
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pain Res., 10 August 2022
Sec. Pain Mechanisms
Volume 3 - 2022 | https://doi.org/10.3389/fpain.2022.943360
This article is part of the Research TopicPerspectives on Music and Pain: from evidence to theory and applicationView all 11 articles
 Susanne Metzner1,2,3*†
Susanne Metzner1,2,3*† Marc N. Jarczok4†
Marc N. Jarczok4† Irina Böckelmann5†
Irina Böckelmann5† Sina Glomb3Manuela Delhey4
Sina Glomb3Manuela Delhey4 Harald Gündel4†Jörg Frommer3†
Harald Gündel4†Jörg Frommer3†Music-imaginative Pain Treatment (MIPT) is a form of music therapy addressing pain experience and affective attitudes toward pain. It includes two self-composed music pieces: one dedicated to the pain experience (pain music, PM) and the other to healing imagination (healing music, HM). Our non-experimental study addresses patients with chronic somatoform pain disorders participating in MIPT. The goal is to gain insight into the direct effect mechanisms of MIPT by combining outcome measures on both the objective physiological and subjective perception levels. The research questions are directed toward changes in pain experience and heart rate variability and their correlations. Thirty-seven hospitalized patients with chronic or somatoform pain disorders receiving MIPT participated in this study. Demographic data and psychometric measures (Symptom Check List SCL90, Childhood Trauma Questionnaire CTQ) were collected to characterize the sample. Subjective pain experience was measured by McGill Pain Questionnaire (SF-MPQ), and Heart Rate Variability by 24 h-ECG. Data analysis shows a reduction of reported pain from MT1 = 19.1 (SD = 7.3) to MT2 = 10.6 (SD = 8.0) in all dimensions of the SF-MPQ. HRV analyses shows a reduced absolute power during PM and HM, while a relative shift in the autonomic system toward higher vagal activity appears during HM. Significant correlations between HRV and MPQ could not be calculated. Findings are interpreted as a physiological correlate to the psychological processes of the patients. Future studies with more participants, a control-group design, and the integration of medium- and long-term effects are recommended.
In the context of pain treatment common music interventions utilize the simple listening to recorded music with the aim to enhance relaxation or distraction in painful situations. In contrast to this, professional music therapy focusses on psychic or interactive processes set in motion by playing music or listening to it. This corresponds to a more active involvement through emotional engagement and cognitive reflection within a therapeutic relationship. This approach is particularly relevant for chronic pain disorders.
In Germany, music therapy has a long tradition as part of the multi-professional treatment of hospitalized patients in departments for psychosomatic medicine (1). According to the national S3-guideline on “non-specific, functional and somatoform physical complaints” (2), music therapy is mentioned as a viable accompanying therapy approach, particularly for severe courses of disease. In this context, Music-imaginative Pain Treatment (MIPT) is an intervention that proves to be increasingly successful. It was initially developed as “entrainment” within a single session (3, 4) and later established as a manualized treatment by Metzner (5).
MIPT makes use of live music. In a room equipped with various musical instruments, the patient develops two pieces of music with the assistance of a trained music therapist. The first composition corresponds to the patient's experience of pain (“pain music”), while the other explores the ideas, or imaginations, of relief (“healing music”). Thereafter the therapist performs the two pieces of music, one after the other, as the patient is listening (application phase). MIPT involves a trusting, supportive therapeutic relationship and thorough verbal processing of what has appeared during the therapy sessions.
By presenting the two compositions one after another in the application phase a shift of pain experience in terms of intensity can be observed but predominantly in terms of the pain's qualitative character. Hauck et al. (6) found different patterns of neuronal activations in healthy subjects depending on which of the two compositions were presented. This correlated with the likewise different pain ratings during listening to PM and HM. Therefore, MIPT flexibilises the pain experience and furthermore the affective attitudes toward the pain. It increases the feeling of self-efficacy and promotes communication skills (7). The modification of the pain experience can be appropriately explained as a 2-folded approach. On one side, a transmodal process links affective-sensory pain with auditive music experience; on the other side, an imaginative activity leads to an assignment of musical symbols to pain (5).
Empirical research of MIPT has focused either on the activation of neuronal processes by MEG resp. EEG-measures (6, 8) or on therapeutic processes by qualitative studies (9, 10). Up to now, outcome studies (3, 11, 12) show promising results, but they are not transferable to patients with somatoform pain disorders, and existing systematic reviews do not include studies on this clientele (13–16).
As music can influence heart rate variability (HRV) (17–19), not solely psychosocial but also (neuro-) physiological effects of MIPT can be assumed. HRV is considered an indicator of autonomic regulation/counter-regulation in patients with chronic pain disorders. Already in 1992, Gebhart and Rendich (20) assumed that the vagal afferents are an integral component of endogenous pain control systems. Koenig et al. (21) conducted a systematic review and meta-analysis on seven studies investigating group differences in vagally mediated HRV-Parameters in patients with headache disorders. The HRV-Parameters RMSSD and HF were reduced, but the authors emphasized the need for further research, as meta-regression analyses on covariates revealed significant differences by clinical etiology, age, gender, and length of HRV recording.
The spectral indices of cardiovascular autonomic control as measured by the spectral analysis of heart period and the mean systolic arterial pressure in women with Fibromyalgia syndrome seem to present good relative reliability. The FMS patients exhibited reduced activation of the sympathetic nervous system (in the LF power, heart rate, and mean arterial pressure) (22). However, a previous study (23) does not indicate dysregulation of spontaneous baroreflex sensitivity.
Our study addresses patients with chronic somatoform pain disorders participating in MIPT. The primary goal is to gain insight into the direct effect mechanisms of MIPT by combining outcome measures on both the objective physiological and subjective perception levels. Our non-experimental study is considered a first step toward collecting quantitative data under naturalistic conditions. Findings of interrelationships between physiological changes during MIPT and short-time positive effects in pain ratings would form the basis for an extensive RCT.
Based on clinical observations, we expected to observe a reduction of sensory and affective pain experience after MIPT. Further, we were concerned with whether this is reflected on a physiological level by an increase in parasympathetic activity. Specifically, the research questions of our study were as follows: 1. Does the experience of pain improve between the start (T1) and the end of MIPT (T2)? 2. Is it possible to measure different response reactions in the autonomic nervous system when the patient listens to his/her two music pieces? 3. Are pain ratings at T2 correlated with changes in HRV-Parameters during MIPT? Based on clinical experience and evidence-based data from HRV changes in healthy subjects, we hypothesized:
H1–Subjective pain experienced at the beginning of MIPT (T1) is significantly improved after listening to the two music pieces (T2).
H2–Parasympathetic activity significantly increases while listening to the second music piece (“healing music”).
H3–Increased parasympathetic activity while listening to the second music piece (“healing music”) correlates negatively to the reduction of pain experienced after MIPT (T2).
This study recruited participants consecutively between 09/2016 and 10/2020 from hospitalized pain patients at the Department of Psychosomatic Medicine and Psychotherapy, University Hospital, Otto-von-Guericke-University Magdeburg, and the Department of Psychosomatic Medicine and Psychotherapy, University Medical Centre Ulm, both in Germany. After the specialist assessment, all patients who met the inclusion criteria were referred to MIPT within the first week of hospitalization. Inclusion criteria were the following primary ICD-10 diagnoses: Chronic pain disorder (F45.40 and F45.41) or somatoform pain disorders (F45.0, F45.1, F45.2, F45.3, F45.8, F45.9). Since this study uses a naturalistic study design, patients who took special heart medication (beta-blockers, ACE inhibitors, antiarrhythmics) or psychotropic drugs and analgesics, including opiates, were not excluded. Medication was systematically documented and taken into account in the data analysis. Exclusion criteria were a diagnosis of acute cardiac arrhythmias and previous participation in MIPT.
The study was approved by the ethics committees of the University Hospital and Medical Faculty of Otto von-Guericke-University Magdeburg (File reference: 179/16) and the University Medical Center Ulm (File reference: 201/18). It was carried out following the recommendation of the ICH-GCP guidelines, Declaration of Helsinki. All participants gave written informed consent before participation.
The participants received MIPT in the initial phase of the inpatient stay as the only music-therapeutic intervention. The intervention follows the manualized four treatment steps, which are usually divided into three sessions of 50 min each (5): 1. structured pain interview; 2. “composition phase”: creating a music piece addressing the pain experience (“pain music” PM) and another music piece addressing imaginations of relief (“healing music” HM); 3. “application phase”: live performance of the self-composed music pieces by the music therapist to the patient combined with 4. subsequent verbal reflection.
Figure 1 shows the course of intervention as follows: Patients were equipped with an ECG-Holter monitor (see below) at a minimum of 4 h before the 3rd MIPT-session (“application phase”) to accommodate the device. The intervention started with a greeting, a short reflection on the current state of health and on PM's and HM's veracity. Then, patients were seated in a comfortable position. Hand signals were agreed upon before the arrangement of the music. They serve as indicators for the beginning, end, tempo, and dynamics because there is no conversation during the music intervention itself. After a resting phase, participants listened to the music pieces performed by the music therapist.
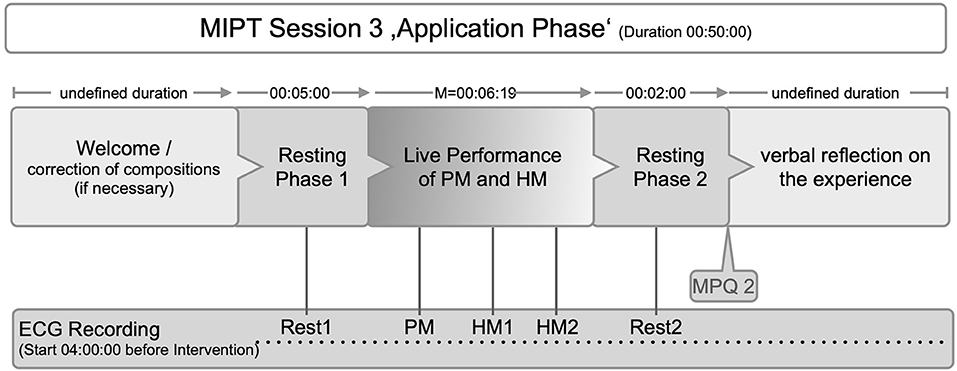
Figure 1. Course of the intervention (ECG, Electrocardiogramm; MPQ 2, McGill Pain Questionaire at T2; PM, pain music; HM, healing music; Rest1/PM/HM1/HM2/Rest2, time points for HRV analyses).
Basic demographic items and potential confounding variables (shift work, chronic medication with influence on the heart rhythm, diabetes mellitus, untreated thyroid diseases and treated thyroid diseases with thyroid blood parameters outside the normal range, cardiac diseases, use of nocturnal oxygen or nightly continuous positive airway pressure) were collected with the MIGA questionnaire (24).
To capture the burden of symptoms in the intervention group immediately after admission to the hospital (T0), we used the following questionnaires: Symptom Check List (SCL90) (25) with 90 items and the German version of the Childhood Trauma Questionnaire (CTQ) (26) with 25 items. The German short version of the McGill Pain Questionnaire (SF-MPQ) (27) measures the subjective pain experience before (T1) and after (T2) MIPT. It records the sensory component (sum of 11 items) and the affective pain qualities (sum of four items).
Live performances of PM and HM during the “application phase” were audiotaped. The duration of the music was calculated to the second. Figure 2 shows the timepoints for the psychometric and musical data collection.
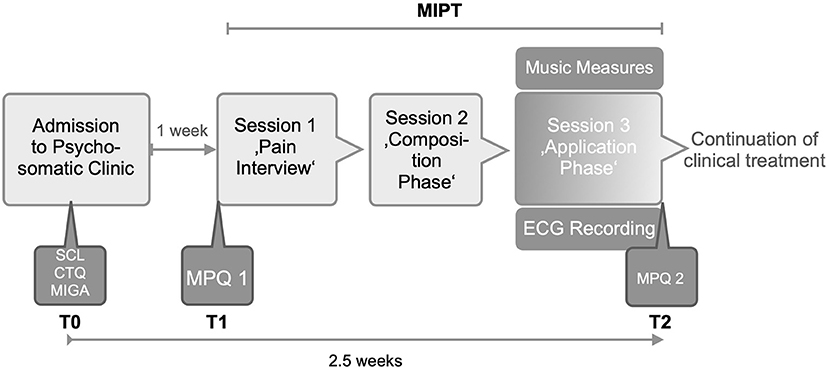
Figure 2. Study design (MIPT, Music-imaginative Pain Treatment; SCL, Symptom Check List; CTQ, Childhood Trauma Questionnaire; MIGA, MIGA Questionnaire; MPQ, McGill Pain Questionnaire; ECG, Electrocardiogramm).
The basis for the HRV analysis were 24-h ECG recordings (model: MT-101 or Medilog® AR12 PLUS Schiller AG, Baar, Switzerland) from voluntary patients who had participated in pain therapy. For this purpose, a 2-channel ECG recording at a sampling rate of 1,000 Hz is stored on the SD card located in the Holter ECG. The raw data RR time series (NN-Interval resp. Normal beat-to-Normal beat) were transferred to the Medilog® DARWIN2 Enterprise analysis software package for the total recording time (artifact correction). The data were checked automatically and visually by a healthcare professional for clinical abnormalities and converted into text files comprising consecutive NN intervals. The subjects completed an activity protocol to note the activities in the following 24 h while wearing the ECG.
The HRV parameters were calculated with the Kubios HRV 3.4.3 software (University of Eastern Finland, Kuopio, Finland). The measuring NN intervals and the HRV analysis correspond to the quality criteria recommendations according to the national and international guidelines (28, 29).
Taking the ECG measurement into account, some experimental modifications had to be introduced, i.e., 5-min rest periods before and after the music. The composition representing the pain experience (PM) is played for at least 2 min, and the composition representing the idea of alleviation (HM) is played immediately afterward for at least 5 min. If the respective music pieces fall below the specified time periods, participants are to be regarded as dropouts due to a lack of evaluability on the HRV markers.
Artifact correction was done with an artifact identification threshold of 0.3 s and a smoothness prior method for detrending NN intervals (Lambda = 500, fc = 0.035 Hz). Mean RR and HRV parameters from time and frequency domains were calculated. Calculated time domain parameters were the standard deviation of NN intervals (SDNN) and the root mean square of successive RR interval difference (RMSSD) in milliseconds. The following frequency domain parameters were calculated using the autoregressive methods (AR): Total power (TP), the low frequency (LF) from 0.04 to 0.15 Hz, and high frequency (HF) from 0.15 to 0.40 Hz. Additionally, the relative power of the HF band (%) was calculated for each experimental phase. Because the shortest experimental phase has a duration of 2 min, the Total Power consisted primarily of HF and LF.
The experimental phases are a resting period before program start (Rest 1), “pain music” period (PM), “healing music” period (HM 1) with first 2 min and last 2 min (HM 2), and resting period at the end (Rest 2) (see Figure 1).
All data were checked for normality using the Shapiro Wilk‘s test. The hypotheses were tested using t-tests for paired (within-subject) and independent (between-group) samples. Similarly, a non-parametric test was applied for paired (Wilcoxon sign rank) and independent (Wilcoxon rank-sum aka Mann-Whitney U test) samples to confirm parametric results. Statistical significance was set to p < 0.05 two-sided. All statistical analyses were calculated using Stata v15.1 SE (Stata Corp. College Station, Texas).
Initially, 51 participants were recruited. This number was reduced by 14 dropouts (1 weak health condition, one refusal of study participation, three early treatment termination, nine insufficient ECG data). No causal connection to music therapy was reported. The final sample comprised 37 participants with chronic or somatoform pain disorders who engaged in MIPT for the duration of the study. A balanced distribution of participants between the two clinics could not be achieved due to the different resources. Therefore, 64.4 % of the sample comes from Magdeburg.
Table 1 provides an overview of the demographic data, psychometric and musical measures, that characterize our sample. The mean age of all participants was 50 years (SD = 10.9), 33% were diagnosed with Chronic pain disorder (ICD-10: F45.40 and F45.41). The symptom burden of our sample, measured with SCL 90, showed high values in Global Severity: 1.4 (SD = 0.7). The CTQ total mean (n = 36) was M = 55.6 (SD = 11.5). The prevalence in the subscales was highest for the emotional abuse M = 11.6 (6.6), emotional neglect M = 16.3 (6.1) and physical neglect M = 10.7 (2.7).
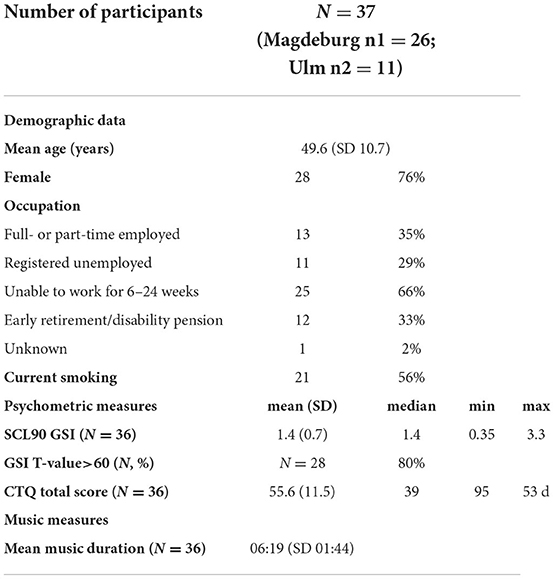
Table 1. Demographic Data, psychometric measures, and musical data: SCL90, Symptom Check List; GSI, Global Severity Index; CTQ, Childhood Trauma Questionnaire.
A total number of each 36 PM and 36 HM have been composed. The mean duration of combined PM and HM during the application phase was 06:19 min (SD 01:44). The musical characteristics varied according to the subjective pain experience and imagination of relief. Two examples of PM and HM are provided as Supplementary material.
All patients that were included in the study completed the full questionnaires. Cronbach's alpha on the sensory scale was 0.67 (T0) and 0.82 (T1). Cronbach's alpha on the affective scale was 0.52 (T0) and 0.71 (T1). Table 2 shows that there is a reduction of reported pain from MT1 = 19.1 (SD = 7.3) to MT2 = 10.6 (SD = 8.0) and in all dimensions of the MPQ-SF. These data confirm our first hypothesis stating a significant reduction of sensory and affective pain experience shortly after the completion of MIPT.
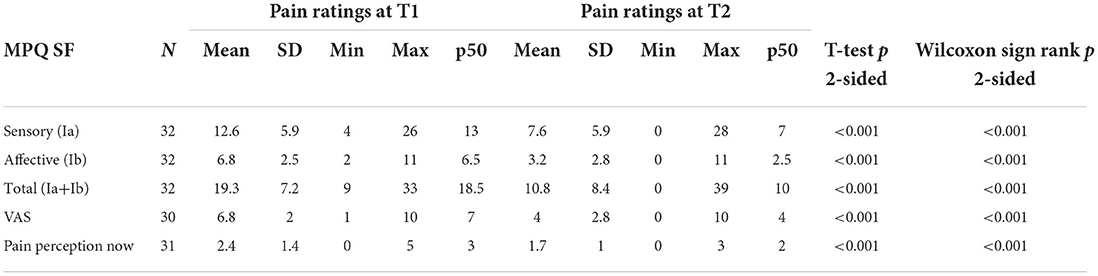
Table 2. Pain ratings at two timepoints measured by McGill Pain Questionnaire (German Short Form).
Since the HRV data may have high interindividual variability and different reactivity, the baseline data were determined beforehand as a starting point to perform the individual normalization. The HRV during resting measurements is subject to only a few influences. As mentioned in the sample section, there were dropouts due to insufficient ECG data. Experimental periods with an artifact rate of 5% or higher were excluded from the analysis (nine periods in three patients). Six patients had an ECG that could not be analyzed due to high age and diagnose-related ectopic beats. Table 3 shows the cardiologic baseline measures of the sample.
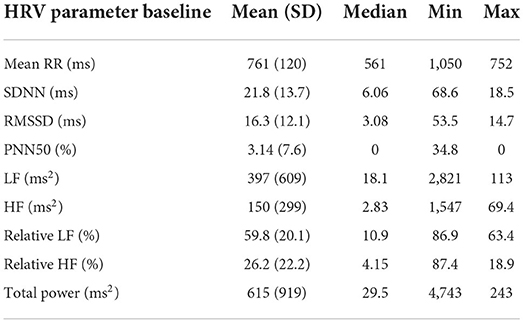
Table 3. Cardiologic baseline measures.
The short analysis phases were selected to investigate the mean differences of the Mean RR and HRV parameters during the test phases “pain music” (PM) and “healing music” (HM1). Table 4 documents physiological data during PM and HM1 2 min after each piece of music have started.
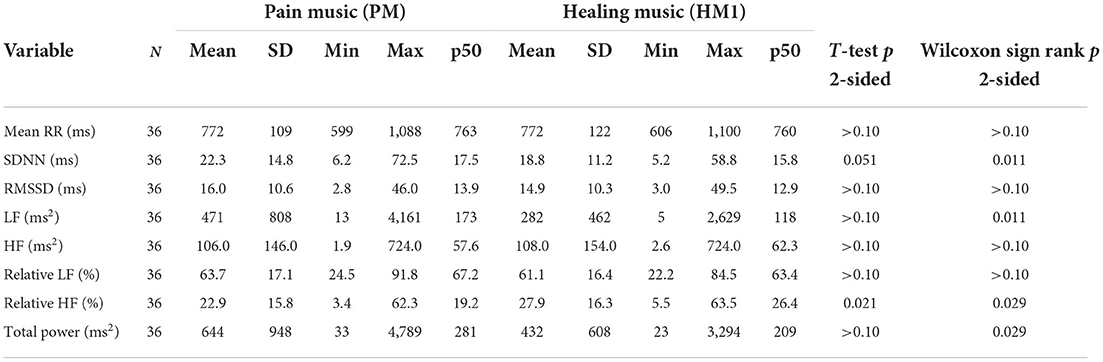
Table 4. Comparison of Mean RR and HRV parameters in the phase during Pain Music (PM) and Healing Music (HM1).
The HRV parameter Total Power (TP), which reflects the overall variability, is reduced (p = 0.0288) in the phase of the HM (644.0 ms; SD = 948.0 ms vs. 432.0 ms; SD = 608.0 ms2). The parameter Total Power reflects the overall level of the autonomic-regulation status, which means that the regulation status is lower during HM. Even when using a correction factor, the comparability of the determined absolute frequency powers seems to be limited due to the strong spread. The standard deviations (SD) are larger than the mean values of these parameters.
The relative Power (%) in the HF band (HF-Power %) is completely different. The HF band reflects parasympathetic activity. It's relative power increases during HM1 [22.9% (SD = 15.8%) vs. 27.9% (SD = 16.3%); p = 0.0288]. Figure 3 shows boxplots of a 2-min study phase for four selected HRV parameters.
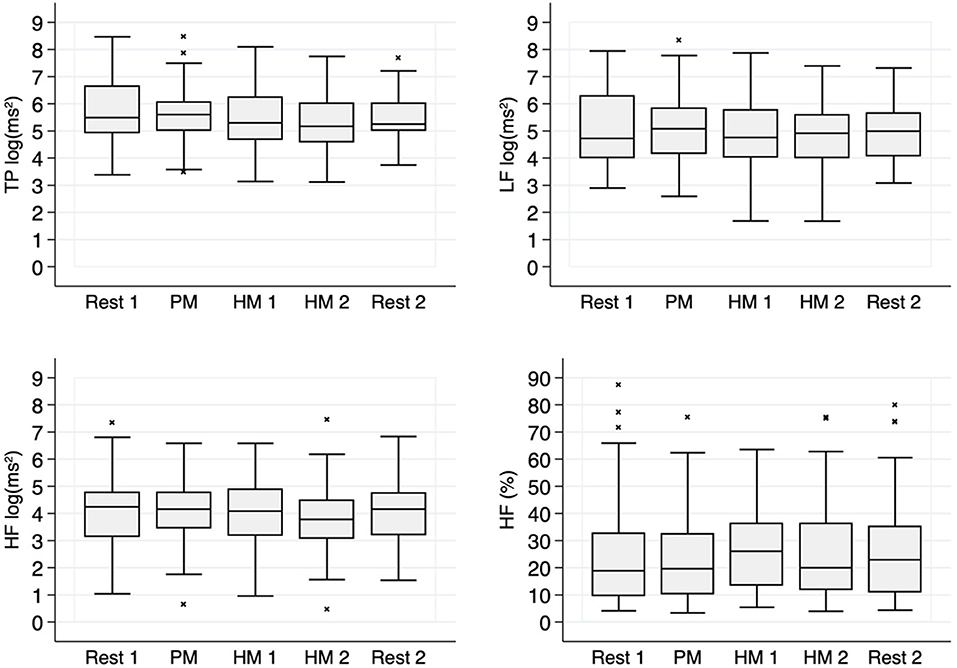
Figure 3. HRV-Parameter from frequency domain: Rest: Resting period before (1; N = 37) and after (2; N = 37) music, PM: Pain Music (N = 37), HM: Healing Music first 2 min (1; N = 36) and last 2 min (2; N = 36). The sample size differs due to a shorter duration of HM in one case.
The modulation of the parasympathetic tone helps to maintain the dynamic vegetative regulation. The absolute power in this respiratory band does not differ in these two phases. So, while the absolute power is reduced in TP and HF, there appears to be a relative shift in the autonomic system toward higher vagal activity.
Although negative correlations between the change of HRV parameters from PM-HM1 with the actual pain experience were observed in this sample, the parametric and non-parametric correlation coefficients were small and not significant.
While in our study a significant reduction in pain experience before (T1) and after (T2) MIPT was found, the data on heart rate variability during the “application phase” of MIPT were much more complex than expected. Significant correlations between the two variables could not be calculated. These findings require more detailed analysis and interpretation in the following.
Chronic pain is a multidimensional phenomenon related to somatic illness, personal life history, psychological vulnerability, and interpersonal relationships. A particular therapeutic challenge is posed by the group of patients with chronic somatoform pain disorder included in our study. This clientele has a somatic understanding of illness predominantly. Demographic data of the study participants revealed a precarious professional situation, while the psychometric data showed a particularly increased symptom burden. Furthermore, our sample is characterized by childhood traumatization, notably emotional abuse and neglect. The psychologically harsh living conditions in childhood can lead to a lack of ability to differentiate between physical pain and affects (30), and can be accompanied by incoherent verbal and nonverbal communication (31). This gives reason to integrate music therapy as a partly nonverbal element of Germany's multimodal inpatient treatment of chronic pain.
Our measures show a significant reduction in the pain ratings in a period of < 2 weeks, and our first hypothesis, H1, can therefore be confirmed. However, the improvement cannot be attributed to our intervention alone, as MIPT is an element of a multimodal inpatient treatment concept and because of lack of a control condition. Other studies on MIPT with comparable clients are not yet available, not even when applying another music therapy intervention. Therefore, we cannot relate our results to available data sets.
Considering that long standstills often characterize the treatment of chronic somatoform pain disorders, our results are nevertheless remarkable. Even minor improvements can be interpreted as a positive sign that an intervention has started working. The contribution of MIPT we regard as a music-induced change in pain perception. Compared to music therapy approaches that use music for relaxation, mindfulness, or distraction, patients in MIPT are encouraged to engage with their pain experience actively and directly. By creating a musical product and communicating in this way, subjective pain experience becomes an object of perception, resulting in perceptual structures and habituated attitudes changing. Not only moments of altered pain perception in the initial phase of the inpatient stay but experiences of self-efficacy are decisive for the treatment progress, as they raise the patients' hope and increase motivation.
The role of vagal afferents in the modulation of pain is established. A systematic review by Koenig et al. (32 includes 20 studies on HRV in healthy adults with experimentally induced pain. It shows an increase in sympathetic-baroreflex activity indexed by an increase in low frequency (LF) spectrum and a decrease in vagal-parasympathetic activity indexed by a decrease in high frequency (HF) spectrum. Healthy individuals with self-reported pain symptoms may have lower parasympathetic activity, indexed by pNN05, RMSSD, and HF (33).
Our HRV data found a more complex situation than has been found in music intervention studies with healthy people. In our view, this might be due to fundamental differences between healthy and severely ill persons. The clinical picture of chronic pain patients is often associated with pronounced vegetative accompanying symptoms in addition to the pain symptoms. The pain perception includes the hypothalamic-pituitary-adrenal axis (HPA axis) with involvement of the autonomic nervous system (ANS) (23). This demonstrates a reduced ability to be activated and adapted to stressful situations in chronic pain patients. People with reduced sympathetic activity show a deficit of pain-inhibiting mechanisms with an increased pain perception (34). On this basis, it is remarkable that the measured HRV changes refer to very low durations of the music in our study. Despite a manifest baseline situation, the immediate effect of listening to the self-composed music can be observed well between the measuring time points during the application phase of MIPT.
We explain our findings psychologically because there is no physiological reference data so far. In the beginning, the HRV parameter Total Power (TP) remains approximately the same during the “pain music” compared to the resting phase, probably caused by tension when anticipating what is about to come. In the phase of “healing music,” TP, mainly comprising of HF and LF, decreased. As exciting music decreases the HRV (17), HM can no longer be understood as relaxation music but as one that can be thrilling for the patient with chronic pain. Interestingly, when HM started and TP tendentially decreased, HF percentage increased. This indicates a shift toward lower mixed sympathetic and parasympathetic activity. We interpret our findings as a physiological correlate of the psychological work of the patients, which, generally speaking, consists in resolving the conflict between the desire for healing and the fear of change. Given the complexity of the physiological data and the lack of significance, our hypotheses H2 and H3 cannot be confirmed.
The small sample size and the lack of a control group limit the validity of our results. The high dispersion of data does not allow a statement about general tendencies of physiological reactions to the intervention. We attribute this to the characteristics of our naturalistic study and the range of individual propensities within our sample. Different cardiologic and psychopathological starting points could have been the reason for different reactions to the music therapy treatment. This might explain why a significant correlation between HRV and MPQ could not be calculated.
Our present study is unique so far. Although our results are only indicative, they have raised research questions for future studies. They also provide insight into immediate physiological reactions to self-composed music pieces as well as into complex physiological and psychological interactions during MIPT. Therefore, our study has increased knowledge of individualized chronic pain treatment with an activating and partly confronting model of music therapy. In a follow-up study, we recommend including a control group and expanding to measurements of intermediate and longer-term impacts of MIPT.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by University Hospital and Medical Faculty of Otto-von-Guericke-University Magdeburg (File reference: 179/16) University Medical Center Ulm (File reference: 201/18). The patients/participants provided their written informed consent to participate in this study.
SM, JF, IB, and SG: conception and design. SG and MD: study therapists. MJ: statistical analysis plan. SM, IB, MJ, JF, and HG: first draft. All authors reviewed and edited the manuscript.
The authors would like to thank Kristin Kapahnke for conducting some MIPTs, Sabine Darius for the EEG measurements, and Michael Riesemann for initial data preparation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2022.943360/full#supplementary-material
Supplementary Audios 1 and 2. Pain Music (PM).
Supplementary Audios 3 and 4. Healing Music (HM).
1. Schmidt HU, Kächele H, Oerter U, Scheytt-Hölzer N. Musiktherapie in der deutschen Psychosomatik: Krankenversorgung, Weiterbildung, Forschung. Psychotherapeut. (2003) 48:155–65. doi: 10.1007/s00278-003-0306-5
2. Schaefert R, Hausteiner-Wiehle C, Häuser W, Ronel J, Herrmann M, Henningsen P. Klinische Leitlinie. Nicht-spezifische, funktionelle und somatoforme Körperbeschwerden. Deutsches Ärzteblatt. (2012) 109:803–19. doi: 10.3238/arztebl.2012.0803
3. Rider M. Entrainment mechanisms are involved in pain reduction, muscle relaxation, and music-medicated imagery. J Music Ther. (1985) 22:183–92. doi: 10.1093/jmt/22.4.183
4. Dileo C, Bradt J. Entrainment, resonance, and pain-related suffering. In: Dileo C, editor. Music Therapy and Medicine: Theoretical and Clinical Applications. MD: AMTA, Silver Spring (1999). p. 181–8.
5. Metzner S. A polyphony of dimensions: music, pain and aesthetic perception. Music Med. (2012) 4:164–71. doi: 10.1177/1943862112449486
6. Hauck M, Metzner S, Rohlffs F, Lorenz J, Engel AK. The influence of music and music therapy on neuronal pain induced oscillations measured by MEG. Pain. (2013) 154:539–47. doi: 10.1016/j.pain.2012.12.016
7. Metzner S, Frommer J. Die performative und bedeutungsgenerierende Dimension von Musik in der musiktherapeutischen Schmerzbehandlung. Psychodynamische Psychotherapie/Sonderheft Musiktherapie. (2014) 224–33. Available online at: https://elibrary.klett-cotta.de/basket/cart
8. Hunt AM, Fachner J, Clark-Vetri R, Raffa RB, Rupnow-Kidd C, Maidhof C, et al. Neuronal effects of listening to entrainment music versus preferred music in patients with chronic cancer pain as measured via EEG and LORETA imaging. Front Psychol. (2021) 12:588788. doi: 10.3389/fpsyg.2021.588788
9. Schrauth T. Die Musik der musik-imaginativen Schmerzbehandlung. Musiktherapeutische Umschau. (2015) 36:224–35. doi: 10.13109/muum.2015.36.3.224
10. Metzner S. Darstellung und Transformation von Schmerzerleben in der Musik-imaginativen Schmerzbehandlung. Göttingen: Vandenhoeck and Ruprecht unipress (2018). doi: 10.14220/9783737008020
11. Bradt J. The effects of music entrainment on postoperative pain perception in pediatric patients. Music Med. (2010) 2:150–7. doi: 10.1177/1943862110369913
12. Kwan M, Soek A, Seah T. Music therapy as a non-pharmacological adjunct to pain management: Experiences at an acute hospital in Singapore. Prog Palliat Care. (2012) 21:151–7. doi: 10.1179/1743291X12Y.0000000042
13. Koenig J, Warth M, Oelkers-Ax R, Wormit A, Bardenheuer HJ, Resch F, et al. I need to hear some sounds that recognize the pain in me: an integrative review of a decade of research in the development of active music therapy outpatient treatment in patients with recurrent or chronic pain. Music Med. (2013) 5:150–61. doi: 10.1177/1943862113490739
14. Lee JH. The effects of music on pain: a meta-analysis. J Music Ther. (2016) 53:430–77. doi: 10.1093/jmt/thw012
15. Garza-Villarreal EA, Pando V, Vuust P, Parsons D. Music-induced analgesia in chronic pain conditions: a systematic review and meta-analysis. Pain Physician. (2017) 20:597–610. doi: 10.36076/ppj/2017.7.597
16. Martin-Saavedra JS, Vergara-Mendez LD, Talero-Gutiérrez C. Music is an effective intervention for the management of pain: an umbrella review. Complement Ther Clin Pract. (2018) 32:103–14. doi: 10.1016/j.ctcp.2018.06.003
17. Koelsch S, Jancke L. Music and the heart. Eur Heart J. (2015) 36:3043–9. doi: 10.1093/eurheartj/ehv430
18. Fuchs D, Hillecke TK, Warth M. Relaxation effects of musially guided resonance breathing: a randomized controlled pilot study. Music Med. (2018) 10:104–12. doi: 10.47513/mmd.v10i2.576
19. Mojtabavi H, Saghazadeh A, Valenti VE, Rezaei N. Can music influence cardiac autonomic system? a systematic review and narrative synthesis to evaluate its impact on heart rate variability. Complement Ther Clin Pract. (2020) 39:101162. doi: 10.1016/j.ctcp.2020.101162
20. Gebhart GF, Randich A. Vagal modulation of nociception. APS J. (1992) 1:26–32. doi: 10.1016/S1058-9139(06)80007-0
21. Koenig J, DeWayne P, Williams P, Kemp AH, Thayer JF. Vagally mediated heart rate variability in headache patients—a systematic review and meta-analysis. Cephalalgia. (2016) 36:265–78. doi: 10.1177/0333102415583989
22. Andrade CP, Zamunér AR, Forti M, de França TF, da Silva E. Reliability of heart period and systolic arterial pressure variabilities in women with fibromyalgia syndrome. Clin Rheumatol. (2016) 35:2347–52. doi: 10.1007/s10067-016-3284-z
23. Friederich HC, Schellberg D, Mueller K, Bieber C, Zipfel S, Eich W. Stress und autonome Dysregulation bei Patienten mit einem Fibromyalgiesyndrom. Schmerz. (2005) 1:185–94. doi: 10.1007/s00482-004-0335-1
24. Sammito S. Alters- und geschlechtsabhängige Referenzwerte für die Herzfrequenzvariabilität. Habilitationsschrift. Magdeburg: Medizinische Fakultät der Otto-von-Guericke-Universität Magdeburg (2017).
25. Franke GH. Die Symptom-Checkliste von Derogatis* Deutsche Version* Manual, 2nd ed, revised [Symptom Checklist of Derogatis* German version*Manual, 2nd ed., revised], Göttingen: Beltz (2002).
26. Wingenfeld K, Spitzer C, Mensebach D, Grabe JH, Hill A, Gast U, et al. Die deutsche Version des Childhood Trauma Questionnaire (CTQ): Erste Befunde zu den psychometrischen Kennwerten. PPmP. (2010) 60:442–50. doi: 10.1055/s-0030-1247564
27. Melzack R. The short-form McGill pain questionnaire. Pain®. (1987) 30:191–7. doi: 10.1016/0304-3959(87)91074-8
28. Sammito S, Thielmann B, Seibt R, Klussmann A, Weippert M, Böckelmann I. Guideline for the application of heart rate and heart rate variability in occupational medicine and occupational science. ASU Int. (2015) 6:1–29. doi: 10.17147/ASUI.2015-06-09-03
29. Task Force of The European Society of Cardiology and The North American Society of Pacing and Electrophysiology. Heart rate variability: standards of measurement, physiological interpretation, and clinical use. Circulation. (1996) 93:1043–65.
30. Egle UT, Nickel R, Hoffmann SO. Psychodynamische Psychotherapie bei chronischem Schmerz. In: Kröner-Herweg B, Frettlöh J, Klinger R, Nilges P, editors. Schmerzpsychotherapie. Heidelberg: Springer (2007). p. 617–24. doi: 10.1007/978-3-540-72284-7_34
31. Merten J, Brunnhuber S. Facial expression and experience of emotions in psychodynamic interviews with patients suffering from a pain disorder. Psychopathology. (2004) 37:266–71. doi: 10.1159/000081982
32. Koenig J, Jarczok MN, Ellis RJ, Hillecke TK, Thayer JF. Heart rate variability and experimentally induced pain in healthy adults: a systematic review. Eur J Pain. (2014) 18:301–14. doi: 10.1002/j.1532-2149.2013.00379.x
33. Koenig J, Jarczok MN, Ellis RJ, Warth W, Hillecke TK, Thayer JF. Lowered parasympathetic activity in apparently healthy subjects with self-reported symptoms of pain: preliminary results from a pilot study. Pain Practice. (2015) 15:314–8. doi: 10.1111/papr.12177
Keywords: psychosomatics, somatoform pain disorder, music-imaginative pain treatment, heart rate variability, pain perception
Citation: Metzner S, Jarczok MN, Böckelmann I, Glomb S, Delhey M, Gündel H and Frommer J (2022) Improvement of pain experience and changes in heart rate variability through music-imaginative pain treatment. Front. Pain Res. 3:943360. doi: 10.3389/fpain.2022.943360
Received: 13 May 2022; Accepted: 20 July 2022;
Published: 10 August 2022.
Edited by:
Eduardo A. Garza-Villarreal, Universidad Nacional Autónoma de México, MexicoReviewed by:
Christie Ramos Andrade Leite-Panissi, University of São Paulo, BrazilCopyright © 2022 Metzner, Jarczok, Böckelmann, Glomb, Delhey, Gündel and Frommer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanne Metzner, U3VzYW5uZS5NZXR6bmVyQHVuaS1hLmRl
†ORCID: Susanne Metzner orcid.org/0000-0001-6745-7337
Marc N. Jarczok orcid.org/0000-0002-6055-385X
Irina Böckelmann orcid.org/0000-0002-3905-3527
Harald Gündel orcid.org/0000-0001-7827-320X
Jörg Frommer orcid.org/0000-0002-0262-4621
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.