
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pain Res. , 27 May 2022
Sec. Pain Mechanisms
Volume 3 - 2022 | https://doi.org/10.3389/fpain.2022.885570
This article is part of the Research Topic Socio-Psychological Influences on Pain View all 6 articles
 Irina Kudrina1,2*
Irina Kudrina1,2* Gillian Bartlett1,3†
Gillian Bartlett1,3† M. Gabrielle Pagé4,5†Yoram Shir2Leon Tourian2,6
M. Gabrielle Pagé4,5†Yoram Shir2Leon Tourian2,6 Manon Choinière4,5†Isabelle Vedel1†
Manon Choinière4,5†Isabelle Vedel1†Adolescents and young adults (AYAs) represent a unique population with distinct psycho-social risks and care needs. About 10% of AYAs live with chronic pain (CP) and transition to adult pain care between 16 and 25 years of age. These transitions in care happen simultaneously with other bio-psycho-social changes and require flexible multi-disciplinary support models. As it stands, transitional pain care appears suboptimal, fragmented, and opportunistic in Quebec (Canada). The objective of this Brief Report is, therefore, to present our study findings and propose a multi-disciplinary transitional framework vision applicable to AYAs living with CP. Data were collected using a sequential-consensual qualitative design with a longitudinal participatory component. The consecutive stages of this work included an exploratory stage, semi-structured interviews with primary care providers, and inter-disciplinary deliberative stakeholder consultation groups. The deductive inductive thematic approach and the three-level Health Care Transition Research Consortium's theoretical framework were used to analyze the data. A representative group of stakeholders discussed findings from the first two steps, made fifteen actionable recommendations and formulated their vision of a transitional pain care model that can be further adapted in other settings. The study results present important insights into various psycho-social factors associated with transitional pain care for AYAs.
An estimated 9–12% of Canadians aged 12 to 44 years live with chronic pain (CP) condition (1). CP persists beyond 3 months (2) and disproportionately affects already vulnerable populations (3) resulting in a significant societal cost (4–6). A comprehensive conceptualization of CP involves an interplay of bio-psycho-socio-cultural factors and cognitive experiences resulting in sensory, affective, motivational responses, and expressions of suffering (2, 7). Adolescents and young adults (AYAs) living with CP represent a unique population with specific psycho-social risks and care needs (8, 9). It can even be argued that due to several modifiable risk factors affecting decades of their functional lives ahead, this population needs the utmost attention from the medical and research communities. Yet, for the public, CP is commonly associated with a visible injury or an advanced age thus limiting the development of pain-focused policies and initiatives targeting youths.
CP is known to influence the neuro- and social development of children and youths (10, 11), who might be survivors of traumatic experiences related to pediatric procedures (12), stressful life events (13), stigma related to pain, and mental health (14) that perpetuate CP into the adulthood (15). There is limited research on cultural and racial differences to understand AYAs' pain experiences and choices of pain management modalities (7). In a multi-cultural country like Canada, such a lack of visibility risks worsening already existing inequity and inequality in the allocation of resources for AYAs.
The last stage of transition and integration to adult services is almost a decade long (16–25 years of age) and happens simultaneously with transitions in vocational training and employment, social and family responsibilities, rendering AYAs prone to multiple stressors and poor clinical outcomes (16, 17), extensive use of emergency services (18), and overall worsening of psycho-social indicators (19). AYAs are known to be at a risk of new psychiatric diagnoses (20–22), experimentation with substances and high-risk behaviors (23–25), sexually transmitted infections (26, 27), sedentary lifestyles (28), and poor eating habits (29). In the pandemic context, loneliness and low education among youths are associated with increased use or initiation of cannabis, e-cigarettes, and binge drinking (30) and opioid and stimulant-associated mortality (31, 32). AYAs living with CP are at especially high risk of suicidality (33). Thus, this population presents with a distinct baseline risk profile that substantiates the need for an urgent shift in clinical thinking, interventions, and research focus.
The Canadian Association of Pediatric Health Centers (CAPHC) guideline (34) recommends that all young patients with chronic conditions should be registered with a community-based primary care provider (PCP). However, there is a very limited literature on post-transfer practices and almost no data on pain-relevant transitional multidisciplinary models of care (35) to involve PCPs longitudinally. In a review of the published scientific and gray literature (35), we identified that only three out of fifteen transitional models described at least some involvement of primary care. All identified programs were initiated by pediatric specialties with an overall limited adult practitioners' and PCPs' input.
Pediatric care ends when adolescents are discharged at the age of 18, which makes the small number of existing transitional programs unipolar and narrowly focused on the preparation for the transfer to adult services. As our understanding of the PCPs' role in transitions, including training requirements, is developing (36), the scope of the necessary knowledge and skills in adolescent and pain medicine remains unidentified. Confounding is the limited availability of PCPs in Canada and especially in Quebec where this study took place. Due to the lack of standardized transitional outcomes, identified programs were not systematically funded or evaluated. In addition, there is a paucity of evidence on dedicated CP transition pathways and the role of recipient adult services. However, there is an agreement in the literature that the transitional care provision should be developmentally appropriate (37) rather than age-based (38) and would account for a variety of psycho-social factors along the transition trajectory.
The objective of this Brief Report is, therefore, to present our study findings of the psycho-social factors relevant to the transitional pain care for AYAs and propose a multi-disciplinary transitional framework vision pertinent to the pain field and applicable to this important population segment.
Data were collected using a sequential-consensual qualitative design (39) with a longitudinal participatory component (40, 41). The three consecutive stages included: stage 1, an exploratory stage that informed further steps, followed by stage 2, semi-structured interviews with twelve PCPs, and concluded with stage 3, three inter-disciplinary deliberative stakeholder consultations groups. Three AYAs patient-partners were involved longitudinally in the entirety of the project, directing its development, validating study findings, and helping with the understanding of the findings' significance.
For data collection and further analysis, we applied hierarchical frameworks based on the CAPHC guideline (34) and Health Care Transition Research Consortium (HCTRC) theoretical approach (42). The CAPHC guideline is concerned with transitional processes, tools, and resources at the personal, clinical, and system levels. The HCTRC theoretical framework offers a comprehensive description of variables important for patients with complex care needs in the individual, family and social support, environmental, and healthcare system domains. We adopted this approach by categorizing our findings hierarchically and conceptualizing all results into the three domains: individual, service, and healthcare system levels. A detailed description of methodology and findings are provided elsewhere (35).
The study involved a multi-disciplinary team of the McGill pain clinic [McGill University Healthcare Network (43)], primary care providers, allied professionals, and AYAs patient-partners. The second and third stages were informed by the preliminary findings from the first (exploratory) stage.
In stage 1, a core clinical research team interviewed active AYA patients and their supporters during their clinical encounters for over 1 year.
In stage 2, the input from PCPs was sought. A random purposeful sampling strategy was employed (44, 45). Sample adequacy (46) was assured. We searched our administrative hospital database and sent invitations to more than 30 PCPs. The final sample resulted in 12 participants, aged 29–70, with a wide range of experiences (family medicine groups, emergency medicine, solo practice, private office) and a number of years in practice (3–40 years). Seven participants were men, and a majority were English-speaking (N-9).
In stage 3, three deliberative stakeholder consultation groups (47, 48) concluded the project: (i) clinicians, (ii) allied healthcare professionals (AHP), and (iii) AYAs and their supporters. We chose a purposive homogenous sampling technique (44, 45) to recruit individuals who possess specific characteristics: those who have clinical, non-clinical, and patient experiences in McGill Healthcare Network and are familial with different institutional policies and processes in place. The final group composition thus represented primary and tertiary care professionals at different stages of their careers (nurses, medical residents, staff clinicians, and a clinical director), seven AHP (clinical psychologists, social worker, public health researcher, physiotherapists, and an administrative director), and six AYAs and their supporters. As some qualitative studies might be concerned with a degree of data generalization, determining an appropriate sample size was important. Onwuegbuzie et al. (44) reviewed qualitative literature and showed that in most cases, a group size of 6–12 participants allows for sufficient opportunities to share rich insights, sustain discussions, and present a sufficiently large spectrum of opinions. In homogenous sampling, to realistically reach a data saturation point, a total of 12–20 data sources might be necessary. Thus, to achieve informational redundancy and data saturation in our three groups, we selected a sample size of 6–7 participants per group.
In stage 1, data collection was informed by the CAPHC (34) guideline. The team evaluated AYA patients' feedback during their clinical encounters and analyzed existing transitional literature, tools, and protocols. All findings were discussed, summarized, and conceptualized during the meetings with a larger clinical research team and patient partners. Two bilingual (English and French) interview guides (49) were constructed based on the emerged themes, one for stage 2 and one for stage 3.
Each participant chose an alias and signed informed consent. Individual interviews and group deliberations were recorded; transcripts were anonymized and transcribed verbatim.
In stage 2, semi-structured interviews explored how PCPs structured their practices, their comfort level providing transitional and pain care for AYAs with CP, and what role they can play in transitions.
In stage 3, to transfer knowledge (39) from stages 1 and 2, participants received a summary of the study findings and then were asked to deliberate on transitional guidelines and endorse relevant recommendations. We thus included decision-makers and key stakeholders in the shared decision-making process (48, 50), mitigating power differentials.
We performed an iterative deductive inductive thematic analysis of the transcribed bilingual data collected in stages 2 and 3 using QRS International's NVivo11 software (2015, London) (51). The three-level (individual, service, and healthcare system (system)) transitional framework was adopted. The deductively coded data were categorized into the corresponding framework domains. The inductive analysis allowed for the emergence of the new codes. The reviewers iteratively identified and discussed emerging themes and drew conclusions.
Data from stages 1 and 2 were used to inform stage 3. We present a summary of the main findings from stages 2 and 3 supported by the quotes from participants. At the individual (patient) level, all participants agreed that the integration of adult services and building youths' capacity for self-management should be the focus. At the service level, the improvement in the inter-disciplinary care coordination and communications were noted in all three stages. Overall, our findings indicate that the most important barriers to overcome were identified at the system level. Even individual and service variables were frequently discussed as a function of the system level barrier and facilitators. Due to a high degree of fragmentation of the medical care provision, the need for more robust and structured transitional care was recognized by all participants. Unexpectedly, the initial concern about mental health and addiction, discussed in the exploratory and interview with PCPs stages, was not included in the final set of recommendations. Below, we summarize each level in more detail as matched to chosen CAPHC guideline recommendations and by applying HCTRC theoretical framework variables as appropriate for our setting.
Individual transition planning was discussed by the clinicians and AHP groups. Their views converged stating that due to the pediatric and adult care models differences, AYAs' would benefit from a patient peer support network to undergo “an orientation session [with] their parents where the whole process can be explained, and we're (pain service team) up front setting expectations about what this service is about…kind of concrete protocols or concrete steps that could be implemented at the system level to facilitate that transition” (Earth, AHP). Transitional planning was strongly supported by the PCPs who felt that AYAs live through very complex times when “…nothing is settled. It's shifting sands in every way, within their personal life, their professional life, their studies, their love life, their whatever, their family relations… So, … they're much more vulnerable to screwing up” (Dr. Office). Another PCP emphasized how AYA's planning capacity could still be in development, “I think it has to do with how their brains work, and they're more impulsive, and they're more in their present. So, if it's not in the front of their awareness, they, other things are more important, and that's what they focus on” (Dr. Diego). These sentiments were echoed by the stage 3 group participants, who saw transition planning as multi-faceted and continued with the adult provider teams.
Clinicians and patient groups agreed on the need for accommodations of the AYAs' vocational and working schedules, recommended a telephone helpline (clinicians), and implementation of “drop-in hours” similar to walk-in clinics (patients). Clinicians emphasized that “… it's even more important sometimes in this group of people who do have chronic pain, who miss a lot of schools, who miss a lot of working opportunities, to give them the flexibility to have later evenings, or early mornings, that we promote that they don't miss school or don't miss work” (Paris). AYAs insisted that the timely supporting documentation plays a crucial role in validating their limitations and obtaining disability-related accommodations “so that I can keep up with the other students and sometimes just to get those kinds of letters and stuff can take months… if I have midterms, if I have finals in university, I need them right now… getting documents, simple documents and such becomes really, really tough.” (July).
One of the most contentious points was the need for improved communication strategies to ensure “safe, caring and effective transitions.” One of the most discussed solutions was a shared electronic online platform accessible to patients and healthcare providers that “…would house information… [be] patient friendly… [with] a visual component that might be more interactive” (Rio, clinician). Such technology could be multi-functional and serve for the confidential information exchange, as an administrative tool. There might be a patient portal offering virtual orientation sessions, the ability to contact the team, and assisting with a standardized transition process by providing “…a web-based referral form that obtains the essential information needed by the pain treatment clinic” (Titan, AHP). Such a platform was also seen as a safe space for case discussions and knowledge exchange with “…the hub experts of the pain clinic and then physicians, it's not limited to physicians, but allied healthcare professionals in the community” (Earth, AHP). Here, the participants mentioned the technological advantages of an ECHO (52)-like knowledge translation model already adopted across jurisdictions.
The agreement on the involvement of PCPs was unanimous and participants felt that the benefits are mutual. Thus, AHP desired ongoing assistance from the PCPs, and clinicians pictured PCPs as a longitudinal “safety net” for AYAs in transition. Patient participants recommended the involvement of PCPs more as patients' allies and supporters during their adaptation period. PCPs desired that AYAs were “…working closely… having regular contact with [their] primary care physician, that's something that often doesn't happen in chronic pain, people show up when they have an exacerbation, whereas this should be something that's managed on a regular basis with … a global treatment plan as opposed to a reactive type of plan” (Dr. MDZERO).
A pivot nurse position was another idea supported by all participants and discussed extensively in all stages. This role was seen as quite extensive and would include monitoring patient's attachment to primary care services and appointment attendance, ensuring the smoothness of ongoing communication between patients and involved healthcare professionals, informing and educating the patient, and be the first line of contact, “like a resource person that people can call at all times…” (Montreal, clinician). Patients hoped that the pivot nurse could absorb some of the physician's responsibilities, “tell[-ing] you “You know what? Come into the hospital, I'm going to squeeze you in right away”…the root of the problem, is the fact that there is no person in the middle… and [there] has to be someone else in the middle, not the patient.” (June, patient). The pivot nurse was seen as a patient advocate to “communicate between primary care providers and… pain specialists” (June, patient) and liaise with other professionals, “be the go-between” team member. (Jupiter, AHP). This would be “…paramount because … unless you have that advocate or unless you can really advocate for yourself, not everyone has that makeup to really put themselves out there…” (February).
Discussing professional collaborations, participants realized there might be some fundamental differences in how primary and specialty adult services are set up, which might be confusing for the AYAs, affecting their expectations from the services and different care providers. As one of the AHP group participants put it, “…it speaks perhaps with the philosophy of family physicians vs. other physicians, where they're kind of cats vs. dogs. Where I think it's hard to herd cats. It's not a hierarchical structure as it would be in a hospital setting…So that you have to be careful with it.” (Titan).
All stakeholders agreed that there is a need for a consistent approach to transitional pain care pan-provincially. The tertiary care providers qualified most referral information as incomplete with “the details there are grosso modo, they are just sort of ticked off” (Rio, clinician). PCPs, on the other hand, described their confusion about pain services saying that “there should be a site or something that gives us the adequate [information on the services]- because it doesn't go through the CRDS [central online depository], so you have to know where you're sending them.” (Dr. Lily). One of the AYAs interviewed in the first phase exclaimed “My family doctor? No, she had no idea how to help me and where to send me.” Another patient recommended implementing “a standardized transition system…Maybe a task force of different… doctors … who lay out their… 10 steps that need to happen when a patient aged 17 goes through for the next 12 months until they are kicked out [of pediatric services] and they start at the [adult] hospital.” (February).
Training for healthcare workers was another extensively discussed variable. For example, a patient supporter described her attempt to intervene “[as she] saw a medical practitioner talking to July [AYA patient], who thought he had a 50-year-old, or a 40-year-old in front of him… [and supporter] was shut down because of the fact that she's obviously over 14.” (May). An experienced educator AHP gave examples on his work with family medicine trainees evaluating AYAs who are “different from older adults, who require different interviewing and management techniques…” (Titan). A patient echoed these sentiments by emphasizing that gaps in training might be also associated with the perceived stigma: “I just noticed that a lot of … doctors seem to be more kind of against like, “Oh, there's nothing wrong with you” or… they try but maybe they don't have the knowledge that they need…” (March). The stigma of CP in a young patient was discussed by PCPs as something pervasive and omnipresent, one of the PCPs explained “…[e]verybody will open the door for an old person with a cane or a walker, right, but a young person, everybody looks at them, and it's almost like they have leprosy. It's like there's something wrong with them, what did they do, you know” (Dr. Lily). Another PCPs stated, “I've been told that chronic pain is just as common in children and young people as it is in adults. I was very surprised by that information…” (Dr. Diego).
A more detailed description of quotes and CAPHC-matched recommendations is found here (35).
We conducted a three-stage qualitative study on transitional pain services for AYAs in the McGill Healthcare Network and involved a diverse group of informants. The stakeholders discussed a complex interplay among the inter-disciplinary care provision, longitudinal primary care support, stigma, and other psycho-social determinants. The deliberative stakeholder consultation groups reviewed the findings of the first two steps, the transitional CAPHC guideline (R-1–3, 4–6, 9, 10, 13–15, 17) and formulated a set of 15 actionable recommendations (Table 1). The HCTRC theoretical framework was applied to formulate the vision for the transitional pain care model (Table 2).
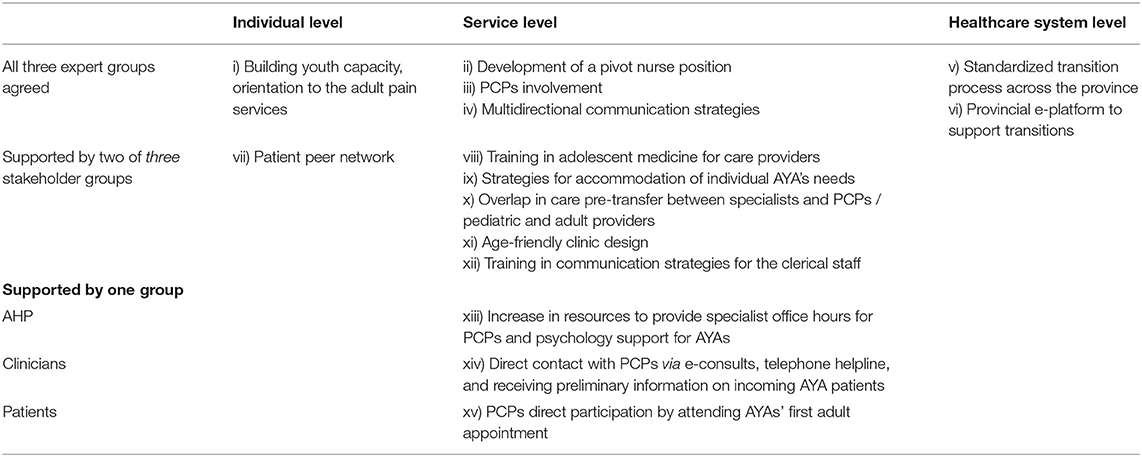
Table 1. Summary of 15 actionable recommendations.
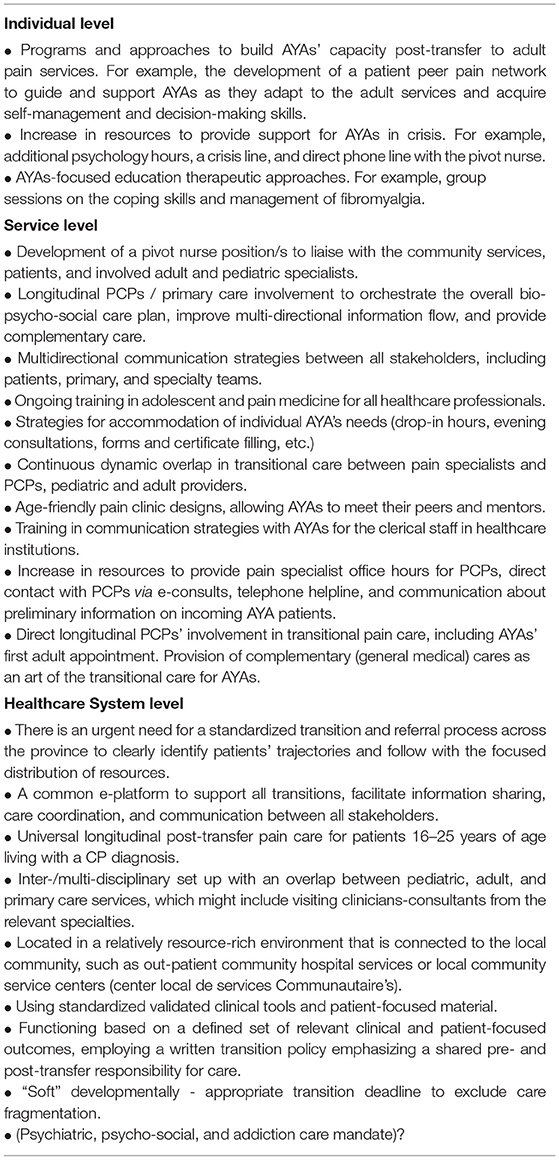
Table 2. TRAST transitional pain care model would involve all three levels.
The main findings evolved around AYAs' pain experiences at three different levels, individual patient, service, and healthcare system levels. Interestingly, the focus of most discussions was on strategies with a direct impact on the AYA function within the system: building youth's capacity to navigate the system, orientation to adult pain services, development of a pivot nurse position to have a “go-to person,” PCPs' involvement in a role of an AYAs' ally when integrating into the new system, multidirectional communication strategies, standardization and predictability of the transition processes across the province, and implementation of the e-platform. This focus on the system's shortcomings likely stems from the AYAs' need for a more unambiguous and predictable environment that would limit “shifting sands” and allow for better function and coping.
Most but not all participants chose the development of a patient peer network, training in adolescent medicine for care providers, strategies on accommodations of individual AYA's needs, overlap in care, pre-transfer between specialists and PCPs/pediatric and adult providers, age-friendly clinic designs, and training in communication strategies for the clerical staff as important local initiatives that would strengthen transitional care. Resource-heavy recommendations (PCPs direct participation by attending AYAs' first adult appointment, increase in resources to provide specialist office hours for PCPs and psychology support for AYAs, direct contact with PCPs via e-consults, telephone helpline, receiving preliminary information on incoming AYA patients) were supported only by one enthusiastic group (patients, AHP and clinicians, respectively).
Participants, especially PCPs and AYAs, spent significant time discussing CP in young patients as being invisible, poorly understood by society, and not accommodated by the healthcare and educational systems. It was felt that this added layer of stress prevents AYAs from reaching their full potential resulting in poor psycho-social outcomes. The lack of resources for AYAs stems from the poor recognition of this vulnerable population, leading to the social insensitivity to pain in AYAs and its artificially diminished importance to society (7, 22). AYAs felt not believed and frequently dismissed as being unimportant, underscoring the need for a large scale significant educational efforts beyond healthcare providers that would reach different segments of society. With the involvement of decision-makers, focused funding for the development of pan-provincial transitional programs, e-platforms, and local resources, such as pivot nurses, will follow. The leitmotif of invisible pain in young patients was present in all discussions, thus stressing the urgent need to clearly define and recognize this population, in the same way as, for example, vulnerable elderly or children.
Suicide is already the second leading cause of mortality among Canadian youth (53) pre-pandemic. Although important as the individual patient-based outcomes, substance use and mental health were discussed only during the first two stages, but not during the project's final stage and thus, were not included in the final set of recommendations. It is possible that the discussion of some individual-level variables was regarded as rather secondary to a more global issue of the recognition and validation of CP experiences lived by AYAs in today's system. As the vision for the transitional framework starts taking shape, a more detailed and nuanced discussion of the individual factors will get more traction with the PCPs and AYAs presently struggling with the system imperfections, fragmentation, and severe lack of resources.
The need for accommodations in educational environments, pressure to obtain formal documentation, struggles to accomplish the same work as their peers, and desire to have additional opportunities for pain-related visits (drop off hours, telephone calls with a pivot nurse, on-line communication portal with team) underscored today fast-paced and highly competitive environment outside of the clinical setting that puts AYAs in a significant disadvantage socially but also medically. Patient supporters and PCPs admitted that AYAs are having difficulty planning, acting “in a reactive way” when the crisis has already arrived. Greig and Tellier described AYAs as those “…who are still in the process of acquiring autonomy, have marked similarities with adolescents and differ from older individuals who have attained full independence” (8). Furthermore, executive skills acquisition, such as planning, selective attention, and self-regulation, is fully attained around the mid-20s (54, 55) or even later in life, resulting in the need for more guidance and developmentally appropriate care (37) during this decade of transitions.
Sensitizing care providers to the existence of pain in AYAs and providing training in pain management were among the most discussed topics. To be able to recognize CP in AYAs, and properly assess and manage it, a curricula improvement for all healthcare professionals is urgently needed (56, 57). This might be easily achievable now with the explosion of web-based modules, applications, and online certificates. Yet, a common vision is required to structure educational efforts.
Multidisciplinary treatments are preferred but remain poorly accessible, and symptoms deteriorate while patients are waiting for clinic appointments (58, 59). Coupled with an imperfectly structured and understaffed system, the funding for sustainable models of transitional multidisciplinary services is critical for managing CP in AYAs. The rich insights can be gathered from the patient partners and their supporters, especially when they are provided with various advisory and governing opportunities within the same institutions, they get their treatments from. Development of the core outcomes in the psycho-socio-cognitive domains and decentralization of pain services with a shift away from the hospital-based services and closer to the AYAs' “medical home” (60–63) is an already existing vision (64).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by St Mary's Hospital Ethics Review Board. McGill University. The patients/participants provided their written informed consent to participate in this study.
IK developed the original study idea, led the project, and wrote a draft of the manuscript. GB, MP, YS, LT, MC, and IV participated in all study steps, idea development, meetings, discussions, and conceptualization of the study findings, were involved in writing or proof-read the manuscript. All authors contributed to the article and approved the submitted version.
The study received support from the Réseau de connaissances en services et soins de santé intégrés de première ligne du Québec (Réseau-1 Québec), grant # 29053. Louise and Alan Edwards Clinical Research on Pain fellowship support. La Lettre d'entente no 250 (recherche en médecine de famille) salary support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
2. Treede R-D, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. (2019) 160:19–27. doi: 10.1097/j.pain.0000000000001384
3. Canada H. An Action Plan for Pain in Canada 2021. Available online at: https://www.canada.ca/content/dam/hc-sc/documents/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2021-rapport/report-rapport-2021-eng.pdf
4. Simon LS. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. J Pain Palliat Care Pharmacother. (2012) 26:197–8. doi: 10.3109/15360288.2012.678473
5. Dahlhamer J, Lucas J, Zelaya C, Nahin R, Mackey S, DeBar L, et al. Prevalence of chronic pain and high-impact chronic pain among adultsalth-canada/pu, 2016. Morbid Mortal Wkly Rep. (2018) 67:1001. doi: 10.15585/mmwr.mm6736a2
6. Hogan M-E, Taddio A, Katz J, Shah V, Krahn M. Incremental health care costs for chronic pain in Ontario, Canada: a population-based matched cohort study of adolescents and adults using administrative data. Pain. (2016) 157:1626–33. doi: 10.1097/j.pain.0000000000000561
7. Eccleston C, Fisher E, Howard RF, Slater R, Forgeron P, Palermo TM, et al. Delivering transformative action in paediatric pain: a lancet child & adolescent health commission. Lancet Child Adolescent Health. (2021) 5:47–87. doi: 10.1016/S2352-4642(20)30277-7
8. Greig AA, Tellier PP. Le guide de santé Greig pour jeunes adultes: Soins préventifs pour les jeunes adultes de 18 à 24 ans. Canad Fam Phys. (2019) 65:e325–8.
9. Greig AA, Tellier PP. Greig health record for young adults: Preventive health care for young adults aged 18 to 24 years. Canad Fam Phys. (2019) 65:539–42.
10. Eccleston C, Wastell S, Crombez G, Jordan A. Adolescent social development and chronic pain. Eu J Pain. (2008) 12:765–74. doi: 10.1016/j.ejpain.2007.11.002
11. Walker SM. Overview of neurodevelopment and pain research, possible treatment targets. Best Pract Res Clin Rheumatol. (2014) 28:213–28. doi: 10.1016/j.berh.2014.03.007
12. Alberts NM, Gagnon MM, Stinson JN. Chronic pain in survivors of childhood cancer: a developmental model of pain across the cancer trajectory. Pain. (2018) 159:1916–27. doi: 10.1097/j.pain.0000000000001261
13. Lampe A, Doering S, Rumpold G, Spmental model of pain across the cancer . Chronic pain syndromes and their relation to childhood abuse and stressful life events. J Psychosom Res. (2003) 54:361–7. doi: 10.1016/S0022-3999(02)00399-9
14. Wakefield EO, Zempsky WT, Puhl RM, Litt MD. Conceptualizing pain-related stigma in adolescent chronic pain: a literature review and preliminary focus group findings. Pain Reports. (2018) 3(Suppl 1):679. doi: 10.1097/PR9.0000000000000679
15. Davis DA, Luecken LJ, Zautra AJ. Are reports of childhood abuse related to the experience of chronic pain in adulthood? : a meta-analytic review of the literature. Clin J Pain. (2005) 21:398–405. doi: 10.1097/01.ajp.0000149795.08746.31
16. Van Walleghem N, MacDonald CA, Dean HJ. Evaluation of a systems navigator model for transition from pediatric to adult care for young adults with type 1 diabetes. Diabetes Care. (2008) 31:1529–529:8es Care2337/dc07-2247
17. Prestidge C, Romann A, Djurdjev O, Matsuda-Abedini M. Utility and cost of a renal transplant transition clinic. Pediatric Nephrology. (2012) 27:295–302. doi: 10.1007/s00467-011-1980-0
18. Callahan ST, Cooper WO. Changes in ambulatory health care use during the transition to young adulthood. J Adolesc Health. (2010) 46:407–13. doi: 10.1016/j.jadohealth.2009.09.010
19. Park MJ, Scott JT, Adams SH, Brindis CD, Irwin Jr CE. Adolescent and young adult health in the United States in the past decade: little improvement and young adults remain worse off than adolescents. J Adolescent Health. (2014) 55:3–16. doi: 10.1016/j.jadohealth.2014.04.003
20. Pless IB, Power C, Peckham CS. Long-term psychosocial sequelae of chronic physical disorders in childhood. Pediatrics. (1993) 91:1131–6. doi: 10.1542/peds.91.6.1131
21. Wolman C, Resnick MD, Harris LJ, Blum RW. Emotional well-being among adolescents with and without chronic conditions. J Adolesc Health. (1994) 15:199–204. doi: 10.1016/1054-139X(94)90504-5
22. Carver J, Cappelli M, Davidson S. Taking the Next Step Forward: Building A Responsive Mental Health And Addictions System for Emerging Adults: Mental Health Commission of Canada Commission de la santé mentale du Canada (2015).
23. Mundt MP, Zakletskaia LI, Fleming MF. Extreme college drinking and alcoholphysical disorders in Alcohol: Clin Exper Res. (2009) 33:1532–8. doi: 10.1111/j.1530-0277.2009.00981.x
24. Badiani A, Boden JM, De Pirro S, Fergusson DM, Horwood LJ, Harold GT. Tobacco smoking and cannabis use in a longitudinal birth cohort: evidence of reciprocal causal relationships. Drug Alcohol Depend. (2015) 150:69–76. doi: 10.1016/j.drugalcdep.2015.02.015
25. Mason MJ, Luckey B. Young adults in alcohol-other drug treatment: an understudied population. Alcohol Treat Q. (2003) 21:17–32. doi: 10.1300/J020v21n01_02
26. Suris J-C, Resnick MD, Cassuto N, Blum RW. Sexual behavior of adolescents with chronic disease and disability. J Adolescent Health. (1996) 19:124–31. doi: 10.1016/1054-139X(95)00282-W
27. Valencia LS, Cromer BA. Sexual activity and other high-risk behaviors in adolescents with chronic illness: a review. J Pediatr Adolesc Gynecol. (2000) 13:53–64. doi: 10.1016/S1083-3188(00)00004-8
28. Tremblay MS, LeBlanc AG, Janssen I, Kho ME, Hicks A, Murumets K, et al. Canadian sedentary behaviour guidelines for children and youth. Applied Physiol, Nutr Metabol. (2011) 36:59–64. doi: 10.1139/H11-012
29. Taylor JP, Evers S, McKenna M. Determinants of healthy eating in children and youth. Can J Public Health. (2005) 96:S20–6. doi: 10.1007/BF03405197
30. Sylvestre M-P, Dinkou GDT, Naja M, Riglea T, Pelekanakis A, B Publique, et al. A longitudinal study of change in substance use from before to during the COVID-19 pandemic in young adults. Lancet Reg Health-Am. (2022) 8:100168. doi: 10.1016/j.lana.2021.100168
31. Canada Go. Opioid- and Stimulant-related Harms in Canada Published: (December 2021) 2022 Available online at: https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/
32. Control BCCfD. BCCDC Mortality Context App 2022 Available online at: https://bccdc.shinyapps.io/Mortality_Context_ShinyApp/?fbclid=IwAR1T HWB4k48w8y6i0Ab5sU6GjcxOQorXCN49vC6gRgsZWAmaaVo6l9W0HTI
33. Hinze V, Crane C, Ford T, Buivydaite R, Qiu L, Gjelsvik B. The relationship between pain and suicidal vulnerability in adolescence: a systematic review. Lancet Child Adolesc Health. (2019) 3:899–916. doi: 10.1016/S2352-4642(19)30267-6
34. Stromquist L, Paone M, Amaria K, Andrew G, Begg J, Cashen N, et al. A Guideline For Transition From Paediatric to Adult Health Care for Youth With Special Health Care Needs: A National Approach. Ottawa (ON): Canadian Association of Paediatric Health Centres. (2016).
35. Kudrina I. TRAnsitional STructured pain care for adolescents and young adults: TRAST model. [Master's thesis]. [Montreal, QC, Canada]: University of McGill. Available online at: https://escholarship.mcgill.ca/concern/theses/6w924h58d?locale=en
36. Bhawra J, Toulany A, Cohen E, Hepburn C, Guttmann A. Primary care interventions to improve transition of youth with chronic health conditions from paediatric to adult healthcare: a systematic review. BMJ Open. (2016) 6:e011871. doi: 10.1136/bmjopen-2016-011871
37. Farre A, Wood V, Rapley T, Parr JR, Reape D, McDonagh JE. Developmentally appropriate healthcare for young people: a scoping study. Arch Dis Child. (2015) 100:144–51. doi: 10.1136/archdischild-2014-306749
38. Singh S, Anderson B, Liabo K, Ganeshamoorthy T. Supporting young people in their transition to adults' services: summary of NICE guidance. BMJ. (2016) 353:i2225. doi: 10.1136/bmj.i2225
39. Groleau D, Zelkowitz P. Enhancing generalizability: moving from an intimate to a political voice. Qual Health Res. (2009) 19:416–26. doi: 10.1177/1049732308329851
40. White MA, Verhoef MJ. Toward a patient-centered approach: incorporating principles of participatory action research into clinical studies. Integr Cancer Ther. (2005) 4:21–4. doi: 10.1177/1534735404273727
41. Cook T editors. Where Participatory Approaches Meet Pragmatism in Funded (health) Research: The Challenge of Finding Meaningful Spaces. Forum: Qualitative Social Research (2012) Newcastle: Forum Qualitative Sozialforschung.
42. Betz CL, Ferris ME, Woodward JF, Okumura MJ, Jan S, Wood DL. The health care transition research consortium health care transition model: a framework for research and practice. J Pediatr Rehabil Med. (2014) 7:3–15. doi: 10.3233/PRM-140277
43. RUIS McGill. RUIS (réseau universitaire intégré de santé) McGill's Centre of Expertise in Chronic Pain (CECP): McGill University (2019). Available online at: https://mcgill.ca/ruischronicpain/
44. Onwuegbuzie AJ, Leech NL. A call for qualitative power analyses. Qual Quant. (2007) 41:105–21. doi: 10.1007/s11135-005-1098-1
45. Miles MB, Huberman AM. Qualitative data analysis: An Expanded Sourcebook: Phoenix, AZ: Sage (1994).
46. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. (2018) 18:1–18. doi: 10.1186/s12874-018-0594-7
47. Rothwell E, Anderson R, Botkin JR. Deliberative discussion focus groups. Qual Health Res. (2016) 26:734–40. doi: 10.1177/1049732315591150
48. Nugus P, Ranmuthugala G, Travaglia J, Greenfield D, Lamothe J, Hogden A, et al. Advancing interprofessional theory: deliberative democracy as a participatory research antidote to power differentials in aged care. J Interprof Edu Prac. (2019) 15:100–11. doi: 10.1016/j.xjep.2018.09.005
49. Patton MQ. Qualitative evaluation and research methods. Washington, DC: SAGE Publications, inc (1990).
51. NVIVO software. Qualitative data analysis. 2021 [cited 2021. Available online at: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home
52. Sanjeev Arora UoNM. About project ECHO. (2021). Available online at: https://hsc.unm.edu/echo/about-us/
53. Bennett K, Rhodes AE, Duda S, Cheung AH, Manassis K, Links P, et al. A youth suicide prevention plan for Canada: a systematic review of reviews. The Canadian Journal of Psychiatry. (2015) 60:245dian Journal 1177/070674371506000603
54. Casey BJ, Getz S, Galvan A. The adolescent brain. Develop Rev. (2008) 28:62–77. doi: 10.1016/j.dr.2007.08.003
55. Blakemore S-J, Robbins TW. Decision-making in the adolescent brain. Nat Neurosci. (2012) 15:1184–91. doi: 10.1038/nn.3177
56. Klein D, Mehta K. Training in adolescent health: how much have second-year residents had? Can Fam Phys. (2006) 52:980–1.
57. Roy É, Côté RJ, Hamel D, Dubé P-A, Langlois É, Labesse ME, et al. Opioid prescribing practices and training needs of Québec family physicians for chronic non-cancer pain. Pain Res Manag. (2017) 2017 :5910. doi: 10.1155/2017/1365910
58. Deslauriers S, Roy J-S, Bernatsky S, Feldman DE, Pinard AM, Desmeules F, et al. Factors associated with waiting times for persons with rheumatic conditions in multidisciplinary pain treatment facilities. J Pain Res. (2019) 12:2379. doi: 10.2147/JPR.S206519
59. Choini 10.associated with waiting times for persons with rheu, et al. The Canadian STOP-PAIN projectg times: who are the patients on the waitlists of multidisciplinary pain treatment facilities? Can J Anesth/J canadien dtients on t. (2010) 57:539–48. doi: 10.1007/s12630-010-9305-5
60. American Academy of Pediatrics. Transition clinical report authoring group. Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics. (2011) 128:182. doi: 10.1542/peds.2011-0969
61. Canada CoFPo. FAMILY PRACTICE —THE PATIENT'S MEDICAL HOME 2019. Available online at: https://patientsmedicalhome.ca/files/uploads/PMH_VISION2019_ENG_WEB_2.pdf (accessed 2019 October 28)
62. Canada TCoFPo. Patient's medical home 2021 Available online at: https://patientsmedicalhome.ca/ (accessed July 12, 2021])
63. Canada TCoFPo. PMH in Quebec 2021 Available online at: https://patientsmedicalhome.ca/pmh-in-canada/pmh-quebec/
Keywords: adolescents and young adults, chronic pain, psychosocial factors, transitional care, model (5)
Citation: Kudrina I, Bartlett G, Pagé MG, Shir Y, Tourian L, Choinière M and Vedel I (2022) Transitional Pain Care in Quebec: Did We Forget Our Youths? A Brief Research Report. Front. Pain Res. 3:885570. doi: 10.3389/fpain.2022.885570
Received: 28 February 2022; Accepted: 25 April 2022;
Published: 27 May 2022.
Edited by:
Marcos Fabio DosSantos, Federal University of Rio de Janeiro, BrazilReviewed by:
Carolina Kaminski Sanz, Federal University of Rio de Janeiro, BrazilCopyright © 2022 Kudrina, Bartlett, Pagé, Shir, Tourian, Choinière and Vedel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Irina Kudrina, SXJpbmEua3VkcmluYUBtY2dpbGwuY2E=
†These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.