Certain limitations are associated with claims data use. The presence of a diagnosis code on a medical claim is not a positive presence of disease, as the diagnosis code may be incorrectly coded or included as rule-out criteria rather than the actual disease. Additionally, administrative claims data do not contain clinical variables, such as weight, which would have been valuable in the pediatric population. Lastly, as back pain has been identified in both IV ibuprofen and ketorolac as a common side effect, it cannot be ruled out that these claims were coded as ADR rather than reason for drug administration.
This real-world evidence study is the first to compare IV ibuprofen and ketorolac using an all-payor database which demonstrated that IV ibuprofen reduced the incidence of unfavorable outcomes and was associated with less healthcare utilization. Results revealed a significant reduction in renal dysfunction, hematuria, abdominal/pelvic pain, headache, nausea/vomiting, LOS, and outpatient costs in the adult population that received IV ibuprofen compared to ketorolac. Inpatient visits were higher however in the IV ibuprofen arm. The pediatric population also showed a reduction in abdominal/pelvic pain, headache, nausea/vomiting, LOS and overall HCRU, including reduction in EGD/colonoscopies in the 29-day follow up timeframe. In summary, the results of this study highlight the potential for IV ibuprofen to offer a safer compared to ketorolac, while reducing the burden on healthcare systems.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article because existing dataset from all-payor database utilized. No identifiable data.
MA: Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Validation, Writing – review & editing. JR-S: Data curation, Formal Analysis, Investigation, Software, Validation, Writing – review & editing. IC: Data curation, Formal Analysis, Investigation, Software, Validation, Writing – review & editing. IM-P: Funding acquisition, Investigation, Validation, Writing – review & editing. JM: Funding acquisition, Investigation, Validation, Writing – review & editing. ED: Funding acquisition, Investigation, Validation, Visualization, Writing – review & editing. TH: Conceptualization, Funding acquisition, Investigation, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Supported by Cumberland Pharmaceuticals.
MA, JR-S and IC were employed by STATinMED, LLC.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2024.1484948/full#supplementary-material
1. Olsen S, Neale G, Schwab K, Psaila B, Patel T, Chapman EJ, et al. Hospital staff should use more than one method to detect adverse events and potential adverse events: incident reporting, pharmacist surveillance and local real-time record review may all have a place. Qual Saf Health Care. (2007) 16(1):40–4. doi: 10.1136/qshc.2005.017616
2. Pirmohamed M, James S, Meakin S, Green C, Scott AK, Walley TJ, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. Br Med J. (2004) 329(7456):15–9. doi: 10.1136/bmj.329.7456.15
3. Aronson JK. Distinguishing hazards and harms, adverse drug effects and adverse drug reactions: implications for drug development, clinical trials, pharmacovigilance, biomarkers, and monitoring. Drug Saf. (2013) 36(3):147–53. doi: 10.1007/s40264-013-0019-9
4. Coleman JJ, Pontefract SK. Adverse drug reactions. Clin Med (Lond). (2016) 16(5):481–5. doi: 10.7861/clinmedicine.16-5-481
5. Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. (1998) 279(15):1200–5. doi: 10.1001/jama.279.15.1200
6. Sultana J, Cutroneo P, Trifiro G. Clinical and economic burden of adverse drug reactions. J Pharmacol Pharmacother. (2013) 4(Suppl 1):S73–7. doi: 10.4103/0976-500X.120957
7. Rolfes L, van Hunsel F, Taxis K, van Puijenbroek E. The impact of experiencing adverse drug reactions on the patient’s quality of life: a retrospective cross-sectional study in The Netherlands. Drug Saf. (2016) 39(8):769–76. doi: 10.1007/s40264-016-0422-0
8. Ketorolac Package insert. Deerfield, IL: Baxter Healthcare Corporation (2018). https://www.baxterpi.com/pi-pdf/Ketorolac+PI_Nov+2018.pdf
9. Gillis JC, Brogden RN. Ketorolac. A reappraisal of its pharmacodynamic and pharmacokinetic properties and therapeutic use in pain management. Drugs. (1997) 53(1):139–88. doi: 10.2165/00003495-199753010-00012
10. Sheth KR, Bernthal NM, Ho HS, Bergese SD, Apfel CC, Stoicea N, et al. Perioperative bleeding and non-steroidal anti-inflammatory drugs: an evidence-based literature review, and current clinical appraisal. Medicine (Baltimore). (2020) 99(31):e20042. doi: 10.1097/MD.0000000000020042
11. Camu F, Vanlersberghe C, Lauwers MH. Timing of perioperative non-steroidal anti-inflammatory drug treatment. Acta Anaesthesiol Belg. (1996) 47(3):125–8.8959197
13. Glover CD, Berkenbosch JW, Taylor MB, Patel NV, Kaelin B, Gibson BHY, et al. A multi-center evaluation of the pharmacokinetics and safety of intravenous ibuprofen in infants 1-6 months of age. Paediatr Drugs. (2023) 25(5):585–93. doi: 10.1007/s40272-023-00576-9
14. Uribe AA, Arbona FL, Flanigan DC, Kaeding CC, Palettas M, Bergese SD. Comparing the efficacy of IV ibuprofen and ketorolac in the management of postoperative pain following arthroscopic knee surgery. A randomized double-blind active comparator pilot study. Front Surg. (2018) 5:59. doi: 10.3389/fsurg.2018.00059
15. Le V, Kurnutala L, SchianodiCola J, Ahmed K, Yarmush J, Daniel Eloy J, et al. Premedication with intravenous ibuprofen improves recovery characteristics and stress response in adults undergoing laparoscopic cholecystectomy: a randomized controlled trial. Pain Med. (2016) 17(6):1163–73. doi: 10.1093/pm/pnv113
16. Tulunay FC. NSAIDs: behind the mechanisms of action. Funct Neurol. (2000) 15(Suppl 3):202–7.11200793
17. Garcia Rodriguez LA, Cattaruzzi C, Troncon MG, Agostinis L. Risk of hospitalization for upper gastrointestinal tract bleeding associated with ketorolac, other nonsteroidal anti-inflammatory drugs, calcium antagonists, and other antihypertensive drugs. Arch Intern Med. (1998) 158(1):33–9. doi: 10.1001/archinte.158.1.33
18. Perazella MA, Buller GK. NSAID nephrotoxicity revisited: acute renal failure due to parenteral ketorolac. South Med J. (1993) 86(12):1421–4. doi: 10.1097/00007611-199312000-00025
19. Warner TD, Giuliano F, Vojnovic I, Bukasa A, Mitchell JA, Vane JR. Nonsteroid drug selectivities for cyclo-oxygenase-1 rather than cyclo-oxygenase-2 are associated with human gastrointestinal toxicity: a full in vitro analysis. Proc Natl Acad Sci U S A. (1999) 96(13):7563–8. doi: 10.1073/pnas.96.13.7563
20. Castellsague J, Riera-Guardia N, Calingaert B, Varas-Lorenzo C, Fourrier-Reglat A, Nicotra F, et al. Safety of non-steroidal anti-inflammatory drugs P. individual NSAIDs and upper gastrointestinal complications: a systematic review and meta-analysis of observational studies (the SOS project). Drug Saf. (2012) 35(12):1127–46. doi: 10.1007/BF03261999
21. Lucas GNC, Leitao ACC, Alencar RL, Xavier RMF, Daher EF, Silva Junior GBD. Pathophysiological aspects of nephropathy caused by non-steroidal anti-inflammatory drugs. J Bras Nefrol. (2019) 41(1):124–30. doi: 10.1590/2175-8239-jbn-2018-0107
22. Feldman HI, Kinman JL, Berlin JA, Hennessy S, Kimmel SE, Farrar J, et al. Parenteral ketorolac: the risk for acute renal failure. Ann Intern Med. (1997) 126(3):193–9. doi: 10.7326/0003-4819-126-3-199702010-00003
23. Schoch PH, Ranno A, North DS. Acute renal failure in an elderly woman following intramuscular ketorolac administration. Ann Pharmacother. (1992) 26(10):1233–6. doi: 10.1177/106002809202601007
24. Corelli RL, Gericke KR. Renal insufficiency associated with intramuscular administration of ketorolac tromethamine. Ann Pharmacother. (1993) 27(9):1055–7. doi: 10.1177/106002809302700908
25. Buller GK, Perazella MA. Acute renal failure and ketorolac. Ann Intern Med. (1997) 127(6):493–4. doi: 10.7326/0003-4819-127-6-199709150-00022
26. Boras-Uber LA, Brackett NC Jr. Ketorolac-induced acute renal failure. Am J Med. (1992) 92(4):450–2. doi: 10.1016/0002-9343(92)90283-H
27. Haragsim L, Dalal R, Bagga H, Bastani B. Ketorolac-induced acute renal failure and hyperkalemia: report of three cases. Am J Kidney Dis. (1994) 24(4):578–80. doi: 10.1016/S0272-6386(12)80215-0
28. Quan DJ, Kayser SR. Ketorolac induced acute renal failure following a single dose. J Toxicol Clin Toxicol. (1994) 32(3):305–9. doi: 10.3109/15563659409017963
29. Fong J, Gora ML. Reversible renal insufficiency following ketorolac therapy. Ann Pharmacother. (1993) 27(4):510–2. doi: 10.1177/106002809302700422
31. Laine L. GI risk and risk factors of NSAIDs. J Cardiovasc Pharmacol. (2006) 47(Suppl 1):S60–66. doi: 10.1097/00005344-200605001-00011
32. Baker L, Kate Bundorf M, Devlin A, Kessler D. Why don't commerical health plans use prospective payments? Am J Health Econ. (2019) 5(1):465–80. doi: 10.1162/ajhe_a_00127
33. Gobble RM, Hoang HLT, Kachniarz B, Orgill DP. Ketorolac does not increase perioperative bleeding: a meta-analysis of randomized controlled trials. Plast Reconstr Surg. (2014) 133(3):741–55. doi: 10.1097/01.prs.0000438459.60474.b5
34. Fragen RJ, Stulberg SD, Wixson R, Glisson S, Librojo E. Effect of ketorolac tromethamine on bleeding and on requirements for analgesia after total knee arthroplasty. J Bone Joint Surg Am. (1995) 77(7):998–1002. doi: 10.2106/00004623-199507000-00004
35. Southworth SR, Woodward EJ, Peng A, Rock AD. An integrated safety analysis of intravenous ibuprofen (caldolor((R))) in adults. J Pain Res. (2015) 8:753–65. doi: 10.2147/JPR.S93547
36. Weisz RD, Fokin AA, Lerner V, Flynt A, Macias-Perez I, Pavliv L, et al. Intravenous ibuprofen reduces opioid consumption during the initial 48 hours after injury in orthopedic trauma patients. J Orthop Trauma. (2020) 34(7):341–7. doi: 10.1097/BOT.0000000000001733
37. Erdogan Kayhan G, Sanli M, Ozgul U, Kirteke R, Yologlu S. Comparison of intravenous ibuprofen and Acetaminophen for postoperative multimodal pain management in bariatric surgery: a randomized controlled trial. J Clin Anesth. (2018) 50:5–11. doi: 10.1016/j.jclinane.2018.06.030
38. Gago Martinez A, Escontrela Rodriguez B, Planas Roca A, Martinez Ruiz A. Intravenous ibuprofen for treatment of post-operative pain: a multicenter, double blind, placebo-controlled, randomized clinical trial. PLoS One. (2016) 11(5):e0154004. doi: 10.1371/journal.pone.0154004
39. Kroll PB, Meadows L, Rock A, Pavliv L. A multicenter, randomized, double-blind, placebo-controlled trial of intravenous ibuprofen (i.v.-ibuprofen) in the management of postoperative pain following abdominal hysterectomy. Pain Pract. (2011) 11(1):23–32. doi: 10.1111/j.1533-2500.2010.00402.x
40. Shepherd DM, Jahnke H, White WL, Little AS. Randomized, double-blinded, placebo-controlled trial comparing two multimodal opioid-minimizing pain management regimens following transsphenoidal surgery. J Neurosurg. (2018) 128(2):444–51. doi: 10.3171/2016.10.JNS161355
41. Southworth S, Peters J, Rock A, Pavliv L. A multicenter, randomized, double-blind, placebo-controlled trial of intravenous ibuprofen 400 and 800 mg every 6 h in the management of postoperative pain. Clin Ther. (2009) 31(9):1922–35. doi: 10.1016/j.clinthera.2009.08.026
42. Moss JR, Watcha MF, Bendel LP, McCarthy DL, Witham SL, Glover CD. A multicenter, randomized, double-blind placebo-controlled, single dose trial of the safety and efficacy of intravenous ibuprofen for treatment of pain in pediatric patients undergoing tonsillectomy. Paediatr Anaesth. (2014) 24(5):483–9. doi: 10.1111/pan.12381
43. Patel NK, Shah SJ, Lee NK, Gao Q, Carullo VP, Yang CJ. Intraoperative intravenous ibuprofen use is not associated with increased post-tonsillectomy bleeding. Int J Pediatr Otorhinolaryngol. (2020) 133:109965. doi: 10.1016/j.ijporl.2020.109965
44. Viswanath A, Oreadi D, Finkelman M, Klein G, Papageorge M. Does pre-emptive administration of intravenous ibuprofen (caldolor) or intravenous Acetaminophen (ofirmev) reduce postoperative pain and subsequent narcotic consumption after third molar surgery? J Oral Maxillofac Surg. (2019) 77(2):262–70. doi: 10.1016/j.joms.2018.09.010
Keywords: NSAID, adverse drug reaction (ADR), intravenous ibuprofen, ketorolac, side effect, healthcare resource utilization, patient safety
Citation: Afolabi M, Rodriguez-Silva J, Chopra I, Macias-Perez I, Makii J, Durr E and Human T (2025) Real-world evaluation of select adverse drug reactions and healthcare utilization associated with parenteral Ibuprofen and ketorolac in adult and pediatric patients. Front. Pain Res. 5:1484948. doi: 10.3389/fpain.2024.1484948
Received: 23 August 2024; Accepted: 31 October 2024;
Published: 7 January 2025.
Edited by:
Carl-Olav Stiller, Karolinska Institutet (KI), SwedenReviewed by:
Dmytro Dmytriiev, National Pirogov Memorial Medical University, UkraineCopyright: © 2025 Afolabi, Rodriguez-Silva, Chopra, Macias-Perez, Makii, Durr and Human. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Theresa Human, dGh1bWFuQGN1bWJlcmxhbmRwaGFybWEuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.