 Vinicius Tieppo Francio
Vinicius Tieppo Francio Benjamin D. Westerhaus
Benjamin D. Westerhaus Adam Rupp1
Adam Rupp1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pain Res. , 25 February 2022
Sec. Neuromodulatory Interventions
Volume 3 - 2022 | https://doi.org/10.3389/fpain.2022.835519
Chronic low back pain remains highly prevalent, costly, and the leading cause of disability worldwide. Symptoms are complex and treatment involves an interdisciplinary approach. Due to diverse anatomical etiologies, treatment outcomes with interventional options are highly variable. A novel approach to treating chronic axial low back pain entails the use of peripheral nerve stimulation to the lumbar medial branch nerve, and this review examines the clinical data of the two different, commercially available, non-spinal neuromodulation systems. This review provides the clinician a succinct narrative that presents up-to-date data objectively. Our review found ten clinical studies, including one report of two cases, six prospective studies, and three randomized clinical trials published to date. Currently, there are different proposed mechanisms of action to address chronic axial low back pain with different implantation techniques. Evidence suggests that peripheral nerve stimulation of the lumbar medial branch nerve may be effective in improving pain and function in patients with chronic axial low back pain symptoms at short and long term follow up, with good safety profiles. Further long-term data is needed to consider this intervention earlier in the pain treatment algorithm, but initial data are promising.
Axial low back pain (LBP) is a complex syndrome involving nociceptive and neuropathic pain with potential for compensatory structural changes in ligamentous and myofascial components, leading to a challenging diagnosis and therapeutic course in clinical practice (1). Chronic axial LBP is defined as pain localized along the lower back region without radicular or referred pain pattern into the extremities, lasting for at least 6 months and is often associated with complex biopsychosocial factors leading to significant impairments in function and quality of life (QoL) (1, 2). Acute LBP is a common health problem that affects roughly 75–85% of all people at some point in their life, and it is the second most common reason for physician visits (3–5). Fortunately, most cases of acute LBP have a favorable outcome, with the majority of patients fully recovering within the first 2–4 weeks, and 90% of patients recovering by 12 weeks. However, recurrence of LBP is common, with rates of up to 50% within 1 year (6). In addition, each subsequent episode connotes a 10–15% chance for chronicity (7). Owing to this high prevalence and incidence of recurrence, the economic impact is staggering, with the majority of costs deriving from missed work days, rather than direct healthcare costs. Approximately only 50% of patients who take off work for 6 months due to LBP return to work, and an estimated 1% of the U.S. population is chronically disabled because of LBP (5–8).
The etiology of axial LBP is vague and difficult to determine precisely. Estimates suggest <15% of LBP causes are identified, leaving the majority idiopathic (7, 9, 10). Some identifiable causes of axial LBP include myofascial pain, discogenic pain, facet-mediated pain, vertebral endplate injury, disc herniation without radiculopathy, central or neuroforaminal spinal stenosis without radiculopathy, sacroiliac joint pain, and fibromyalgia. Other less common causes are osteoporotic fracture, metastatic or primary neoplasm, infection, rheumatologic conditions including ankylosing spondylitis, or vascular conditions like abdominal aortic aneurysm rupture (7, 10) An overlooked etiology of chronic axial LBP is the complex interaction between multifidus muscle and morphology changes leading to dysfunction and impaired sensorimotor control of lumbar intervertebral stability (9, 11–13). Oftentimes, the diagnosis is not simply one pathology, but rather combining overlapping conditions, which suggests the multifactorial nature of axial LBP. Despite the ongoing quest to find Occam's razor for LBP, physicians work to treat the simplest cause of low back pain given a thorough history, physical exam, and imaging.
Management of axial LBP focuses on conservative therapies such as ice, topicals, antiinflammatories, light stretching, professionally directed physical therapy, and gradual return to activity. With increasing pain, disability, pain duration, or failure of treatment, interventional approaches are subsequently attempted. Common interventional modalities include epidural steroid injections (ESI), medial branch blocks (MBB), intraarticular facet injections, lumbar radiofrequency ablation (RFA) of medial branches of dorsal rami or basivertebral nerve, mechanical surgical procedures (including posterior stabilization, interspinous spacers, or minimally invasive decompression) and neuromodulation, including spinal cord stimulation (SCS), or peripheral nerve stimulation (PNS) (10, 14, 15).
This review seeks to examine the current concepts of PNS of the lumbar medial branch nerve (LMBN) of the dorsal ramus by looking at current clinical data and contrasting with other interventional treatments options for chronic axial LBP.
This study is a review aimed at appraising current concepts in non-spinal neuromodulation for chronic axial LBP, particularly PNS of the LMBN. Data sources included PubMed, MEDLINE, Google Scholar, and Cochrane Library indexed manuscripts. Literature search was conducted between July 2021 and October 2021 for entries with keywords of “peripheral nerve stimulation” and “multifidus” and “lumbar medial branch.” Inclusion criteria were human studies in the English language, such as randomized trials, observational studies, prospective studies, and case series. All records were identified and appraised independently by the authors in a standardized, unbiased, unblinded fashion using the same approach to reduce the risk of selection bias and standardized inclusion and exclusion criteria. Book chapters, non-human clinical studies, and letters to the editors were excluded (Table 1). For all studies included, data synthesis, data analyses, quality appraisal, outcome measurements, and risk of bias assessment were performed by the authors. Data extracted from current published studies are summarized in Table 2.
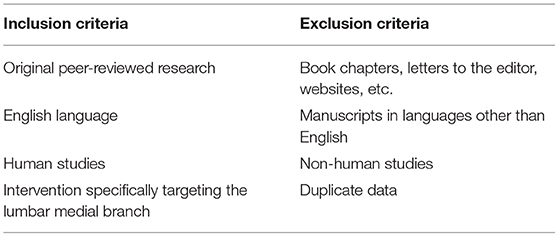
Table 1. Inclusion and exclusion criteria of the literature review.
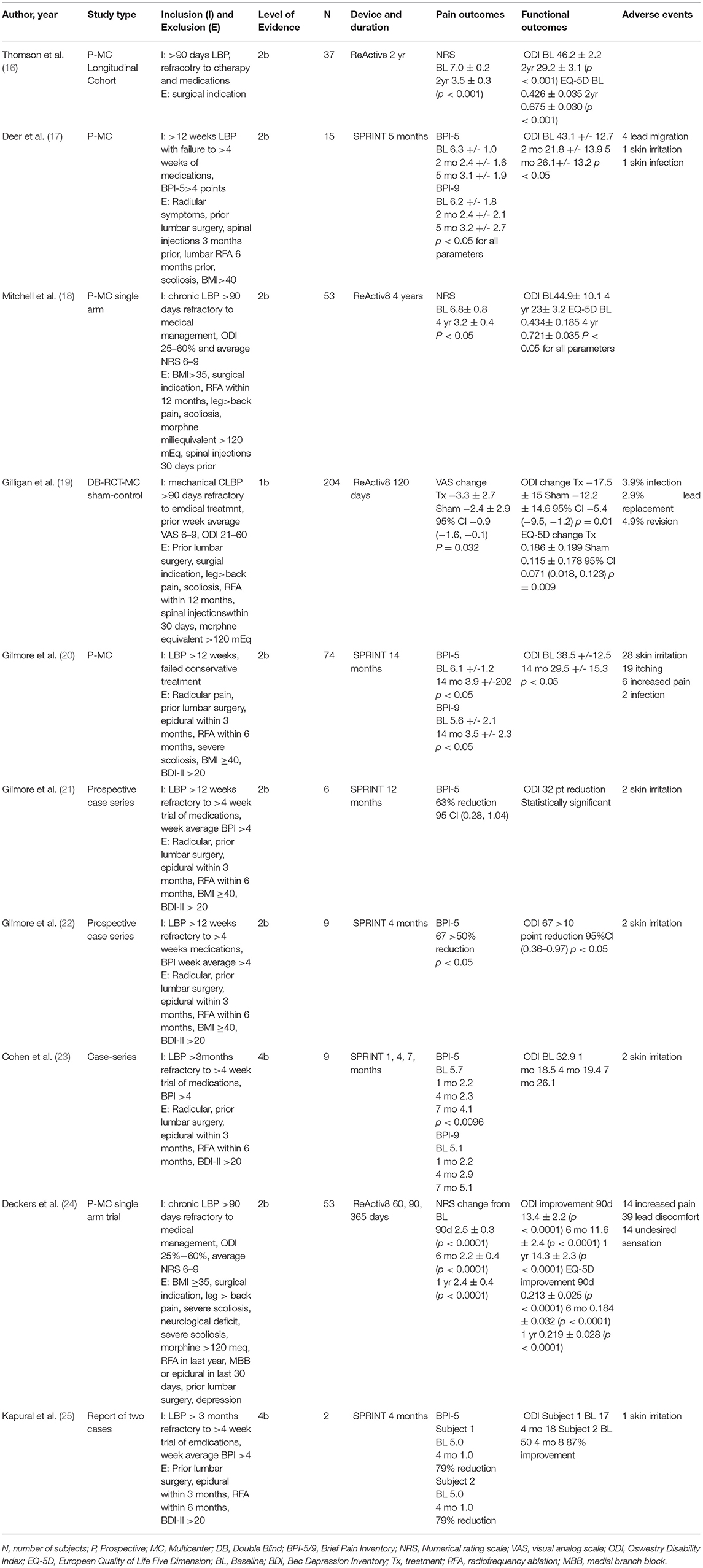
Table 2. Summary of findings.
Currently, there are two types of PNS implantation systems targeting the LMBN: the 60-day percutaneous PNS implant (SPRINT) and the permanently implanted restorative LMBN PNS (ReActiv8). The SPRINT platform proposes a mechanism that is palliative and theorized to modulate afferent pain signals that originate peripherally and move centrally, by means of a fine wire electrode. The ReActiv8 system proposes a mechanism that is restorative and theorized to stimulate efferent signals that originate with the device and cause the multifidus muscle to contract in a rehabilitative fashion. Our search found 25 results for peripheral nerve stimulation and multifidus and 23 results for peripheral nerve stimulation and lumbar medial branch nerve keywords. Forty-eight results were accessed for eligibility, 38 results were excluded from Table 1 since these did not involve human clinical data and/or were duplicates. A total of 10 clinical studies were included, including one randomized controlled trial, one report of two cases and eight prospective case series. These were reviewed, appraised, summarized, and listed in Table 2.
Chronic axial LBP is a highly prevalent and debilitating diagnosis associated with complex biopsychosocial factors treated with inconsistent management and limited successful outcome rates due to numerous anatomical etiologies (10, 26). Due to its complexity, it often requires an interdisciplinary rehabilitative treatment with numerous interventional procedures available for targeting chronic axial LBP, such as epidural steroid injections, facet joint injections, nerve blocks, SCS, etc. each with varying levels of efficacy given the poor specificity of the diagnosis.
There has been a lack of well-designed randomized, controlled studies to determine the effectiveness of epidural steroid injections (ESI) for chronic axial LBP alone, though evidence may favor its use in radicular LBP. Abdi et al. (27) found the evidence is indeterminate in the management of axial LBP and Staal et al. (28) concluded that there was no strong evidence for or against the use of ESI for chronic axial LBP (27, 28). More recently, Manchikanti et al. (29, 30) systematic review and randomized clinical trial found fair evidence for the utilization of caudal and interlaminar ESI and limited for transforaminal ESI (29, 30). Perhaps due to relative inexpensiveness and easy accessibility, ESI are commonly performed to manage symptoms associated with chronic axial LBP, however this targets an acute inflammatory etiology, often not the cause of more chronic axial LBP. SCS effectiveness has been well-documented for chronic lumbar radiculopathy after failed lumbar spine surgery and for complex regional pain syndrome, however there is low-quality evidence that SCS is effective in patients with axial LBP alone (26, 31–36). There are numerous proposed mechanisms of action for SCS, from dorsal column inhibition, to modulating wide-dynamic range neurons, glial cells, ascending and descending pathways; however, all these have a palliative neuromodulatory therapeutic paradigm (31, 36).
Data is slightly more favorable toward the use of intraarticular facet steroid injection for temporary palliation of facet-mediated pain. The systematic review of Manchikanti et al. (37) concluded that there is low-grade evidence for long-term improvement of facet joint pain with intraarticular facet injection, however Mayer et al. (38) found no significant difference in pain and disability comparing facet injections and exercise therapy groups, both with statistically significant improvement (37, 38). Facet joint nerve blocks of the LMBN have been shown to be of diagnostic value for facet-mediated pain, particularly prior to LMBN radiofrequency ablation (RFA). Both facet joint intraarticular injections and LMBN blocks have been shown to improve pain and function short-term, but results are equivocal at long-term (39, 40). Lumbar RFA has been shown to improve pain, function, and QoL at 6-months; however results were not significantly different when compared to intraarticular facet injections (41). There is moderate level I evidence supporting the use of LMBN RFA as a palliative interventional treatment for chronic facet-mediated pain in selected patients (42, 43). Yet, LMBN RFA may have deleterious effects, particularly from the dual innervation of the dorsal ramus of the LMBN to the facet joint and toward the multifidus muscle. LMBN RFA leads to the subsequent denervation of the multifidus muscle. Multifidus denervation leading to disuse atrophy may cause a vicious cycle of dysfunction among the three spinal stabilizing systems (spinal column, spinal muscles, and neural control unit) causing repetitive tissue injury, suboptimal stabilization of forces, improper tissue overloading, intersegmental spinal instability, impaired sensorimotor control, and chronic nociceptive and neuroplastic changes. Thus, a proposed more conservative multifidus sparing RFA would be preferred targeting the terminal end branches of the medial branch of the dorsal root, directly over the facet joint capsule (44). Targeting the LMBN has long proven to have therapeutic value. The most effective means to do so, however, has taken on several different appearances over the past decades in the interventional spine realm, from facet joints injections and blocks to neurotomy and rhizotomy.
More recently, interventional techniques have involved electrically modulating the LMBN, by either modulating pain signals from it or stimulating signals to it to induce multifidus muscle contraction. Two platforms have formally studied targeting the LMBN with differing techniques and mechanisms: SPRINT and ReActiv8. SPRINT works as a 60-day percutaneous PNS platform targeting the LMBN, utilizing a temporary device with cyclical stimulation for 6 h per day for 60 days. The SPRINT has a fine wire that can be implanted under fluoroscopy or ultrasound at any of the LMBN unilaterally or bilaterally. At the 2-month mark, the physician removes the device, as per Food and Drug Administration (FDA) approval. Electrical parameters used by this platform were studied at a frequency of 12 Hz and an amplitude of 5–20 mA (21). Like traditional PNS, the proposed mechanism of action is primarily modulation of the afferent pain signal and disruption of the central sensitization of pain. Secondarily, there is stimulation of efferent nerve signals to activate muscles (21). The ReActiv8 device shares a similar anatomical target, the LMBN, however differs in some key elements. It is a permanent implant with a subcutaneous pulse generator utilizing a more traditional lead design with four electrodes and specialty tines to secure the leads within the intertransversarii muscle next to the L2 LMBN above the L3 transverse process bilaterally. Electrical parameters are similar to SPRINT, with frequency of 20 Hz and amplitude of about 2.5 mA; however, it has a ramp up period, then plateaus, followed by a ramp down period, giving it a more prescribed pattern for each of its two 30-min sessions per day. This is implanted under fluoroscopy, and although the device is not temporary by design, it can be explanted at patient request. The proposed mechanism of action for ReActiv8 is restorative neurostimulation with its primary effector as the efferent nerve to stimulate multifidus muscle contraction in a rehabilitative fashion to increase spinal segmental stability. Central desensitization is thought to be secondary effects of its mechanism of action (19). Similarities and differences of these platforms are summarized in Table 3.

Table 3. Similarities and differences between two different PNS systems for chronic low back pain.
Percutaneous PNS of the LMBN is a relatively new modality, and to date, there are 10 human, clinical studies focusing on non-spinal neuromodulation for chronic axial LBP (16–25). Kapural et al. (25) was the first to publish clinical data using the SPRINT device. Two patients were included, which can only demonstrate general feasibility of the device, and clinical outcomes cannot be reasonably generalized from these two case reports. Cohen et al. (23) conducted a small prospective case series with nine subjects evaluated monthly for a year. They found a statistically significant reduction in both pain and functional scores at all time points. In addition, 83% reported improvement in their quality of life [PGIC 95% CI (0.54–1.13)], which is not a significant value (23). The low patient number is a substantial caveat to generalizing these data, as the risk of spontaneous regression is high.
Gilmore and colleagues produced much of the subsequent literature on the 60-day percutaneous PNS platform. In the 2019 study, they performed a prospective case series with nine patients over 4 months, and demonstrated statistically significant improvement in pain and function when considering >50% pain reduction and >10 point reduction on ODI, respectively (BPI-5 67 >50% reduction p > 0.05, ODI 67% >10 point reduction, 95%CI 0.36–0.97), p >0.05) (22). In this study, the reader should bear in mind the small patient sample and relative data analysis, as objective data would be more robust for extrapolating conclusions. In the 2020 study, Gilmore et al. (21) followed up on six of the previously reported patients at 12 months. This study sought to demonstrate durability of the therapy. There was a statistically significant improvement in function with 32 point reduction as measured by ODI, and there was 63% reduction in pain on BPI-5 that was not statistically significant [95 CI (0.28, 1.04)] (21). Again, with a small sample size, this study can only reasonably conclude the feasibility of the therapy.
Deer et al. (17) conducted a slightly larger prospective multicenter study with 15 subjects and extended their data collection to 5 months. The endpoints used were brief pain inventory (BPI-5), Oswestry disability index (ODI) and brief pain inventory (BPI-9). They found statistically significant pain and functional score improvements at both 2 and 5 month time periods. In addition to this 67 and 80% of patients at 2 and 5 months, respectively had >50% pain reduction. They reported similar trends in both pain interference and disability. At 2 months, 87% of the patients had statistically significant changes in two or more endpoints, which decreased to 73% at 5 months. 93% had clinically significant improvement in at least 1 category at all time points (17). The most recent and robust study of the 60-day percutaneous PNS technique comes from Gilmore et al. (20). In this study, 74 patients across multiple centers were followed for 8 months, with longer follow up visits completed in 51 patients. Pain intensity measured by BPI-5 was improved at 2, 5, and 8 months after implantation in a significant manner (baseline 6.1 to 3.3, 3.6, 3.9 at 2, 5, and 8 months, respectively, p < 0.05). Functional data also demonstrated significant improvement at these intervals (baseline 38.5 on ODI to 22.9, 25.0, and 27.5 at 2, 5, and 8 months, respectively, p < 0.05). The most common adverse events were dermatologic, with skin irritation in 34 of 89 patients (19).
The permanently implanted restorative LMBN PNS system comprises the other arm of the non-spinal neuromodulation for chronic axial LBP scheme. This device is implanted in a minimally invasive fashion, and then stimulates the medial branch of the bilateral L2 LMBN at 20 Hz for 10 s with 20 s off for 30 min twice daily. Deckers et al. (24) initiated the first investigation with 53 subjects in a prospective multicenter trial. Parameters included numeric rating scale (NRS), ODI and quality of life questionnaire (EQ-5D) measured at 3, 6 and 12 months. They found statistically significant improvements in all categories at each time point (p < 0.0001). Deeper analysis of the data to include minimal clinically important difference (MCID) showed that for NRS which required >2pt improvement, 63%, 61%, and 57% of patients reached MCID at 3, 6, and 12 months, respectively (p < 0.0001). This trend was similar to EQ-5D (MCID >0.3). ODI with a MCID >10, had an increasing trend with 52, 57, 60% patient's reaching MCID at 3, 6, 12 months, respectively. 87% of patients at 1 year had MCID in at least 1 category (24).
Following this study, Gilligan et al. (19) published the first double-blinded, randomized, multicenter control trial with 204 patients. They blinded patients and physicians by implanting all subjects and randomizing whether a patient received either therapeutic stimulation or sham stimulation. They evaluated VAS, ODI, and EQ-5D for 120 days. The primary endpoint was based on responder obtaining 30% relief on the LBP visual analog scale without analgesics increase. Then, at 120 days from implantation, the subjects in the sham group crossed over to therapeutic stimulation, and outcome measures were tabulated out to 1 year. At 120 days post-op, the results were inconclusive with a responder rate of 57.1% (treatment) vs 46.6% (sham) (difference 10.4%, 95% CI −3.3 to 24.1%, p = 0.138). However, deeper analysis of the data shows that though the primary outcome was not significant, the actual values of functional outcome measures were significantly improved at 120 days for the treatment group compared to the sham in ODI (difference −5.4 95% CI −9.5 to −1.2, p = 0.011) and EQ-5D (Difference 0.071 95% CI 0.018 to 0.123, p = 0.009) respectively, though VAS trended toward significance (Difference −0.9, 95% CI −1.6 to −0.1, p = 0.032) (19). Next, Thomson et al. (16) investigated NRS, ODI, and EQ-5D changes on 37 patients for 2 years. They found that at 2 years all outcome measures had significantly improved from baseline (p < 0.001) (16). This study design was a prospective, multicenter, longitudinal cohort, and although it is not level 1 evidence, it addresses most causes of bias and presents long-term data, but in a rather small sample size. An important critique is that the data analysis did not include patients who explanted due to inefficacy of the therapy, so the true responder rates may be over-stated. Lastly, Mitchell et al. (18) studied 53 patients in a prospective, multicenter, single arm trial that extended to4 years. Again, all outcome (NRS, ODI, EQ-5D) measures were significantly increased from baseline at the 4-year mark (p < 0.05). Moreover, Mitchell found that 62.5% of participants had clinically meaningful improvement in both NRS and ODI (18). In this study, though the sample size was modest, the long-term follow up is notable as it is the only study in this review with this follow up length. Again, though, true responder rate may be overstated due to the number of patients lost to follow up or explanted, which would be a helpful analysis that is not described in the paper. Overall, the complication rate with this intervention was exceedingly low in comparison with other devices, though adverse events include skin irritation and infections (21).
Both approaches of PNS of the LMBN present unique and promising approaches to treat chronic axial LBP with non-spinal neuromodulation in selected patients who are recalcitrant to conservative treatments. These provide exciting therapies to physicians whose only options previously were epidural injections, medial branch blocks, or RFA, which now may seem counter-intuitive to the therapies reviewed here. Although the two interventions have similar anatomical targets, their approaches, stimulation patterns, chronicity of treatment, and even lead design are quite different. The 60-day percutaneous PNS seeks to provide more palliative peripheral nerve stimulation of the medial branch with thin wire leads and external pulse generator, temporarily implanted for 60-days. Low-frequency pulse train stimulation of the LMBN terminal branches activates both sensory afferents and muscle efferent fibers, producing proprioceptive signals in large diameter fibers that convergently directly activate sensory afferents engaging in the spinal cord gating mechanism. Data are limited but have demonstrated sustained results, even after cessation of 60-day temporary stimulation for patients with multifactorial chronic axial low back pain, including degenerative disc disease, lumbar spondylosis, lumbar facet arthropathy, discogneic pain, etc (17, 20–23, 25). The permanently implanted restorative LMBN PNS system, on the other hand, has a more regimented minimally invasive technique. It specifically targets the L2 LMBN as it traverses over the L3 transverse process and seeks to address multifidus dysfunction to enhance sensorimotor control by restorative neurostimulation for 30 min twice a day at a higher amplitude, without expectation of device explanation. This restorative stimulation has a longer time to maximum impact, and it may take several months for a meaningful clinical improvement to accrue as it is directed to address multifidus muscle dysfunction and impaired sensorimotor control, postulated the root cause of axial low back pain with neuroplastic changes leding to chronicity (19). As research continues to grow examining these two systems, we will gain a deeper understanding of the ideal patient population best suited for each system. For now, it may be hypothesized that SPRINT may be better for the patient who has more of a neuropathic component to multifactorial chronic LBP with disc degeneration, facet arthrpathy, or seeking more immediate analgesia than restoration, without multifidus atrophy, is not able to undergo general anesthesia or otherwise does not want a permanent implant. The ReActiv8 system may be better suited for more active patients with multifidus atrophy on imaging and multifidus dysfunction on physical exam, who are seeking restorative neurostimulation and are motivated and open to the prospect of a permanent implantable device with a long-term durability effect. There is the possibility, too, that these two platforms exist on a continuum or are complementary, and both of these systems may be attempted in select patients. These two approaches can present obvious benefits and drawbacks in different patient populations, which is outside the scope of this review to discuss.
With the firm understanding in differing approaches and proposed mechanisms of action, we caveat some of this discussion with the fact that comparing two different therapies is difficult. Studies examining the permanently implanted restorative LMBN PNS system present more robust clinical data, with respect to rigor of study design, sample size, and follow up time. Their rates of patients who followed up is also slightly better, though both therapies have rather high lost-to-follow-up rates. This may be from device complication, explanation, or patients who are doing well. We also recognize that the global COVID-19 pandemic may have complicated consistent follow up as well. Yet, studies that looked at permanently implanted restorative LMBN PNS need more transparency into loss of follow up and explanation. Comparing primary endpoints of pain reduction and functional improvement, the 60-day percutaneous PNS system demonstrated better early outcomes, though durability appears to favor the permanently implanted restorative LMBN PNS system. This is an important observation considering the two different mechanisms that these therapies utilize. Neither system has examined post-procedural structural changes in the neuromuscular anatomy at long term. Further studies are warranted to investigate post-procedural imaging or electromyographic changes, and when one technology may be preferred or indicated over the other. In addition, comparing each LMBN PNS therapy vs. conventional treatment, namely LMBN blocks and/or RFA, would be an important addition to the literature. Ultimately, it would seem these two modalities—treating the nerve and destroying the nerve—are diametrically opposed. It is therefore of upmost importance for physicians to understand different anatomical etiologies of chronic axial LBP (i.e., facet-mediated pain vs. multifidus dysfunction), their therapeutic paradigms, and the proper patient selection criteria for these contrasting interventions.
As per the constraints of our review, there are only 10 studies published to date, one randomized controlled trial, one report of two cases and eight prospective studies. The available literature on PNS of the LMBN has limitations. All published studies to date have been industry sponsored, which evidently potentialize the risk of publication bias and conflict of interest. In fact, our study is non-sponsored by industry and we aimed to provide a non-biased comprehensive overview of current data on LMBN PNS of the two commercially available systems. It is always prudent to comment on the limitations of generalizability in such a setting. Data is in its infancy and more robust and larger studies are needed, including regression analysis of non-responders, subgroup analysis, and categorizing patient selection more specifically, including validation of multifidus dysfunction and standardization of inclusion and exclusion criteria in relationship to the pain generator addressed by the intervention. Perhaps this is the essential difference to clarify between these available devices, that although both target the LMBN, one addresses proposed dysfunction of the multifidus, while the other focuses on chronic axial LBP with different etiologies. Therefore, because our review evaluated different devices with proposed different mechanisms of action and clinical indications, thus a high level of heterogeneity is introduced. As we seek more personalized medicine within interventional spine and pain, we will need to continue to answer these questions to provide our patients with safe and superior outcomes.
This review examines the clinical data of two different non-spinal neuromodulation systems for the treatment of chronic axial LBP. This provides the clinician a succinct narrative that presents these data objectively. Evidence suggests that PNS of the LMBN is safe and effective to improve pain and function in patients with chronic axial LBP symptoms at short and long term. With continued advancements in neuromodulation technology from ongoing research, miniaturization of devices, sophistication of procedural techniques, and wireless capability, we have the promising ability to target a highly prevalent and costly condition with PNS of the LMBN.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
DS is a research investigator for Mainstay Medical.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Förster M, Mahn F, Gockel U, Brosz M, Freynhagen R, Tolle TR, et al. Axial low back pain: one painful area–many perceptions and mechanisms. PLoS ONE. (2013) 8:e68273. doi: 10.1371/journal.pone.0068273
2. Schmidt CO, Schweikert B, Wenig CM, Schmidt U, Gockel U, Freynhagen R, et al. Modelling the prevalence and cost of back pain with neuropathic components in the general population. Eur J Pain. (2009) 13:1030–5. doi: 10.1016/j.ejpain.2008.12.003
3. Wong AYL, Karppinen J, Samartzis D. Low back pain in older adults: risk factors, management options and future directions. Scoliosis Spinal Disord. (2017) 12:14. doi: 10.1186/s13013-017-0121-3
4. Sauver JLS, Warner DO, Yawn BP, Jacobson J, Gree MEM, Pankratz JJ, et al. Why do patients visit their doctors? assessing the most prevalent conditions in a defined US population. Mayo Clin Proc. (2014) 88:56–67. doi: 10.1016/j.mayocp.2012.08.020
5. Henschke N, Kamper SJ, Maher CG. The epidemiology and economic consequences of pain. Mayo Clin Proc. (2015) 90:139–47. doi: 10.1016/j.mayocp.2014.09.010
6. Anderson GB. Epidemiology of low back pain. Acta Orthop Scand Suppl. (1998) 281:28–31. doi: 10.1080/17453674.1998.11744790
7. Hoy D, Brooks P, Blyth F, Buchbinder R. The epidemiology of low back pain. Best Pract Res Clin Rheumatol. (2010) 24:769–81. doi: 10.1016/j.berh.2010.10.002
8. Maniadakis N, Gray A. The economic burden of back pain in the UK. Pain. (2000) 84:95–103. doi: 10.1016/S0304-3959(99)00187-6
9. Russo M, Deckers K, Eldabe S, Kiesel K, Gilligan C, Vieceli J, et al. Muscle control and non-specific chronic low back pain. Neuromodulation. (2018) 21:1–9. doi: 10.1111/ner.12738
10. Urits I, Burshtein A, Sharma M, Testa L, Gold PA, Orhurhu V, et al. Low back pain, a comprehensive review: pathophysiology, diagnosis, and treatment. Curr Pain Headache Rep. (2019) 23:23. doi: 10.1007/s11916-019-0757-1
11. Massé-Alarie H, Beaulieu LD, Preuss R, Schneider C. Corticomotor control of lumbar multifidus muscles is impaired in chronic low back pain: concurrent evidence from ultrasound imaging and double-pulse transcranial magnetic stimulation. Exp Brain Res. (2016) 234:1033–45. doi: 10.1007/s00221-015-4528-x
12. Seyedhoseinpoor T, Taghipour M, Dadgoo M, Sanjari MA, Takamjani IE, Kazemnejad A, et al. Alteration of lumbar muscle morphology and composition in relation to low back pain: a systematic review and meta-analysis. Spine J. (2021). doi: 10.1016/j.spinee.2021.10.018. [Epub ahead of print].
13. Goubert D, Oosterwijck JV, Meeus M, Danneels L. Structural changes of lumbar muscles in non-specific low back pain: a systematic review. Pain Physician. (2016) 19:E985–1000. doi: 10.36076/ppj/2016.19.E985
14. Tieppo Francio V, Sherwood D, Twohey E, Barndt B, Pagan-Rosado R, Eubanks J, et al. Developments in minimally invasive surgical options for vertebral pain: basivertebral nerve ablation - a narrative review. J Pain Res. (2021) 14:1887–907. doi: 10.2147/JPR.S287275
15. Kreiner DS, Matz P, Bono CM, Cho CH, Easa JE, Ghiselli G, et al. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of low back pain. Spine J. (2020) 20:998–1024. doi: 10.1016/j.spinee.2020.04.006
16. Thomson S, Chawla R, Love-Jones S, Sharma M, Vajramani G, Williams A, et al. Restorative neurostimulation for chronic mechanical low back pain: results from a prospective multi-centre longitudinal cohort. Pain Ther. (2021) 10:1451–65. doi: 10.1007/s40122-021-00307-3
17. Deer TD, Gilmore G, Desai MJ, Li SC, DePalma MJ, Hopkins TJ, et al. Percutaneous peripheral nerve stimulation of the medial branch nerves for the treatment of chronic axial back pain in patients after radiofrequency ablation. Pain Med. (2021) 22:548–60. doi: 10.1093/pm/pnaa432
18. Mitchell B, Deckers K, Smedt KD, Russo M, Georgius P, Green M, et al. Durability of the therapeutic effect of restorative neurostimulation for refractory chronic low back pain. Neuromodulation. (2021) 24:1024–32. doi: 10.1111/ner.13477
19. Gilligan C, Volschenk W, Russo M, Green M, Gilmore C, Mehta V, et al. An implantable restorative-neurostimulator for refractory mechanical chronic low back pain. Pain. (2021) 162:2486–98. doi: 10.1097/j.pain.0000000000002258
20. Gilmore CA, Desai MJ, Hopkins TJ, Li S, DePalma MJ, Deer TR, et al. Treatment of chronic axial back pain with 60-day percutaneous medial branch PNS: primary end point results from a prospective, multicenter study. Pain Pract. (2021) 21:877–89. doi: 10.1111/papr.13055
21. Gilmore CA, Kapural L, McGee MJ, Boggs JW. Percutaneous peripheral nerve stimulation for chronic low back pain: prospective case series with 1 year of sustained relief following short-term implant. Pain Pract. (2020) 20:310–20. doi: 10.1111/papr.12856
22. Gilmore CA, Kapural L, McGee M, Boggs J. Percutaneous peripheral nerve stimulation (PNS) for the treatment of chronic low back pain provides sustained relief. Neuromodulation. (2019) 22:615–20. doi: 10.1111/ner.12854
23. Cohen S, Gilmore C, Kapural L, Hanling SR, Plunkett AR, McGee MJ, et al. Percutaneous peripheral nerve stimulation for pain reduction and improvements in functional outcomes in chronic low back pain. Mil Med. (2019) 184(Suppl. 1):537–41. doi: 10.1093/milmed/usy310
24. Deckers K, De Smedt K, Mitchell B, Vivian D, Russo M, Georgius P, et al. New therapy for refractory chronic mechanical low back pain-restorative neurostimulation to activate the lumbar multifidus: one year results of a prospective multicenter clinical trial. Neuromodulation. (2018) 21:48–55. doi: 10.1111/ner.12741
25. Kapural L, Gilmore CA, Chae J, Rauck RL, Cohen SP, Saulino MF, et al. Percutaneous peripheral nerve stimulation for the treatment of chronic low back pain: two clinical case reports of sustained pain relief. Pain Pract. (2018) 18:94–103. doi: 10.1111/papr.12571
26. Tieppo Francio V, Polston KF, Murphy MT, Hagedorn JM, Sayed D. Management of chronic and neuropathic pain with 10 kHz spinal cord stimulation technology: summary of findings from preclinical and clinical studies. Biomedicines. (2021) 9:644. doi: 10.3390/biomedicines9060644
27. Abdi S, Datta S, Trescot AM, Schultz DM, Adlaka R, Atluri SL, et al. Epidural steroids in the management of chronic spinal pain: a systematic review. Pain Physician. (2007) 10:185–212. doi: 10.36076/ppj.2007/10/185
28. Staal JB, de Bie R, de Vet HC, Hildebrandt J, Nelemans P. Injection therapy for subacute and chronic low-back pain. Cochrane Database Syst Rev. (2008) 2008:CD001824. doi: 10.1002/14651858.CD001824.pub3
29. Manchikanti L, Cash KA, McManus CD, Pampati V, Benyamin RM. A randomized, double-blind, active-controlled trial of fluoroscopic lumbar interlaminar epidural injections in chronic axial or discogenic low back pain: results of 2-year follow-up. Pain Physician. (2013) 16:E491–504. doi: 10.36076/ppj.2013/16/E494
30. Manchikanti L, Abdi S, Atluri S, Benyamin RM, Boswell MV, Buenaventura RM, et al. An update of comprehensive evidence-based guidelines for interventional techniques of chronic spinal pain: part II: guidance and recommendations. Pain Physician. (2013) 16:S49–283. doi: 10.36076/ppj.2013/16/S49
31. Caylor J, Reddy R, Yin S, Cui C, Huang M, Huang C, et al. Spinal cord stimulation in chronic pain: evidence and theory for mechanisms of action. Bioelectron Med. (2019) 5:12. doi: 10.1186/s42234-019-0023-1
32. Sayed D, Kallewaard JW, Rotte A, Jameson J, Caraway D. Pain relief and improvement in quality of life with 10 kHx SCS therapy: summary of clinical evidence. CNS Neurosci Ther. (2020) 26:403–15. doi: 10.1111/cns.13285
33. Al-Kaisy A, Palmisani S, Smith TE, Carganillo R, Houghton R, Pang D, et al. Long-term improvements in chronic axial low back pain patients without previous spinal surgery: a cohort analysis of 10-kHz high-frequency spinal cord stimulation over 36 months. Pain Med. (2018) 19:1219–26. doi: 10.1093/pm/pnx237
34. Al-Kaisy A, Van Buyten JP, Kapural L, Amirdelfan K, Gliner B, Caraway D, et al. 10 kHz spinal cord stimulation for the treatment of non-surgical refractory back pain: subanalysis of pooled data from two prospective studies. Anesthesia. (2020) 75:775–84. doi: 10.1111/anae.15036
35. Russo M, Brooker C, Cousins MJ, Taylor N, Boesel T, Sullivan R, et al. Sustained long-term outcomes with closed-loop spinal cord stimulation: 12-month results of the prospective, multicenter, open-label avalon study. Neurosurgery. (2020) 15:485–95. doi: 10.1093/neuros/nyaa003
36. Malinowski MN, Chopra PR, Tieppo Francio V, Budwany R, Deer TR. A narrative review and future considerations of spinal cord stimulation, dorsal root ganglion stimulation and peripheral nerve stimulation. Curr Opin Anaesthesiol. (2021) 34:774–80. doi: 10.1097/ACO.0000000000001072
37. Manchikanti L, Kaye AD, Boswell MV, Bakshi S, Gharibo CG, Grami V, et al. A systematic review and best evidence synthesis of the effectiveness of therapeutic facet joint interventions in managing chronic spinal pain. Pain Physician. (2015) 18:E535–82. doi: 10.36076/ppj.2015/18/E535
38. Mayer TG, Gatchel RJ, Keeley J, McGeary D, Dersh J, Anagnostis C, et al. randomized clinical trial of treatment for lumbar segmental rigidity. Spine. (2004) 29:2199–205. doi: 10.1097/01.brs.0000142009.73869.8d
39. Manchikanti L, Singh V, Falco FJ, Cash K, Pampati V. Lumbar facet joint nerve blocks in managing chronic facet joint pain: one-year follow-up of a randomized, double-blind controlled trial: clinical trial NCT00355914. Pain Physician. (2008) 11:121–32. doi: 10.36076/ppj.2008/11/121
40. Kennedy DJ, Huynh L, Wong J, Mattie R, Levin J, Smuck M, et al. Corticosteroid injections into lumbar facet joints: a prospective, randomized, double-blind placebo-controlled trial. Am J Phys Med Rehabil. (2018) 97:741–6. doi: 10.1097/PHM.0000000000000960
41. Lakemeier S, Lind M, Schultz W, Fuchs-Winkelmann S, Timmesfeld N, Foelsch C, et al. A comparison of intraarticular lumbar facet joint steroid injections and lumbar facet joint radiofrequency denervation in the treatment of low back pain: a randomized, controlled, double-blind trial. Anesth Analg. (2013) 117:228–35. doi: 10.1213/ANE.0b013e3182910c4d
42. Manchikanti L, Kaye AD, Soin A, Albers SL, Beall D, Latchaw R, et al. Comprehensive evidence-based guidelines for facet joint interventions in the management of chronic spinal pain: american society of interventional pain physicians (ASIPP) guidelines facet joint interventions 2020 guidelines. Pain Physician. (2020) 23:S1–127. doi: 10.36076/ppj.2020/23/S1
43. Lee DW, Pritzlaff S, Jung MJ, Ghosh P, Hagedorn JM, Tate J, et al. Latest evidence-based application for radiofrequency neurotomy (LEARN): best practice guidelines from the american society of pain and neuroscience (ASPN). J Pain Res. (2021) 14:2807–31. doi: 10.2147/JPR.S325665
Keywords: peripheral nerve stimulation, multifidus, lumbar medial branch, low back pain, neuromodulation
Citation: Tieppo Francio V, Westerhaus BD, Rupp A and Sayed D (2022) Non-Spinal Neuromodulation of the Lumbar Medial Branch Nerve for Chronic Axial Low Back Pain: A Narrative Review. Front. Pain Res. 3:835519. doi: 10.3389/fpain.2022.835519
Received: 14 December 2021; Accepted: 28 January 2022;
Published: 25 February 2022.
Edited by:
Cletus Cheyuo, University of Toronto, CanadaReviewed by:
Holger Joswig, Health and Medical University Potsdam, GermanyCopyright © 2022 Tieppo Francio, Westerhaus, Rupp and Sayed. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dawood Sayed, ZHNheWVkQGt1bWMuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.