
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pain Res. , 24 December 2021
Sec. Pain Mechanisms
Volume 2 - 2021 | https://doi.org/10.3389/fpain.2021.740897
This article is part of the Research Topic Mechanisms of Chronic Pain and Individualized Medicine View all 4 articles
 Tania Augière1,2
Tania Augière1,2 Audrey Desjardins1,2
Audrey Desjardins1,2 Emmanuelle Paquette Raynard3
Emmanuelle Paquette Raynard3 Clémentine Brun1
Clémentine Brun1 Anne Marie Pinard1,4
Anne Marie Pinard1,4 Martin Simoneau1,5
Martin Simoneau1,5 Catherine Mercier1,2*
Catherine Mercier1,2*Fibromyalgia is a chronic pain syndrome characterized by sensorimotor deficits and distortions of body representation, that could both be caused by alterations in sensory processing. Several studies suggest a hypersensitivity to various sensory stimulations in fibromyalgia but results on detection of both noxious and non-noxious tactile stimulation, which are particularly relevant for body representation and motor control, remain conflicting. Therefore, the aim of this study is to systematically review and quantify the detection thresholds to noxious and non-noxious tactile stimuli in individuals with fibromyalgia compared to pain-free controls. A systematic review and a meta-analysis were performed in the MEDLINE, EMBASE, CINAHL, Cochrane, PsycInfo and Web of Science databases using keywords related to fibromyalgia, tactile pain detection threshold, tactile detection threshold and quantitative sensory testing. Nineteen studies were included in the review, with 12 in the meta-analysis. Despite the heterogeneity of the results, the data from both the review and from the meta-analysis suggest a trend toward hyperalgesia and no difference of sensitivity to non-noxious tactile stimuli in participants with fibromyalgia compared to healthy controls. This contradicts the hypothesis of a general increase in responsiveness of the central nervous system to noxious and non-noxious stimulations in fibromyalgia. This study shows no alteration of the sensitivity to non-noxious tactile stimulation in fibromyalgia, suggesting that an altered unimodal processing is not sufficient to explain symptoms such as sensorimotor impairments and body representation distortions. Future research should investigate whether alterations in multisensory integration could contribute to these symptoms.
Fibromyalgia is a chronic widespread pain syndrome that affects 2% of the world population (1, 2) and is characterized by various symptoms including sensorimotor deficits (3–5) and distortions of body representation (6–10). These symptoms could partly stem from an altered processing of sensory information. Intact unimodal processing of sensory information is essential for subsequent integration of these signals among other information (i.e. multimodal integration), which is at the core of body representation (11, 12) and motor control (13–15).
An extensive literature on unimodal processing of sensory information suggests that persons with fibromyalgia are hypersensitive to auditory stimulations (16–20), olfactory stimulations (21), and somatosensory stimulations, such as thermal (22–32), pressure (22, 24, 25, 27, 28, 30, 32–36) and electrical stimulations (22, 33, 37). In fact, the presence of body areas hypersensitive to pressure, called tender points, is one of the most common symptoms of fibromyalgia (38). This hyperalgesia (i.e., hypersensitivity to noxious stimuli) is often accompanied by allodynia [i.e., a painful response to non-noxious stimuli such as light touch or warmth (39)] and is not restricted to tender points (40, 41). Several studies show an altered perception of both noxious and non-noxious stimulations in fibromyalgia (24, 28, 30, 42). Using thermal stimulation, Kosek et al. (41) demonstrated an increased sensitivity to noxious and non-noxious stimulations on sites of maximal pain and a decreased sensitivity to both types of stimulation on sites of minimal pain. However, other authors reported contradictory findings regarding the altered perception of non-noxious stimuli (22, 31, 43–45) or its direction (42). These somatosensory alterations are measured with Quantitative Sensory Testing (QST), a standardized method used to assess sensory system functioning (46). The test procedure enables to obtain and to compare the detection thresholds to various stimuli (tactile, thermal, pressure etc.) between groups of individuals. A recent systematic review (47) examined the perception of thermal stimulation in fibromyalgia and showed that most studies using QST reported hyperalgesia to cold (82% of the studies) and heat stimulations (77% of the studies) in fibromyalgia but no alterations in the detection of non-noxious cold stimulations (70.6%). However, results on the alterations of perception of noxious and non-noxious stimuli for other sensory modalities in fibromyalgia remain conflicting.
Processing of tactile stimulation has been highlighted as particularly relevant for body representation (48) and motor control (49), two aspects that have been shown to be altered in individuals with fibromyalgia. Therefore, the aim of the present study is to systematically review and quantify the detection thresholds to noxious and non-noxious tactile stimuli in individuals with fibromyalgia compared to pain-free controls. According to the symptomatology of fibromyalgia, it is hypothesized that individuals with fibromyalgia would exhibit hypersensitivity to both noxious (i.e., hyperalgesia) and non-noxious stimuli (hyperesthesia).
This systematic review was conducted in accordance with the PRISMA statement (50).
The protocol of the review was registered in PROSPERO (www.crd.york.ac.uk/prospero), an international database for the prospective registration of systematic reviews on the 08/27/20 (registration number: CRD42020198167).
A systematic search was conducted on the 06/18/20 by a professional librarian in the electronic databases MEDLINE, EMBASE, CINAHL, Cochrane, PsycInfo and Web of Science (see Supplementary Material). The search was restricted to studies in English and in French, with no publication date limit. Keywords used for the search included “Fibromyalgia,” “Quantitative sensory testing,” “Tactile detection threshold,” and “Tactile pain detection threshold.” The strategy was personalized for each database. An additional manual search was performed in the reference lists of the included articles. Search results were exported to Covidence (www.covidence.org), a systematic review management website, for automatic duplicates removal.
Only peer-reviewed papers were included in the systematic review. To be included, studies had to include (1) a fibromyalgia group and a pain-free group; and (2) a measure of tactile detection thresholds (TDT) or tactile pain detection thresholds (TPT). Comorbidities could be present in the fibromyalgia group and there was no age restriction for either participant groups. Animal studies and studies written neither in English nor in French were excluded.
The selection process followed 2 steps. First, two reviewers (T.A. and A.D.) independently screened the titles and abstracts of the articles according to the inclusion and exclusion criteria. If there was any uncertainty regarding the eligibility of a study, the paper was kept for the second step. Then, the two reviewers independently reviewed the full text of the selected articles, still according to the inclusion and exclusion criteria. For each step, an agreement between the two reviewers had to occur to include the article. If a disagreement arose, a discussion between the two reviewers occurred to reach a consensus, or the judgement of a third author (C.B. or C.M.) was sought if needed.
The quality of the included studies was independently assessed by the two reviewers according to the Standard quality assessment criteria for evaluating primary research papers from a variety of fields (51). This quality assessment tool includes 14 criteria, each evaluated on a 2-point scale (2 – element sufficiently described, and no added bias introduced in the results; 1 – element not sufficiently described but no added bias introduced in the results; 0 – element not mentioned or added bias in the results). The quality score of each study was expressed as a percentage and interpreted with the following scale (52): 90% and more is a very high quality, 80–89% is a high quality, 70–79% is a moderate quality, 60–69% is a low quality, 59% and less is a very low quality. Because three of the 14 criteria related to interventional studies, only 11 criteria were used for quality assessment.
The Gwet's coefficient was calculated for each criterion of the quality scale to evaluate the inter-rater agreement (53). The agreement was interpreted as poor (inferior to 0.0), slight (0.0 to 0.20), fair (0.21 to 0.40), moderate (0.41 to 0.60), substantial (0.61 to 0.80), or almost perfect [0.81 to 1.00 (53)]. Any discrepancy between the evaluation of the two reviewers was resolved by a consensual decision, or the judgement of a third author was sought if needed.
The following variables were extracted from the included articles:
1) sample data (number of participants in each group, age, sex, mean pain intensity of the participants with fibromyalgia, whether medication was stopped prior to participation);
2) methodological characteristics (threshold type, tool used, threshold assessment method, threshold definition, stimulated sites and whether they were painful in the fibromyalgia group, order of the presentation if several modalities of stimulation were tested in the same study, statistical tests performed);
3) the results (means and standard deviations of the thresholds for each group according to the stimulated site, t- or F-value, p-value).
In order to quantify the threshold difference between the fibromyalgia and the control group, Cohen's d, a quantification of effect size (54), was calculated using the website EffectSizeCalculator (www.campbellcollaboration.org/escalc/html/EffectSizeCalculator-SMD1.php). If data were missing to calculate Cohen's d, an email was sent to the corresponding author to obtain the required data. In our study, a positive d reflected a hyposensitivity (hypoesthesia or hypoalgesia, for non-noxious and noxious stimuli, respectively), to tactile stimuli in fibromyalgia and a negative d was associated to a hypersensitivity (hyperesthesia or hyperalgesia) in fibromyalgia.
To synthesize the effect sizes of the included studies, a global effect size D was calculated with an univariate random-effects model (55) for each threshold (TDT and TPT) using R Studio (RStudio, Inc., Boston, MA). The random-effects model accounts for the variability between the studies included. D was calculated using one effect d per study because the conditions of application of the effect size prohibits the use of dependent samples. Hence, the “distal upper limb area” (hand, wrist, forearm) was chosen as a common stimulation area. This area was selected because (1) it was the most frequently stimulated area across studies and therefore allowed for a larger number of studies to be included in the meta-analysis and (2) it is not a tender point in fibromyalgia and thus it would indicate whether somatosensory alterations in fibromyalgia were generalized to non-tender sites. The studies excluded from the meta-analysis were synthesized in the qualitative analysis to assess the risk of bias due to missing results in the meta-analysis.
Heterogeneity was assessed with Cochran's Q (56).
The electronic literature search yielded 4,924 articles, among which 2,049 duplicates were removed by Covidence. The screening of titles and abstracts led to the exclusion of 2,513 additional articles. The full-text analysis led to the exclusion of 343 supplementary articles because there were not scientific papers (n = 179), they did not measure tactile thresholds (n = 116), they were duplicates (n = 24), they did not include a pain-free control group (n = 17), they were not written in English nor in French (n = 4) or they did not include a fibromyalgia group (n = 3). The selection process is reported in the PRISMA flow-chart (Figure 1). In total, 19 studies were included in the systematic review. The extraction table is available in the Supplementary Material.
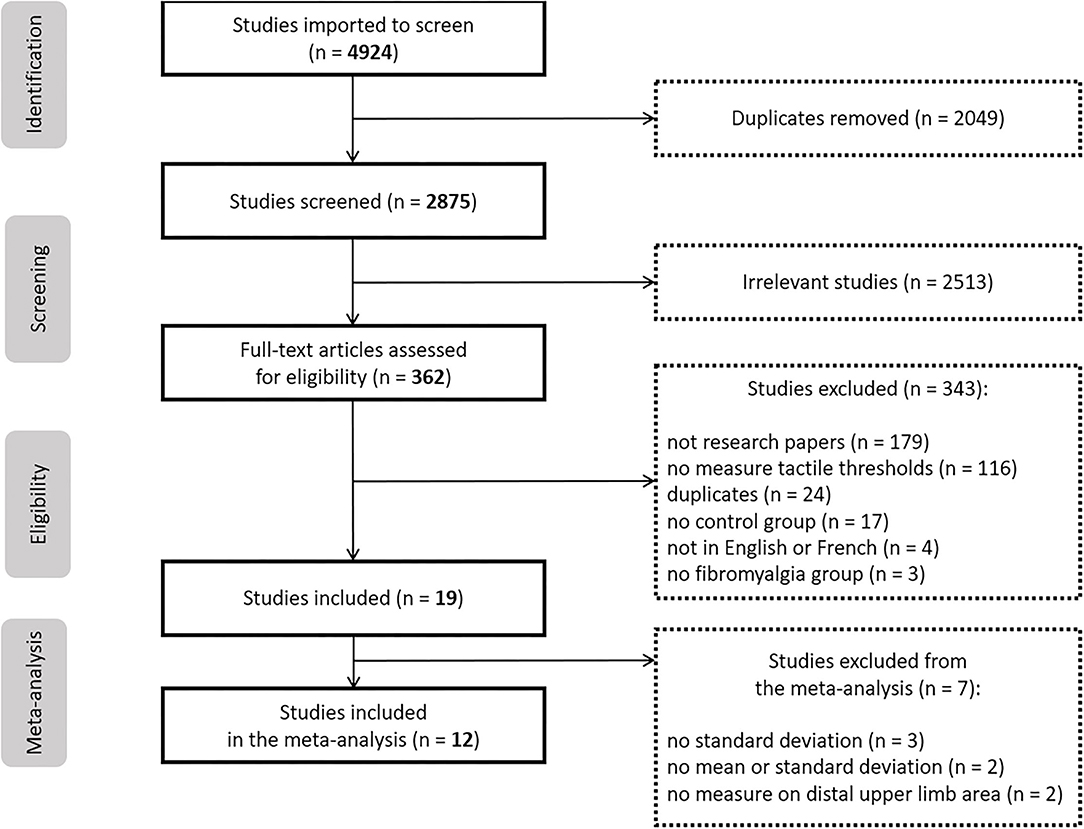
Figure 1. PRISMA flowchart.
Of these 19 studies, 14 included TDT assessments and 14 included TPT assessments. Twelve articles were included in the meta-analysis, for a total of eight studies with TDT assessment and nine studies with TPT assessment (some studies assessing both types of thresholds). The remaining seven studies were excluded from the meta-analysis because: 1- the standard deviation of the threshold was missing (n = 3); 2- the threshold was only expressed in z-score (n = 2); 3- the distal upper limb area was not studied (n = 2). The corresponding authors of these studies were contacted to obtain the missing data, but they either did not respond (n = 5) or could not provide the missing information (n = 2).
According to Gwet's coefficient, the mean inter-rater agreement across all criteria was almost perfect (0.81 ± 0.15). Among the 11 criteria, the coefficient ranged from 0.57 to 1.
After consensus between the two reviewers, the mean quality score was high (80.9 ± 7.7%) and ranged from 65.9% (low) to 90.9% (very high) across all the studies.
In total 690 individuals with fibromyalgia and 643 pain-free controls were included. All participants were adults (mean age of 45.7 ± 6.2). 95.7% of participants with fibromyalgia and 86.6% of pain-free controls were women [one study did not indicate the proportion of men and women (57)]. Fourteen studies out of the 19 reported a mean pain intensity rating, either at the moment of the participation [n = 10; (24, 27, 31, 34, 36, 37, 57–60)] or within the last month prior [n = 4; (30, 33, 35, 61)]. In nine studies, including five in the meta-analysis (32, 57, 59, 61, 62), individuals with fibromyalgia were instructed to stop taking their medication prior to their participation (27, 30, 32, 33, 57, 59, 61–63).
For the meta-analysis, 474 individuals with fibromyalgia and 461 pain-free controls were included. The mean age was 45.4 ± 7.4 years, 94.3% of participants with fibromyalgia and around 85.4% of pain-free controls were women.
The TDT was assessed with Von Frey filaments in all studies except one (60) in which unspecified nylon filaments were used. For the TPT, five studies involved pinprick stimulators (27, 28, 30, 32, 35, 36, 61), five involved Von Frey filaments (34, 37, 57, 62, 63), one involved unspecified nylon filaments (60) and one involved disposable needles (59).
Out of the 19 studies, 15 used the method of limits (24, 27, 28, 30, 32, 34–37, 41, 57, 60–63), one the staircase method (58) and three did not report the method used (31, 33, 59). In the method of limits, the stimulus intensity increases or decreases continuously, and the participants have to say when they detect or stop detecting the stimulation (46), whereas in the staircase method, the stimulus intensity increases or decreases according to whether the participant detects the stimulus (64).
The most frequently stimulated site was the hand [13 studies (24, 27, 28, 30, 31, 34, 35, 57–62)], then the back [seven studies (27, 28, 30, 33, 37, 60, 61)], the foot (30, 35, 36), the face (28, 59, 60) and the forearm (32, 37, 63); three studies each, and the elbow (58), the tibia (59), and the sternum (24) (one study each).
Three studies reported a hypoesthesia in persons with fibromyalgia compared to controls (34, 36, 60), whereas eight studies reported no difference between the groups (27, 30, 31, 33, 35, 58, 59, 61). The remaining three studies reported either no significant difference or a hypoesthesia, depending on the site stimulated (24, 28, 41). As shown in Table 1, the studies reporting a significant difference between the groups were not of better or lower quality than the studies reporting no difference. Moreover, no substantial differences were identified across these studies in terms of methodology, sample sizes, or mean pain ratings.
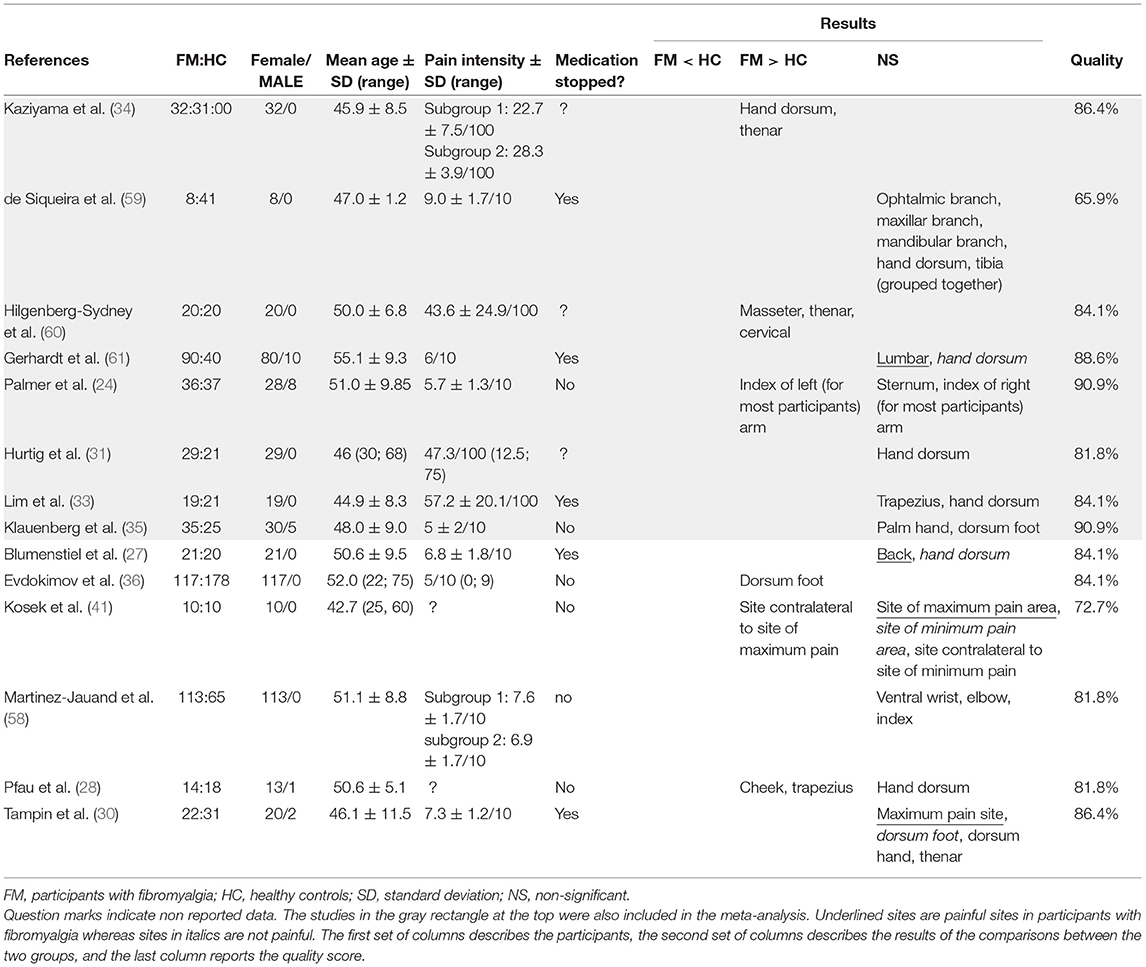
Table 1. Studies included in the review with measures of TDT.
The eight studies included in the meta-analysis yielded a non-significant summarized effect size D of 0.61 (Figure 2). Cochran's Q revealed a significant heterogeneity in the studies' results [Q (df = 7) = 90.26, p < 0.0001]. The study with the extreme result (34) was of high quality (score of 86%). No notable difference was found between this study and the rest of the studies included in the meta-analysis.
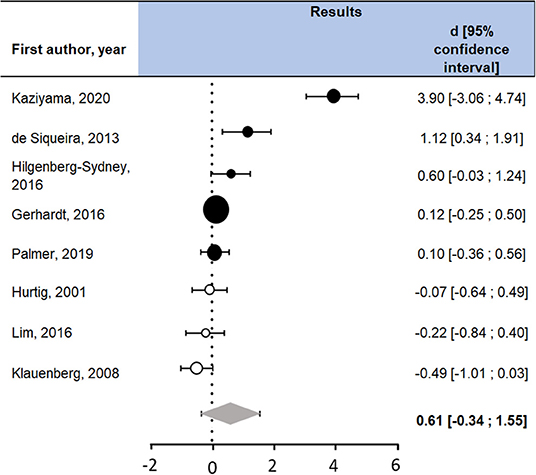
Figure 2. Studies included in the meta-analysis with measures of TDT. FM, participants with fibromyalgia; HC, healthy controls; SD, standard deviation. Question marks indicate non-reported data. A positive d (in black) can be interpreted as a hypoalgesia in participants with fibromyalgia compared to healthy controls, whereas a negative d (in white) means there is a hyperalgesia in participants with fibromyalgia compared to healthy controls. The summarized Cohen's d is represented by the gray diamond. Confidence intervals containing zero means the d is not statistically significant.
Given the heterogeneity of the results, it is difficult to draw a conclusion regarding the difference of perception of non-noxious tactile stimulation between individuals with fibromyalgia and controls.
Six studies reported a hyperalgesia in participants with fibromyalgia compared to controls (27, 32, 34, 57, 60, 62) whereas two reported a hypoalgesia (36, 59) and four reported no significant difference between the groups (30, 35, 61, 63). In two studies, either no significant difference or an hyperalgesia was observed, depending on the stimulated site (28, 37). As shown in Table 2, no notable differences in quality scores, methodology, sample sizes, or mean pain ratings were found between the studies reporting different results.
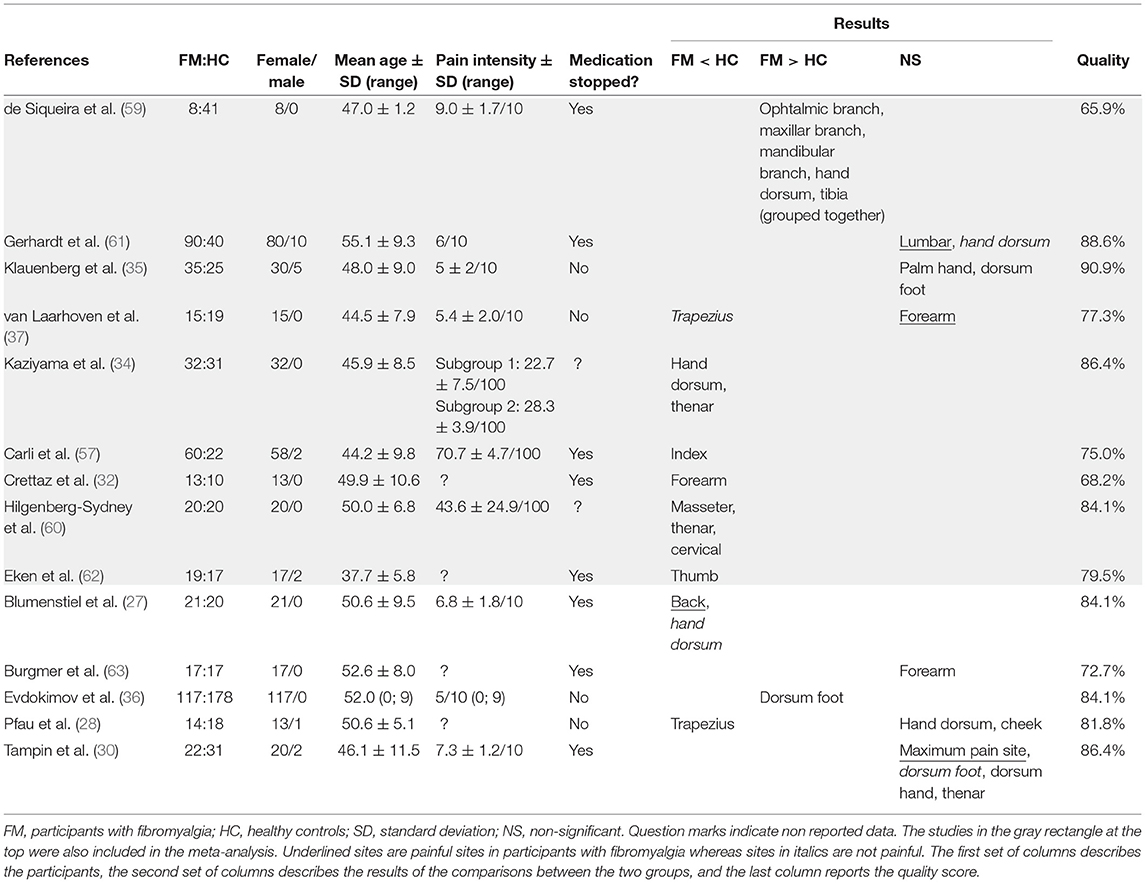
Table 2. Studies included in the review with measures of TPT.
The nine studies included in the meta-analysis resulted in a non-significant D of −0.81, with a tendency toward hyperalgesia in fibromyalgia (Figure 3). Cochran's Q showed a significant heterogeneity [Q (df = 8) = 73.37, p < 0.0001]. The study with the extreme result (62) was of moderate quality (score of 79%). No notable difference was found between this study and the rest of the studies included in the meta-analysis.
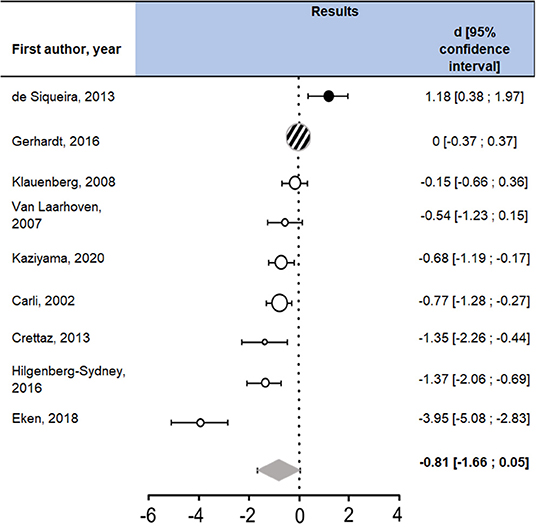
Figure 3. Studies included in the meta-analysis with measures of TPT. FM, participants with fibromyalgia; HC, healthy controls; SD, standard deviation. Question marks indicate non-reported data. A positive d (in black) can be interpreted as a hypoalgesia in participants with fibromyalgia compared to healthy controls, whereas a negative d (in white) means there is a hyperalgesia in participants with fibromyalgia compared to healthy controls. Gerhardt et al.'s study indicated a d equal to zero, represented by a striped circle. The summarized Cohen's d is represented by the gray diamond. Confidence intervals containing zero means the d is not statistically significant.
The data suggest a trend toward hyperalgesia in fibromyalgia, though the heterogeneity of the results prevents a definitive conclusion.
This work is the first to systematically review findings from studies assessing sensitivity to noxious and non-noxious tactile stimuli in individuals with fibromyalgia. Findings were yielded from 19 studies with an overall high quality and the results of 12 of these studies were synthesized in a meta-analysis. Despite the heterogeneity of the results, the data suggest a trend toward hyperalgesia and no difference of sensitivity to non-noxious tactile stimuli in participants with fibromyalgia compared to healthy controls, at least outside of tender points, which contradicts the hypothesis of a general increase in responsiveness of the central nervous system to noxious and non-noxious stimulations in fibromyalgia (65, 66). In this section, the implications of these results and the substantial heterogeneity of the results of the studies included will be discussed, then the limitations of this review will be examined, and finally some perspectives will be proposed.
Several studies reported differences in cerebral activation evoked by noxious stimuli in individuals with fibromyalgia compared to controls. In a study in which participants received noxious stimuli of similar intensity, individuals with fibromyalgia showed higher activation in pain-related areas (operculo-insular regions, anterior cingulate cortex, basal ganglia, parietal cortex) and motor areas (motor cortices, supplementary motor area, cerebellum) compared to controls, and rated the stimulation as more painful (67). In studies in which subjective pain intensity was matched rather than the noxious stimuli (leading to lower stimuli applied in participants with fibromyalgia), individuals with fibromyalgia displayed higher activation of pain-related regions including the primary and secondary somatosensory cortices (68, 69), the anterior insula (67), the anterior cingulate cortex (69), and motor regions such as the supplementary motor area and the basal ganglia (67). They also showed less activation of the thalamus (69) and reduced functional connectivity in the pain inhibitory network [between the anterior cingulate cortex and the amygdala, the hippocampi, and the brainstem and between the thalamus and the orbitofrontal cortex (70)], compared to controls. Moreover, in an event-related potentials study, the amplitude of laser-evoked potentials N170 and P390 was higher and broader at central and frontocentral electrodes in participants with fibromyalgia compared to controls (71).
Differences in cerebral activation evoked by non-noxious stimuli were also observed between persons with fibromyalgia and healthy controls. Two studies using electroencephalography, one studying event-related potentials and the other oscillation frequencies, showed divergences between the cerebral responses of the two groups (72, 73). Montoya et al. (72) found that the same non-noxious pressure stimulation elicited lower event-related potentials in the primary somatosensory cortex in the fibromyalgia group while Fallon et al. (73) identified a suppression of beta oscillations in individuals with fibromyalgia in the primary and secondary somatosensory cortices, and the insula. However, the detection of the non-noxious stimulations was not measured in these studies. In a functional magnetic resonance imaging study, Cook et al. (74) assessed the detection of warmth in participants with fibromyalgia and healthy controls. They reported no differences between the groups at the behavioral level but found more activation in the anterior cingulate cortex, the insula, the prefrontal cortex, and the supplementary motor area during the stimulation in the fibromyalgia group. These results suggest an amplified cerebral response to noxious and non-noxious stimuli in fibromyalgia, which, for the latter, is not necessarily accompanied by a decreased perceptual threshold. Although it might appear contradictory, it is important to keep in mind that the detection of the stimulus is only one of many steps in the processing of somatosensory stimuli.
In the present study a trend toward hyperalgesia was detected. Contrary to our expectations, no hyperesthesia was observed; in fact, if anything, the trend for abnormal sensitivity to non-noxious stimulations was in the opposite direction, that is toward hypoesthesia. This is consistent with the generalized hypervigilance hypothesis, which claims that persons with fibromyalgia allocate more attention to aversive and noxious stimuli (75–77). It was born as an explanation for studies reporting heightened perception of various aversive stimuli [pressure (78, 79), thermal (22), auditory, and visual (80)] in individuals with fibromyalgia and could lead to amplified perceived pain intensity and frequency (81, 82).
However, studies assessing allocation of attention on aversive stimuli reported conflicting results. Gonzalez et al. (83) examined attentional allocation to aversive non-somatosensory stimulations in an emotional Stroop task and reported that participants with fibromyalgia displayed a tendency to allocate more attention (i.e., they were slower at reading the colors of the words) to negative words and words characterizing fibromyalgia symptoms, related to positive words, but also showed a significant attentional bias to neutral words (vs. positive words), in comparison to controls; the attentional bias was therefore not specific to aversive stimuli and was generalized to neutral stimuli. On the other hand, in a dual task requiring the detection of noxious tactile stimuli and innocuous visual stimuli, Peters et al. (84) reported that participants with fibromyalgia were not better at detecting the noxious tactile stimuli compared to healthy participants and concluded that no alterations in attention were observed in this group.
The lack of altered sensitivity to non-noxious stimulations could indicate that alterations of unimodal processing of somatosensory information are not generalized to both noxious and non-noxious stimuli in individuals with fibromyalgia. Thus, the sensorimotor impairments (3–5) and distortions of body representations (6–10) observed in this syndrome cannot be explained only by perturbations of unimodal processing of somatosensory information. An important aspect to keep in mind is that only detection thresholds were assessed in this study. Therefore, alterations in higher level processes, such as multimodal processing, could still be altered. Further research on the integration of somatosensory information among other sensory and motor information in fibromyalgia could shed a light on these mechanisms. Another phase of unimodal processing could also be altered. Auld et al. (85) proposed a dissociation between tactile registration (i.e., “the initial awareness of sensory information”), measured by TDT and TPT; and tactile perception, which involves “processing registered stimuli to create an internal representation with understanding of spatial, temporal, and modality-specific characteristics” and is assessed with higher-level tasks including identifying an object by touching it (i.e., stereognosis) or localizing a tactile stimuli with eyes closed. Given this dissociation, alterations of tactile perception in fibromyalgia cannot be dismissed and future research on unimodal somatosensory processing should focus on this aspect.
The tests of heterogeneity concluded on significant divergences between the results of the studies of the meta-analysis. Heterogeneity in the clinical characteristics of individuals with fibromyalgia is a possible cause. In the studies included, average pain intensity ranged from mild [22.7/100; (34)] to severe [9/10; (59)], which indicates variations of severity across participants. To compensate for this variability, the fibromyalgia group was split into subgroups in two studies (31, 34). In the literature, no consensus for dividing individuals with fibromyalgia into subgroups exists and various criteria are used (86–88). Moreover, the present results encompass studies published over several decades, with different diagnostic criteria.
Differences in medication could also introduce a bias. Participants with fibromyalgia were instructed to stop taking their medication prior to their participation in less than half of the studies of the review [47%; (27, 30, 32, 33, 57, 59, 61–63)] and of the meta-analysis [42%; (32, 57, 59, 61, 62)]. Medication commonly used to alleviate fibromyalgia symptoms have been shown to reduce sensitivity to somatosensory stimuli (89–91) and to have an effect on cerebral activation of pain processes (91). However, for ethical reasons and to prevent a recruitment bias, the interruption of medication is not always the solution. Finally, discrepancies in the duration of the participation could have influenced the results. Some studies involved only a short QST [e.g., van Laarhoven et al. (37)] while others consisted of a long QST accompanied by other measures [e.g., Gerhardt et al. (61)]. These divergences could lead to disparities in attention and fatigue, and impact the obtained measures (92, 93).
This study has several limitations. Only nine and seven studies were included in the meta-analysis TPT and TDT, respectively. This was partly due to our inability to retrieve all missing data to calculate Cohen's d for each group comparison.
Additionally, to reduce the variability of our results and facilitate their interpretation, measures on the distal upper limb area only were included in the meta-analysis. This further reduced the number of studies included and prevents from generalizing the results to all body parts. However, even though various sites are comprised in this area (i.e., finger, thenar, dorsum of hand, wrist, forearm) and pertains to various dermatomes (94, 95), Cohen's d normalizes these discrepancies. Moreover, none of these sites are tender points.
In conclusion, the systematic review and meta-analysis show no alterations of detection of tactile stimulations in individuals with fibromyalgia, compared to healthy controls, apart from a trend toward hyperalgesia. Considering the heterogeneity of the studies, future research need to investigate whether alterations in higher-level processes, such as multimodal integration of sensory information, are present and could contribute to sensorimotor deficits and anomalies of body representation in fibromyalgia. Indeed, some recent studies point toward deficits in visuoproprioceptive integration in this syndrome (96, 97).
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
TA was supported by a fellowship from the Centre interdisciplinaire de recherche en réadaptation et integration sociale (Cirris) and CM was supported by an Emeritus salary award from the Fonds de la recherche Québec-Santé (grant no: #251649).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2021.740897/full#supplementary-material
FM, participants with fibromyalgia; HC, healthy controls; TDT, tactile detection threshold; TPT, tactile pain detection threshold.
1. Rusu C, Gee ME, Lagacé C, Parlor M. Chronic fatigue syndrome and fibromyalgia in Canada: Prevalence and associations with six health status indicators. Health Promotion Chronic Dis Prevent Canada. (2015) 35:3–11. doi: 10.24095/hpcdp.35.1.02
2. Branco JC, Bannwarth B, Failde I, Abello Carbonell J, Blotman F, Spaeth M, et al. Prevalence of fibromyalgia: A survey in five European countries. Semi Arthritis Rheumatism. (2010) 39:448–53. doi: 10.1016/j.semarthrit.2008.12.003
3. Heredia-Jimenez J, Orantes-Gonzalez E, Soto-Hermoso VM. Variability of gait, bilateral coordination, and asymmetry in women with fibromyalgia. Gait Posture. (2016) 45:41–4. doi: 10.1016/j.gaitpost.2016.01.008
4. Bennett R, Russell JI, Choy E, Spaeth M, Mease P, Kajdasz D, et al. Evaluation of patient-rated stiffness associated with fibromyalgia: a post-hoc analysis of 4 pooled, randomized clinical trials of duloxetine. Clin Therap. (2012) 34:824–37. doi: 10.1016/j.clinthera.2012.02.013
5. Jones KD, Horak FB, Winters-Stone K, Irvine JM, Bennett RM. Fibromyalgia is associated with impaired balance and falls. J Clin Rheumatol. (2009) 15:16–21. doi: 10.1097/RHU.0b013e318190f991
6. Martínez E, Aira Z, Buesa I, Aizpurua I, Rada D, Azkue JJ. Embodied pain in fibromyalgia : Disturbed somatorepresentations and increased plasticity of the body schema. PLoS ONE. (2018) 13:e0194534. doi: 10.1371/journal.pone.0194534
7. Martínez E, Guillen V, Buesa I, Azkue JJ. A distorted body schema and susceptibility to experiencing anomalous somatosensory sensations in fibromyalgia syndrome. Clin J Pain. (2019) 35:887–93. doi: 10.1097/AJP.0000000000000754
8. Akkaya N, Akkaya S, Atalay NS, Balci CS, Sahin F. Relationship between the body image and level of pain, functional status, severity of depression, and quality of life in patients with fibromyalgia syndrome. Clin Rheumatol. (2012) 31:983–8. doi: 10.1007/s10067-012-1965-9
9. Valenzuela-Moguillansky C. Pain and body awareness: An exploration of the bodily experience of persons suffering from fibromyalgia. Construct Found. (2013) 8:339–50.
10. Boyington J, Schoster B, Callahan L, Boyington JEA, Schoster B, Callahan LF. Comparisons of body image perceptions of a sample of black and white women with rheumatoid arthritis and fibromyalgia in the US. Open Rheumatol J. (2015) 9:1–7. doi: 10.2174/1874312901409010001
11. Dieguez S, Lopez C. The bodily self: Insights from clinical and experimental research. Ann Phys Rehabilitation Med. (2017) 60:198–207. doi: 10.1016/j.rehab.2016.04.007
12. Tsakiris M, Haggard P. The rubber hand illusion revisited: Visuotactile integration and self-attribution. J Experi Psychol. (2005) 31:80–91. doi: 10.1037/0096-1523.31.1.80
13. Cluff T, Crevecoeur F, Scott SH. A perspective on multisensory integration and rapid perturbation responses. Vision Res. (2015) 110:215–22. doi: 10.1016/j.visres.2014.06.011
14. Crevecoeur F, Munoz DP, Scott SH, Crevecoeur F, Munoz DP, Scott SH, et al. Dynamic multisensory integration: somatosensory speed trumps visual accuracy during feedback control. J Neurosci. (2016) 36:8598–611. doi: 10.1523/JNEUROSCI.0184-16.2016
15. Lebar N, Danna J, Moré S, Mouchnino L, Blouin J. On the neural basis of sensory weighting: Alpha, beta and gamma modulations during complex movements. NeuroImage. (2017) 150:200–12. doi: 10.1016/j.neuroimage.2017.02.043
16. Carillo-de-la-Peña MT, Triñanes Y, González-Villar A, Gómez-Perretta C, García-Larrea L. Filtering out repetitive auditory stimuli in fibromyalgia : A study of P50 sensory gating. Eur J Pain. (2014) 2014:1–9. doi: 10.1002/ejp.627
17. Choi W, Lim M, Kim JS, Chung CK. Habituation deficit of auditory N100m in patients with fibromyalgia. Eur J Pain. (2016) 20:1634–43. doi: 10.1002/ejp.883
18. Hollins M, Harper D, Gallagher S, Owings EW, Lim PF, Miller V, et al. Perceived intensity and unpleasantness of cutaneous and auditory stimuli: An evaluation of the generalized hypervigilance hypothesis. Pain. (2009) 141:215–21. doi: 10.1016/j.pain.2008.10.003
19. Wilbarger JL, Cook DB. Multisensory hypersensitivity in women with fibromyalgia: Implications for well being and intervention. Arch Phys Med Rehabilitation. (2011) 92:653–6. doi: 10.1016/j.apmr.2010.10.029
20. Geisser ME, Glass JM, Rajcevska LD, Clauw DJ, Williams DA, Kileny PR, et al. A psychophysical study of auditory and pressure sensitivity in patients with fibromyalgia and healthy controls. J Pain. (2008) 9:417–22. doi: 10.1016/j.jpain.2007.12.006
21. Schweinhardt P, Sauro KM, Bushnell MC. Fibromyalgia: A disorder of the brain? Neuroscientist. (2008) 14:415–21. doi: 10.1177/1073858407312521
22. Lautenbacher S, Rollman GB, McCain GA. Multi-method assessment of experimental and clinical pain in patients with fibromyalgia. Acta Anaesthesiol Scand. (1994) 51:582–6. doi: 10.1016/0304-3959(94)90046-9
23. Lautenbacher S, Rollman GB. Possible deficiencies of pain modulation in fibromyalgia. Clin J Pain. (1997) 13:189–96. doi: 10.1097/00002508-199709000-00003
24. Palmer S, Bailey J, Brown C, Jones A, McCabe CS. Sensory function and pain experience in arthritis, complex regional pain syndrome, fibromyalgia syndrome and healthy volunteers: a cross-sectional study. Clin J Pain. (2019) 35:894–900. doi: 10.1097/AJP.0000000000000751
25. Tampin B, Briffa NK, Slater H. Self-reported sensory descriptors are associated with quantitative sensory testing parameters in patients with cervical radiculopathy, but not in patients with fibromyalgia. Eur J Pain. (2013) 17:621–33. doi: 10.1002/j.1532-2149.2012.00227.x
26. Desmeules JA, Cedraschi C, Rapiti E, Baumgartner E, Finckh A, Cohen P, et al. Neurophysiologic evidence for a central sensitization in patients with fibromyalgia. Arthritis Rheumatism. (2003) 48:1420–9. doi: 10.1002/art.10893
27. Blumenstiel K, Gerhardt A, Rolke R, Bieber C, Tesarz J, Friederich HC, et al. Quantitative sensory testing profiles in chronic back pain are distinct from those in fibromyalgia. Clin J Pain. (2011) 27:682–90. doi: 10.1097/AJP.0b013e3182177654
28. Pfau DB, Rolke R, Nickel R, Treede RD, Daublaender M. Somatosensory profiles in subgroups of patients with myogenic temporomandibular disorders and fibromyalgia syndrome. Pain. (2009) 147:72–83. doi: 10.1016/j.pain.2009.08.010
29. Smith BW, Tooley EM, Montague EQ, Robinson AE, Cosper CJ, Mullins PG. Habituation and sensitization to heat and cold pain in women with fibromyalgia and healthy controls. Pain. (2008) 140:420–8. doi: 10.1016/j.pain.2008.09.018
30. Tampin B, Slater H, Hall T, Lee G, Briffa NK. Quantitative sensory testing somatosensory profiles in patients with cervical radiculopathy are distinct from those in patients with nonspecific neck-arm pain. Pain. (2012) 153:2403–14. doi: 10.1016/j.pain.2012.08.007
31. Hurtig IM, Raak RI, Kendall SA, Gerdle B, Wahren LK. Quantitative sensory testing in fibromyalgia patients and in healthy subjects: Identification of subgroups. Clin J Pain. (2001) 17:316–22. doi: 10.1097/00002508-200112000-00005
32. Crettaz B, Marziniak M, Willeke P, Young P, Hellhammer D, Stumpf A, et al. Stress-induced allodynia - evidence of increased pain sensitivity in healthy humans and patients with chronic pain after experimentally induced psychosocial stress. PLoS ONE. (2013) 8:e069460. doi: 10.1371/journal.pone.0069460
33. Lim M, Roosink M, Kim JS, Kim H, Lee EB, Son KM, et al. Augmented pain processing in primary and secondary somatosensory cortex in fibromyalgia: a magnetoencephalography study using intra-epidermal electrical stimulation. PLoS ONE. (2016) 11:e0151776. doi: 10.1371/journal.pone.0151776
34. Kaziyama HH, Barbour J, Galhardoni R, Aparecida da Silva V, de Siqueira SRDT, Listik C, et al. Sifting the wheat from the chaff? Evidence for the existence of an asymmetric fibromyalgia phenotype. Eur J Pain. (2020) 24:1635–47. doi: 10.1002/ejp.1620
35. Klauenberg S, Maier C, Assion HJ, Hoffmann A, Krumova EK, Magerl W, et al. Depression and changed pain perception: Hints for a central disinhibition mechanism. Pain. (2008) 140:332–43. doi: 10.1016/j.pain.2008.09.003
36. Evdokimov D, Frank J, Klitsch A, Unterecker S, Warrings B, Serra J, et al. Reduction of skin innervation is associated with a severe fibromyalgia phenotype. Ann Neurol. (2019) 86:504–16. doi: 10.1002/ana.25565
37. van Laarhoven AIM, Kraaimaat FW, Wilder-Smith OH, van de Kerkhof PCM, Cats H, van Riel PLCM, et al. Generalized and symptom-specific sensitization of chronic itch and pain. J Eur Acad Dermatol Venereol. (2007) 21:1187–92. doi: 10.1111/j.1468-3083.2007.02215.x
38. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. Criteria for the classification of fibromyalgia. Report of the multicenter criteria committee. Arthritis Rheumatism. (1990) 33:160–72. doi: 10.1002/art.1780330203
39. Staud R, Domingo MA. Evidence for abnormal pain processing in fibromyalgia syndrome. Pain Med. (2001) 2:208–15. doi: 10.1046/j.1526-4637.2001.01030.x
40. Staud R, Vierck CJ, Cannon RL, Mauderli AP, Price DD. Abnormal sensitization and temporal summation of second pain (wind-up) in patients with fibromyalgia syndrome. Pain. (2001) 91:165–75. doi: 10.1016/S0304-3959(00)00432-2
41. Kosek E, Ekholm J, Hansson P. Sensory dysfunction in fibromyalgia patients with implications for pathogenic mechanisms. Pain. (1996) 68:375–83. doi: 10.1016/S0304-3959(96)03188-0
42. Da Silva LA, Kaziyama HHS, Teixeira MJ, De Siqueira SRDT. Quantitative sensory testing in fibromyalgia and hemisensory syndrome: Comparison with controls. Rheumatol Int. (2013) 33:2009–17. doi: 10.1007/s00296-013-2675-6
43. Kosek E, Hansson P. Modulatory influence on somatosensory perception from vibration and heterotopic noxious conditioning stimulation (HNCS) in fibromyalgia patients and healthy subjects. Pain. (1997) 70:41–51. doi: 10.1016/S0304-3959(96)03295-2
44. Gibson SJ, Littlejohn GO, Gorman MM, Helme RD, Granges G. Altered heat pain thresholds and cerebral event-related potentials following painful CO2 laser stimulation in subjects with fibromyalgia syndrome. Pain. (1994) 58:185–93. doi: 10.1016/0304-3959(94)90198-8
45. Berglund B, Harju EL, Kosek E, Lindblom U. Quantitative and qualitative perceptual analysis of cold dysesthesia and hyperalgesia in fibromyalgia. Pain. (2002) 96:177–87. doi: 10.1016/S0304-3959(01)00443-2
46. Mücke M, Cuhls H, Radbruch L, Baron R, Maier C, Tölle T, et al. Quantitative sensorische Testung (QST). Schmerz. (2016) 2016:1–8. doi: 10.1007/978-3-662-46517-2_9
47. Berwick RJ, Siew S, Andersson DA, Marshall A, Goebel A. A systematic review into the influence of temperature on fibromyalgia pain: meteorological studies and quantitative sensory testing. J Pain. (2021) 22:473–86. doi: 10.1016/j.jpain.2020.12.005
48. Haggard P, Taylor-Clarke M, Kennett S. Tactile perception, cortical representation and the bodily self. Curr Biol. (2003) 13:170–3. doi: 10.1016/S0960-9822(03)00115-5
49. Ackerley R, Kavounoudias A. The role of tactile afference in shaping motor behaviour and implications for prosthetic innovation. Neuropsychologia. (2015) 79:192–205. doi: 10.1016/j.neuropsychologia.2015.06.024
50. Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D, Antes G, et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
51. Kmet LM, Lee RC, Cook LS. Standard quality assessment criteria for evaluating primary research papers from a variety of fields. HTA Initiative. (2004) 2004:1–22. doi: 10.7939/R37M04F16
52. Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. (2011) 64:401–6. doi: 10.1016/j.jclinepi.2010.07.015
53. Gwet K. Handbook of Inter-Rater Reliability Fourth Edition. Gaithersburg, MD: Advanced Analytics, LLC. (2014). doi: 10.1002/9781118445112.stat06882
54. Cohen J. Statistical Power for the Behavioral Sciences (2nd Edition). Hillsdale, NJ: Laurence Erlbaum and Associates (1988).
55. Berkey CS, Hoaglin DC, Mosteller F, Colditz GA. A random-effects regression model for meta-analysis. Statistics Med. (1995) 14:395–411. doi: 10.1002/sim.4780140406
56. Cochran WG. The Combination of Estimates from Different Experiments Published by : International Biometric Society Stable URL : http://www.jstor.org/stable/3001666 REFERENCES Linked references are available on JSTOR for this article : You may need to log in to JSTOR. Biometrics. (1954) 10:101–29. doi: 10.2307/3001666
57. Carli G, Suman AL, Biasi G, Marcolongo R. Reactivity to superficial and deep stimuli in patients with chronic musculoskeletal pain. Pain. (2002) 100:259–69. doi: 10.1016/S0304-3959(02)00297-X
58. Martínez-Jauand M, Sitges C, Rodríguez V, Picornell A, Ramon M, Buskila D, et al. Pain sensitivity in fibromyalgia is associated with catechol-O- methyltransferase (COMT) gene. Eur J Pain. (2013) 17:16–27. doi: 10.1002/j.1532-2149.2012.00153.x
59. De Siqueira SRDT, Teixeira MJ, De Siqueira JTT. Orofacial pain and sensory characteristics of chronic patients compared with controls. Oral Surg Oral Med Oral Pathol Oral Radiol. (2013) 115:e37–45. doi: 10.1016/j.oooo.2013.02.014
60. Hilgenberg-Sydney PB, Kowacs PA, Conti PCR. Somatosensory evaluation in dysfunctional syndrome patients. J Oral Rehabilitation. (2016) 43:89–95. doi: 10.1111/joor.12344
61. Gerhardt A, Eich W, Janke S, Leisner S, Treede RD, Tesarz J. Chronic widespread back pain is distinct from chronic local back pain. Clin J Pain. (2016) 32:568–79. doi: 10.1097/AJP.0000000000000300
62. Eken A, Gökçay D, Yilmaz C, Baskak B, Baltaci A, Kara M. Association of fine motor loss and allodynia in fibromyalgia: An fNIRS study. J Motor Behav. (2018) 50:664–76. doi: 10.1080/00222895.2017.1400947
63. Burgmer M, Pfleiderer B, Maihöfner C, Gaubitz M, Wessolleck E, Heuft G, et al. Cerebral mechanisms of experimental hyperalgesia in fibromyalgia. Eur J Pain. (2012) 16:636–47. doi: 10.1002/j.1532-2149.2011.00058.x
64. Cornsweet TN. The staircase-method in psychophysics. Am J Psychol. (1962) 75:485–91. doi: 10.2307/1419876
65. Coppieters I, Meeus M, Kregel J, Caeyenberghs K, De Pauw R, Goubert D, et al. Relations between brain alterations and clinical pain measures in chronic musculoskeletal pain: a systematic review. J Pain. (2016) 17:949–62. doi: 10.1016/j.jpain.2016.04.005
66. Lee YC, Nassikas NJ, Clauw DJ. The role of the central nervous system in the generation and maintenance of chronic pain in rheumatoid arthritis, osteoarthritis and fibromyalgia. Arthritis Res Ther. (2011) 13:3306. doi: 10.1186/ar3306
67. Pujol J, López-Solà M, Ortiz H, Vilanova JC, Harrison BJ, Yücel M, et al. Mapping brain response to pain in fibromyalgia patients using temporal analysis of fMRI. PLoS ONE. (2009) 4:e05224. doi: 10.1371/journal.pone.0005224
68. Gracely RH, Petzke F, Wolf JM, Clauw DJ. Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheumatism. (2002) 46:1333–43. doi: 10.1002/art.10225
69. Bradley LA, McKendree-Smith NL, Alberts KR, Alarcón GS, Mountz JM, Deutsch G. Use of neuroimaging to understand abnormal pain sensitivity in fibromyalgia. Curr Rheumatol Rep. (2000) 2:141–8. doi: 10.1007/s11926-000-0054-2
70. Jensen KB, Loitoile R, Kosek E, Petzke F, Carville S, Fransson P, et al. Patients with fibromyalgia display less functional connectivity in the brain's pain inhibitory network. Mol Pain. (2012) 8:1–9. doi: 10.1186/1744-8069-8-32
71. Lorenz J, Grasedyck K, Bromm B. Middle and long latency somatosensory evoked potentials after painful laser stimulation in patients with fibromyalgia syndrome. Electroencephalography Clin Neurophysiol. (1996) 100:165–8. doi: 10.1016/0013-4694(95)00259-6
72. Montoya P, Sitges C, García-Herrera M, Rodríguez-Cotes A, Izquierdo R, Truyols M, et al. Reduced brain habituation to somatosensory stimulation in patients with fibromyalgia. Arthritis Rheumatism. (2006) 54:1995–2003. doi: 10.1002/art.21910
73. Fallon N, Chiu YH, Li X, Nurmikko TJ, Stancak A. Ipsilateral cortical activation in fibromyalgia patients during brushing correlates with symptom severity. Clin Neurophysiol. (2013) 124:154–63. doi: 10.1016/j.clinph.2012.06.014
74. Cook DB, Lange G, Ciccone DS, Liu WC, Steffener J, Natelson BH. Functional imaging of pain in patients with primary fibromyalgia. J Rheumatol. (2004) 31:364–78.
75. McDermid AJ, Rollman GB, McCain GA. Generalized hypervigilance in fibromyalgia: Evidence of perceptual amplification. Pain. (1996) 66:133–44. doi: 10.1016/0304-3959(96)03059-X
76. Rollman GB, Lautenbacher S. Hypervigilance effects in fibromyalgia: pain experience and pain perception. Prog Fibromyalgia Myofascial Pain. (1993) 1985:149–59.
77. Chapman CR. Pain: The perception of noxious events. In: Sternbach RA, editor. The Psychology of Pain. New York, NY: Raven Press (1978).
78. Smythe H. Tender points: Evolution of concepts of the fibrositis/fibromyalgia syndrome. Am J Med. (1986) 81:2–6. doi: 10.1016/0002-9343(86)90865-X
79. Scudds RA, Rollman GB, Harth M, McCain GA. Pain perception and personality measures as discriminators in the classification of fibrositis. J Rheumatol. (1986) 14:563–70.
80. Waylonis GW, Heck W. Fibromyalgia syndrome: New associations. Am J Phys Med Rehabilitation. (1992) 71:343–8. doi: 10.1097/00002060-199212000-00006
81. Ferguson RJ, Ahles TA. Private body consciousness, anxiety and pain symptom reports of chronic pain patients. Behav Res Ther. (1998) 36:527–35. doi: 10.1016/S0005-7967(98)00048-5
82. Ahles TA, Cassens HL, Stalling RB. Private body consciousness, anxiety and the perception of pain. J Behav Ther Experi Psychiatry. (1987) 18:215–22. doi: 10.1016/0005-7916(87)90003-6
83. González JL, Mercado F, Barjola P, Carretero I, López-López A, Bullones MA, et al. Generalized hypervigilance in fibromyalgia patients: An experimental analysis with the emotional Stroop paradigm. J Psychosomatic Res. (2010) 69:279–87. doi: 10.1016/j.jpsychores.2010.05.002
84. Peters ML, Vlaeyen JWS, Van Drunen C. Do fibromyalgia patients display hypervigilance for innocuous somatosensory stimuli? Application of a body scanning reaction time paradigm. Pain. (2000) 86:283–92. doi: 10.1016/S0304-3959(00)00259-1
85. Auld ML, Boyd RN, Moseley GL, Johnston LM. Tactile assessment in children with cerebral palsy: A clinimetric review. Phys Occupat Ther Pediatrics. (2011) 31:413–39. doi: 10.3109/01942638.2011.572150
86. Wilson HD, Starz TW, Robinson JP, Turk DC. Heterogeneity within the fibromyalgia population: Theoretical implications of variable tender point severity ratings. J Rheumatol. (2009) 36:2795–801. doi: 10.3899/jrheum.090432
87. Yim YR, Lee KE, Park DJ, Kim SH, Nah SS, Lee JH, et al. Identifying fibromyalgia subgroups using cluster analysis: Relationships with clinical variables. Eur J Pain. (2017) 21:374–84. doi: 10.1002/ejp.935
88. Bartley EJ, Robinson ME, Staud R. Pain and fatigue variability patterns distinguish subgroups of fibromyalgia patients. J Pain. (2018) 19:372–81. doi: 10.1016/j.jpain.2017.11.014
89. Wodehouse T, Poply K, Ramaswamy S, Snidvongs S, Bourke J, Tahir H, et al. A pilot study investigating whether quantitative sensory testing alters after treatment in patients with fibromyalgia. Br J Pain. (2018) 12:250–6. doi: 10.1177/2049463718776336
90. Acet G. The comparation of the effectiveness of amitriptilin and pregabalin treatment in fibromyalgia patients. Northern Clin Istanbul. (2017) 4:151–9. doi: 10.14744/nci.2017.61687
91. Petzke F, Jensen KB, Kosek E, Choy E, Carville S, Fransson P, et al. Using fMRI to evaluate the effects of milnacipran on central pain processing in patients with fibromyalgia. Scand J Pain. (2013) 4:65–74. doi: 10.1016/j.sjpain.2012.10.002
92. Villemure C, Bushnell MC. Cognitive modulation of pain: How do attention and emotion influence pain processing? Pain. (2002) 95:195–9. doi: 10.1016/S0304-3959(02)00007-6
93. Dailey DL, Keffala VJ, Sluka KA. Do cognitive and physical fatigue tasks enhance pain, cognitive fatigue, and physical fatigue in people with fibromyalgia? Arthritis Care Res. (2015) 67:288–96. doi: 10.1002/acr.22417
94. Ackerley R, Carlsson I, Olausson H, Backlund Wasling H, Wester H, Olausson H, et al. Touch perceptions across skin sites: Differences between sensitivity, direction discrimination and pleasantness. Front Behav Neurosci. (2014) 8::54. doi: 10.3389/fnbeh.2014.00054
95. Craig JC, Lyle KB. A comparison of tactile spatial sensitivity on the palm and fingerpad. Perception Psychophysics. (2001) 63:337–47. doi: 10.3758/BF03194474
96. Brun C, McCabe CS, Mercier C. The contribution of motor commands to the perturbations induced by sensorimotor conflicts in fibromyalgia. Neuroscience. (2020) 434:55–65. doi: 10.1016/j.neuroscience.2020.03.017
Keywords: chronic pain, somatosensory, quantitative sensory testing, touch, integration
Citation: Augière T, Desjardins A, Paquette Raynard E, Brun C, Pinard AM, Simoneau M and Mercier C (2021) Tactile Detection in Fibromyalgia: A Systematic Review and a Meta-Analysis. Front. Pain Res. 2:740897. doi: 10.3389/fpain.2021.740897
Received: 13 July 2021; Accepted: 29 November 2021;
Published: 24 December 2021.
Edited by:
Trine Andresen, Molecular Diagnostic and Clinical Research Unit, DenmarkReviewed by:
Antti Pertovaara, University of Helsinki, FinlandCopyright © 2021 Augière, Desjardins, Paquette Raynard, Brun, Pinard, Simoneau and Mercier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catherine Mercier, Y2F0aGVyaW5lLm1lcmNpZXJAcmVhLnVsYXZhbC5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.