 Santiago Galán1,2
Santiago Galán1,2 Rocío de la Vega1,3*
Rocío de la Vega1,3* Rosa Esteve1,3
Rosa Esteve1,3 Alicia E. López-Martínez1,3
Alicia E. López-Martínez1,3 Mariano Fernández Baena4
Mariano Fernández Baena4 Carmen Ramírez-Maestre1,3
Carmen Ramírez-Maestre1,3
- 1Instituto de Investigación Biomédica de Málaga (IBIMA Plataforma BIONAND), Málaga, Spain
- 2Red de Investigación en Cronicidad, Atención Primaria y Prevención y Promoción de la Salud (RICAPPS), Málaga, Spain
- 3Personalidad, Evaluación y tratamiento Psicológico, Facultad de Psicología y Logopedia, Andalucía Tech, Universidad de Málaga (Spain), Málaga, Spain
- 4Unidad del Dolor, Hospital Regional de Málaga, Málaga, Spain
Background: Opioids are being prescribed widely, and increasingly, for the treatment of chronic non-cancer pain (CNCP). However, several side effects are associated with mid- and long-term opioid use and, for certain patients, with the risk of problematic opioid use. The aim of this study is to know the perception of the physicians about which variables could be associated with increased risk of patients with CNCP developing a problem of abuse or misuse of the prescribed opioid medication.
Methods: Twenty-nine physicians with experience in CNCP pain management and opioids prescription participated in a two-round Delphi study focused on the risk factors for opioid misuse and abuse.
Results: The variables that reached consensus regarding their relationship with the increased risk of suffering a problem of opioid abuse or misuse were: (1) Experiencing pain on a daily basis, (2) previous use of high-dose opioids, (3) generalized anxiety, (4) hopelessness, (5) benzodiazepine intake, (6) use of opioids for reasons other than pain, (7) family problems, family instability or family breakdown, and (8) having access to several opioid prescribers. The only variable that reached consensus regarding it not being associated to a possible risk of abuse or misuse was having mild pain intensity (0–4 on a NRS-11).
Conclusions: This study provides useful information that could help make decisions about the use of opioids for CNCP treatment and prevent future difficulties. Prospective studies testing the relationship of the variables that reached consensus with the risk of opioid misuse and abuse are warranted.
Significance: This study shows the variables of CNCP that the professional must take into account in order to avoid possible problems when prescribing opioids.
Introduction
Chronic non-cancer pain (CNCP) is defined as pain lasting or recurring for more than 3 months that is not due to a malignancy (1) and it has as a consequence a reduction in quality and quantity of life (2). It is a common problem, affecting more than 1 in 5 adults in America and resulting in elevated social costs (3). In Europe, the 1-month prevalence of moderate-to-severe CNCP reached 19% (4).
Despite multidisciplinary treatments being recommended as a first option of treatment (5, 6), opioids are being prescribed widely, and increasingly, for chronic pain management (7, 8). In Spain, the annual number of patients receiving at least one opioid prescription more than doubled, reaching to 722,838 in 2018 (9). The decision of conducting opioid prescription is not exclusively based on pain characteristics. Certain patient factors influence physicians’ decisions on using opioids, for example: being a woman (10), being older, reporting higher levels of pain intensity and depressive symptoms, reporting lower levels of pain-acceptance (10, 11), patients’ nonverbal communications of pain, distress, and suffering (12), patient´s trustworthiness, race and ethnicity, and the concern for risk of misuse (13), among others.
Unfortunately, a number of side effects, such as constipation, dizziness, and nausea, and serious side effects, such as addiction, are associated with the medium- and long-term use of opioids for CNCP (1, 14). The professional prescribing the opioids is also related to the risk of presenting side effects. For example, in comparation with other specialists, prescriptions from Primary Care providers have been associated with higher rates of opioid overdose deaths (15). Physicians’ knowledge of risk factors is also a variable to consider. Several studies have shown the relationship between the lack of knowledge of clinicians and stigma and also with a worse approach to long-term treatment (16, 17). Additionally, the use of opioids is controversial because of the risk of problematic opioid use (18) and the elevated risk of abuse and/or misuse (19). Misuse is defined as the use of opioid in a way that is different to the directed pattern of use, without considering the presence or absence of harm or adverse effects, and abuse is defined as the intentional use of the opioid for a nonmedical purpose, such as relaxation or altering one’s state of consciousness (20).
It has been shown that this risk is not the same for all patients; biopsychosocial patient factors such as: civil status, pain duration, mental health-related quality of life, and cigarette smoking, are associated with the risk of opioid abuse (21). Higher anxiety and depression levels have also shown to be significantly associated with increased opioid misuse (22) and also the presence of psychological disorders, such as post-traumatic stress disorder (PTSD) (5). However, there is a lack of research that provides a comprehensive overview of these variables.
A current systematic review have found a lack of consistent findings on the risk factors related to concurrent chronic pain and substance misuse (23). Given the lack of research, a Delphi methodology can provide evidence by generating consensus by a group of experts (24, 25). Therefore, we conducted a Delphi study to evaluate physicians’ perception regarding which variables could be associated with an increased risk of patients with CNCP developing a problem of abuse or misuse of the prescribed opioid medication.
Material and method
Study design
We conducted a Delphi study to address our aims. A Delphi method involves finding a group of experts in a specific topic and then asking them their opinions about a question of interest, in different and anonymous rounds. This method is frequently used to provide the most accurate answers to hard-to-answer questions (26, 27).
Participants
In order to be eligible to participate as an expert, participants were required to: (1) attend patients with CNCP, (2) have expertise in opioid prescribing for chronic pain, and (3) speak Spanish. We used the snowball procedure to recruit experts into the Delphi panel (28). We first identified two experts who work in a Pain Clinic and we asked them to identify other experts who might be interested in participating. The group of experts should not be less than seven and the maximum is considered around 30 (29).
Measures and procedures
This study was approved by the Institutional Ethics Review Board of the University of Málaga (CEUMA 66-2019-H) and the Regional Hospital Ethics Committee (CEI181021). It was conducted in accordance with the Declaration of Helsinki and Law 14/2007, of July 3, on Biomedical Research. The study information was sent via email or WhatsApp to potential participants. In this information, a link providing access to the informed consent form and the survey questions was added. The entire Delphi process occurred online via LimeSurvey. Participants did not receive any compensation for their time. Two rounds were needed to achieve consensus. Participants were the same in both rounds. Participating experts did not know the identity of the other members of the panel. Each round remained open for 1 month, and fortnightly reminder emails were sent. Two reminders per round were sent.
Round I
First, basic demographic and professional information was collected from the participants: age, sex, type of work center, position, years of experience and opioid prescription frequency. Using open-ended questions, panelists were then asked to identify all the variables that could be associated to the fact that a patient with CNCP could develop a problem of abuse or misuse of the prescribed opioid medication.
Round II
We presented all participants that had responded to Round I with the categories and items created in Round I. Participants were asked to rate the magnitude of the association of each item with an increased risk of suffering a problem of abuse or misuse on a scale of 1–10 (1 = Not at all associated, 10 = Extremely associated). The experts had the option to include new items if they considered that information was missing.
Data analysis
Round I
We used means and ranges for continuous variables and numbers and percentages for categorical variables to summarize demographic and descriptive data from the study participants. We used the constant comparative analysis method (30) to qualitatively analyze and categorize data from the Round I open-ended question about the variables that could be associated to the fact that a CNCP could develop a problem of abuse or misuse of the prescribed opioid medication. Two of the authors (SG and RV) created the categories independently. Any disagreement was resolved by consensus. Those categories were then presented to the participants in Round II.
Round II
We recoded the ratings on the 1–10 scale as follows: responses ≤3 as “Not associated”, 4–7 as “Uncertain association”, and ≥8 as “Associated”.
We fist defined disagreement with the idea that a particular variable is related to increased risk of developing an opioid abuse or misuse problem if one-third or more participants responded in the “Not associated” range and one-third in the “Associated” range. Consensus was defined as the absence of disagreement. In the same line, at least 75% of the participants needed to respond with “Associated”, or “Not associated”, to determine that consensus was achieved for that item. This criterion is based on the median threshold used to define consensus in the Delphi method (31).
Results
Round I
Twenty-nine physicians based in Spain participated in the first Delphi round, 66% of these were men. The majority (83%), worked at a hospital and 66% were pain specialists. Their mean age was 38.2 years. Table 1 summarizes additional details regarding the demographic characteristics of the Round I participants.
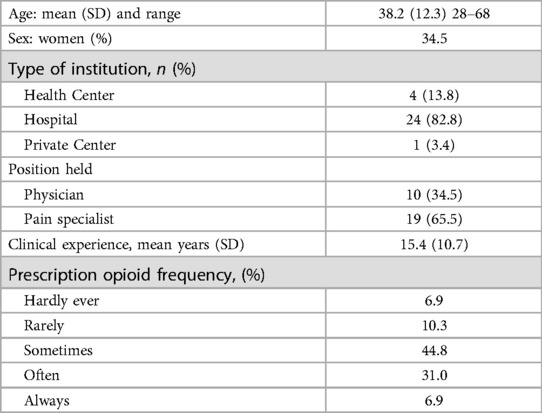
Table 1. Characteristics of participants from round I (n = 29).
Eleven categories were created from the answers obtained in the Round I open-ended question: (1) patient’s sociodemographic variables, (2) diagnoses and types of pain, (3) pain characteristics, 4) having other pathologies or diagnoses (different from the one that directly causes pain), (5) previous treatments that the patient had received for pain, (6) psychiatric history, (7) intellectual level, (8) psychological aspects that can influence the subjective perception of pain, (9) behaviors that the patient had had in the past, (10) possible alarm signs that the professional might observe in the patient’s behavior at the clinic visit, and (11) current circumstances surrounding the patient. The results of Round I are summarized in Table 2.

Table 2. Results from round I.
Round II
Eighteen physicians (62%) of Round I participated in Round II. Despite being offered the option to add new information that had not been collected in the results of Round I, participants did not provide any new items. On the other hand, there was no disagreement between the participants, that is, no items were marked as unassociated by one-third or more participant responses AND one-third as associated by one-third participant responses.
The variables that reached consensus regarding their relationship with the increased risk of suffering a problem of opioid abuse or misuse were: (1) experiencing pain on a daily basis, (2) previous use of high-dose opioids, (3) generalized anxiety, (4) hopelessness, (5) benzodiazepine intake, (6) use of opioids for reasons other than pain, (7) family problems, family instability or family breakdown, and (8) having access to several opioid prescribers. The only variable that reached consensus regarding it not being associated to a possible risk of abuse or misuse was having mild pain intensity [0–4 on a Numerical Rating Scale (NRS-11)]. Finally, there were a number of variables that reached consensus regarding an uncertain association: (1) Medium education level, (2) type of pain: chronic nociceptive pain, (3) moderate pain Intensity, (4) pain duration from 6 months to a year, and (5) medium or (6) high intellectual level. The percentage item scores of each item are presented in Table 3.
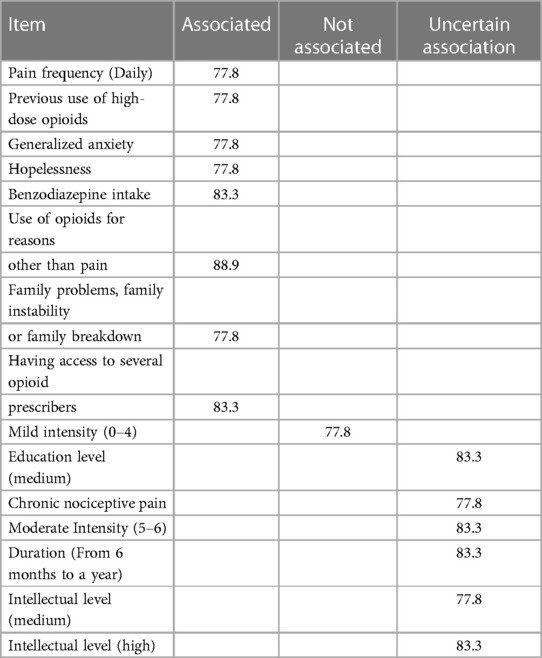
Table 3. Results from round II.
Discussion
In this study, we used a Delphi method to better understand the variables that could be associated with the risk that a patient with CNCP could develop a problem of abuse or misuse of the prescribed opioid medication.
Based on the patient’s history, there are a number of variables that the participating experts agreed that could be playing a role on opioid abuse or misuse risk. These variables were: having generalized anxiety, previous use of high-dose opioids and/or using of opioids for reasons other than pain (e.g., to sleep, to relax) and benzodiazepine intake. Those variables can be easily screened for by checking the patient’s medical record.
In line with the experts’ opinion, the association between the risk of opioid abuse or misuse and mental disorders has been well documented in the literature. For example, patients who report higher levels of psychological distress (anxiety and/or depression) and symptoms of a psychological disorder such as PTSD tend to be at higher risk of opioid misuse (5, 11, 22, 32, 33). Additionally, the history of use of high doses of opioids and benzodiazepines, or of opioids for other uses than those related to pain, are in line with the results obtained in other studies such as Skurtveit et al. with a sample of 17,074 participants. They suggest that earlier use of benzodiazepines may predict repeated use of opioids (34). In the same line, the results obtained by Cheatle et al. show that taking multiple doses of prescribed opioids together is related with misuse (35). But, not only in the past, a current opioid prescription has shown to increase the risk for opioid misuse (36, 37).
Based on the patient´s current circumstances, the variables that obtained the greatest consensus in our study were: a daily presentation of pain, having feelings of hopelessness, family problems, family instability or family breakdown, and having access to several opioid prescribers (e.g., private and public insurance, pain clinic, etc.).
Previous studies have evaluated the relationship between pain duration and the risk of abuse or misuse. In a longitudinal study, pain frequency appeared to be associated with an increased risk for opioid abuse or misuse /dependence, specifically, when the participant had been in pain for more than 16 days (6).
Our expert group agreed to find hopelessness related to the risk of opioid abuse or misuse. We have not found studies that link hopelessness with the risk of abuse or misuse (or to point to the opposite direction). However, there are studies that show the relationship between hopelessness and depression (38) and we have already shown the close relationship between depression and abuse or misuse, so we should consider assessing hopelessness as a potential risk factor. In addition, there are findings showing that hopelessness and substance abuse are related to PTSD symptoms severity (39). In fact, our results showed that the expert panel agreed to consider generalized anxiety and benzodiazepine intake as variables related with the increased risk of suffering a problem of opioid abuse or misuse. These variables have also been associated with PTSD (5).
Family problems, family instability or family breakdown have also been studied previously. A recent study with a sample of 8,103 students found that those who have family problems were significantly more likely to misuse opioids than students who did not report experiencing these relationship problems (40).
Finally, our expert group pointed out having access to several opioid prescribers as a risk variable. The study of Adewumi et al. is in line with these results and it also concludes that high doses of opioids at the start of treatment and low socioeconomic status are related to a high probability of having multiple prescribers (41).
Interestingly, our expert group agreed to find “mild pain intensity” as a non-risk variable. This finding is compatible with the work by Ives et al. and Cózar et al., that found no relationship between pain scores and opioid misuse (42).
The current study has several limitations that should be taken into consideration. Most of our results come from participants who work in the hospital setting (83%); No information on the level of training that experts had in addiction to opioid treatment was recorded. We do not know if these results would be the same if we had had more opinions from professionals from other fields such as primary healthcare centers or from other countries. This fact could also explain why some variables did not emerge, despite of that recent literature has pointed them out as key risk factors in predicting opioid abuse (e. g., the appearance of withdrawal symptoms and/or craving) (43–45).Therefore, future research could replicate these results considering the inclusion of this sample.
Future lines of research should: (1) evaluate the variables proposed by the experts and confirm whether there is real future risk of abuse or misuse in a prospective study and, (2) create and validate a questionnaire collecting the variables found in order to evaluate them systematically and easily.
Regarding the clinical practice, these findings may be useful for training physicians who prescribe or follow-up chronic pain patients using opioids to identify and minimize the risks associated with long-term opioid prescriptions. Furthermore, hospitals may benefit from screening their patients’ clinical records to look for the potential risk factors (e.g., prior opioid or benzodiazepine prescriptions) as well as considering conducting interviews with them to asses potentially negative current situations (e.g., family problems) or administering questionnaires to assess psychological variables (e.g., feelings of hopelessness) and, of course, assessing pain (intensity and frequency). As a result of this, additional monitoring could be put in place to follow-up on patients considered “at risk” in light of these variables.
Despite the dangers associated with the use of opioids in the treatment of CNCP, they are widely used. Clinicians have a very important role in this issue. This study provides useful information that could help them make decisions about the prescription of opioids for CNCP treatment and to monitor patients at risk of misuse and abuse, in order to prevent future difficulties.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was approved by the Institutional Ethics Review Board of the University of Málaga (CEUMA 66-2019-H) and the Regional Hospital Ethics Committee (CEI181021). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SG: Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review and editing. RV: Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review and editing. RE: Investigation, Methodology, Writing – review and editing. AL-M: Investigation, Methodology, Writing – review and editing. MF: Investigation, Writing – review and editing. CR-M: Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was partly funded by grants from the Spanish Ministry of Science and Competitiveness, PID2019-106086RB-I00; the Regional Government of Andalusia, UMA20-FEDERJA-118. SG’s salary is supported by a Sara Borrell grant (CD19/00022), from ISCIII; RV’s salary is supported by a RYC2018-024722-I from the Spanish Ministry of Science and Innovation.
Acknowledgments
The authors thank M.A. for their feedback and support. The authors are also grateful to all the professionals who participated in the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Els C, Jackson TD, Kunyk D, Lappi VG, Sonnenberg B, Hagtvedt R, et al. Adverse events associated with medium- and long-term use of opioids for chronic non-cancer pain: an overview of cochrane reviews. Cochrane Database Syst Rev. (2017) 2017:CD012509. doi: 10.1002/14651858.CD012509.pub2
2. Andrew R, Derry S, Taylor RS, Straube S, Phillips CJ. The costs and consequences of adequately managed chronic non-cancer pain and chronic neuropathic pain. Pain Pract. (2014) 14:79–94. doi: 10.1111/papr.12050
3. Yong RJ, Mullins PM, Bhattacharyya N. Prevalence of chronic pain among adults in the United States. Pain. (2022) 163(2):E328–32. doi: 10.1097/j.pain.0000000000002291
4. Reid KJ, Harker J, Bala MM, Truyers C, Kellen E, Bekkering GE, et al. Epidemiology of chronic non-cancer pain in Europe: narrative review of prevalence, pain treatments and pain impact. Curr Med Res Opin. (2011) 27(2):449–62. doi: 10.1185/03007995.2010.545813
5. López-Martínez AE, Reyes-Pérez Á, Serrano-Ibáñez ER, Esteve R, Ramírez-Maestre C. Chronic pain, posttraumatic stress disorder, and opioid intake: a systematic review. World J Clin Cases. (2019) 7(24):4254–69. doi: 10.12998/wjcc.v7.i24.4254
6. Edlund MJ, Sullivan MD, Han X, Booth BM. Days with pain and substance use disorders. Clin J Pain. (2013) 29(8):689–95. doi: 10.1097/AJP.0b013e318270fa77
7. Kaye AD, Jones MR, Kaye AM, Ripoll JG, Galan V, Beakley BD, et al. Prescription opioid abuse in chronic pain: an updated review of opioid abuse predictors and strategies to curb opioid abuse: part 1. Pain Physician. (2017) 20:S93–109. doi: 10.36076/ppj.2017.s109
8. Reuben DB, Alvanzo AAH, Ashikaga T, Bogat GA, Callahan CM, Ruffing V, et al. National institutes of health pathways to prevention workshop: the role of opioids in the treatment of chronic pain. Ann Intern Med. (2015) 162(4):295–300. doi: 10.7326/M14-2775
9. Hurtado I, García-Sempere A, Peiró S, Sanfélix-Gimeno G. Increasing trends in opioid use from 2010 to 2018 in the region of valencia, Spain: a real-world, population-based study. Front Pharmacol. (2020) 11:612556. [cited 2023 Sep 19]. doi: 10.3389/fphar.2020.612556
10. Tong ST, Hochheimer CJ, Brooks EM, Sabo RT, Jiang V, Day T, et al. Chronic opioid prescribing in primary care: factors and perspectives. Ann Fam Med. (2019) 17(3):200–6. doi: 10.1370/afm.2357
11. Ramírez-Maestre C, Reyes-Pérez Á, Esteve R, López-Martínez AE, Bernardes S, Jensen MP. Opioid pain medication prescription for chronic pain in primary care centers: the roles of pain acceptance, pain intensity, depressive symptoms, pain catastrophizing, sex, and age. Int J Environ Res Public Health. (2020) 17(17):1–15. doi: 10.3390/ijerph17176428
12. Turk DC, Okifuji A. What factors affect physicians’ decisions to prescribe opioids for chronic noncancer pain patients? Clin J Pain. (1997) 13(4):330–6. doi: 10.1097/00002508-199712000-00011
13. Sinnenberg LE, Wanner KJ, Perrone J, Barg FK, Rhodes K V, Meisel ZF. What factors affect physicians’ decisions to prescribe opioids in emergency departments? MDM Policy Pract. (2017) 2(1):238146831668100. doi: 10.1177/2381468316681006
14. Højsted J, Sjøgren P. Addiction to opioids in chronic pain patients: a literature review. Eur J Pain. (2007) 11:490–518. doi: 10.1016/j.ejpain.2006.08.004
15. Porucznik CA, Johnson EM, Rolfs RT, Sauer BC. Specialty of prescribers associated with prescription opioid fatalities in Utah, 2002–2010. Pain Med (United States). (2014) 15(1):73–8. doi: 10.1111/pme.12247
16. Lihi R, Yael D, Silviu B, Anat S, Marsha W, Stacy S, et al. Stigma and level of familiarity with opioid maintenance treatment (OMT) among specialist physicians in Israel. Harm Reduct J. (2023) 20(1):134. [cited 2023 Sep 29]. doi: 10.1186/s12954-023-00869-9
17. Gugala E, Briggs O, Moczygemba LR, Brown CM, Hill LG. Opioid harm reduction: a scoping review of physician and system-level gaps in knowledge, education, and practice. Subst Abus. (2022) 43:972–87. [cited 2023 Sep 29]. doi: 10.1080/08897077.2022.2060423
18. Campbell G, Bruno R, Lintzeris N, Cohen M, Nielsen S, Hall W, et al. Defining problematic pharmaceutical opioid use among people prescribed opioids for chronic noncancer pain: do different measures identify the same patients? Pain. (2016) 157(7):1489–98. doi: 10.1097/j.pain.0000000000000548
19. Volkow ND, Jones EB, Einstein EB, Wargo EM. Prevention and treatment of opioid misuse and addiction: a review. JAMA Psychiatry. (2019) 76(2):208–16. doi: 10.1001/jamapsychiatry.2018.3126
20. Vowles KE, McEntee ML, Julnes PS, Frohe T, Ney JP, Van Der Goes DN. Rates of opioid misuse, abuse, and addiction in chronic pain: a systematic review and data synthesis. Pain. (2015) 156:569–76. doi: 10.1097/01.j.pain.0000460357.01998.f1
21. Pagé MG, Saïdi H, Ware MA, Choinière M. Risk of opioid abuse and biopsychosocial characteristics associated with this risk among chronic pain patients attending a multidisciplinary pain treatment facility. Clin J Pain. (2016) 32(10):859–69. doi: 10.1097/AJP.0000000000000337
22. Esteve R, Marcos E, Reyes-Pérez Á, López-Martínez AE, Ramírez-Maestre C. Pain acceptance creates an emotional context that protects against the misuse of prescription opioids: a study in a sample of patients with chronic noncancer pain. Int J Environ Res Public Health. (2021) 18(6):1–12. doi: 10.3390/ijerph18063054
23. Voon P, Karamouzian M, Kerr T. Chronic pain and opioid misuse: a review of reviews. Subst Abuse Treat Prev Policy. (2017) 12. [cited 2023 Sep 29]. doi: 10.1186/s13011-017-0120-7
24. Keeney S, Hasson F, McKenna H. The delphi technique in nursing and health research. The delphi technique in nursing and health research. Hoboken, NJ, USA: Wiley (2011).
25. Merlin JS, Young SR, Azari S, Becker WC, Liebschutz JM, Pomeranz J, et al. Management of problematic behaviours among individuals on long-term opioid therapy: protocol for a delphi study. BMJ Open. (2016) 6(5):e011619. doi: 10.1136/bmjopen-2016-011619
26. Galán S, de la Vega R, Tomé Pires C, Racine M, Solé E, Jensen MP, et al. What are the needs of adolescents and young adults after a cancer treatment? A Delphi Study. Eur J Cancer Care (Engl). (2017) 26(2):e12488. doi: 10.1111/ecc.12488
27. Humphrey-Murto S, Varpio L, Wood TJ, Gonsalves C, Ufholz LA, Mascioli K, et al. The use of the delphi and other consensus group methods in medical education research: a review. Acad Med. (2017) 92:1491–8. doi: 10.1097/ACM.0000000000001812
28. Snijders TAB. Estimation on the basis of snowball samples: how to weight? Bull MéThodologie Sociol. (1992) 36(1):59–70. doi: 10.1177/075910639203600104
29. Varela-Ruiz M, Díaz-Bravo L, García-Durán R. Descripción y usos del método delphi en investigación del área de la salud. Investig en Eduación Médica. (2012) 1(2):90–5.
30. Miles MB, Huberman AM, Saldana J. Qualitative data analysis: A methods sourcebook. 3rd Ed. Phoenix, AZ, USA: SAGE Publications I (2014). 408.
31. Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of delphi studies. J Clin Epidemiol. (2014) 67(4):401–9. doi: 10.1016/j.jclinepi.2013.12.002
32. Chang Y-P. Factors associated with prescription opioid misuse in adults aged 50 or older. Nurs Outlook. (2018) 66(2):112–20. doi: 10.1016/j.outlook.2017.10.007
33. Manchikanti L, Giordano J, Boswell M V, Fellows B, Manchukonda R, Pampati V. Psychological factors as predictors of opioid abuse and illicit drug use in chronic pain patients. J Opioid Manag. (2007) 3(2):89–100. doi: 10.5055/jom.2007.0045
34. Skurtveit S, Furu K, Bramness J, Selmer R, Tverdal A. Benzodiazepines predict use of opioids—a follow-up study of 17,074 men and women. Pain Med. (2010) 11(6):805–14. doi: 10.1111/j.1526-4637.2010.00870.x
35. Cheatle MD, O’Brien CP, Mathai K, Hansen M, Grasso M, Yi P. Aberrant behaviors in a primary care-based cohort of patients with chronic pain identified as misusing prescription opioids. J Opioid Manag. (2013) 9(5):315–24. doi: 10.5055/jom.2013.0174
36. Hah JM, Sturgeon JA, Zocca J, Sharifzadeh Y, Mackey SC. Factors associated with prescription opioid misuse in a cross-sectional cohort of patients with chronic non-cancer pain. J Pain Res. (2017) 10:979–87. doi: 10.2147/JPR.S131979
37. Setnik B, Roland CL, Sommerville KW, Pixton GC, Berke R, Calkins A, et al. A multicenter, primary care-based, open-label study to identify behaviors related to prescription opioid misuse, abuse, and diversion in opioid-experienced patients with chronic moderate-to-severe pain. J Pain Res. (2015) 8:361–73. doi: 10.2147/JPR.S82396
38. Liu RT, Kleiman EM, Nestor BA, Cheek SM. The hopelessness theory of depression: a quarter-century in review. Clin Psychol Sci Pract. (2015) 22(4):345–65. doi: 10.1111/cpsp.12125
39. Raman U, Bonanno PA, Sachdev D, Govindan A, Dhole A, Salako O, et al. Community violence, PTSD, hopelessness, substance use, and perpetuation of violence in an urban environment. Community Ment Health J. (2021) 57(4):622–30. doi: 10.1007/s10597-020-00691-8
40. Qeadan F, Madden EF, Bern R, Parsinejad N, Porucznik CA, Venner KL, et al. Associations between opioid misuse and social relationship factors among American Indian, Alaska native, and native Hawaiian college students in the U.S. Drug Alcohol Depend. (2021) 222:108667. doi: 10.1016/j.drugalcdep.2021.108667
41. Adewumi AD, Maravilla JC, Alati R, Hollingworth SA, Hu X, Loveday B, et al. Multiple opioid prescribers: a genuine quest for treatment rather than aberrant behaviour. A two-decade population-based study. Addict Behav. (2020) 108:106458. doi: 10.1016/j.addbeh.2020.106458
42. Ives TJ, Chelminski PR, Hammett-Stabler CA, Malone RM, Perhac JS, Potisek NM, et al. Predictors of opioid misuse in patients with chronic pain: a prospective cohort study. BMC Health Serv Res. (2006) 6(1):46. doi: 10.1186/1472-6963-6-46
43. Coloma-Carmona A, Carballo JL, Rodríguez-Marín J, Pérez-Carbonell A. Withdrawal symptoms predict prescription opioid dependence in chronic pain patients. Drug Alcohol Depend. (2019) 195:27–32. [cited 2023 Sep 19]. doi: 10.1016/j.drugalcdep.2018.11.013
44. McHugh RK, Fitzmaurice GM, Carroll KM, Griffin ML, Hill KP, Wasan AD, et al. Assessing craving and its relationship to subsequent prescription opioid use among treatment-seeking prescription opioid dependent patients. Drug Alcohol Depend. (2014) 145:121–6. [cited 2023 Sep 19]. doi: 10.1016/j.drugalcdep.2014.10.002
Keywords: opioid, abuse risk, misuse, Delphi method, chronic pain
Citation: Galán S, de la Vega R, Esteve R, López-Martínez AE, Fernández Baena M and Ramírez-Maestre C (2023) Physicians' perception about predictors of opioid abuse in patients with chronic non-cancer pain: a Delphi study. Front. Pain Res. 4:1269018. doi: 10.3389/fpain.2023.1269018
Received: 28 July 2023; Accepted: 10 October 2023;
Published: 19 October 2023.
Edited by:
Rupesh K. Gautam, Indore Institute of Pharmacy (IIP), IndiaReviewed by:
Thomas J. Martin, Wake Forest University, United StatesJose Luis Carballo, Miguel Hernández University of Elche, Spain
Ainhoa Coloma-Carmona, Miguel Hernández University of Elche, Spain
© 2023 Galán, de la Vega, Esteve, López-Martínez, Fernández Baena and Ramírez-Maestre. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rocío de la Vega cm9jaW8uZGVsYXZlZ2FAdW1hLmVz